")
Back to Journals » Open Access Emergency Medicine » Volume 15
Evaluating the Triage of Suspected COVID-19 Cases in Sudan’s Emergency Settings: A Clinical Audit
Authors Ibrahim BE , El-Amin RO , Abdulla STA
Received 1 August 2023
Accepted for publication 11 October 2023
Published 18 October 2023 Volume 2023:15 Pages 373—382
DOI https://doi.org/10.2147/OAEM.S433240
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Bayan E Ibrahim,* Rahba Osman El-Amin,* Safia Tarig Adam Abdulla*
Faculty of Medicine, University of Khartoum, Khartoum, Sudan
*These authors contributed equally to this work
Correspondence: Bayan E Ibrahim, Email [email protected]
Background: The inevitable coronavirus disease 2019 global pandemic has severely affected Sudan’s fragile healthcare system. The authors share the experience of COVID-19 triage in the emergency departments of five public hospitals in Khartoum state, Sudan.
Methods: A clinical audit was conducted in December 2020 using the Centers for Disease Control and Prevention Checklist and Monitoring Tool for Triage of Suspected COVID-19 Cases. The tool was categorised into 5 domains and 38 indicators.
Results: Only three hospitals had hand hygiene stations in their triage areas: Ibrahim Malik, Omdurman, and Al-Nau. Omdurman Teaching Hospital was the sole hospital with a designated respiratory waiting area. At Al-Nau and Omdurman Hospitals, all respiratory symptomatic patients wore a facemask or alternative. Ibrahim Malik and Bahri Teaching Hospitals had 60% and 50% compliance, respectively, while none at El-Tamayouz Hospital did. No posters or job aids were present in donning and doffing areas. Heavy duty gloves were worn only at Ibrahim Malik (50%) and Omdurman (20%). 100% of staff wore closed-toe footwear at Ibrahim Malik and Omdurman, 75% at El-Tamayouz, 63% at Bahri, and none at Al-Nau.
Conclusion: The healthcare facilities displayed significant shortcomings in preparedness and response to COVID-19, with variations across hospitals in infrastructure, human resources, and procedures. To better combat future outbreaks, systemic improvements and a focused approach on consistent staff training, standard triage algorithms, and adequate PPE availability are imperative.
Keywords: severe acute respiratory syndrome coronavirus 2, SARS‑CoV‑2, coronavirus disease 2019, COVID-19, triage, emergency departments, Sudan
Introduction
The global pandemic caused by the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), the novel virus responsible for coronavirus disease 2019 disease (COVID-19) has had an effect on the health systems at every level. The first wave of the pandemic reached sub-Saharan African (SSA) nations later, with peak infections occurring in July 2020. On March 13, 2020, Sudan, a country with a population of 46 million in SSA,1 reported its first COVID-19 case.2 During the second wave (from the period of October 22, 2020–February 28, 2021) a total of almost 17, 000 cases had been confirmed, with the highest number of confirmed cases appearing in Khartoum State.2 The majority of COVID-19 cases in Sudan that have been reported and brought in are thought to have originated in Khartoum, the country’s capital and primary international air travel centre.
The majority of tertiary healthcare facilities in Sudan are located in the capital, which is similar to other African nations where there are notable disparities in service distribution. Additionally, Sudan’s “public” healthcare system has no funding at all, making it unable to respond to a pandemic rapidly.3 As the methods of diagnosis were still unclear at the start of the pandemic, there were no local protocols or specific instructions on how to handle COVID-19 patients or suspected cases. The absence of a triage mechanism in hospitals made it difficult to distinguish patients with COVID-19 from those with other symptoms and illnesses.4,5 The absence of healthcare professionals (HCPs) to manage the services for the general population eventually prompted the closure of some healthcare facilities. Medicines and personal protective equipment (PPE) were also severely in short supply across the country.5,6 There was also an increase in room occupancy as a result of the full loss of continuity and flow inside these facilities, which raised the risk of nosocomial infection among hospital staff, uninfected co-patients, and other patients presenting with various health issues. Hospitals were not prepared enough to handle the COVID-19 pandemic, which resulted in unintentional HCP exposure, poor patient outcomes, and disruptions to the regular provision of vital healthcare services.7
The Federal Ministry of Health implemented the integration of COVID-19 preventative and control measures which included necessitating the establishment of triage systems in emergency settings, to lessen these hurdles and help contain the spread of COVID-19.8 Establishing an efficient triage is a critical initial step in emergency care during a pandemic, to enable healthcare professionals to rapidly assess patients’ conditions and allocate appropriate levels of care based on urgency while ensuring the safety of healthcare workers and other patients. Since there have been limited publications from Sub-Saharan African nations on their established triage systems and protocols for suspected COVID-19 cases,9–12 we aimed to evaluate the triage process for suspected COVID-19 cases in the emergency settings of Khartoum’s hospitals. Through a comprehensive clinical audit, this paper provides valuable insights into the strengths and weaknesses of the current triage systems in place for suspected COVID-19 cases in Sudan. By identifying areas that require improvement, healthcare organizations can refine their protocols to enhance patient safety, optimize resource allocation, and improve overall emergency department efficiency. Ultimately, this study aims to contribute to the ongoing efforts in combating the COVID-19 pandemic by ensuring that triage processes are effective in identifying and managing suspected cases in emergency settings. An updated COVID-19 hospital assessment tool was used to undertake an observational assessment of the Emergency departments (EDs) of five public hospitals in Khartoum, Sudan, to identify areas for improvement in the COVID-19 triage protocols.
Materials and Methods
Study Design and Setting
This was a cross-sectional study conducted throughout December 2020 in the emergency rooms (ERs) of general public hospitals in Khartoum state. All the hospitals with functioning isolation wards at the time of the study were included, these being Ibrahim Malik, Al-Nau, Omdurman, Bahri and El-Tamayouz Hospitals.
Data Collection
The data for this study was collected using the CDC Checklist and Monitoring Tool for Triage of Suspected COVID-19 Cases in Non-US Healthcare Settings to assess the COVID-19 triage.13 This tool is meant to help HCFs (Healthcare Facilities) in preventing the spread of COVID-19 among patients and HCPs. It can also be used to assist HCFs in monitoring the progress of implementing critical components of triage.
We categorised the checklist into five domains and under these domains were 38 indicators in total. The domains were: General, Triage area, Respiratory waiting area, Triage process and PPE. The following items were observed in the five hospitals for assessment:
General
- A phone number so patients could call in before presenting to the facility.
- The main emergency entrance has signs directing patients with respiratory symptoms to proceed directly to the registration desk;
- Signs on respiratory hygiene and cough etiquette are posted at the main emergency entrance, waiting area and by the elevators;
- Hand hygiene stations at the main emergency entrance.
Triage Area
- A separate registration desk for patients coming in with respiratory symptoms;
- Physical barriers between staff and patients (eg, plastic/glass window);
- Triage algorithm/questionnaires;
- Face masks for patients with respiratory symptoms;
- Tissue paper for patients with respiratory symptoms;
- Hand hygiene stations;
- Trash bins with a lid;
- Dedicated clinical staff assigned for triage;
- Dedicated clinical staff are trained on triage procedures and COVID-19 symptoms;
- Area cleaned and disinfected twice a day;
- Area cleaned and disinfected using 0.1% chlorine or 70% alcohol.
Respiratory Waiting Area
- A single room with a door;
- Area is well ventilated;
- Signage indicating “respiratory waiting area”;
- Signage on respiratory hygiene and cough etiquette;
- Chairs or benches are separated from each other by at least 1 m apart;
- Paper tissues;
- Hand hygiene stations;
- Trash bins with lids;
- Dedicated toilets;
- Patients are separated from each other by at least 1 m;
- Area cleaned and disinfected twice a day;
- Area cleaned and disinfected using 0.1% chlorine or 70% alcohol.
Triage Process
- Every patient is evaluated for respiratory symptoms;
- Triage staff use triage algorithm/questionnaire for every patient;
- Every patient with respiratory symptoms is wearing a facemask (or an alternative);
- Every patient that meets COVID-19 suspect case definition is immediately isolated/separated into “respiratory waiting area”.
- Facility has a policy to limit family members accompanying patients to the “respiratory waiting area”.
Personal Protective Equipment (PPE)
- Availability of PPE including: face masks, eye protection, gowns, gloves, heavy duty gloves, and boots;
- Staff are trained on proper PPE use, including donning and doffing;
- Separate PPE donning and doffing areas;
- Donning and doffing posters (or job aids) in PPE donning and doffing areas;
- Hand hygiene stations in PPE donning and doffing areas;
- HCWs conducting evaluations of patients with respiratory symptoms wear face masks, eye protection, gloves and gowns;
- Environmental service staff in triage, waiting and examination areas wear face masks, eye protection, heavy duty gloves, gowns and closed-toe shoes or boots.
The assessor conducted a thorough evaluation of the facility to determine its compliance with the specified criteria of the checklist. To ensure precision, the assessor adhered to the instructions provided in the checklist, categorizing each item as either “Yes” or “No”. Additionally, numerical values were recorded in the designated “# and Total #” columns, indicating the count of items that met the criteria out of the total number of items. To offer a comprehensive assessment, percentages were calculated in the “% column” by dividing the number of items meeting the criteria by the total number of items.
Data Analysis
After the entry of the obtained data into a Microsoft Excel file, descriptive analyses were conducted to characterise the COVID-19 triage status of the five ERs. Then the items that were answered with a yes/no were tabulated in a tick and cross format. Each indicator was given an arbitrary value of “one” and the percentage scores for each hospital across the five domains were calculated. A number of indicators necessitated that multiple objects or people be assessed; here, percentages of such items were calculated and described in the text.
Results
General Domain
Data on this domain are all provided in Table 1.
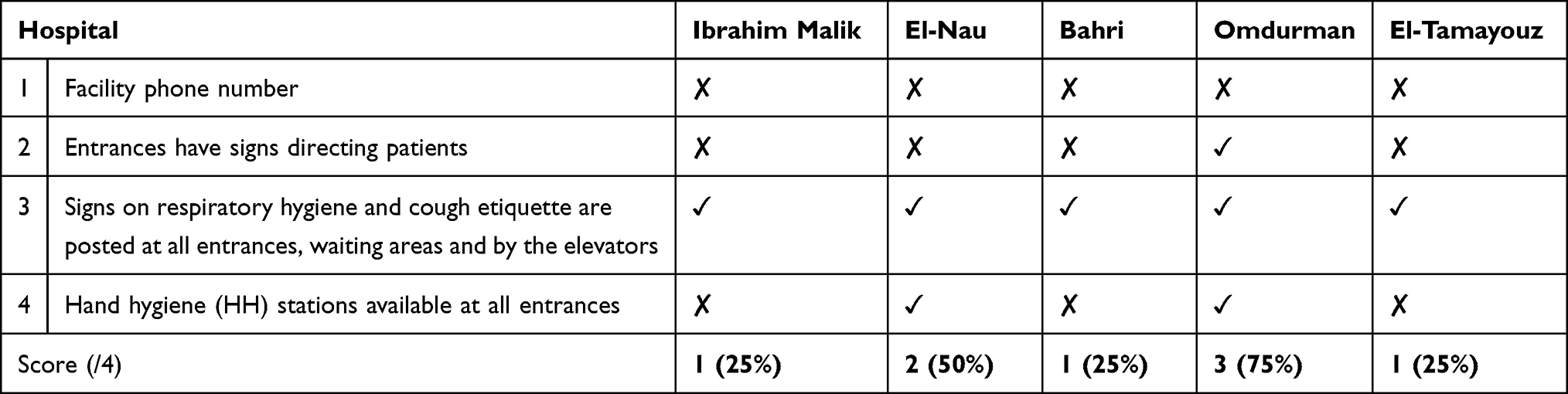 |
Table 1 Assessment of the General Domain at the Emergency Departments (EDs) (n = 5) |
Triage Area Domain
Hand Hygiene Stations
Only three hospitals had a hand hygiene station in their triage area, these being Ibrahim Malik, Omdurman and Al-Nau. Both Ibrahim Malik and Omdurman Teaching Hospitals had only one hand hygiene station, while Al-Nau Hospital had two. Fortunately, all the hand hygiene assessed in the three hospitals were found to be functioning.
Trash Bins
All the bins observed in this study had no lids.
Training of Dedicated Clinical Staff on Triage Procedures and COVID-19 Symptoms
In hospitals where training was available, all of the dedicated clinical staff were trained on triage procedures and COVID-19 symptoms.
Further data on the triage domain are provided in Table 2.
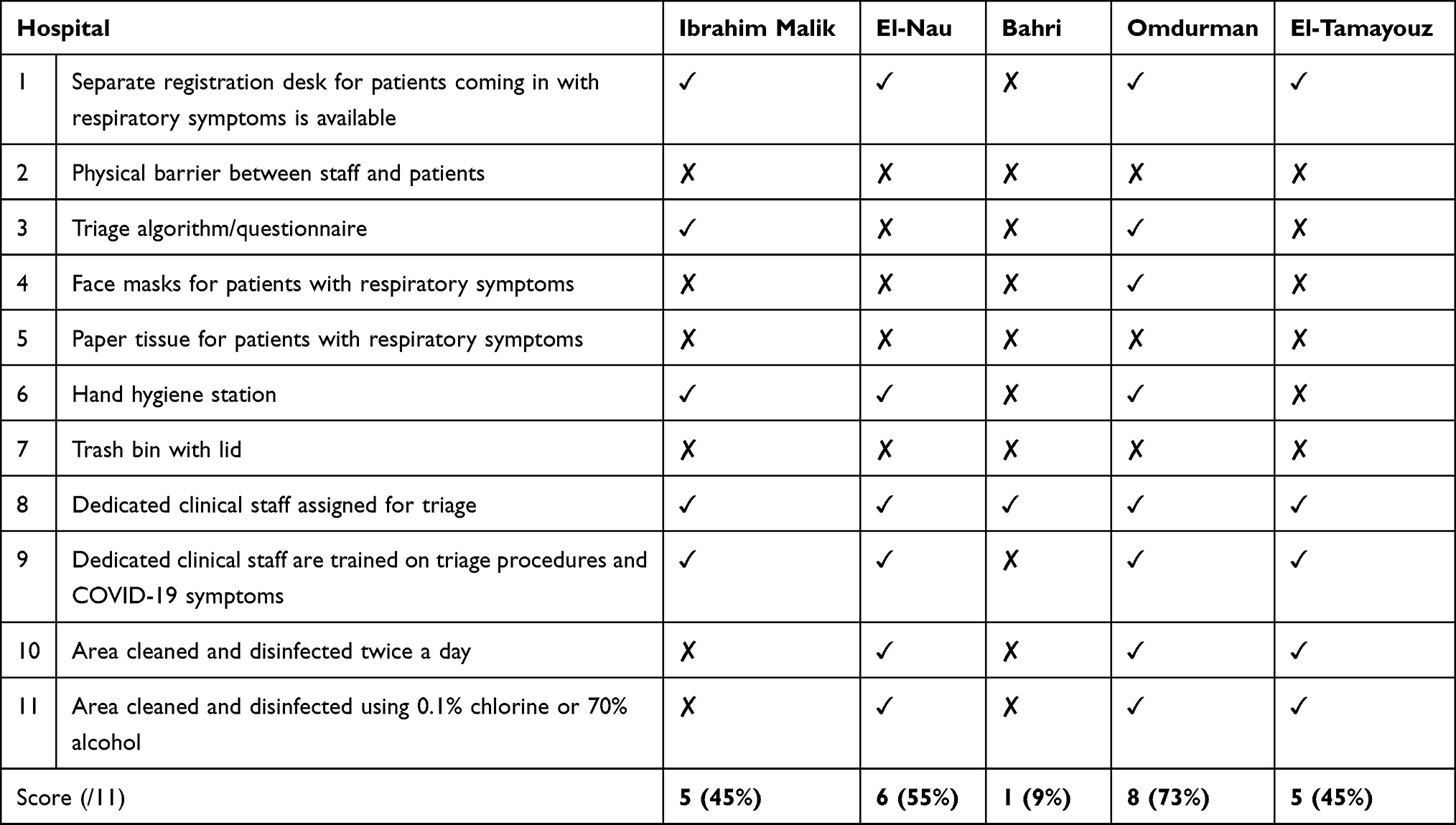 |
Table 2 Assessment of the Triage Area at the EDs (n = 5) |
Respiratory Waiting Area Domain
The only hospital assessed in this study that had a respiratory waiting area was Omdurman Teaching Hospital. The respiratory area at Omdurman Teaching Hospital met all the criteria of the checklist, except for the presence of paper tissues and trash bins with lids.
In the other four hospitals that did not have a separate respiratory waiting area, patients with high clinical suspicion of COVID-19 were sent to an appropriate facility for confirmation of the diagnosis. If by chance, a bed was available in the aforementioned facilities and the patient required admission, they were then transported to the hospital’s isolation ward. In some instances, the patients were brought to the isolation wards via ambulance.
Triage Process Domain
Algorithm
In all the hospitals, where available, algorithms were used for triage.
Assessing Facemask/Alternative Wear in Patients with Respiratory Symptoms in the Triage Area
All of the patients with respiratory symptoms visiting Al-Nau and Omdurman Hospitals wore a facemask or an alternative at the time of the study. On the other hand, 60% and 50% of the patients visiting Ibrahim Malik and Bahri Teaching Hospitals wore a facemask or an alternative, respectively. Devastatingly, all the patients visiting El-Tamayouz Hospital neither wore a facemask nor an alternative.
Further data on the triage process is given in Table 3.
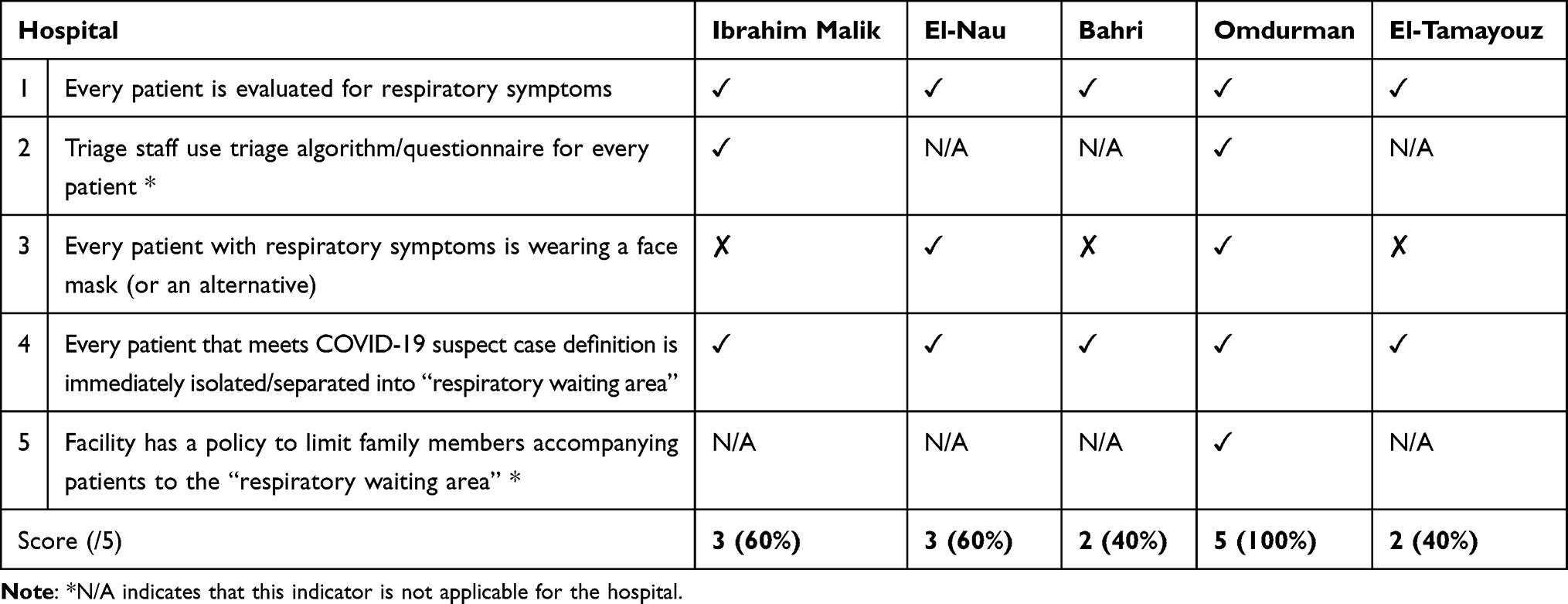 |
Table 3 Assessment of the Triage Process at the EDs (n = 5) |
PPE Domain
Unfortunately, there were no posters or job aids observed in any of the donning and doffing areas. Further information on the PPE domain is found in Table 4.
 |
Table 4 Assessment of the Hospital PPE Availability at the EDs (n = 5) |
HCPs Conducting Physical Evaluations on Patients with Respiratory Symptoms
Providentially, all of the staff members conducting physical evaluations on patients with respiratory symptoms who were observed in this study were trained on proper PPE use including donning and doffing. Additionally, they all wore face masks and gloves.
However, a discrepancy was seen between the number of observed staff members who wore gowns in the five hospitals. For instance, only 80% of the staff at Ibrahim Malik Teaching Hospital wore gowns and tragically, none of the staff at El-Tamayouz did. Otherwise, all the staff in the other hospitals wore gowns. Likewise, there was an obvious disparity in the number of staff wearing eye protection in the five hospitals. All the staff at Al-Nau and Bahri Hospitals wore a face shield or goggles. Contrarily, only 80% of the staff at Omdurman Teaching Hospital wore eye protection. Moreso, none at Ibrahim Malik Teaching Hospital did. Additional information on the use of PPE among HCPs conducting physical evaluations on patients with respiratory symptoms is provided in Table 5.
 |
Table 5 Assessment of the Use of PPE Amongst HCPs at the Hospitals (n = 5) |
Environmental Staff
In terms of the environmental staff working at the triage, waiting and examination areas, all wore a facemask but for those in El-Tamayouz Hospital, where only 75% of the observed staff wore one. Furthermore, the only staff observed wearing eye protection and gowns worked in Omdurman Hospital and even there only 20% of the staff had them donned.
Additionally, the only two hospitals where the staff wore heavy duty gloves were Ibrahim Malik and Omdurman Teaching Hospitals. On top of that, only 50% and 20% of the staff were attired in heavy duty gloves in the respective aforementioned hospitals. Lastly, all of the staff at Ibrahim Malik and Omdurman Teaching Hospital wore closed-toe shoes or boots. On the contrary, only 75% of the staff at El-Tamayouz and 63% of those at Bahri wore closed-toe footwear. Catastrophically, none of the staff at Al-Nau Hospitals did. Further data on the use of PPE amongst environmental service staff can be found in Table 5.
Discussion
Patients with SARS-CoV-2 infection initially come into touch with healthcare providers in EDs, thus they form an integral part of the disease prevention and control system. We share the experiences of Sudan’s response to this major public health crisis, by reporting on the standards of COVID-19 triage that are in place at 5 national health facility EDs in Sudan. According to our knowledge, this is the only study that has been done with the goal of evaluating the COVID-19 triage procedure in emergency rooms in Sudan.
Our findings show that, while there was some variation between hospitals and a general lack of readiness in terms of human resources, staff welfare, and the availability of essential supplies for the COVID-19 response, the majority of departments surveyed were not adequately prepared for the second wave at the time. Yet, common features also emerged. Various hospitals demonstrated diverse experiences across some dimensions. For instance, it was discovered that all hospitals have notices about coughing manners and respiratory hygiene placed at all entrances, waiting areas, and beside the elevators.
Furthermore, all hospitals neither had trash bins with lids nor a facility phone number. As unfortunate the latter findings are, they are not surprising, as public hospitals in Sudan have always lacked these resources, as they were never deemed a priority amidst the other serious capacity and resource constraints. It is crucial to note, however, that facility phone numbers and triage hotlines can be used in creative ways to save money on medical care by acting as efficient information touchpoints for gathering longitudinal patient data and easing congestion that would otherwise worsen disease propagation. This will assist overworked hospital systems in giving symptomatic patients with risk factors for serious disease the highest priority for acute care resources.
Also, successful triage of acute care resources depends on employees having received proper training on COVID-19 symptoms. A three-day capacity-building workshop on treatment pathways, standard operating procedures, and clinical guidelines for infection control and prevention (ICP) was attended by staff in a rural remote mountainous region of Pakistan, according to a recent study on the development of COVID-19 emergency response centers (ERCs).12 It is regrettable to learn that one of the public hospitals evaluated in our study failed to provide the committed clinical staff with triage training and information on COVID-19 symptoms. The latter finding is devastating as it is well known that clear communication and training of healthcare facility staff is vital to ensure that the triage process is properly implemented in order to prevent the transmission of COVID-19.
The cornerstone of triage is the evaluation of patients for respiratory symptoms using a consistent algorithm. In all the hospitals in our study, every patient was evaluated for respiratory symptoms. However, only 2 of these hospitals complied with the use of an available standard triage algorithm. This inconsistency might have led to the subjective evaluation of patients by the HCPs. Contrarily, several countries’ hospitals implemented strict screening procedures at their entrances with a commitment to the use of a standard triage algorithm.14–16 As per guidelines, patients found to have respiratory symptoms should wear facemasks or an alternative for ICP purposes. However, in the majority of the hospitals surveyed, patients with respiratory symptoms wore neither. Only Omdurman hospital provided face masks for patients with respiratory symptoms. A possible explanation could be that the Swiss medical organisation Médecins Sans Frontières (MSF) provided assistance to the emergency room at Omdurman Teaching Hospital in order to combat the pandemic.17 Unlike our findings, studies from Singapore, China and Switzerland showed patients were provided with face masks at the ED entrances.15,16,18 Hence, our study revealed poor adherence to the international guidelines in regards to face mask wearing.19,20 This could be explained partly by the lack of availability of resources.
Another necessary ICP measure is the presence of a separate waiting area as it concentrates related resources in one area of the hospital. A number of studies reported that suspected COVID-19 patients were directed to a separate waiting area.14–16,18 In our study, only Omdurman hospital had a separate waiting area. One possible explanation is that Omdurman Teaching Hospital is the largest hospital in Sudan with an abundance of space for a respiratory waiting area.17 In other hospitals where there was no respiratory waiting area, patients suspected of having COVID-19 were sent off to get tested in a different facility, and confirmed cases were directed immediately to isolation wards.
Additionally, the proper use of PPE is essential to prevent the transmission of the virus from the possible COVID-19 patients. However, many countries worldwide, including a number of African countries, have experienced a shortage of PPE during the pandemic.21–23 On the other hand, we observed that all of the hospitals in this study had most of their PPE present in stock. However, it must be noted that the checklist used in this study does not assess the number of available PPE, the exact ratio of the number of available PPE to the number of staff nor the reuse of PPE. Hence, the presence of PPE only and not their abundance in stock was assessed. This may account for the differences seen with the other countries in the studies mentioned above. Despite our observation of the presence of PPE, our study reveals a disparity in the adherence to PPE according to the type of staff. For example, there was a poor compliance of environmental staff to PPE in comparison to HCPs conducting physical examinations on patients with respiratory system symptoms. A possible explanation for this disparity in compliance to PPE could be the higher perceived risk of COVID-19 infection among the HCPs in close contact with suspected COVID-19 patients.18
Furthermore, a devastating incongruence in scores was seen between El-Tamayouz and the other hospitals, where El-Tamayouz scored the least in the Hospital PPE availability and the HCPs conducting physical evaluations on patients with respiratory symptoms. The disparity among the other hospitals and El-Tamayouz can be attributed to political reasons, where the latter lost its administrative and financial support of a former minister of health with his upheaval from his position following the nationwide revolution that took place in December 2019. Moreover, it is upsetting to report that the hospitals in our study showed inadequacy in one of the crucial aspects of ICP, this being the establishment of separate donning and doffing rooms with posters on the proper ways of donning and doffing. Our findings revealed less than half of the hospitals had separate donning and doffing room space, these being similar to the results of another study.21 Unfortunately, none of these areas had posters on the proper ways of donning and doffing. The lack of preparedness of staff to protect themselves and the disparity of PPE availability among hospitals could lead to an increase in the number of infected personnel. As a result, hospital management teams should review and revise the hospital’s IPC protocols. In order to avoid national shortages of vital PPE, governments should provide clear guidelines on the use of PPE and act sooner to obtain appropriate supplies and stockpiles in case of an outbreak. Also, to limit the possibility of PPE shortages at critical moments, regional medical supply production should be considered for all continents.
A limitation of this study is the potential for bias due to the small sample size of hospital services included in our locally collected data.
Conclusion
The results from the evaluated EDs showed that the healthcare facilities in Sudan have deficiencies in their COVID-19 response-related architecture, equipment, human resources, processes, and procedures. These less-than-ideal practices reported from the second wave of the pandemic demonstrate the necessity of a comprehensive, system-wide reform. In the event of future COVID-19 waves or other pandemics, policy makers at the local, and national level, as well as healthcare managers, need to consider how workplace factors, such as staff training on triage procedures, use of consistent algorithms for triage and availability of PPE can improve the experience and well-being of both HCPs and patients.
Abbreviations
ACEP, American College of Emergency Physicians; CDC, Centers for Disease Control and Prevention; COVID-19, coronavirus disease 2019; EDs, Emergency Departments; ER, Emergency room; ERCs, Emergency response centres; HCPs, Healthcare personnel; ICP, Infection prevention and control; LMICs, Low and Middle-Income Countries; MSF, Médecins Sans Frontières; PPE, Personal protective equipment; SARS‑CoV‑2, Severe acute respiratory syndrome coronavirus 2; SSA, sub-Saharan Africa.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval
The study was approved by the ethical committee of the Department of Community Medicine, University of Khartoum (Reference Number 1/2022Com.med). Consent for participation was not applicable as the study did not involve any human participants or any data that could lead to human identification.
Acknowledgments
We would like to thank Dr. Elfatih Malik for his expertise and assistance throughout all aspects of our study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Worldometer. Sudan population (live); 2004. Available from: https://www.worldometers.info/world-population/sudan-population/.
2. Musa TH, El Bingawi HM, Musa IH, et al. COVID-19 in Sudan: response towards control and prevention. Med J Malaysia. 2020;75(4):403–405. PMID: 32724003.
3. Fadul N, Hussein ME, Fadul AA. Re-opening Sudan: the balance between maintaining daily living and avoiding the next peak of COVID-19. Curr Trop Med Rep. 2021;8(3):231–237. doi:10.1007/s40475-021-00237-2
4. Aljak ER, Eldigail M, Mahmoud I, et al. The first laboratory-confirmed imported infections of SARS-CoV-2 in Sudan. Trans R Soc Trop Med Hyg. 2020;115(1):103–109. doi:10.1093/trstmh/traa151
5. Ahmed A, Mohamed NS, El-Sadig SM, et al. COVID-19 in Sudan. J Infect Dev Ctries. 2021;15(02):204–208. doi:10.3855/jidc.14520
6. El-Sadig SM, Fahal LA, Abdelrahim ZB, et al. Impact of COVID-19 on doctors and healthcare providers during the pandemic in Sudan. Trans R Soc Trop Med Hyg. 2021;115(6):577–578. doi:10.1093/trstmh/trab016
7. El-Sadig SM, Mohamed NS, Ahmed ES, et al. Obstacles faced by healthcare providers during COVID-19 pandemic in Sudan. J Infect Dev Ctries. 2021;15(11):1615–1617. doi:10.3855/jidc.14520
8. Tolu LB, Ezeh A, Feyissa GT. How prepared is Africa for the COVID-19 pandemic response? The case of Ethiopia. Risk Manag Healthc Policy. 2020;13:771–776. doi:10.2147/RMHP.S258273
9. Umviligihozo G, Mupfumi L, Sonela N, et al. Sub-Saharan Africa preparedness and response to the COVID-19 pandemic: a perspective of early career African scientists. Wellcome Open Res. 2020;5:163. doi:10.12688/wellcomeopenres.16070.3
10. Nakkazi E. Oxygen supplies and COVID-19 mortality in Africa. Lancet Respir Med. 2021;9(4):39. doi:10.1016/S2213-2600(21)00087-4
11. Biomedical equipment for COVID-19 case management, Malawi facility survey report. Seattle, WA: Path; 2021.
12. Jan R, Uddin M, Ullah I, et al. Developing COVID‐19 emergency response centres in geographically challenged areas of Pakistan: a case study of the Aga Khan Development Network. Int J Health Plann Manage. 2021;36(6):1990–1997. doi:10.1002/hpm.3286
13. Non-US HCF triage checklist. Centers for Disease Control and Prevention. Available from: https://www.cdc.gov/coronavirus/2019-ncov/downloads/non-US-HCF-triage-checklist.pdf.
14. Kim JH, An JAR, Min PK, et al. How South Korea responded to the Covid-19 outbreak in Daegu. NEJM Catalyst. 2021;1(4). doi:10.1056/CAT.20.0159
15. Quah LJJ, Tan BKK, Fua TP, et al. Reorganising the emergency department to manage the COVID-19 outbreak. Int J Emerg Med. 2020;13(1). doi:10.1186/s12245-020-00294-w
16. Wang Q, Wang X, Lin H. The role of triage in the prevention and control of COVID-19. Infect Control Hosp Epidemiol. 2020;41(7):772–776. doi:10.1017/ice.2020.185
17. All Africa. Sudan: MSF inaugurates new center in Omdurman hospital for treatment of coronavirus patients; 2020. Available from: https://allafrica.com/stories/202008060460.htm/.
18. Peros G, Gronki F, Molitor N, et al. Organising a COVID-19 triage unit: a Swiss perspective. Emerg Microbes Infect. 2020;9(1):1506–1513. doi:10.1080/22221751.2020.1787107
19. Centers for Disease Control and Prevention. Standard operating procedure (SOP) for triage of suspected COVID-19 patients in non-US healthcare settings: early identification and prevention of transmission during triage; 2021. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/non-us-settings/sop-triage-prevent-transmission.html/.
20. World Health Organization. COVID-19 infection prevention and control: preparedness checklist for long-term care facilities]; 2021. Available from: https://apps.who.int/iris/handle/10665/339488/.
21. Boškoski I, Gallo C, Wallace MB, Costamagna G. COVID-19 pandemic and personal protective equipment shortage: protective efficacy comparing masks and scientific methods for respirator reuse. Gastrointest Endosc. 2020;92(3):519–523. doi:10.1016/j.gie.2020.04.048
22. Mulu GB, Kebede WM, Worku SA, Mittiku YM, Ayelign B. Preparedness and responses of preparedness and responses of healthcare providers to combat the spread of COVID-19 among North Shewa Zone Hospitals, Amhara, Ethiopia, 2020. Infect Drug Resist. 2020;13:3171–3178. doi:10.2147/IDR.S265829
23. Ye G, Lin H, Chen S, et al. Environmental contamination of SARS-CoV-2 in healthcare premises. J Infect. 2020;81(2):1–5. doi:10.1016/j.jinf.2020.04.034
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.