Back to Journals » Advances in Medical Education and Practice » Volume 17
Evaluating Student Engagement and Effectiveness of the Scenario-Case Discussion Learning Model in Medical Microbiology Education
Authors Chen J, Li X, Zhang T ![]() , Chen X, Jiang P, Xue X, Li W
, Chen X, Jiang P, Xue X, Li W
Received 2 April 2026
Accepted for publication 26 June 2026
Published 10 July 2026 Volume 2026:17 611466
DOI https://doi.org/10.2147/AMEP.S611466
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sateesh Arja
Jun Chen,1 Xinyang Li,2 Ting Zhang,1 Xinan Chen,1 Pengfei Jiang,1 Xiangyang Xue,1 Wenshu Li1
1Department of Pathogen Biology and Immunology, School of Basic Medical Sciences, Wenzhou Medical University, Zhejiang, 325032, People’s Republic of China; 2Department of Clinical Medicine, School of First Clinical Medicine, Wenzhou Medical University, Zhejiang, 325032, People’s Republic of China
Correspondence: Xiangyang Xue, Email [email protected] Wenshu Li, Email [email protected]
Purpose: Case-based learning (CBL) in medical microbiology teaching serves as a crucial pedagogical link that bridges foundational knowledge and clinical thinking, but student participation, enthusiasm, and initiative are often lacking during the foundational learning stage. We designed a scenario-case discussion (SCD) model and evaluated its effectiveness in ensuring that under the student-centered principle, each student is motivated to actively participate and engages in self-directed learning and knowledge reconstruction.
Methods: SCD activity was conducted over three academic years involving 240 second-year undergraduate medical students majoring in clinical medicine for a prospective quasi-experiment. Participants were divided into two classes: one receiving conventional CBL (120 students) and the other receiving SCD model (120 students). Knowledge comprehension and retention were assessed through content-based tests, while student engagement was evaluated based on classroom interactions and post-class feedback. Participant perceptions of the SCD were evaluated via questionnaires.
Results: Despite slight variability in participants’ age and gender, both the SCD and control classes showed significant improvement in pre- and post-test scores. Particularly noteworthy is the greater gain observed in the SCD group compared to the control class (mean increase: 1.99 vs. 1.03 points; P < 0.05). Analysis of final examination revealed that scores in the SCD class were significantly higher than those in the control class across all academic years (P < 0.05 for all). Post-class questionnaires showed that over 74% of students gained a positive learning experience, such as stimulated interests, enhanced initiative, proactivity, a first-hand understanding of the doctor-patient relationship, and a better comprehension of the course content. Most notably, as many as 96.67% of the students agreed that the SCD approach ensured the participation of every student. Encouragingly, the SCD class demonstrated a significantly higher frequency of questions raised both in and after class.
Conclusion: The SCD teaching model significantly improved the educational outcomes of CBL sessions in medical microbiology. Given the current educational goal of fostering students as constructors and creators of knowledge, the SCD teaching practice may serve as a positive driver.
Keywords: medical microbiology, scenario-case discussion, evaluation, educational outcomes
Introduction
In the modern era of medical science, innovative educational activities emphasize a student-centered approach, highlighting the guiding role of instructors.1 This approach encourages students to “connect the dots” across multiple dimensions of learning, promoting active knowledge acquisition and facilitating the transformation of theoretical knowledge into practical competency.2 Medical microbiology is a fundamental course for infectious diseases and serves as a bridging course that establishes the correlation between pathogens and clinical diseases. In addition to theoretical teaching and experimental teaching, the case-based learning (CBL) session is also an important component of this course, which is an excellent practical activity for training students to develop clinical reasoning.3 In essence, it is a form of the flipped classroom (FC), which is student-centered.4–6 The CBL teaching mode adopted by our teaching team includes the following: based on the provided clinical case, each group was required to analyze the pathogen responsible for the disease, describes its biological characteristics, pathogenic features, diagnostic and prevention principles, raises questions and conducts discusses.
Although CBL promotes active learning, enhances classroom vitality, and creates a positive learning atmosphere, the actual teaching outcomes of CBL implemented by our team have been unsatisfactory. The key reasons are: First, the students are sophomores (second-year university students) with weak knowledge application skills. Second, student participation is low (often only 1–2 students per group complete the presentation task) and their enthusiasm is insufficient. Third, it cannot guarantee that every student has a clear learning task, and there is a lack of means to control substantive collaboration within groups. Therefore, improving the quality of CBL learning, attending to the progress and responses of each student, and cultivating students’ sense of responsibility and interest in learning have long been a central concern of our teaching team.
“Scenario-based learning (SBL)” is a structured learning model driven by roles, using a script as a vehicle and scenario-based tasks as challenges. It transforms the classroom into a “knowledge drama” allowing students to actively engage in “performance” and “collaboration” to achieve autonomous knowledge construction, deep processing, and creative application.7 This learning model is particularly suitable for fields like medical education that require high contextualization, strong interactivity, and deep immersion.8 The learning process unfolds progressively through acts: ① Students understand the scenario and their own roles; ② Driven by their role identity, they independently consult materials, collaborate in groups, analyze, discuss, and produce knowledge outputs; ③ They present their findings in their role (eg., as a “diagnosis and treatment plan presentation”) and respond to questions from multiple sides; ④ After stepping “out of character”, students debrief and reflect, while the teacher, acting as the “director”, provides a summary and evaluation. SBL has the key advantage of overcoming insufficient student participation; role identity gives students a sense of responsibility and immersion, significantly enhancing intrinsic motivation. Research indicates that scenario-based role-playing courses can significantly improve medical students’ communication skills and teamwork abilities.9 SBL promotes deep learning and knowledge restructuring,10 and has significant advantages in improving medical students’ integration of theory and practice, self-directed learning ability, communication skills, humanistic literacy, professional identity, and teaching satisfaction.11 Furthermore, a study has shown that a teaching model combining scenario integration and case discussion (ie., scenario-case discussion, SCD) can significantly benefit pre-clinical medical students in their professional course learning, leading researchers to advocate for this teaching model in pre-clinical education.12
SCD is a highly immersive teaching method that transforms case discussions into a multi-act dramatic narrative. Students advance their learning by taking on different roles, analyzing staged information, and engaging in dynamic decision-making.13–15 It is an innovative teaching model that integrates a “scenario script” with a “clinical case” to enhance students’ learning initiative and clinical reasoning ability. Compared with conventional CBL teaching, the scenario-act design achieves deeper cognitive and emotional involvement through “suspense”, “rhythm control”, and “decision pressure”, while ensuring effective control of everyone’s participation. By releasing information in stages, students immerse themselves in simulating patients, doctors, or presenters, making judgments or performing based on the available information in each act. This deepens the professional reasoning process, forces the thinking process to “slow down” and become visible. In each act’s discussion, the thinking is clarified: What are the characteristic manifestations of the disease? What is my diagnosis/judgment? What key information am I basing this on? How does this information link to the pathogen? This repeated training externalizes implicit, rapid professional thinking into a structured thinking process that can be examined, discussed, and optimized, precisely enhancing the core competencies of critical thinking and clinical reasoning. Furthermore, the SCD method, through scenario integration, achieves the “active and practical application” of knowledge. For example, in the case analysis segment, students playing the role of a doctor are better able to appreciate obtaining key information from potentially unclear patient descriptions, thereby learning communication skills, empathy, and professional values far beyond rote learning.16 In the interactive segments, the ability to integrate and apply knowledge is demonstrated. Students need to actively recall and integrate knowledge points scattered across multiple courses like microbiology, pathology, and pharmacology, applying them instantly within dynamic case scenarios. This process exercises teamwork skills including listening, speaking, communicating, and building consensus.
Therefore, given the advantages of the SCD teaching model, our teaching team has adopted the SCD method in medical microbiology teaching, aiming to evaluate its effectiveness in terms of knowledge retention, student participation, teaching perception, and continuous learning ability. Based on the characteristics of our medical microbiology course setup, the specific SCD scheme we applied consists of three modules: ① Pre-class: guidance, role assignment, preparation, and pre-test; ② In-class: case-based presentation, role-playing, interactive questioning, class summary, and in-class test; ③ Post-class: feedback, submission of materials, and a final semester exam for assessment. In the contemporary era of highly developed internet, multi-dimensional learning models have become essential.17,18 The adoption of the SCD teaching model in the medical microbiology course cultivates clinical reasoning skills in pre-clinical medical students and encourages them to engage in self-directed learning and knowledge reconstruction.
Materials and Methods
Study Design and Participant Selection
A prospective quasi-experimental study utilizing a non-randomized control group design was conducted over three academic years (2022/23, 2023/24, and 2024/25). For each academic year, four classes (20 students per class) majoring in clinical medicine were selected to participate in the pedagogical practice. These four classes were divided into two groups: two classes received conventional CBL, while the other two received SCD instruction. Each of the two teaching models lasted for 4 class hours (totaling 160 minutes) per session and was conducted once per academic year. A total of 240 second-year undergraduate medical students by the cluster sampling from Wenzhou Medical University were enrolled in this program and had provided informed consent. All research stages were conducted in strict accordance with the project plan authorized by the Expert Committee of the School of Basic Medical Sciences at Wenzhou Medical University. Participants were notified of their right to withdraw from the study at any time without providing a reason. The allocation of classes to either the SCD group or the control group was determined by a drawing of lots.
Implementation of the Pedagogical Process
The SCD pedagogical model was implemented and evaluated across the selected classes over three academic years. Throughout this period, the course content, syllabus, faculty resources, and instructional methodologies remained consistent. To minimize instructor variability, a single lead instructor, nationally certified by the “Key Faculty Training Program” sponsored by the Ministry of Education of China, conducted both the experimental SCD and conventional CBL classes, ensuring pedagogical rigor. The SCD instructional model was executed in three stages: pre-class, in-class, and post-class. The specific tasks and real classroom scenarios for each stage are illustrated in Figure 1.
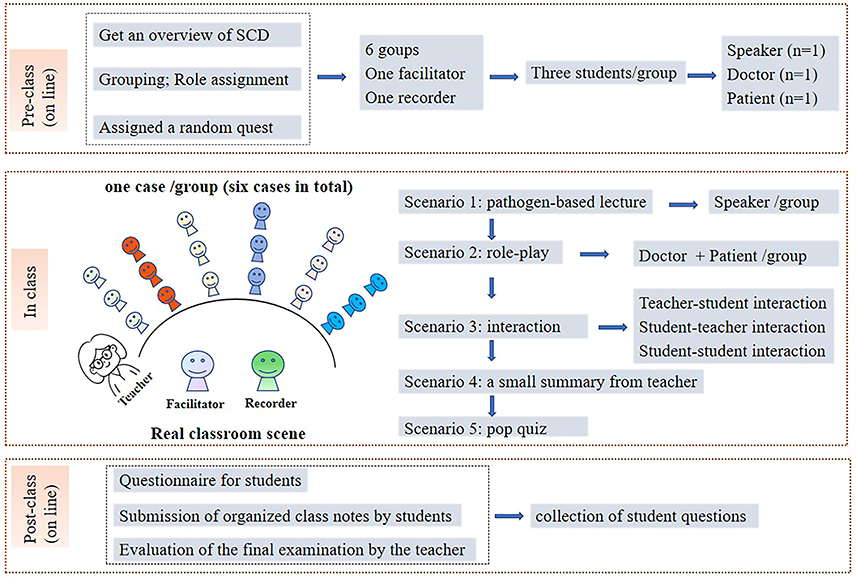 |
Figure 1 Schematic diagram of the SCD teaching model. |
Stage 1 (Pre-class, online): Before implementation, students first gain an overview of SCD via an online learning platform (https://www.zjooc.cn/) and then complete three specific tasks online.
- Task 1 (Grouping and role allocation): The learning platform utilized a digital “drawing of lots” to designate one facilitator and one recorder. The remaining students were organized into six groups of three. Within each group, roles were assigned as Keynote Speaker, Doctor, and Patient, also determined via random selection, and detailed task descriptions for each role were accessible through the “SCD Teaching” module on the platform.
- Task 2 (Case acquisition and role preparation): Cases were assigned to groups using a randomized draw. Once allocated, the details of six cases were made public to the entire class to ensure that every student conducted thorough pre-study and preparation for all clinical scenarios. Groups were required to prepare their presentation slides and role-play simulations based on their assigned cases.
- Task 3 (Baseline assessment): Students completed a set of pre-test randomly selected from a single case on the learning platform at a given time and place to evaluate their initial understanding of the course content.
Stage 2 (In-class, in-person): The SCD pedagogical session is structured into five “scenarios”, with a facilitator student hosting the entire process:
- Scenario 1 (Keynote presentation): The speaker from each group delivers a 5-minute presentation on the assigned case-related pathogen, covering its primary biological characteristics, pathogenicity, laboratory diagnosis, and prevention/treatment protocols. The recorder and other students take notes on key information.
- Scenario 2 (Role-play simulation): The remaining two students in each group role-play as the patient and the doctor. They enact a clinical scenario where the patient describes symptoms and the doctor responds based on the narratives and physical examination reports. This interactive session aims to complete the clinical diagnostic process within 10 minutes. The recorder documents the major points.
- Scenario 3 (Interactive discussion): A Q&A session involving teacher-to-student, student-to-teacher, and student-to-student interactions is conducted regarding the case and the associated pathogen. This segment lasts 10 minutes, with the recorder documenting the discussion highlights.
- Scenario 4 (Classroom summary): The teacher provides a 3-minute summary of the overall session and student performance, synthesizing the core learning content and highlighting critical focus areas or common pitfalls.
- Scenario 5 (In-class assessment): Students complete a 7-minute online quiz via mobile devices or laptops, based on the same case as the pre-class test but with increased difficulty, to assess their depth of learning.
Stage 3 (Post-class, online): After the in-class sessions, students are required to complete the following tasks:
- Task 1 (Perception survey): A questionnaire is administered to collect students’ feedback, perceptions, and attitudes toward the SCD pedagogical model.
- Task 2 (Submission of class notes): Every student must submit a set of organized and refined classroom notes based on the session’s discussions and presentations.
- Task 3 (Final learning outcome evaluation): At the end of the semester, the teacher evaluate and compare the final academic performance of the SCD groups versus the control groups to assess long-term learning efficacy.
Meanwhile, conventional CBL teaching served as the control group for the SCD intervention, as described below:
Stage 1 (Pre-class, online): Students were randomly divided into six groups of three or four, received case materials, and completed a pre-class test (eg., baseline assessment) via an online learning platform (https://www. zjooc. cn/). Groups were required to prepare their presentation slides.
Stage 2 (In-class, in-person): Organized by the teacher.
- Presentation: The speaker from each group delivers a 20-minute presentation similar to that described in Scenario 1 of the SCD class.
- Interactive discussion: A Q&A session similar to that described in Scenario 3 of the SCD class is then conducted, lasting 5 minutes.
- Classroom summary: The teacher provides a 3-minute summary similar to that described in Scenario 4 of the SCD class.
- In-class assessment: Students complete a 7-minute online quiz similar to that described in Scenario 5 of the SCD class.
Stage 3 (Post-class, online): After the in-class sessions, the tasks are as follows:
- Students: submit a set of organized and refined classroom notes based on the session’s discussions and presentations.
- Teachers: evaluation of final learning outcome.
Data Collection
Clinical cases of bacterial and viral infectious diseases, were randomly selected from the institutional case library established by the Department of Medical Microbiology at the School of Basic Medical Sciences, Wenzhou Medical University. Six cases were extracted per class (ensuring identical case sets for both SCD and CBL). A detailed case example of HBV infection is provided in Supplementary document 1.
The SCD and control groups underwent pre-class baseline tests and post-class tests centered on the pathogen-related knowledge framework addressed in the case, also including the end-of-semester examinations. All test items were sourced from the “Medical Microbiology Item Bank” established by the Department of Medical Microbiology at the School of Basic Medical Sciences, Wenzhou Medical University. Additionally, a post-class perception questionnaire consisting of eight items was administered exclusively to the SCD group to assess the model across five dimensions: interest, comprehension, motivation, learning experience, and practical utility. Responses were collected using a 5-point Likert scale, with options ranging from “Strongly Agree” and “Agree” to “Neutral”, “Disagree” and “Strongly Disagree”. The reliability and validity of both the test questions and the questionnaire were examined.
Assessment Metrics
The primary evaluation metric was student knowledge scores, derived from three sources: pre-tests, post-tests, and a standardized final examination at the end of the semester. Student engagement was quantitatively monitored for both the SCD and control groups. This included: (i) in-person engagement: the frequency of students answering and posing questions during the session. (ii) extended engagement: the total number of academic questions raised by students from the conclusion of the session until the end of the semester. It should be noted that only course-content-related questions were included in the tally; non-academic inquiries were excluded.
Statistical Analysis
The collected assessment data were entered into Microsoft Excel (Microsoft Corp.) spreadsheets, and statistical analyses were performed using GraphPad Prism 9.5 (GraphPad Software Inc). Descriptive statistics are presented as frequencies (percentages), means, standard deviations (SD), and 95% confidence intervals (95% CI). A one-way analysis of variance (ANOVA) was employed for broader comparisons, while Student’s t-test was used to compare differences between the SCD group and the control group. Statistical significance was defined as P < 0.05. Feedback and survey results are presented as percentages.
Results
A total of 240 second-year undergraduate medical students were enrolled in the study. The mean ages of samples from the 2022/23, 2023/24, and 2024/25 academic years were 20.08 years (SCD class) /20.17 years (control class), 20.15 years (SCD class) /20.11 years (control class), and 20.12 years (SCD class) /20.03 years (control class), respectively. The corresponding standard deviations were 0.69 years (SCD class) /0.74 years (control class), 0.74 years (SCD class) /0.75 years (control class), and 0.82 years (SCD class) /0.66 years (control class), respectively, showing some variability in the age of the participants (Table 1). In 2022/23, the SCD class had 54.17% male and 45.83% female students, while the control class had 51.67% male and 48.33% female students. In 2023/24, the SCD class had 55.00% male and 45.00% female students, while the control class had 52.50% male and 47.50% female students. In 2024/25, the SCD class had 53.33% male and 46.67% female students, while the control class had 55.83% male and 44.17% female students (Table 2).
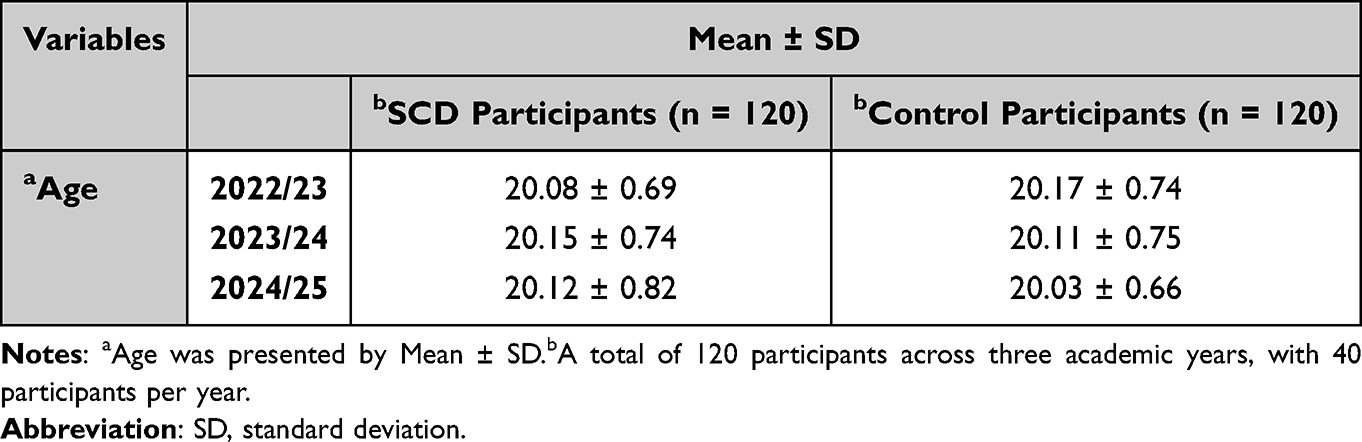 |
Table 1 Mean Age of Participants |
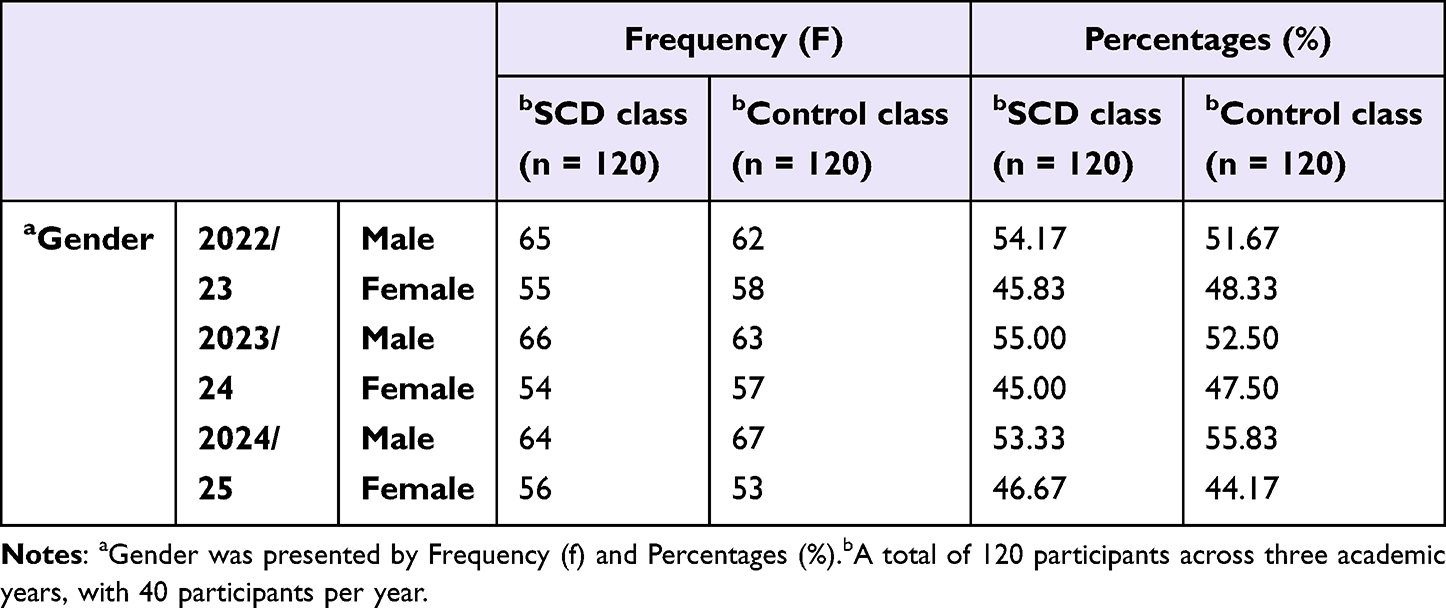 |
Table 2 Gender Status of Participants |
Pre-class learning assessments conducted for 80 students each academic year (40 in the control group and 40 in the SCD group) showed no statistically significant differences in mean knowledge scores between the SCD and control groups (P < 0.05). This suggests that the baseline knowledge levels of both groups were comparable. However, post-class learning effectiveness tests revealed that the SCD group achieved significantly higher scores than the control group (P < 0.05, shown in Figure 2), suggesting that the SCD model yielded superior instructional outcomes. Analysis of the knowledge score increments (post-test minus pre-test) showed that both groups experienced a significant increase in scores following the sessions (P < 0.05). Specifically, the SCD group showed a mean increase of 1.99 ± 0.02 points over the three academic years, while the control group showed a mean increase of 1.03 ± 0.12 points. This improvement was significantly more pronounced in the SCD group compared to the control group (P < 0.05, shown in Table 3). All reliability and validity indicators of the test items met the required psychometric standards. Specific pre-class and post-class test questions based on the clinical case of “HBV Infectious Disease” along with a brief analysis of the reliability and validity testing, are provided in Supplementary document 2.
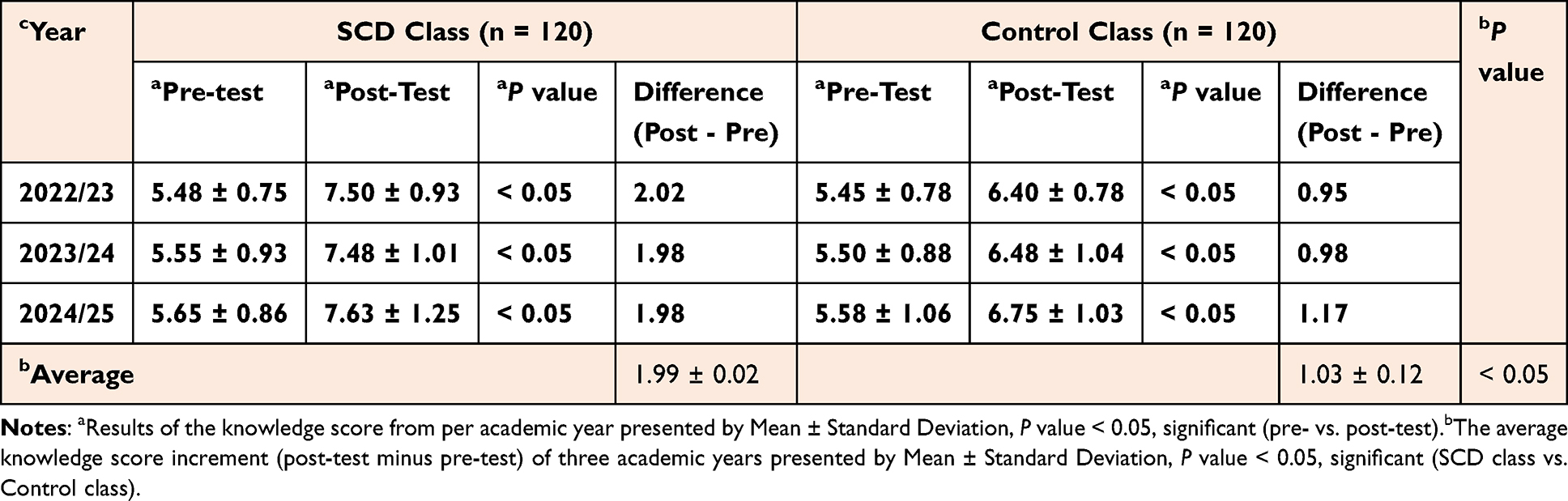 |
Table 3 Change in Knowledge Score Increments |
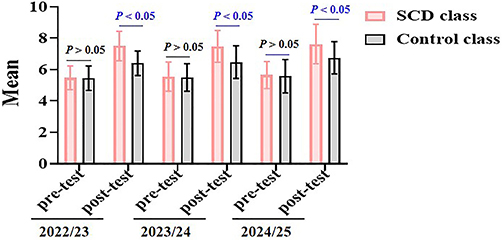 |
Figure 2 Comparison of knowledge scores of pre- and post-test. A total of 80 students per year were included in the analysis. |
Similarly, analysis of the final examination results over the three academic years demonstrated that the SCD group achieved superior academic performance each year. Compared to their respective control groups, the differences were statistically significant (P < 0.05, shown in Figure 3).
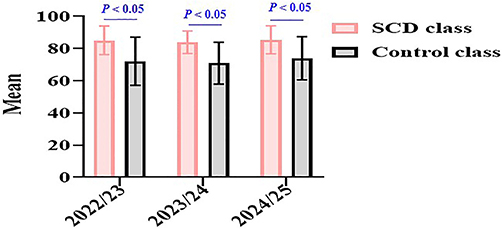 |
Figure 3 Comparison of the final examination over the three academic years. |
A total of 120 valid questionnaire responses were collected in the SCD group across three academic years and analyzed using SPSS 26.0 software. The results demonstrated that the overall Cronbach’s α coefficient for all scale items was 0.842 (> 0.8), showing good reliability. Furthermore, both content validity and construct validity of the questionnaire met the required standards. Over 80% of students believed that the SCD model stimulated their interests in learning and fostered a vibrant classroom atmosphere. 75.83% of students felt that SCD effectively enhanced their initiative and proactivity in learning. 74.17% of students reported gaining a first-hand, experiential understanding of the doctor-patient relationship. More than 70% of students stated that the SCD format improved their comprehension of the discussion topics, and these students expressed a willingness to invest more time and effort into the course activities and agreed that the SCD model should be piloted in other medical curricula. Most notably, 96.67% of students agreed that the SCD approach effectively ensured the participation of every student (shown in Figure 4).
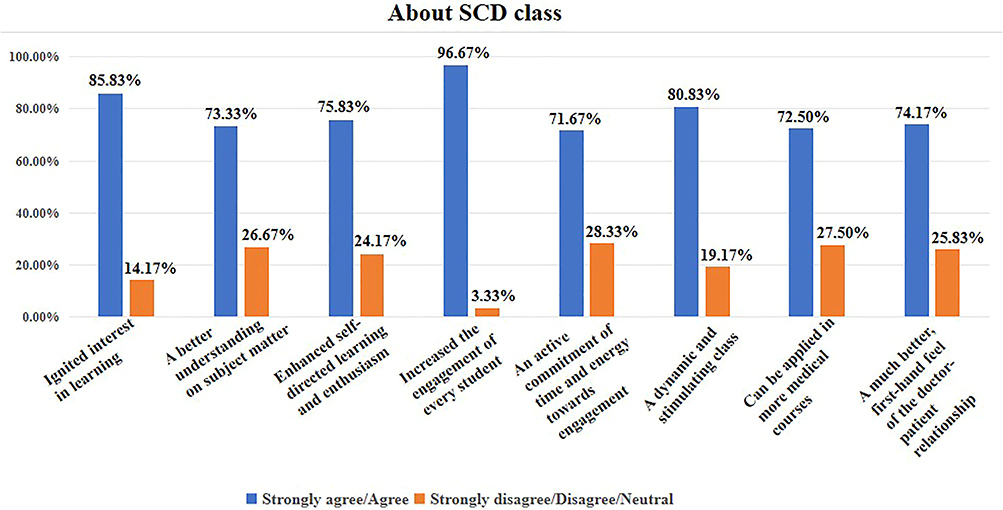 |
Figure 4 Questionnaire feedback on the SCD teaching model. A total of 120 students across three years were included in the analysis. |
Over the three academic years, students in the SCD group recorded a total of 105 instances of answering and posing questions in-class, compared to 41 instances in the control group.
Regarding engagement from the end of the case-based discussion sessions to the end of the semester, students in the SCD group further raised a total of 39 academic inquiries related to the course content across the three years, while 19 inquiries were raised in the control group (shown in Table 4). These results suggest that the SCD model fosters superior sustained learning effects and continuous interest in the curriculum.
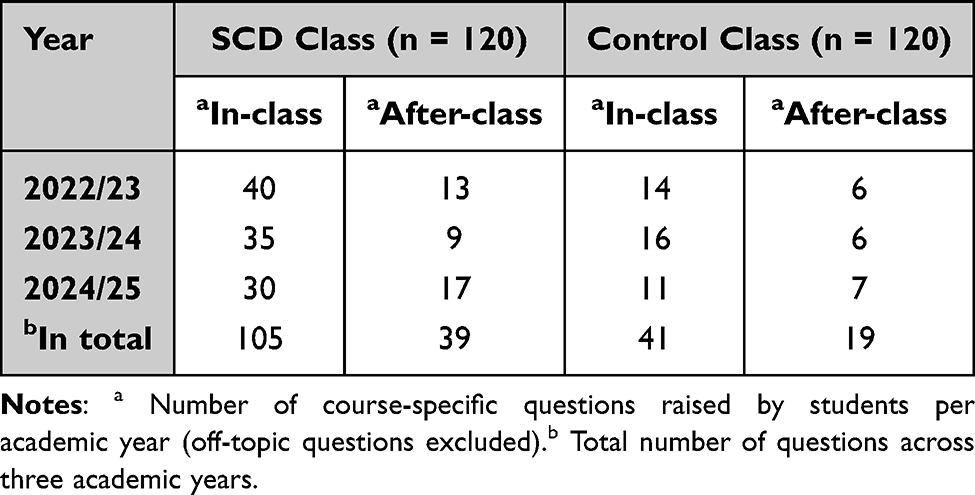 |
Table 4 Track Student Engagement Frequency Both in- and After-Class Sessions |
Discussion
“Clinical case” refers to a real or simulated medical document or scenario description that records the complete process of a patient’s disease onset, development, diagnosis, treatment, and prognosis. It typically includes core information such as the patient’s chief complaint, history of present illness, past medical history, physical examination findings, laboratory data, and imaging findings. Serving as a bridge connecting theory and practice, a vehicle for training clinical reasoning, a driver for stimulating active learning, and a scenario for building communication and collaboration skills, it enables knowledge integration, establishes clinical reasoning, enhances analytical ability, and achieves knowledge synthesis and application.19,20 Case-based learning (CBL) sessions of medical microbiology are designed to establish a student-centered, self-directed learning model that emphasizes the critical correlation between pathogens and clinical manifestations.21,22
However, we found that despite the positive learning outcomes achieved through years of CBL teaching practice, student engagement and initiative have not yet reached the expected goals. In this study, the SCD model was implemented within the teaching practice of medical microbiology. Compared to conventional CBL, significant improvements were observed across multiple dimensions, including student engagement, classroom vitality, positive feedback, academic scores, and sustained enthusiasm for learning. Most encouragingly, the SCD model ensured 100% participation of all students during the sessions, with 96.67% of students confirming in their post-class feedback that the SCD approach provides a viable framework for ensuring the involvement of every participant.
The SCD model adopted in this study represents an enhancement and refinement of conventional CBL. The most significant challenge for the smooth progress of SCD lies in ensuring that students complete the assigned readings, preview, and organization of learning materials prior to class. Previous research has indicated that inadequate student preparation and insufficient guidance can severely compromise classroom learning outcomes.23,24 The SCD model, which unfolds through role-playing and situational immersion, incorporates elements of fun and gamification, thereby incentivizing students to engage more proactively in pre-class preparation. Our findings reveal that 71.67% of students were willing to invest more time and effort into the SCD activities. Furthermore, the allocation of specific roles and tasks to every student served as a catalyst for thorough pre-class engagement. Literature suggests that well-prepared students consistently exhibit superior classroom performance.25,26 In our study, 85.83% of students reported that their interests in learning was ignited, while 80.83% noted a vibrant classroom atmosphere and a compelling instructional process. The effectiveness of such “gamified” pedagogical models in improving learning outcomes has been supported by related studies. For instance, one study evaluated role-playing in a pharmacology curriculum and found that it increased student engagement, promoted rational prescribing, and contributed to safer clinical practices.27 Another study utilized educational games to create a learner-centered environment, providing immersive experiences that stimulated student interest and learning motivation.28
Medicine is a highly practice-oriented profession, and medical education must achieve a profound transformation from “knowledge storage” to “competency generation”. Compared with conventional CBL, the multi-act design of SCD characterized by “suspense”, “paced control”, and “decision-making pressure” facilitates deeper cognitive and emotional engagement, effectively nurturing students’ higher-order thinking skills. During each stage of the discussion, students are required to articulately state: What are the characteristics of the associated pathogen (Etiology)? What is the diagnosis or judgment (Conclusion)? What critical information from the case supports this (Evidence)? And how does this information link to the pathogen to derive the conclusion (Reasoning Chain)? Through such repetitive training, implicit and rapid expert intuition is externalized into a structured thinking process that can be examined, discussed, and optimized. This precisely enhances the core competencies of critical thinking and clinical reasoning, leading to a significant improvement in students’ professional competence and capacity for lifelong learning.29 Our study demonstrates this impact: students in the SCD group raised a total of 144 relevant questions (105 from in-class and 39 from after class), whereas the conventional group raised only 60 (41 from in-class and 19 from after class). The SCD model bolsters independent reflection and extended learning, representing a highly encouraging and beneficial outcome.
By assuming specific roles (doctor or patient), students in the SCD model transition from being “passive observers analyzing a case” to “active stakeholders bearing the consequences of their decisions”. This sense of role immersion naturally triggers emotional investment, analytical reasoning, communicative experience, and the mobilization of knowledge.30 Consequently, clinical problems become vivid and tangible, allowing students to experience the emotional impact of medical scenarios.31 This depth of engagement ensures that the learning of communication skills, empathy, and professional values far exceeds the limitations of theoretical study. A recent study evaluating game-based learning in nursing education concluded that such models primarily facilitate learning outcomes within the cognitive domain.32 SCD truly realizes a student-centered pedagogical model, where the instructor’s role evolves from a “lecturer” into a “screenwriter, director, and facilitator”. Instructors pose catalytic questions at critical junctures (eg., “At this moment, as the doctor, how would you distill critical information from this narrative to make a judgment?”), guiding students toward reflective synthesis. Because student decisions are diverse, the trajectory of a case often extends beyond preset boundaries, making the classroom a space of intellectual generativity and challenge. The instructor guides the session based on students’ real-time responses, transforming teaching into a genuine co-creative process. Finally, SCD provides an objective and equitable window for formative assessment. By observing each student’s discourse, reasoning, and role-playing throughout every act, instructors can clearly evaluate individual strengths and weaknesses in knowledge application, logical thinking, and communicative expression. This provides a direct empirical basis for personalized guidance and feedback.
Although this study achieved student-centered participation with everyone involved, the greatest challenge during implementation was that the class size was relatively large. According to the current medical microbiology teaching schedule and setup at our school, a class of 20 students requires 6 cases to ensure that every student has a role and task, which means that the time allocated to each individual is too short, limiting the depth and breadth of interaction. Our experience suggests that a smaller-class SCD teaching model with 11 students and 3 cases may be a better option. Additionally, the limitations of this study are as follows: ① we only assessed learning outcomes up to the end of the semester; whether students can maintain long-term attention and interest in the course, as well as the sustained retention of knowledge, was not included in the scope of this study’s evaluation. ② throughout the three academic years, only one instructor was involved, and whether instructor bias existed was also not examined.
Conclusion
The SCD pedagogical model is more effective than conventional CBL model, providing a proactive paradigm for advancing student-centered, self-directed medical education. Students provided positive feedback on the SCD approach that effectively addresses the deficiencies in knowledge integration and practical competency commonly encountered during the study of medical microbiology.
Ethical Approval
This study received ethical approval from the Ethics Committee of Wenzhou Medical University (the approval number WMUEC-2022-034). This educational research was conducted under the full supervision of the Teaching Guidance Committee of the School of Basic Medical Sciences, Wenzhou Medical University. The committee reviewed the overall study design, experimental content, and related materials. All research studies on individuals were performed in accordance with the Helsinki Declaration. Written informed consent to participate in this study was provided by the participants.
Funding
This study was supported by Wenzhou Medical University Teaching Innovation Team Project (Wenzhou Medical University Education [2023] No. 59).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ribeiro LMC, de Carvalho Filho MA. From learners to healers: the essential link between student-centred education and patient-centred care. Med Educ. 2026;60:215–11. doi:10.1111/medu.70096
2. Stoddard HA, Lee AC, Gooding HC. Empowerment of learners through curriculum co-creation: practical implications of a radical educational theory. Teach Learn Med. 2025;37:261–267. doi:10.1080/10401334.2024.2313212
3. Singhal A. Case-based learning in microbiology: observations from a north west indian medical college. Int J Appl Basic Med Res. 2017;7(Suppl 1):S47–S51. doi:10.4103/ijabmr.IJABMR_146_17
4. Somaa F. The flipped classroom approach: a review of cognitive styles and academic performances. Cureus. 2024;16:e63729. doi:10.7759/cureus.63729
5. Kaushik JS, Raghuraman K, Verma S, et al. Online interactive flipped classroom teaching in pediatrics for medical undergraduates. Cureus. 2023;15:e37603. doi:10.7759/cureus.37603
6. Najotra DK, Ghai S, Khan I, et al. Learner-centered microbiology teaching via the flipped classroom model: insights from a mixed-methods educational study. Ann Afr Med. 2026. doi:10.4103/aam.aam_597_25
7. Mamakli S, Alimoğlu MK, Daloğlu M. Scenario-based learning: preliminary evaluation of the method in terms of students’ academic achievement, in-class engagement, and learner/teacher satisfaction. Adv Physiol Educ. 2023;47(1):144–157. doi:10.1152/advan.00122.2022
8. Gonella S, Viottini E, Gastmans C, et al. Lived experience of ethical challenges among undergraduate nursing students during their clinical learning. Nurs Ethics. 2025;32(3):814–827. doi:10.1177/09697330241262311
9. Lavanya KM, Somu LK, Mishra SK. Effectiveness of scenario-based role-play as a method of teaching soft skills for undergraduate medical students. Int J Appl Basic Med Res. 2024;14(2):78–84. doi:10.4103/ijabmr.ijabmr_431_23
10. Mianehsaz E, Saber A, Tabatabaee SM, Faghihi A. Teaching medical professionalism with a scenario-based approach using role-playing and reflection: a step towards promoting integration of theory and practice. J Adv Med Educ Prof. 2023;11(1):42–49. doi:10.30476/JAMP.2022.95605.1651
11. Hao M, Kang X, Xiaojing L, Wang L, Chen L. Assessing the impact of standardized-patient scenario-based simulation teaching combined with serialized micro-course instruction in pediatric nursing teaching. J Trop Pediatr. 2025;71(4):fmaf031. doi:10.1093/tropej/fmaf031
12. Lin Y-P, Liu C-H, Chen Y-T, Uen Shuen L. Scenario- and discussion-based approach for teaching preclinical medical students the socio-philosophical aspects of psychiatry. Philos Ethics Humanit Med. 2023;18(1):15. doi:10.1186/s13010-023-00146-4
13. Chen Y, Zhang X, Shi L, et al. Role-playing: an effective method for clinical novitiate teaching of infectious diseases. Med Sci Educ. 2020;31:53–57. doi:10.1007/s40670-020-01031-x
14. Armitage-Chan E, Whiting M. Teaching Professionalism: using role-play simulations to generate professionalism learning outcomes. J Vet Med Educ. 2016;43:359–363. doi:10.3138/jvme.1115-179R
15. Yongqiao L, Junjie Gavin W, Zhang D, et al. The efficacy of virtual reality flipped learning with collaborative role-playing in nursing education. BMC Nurs. 2025;24:1102. doi:10.1186/s12912-025-03709-2
16. Evgeniou E, Loizou P. Simulation-based surgical education. ANZ J Surg. 2013;83(9):619–623. doi:10.1111/j.1445-2197.2012.06315.x
17. Chao C-T, Liang J-C. The development and validation of a multi-dimensional medical students’ learning self-efficacy questionnaire for clinical education. Med Educ Online. 2025;30:2534053. doi:10.1080/10872981.2025.2534053
18. Bigdeli S, Aalaa M, Sandars J. Multi-dimensional model of cooperative learning. J Adv Med Educ Prof. 2024;12(1):66–67. doi:10.30476/JAMP.2023.97756.1778
19. Bintley HL, Bell A, Ashworth R. Remember to breathe: teaching respiratory physiology in a clinical context using simulation. Adv Physiol Educ. 2019;43(1):76–81. doi:10.1152/advan.00148.2018
20. Eseonu O, Carachi R, Brindley N. Case-based anatomy teaching: a viable alternative? Clin Teach. 2013;10(4):236–241. doi:10.1111/tct.12013
21. Weidenbusch M, Lenzer B, Sailer M, et al. Can clinical case discussions foster clinical reasoning skills in undergraduate medical education? A randomised controlled trial. BMJ Open. 2019;9:e025973. doi:10.1136/bmjopen-2018-025973
22. Wang X, Che X, Tang X, et al. Application of combined teaching method of case-based-learning and clinical pathway in practical gynecological teaching. PeerJ. 2024;12:e17813. doi:10.7717/peerj.17813
23. Han S. Flipped classroom: challenges and benefits of using social media in English language teaching and learning. Front Psychol. 2022;13:996294. doi:10.3389/fpsyg.2022.996294
24. Morales MLN, Bello CCL, Pérez-Méndez L. The flipped classroom as a method to improve learning in radiology. Radiologia. 2026;68(1):501728. doi:10.1016/j.rxeng.2025.501728
25. Diel RJ, Yom KH, Ramirez D, et al. Flipped ophthalmology classroom augmented with case-based learning. Digit J Ophthalmol. 2021;27:1–5. doi:10.5693/djo.01.2021.01.004
26. Wang Y, Wen-Jie S, Jia-Cen L, et al. Flipped Classroom Model in the standardized training of anesthesiology residents. Asian J Surg. 2023;46:4899–4900. doi:10.1016/j.asjsur.2023.05.177
27. Tekeş E, Güngör B, Sılan C, et al. Enhancing pharmacology education through role-play: impact on student attitudes. BMC Med Educ. 2025;25:1306. doi:10.1186/s12909-025-07900-6
28. Strickland HP, Kaylor SK. Bringing your a-game: educational gaming for student success. Nurse Educ Today. 2016;40:101–103. doi:10.1016/j.nedt.2016.02.014
29. Dandan M, Ning S, Hou R, et al. Unlocking expertise: the application of threshold concepts in scenario simulations in undergraduate clinical teaching. Front Med. 2025;12:1690297. doi:10.3389/fmed.2025.1690297
30. Jiaqi L, Hou C, Yang D, et al. Enhancing forensic clinical competence through scenario-based simulation: a comparative study of educational outcomes in Chinese medical students. PLoS One. 2025;20(11):e0336273. doi:10.1371/journal.pone.0336273
31. Antikchi M, Heydari S, Bakhshi F. The effect of game-based scenario writing on the clinical reasoning of internship nursing students in cardiovascular emergencies and critical care units. BMC Med Educ. 2025;25(1):597. doi:10.1186/s12909-025-07079-w
32. Ozdemir EK, Dinc L. Game-based learning in undergraduate nursing education: a systematic review of mixed-method studies. Nurse Educ Pract. 2022;62:103375. doi:10.1016/j.nepr.2022.103375
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.