Back to Journals » Advances in Medical Education and Practice » Volume 16
Evaluating Unstructured Clinical Teaching During Rotations: How Medical Students’ Experiences in Paediatrics and Gynaecology Influence Perceived Learning Outcomes
Authors Hannula V ![]() , Lehtovirta L, Kourunen L, Sumanen M
, Lehtovirta L, Kourunen L, Sumanen M
Received 16 February 2025
Accepted for publication 20 June 2025
Published 31 July 2025 Volume 2025:16 Pages 1297—1304
DOI https://doi.org/10.2147/AMEP.S523181
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Verneri Hannula,1,2 Lari Lehtovirta,1 Linda Kourunen,1 Markku Sumanen1
1Faculty of Medicine and Health Technology, Tampere University, Tampere, Finland; 2Tampere University Hospital, The Wellbeing Services County of Pirkanmaa, Tampere, Finland
Correspondence: Markku Sumanen, Email [email protected]
Objective: Learning in the clinical environment is crucial for students to enhance practical skills. However, due to the variability of clinical settings, providing consistent teaching and sufficient patient cases can be challenging. As a result, the perceived quality of rotations often varies. Previous studies have reported mixed findings on whether teaching quality or patient encounters influence students’ perceptions of rotation quality or exam performance. Additionally, previous studies have often focused on structured teaching in clinical settings. We aimed to explore how students’ evaluations of clinical teaching outside structured learning events during rotations impact the perceived achievement of learning goals.
Methods: We analysed student evaluations from paediatric and gynaecology rotations at Tampere University Medical School during the 2021– 2022 academic year. Evaluations covered clinical teaching quality, opportunities to examine patients, and perform procedures. A linear regression model was used to assess the influence of these factors on the perceived achievement of learning goals, with the statement “I achieved the given learning goals” as the dependent variable.
Results: A total of 140 students evaluated the paediatric and 142 the gynaecology rotations, providing 833 and 1188 evaluations, respectively. All questions received mean scores above 5 on a 7-point scale. The mean for achieving learning goals was 5.6 for paediatrics and 5.7 for gynaecology. All independent variables showed significant associations with the dependent variable, with “The use of time was meaningful” having the greatest impact.
Conclusion: Students generally reported successfully achieving their learning goals in both rotations. Notably, the perceived meaningful use of time had the greatest impact on the perceived achievement of learning outcomes.
Keywords: clinical teaching, paediatrics, gynaecology, undergraduate medical education, rotation
Introduction
Learning in the clinical environment is essential, as it allows students to apply theoretical knowledge in practice and deepen both their knowledge and practical skills.1,2 Additionally, it provides opportunities for students to develop their professional identity.1 While medical school education has been systematically developed, the development of clinical teaching has been more arbitrary.3
Likewise, teaching in the clinical environment is often haphazard.4 Students learn from a variety of supervisors, and the patient mix can vary significantly.5 Learning is dictated by the availability of patients and the nature of their cases.6,7 Additionally, patient consent is required, and not all patients are willing to have students involved in their care.3 Therefore, securing enough patient cases for practice can be challenging, and addressing specific learning objectives may be even more difficult.
The clinical environment presents several challenges for students. Placements can range from a few hours to several weeks, and students often find themselves in unfamiliar settings, with staff and practices they do not know.8 The perceived quality of teaching and patient volume can vary across clinical placements.5,9 Moreover, clinical placements often include non-instructive time for students, which, in some cases, can account for up to 20% of the total time.10 In addition, the role of the students is often marginal, and they may fear hindering the workflow.8 However, a willingness from healthcare staff to teach can help overcome those barriers.
Previous studies have examined how teaching quality and patient volume impact evaluations of clinical placements and students’ exam scores.10–14 While some research suggests that teaching quality and patient volume are linked to positive evaluations of clinical placements,15 the evidence on their effect on students’ exam scores is mixed.5,13,16,17 In addition, studies have primarily focused on doctor educators, often neglecting the teaching provided by other healthcare professionals.18
There is evidence of differences and the influence of various factors on effective teaching in clinical education.19 Among the teaching and learning factors with the largest effect sizes, learning goal setting stands out.19 However, most of the other identified and ranked factors are not directly applicable outside of structured learning activities in clinical placements. In Finland, undergraduate medical education follows common learning objectives that are partially aligned with the international CanMEDS and Tomorrow’s Doctors frameworks.20–22
Previous studies have often focused on structured teaching within clinical settings, while findings related to unstructured learning have been inconsistent. Therefore, we aimed to investigate how students’ perceptions of clinical teaching outside structured learning activities during their clinical placements influence their perceived achievement of learning goals.
Our research questions were:
- How do students evaluate various aspects of their clinical placements?
- How do these evaluations affect perceived achievement of the learning goals?
Methods
The study was conducted at Tampere University Medical School, focusing on all student evaluations from paediatric and gynaecology rotations during the 2021–2022 academic year. Both rotations lasted nine weeks and included multiple clinical placements where students learned alongside clinicians. The duration of these placements ranged from one day to two weeks, with specific learning goals defined by the medical school as part of the formal curriculum for each placement. Therefore, each placement has a framework outlining what should be taught to the students. However, as clinicians change, the teaching also varies. The Degree Planning Committee of the medical school uses students’ evaluations to assess and improve both the clinical rotations and their individual placements.
While students also participated in teaching activities specifically arranged by the university, this study concentrated on learning in clinical settings and excluded evaluations of these teaching activities. Depending on their individual schedules, students participated in the paediatric and gynaecology rotations during either the spring of their fourth year or the fall of their fifth year. By including evaluations from both the spring and fall semesters, we captured responses from students at different phases of their studies. Completing evaluations for the rotations was mandatory. Hence, in practice, our study included students who participated in either or both rotations. A few students did not complete their evaluations before data collection, and therefore their responses were not included.
Evaluations were collected using Google Forms, with students providing separate evaluations for each placement they attended during the rotation. The paediatric rotation included six different placements, while the gynaecology rotation included nine. Not all students participated in every placement.
Students rated their experiences on a scale from 1 to 7, where 1 indicated “very bad” and 7 indicated “very good”. The questions were:
- Teaching provided by hospital doctors
- Doctors’ willingness to teach
- Teaching provided by healthcare staff (only in paediatrics)
- Healthcare staff’s willingness to teach
- I had enough opportunities to examine patients
- I had enough opportunities to perform procedures (only in gynaecology)
- The use of time was meaningful
- I achieved the given learning goals
Data Analysis
The evaluation data were left-skewed, so both medians and means were calculated for each question separately. Our specific interest laid in students’ achievement of their learning goals. We hypothesised that other aspects influence the perceived fulfilment of the learning goals. Consequently, we constructed a linear regression model in which “I achieved the given learning goals” was the dependent variable. Although the outcome variable was measured on a 7-point ordinal scale, it was treated as continuous in the linear regression models, in line with common practice. The normality of residuals was assessed and deemed sufficiently met for the purposes of this analysis. Both univariable and multivariable regression analyses were conducted.
Since our primary research interest was at the course level rather than the level of individual placements, we pooled all responses from the different placements separately for both paediatrics and gynaecology rotations. The structure and learning goals of the placements were similar enough to justify pooling responses for each course.
To avoid multicollinearity in the regression models, we examined the correlations among the independent variables. There was a strong correlation between the questions “teaching provided by hospital doctors” and “doctors’ willingness to teach”, as well as between the questions “teaching provided by healthcare staff” and “healthcare staffs’ willingness to teach” (in paediatrics), and between “I had enough opportunities to examine patients” and “I had enough opportunities to perform procedures” (in gynaecology). Due to the observed correlations, we combined these items into composite sum variables, which were then used as independent variables in the regression models. All predictors in both models had variance inflation factors (VIFs) below 4. Additionally, we examined the effect of the semester within the model.
We conducted the analysis using SPSS version 29, considering results statistically significant if P<0.05. Additionally, we calculated 95% confidence intervals. Standardized beta coefficients were interpreted as measures of effect size. Values between 0.10 and 0.29 were considered small, between 0.30 and 0.49 as medium, and 0.50 or greater as large.23
Results
A total of 140 students evaluated the paediatric rotation during the 2021‒2022 academic year, with 71 (51%) participating in the fall of 2021 and 69 (49%) in the spring of 2022. Collectively, students provided 833 evaluations across the six placements. Similarly, 142 students evaluated the gynaecology rotation, with 72 (51%) during the fall of 2021 and 70 (49%) in the spring of 2022. In total, students submitted 1188 evaluations across the nine placements.
Figure 1 illustrates the means and standard errors calculated from students’ evaluations for various questions. Overall, evaluations were positive, with all questions receiving mean scores above 5 (on a scale from 1 to 7) in both fields. Notably, the means for the question “I achieved the given learning goals” were 5.6 for paediatrics and 5.7 for gynaecology. Gynaecology slightly outperformed paediatrics in all questions except for “teaching provided by hospital doctors”. The median scores for the questions “teaching provided by healthcare staff” and “I had enough opportunities to examine patients” in paediatrics were both 5, while the median scores for all other questions in both rotations were 6.
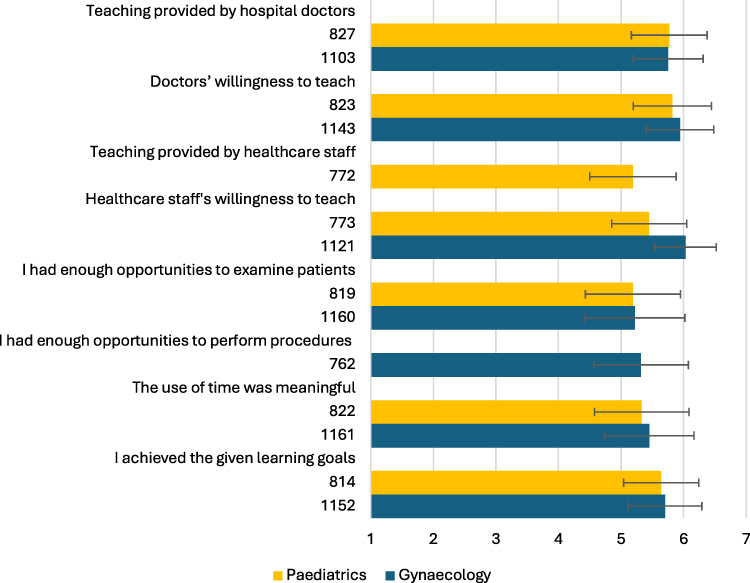 |
Figure 1 Students’ evaluations of teaching, learning opportunities, and achievement of learning goals in paediatrics (yellow) and gynaecology (blue) rotations. Mean values and standard errors are shown for each item, rated on a 1–7 scale (1 = very bad, 7 = very good). The numbers below each item indicate the absolute number of responses per rotation. |
Table 1 shows the results of the linear regression model constructed from evaluations of paediatric clinical placements. In the multivariable model, all independent variables, except for semester, demonstrated statistically significant associations with the dependent variable. The variable “The use of time was meaningful” had the greatest impact in the model (Standardized coefficients Beta = 0.29, p<0.001).
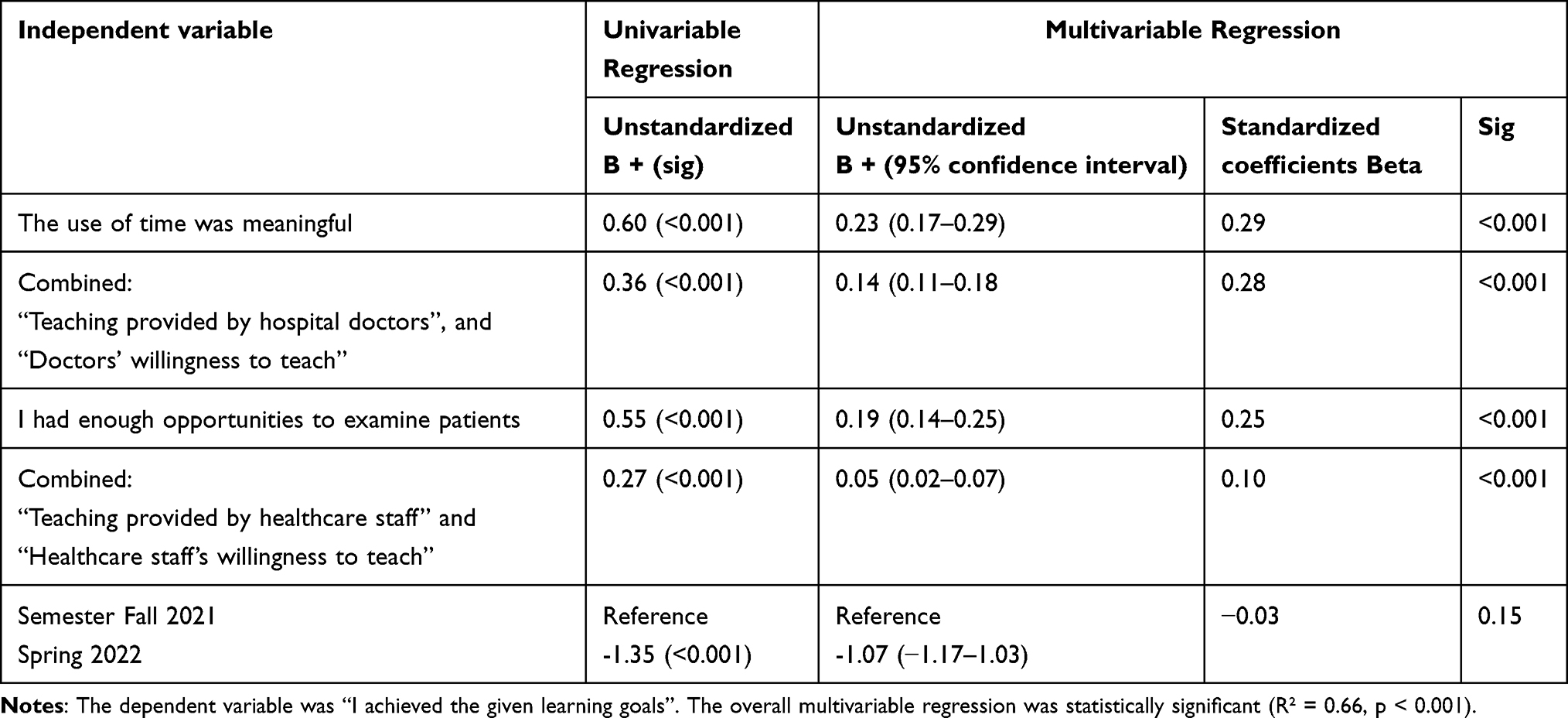 |
Table 1 Linear Regression Model on Students’ Evaluations of Paediatric Clinical Placements (n = 760) |
Similarly, Table 2 presents the results of the linear regression model examining evaluations from gynaecology rotations. In the multivariable model, all independent variables were associated with the dependent variable. In this model, the variable “The use of time was meaningful” also had the greatest impact in the model (Standardized coefficients Beta = 0.40, p<0.001). However, the combined variable “teaching provided by hospital doctors” and “doctors’ willingness to teach” had a noticeably smaller impact in the gynaecology model compared to the paediatric model.
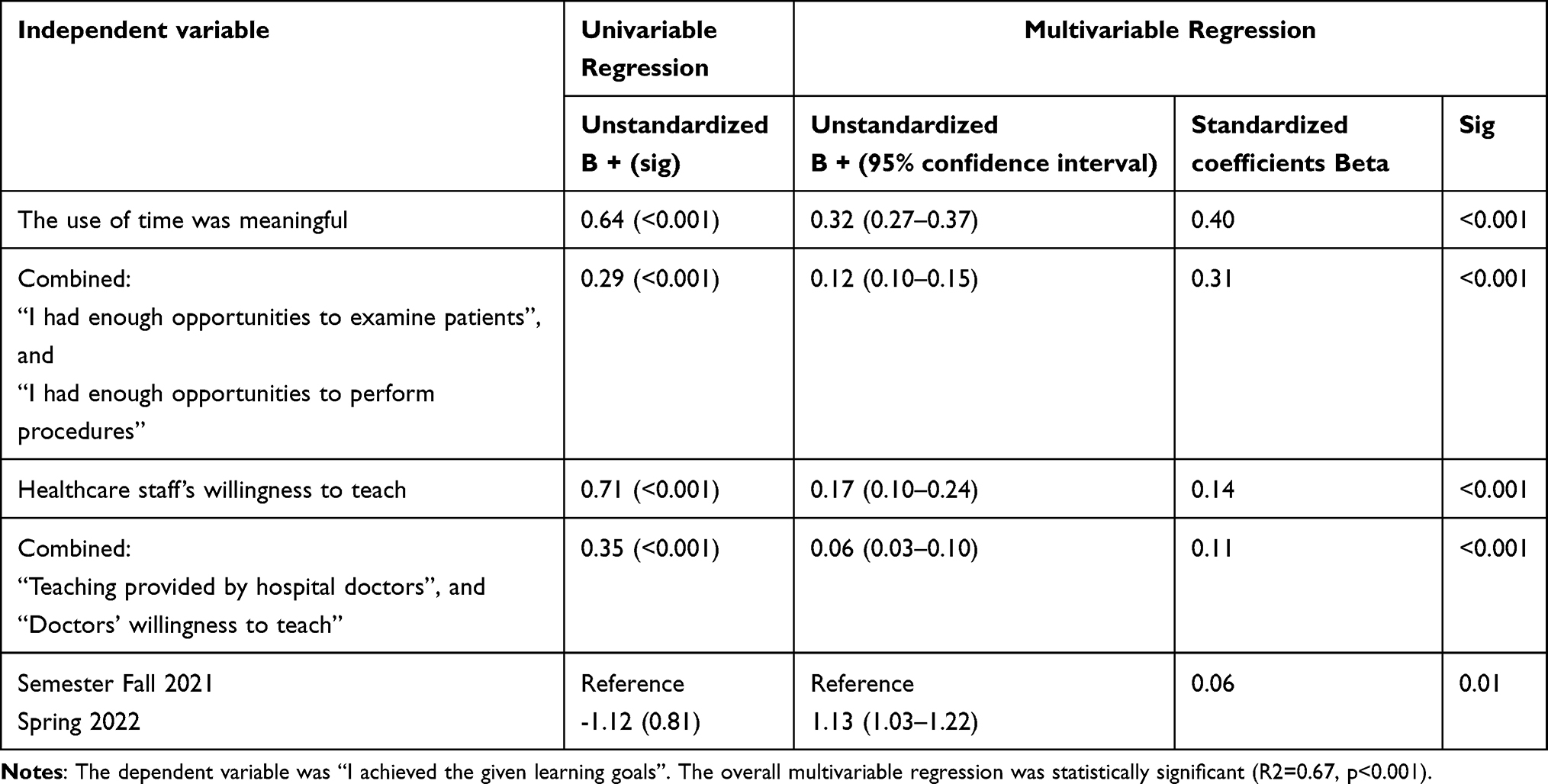 |
Table 2 Linear Regression Model on Students’ Evaluations of Gynaecology Clinical Placements (n = 717) |
Discussion
Overall, the clinical rotations in paediatrics and gynaecology received positive evaluations, with students indicating that they felt they had effectively achieved the given learning goals. Our study revealed that the question “the use of time was meaningful” had the greatest impact on perceived achievement of the learning goals, although its effect size was only medium in gynaecology and small in paediatrics. In gynaecology, the quality of teaching by doctors and their willingness to teach did not correspond to learning goals as strongly as in paediatrics.
The finding that meaningful use of time had the greatest impact on the achievement of learning goals aligns with previous research, which has indicated that the time spent in rotations does not directly correlate with students’ ratings of rotation effectiveness. Instead, the time spent in rotations, excluding reported non-instructive time, demonstrated a correlation with the perceived effectiveness.10 Likewise, another study found that time spent on self-directed consultations and observing doctors correlated with perceptions of learning environment quality.24 However, this study did not identify a correlation between unproductive time and evaluations.24 In another previous study, paediatrics and gynaecology/obstetrics rotations had the highest amount of non-instructive time.10 In general, clinical teaching guides recommend that physicians allow students to take on active roles according to their skill level.3,25 If the clinical situation is too busy for optimal learning or if opportunities for learning are limited, it may be more beneficial for the student to follow another professional or to be directed towards self-learning.6
Our finding that ratings for doctors’ teaching and willingness to teach significantly impacted the achievement of learning goals in the paediatrics rotation supports the conclusions of previous studies. An earlier study found that the quality of supervision had both a direct effect on students’ clinical competence, as measured through exams, and an influence on the number of patients encountered.5 When comparing students who worked with the best and worst-rated house staff during their medical clerkships, Griffith et al observed differences in performance tests.12 However, these differences were relatively small and varied according to the house staff’s training phase.12 Likewise, subsequent studies have produced inconsistent results regarding whether the teaching provided by residents or attending doctors has greater impact on students’ learning.13,16 Dolmans et al found that both the quality of supervision and the patient mix (including the number of patients and variety of diseases) affected students’ perceived quality of clinical rotations, however, whether the quality of supervision improves the diversity of patient mix has shown mixed findings.15,17
Our finding that the combined variable “doctors’ teaching and willingness to teach” had a noticeably lower impact in gynaecology compared to paediatrics is somewhat surprising, although the effect sizes were small in both models. However, the willingness of other healthcare professionals to teach was rated higher in gynaecology and received the best average evaluations across all questions. During the gynaecology rotation, students regularly work with midwives, particularly in maternity wards. It can be assumed that midwives are accustomed to teaching medical students and have developed strong teaching skills. Additionally, midwives have been previously recognised as excellent teachers.26 It is also encouraging that students rated the willingness of other health professionals to teach highly, as this factor had an even greater effect on achieving learning goals in gynaecology compared to the doctors’ teaching and willingness to teach.
In paediatrics, having a sufficient number of patients to examine had the third-largest impact on perceived fulfilment of the learning goals, although the effect size was small. In gynaecology, the number of patients examined, and procedures performed had a medium effect size and represented the second-largest impact in the model. Earlier, a study identifying weaknesses in poorly rated clinical supervision found that students expressed dissatisfaction with having too few opportunities to examine patients independently and practice clinical skills.27 Kim et al also found a small positive relationship between the number of patients interviewed and examined during clerkships and students’ examination scores.14 However, Wimmers et al did not find a direct relationship between the number of patients encountered and students’ clinical competence.5
In gynaecology, patients may refuse to allow medical students to perform physical or pelvic examinations, a situation that occurs more frequently with male students.28–30 This reluctance can sometimes be avoided if the patient is scheduled to see a male clinician for her care or has prior experience with medical students.28 In Sweden, there are trained “professional patients” who allow students to perform vaginal examinations and provide feedback.29 These professional patients offer a valuable way for students to practice real pelvic examinations, though they cannot fully substitute for all patient encounters.
A study that identified barriers to students performing pelvic examinations found that, compared to staff, students were more likely to perceive a lack of interest in teaching and limited opportunities to perform the examinations as obstacles.30
The differing results between paediatric and gynaecology placements may partly be explained by the distinct learning environments and objectives, which reflect the differences between conservative and operative fields. Patel and Dauphinee found that students perceived their learning experiences differently when comparing evaluations in surgery, internal medicine, and paediatrics.9 The acquisition of clinical skills was lower in paediatrics, while factual knowledge was higher.9 This suggests that both the learning goals and students’ perceptions may vary across different medical fields.
The small impact of the semester variable in gynaecology may be attributed to the differing experience levels between students in their fifth year (fall) and those in their fourth year (spring). Fifth-year students have more clinical rotation experience, and, in Finland, they are eligible to work as doctors for the first time during their summer break before fifth year studies. This additional experience may improve their ability to manage their own learning during rotations. However, the effect size of the semester was minimal compared to other variables in the model. Additionally, univariable analyses provided mixed results when compared to the multivariable regressions.
A previous meta-analysis found that several factors related to clinical teaching had large Cohen’s effect sizes in clinical education.19 However, factors such as small-group learning are not directly applicable to unstructured clinical learning.19 In our study, we were able to interpret the effect sizes of various aspects of unstructured clinical activities. Although direct comparison with the findings of the meta-analysis is not entirely appropriate, it is noteworthy that only two independent variables in gynaecology demonstrated medium effect sizes, while all others had smaller effects. Moreover, the differences in effect sizes among our independent variables were, in many cases, relatively minor.
Our study has several limitations. First, we only examined evaluations from one medical school and from two specific fields. Additionally, we did not directly assess the achievement of learning goals but instead relied on students’ self-reported evaluations. However, it is important to consider students’ self-assessments in evaluating educational outcomes. Furthermore, even though we combined certain variables for the regression models, some interrelations between variables likely remain. For instance, previous research found that the quality of supervision affected the number of patients encountered.5 It is important to note that some of the placements were short, and students were evaluating unstructured clinical learning experiences. This should be considered when interpreting the results.
As a strength of our study, almost all the students gave evaluations of the rotations. Therefore, one can assume the selection bias to be very low. Additionally, we had students from fourth and fifth grade, so we were able to identify if study phase had effect on learning goals achieved. Although there were only two fields, we were still capable of measuring the differences between those two.
Conclusions
Our study demonstrated that students generally felt they had successfully achieved their given learning goals in both paediatric and gynaecology rotations. Additionally, students provided positive evaluations for both rotations, with the statement “the use of time was meaningful” having the greatest impact on perceived achievement of the learning goals. Overall, the effect sizes in the models were generally small, and the differences between the effects of the independent variables were in some cases relatively minor.
These findings suggest that medical schools should aim to create a clinical learning environment where unproductive time is minimized, and students are given ample opportunities to examine patients outside of the structured teaching sessions in clinical settings. We found differences between rotations in how teaching by doctors and other healthcare professionals was associated with the achievement of learning goals. It may be beneficial to consider individually, for each rotation, on when students gain most from following doctors and when the involvement of other healthcare professionals can enhance learning. From a physician’s perspective, it is crucial to adopt an active teaching approach, encouraging student participation and facilitating patient examination opportunities. Future research could explore how a brief intervention on teaching methods for physicians in student training settings might impact the achievement of learning goals.
Data Sharing Statement
The datasets analysed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Ethics Approval
The study did not involve any patient data or personal information from the respondents. Researchers could not link specific responses to individual students, and the identities of the students were not disclosed to the researchers. Consequently, an ethical statement was not required according to national regulations. However, permission was obtained from the Degree Planning Committee of Tampere University Medical School.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Dr Verneri Hannula reports grants from The Finnish Medical Association, The Finnish Medical Society Duodecim, and General Practitioners in Finland, outside the submitted work. The authors have no other competing interests in this work.
References
1. Dornan T, Tan N, Boshuizen H, et al. How and what do medical students learn in clerkships? Experience based learning (ExBL). Adv Health Sci Educ. 2014;19(5):721–749. doi:10.1007/s10459-014-9501-0
2. Harden RM, Laidlaw JM. Be FAIR to students: four principles that lead to more effective learning. Med Teach. 2013;35(1):27–31. doi:10.3109/0142159X.2012.732717
3. Dornan T, Conn R, Monaghan H, Kearney G, Gillespie H, Bennett D. Experience based learning (ExBL): clinical teaching for the twenty-first century. Med Teach. 2019;41(10):1098–1105. doi:10.1080/0142159X.2019.1630730
4. Spencer J. Learning and teaching in the clinical environment. BMJ. 2003;326:591–594. doi:10.1136/bmj.326.7389.591
5. Wimmers PF, Schmidt HG, Splinter TAW. Influence of clerkship experiences on clinical competence. Med Educ. 2006;40(5):450–458. doi:10.1111/J.1365-2929.2006.02447.X
6. Sprake C, Cantillon P, Metcalf J, Spencer J. Teaching in an ambulatory care setting. BMJ. 2008;337:a1156. doi:10.1136/bmj.a1156
7. Irby DM, Bowen JL. Time-efficient strategies for learning and performance. Clin Teach. 2004;1(1):23–28. doi:10.1111/j.1743-498X.2004.00013.x
8. Liljedahl M, Björck E, Ponzer S, et al. Navigating without a map: how medical students interact with clinical learning environments. Stud Higher Educ. 2017. doi:10.1080/03075079.2017.1359822
9. Patel VL, Dauphinee WD. The clinical learning environments in medicine, paediatrics and surgery clerkships. Med Educ. 1985;19:54–60. doi:10.1111/j.1365-2923.1985.tb01139.x
10. Dolmans D, Wolfhagen I, Essed GG, Scherpbier AJ, Van Der Vleuten CP. Students’ perceptions of time spent during clinical rotations. Med Teach. 2001;23(5):471–475. doi:10.1080/01421590120075706
11. Durak HI, Vatansever K, Van Dalen J, Van Der Vleuten C. Factors determining students’ global satisfaction with clerkships: an analysis of a two year students’ ratings database. Adv Health Sci Educ Theory Pract. 2008;13(4):495–502. doi:10.1007/S10459-007-9061-7
12. Griffith CH, Wilson JF, Haist SA, Ramsbottom-Lucier M. Do students who work with better housestaff in their medicine clerkships learn more? Acad Med. 1998;73(10):57–59. doi:10.1097/00001888-199810000-00045
13. Roop SA, Pangaro L. Effect of clinical teaching on student performance during a medicine clerkship. Am J Med. 2001;110(3):205–209. doi:10.1016/S0002-9343(00)00672-0
14. Kim JY, Myung SJ. Could clinical experience during clerkship enhance students’ clinical performance? BMC Med Educ. 2014;14(209). doi:10.1186/1472-6920-14-209
15. Dolmans D, Wolfhagen I, Essed G, Scherpbier A, Van der Vleuten C. The impacts of supervision, patient mix, and numbers of students on the effectiveness of clinical rotations. Acad Med. 2002;77(4):332–335. doi:10.1097/00001888-200204000-00016
16. Stern DT, Williams BC, Gill A, Gruppen LD, Woolliscroft JO, Grum CM. Is there a relationship between attending physicians’ and residents’ teaching skills and students’ examination scores? Acad Med. 2000;75(11):1144–1146. doi:10.1097/00001888-200011000-00024
17. De Jong J, Visser M, Van Dijk N, Van Der Vleuten C, Wieringa-De Waard M. A systematic review of the relationship between patient mix and learning in work-based clinical settings. A BEME systematic review: BEME Guide No. 24. Med Teach. 2013;35(6):e1181–e1196. doi:10.3109/0142159X.2013.797570
18. Kandiah DA. Perception of educational value in clinical rotations by medical students. Adv Med Educ Pract. 2017;8:149–162. doi:10.2147/AMEP.S129183
19. Huang PH, Haywood M, O’Sullivan A, Shulruf B. A meta-analysis for comparing effective teaching in clinical education. Med Teach. 2019;41(10):1129–1142. doi:10.1080/0142159X.2019.1623386
20. Merenmies J, Jääskeläinen J, Kortekangas-Savolainen O, et al. Valmistuvan lääkärin osaamistavoitteet (Competency goals for graduating physicians). 2020. Available from: https://www.helsinki.fi/fi/laaketieteellinen-tiedekunta/opiskelu-ja-opetus/osaamistavoitteet/valmistuvan-laakarin-osaamistavoitteet.
21. Frank JR, Snell L, Sherbino J. Royal College:: Publications. CanMEDS 2015 Physician Competency Framework Ottawa: royal College of Physicians and Surgeons of Canada. 2015.
22. General Medical Council. Tomorrow’s Doctors; 2003.
23. Nieminen P. Application of Standardized Regression Coefficient in Meta-Analysis. BioMedInformatics. 2022;2(3):434–458. doi:10.3390/biomedinformatics2030028
24. Van Hell EA, Kuks JBM, Cohen-Schotanus J. Time spent on clerkship activities by students in relation to their perceptions of learning environment quality. Med Educ. 2009;43(7):674–679. doi:10.1111/J.1365-2923.2009.03393.X
25. Irby DM, Wilkerson L. Teaching when time is limited. BMJ. 2008;336(7640):384–387. doi:10.1136/bmj.39456.727199.AD
26. Cotter D, Turner MJ, McAuliffe FM, Higgins MF. Medical students learning experiences of the labour ward: a qualitative research study. Eur J Obstetrics Gynecol Reprod Biol. 2016;206:204–207. doi:10.1016/j.ejogrb.2016.09.022
27. Dolmans D, Wolfhagen I, Heineman E, Scherpbier A. Factors adversely affecting student learning in the clinical learning environment: a student perspective. Educ Health. 2008;20(3). doi:10.4103/1357-6283.101553
28. Nguyen BT, Streeter LH, Reddy RA, Douglas CR. Gender bias in the medical education of obstetrician-gynaecologists in the United States: a systematic review. Aust N Z J Obstetrics Gynaecol. 2022;62(3):349–357. doi:10.1111/ajo.13511
29. Danielsson J, Hadding C, Fahlström M, Ottander U, Lindquist D. Medical students’ experiences in learning to perform pelvic examinations: a mixed-methods study. Int J Med Educ. 2021;12:233–242. doi:10.5116/ijme.617f.b261
30. Bossé J, Woolcott C, Coolen J. Barriers preventing medical students from performing pelvic examinations during obstetrics and gynaecology clinical clerkship rotations. J Obstet Gynaecol Canada. 2019;41(8):1093–1098. doi:10.1016/j.jogc.2018.12.023
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.