Back to Journals » Advances in Medical Education and Practice » Volume 17
Evaluating the Effectiveness of an Integrated PBL–CBL–TBL Teaching Model in Postgraduate Clinical Training
Authors Liu C, Zhang M, Xiao Y, Tong H, Ji R, Wang W, Liang Q, Zu S, Zhao C, Wang Y
Received 10 August 2025
Accepted for publication 13 February 2026
Published 9 March 2026 Volume 2026:17 559725
DOI https://doi.org/10.2147/AMEP.S559725
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Chang Liu,1 Mo Zhang,1 Ying Xiao,1 Hua Tong,1 Ru Ji,1,2 Wei Wang,1,2 Qianfei Liang,1,2 Shuwen Zu,3 Caiyan Zhao,1,2 Yadong Wang1,2
1Department of Infectious Diseases, Hebei Medical University Third Hospital, Shijiazhuang, 050051, People’s Republic of China; 2Teaching and Research Department of Infectious Diseases, Hebei Medical University, Shijiazhuang, 050051, People’s Republic of China; 3Office of Academic Affairs, Hebei Medical University Third Hospital, Shijiazhuang, 050051, People’s Republic of China
Correspondence: Yadong Wang, Department of Infectious Diseases, the Hebei Medical University Third Hospital, Shijiazhuang, 050051, People’s Republic of China, Tel +86-311-66776831 ; +86-18533112392, Email [email protected]
Aim: To evaluate the effectiveness of a combined Problem-Based, Case-Based, and Team-Based Learning (P-C-T) teaching mode in improving academic performance and self-reported learning outcomes among postgraduates specializing in infectious diseases.
Methods: This study enrolled 100 postgraduates (Master of Medicine (MM) and Doctor of Medicine (MD)) specializing in infectious diseases from five medical colleges in Hebei Province between Jan 2020 and Dec 2024. Participants were assigned to either the P-C-T integrated teaching group (n = 68) or the traditional teaching control group (n = 32). The curriculum included infectious disease teaching rounds and lectures. Comparative assessments included pre- and post-class theoretical tests, time-motion analysis of test completion, and a comprehensive questionnaire evaluating teaching satisfaction and competency development.
Results: Baseline pre-class scores showed no significant difference between groups (P > 0.05). Post-intervention, the P-C-T group had significantly higher median total test scores (94.00 [IQR 92.00– 95.00] vs 88.50 [IQR 86.25– 90.00]; P < 0.001) and shorter completion times (43.09 ± 5.92 min vs 47.66 ± 5.39 min; P < 0.001) than the control group. Additionally, the P-C-T group reported significantly higher questionnaire-based satisfaction and perceived learning outcomes (P < 0.001).
Conclusion: The P-C-T integrated teaching mode was associated with higher theoretical test performance, greater learning efficiency, and improved student satisfaction compared with traditional methods. By fostering critical thinking and active engagement, this structured approach may serve as a feasible instructional framework for postgraduate medical education and may help bridge the gap between theoretical learning and complex clinical practice.
Keywords: problem-based learning, case-based learning, team-based learning, teaching practice reform
Introduction
As an important branch of clinical medicine, infectious disease is characterized by strong specialization, explicit cognitive complexity, and a broad spectrum of involvement across organ systems.1 Unlike procedure-based specialties, it demands the mastery of intricate diagnostic reasoning and diverse management strategies for rapidly evolving pathogens, which presents significant challenges for postgraduates to master.1,2 Furthermore, with the rapid development of the discipline, traditional Lecture-Based Teaching (LBT) model, which relies predominantly on passive knowledge transmission from instructors to students, has increasingly revealed its limitations.3 LBT may be insufficient for cultivating the higher-order thinking, autonomous learning abilities, and collaborative problem-solving skills required in such a complex field.4 Consequently, contemporary medical curricula have increasingly prioritized active learning paradigms to enhance student engagement. Among the most prominent active learning strategies are Problem-based Learning (PBL), Case-based Learning (CBL), and Team-based Learning (TBL), which have been introduced to foster deeper cognitive engagement.
Although PBL, CBL, and TBL all adhere to student-centered constructivist principles, they are generally distinguished by differences in instructional sequencing and pedagogical focus.5 PBL is characterized by “self-directed inquiry”. In PBL, students are presented with an open-ended, ill-structured problem before acquiring the relevant knowledge. The learning process is driven by the students’ need to identify learning gaps and construct their own knowledge framework to solve the problem.6,7 Conversely, CBL typically serves as a method of “knowledge application”. It introduces structured clinical cases after students have obtained foundational knowledge through lectures or self-study. Its primary goal is to bridge theory and practice by training students in clinical reasoning and decision-making within a specific context.8,9 Distinct from the former two, TBL focuses on “accountability and process”. It employs a rigid sequence involving individual preparation, readiness assurance tests (individual and team), and immediate feedback, ensuring that students are accountable to their peers and promoting high-performance team dynamics.10,11
While each teaching mode possesses distinct advantages, relying on a single method is often insufficient for the comprehensive training required in infectious diseases—a discipline demanding strong theoretical retention,12 agile clinical reasoning, and collaborative skills. PBL excels in fostering autonomy but may lack efficiency in building a systematic knowledge base; CBL ensures clinical relevance but may not fully challenge independent inquiry; and TBL maximizes engagement but requires strict adherence to structure.13,14 Therefore, an integrated approach that seeks to combine these complementary strengths may offer theoretical advantages over reliance on a single instructional method. Drawing on these complementary advantages, we developed the P-C-T (PBL-CBL-TBL) combined teaching mode. This innovative model amalgamates the self-directed exploration of PBL, the clinical contextualization of CBL, and the collaborative rigor of TBL.
The P-C-T combined teaching mode integrates the distinctive strengths of PBL, CBL, and TBL while emphasizing active learning and collaborative attitudes. Therefore, the primary aim of this study was to evaluate the effectiveness of the P-C-T combined teaching mode in the training of postgraduates specializing in infectious diseases. To achieve this, we enrolled 100 postgraduates with Master of Medicine (MM) and Doctor of Medicine (MD) degrees from five medical colleges in Hebei Province and systematically compared the outcomes of the P-C-T mode against the traditional teaching model.
Methods
Participants Recruitment and Criteria
We enrolled 100 postgraduates with MM Degrees and MD Degrees specializing in infectious diseases (64 females and 36 males) who had obtained degree certificates between January 2020 to December 2024 from five universities including Hebei Medical University, Hebei University Health Science Center, Medical Collage of Hebei University of Engineering, Chengde Medical University and First Clinical Collage of Hebei North University. In the Chinese medical education system, the Master of Medicine (MM) and Doctor of Medicine (MD) tracks have distinct cultivation focuses: MM students prioritize clinical skills combined with standardized residency training, while MD students focus on academic research and advanced clinical proficiency. However, regarding the clinical training in infectious diseases specifically, the learning requirements and standards are consistent for both groups. All participants in this study, regardless of their degree track, adhered to the same infectious disease teaching syllabus and successfully completed the corresponding clinical practice and theoretical learning tasks. This study adopted a historical control design. Among them, 32 students from January 2020 to December 2021 were listed as traditional teaching groups, 68 students from January 2022 to December 2024 received P-C-T teaching mode.
Inclusion criteria: 1) Full-time professional MM Degrees and MD Degrees students specializing in infectious diseases and obtain degree certificate and diploma. 2) Voluntary participation in this study and signed informed consent. Exclusion criteria: 1) Participants who withdrew before termination of the study; 2) Those who have received other teaching reform experiments; 3) The same subject is prohibited from participating in this research twice during the master and doctor study periods. All enrolled students received a three-year clinical teaching practice. All the students were given consent forms and informed that their participation in the quizzes and the survey was voluntary.
Study Design
The postgraduate education in this study was mainly carried out in the form of teaching rounds, academic lectures, and clinical practice. The learning ability, performance and satisfaction of postgraduates with the instructional quality was evaluated by means of process assessment and questionnaire.
P-C-T Combined Teaching Group
Students were divided into groups of 8–10, with a group leader appointed to facilitate communication. The teaching practice was conducted in 4-week distinct periods:
Phase 1: Pre-Class Preparation
For each specific teaching module, instructors prepared classic clinical cases and teaching materials in accordance with the syllabus. One week prior to the session, they distributed these resources—including clinical guidelines, case reports, and literature reviews—to the students. As a mandatory component of the curriculum, students were required to conduct independent self-directed learning using these materials to identify knowledge gaps before the scheduled class. Thirty minutes prior to the session, participants were tasked with completing a 20-question quiz related to the instructional content, which assessed their baseline theoretical knowledge. To facilitate data recording and statistical analysis, the time taken by each student to complete the test was measured in 5-minute intervals.
Phase 2: In-Class Activities (Session 1)
Step 1 Introduction and Case Orientation: As the initial step of the classroom activities, the instructors briefly introduced the theme, goals, and procedures of the current session. They also presented the basic background and context of the clinical case to the students.
Step 2 Student-Led Teaching Rounds and Discussion: During the second phase, students assumed a leadership role throughout the teaching rounds and associated activities. They were tasked with organizing inquiries, conducting physical examinations, and compiling medical records based on the case scenario. Following group deliberations, designated representatives from each group presented the patient’s chief complaint, medical history, physical examination findings, and laboratory test results. Based on this data, they subsequently formulated corresponding diagnoses and treatment plans.
Throughout this process, the instructors oversaw the students’ performance. Their role involved rectifying issues as they arose, guiding students in proper case reporting techniques, and addressing errors or deviations from standard procedures during physical examinations. Furthermore, the instructors facilitated discussions, corrected misconceptions, posed probing inquiries, and structured the plan for the subsequent phase of learning.
Phase 3: Inter-Session Self-Directed Learning
In the week preceding the second classroom discussion, the learning process transitioned into a student-centered phase of intensive preparation. Students were tasked with conducting comprehensive theoretical reviews and literature searches, specifically targeting the core clinical issues identified during the initial stage. Through a combination of independent study and collaborative group discussions, students systematically explored key aspects of the case, including etiology, epidemiology, pathogenesis, and anatomical pathology, as well as relevant diagnostic, treatment, and preventive strategies. This phase ensured that students possessed a solid theoretical foundation prior to the subsequent advanced discussion.
Phase 4: Advanced Classroom Discussion and Synthesis (Session 2)
During the second formal class session, the pedagogical focus shifted to the presentation of findings and the synthesis of knowledge (aligning with the higher-order cognitive skills of the revised Bloom’s taxonomy, such as analyzing and evaluating). Each postgraduate was required to present their individual insights and analysis derived from the inter-session research. Following these presentations, the instructors provided advanced guidance to deepen the learning experience. Instructors focused on imparting knowledge regarding recent advancements in the field, exploring emerging academic frontiers, and interpreting the latest guideline revisions, thereby enhancing the students’ clinical acumen and broadening their professional knowledge base.
Phase 5: Post-Class Assessment and Feedback
Post-class activities were implemented to quantitatively evaluate the effectiveness of the teaching intervention. Within 30 minutes following the conclusion of the second discussion, students completed a post-teaching quiz. To allow for a valid comparison of learning outcomes, this quiz featured questions identical to those in the pre-class assessment, and students were instructed to record their exact answering time (in minutes). Upon finishing all teaching assignments, students were prompted to complete a satisfaction questionnaire regarding the P-C-T combined teaching mode (Figure 1).
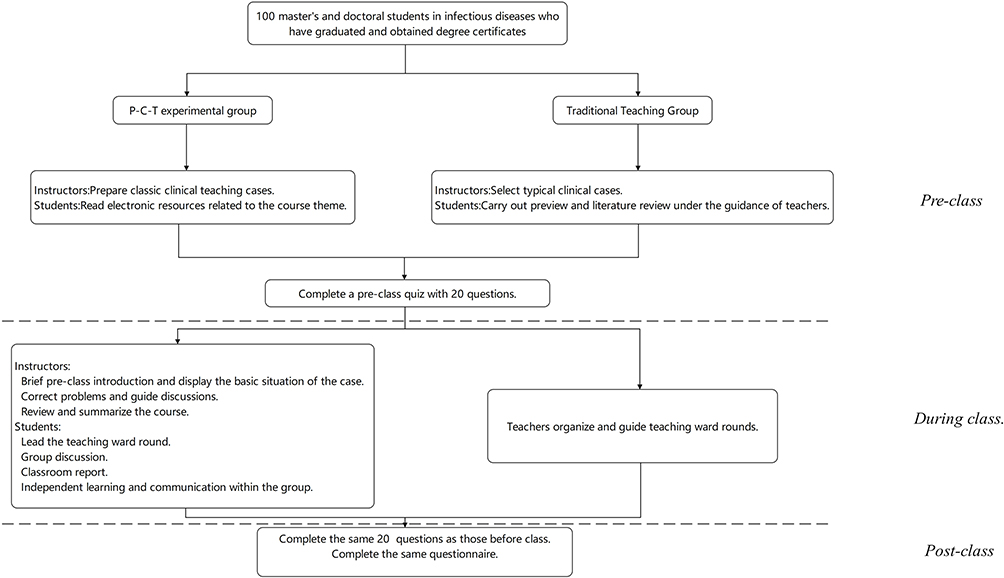 |
Figure 1 Study flowchart and teaching procedures for the P-C-T integrated teaching group and the traditional teaching group. A total of 100 postgraduate trainees (Master of Medicine [MM] and Doctor of Medicine [MD]) specializing in infectious diseases were included and allocated to either the P-C-T experimental group or the traditional teaching group. The flowchart summarizes the instructional sequence across three stages (Pre-class, During class, and Post-class; separated by dashed lines). During the Pre-class stage, instructors prepared clinical teaching cases/materials and students completed preparatory learning; both groups completed a 20-question pre-class quiz. During the During class stage, the P-C-T group implemented student-centered activities (student-led teaching rounds and discussion with instructor facilitation and feedback), whereas the traditional group followed instructor-led teaching rounds/teaching activities guided by teachers. During the Post-class stage, participants completed a post-class quiz using the same 20 questions as the pre-class assessment and completed the same questionnaire. |
Traditional Teaching Group
Students in the traditional teaching group followed a curriculum schedule mirroring that of the P-C-T group, participating in clinical practice activities such as teaching rounds and academic lectures held twice a year. The teaching process was structured into three distinct phases:
Phase 1: Pre-Class Preparation
Prior to the commencement of teaching rounds, instructors selected typical clinical cases in accordance with the teaching syllabus. They subsequently guided students to preview the relevant textbooks and review literature. Additionally, a pre-class quiz was administered, consisting of 20 questions related to the course content that were identical to those used in the P-C-T combined teaching group to ensure baseline comparability.
Phase 2: In-Class Activities
The teaching rounds followed a traditional, instructor-centered pedagogical approach. Instructors delivered didactic lectures covering clinical manifestations, complications, and diagnostic and treatment procedures, tailored to the specific teaching objectives. While instructors incorporated the latest guidelines, consensus statements, and research advancements into their lectures, the primary mode of instruction remained knowledge transmission from teacher to student, rather than student-led inquiry. Throughout the session, instructors supervised the students and addressed any immediate queries.
Phase 3: Post-Class Assessment
Upon the conclusion of the teaching activities, the focus shifted to evaluation. Students completed a post-class assessment identical to that administered to the P-C-T combined teaching group. Finally, to evaluate their learning experience, students filled out the same satisfaction evaluation questionnaire (Figure 1).
Evaluation
Process Assessment
1) The aim of the pre-class and post-class tests was to assess the knowledge acquisition of students during the teaching activities. The test comprised basic theoretical questions (50 points) and clinical case analysis (50 points), totaling 100 points. All questions were designed based on the Revised Bloom’s Taxonomy (Anderson & Krathwohl, 2001), prioritizing the assessment of higher-order thinking skills including analysis and evaluation,15 which categorizes cognitive activities into six distinct levels: memory, understanding, application, analysis, evaluation, and creation. The assessment categories for clinical case analysis were developed based on the Standardized Resident Training Syllabus to ensure content validity. The specific evaluation metrics were reviewed by a panel of senior medical educators to confirm that they accurately reflect the essential clinical competencies required for the postgraduates16 (Note: The internal consistency reliability of these items is reported in the Results section).
2) The questionnaire was structured into two sections: a learning ability questionnaire (LAQ) and a process experience survey (Figure 2). Students were required to complete the questionnaire anonymously, selecting the answers that best describe their actual situations, and were informed that the results of the questionnaire would not impact their academic grades. The learning ability questionnaire entailed a self-assessment of one’s autonomous learning capabilities, covering proficiency in the knowledge, clinical practice skills, complex diagnoses and treatment independent handling skills, and collaborative problem-solving aptitude in clinical scenarios, as well as the satisfaction with the instructional approach, learning efficiency, autonomous learning prowess, research design acumen, and fostering innovative thinking. Adapted from Paul Ramsden’s Course Experience Questionnaire (CEQ)17 and Biggs’ Study Process Questionnaire (SPQ),18 the questionnaire employed a 5-point Likert Scale for evaluation. Positive statements ranged from 10 (strongly agree) to 1 (strongly disagree), while negative statements ranged from 1 (strongly agree) to 10 (strongly disagree). Higher scores on the questionnaire including LAQ and process experience survey indicated more favorable outcomes. The questionnaire’s reliability was assessed yielding a Cronbach’s α coefficient of 0.9.
Figure 2 Continued. Figure 2 Questionnaire items used to assess self-reported learning outcomes and learning experience. This figure presents the full questionnaire administered after completion of the teaching activities. The instrument contains two sections: the Learning Ability Survey (Items 1–15) and the Process Experience Survey (Items 16–27). Items are grouped into conceptual dimensions, including mastery of knowledge system, clinical practical ability, ability to diagnose and treat difficult cases, learning efficiency, autonomous learning ability, level of scientific research design, cultivation of innovative concepts, cultivation of learning interests, and satisfaction with the instructional approach.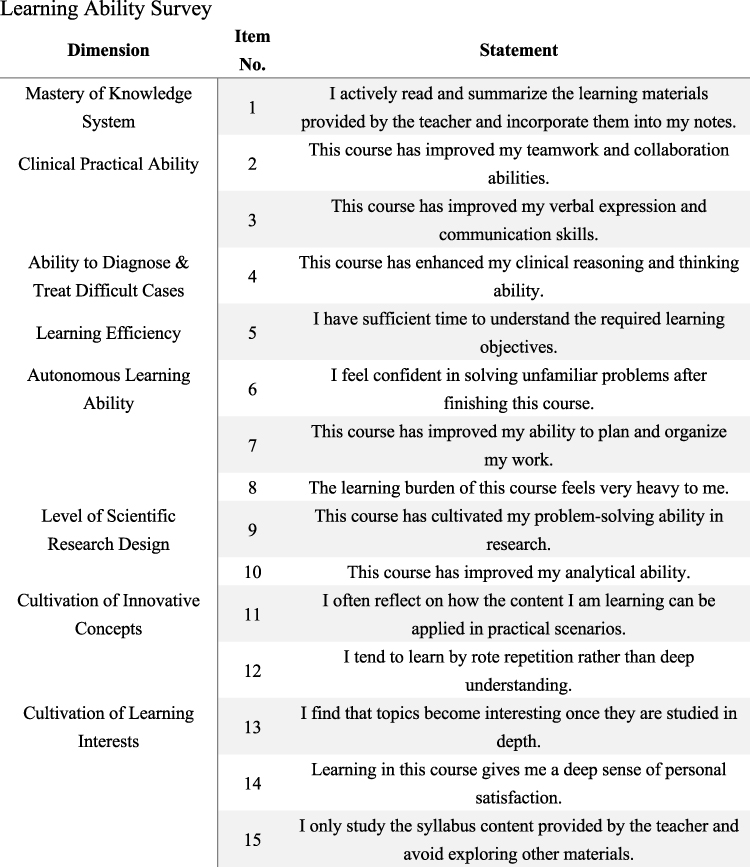
Statistical Analysis
Data management and analysis were performed using Excel and SPSS 27.0 software. Descriptive Statistics: Continuous variables conforming to a normal distribution were expressed as mean ± standard deviation (SD), while non-normally distributed data were presented as median with interquartile range (IQR). Categorical data were described as frequencies and percentages (%). Comparison of Baseline and Outcomes: To assess differences in theoretical test scores and completion times between the two groups, the independent sample t-test was used for normally distributed data, whereas the Mann–Whitney U-test was applied for non-normally distributed data. The Chi-square test was utilized to compare demographic characteristics (eg, gender, grade) to ensure baseline comparability. Pre-post Intervention Analysis: To evaluate the learning improvement within each group (pre-class vs post-class scores), the paired sample t-test was employed. Questionnaire Analysis: Differences in satisfaction scores between groups were analyzed using the Mann–Whitney U-test or independent sample t-test based on data distribution. A two-tailed P-value of less than.05 was considered statistically significant for all analyses.
Result
Basic Characteristics and Information
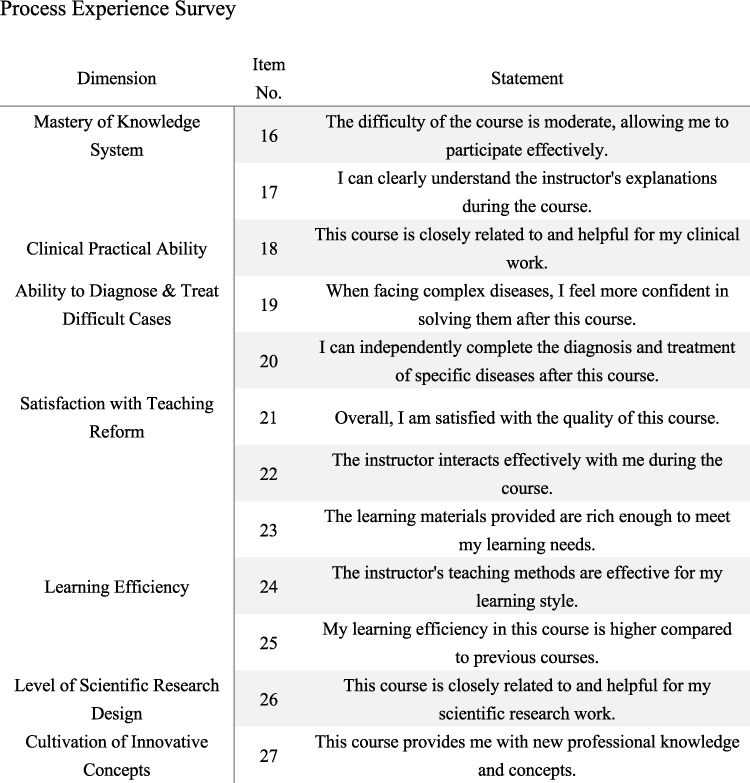
A total of 100 postgraduates with MM Degrees and MD Degrees specializing in infectious diseases were enrolled in this study. They had all finished three years of graduate study and had got their degree certificates. The two groups of postgraduates were comparable in terms of gender, educational background, age, etc., with no statistically significant difference (P>0.05) (Table 1). Throughout the study period, both groups had a 100% classroom attendance rate. Students in the P-C-T combined teaching group all successfully completed the tasks of reading relevant supplementary materials and electronic resources. Meanwhile, students in the traditional teaching group diligently previewed textbooks on time as arranged by the instructors. Both groups timely completed pre-class and post-class tests. A total of 100 questionnaires were distributed, and all 100 were returned, resulting in a 100% recovery rate. Among them, all of the 100 questionnaires were deemed valid, yielding an effective rate of 100%.
 |
Table 1 Basic Characteristics of P-C-T Combined Teaching and Traditional Teaching Group |
Theoretical Performance Difference Between P-C-T Combined Teaching and Traditional Teaching Group
The median total scores, basic theory scores, and clinical case analysis scores of the pre-class test in the P-C-T combined teaching group were 82.00 (80.00, 83.00), 50.00 (49.00, 50.00), and 32.00 (31.00, 33.00) respectively. In comparison, the traditional teaching group achieved scores of 80.00 (79.25, 82.00), 49.00 (48.00, 50.00), and 32.00 (31.00, 33.00) respectively. There was no statistically significant difference in pre-class scores between the two groups (Z=1.722/1.262/0.778, P=0.085/0.207/0.437).
Transitioning to the post-class test results, the median total scores and clinical case analysis scores in the P-C-T combined teaching group were 94.00 (92.00, 95.00) and 37.00 (36.00, 38.00) respectively. Conversely, the traditional teaching group achieved median total scores and clinical case analysis scores of 88.50 (86.25, 90.00) and 34.00 (33.00, 35.00) respectively. A statistically significant difference was observed between the two groups (Z=6.672/6.49, both P<0.001). Moreover, the post-class basic theory test score of the P-C-T combined teaching group was 56.47 ± 1.93, surpassing the score of 53.94 ± 2.02 achieved by the traditional teaching group. The difference was statistically significant (T=5.945, P<0.001).
Upon comparing the performance before and after class, the total scores, basic theory scores, and clinical case analysis scores of the P-C-T combined teaching group increased by 12.22±2.73, 7.34±2.60, and 4.88±0.68 respectively. In contrast, the traditional teaching group saw score increases of 7.44±2.60, 5.06±1.98, and 2.38±1.64 respectively. The improvement in scores of the P-C-T combined teaching group was significantly more pronounced than that of the traditional teaching group, with statistically significant differences (T=8.439/4.826/10.818, all P<0.001) (Table 2).
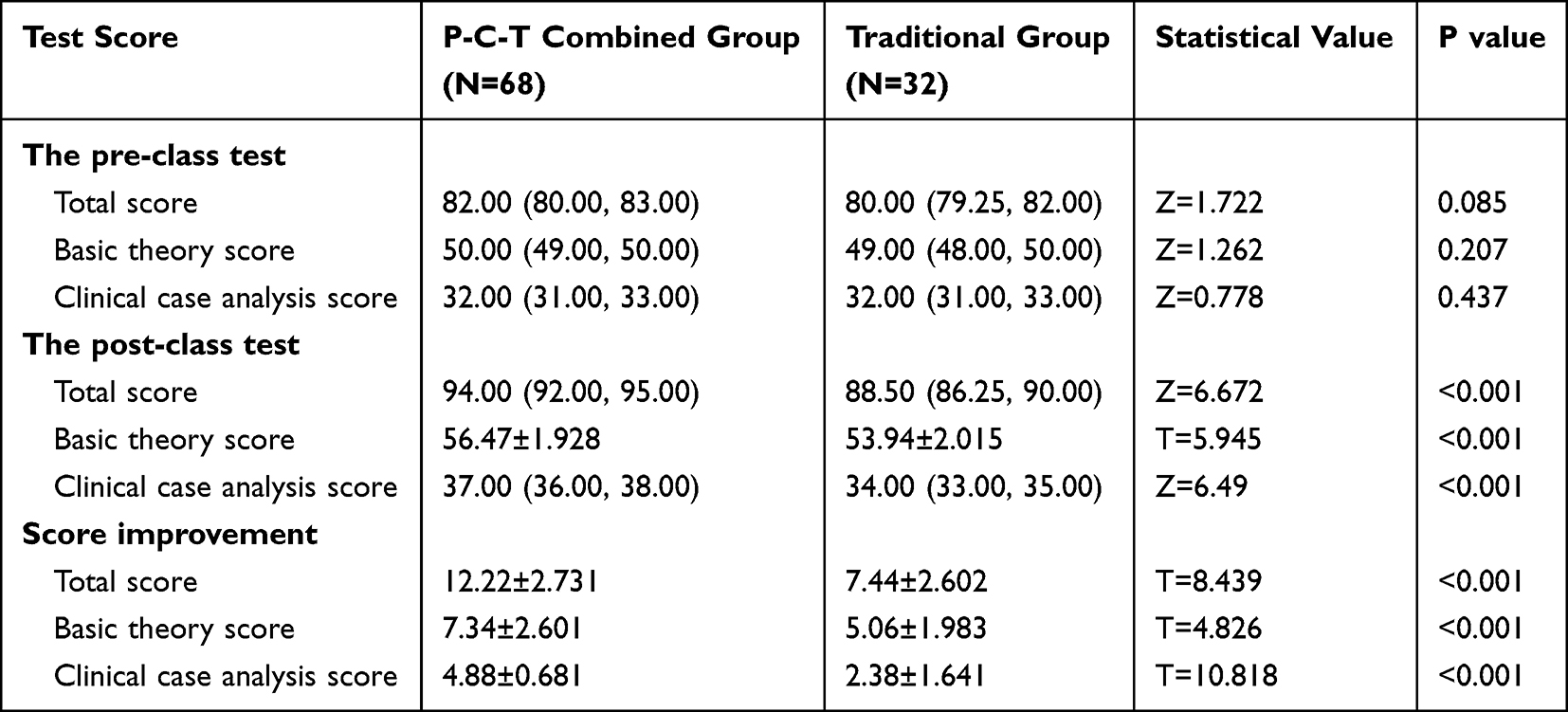 |
Table 2 Theoretical Performance Difference Between P-C-T Combined Teaching and Traditional Teaching Group |
Time Required to Complete Coursework in the P-C-T Combined Teaching and Traditional Teaching Groups
By comparing the time required (in minutes) to complete coursework between the P-C-T combined teaching group and the traditional teaching group, we found that the time allocated to pre-class assignments by students in the P-C-T group was slightly shorter than that of their counterparts in the traditional group (53.25 ± 4.85 min vs 54.53 ± 4.47 min). The difference in mean completion time between the two groups was statistically significant (t = 2.214, P = 0.03). In addition, the time dedicated to post-class assignments in the P-C-T combined teaching group was significantly shorter than that in the traditional teaching group (43.09 ± 5.92 min vs 47.66 ± 5.39 min), with a statistically significant difference between groups (t = 3.38, P < 0.001). Furthermore, when evaluating the reduction in time required to complete coursework from pre-class to post-class, the magnitude of time reduction in the P-C-T combined teaching group was greater than that observed in the traditional teaching group (9.26 ± 5.47 min vs 6.88 ± 4.54 min). This difference was statistically significant (t = 2.25, P = 0.027) (Table 3).
 |
Table 3 Time Required to Complete Coursework in the P-C-T Combined Teaching and Traditional Teaching Groups |
Questionnaire Results Between P-C-T Combined Teaching Group and Traditional Teaching Group
The questionnaire, comprising 27 items across 9 domains, revealed that the P-C-T combined teaching group reported significantly higher levels of self-perceived abilities and learning satisfaction compared with the traditional group (Table 4). Thematically, the improvements were observed in three key areas:
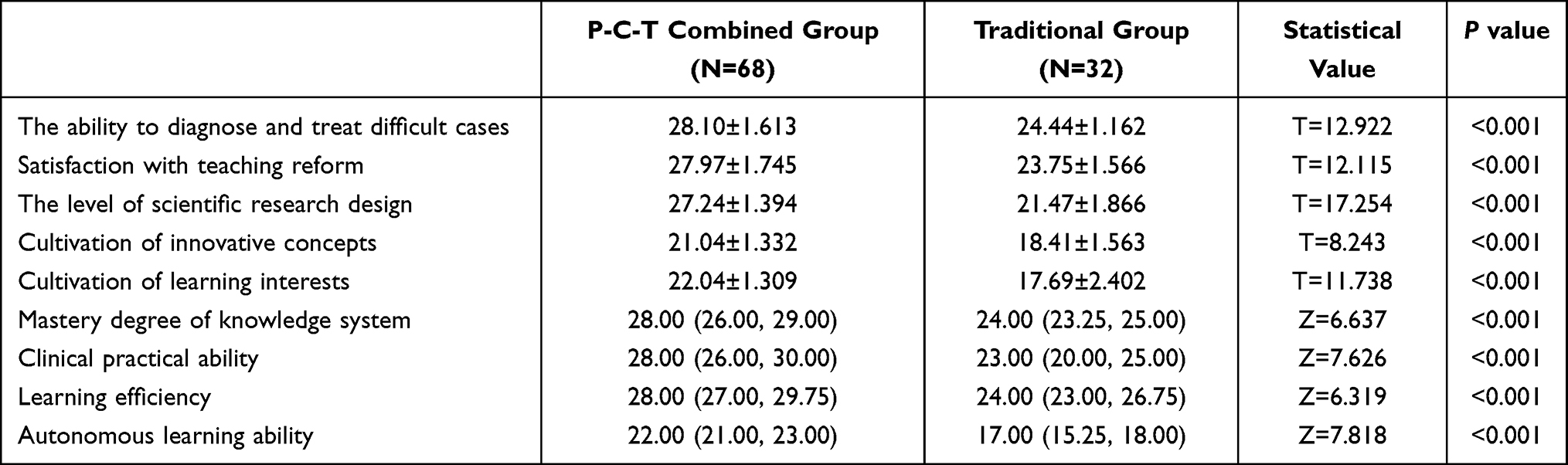 |
Table 4 Questionnaire Results Between P-C-T Combined Teaching and Traditional Teaching Group |
Clinical Competency: Students in the P-C-T group reported significantly higher confidence in diagnosing and managing difficult cases, as well as greater perceived clinical practice ability, compared with the control group (P <0.001). Academic and Research Capabilities: The P-C-T mode notably enhanced students’ scientific research design proficiency and the cultivation of innovative thinking (P < 0.001). Learning Engagement and Efficiency: In terms of the learning process, the P-C-T group expressed superior levels of satisfaction with the teaching reform, learning efficiency, and self-directed learning skills (P < 0.001). Overall, the P-C-T group proved that statistically significant advantages across all assessed domains compared to the traditional teaching group.
Discussion
In recent years, the professional landscape of infectious diseases has evolved significantly, characterized by structural transformations and an expanding scope of diagnosis and treatment.19 Consequently, professionals are tasked with integrating diverse theories and skills to construct a cognitive framework that harmonizes multiple disciplines.20,21 Contemporary medical education increasingly conceptualizes teaching interventions as complex systems rather than isolated techniques, highlighting the importance of integrating complementary instructional strategies to address multifaceted learning outcomes.22 Crucially, mastering this multidisciplinary approach is expected to translate into improved performance on medical board examinations. Furthermore, it directly contributes to optimizing clinical practice and improving patient outcomes by ensuring more precise diagnoses and effective treatment strategies. Therefore, interdisciplinary competence is increasingly important in infectious disease training.
However, the limitations of the traditional teaching mode are gradually becoming apparent in its inability to foster students’ autonomy in thinking and problem resolution. Firstly, the conventional instructor-centric approach fosters passive knowledge absorption, depriving students of the opportunities and cognizance required for active learning.4,23 Consequently, students often exhibit inadequacies in independent learning and problem-solving capabilities.24 Secondly, traditional teaching mode prioritizes knowledge dissemination but falls short in nurturing creativity, critical thinking, and practical acumen. Furthermore, the lack of interactivity and personalization in traditional modes fails to cater to diverse learning needs, thereby dampening enthusiasm and impeding academic outcomes. Hence, it is pressing necessary to explore an educational mode tailored to the training of postgraduates specializing in infectious diseases that aligns with the exigencies of contemporary medical advancements.21,25
PBL, CBL, and TBL represent widely adopted pedagogical frameworks that have garnered considerable attention, each possessing distinct instructional merits. PBL, centered on problem-solving, fosters students’ self-directed learning and the development of effective strategies.6,7 Complementing this, CBL anchors theoretical knowledge in authentic clinical scenarios to enhance clinical acumen, while TBL accentuates collaborative communication and teamwork proficiencies.26 This study integrates these methods into the P-C-T combined teaching mode to leverage their distinct strengths. By synergizing these approaches, the P-C-T mode is intended to support students’ independent learning and problem-solving processes, while fostering positive perceptions of clinical competence. Unlike single-method approaches, this integration creates a comprehensive pedagogical framework that immerses students in real clinical settings, bridging the gap between theoretical knowledge and practical application. Notably, this mode stimulates engagement and encourages active participation, thereby nurturing students’ holistic capabilities.
Regarding academic performance, although there was no disparity in baseline pre-class test scores, the P-C-T group proved that a notable reduction in the time required to complete assessments. This suggests that the P-C-T mode achieves equivalent knowledge proficiency more efficiently, likely attributed to the enriched pre-class preparatory materials.27 Moreover, the post-class test scores revealed a significant elevation in the academic performance of the P-C-T group compared to the traditional group.28 Furthermore, the P-C-T mode appears less susceptible to the “diminishing marginal return effect” compared to traditional methods. While the efficacy of traditional teaching often plateaus despite increased instructional effort, the P-C-T mode sustains performance improvements by continuously engaging students through active problem-solving.29–31 The observed differences in post-class scores and completion times provide preliminary support for the feasibility and potential educational benefits of the P-C-T combined teaching mode.
Beyond objective scores, this study delved into students’ perceptions using a comprehensive questionnaire inspired by Ramsden’s CEQ and Biggs’ SPQ.17,18 The findings unequivocally underscored the heightened acceptance of the P-C-T mode. Students reported significantly higher satisfaction across all domains, particularly with regard to perceived diagnostic confidence, research design awareness, and the cultivation of innovative thinking. These findings corroborate a study by Ramnanan et al, which observed that students exposed to active learning models exhibited a more positive outlook toward their educational journey.32 It should be noted that these questionnaire findings reflect self-reported perceptions rather than objectively measured clinical competence, and previous studies have demonstrated that self-assessment may not reliably correspond to actual performance.
There are several limitations in this study. Primarily, this research was confined to a single academic discipline; given the inherent nuances of infectious diseases, the efficacy of the P-C-T mode in alternative fields may yield disparate results. Secondly, the study utilized a historical control design based on enrollment cohorts rather than random assignment. Additionally, subgroup comparisons were not conducted, precluding insights into potential discrepancies among students of different academic standings. Potential heterogeneity between MM and MD trainees could not be fully examined. Although adapted from established instruments, the structure of the questionnaire may limit construct precision. Finally, due to practical constraints, a blind method was unfeasible, potentially introducing subjective elements that could influence the outcomes.
Conclusion
The P-C-T integrated teaching mode demonstrated favorable associations with theoretical knowledge acquisition and self-reported learning outcomes among infectious disease postgraduates compared with traditional teaching approaches. It effectively bridges the gap between theory and practice by fostering critical clinical thinking, research capabilities, and self-directed learning. While these findings suggest potential educational value, the P-C-T teaching model may be cautiously applied as a structured instructional framework in postgraduate infectious disease training.33 Further multi-center and methodologically rigorous studies incorporating objective performance-based assessments are warranted to refine this model and to determine its broader applicability across diverse clinical training contexts.
Abbreviations
PBL, Problem-based learning; CBL, Case-based learning; TBL, Team-based learning; MM, Master of Medicine; MD, Doctor of Medicine.
Data Sharing Statement
The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study has been approved by the Ethic Committee of the Hebei Medical University (NO. YJGZ202205), China. The study protocol was conducted in accordance with the principles described in the Declaration of Helsinki. All participants were fully informed and consented to their participation in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work has funded by Postgraduate Education Reform Project of Hebei Medical University (YJGZ202205).
Disclosure
The authors declare no competing interests in this work.
References
1. Grundy B, Houpt E. Complexity of infectious diseases compared with other medical subspecialties. Open Forum Infect Dis. 2023;10(9):ofad463. doi:10.1093/ofid/ofad463
2. Arias CA, Pirofski LA. Infectious diseases training in the 21st century: a glass half full or half empty? J Infect Dis. 2024;229(3):621–12. doi:10.1093/infdis/jiad569
3. Baker RE, Mahmud AS, Miller IF, et al. Infectious disease in an era of global change. Nat Rev Microbiol. 2022;20(4):193–205. doi:10.1038/s41579-021-00639-z
4. Prober CG, Heath C. Lecture halls without lectures--a proposal for medical education. N Engl J Med. 2012;366(18):1657–1659. doi:10.1056/NEJMp1202451
5. Hopper MK. Alphabet soup of active learning: comparison of PBL, CBL, and TBL. HAPS Educ. 2018;22(2):144–149. doi:10.21692/haps.2018.019
6. Barrows HS. A taxonomy of problem-based learning methods. Med Educ. 1986;20(6):481–486. doi:10.1111/j.1365-2923.1986.tb01386.x
7. Yew EHJ, Goh K. Problem-based learning: an overview of its process and impact on learning. Health Prof Educ. 2016;2(2):75–79. doi:10.1016/j.hpe.2016.01.004
8. Thistlethwaite JE, Davies D, Ekeocha S, et al. The effectiveness of case-based learning in health professional education. A BEME systematic review: BEME Guide No. 23. Med Teach. 2012;34(6):e421–e444. doi:10.3109/0142159X.2012.680939
9. Zhang W, Wei J, Guo W, et al. Comparing the effects of team-based and problem-based learning strategies in medical education: a systematic review. BMC Med Educ. 2024;24(1):172. doi:10.1186/s12909-024-05107-9
10. Parmelee D, Michaelsen LK, Cook S, Hudes PD. Team-based learning: a practical guide: AMEE guide no. 65. Med Teach. 2012;34(5):e275–e287. doi:10.3109/0142159X.2012.651179
11. Burgess A, van Diggele C, Roberts C, Mellis C. Team-based learning: definition and application. BMC Med Educ. 2020;20(Suppl 2):460. doi:10.1186/s12909-020-02287-y
12. Kibble JD, Bellew C, Asmar A, Barkley L. Team-based learning in large enrollment classes. Adv Physiol Educ. 2016;40(4):435–442. doi:10.1152/advan.00095.2016
13. Zheng QM, Li YY, Yin Q, et al. The effectiveness of problem-based learning compared with lecture-based learning in surgical education: a systematic review and meta-analysis. BMC Med Educ. 2023;23(1):546. doi:10.1186/s12909-023-04531-7
14. Zhao W, He L, Deng W, Zhu J, Su A, Zhang Y. The effectiveness of the combined problem-based learning (PBL) and case-based learning (CBL) teaching method in the clinical practical teaching of thyroid disease. BMC Med Educ. 2020;20(1):381. doi:10.1186/s12909-020-02306-y
15. Anderson LW, Krathwohl DR, eds.. A Taxonomy for Learning, Teaching, and Assessing: A Revision of Bloom’s Taxonomy of Educational Objectives. New York: Longman; 2001.
16. Cook DA, Reed DA. Appraising the quality of medical education research methods: the medical education research study quality instrument and the newcastle-ottawa scale-education. Acad Med. 2015;90(8):1067–1076. doi:10.1097/ACM.0000000000000786
17. Ramsden P. A performance indicator of teaching quality in higher education: the course experience questionnaire. Stud High Educ. 1991;16(2):129–150. doi:10.1080/03075079112331382944
18. Biggs J, Kember D, Leung DY. The revised two-factor study process questionnaire: r-SPQ-2F. Br J Educ Psychol. 2001;71(Pt 1):133–149. doi:10.1348/000709901158433
19. Murray CJL, Ikuta KS, Sharara F; Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
20. Charani E, McKee M, Ahmad R, et al. Optimising antimicrobial use in humans - review of current evidence and an interdisciplinary consensus on key priorities for research. Lancet Reg Health Eur. 2021;7:100161. doi:10.1016/j.lanepe.2021.100161
21. Frank JR, Snell LS, Cate OT, et al. Competency-based medical education: theory to practice. Med Teach. 2010;32(8):638–645. doi:10.3109/0142159X.2010.501190
22. Hean S, Craddock D, Hammick M, Hammick M. Theoretical insights into interprofessional education: AMEE Guide No. 62. Med Teach. 2012;34(2):e78–101. doi:10.3109/0142159X.2012.650740
23. Bunce DM, Neiles KY, Neiles KY. How long can students pay attention in class? A study of student attention decline using clickers. J Chem Educ. 2010;87(12):1438–1443. doi:10.1021/ed100409p
24. Wartman SA. The empirical challenge of 21st-century medical education. Acad Med. 2019;94(10):1412–1415. doi:10.1097/ACM.0000000000002866
25. Powell DE, Carraccio C. Toward competency-based medical education. N Engl J Med. 2018;378(1):3–5. doi:10.1056/NEJMp1712900
26. Alizadeh M, Masoomi R, Mafinejad MK, Parmelee D, Khalaf RJ, Norouzi A. Team-based learning in health professions education: an umbrella review. BMC Med Educ. 2024;24(1):1131. doi:10.1186/s12909-024-06147-x
27. Hmelo-Silver CE, Duncan RG, Chinn CA. Scaffolding and achievement in problem-based and inquiry learning: a response to Kirschner, Sweller, and Clark (2006). Educ Psychol. 2007;42(2):99–107. doi:10.1080/00461520701263368
28. Larsen DP, Butler AC, Roediger HL. Test-enhanced learning in medical education. Med Educ. 2008;42(10):959–966. doi:10.1111/j.1365-2923.2008.03124.x
29. Young JQ, Van Merrienboer J, Durning S, Ten Cate O. Cognitive load theory: implications for medical education: AMEE Guide No. 86. Med Teach. 2014;36(5):371–384. doi:10.3109/0142159X.2014.889290
30. Sweller J. Element interactivity and intrinsic, extraneous, and germane cognitive load. Educ Psychol Rev. 2010;22(2):123–138. doi:10.1007/s10648-010-9128-5
31. Leppink J, van den Heuvel A. The evolution of cognitive load theory and its application to medical education. Perspect Med Educ. 2015;4(3):119–127. doi:10.1007/s40037-015-0192-x
32. Ramnanan CJ, Pound LD. Advances in medical education and practice: student perceptions of the flipped classroom. Adv Med Educ Pract. 2017;8:63–73. doi:10.2147/AMEP.S109037
33. Carraccio C, Wolfsthal SD, Englander R, Ferentz K, Martin C. Shifting paradigms: from Flexner to competencies. Acad Med. 2002;77(5):361–367. doi:10.1097/00001888-200205000-00003
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.