Back to Journals » Clinical Ophthalmology » Volume 15
Evaluating the Safety, Efficacy and Patient Acceptability of Intravitreal Fluocinolone Acetonide (0.2mcg/Day) Implant in the Treatment of Non-Infectious Uveitis Affecting the Posterior Segment
Authors Steeples LR, Pockar S, Jones NP, Leal I ![]()
Received 19 January 2021
Accepted for publication 18 March 2021
Published 7 April 2021 Volume 2021:15 Pages 1433—1442
DOI https://doi.org/10.2147/OPTH.S216912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Laura R Steeples,1,2 Sasa Pockar,1 Nicholas P Jones,1,2 Inês Leal3,4
1Manchester Royal Eye Hospital, Manchester University Hospitals NHS Foundation Trust, Manchester Academic Health Science Centre, Manchester, UK; 2Faculty of Biology, Medicine & Health, University of Manchester, Manchester, UK; 3Ophthalmology Department, Centro Hospitalar Universitário Lisboa Norte, Hospital de Santa Maria, Lisbon, Portugal; 4Centro de Estudos das Ciências da Visão, Faculdade de Medicina, Universidade de Lisboa, Lisbon, Portugal
Correspondence: Laura R Steeples Email [email protected]
Abstract: Long-acting, slow-release injectable fluocinolone intravitreal implants have been approved for the treatment of non-infectious uveitis affecting the posterior segment. We summarise the development of intravitreal fluocinolone implants and discuss the technology including pharmacokinetics. We conducted a systematic review of evidence for the efficacy, safety and patient acceptability of fluocinolone 0.18 mg and 0.19 mg injectable implants. We summarise evidence from the pivotal phase 3 studies that lead to the approval of these implants and evaluate real-world including disease-specific evidence. Safety including injection-related events and long-term adverse events is presented.
Keywords: fluocinolone acetonide implant, non-infectious uveitis, posterior segment, efficacy, safety
Introduction
A diverse group of non-infectious inflammatory conditions affect the uvea in the posterior segment (NIU-PS), including intermediate, posterior and panuveitis. Uveitis is a major cause of vision loss; sustained disease control and/or prevention of recurrences is necessary to prevent structural damage and permanent visual impairment.1 Systemic corticosteroids and systemic immunosuppression (namely, antimetabolites, T-cell inhibitors and, more recently, biologics) are the mainstay of treatment and although effective, may be associated with adverse systemic and ocular effects. Local corticosteroid treatment strategies have been developed to deliver high concentrations of drug in ocular tissues and to limit systemic exposure; efficacy in NIU-PS is established.2–5 Both intravitreal and periocular delivery routes are available for local steroids. In the POINT study, intravitreal therapies were superior to periocular steroid injection.6 Local steroid is used alone or as an adjuvant to systemic therapy and may be necessary as a rescue therapy if there is a disease flare despite systemic treatment.
Slow-release intravitreal corticosteroid implants have been developed to provide stable and sustained concentrations of intravitreal drug which reduce systemic treatment side-effects and minimise the number of local injections. The approved devices contain dexamethasone (OZURDEX®, 0.7 mg, Allergan, Marlowe, UK) or fluocinolone acetonide ((FA) (ILUVIEN®, Alimera Sciences, Aldershot, UK (0.19 mg), Retisert® (0.59 mg, Bausch and Lomb, etc) and YUTIQ® (0.18 mg, EyePoint Pharmaceuticals Inc, Watertown, MA USA)). In this comprehensive review, we discuss the efficacy, safety and patient acceptability of injectable fluocinolone acetonide implants (FAi) (0.18 mg and 0.19 mg inserts) in NIU-PS, including phase 3 clinical trial and real-world data.
Background – Fluocinolone Implants for NIU-PS
There are several different long-acting FAi drug delivery systems for NIU-PS:
0.59 mg Fluocinolone Acetonide Implant
Long-acting, surgically placed FAi implants were developed and investigated in NIU-PS, initially with 2.1 mg and 0.59 mg implants.7–9 Subsequently, the FDA approved in 2005 a 0.59 mg FAi (providing initial release of 0.6 μg/day, reducing to steady state of 0.3–0.4 μg/day) (Retisert, Bausch and Lomb, Rochester, NJ, USA) non-biodegradable implant, inserted via pars plana incision.10 The 0.59 mg implant was compared to systemic treatment in NIU-PS in the multi-centre uveitis treatment trial11 and furthermore against standard of care in chronic NIU-PS by Pavesio et al.12 Studies demonstrated effective control of inflammation in chronic NIU but high rates of raised intraocular pressure (IOP), need for IOP-lowering procedures and cataract requiring surgery, were observed.9,11,12 In one large study in NIU, topical IOP-lowering medications were required in 74.8% of implanted eyes, and IOP-lowering surgeries were performed in 36.6% of implanted eyes by 36 months follow-up.13
0.18/0.19 mg Fluocinolone Acetonide Inserts
Subsequently, revised-dose and injectable intravitreal inserts (0.18 and 0.19 mg) were designed to improve safety and to facilitate insertion, patient comfort and convenience using injection applicators suitable for an office-based setting. These lower-dose inserts were less likely to cause raised IOP requiring medical or surgical intervention or cataract progression needing surgery, compared with the 0.59 mg implant in initial evaluation.14 The YUTIQ and ILUVIEN inserts are almost identical FAi containing 0.18 mg and 0.19mg, respectively. This review will focus on analysis of the available clinical evidence for both 0.18 and 0.19 mg inserts, each delivering fluocinolone acetonide in a dose of 0.2 μg/day.
The Technology
Pharmacokinetics
Fluocinolone is a synthetic fluorinated glucocorticoid ((6a, 11b, 16a)-6,9-difluoro-11,21-dihydroxy-16,17-[(1-methylethylidene)bis-(oxy)]-pregna-1,4-diene-3,20-dione) with low solubility in aqueous.15,16 A human pharmacokinetic study showed that following a 0.2 μg/day insert, peak drug levels in the aqueous (slightly >2ng/mL) were sustained for approximately 3 months, followed by steady-state levels from around 6 months (0.5–1.0ng/mL) for 36 months.17 Therefore, a 0.2 μg/day insert provides stable long-term release of FA, the drug then diffusing from vitreous into retina/choroid and other ocular tissues.17,18 There was no detectable FA in plasma samples from day 1 to month 36.17
ILUVIEN Implant
ILUVIEN, a 0.19mg implant, is a non-biodegradable cylinder containing a FA acetonide drug core.19 The insert releases FA at a rate of 0.2 μg/day for up to 36 months.19 ILUVIEN was approved in 2019 in Europe and the UK for prevention of relapse of NIU-PS.20
YUTIQ Implant
The FDA approved YUTIQ, a 0.18 mg intravitreal implant comprising a drug core within a non-bioerodible polyimide tube, for the treatment of NIU-PS in 2018. The implant releases 0.25 μg/day FA initially, and subsequently is reported as a 0.2 μg/day implant, lasting up to 36 months.21
Both implants are produced in pre-loaded sterile 25-gauge applicators with a needle length of 8.5 mm for ILUVIEN and 3.5 mm for YUTIQ, for intravitreal injection under local anaesthesia (office-based procedure).
Methods
Search Strategy, Selection and Eligibility Criteria
We searched PubMed, Medline, Embase, Cochrane, CINAHL databases and National Institutes of Health database for eligible original publications (case reports, case series, clinical trials and abstracts). The search algorithm is described in detail in Appendix 1. A manual search for further potentially relevant articles was also made using references cited in the identified articles. Published 36 month data were not available for long-term follow-up in one phase 3 clinical study but was available from a conference abstract. We screened EURETINA and American Academy of Ophthalmology annual meeting abstracts (from 2020) for any relevant submissions. The inclusion criteria were as follows: full text was available, clinical data were complete, fluocinolone acetonide 0.18 mg or 0.19 mg implant was used for treatment in cases of non-infectious posterior uveitis. We excluded non-English publications, single case reports, letters to the editor and correspondence. A CONSORT diagram of the process is presented in Appendix 2.
Eligible publication articles were independently screened and extracted by two reviewers. The data extracted are presented in Tables 1 and 2.
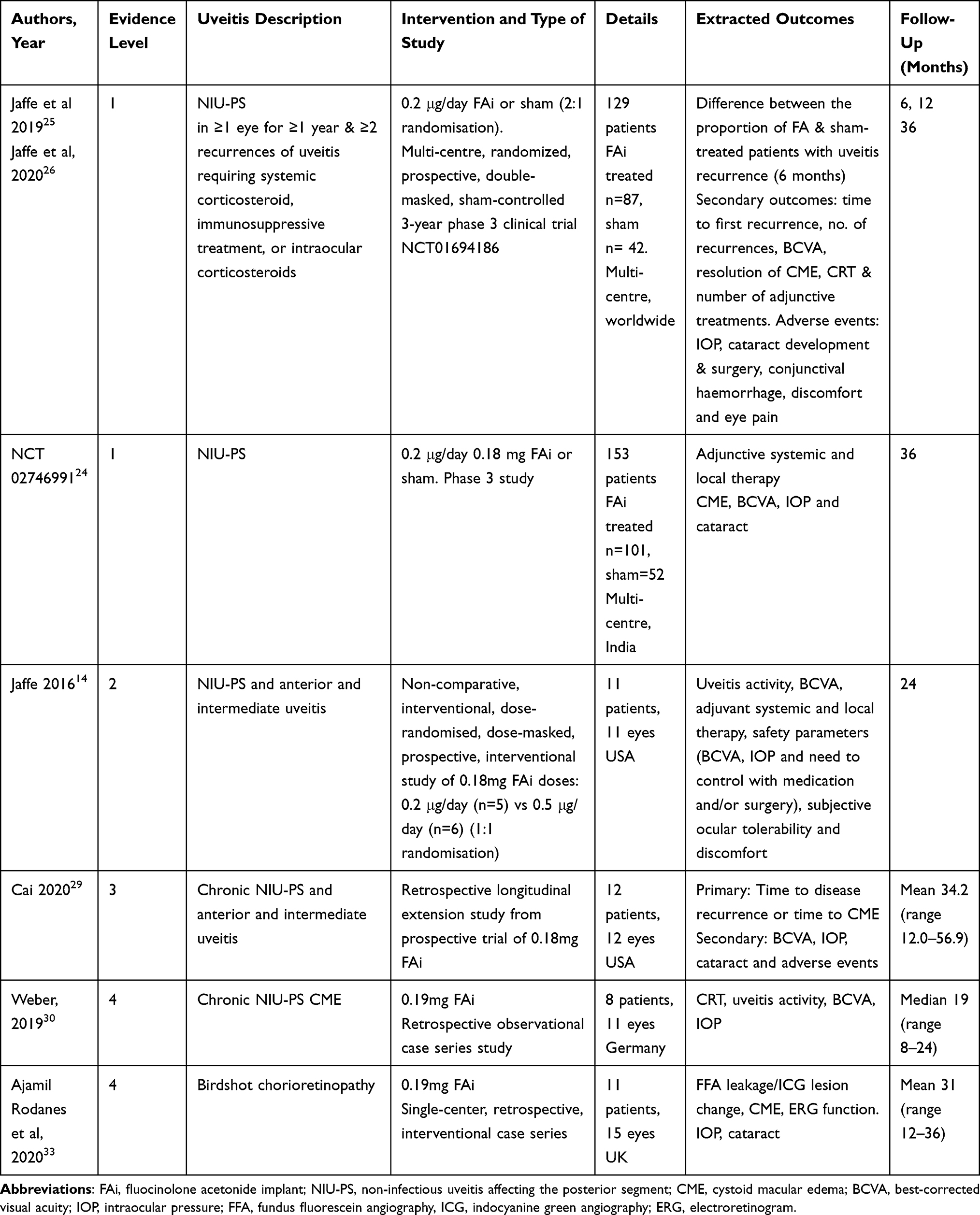 |
Table 1 Summary of Published Studies for Injectable Fluocinolone Acetonide Implants in Non-Infectious Uveitis (0.18 mg and 0.19 mg) |
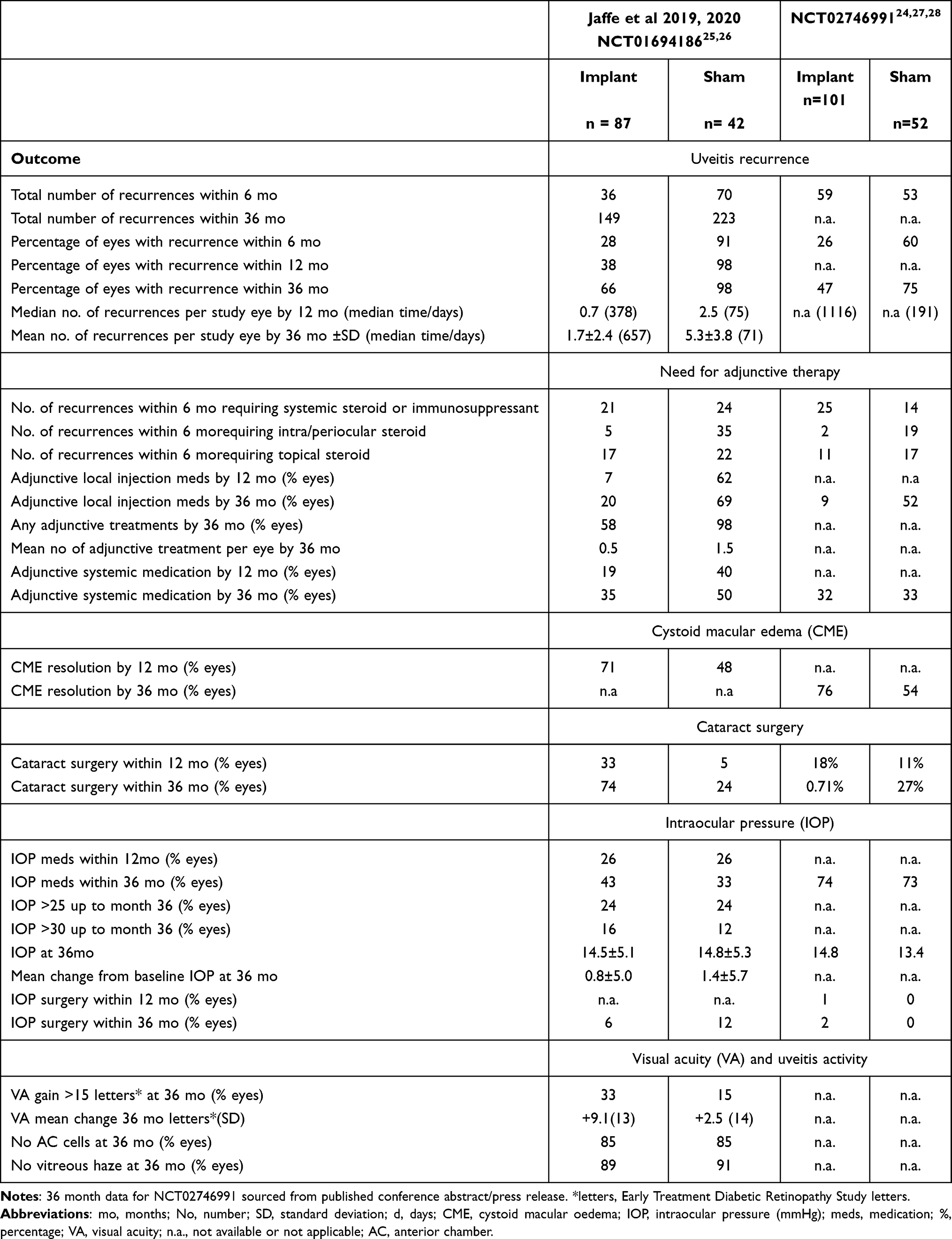 |
Table 2 Summary of Outcomes of Phase 3 Clinical Trial Evaluation of Fluocinolone Implant versus Sham in Chronic Non-Infectious Uveitis Until 36-Months |
Oxford Centre for Evidence-based Medicine tool was used to appraise the quality of evidence evaluated and is presented in Table 1.22
Evidence
A summary of published evidence for 0.18 mg and 0.19 mg FA implants is presented in Table 1. Phase 3 clinical trial outcome data are presented in Table 2.
Phase 3 Clinical Trials
The clinical safety and efficacy of FA implants were evaluated in two pivotal phase 3 randomised ((2:1 FAi:sham injection plus standard of care), prospective, double-masked, parallel-group multi-centre studies (Clinicaltrial.gov identifiers NCT0169418623 and NCT0274699124). Adult patients with chronic NIU-PS of at least one-year duration and involving at least one eye, were recruited with follow-up continuing for 36 months. The primary endpoint in both trials was the proportion of patients who experienced a recurrence of uveitis in the study eye within 6 months of follow-up. In total, 282 subjects were enrolled with 188 patients randomized to the study drug and 98 to sham injection. A summary of published outcomes from these studies, from the original publications at specific time-points, is presented in Table 2. A recurrence of uveitis was defined as either deterioration in best-corrected visual acuity (BCVA), vitreous haze attributable to non-infectious uveitis or the need for rescue medications.
To date, there are now ongoing or published randomised control trials, or other publications, comparing the efficacy and safety of 0.18 and 0.19 mg implants.
Clinical Trial NCT01694186
Jaffe et al reported the 6 month (primary endpoint) and 12 month efficacy and safety analysis in 201925 and 36 month follow-up analysis in 2020.26 Patients were assigned to either FA insert (n = 87) or sham injection (n = 42, total 129). Patients were enrolled if they had a history of at least 2 separate recurrences of uveitis requiring systemic or local treatment or in the previous 12 months had received systemic therapy for a minimum of 3 months or at least 2 peri- or intra-ocular steroids to manage uveitis. Uveitis recurrence was defined by either a 2-step or more increase in either anterior chamber activity or vitreous haze or deterioration in BCVA by 15 letters or more, all compared with any visit prior to month 6. Non-protocol defined recurrences were also analysed if local or systemic treatment was used in a study eye, even if the criteria were not met. A recurrence was assumed and “imputed” in analysis for missing data at 6, 12 and 36 months.
The 6 month (28% and 91%) and 12 month (38% and 98%) uveitis recurrence rates were significantly lower (p< 0.001) with FAi vs sham, respectively. FAi-treated eyes had fewer recurrence episodes (mean 0.7 vs 2.5), required fewer adjunctive local (7% vs 62%) and systemic treatments (19% vs 40%) and had lower incidence of 15-letter or more decrease in BCVA (14% vs 31%) compared with sham-treated eyes. There was a reduction of CME and maintenance or improvement in BCVA.
At 12 months, no new safety concerns were observed.25 A higher rate of cataract was observed in the FAi-treated eye versus sham but the injection procedure was not associated with a higher rate of other adverse events. Medical therapy for raised IOP was similar between the two groups and the FAi arm showed a lower rate of IOP surgery.
Throughout 36 months of follow-up, the favourable efficacy outcomes compared with sham injection continued.26 The FAi treatment group had significantly fewer recurrences, required fewer adjunctive treatments, had significantly longer recurrence-free durations and a higher rate of CME resolution compared with sham-treated eyes. At 36 months, 34.5% of FAi-treated eyes had no disease recurrence or did not need any adjunctive medications, compared with 2.4% of sham eyes. In total, 34.5% of FAi treated eyes received this as a monotherapy. At 36 months, favourable BCVA gains were observed in the FAi-treated eyes; there was a greater mean letter gain, a higher proportion with significant vision improvement and fewer eyes with significant visual loss compared with sham.
One of the limitations of this trial was that imputed recurrences defined as above also included treatment of the fellow eye and systemic anti-inflammatory agents for systemic anti-inflammatory disease. By 36 months, observed protocol-defined uveitis recurrences occurred in a greater percentage in the sham-treated eyes, while in both groups the percentage of imputed recurrence was comparable; however, the treatment reasons were different and not completely understood (more local treatment in the sham group and more systemic treatment in the FAi-treated group). Moreover, missed appointments, counting as imputed recurrences, occurred in the FAi-treated group only. For these reasons, there may have been an overestimation of recurrences in the FAi-treated group. However, the analysis showed that there was greater benefit from FAi treatment, as lower recurrence rate was observed in FAi-treated eyes in the case of both protocol-defined or imputed recurrences (5-fold and 1.5-fold magnitude of the recurrence rate difference between FAi-treated and sham-treated eyes, respectively).25,26 Furthermore, there were no standardized measurements of macular edema in the protocol, enabling the assessment for a given participant, but not between the participants.
Clinical Trial NCT NCT02746991
The second double-masked randomised phase 3 trial enrolled 153 patients from 15 centres in India, with 101 eyes treated with FAi (0.18mg) and 52 eyes received sham injections.24,27,28 At 36 months, the recurrence rate in FAi-treated eyes was significantly lower compared to sham-treated eyes (46.5% vs 75.1%, respectively; p=0.001).27,28 FAi-treated eyes needed fewer local adjunctive therapies (8.9% vs 51.9%, respectively).28 Adjunctive systemic medications were similar between the two groups (31.7% vs 32.7%).28
There was no meaningful difference between BCVA gain or loss of 3 lines or more between the treatment and sham groups.28 Considering eyes with cystoid macular edema (CME) at baseline, 75.8% of FAi-treated eyes (n=33) had CME resolution, comparing to 53.8% of sham-treated eyes (n=13) at 36 months.27,28
Safety
The commonest adverse events associated with intravitreal corticosteroids are cataract and raised IOP. Key adverse events, and their management over 36 months follow-up in the phase 3 studies are presented in Table 2. At 36 months, Jaffe et al observed that IOP was generally controlled in both treatment groups.26 In FAi-treated eyes, 26% required IOP-lowering therapy at 12 months increasing to 42.5% at 36 months, compared with 26% and 33.3% of sham-treated eyes, respectively.25,26 Rates of glaucoma surgery at 12 and 36 months were 3.4% and 5.7%, respectively, in FAi-treated eyes compared with 4.5% and 11.9%, respectively, in sham-treated eyes.25,26 In the second phase 3 study, at 36 months the need for IOP lowering medication was similar between the two groups (74.3% FAi eyes vs 73.1% sham eyes).28 The significantly lower rate of glaucoma surgery in the FAi treatment group contrasts with results from previous Retisert studies at 36 months (36.6%).26 Jaffe et al suggested this effect is attributable to the lower daily corticosteroid dose.26 Long-term outcome data from glaucoma surgery in this cohort are not yet available.
In the second phase 3 study, no meaningful differences were noted between groups regarding mean IOP at 36 months (14.8 mmHg for FAi-treated eyes vs 13.5 mmHg for sham-treated eyes) or IOP-lowering medication (74.3% of FAi-treated eye vs 73.1% of sham-treated eyes).27,28
As anticipated, a high proportion of phakic eyes treated with FAi developed cataract, consistent with data from other corticosteroids (Table 2). Jaffe et al showed that the cataract surgery rate was higher in the FAi study eyes compared with the sham group at 12 months25 (33% and 12%, respectively; odds ratio: 3.7; p < 0.01) and 36 months (73.8 and 23.8%, respectively).26 In the second study FAi-treated eyes were more likely to need cataract extraction during 36 months follow-up (70.5% eyes) compared to sham-treated eyes (26.5%).27,28
Hypotony was reported by Jaffe et al as occurring in 10.3% eyes with FAi 0.19 mg and 11.9% treated with sham injections.26 It was considered temporary and associated with the procedure itself. The difference between FAi-treated and sham-treated eyes was not considered to be meaningful.
Although ocular treatment-emergent adverse events were in general higher in the FAi-treated eyes (total 430) than in sham-treated eyes (total 317), episodes of eye pain, conjunctival hemorrhage, ocular discomfort and blurred vision did not meaningfully differ between groups.26 These events are however typically self-limiting.
Other Studies
Further published evidence, from real-world studies regarding efficacy and safety of FAi (0.18 mg and 0.19 mg) are detailed in Table 1. Overall, there is very little and low evidence grade level real-world evidence in chronic NIU-PS. There were no unexpected safety signals or concerns in these limited studies.
Cai et al29 report retrospective longitudinal follow-up data (minimum 12 months) for 12 patients (12 eyes) who had completed 2 years of prospective clinical trial with FAi 0.18 mg implant.14 The study provides long-term real-world data on effect of FAi, and the first to provide clinical and safety data beyond three years after implantation. The primary endpoint was time to uveitis recurrence or time to CME. A uveitis recurrence was defined as increase in anterior chamber cells by 2 steps or more, increase in vitreous haze score by 2 steps or more, or any increased inflammation in the study eye as determined by the treating physician that required additional anti-inflammatory therapy. CME was defined as a 10% increase in CRT or new cysts on OCT. During follow-up (mean 34.2 months) 42% of eyes had no uveitis or CME recurrence, 42% had a uveitis recurrence (mean time 36.8 months after implantation (range 22.8–36.1 months). The recurrence rate is lower than that reported by Jaffe et al in phase 3 trial.29 However, the definition of recurrence differed from this study, including that missing data did not impute a recurrence, and comparisons in data are very inexact. Elevated IOP, beyond the 24 month trial period, was observed in 4 eyes (timescale was not detailed). This was managed initially with medical therapy and 2 eyes subsequently underwent glaucoma surgery (the authors state to reduce medication burden not uncontrolled IOP). This highlights the need for extended IOP monitoring beyond 24 months. The number of patients and variable follow-up intervals limits this study.
Weber et al reported the clinical outcomes in a small heterogeneous cohort of 8 patients (11 eyes) with chronic NIU-related CME.30 The median duration of CME before FAi implant was 36 months (range 18–108 months). Prior to the treatment with FAi implant, 70% of the eyes had undergone multiple periocular/subconjunctival steroid treatments with triamcinolone and all 11 eyes had been treated with multiple dexamethasone implants. A mean decrease in CRT of 220 μm was observed at 4–6 months post-FAi. No unexpected safety concerns were observed, with cataract surgery required in phakic patients and no IOP medical or surgical interventions needed. The authors of this paper presented outcomes from our centre, with FA 0.19 mg implant, in a small series of patients with chronic NIU-CME, at EURETINA 202031 and have submitted for peer review. A retrospective review of 3 month outcomes of FAi 0.18 mg in 85 eyes with chronic uveitis from a single centre in the USA was presented at the American Academy of Ophthalmology Annual Meeting in 2020.32
Patient Acceptability
Specific outcome measures and data on patient acceptability of the intervention, including efficacy and adverse events, was not available. We note that patient quality of life outcome measures were also not reported in the phase 3 FAi 0.18 mg clinical trials25–28 and evaluation of this would be useful, including evidence regarding patient acceptability. In available real-world studies, there are no reports of concerns regarding patient tolerance and no new safety concerns compared with phase 3 trials.
The current available evidence and expert clinician experience spanning over 5 years of clinical use, indicate that injectable implants are safe, feasible and tolerated in the outpatient setting, with no prolonged events related to the injection procedure.14,26–29,33
Patient acceptability of the side-effect profile, particularly the most frequent side-effects (cataract and raised IOP and their subsequent management) is not available.
Disease Specific Evidence
Clinical outcomes and efficacy for fluocinolone 0.18 mg and 0.19 mg implants in specific uveitic entities are extremely limited with one series in birdshot retinochoroiditis and a few case reports. (Table 1) Evidence is limited by the rarity of these conditions and furthermore by the relatively short-duration since approval of this device in NIU-PS. The phase 3 studies were not designed to evaluate efficacy based on uveitis aetiology.
Birdshot Retinochoroiditis
Ajamil-Rodanes et al reported outcomes with fluocinolone 0.19 mg in Birdshot retinochoroiditis (BRC).33 A retrospective analysis of 11 patients (15 eyes), with average follow-up of 31 months (range 12–36), treated in a single UK centre was performed.
The primary efficacy endpoint was improvement in vascular leakage on fundus fluorescein angiography (FFA), effect on cystoid macular oedema (CME) and resolution of hypofluourescent lesions on indocyanine green angiography (ICGA); secondary measures were improvements on pattern and full-field electroretinogram (PERG; ERG) parameters. Safety outcome measures were intraocular elevation and cataractogenesis. All eyes had FFA leakage at baseline. During follow-up: FFA showed no leakage in 73.4% of eyes between months 6–24 and 86.4% by month 24; 3/15 eyes had CME at baseline and this had resolved in all by 6 months but chorioretinal lesions on ICGA were unchanged. Retinal function improved and macular function improved or was stable in the majority following treatment. 5/15 eyes required IOP-lowering medical treatment and no eyes required IOP lowering surgery and normal mean IOP was reported throughout follow-up (p=0.67). Visually significant cataract was detected in 92% of eyes, with cataract surgery performed at a mean 22±10.2 months post-implantation. This was a much more favourable IOP outcome than that reported in cohorts of patients with BRC treated with the higher-dose fluocinolone implant (0.59 mg).34,35 Rush et al reported outcomes in 22 patients (32 eyes) with 100% of eyes requiring IOP lowering medical therapy and 12 eyes (33.3%) required glaucoma surgery at the end of follow-up.34
The results indicated therapeutic benefit from FAi (0.19 mg) for management of retinal vascular leakage, retinal function and CME.33 Patient acceptability/quality of life was not evaluated. As there was no observed improvement in choroidal lesions the authors concluded fluocinolone 0.19 mg therapy is inadequate in BRC, as monotherapy, to achieve control of choroidal inflammation.
Paediatrics
The safety and efficacy of FAi implants in paediatric patients have not been established.
Efficacy and Safety of Intravitreal Implants in NIU: Comparison of Implants Including Fluocinolone (0.2 µg/day) and Dexamethasone (0.7 mg)
There are no direct head-to-head trials comparing fluocinolone implants (0.19 mg (ILUVIEN) or 0.18 mg (YUTIQ) FAi) with dexamethasone (0.7 mg (OZURDEX)) implant to provide evidence of their efficacy and safety.36 Comparisons between different studies are difficult, with differences in study design, non-standardized study datasets and populations enrolled datasets, endpoints and definitions of recurrence.
In a recent systematic review of intravitreal implants in NIU including 8 different studies and assessing a total of 1621 participants, the authors performed a network meta-analysis to compare 0.18 mg fluocinolone acetonide implants, dexamethasone implant (0.70 mg and 0.35 mg), and sham procedures.36 Datasets comparing implants with sham injections were reviewed using network meta-analysis of outcomes including comparisons of BCVA, vitreous haze, central retinal thickness and adverse events (including cataract and IOP) were made. In the short term, the authors reported dexamethasone (0.7 mg at 1.5 months) superior to fluocinolone (0.18 mg at 1 month) for improving vitreous haze but at 6 months there was no statistically significant difference between them although both implants remained superior to sham treatment. With regards to CME reduction, both dexamethasone and FAi showed significantly greater effect than the sham procedure; however, no differences were found at 6 months. No significant differences were found between the FAi at 12 months and the dexamethasone implant at 6 months for BVCA improvement. From a safety perspective, the authors deemed that data on IOP adverse events were not comparable across implant groups to permit any conclusion to be drawn. Pairwise meta-analysis comparing the FAi with sham procedure suggested that the implant was associated with a decreased risk of uveitis recurrence ant not increases risk of raise of IOP above 25 mmHg or need for IOP medical treatment on uveitis recurrence and IOP. This systematic analysis has significant limitations, based on different follow-up intervals between the interventions and that only one indirect evidence comparing dexamethasone with FAi was available. Therefore, no exact or robust conclusions can be drawn. Further, randomised control trial evaluation is necessary.
Conclusions
Phase 3 clinical long-term studies have demonstrated the efficacy and safety of FAi 0.2 μg/day in chronic NIU-PS. In summary, the implants have been shown to reduce uveitis recurrence rates, to increase the time to recurrence episodes, and to reduce the need for adjuvant therapy. Long-term safety data demonstrate that cataract and raised IOP are the commonest adverse event and are expected with corticosteroid treatment but were safely managed within the studies. To date, there are no randomised control trials comparing 0.18 mg and 0.19 mg implants. There is currently very limited evidence from real-world practice and efficacy in specific uveitis aetiologies. There is also a lack of evidence regarding patient acceptability and quality of life evaluation. Further evaluation including RCTs and real-world multi-centre studies is recommended.
Disclosure
Miss Laura R Steeples reports consultancy fees from Alimera Sciences and Allergan. Professor Nicholas P Jones reports fees for expert panel consultancy from Alimera Sciences, during the conduct of the study. Dr Inês Leal reports consultancy fees from Alimera Sciences. The authors report no other conflicts of interest in this work.
References
1. Nguyen QD, Callanan D, Dugel P, Godfrey DG, Goldstein DA, Wilensky JT. Treating chronic noninfectious posterior segment uveitis: the impact of cumulative damage: proceedings of an expert panel roundtable discussion. Retina. 2006;Suppl:1–16. doi:10.1097/01.iae.0000250601.15893.5f
2. Zarranz-Ventura J, Carreño E, Johnston RL, et al. Multicenter study of intravitreal dexamethasone implant in noninfectious uveitis: indications, outcomes, and reinjection frequency. Am J Ophthalmol. 2014;158(6):1136–1145.e5. doi:10.1016/j.ajo.2014.09.003
3. Lowder C, Belfort R, Lightman S, et al. Dexamethasone intravitreal implant for noninfectious intermediate or posterior uveitis. Arch Ophthalmol. 2011;129(5):545–553. doi:10.1001/archophthalmol.2010.339
4. Steeples LR, Anand N, Moraji J, Jones NP. Clinical outcomes of intravitreal preservative-free triamcinolone preparation (Triesence®) for cystoid macular oedema and inflammation in patients with uveitis. Ocul Immunol Inflamm. 2018;26(7):997–1004. doi:10.1080/09273948.2017.1294185
5. Whitcup SM, Robinson MR. Development of a dexamethasone intravitreal implant for the treatment of noninfectious posterior segment uveitis. Ann N Y Acad Sci. 2015;1358(1):1–12. doi:10.1111/nyas.12824
6. Thorne JE, Sugar EA, Holbrook JT, et al. Periocular triamcinolone vs. intravitreal triamcinolone vs. intravitreal dexamethasone implant for the treatment of uveitic macular edema: the PeriOcular vs. INTravitreal corticosteroids for uveitic macular edema (POINT) Trial. Ophthalmology. 2019;126(2):283–295. doi:10.1016/j.ophtha.2018.08.021
7. Callanan DG, Jaffe GJ, Martin DF, Pearson PA, Comstock TL. Treatment of posterior uveitis with a fluocinolone acetonide implant: three-year clinical trial results. Arch Ophthalmol. 2008;126(9):1191–1201. doi:10.1001/archopht.126.9.1191
8. Sangwan VS, Pearson PA, Paul H, Comstock TL. Use of the fluocinolone acetonide intravitreal implant for the treatment of noninfectious posterior uveitis: 3-year results of a randomized clinical trial in a predominantly Asian population. Ophthalmol Ther. 2015;4:1. doi:10.1007/s40123-014-0027-6
9. Jaffe GJ, Martin D, Callanan D, Pearson PA, Levy B, Comstock T. Fluocinolone acetonide implant (Retisert) for noninfectious posterior uveitis. Thirty-four-week results of a multicenter randomized clinical study. Ophthalmology. 2006;113(6):1020–1027. doi:10.1016/j.ophtha.2006.02.021
10. Retisert Prescribing Information.Bausch and Lomb. Available from: https://www.bausch.com/ecp/our-products/rx-pharmaceuticals/rx-pharmaceuticals/retisert-fluocinolone-acetonide-intravitreal-implant-059-mg#.YAM1ZC90c1I.
11. Kempen JH, Altaweel MM, Holbrook JT, et al. Randomized comparison of systemic anti-inflammatory therapy versus fluocinolone acetonide implant for intermediate, posterior, and panuveitis: the multicenter uveitis steroid treatment trial. Ophthalmology. 2011;118(10):1916–1926. doi:10.1016/j.ophtha.2011.07.027
12. Pavesio C, Zierhut M, Bairi K, Comstock TL, Usner DW. Evaluation of an intravitreal fluocinolone acetonide implant versus standard systemic therapy in noninfectious posterior uveitis. Ophthalmology. 2010;117(3):567–575.e1. doi:10.1016/j.ophtha.2009.11.027
13. Goldstein DA, Godfrey DG, Hall A, et al. Intraocular pressure in patients with uveitis treated with fluocinolone acetonide implants. Arch Ophthalmol. 2007;125(11):1478–1485. doi:10.1001/archopht.125.11.ecs70063
14. Jaffe GJ, Lin P, Keenan RT, Ashton P, Skalak C, Stinnett SS. Injectable fluocinolone acetonide long-acting implant for noninfectious intermediate uveitis, posterior uveitis, and panuveitis: two-year results. Ophthalmology. 2016;123(9):1940–1948. doi:10.1016/j.ophtha.2016.05.025
15. Driot JY, Novack GD, Rittenhouse KD, Milazzo C, Pearson PA. Ocular pharmacokinetics of fluocinolone acetonide after RetisertTM intravitreal implantation in rabbits over a 1-year period. J Ocul Pharmacol Ther. 2004;20(3):269–275. doi:10.1089/1080768041223611
16. Jaffe GJ, Ben-nun J, Guo H, Dunn JP, Ashton P. Fluocinolone acetonide sustained drug delivery device to treat severe uveitis. Ophthalmology. 2000;107(11):2024–2033. doi:10.1016/S0161-6420(00)00466-8
17. Campochiaro PA, Nguyen QD, Hafiz G, et al. Aqueous levels of fluocinolone acetonide after administration of fluocinolone acetonide inserts or fluocinolone acetonide implants. Ophthalmology. 2013;120(3):583–587. doi:10.1016/j.ophtha.2012.09.014
18. Testi I, Pavesio C. Preliminary evaluation of YUTIQTM (fluocinolone acetonide intravitreal implant 0.18 mg) in posterior uveitis. Ther Deliv. 2019;10(10):621–625. doi:10.4155/tde-2019-0051
19. Alimera Sciences Limited. Summary of product characteristics for ILUVIEN 190 micrograms intravitreal implant in applicator. Medicine and Healthcare Products Regulatory Agency I 190 micrograms intravitreal implant in applicator: summary of product characteristics. 2012. Available from: https://www.medicines.org.uk/emc/medicine/27636#gref.
20. Overview Fluocinolone acetonide intravitreal implant for treating recurrent non-infectious uveitis | NICE Guidance. 2019. Available from: https://www.nice.org.uk/guidance/ta590.
21. EyePoint Pharmaceuticals US. YUTIQ: prescribing information. .2018. Available from: www.eyepointpharma.com/wp-content/uploads/2019/01/YUTIQ-USPI-20181120.pdf.
22. Oxford Centre for Evidence-Based Medicine: Levels of Evidence (March. 2009. Available from: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009.
23. EyePoint. Safety and efficacy of an injectable fluocinolone acetonide insert. NLM identifier NCT01694186. Available from: https://www.clinicaltrials.gov/ct2/show/NCT01694186.
24. EyePoint. Safety and Efficacy Study of a Fluocinolone Acetonide Intravitreal (FAI) insert in subjects with chronic non-infectious posterior uveitis. NLM identified NCT02746991. Available from: https://clinicaltrials.gov/ct2/show/NCT02746991.
25. Jaffe GJ, Foster CS, Pavesio CE, Paggiarino DA, Riedel GE. Effect of an injectable fluocinolone acetonide insert on recurrence rates in chronic noninfectious uveitis affecting the posterior segment: twelve-month results. Ophthalmology. 2019;126(4):601–610. doi:10.1016/j.ophtha.2018.10.033
26. Jaffe GJ, Pavesio CE. Effect of a fluocinolone acetonide insert on recurrence rates in noninfectious intermediate, posterior, or panuveitis: three-year results. Ophthalmology. 2020;127(10):1395–1404. doi:10.1016/j.ophtha.2020.04.001
27. Jaffe GJ, Biswas J, Paggiarino DA FAi insert treatment for noninfectious posterior uveitis: three-year results of a confirmatory trial. Abstract paper PA063. American Academy of Ophthalmology Annual Meeting Nov 2020. Available from: https://secure.aao.org/aao/meeting-archive.
28. EyePoint Pharmaceuticals. Press release 36-month follow up data for phase 3 study of YUTIQ. Available from: http://investors.psivida.com/news-releases/news-release-details/eyepoint-pharmaceuticals-announces-positive-topline-36-month.
29. Cai CX, Skalak C, Keenan RT, Grewal DS, Jaffe GJ. Time to disease recurrence in noninfectious uveitis following long-acting injectable fluocinolone acetonide implant. Graefe’s Arch Clin Exp Ophthalmol. 2020;258(5):1023–1030. doi:10.1007/s00417-020-04614-x
30. Weber LF, Marx S, Auffarth GU, et al. Injectable 0.19-mg fluocinolone acetonide intravitreal implant for the treatment of non-infectious uveitic macular edema. J Ophthalmic Inflamm Infect. 2019;9(1). doi:10.1186/s12348-019-0168-9
31. Pockar S, Leal I, Chhabra R, Jones NP, Steeples LR Injectable fluocinolone acetonide implant in non-infectious uveitis: 6-month outcomes from a single UK tertiary centre. Euretina 2020 Virtual Conference, October 2020. Poster abstract. Available from: https://www.euretina.org/congress/amsterdam-2020/virtual-2020-posters/?type=2.
32. Andrews HW, Ganaputra S, Hamdan S, Kim SJ Real-world therapeutic efficacy of fluocinolone acetonide 0.18 mg injectable intravitreal implant in chronic uveitis. Abstract Paper PA066. American Academy of Ophthalmology Annual Meeting, Nov 2020. Available from: https//secure.aao.org/aao/meeting-archive.
33. Ajamil-Rodanes S, Testi I, Luis J, Robson AG, Westcott M, Pavesio C. Evaluation of fluocinolone acetonide 0.19 mg intravitreal implant in the management of birdshot retinochoroiditis. Br J Ophthalmol. 2020. doi:10.1136/bjophthalmol-2020-317372
34. Rush RB, Goldstein DA, Callanan DG, Meghpara B, Feuer WJ, Davis JL. Outcomes of birdshot chorioretinopathy treated with an intravitreal sustained-release fluocinolone acetonide-containing device. Am J Ophthalmol. 2011;151(4):630–636. doi:10.1016/j.ajo.2010.10.005
35. Bajwa A, Aziz K, Foster C. Safety and efficacy of fluocinolone acetonide intravitreal implant (0.59 mg) in birdshot retinochoroidopathy. Retina. 2014;34(11):2259–2268. doi:10.1097/IAE.0000000000000239
36. Vieira R, Sousa-Pinto B, Figueira L. Efficacy and safety of corticosteroid implants in non-infectious uveitis: a systematic review with network meta-analysis. Ocul Immunol Inflamm. 2020;18(1–8):onlineahead of print. doi:10.1080/09273948.2020.1787463
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.