Back to Journals » Vascular Health and Risk Management » Volume 21
Evaluating Rivaroxaban for Thromboprophylaxis in Cancer Patients with Long-Term Venous Access Devices: A Retrospective Cohort Study
Authors Jia B ![]() , Lv H, Gong T, Wang X, Ma Q, Ren Y, Zhang L, Zhong D
, Lv H, Gong T, Wang X, Ma Q, Ren Y, Zhang L, Zhong D
Received 17 July 2025
Accepted for publication 26 October 2025
Published 5 November 2025 Volume 2025:21 Pages 917—925
DOI https://doi.org/10.2147/VHRM.S550388
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Harry Struijker-Boudier
Bin Jia,1,* Hui Lv,2,* Ting Gong,2 Xin Wang,2 Qing Ma,2 Yaoyao Ren,2 Linlin Zhang,2 Diansheng Zhong2
1Department of Lung Cancer, Tianjin Lung Cancer Center, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin’s Clinical Research Center for Cancer, Tianjin, People’s Republic of China; 2Department of Medical Oncology, Tianjin Medical University General Hospital, Heping, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Diansheng Zhong, Tianjin Medical University General Hospital, Department of Medical Oncology, Tianjin, People’s Republic of China, Email [email protected] Linlin Zhang, Tianjin Medical University General Hospital, Department of Medical Oncology, Tianjin, People’s Republic of China, Email [email protected]
Background: Long-term venous access devices, including PICCs and implantable ports, increase the risk of catheter-related thrombosis (CRT) in cancer patients. The role of prophylactic rivaroxaban in this setting remains uncertain.
Methods: We retrospectively analyzed adult cancer patients who underwent peripherally inserted central catheter (PICC) or implantable port (PORT) placement between January 2019 and May 2023. CRT was diagnosed via B-ultrasound. To reduce surveillance bias, only patients who underwent ≥ 4 ultrasound examinations were included. Kaplan–Meier and Cox regression were used to assess the effect of rivaroxaban prophylaxis and to explore subgroup differences.
Results: Among 1,585 patients with upper-limb catheters, 822 met inclusion criteria, with 135 CRT events. The median time to CRT was 55 days (IQR: 29.5– 121.5), and 66.2% occurred within 90 days post-catheterization. Prophylactic rivaroxaban significantly reduced CRT risk (HR = 0.47, 95% CI: 0.33– 0.67; p < 0.001), particularly in high-risk groups such as those with PICC lines or active tumors. No significant benefit was observed in patients with no-evidence-of-disease (NED) or those with cardiac stents, atrial fibrillation, or prior cerebral infarction. In the PORT subgroup, risk reduction was not statistically significant overall (HR = 0.66, p = 0.07), but became significant after excluding NED and cardiovascular conditions (HR = 0.52, p = 0.0195).
Conclusion: Rivaroxaban prophylaxis reduces CRT in cancer patients with long term central venous catheters, particularly those with PICCs or active disease. Routine use appears unnecessary in NED or patients on antiplatelet therapy, highlighting the importance of individualized prophylaxis strategies.
Keywords: anticoagulant, neoplasm, prophylaxis, thrombosis, central venous catheter
Introduction
Long-term venous access is essential in oncology to facilitate chemotherapy and supportive care. According to the latest WoCoVA consensus, the umbrella term central venous catheter (CVC) has been refined into more specific categories, including centrally inserted central catheters (CICCs) and femorally inserted central catheters (FICCs), while peripherally inserted central catheters (PICCs) are classified as medium- to long-term devices. In daily oncology practice, PICCs and totally implantable venous access ports (PORTs) remain the most commonly used long-term venous access devices.
Catheter-related thrombosis (CRT) represents one of the most frequent complications of these devices and is associated with significant morbidity and mortality in cancer patients.1–4 Previous clinical trials and meta-analyses in non-cancer populations have generally not supported routine anticoagulation for CVCs.5 International Society of Thrombosis and Haemostasis (ISTH) consensus based on six randomized trials concluded that LMWH may reduce asymptomatic CRT but does not significantly prevent symptomatic events, nor increase major bleeding risk. Thus, current recommendations favor individualized over universal prophylaxis.6
Meanwhile, guidelines from ASCO and the International Initiative on Thrombosis and Cancer (ITAC) suggest that thromboprophylaxis with low-molecular-weight heparin (LMWH) or direct oral anticoagulants (DOACs), including rivaroxaban, may be considered in high-risk cancer patients.7–9 Rivaroxaban has shown potential in various cancer-associated thrombosis settings, but its preventive role remains uncertain, with outcomes differing by cancer type, risk factors, and treatment context.10–12
This study aimed to evaluate the efficacy of rivaroxaban for thromboprophylaxis in cancer patients with long-term venous access devices (PICCs and PORTs). We further explored which patient subgroups—defined by tumor burden (active disease vs NED) and catheter type (PICC vs PORT)— may benefit most from individualized prophylactic strategies.
Methods
This was a retrospective cohort study conducted in the oncology department of our hospital. We included consecutive adult patients who underwent PICC placement or infusion port implantation between January 1st 2019 and May 31st 2023. Demographic and clinical data were collected from electronic medical records. CRT was defined as thrombosis in the ipsilateral upper limb vein, confirmed by B-ultrasound. For patients with multiple catheterizations, only the first was included, except in subgroup analyses comparing PICC vs PORT and NED vs active malignancy.
PICC placement was performed by trained nurses under ultrasound guidance, puncturing the basilic vein with the modified Seldinger technique. Ports were inserted by physicians under ultrasound guidance via the axillary vein, also using the modified Seldinger technique, with the port chamber positioned in a subcutaneous pocket between the clavicle and ribs. During catheter insertion, intracavitary electrocardiogram (IC-ECG) guidance was used to adjust the catheter tip position at the cavoatrial junction, and post-procedural chest X-ray was performed to confirm the final location. All procedures were conducted under strict aseptic conditions. B-ultrasound was routinely performed prior to each chemotherapy cycle (every 20–30 days, depending on treatment schedule). Patients diagnosed with thrombosis were all included. To reduce follow-up bias, those without thrombosis and with ≤3 B-ultrasound exams were excluded from the analysis. Since August 2020, physicians began routinely recommending rivaroxaban 10 mg daily for 3 months as prophylactic anticoagulation. In practice, outpatient use varied; patients with documented use for >1 month were classified into the prophylaxis group.
Kaplan–Meier and Log rank tests were used to compare CRT-free survival between groups. Subgroup analyses were performed using Cox regression models. All statistical analyses were conducted using R software (version [4.3]) with the survival and survminer packages.
Results
3,124 cancer patients undergoing ≥1 ultrasound screening. Thrombosis was diagnosed in 468 patients (14.97%), with 162 cases involving upper extremities. Among 1,585 patients with long term CVC, 135 developed CRT (8.58%) -including 49 of 287 with PICCs (17.1%) and 86 of 1,298 with PORTs (6.6%) -whereas only 27 cases (1.75%) occurred among the 1541 patients without catherterization. The chi-square test showed that the incidence of upper-extremity thrombosis was significantly higher in the CVC group compared to the non-CVC group (χ2 = 71.01, p < 0.001). To minimize surveillance bias, only patients with ≥4 ultrasounds (intervals >20 days) were considered (n=832); after excluding 10 patients who were already receiving therapeutic-dose rivaroxaban (20 mg once daily) for pre-existing thrombosis, a total of 822 patients were included in the final analysis (Figure 1).
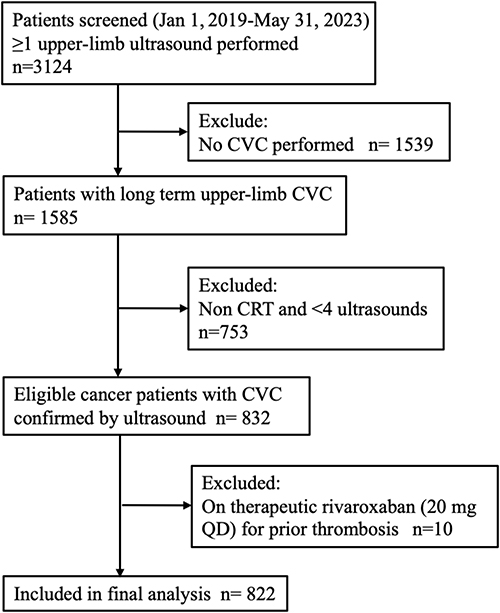 |
Figure 1 Selection Flowchart of Cancer Patients with Long-Term Central Venous Access Devices (PICC and PORT). |
Of these 135 CRT patients, the median time to CRTwas 55 days (IQR: 29.5–121.5 days), with 90 patients (66.2%) experiencing thrombosis within 90 days post-catheterization (Figure 2). The median following up days were 293 days (95% CI:274–312).
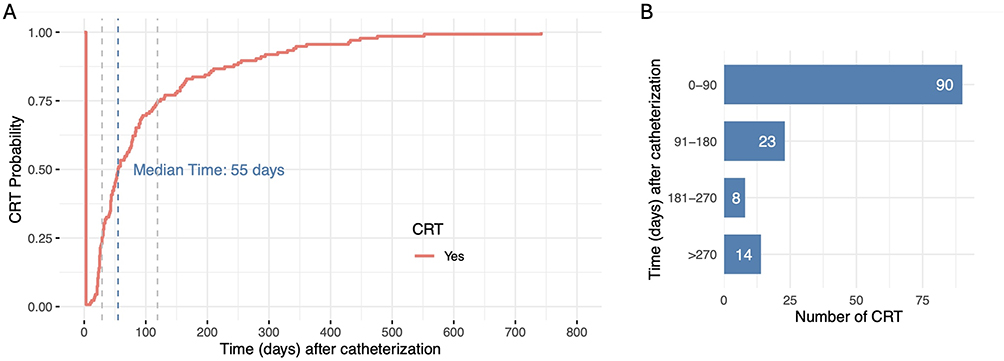 |
Figure 2 Time-to-CRT Distribution of After Catheterization. (A) Kaplan–Meier curve showing the cumulative probability of CRT over time following catheterization. (B) Number of CRT events by time intervals; most occurred within 90 days. |
Among the included patients, 582 received prophylactic rivaroxaban, while 240 did not receive any anticoagulation therapy. In the primary analysis, prophylactic use of rivaroxaban significantly reduced the risk of CRT across the entire cohort compared to non-use (HR = 0.47, 95% CI: 0.33–0.67; p < 0.001), as shown in the Kaplan-Meier survival curves (Figure 3).
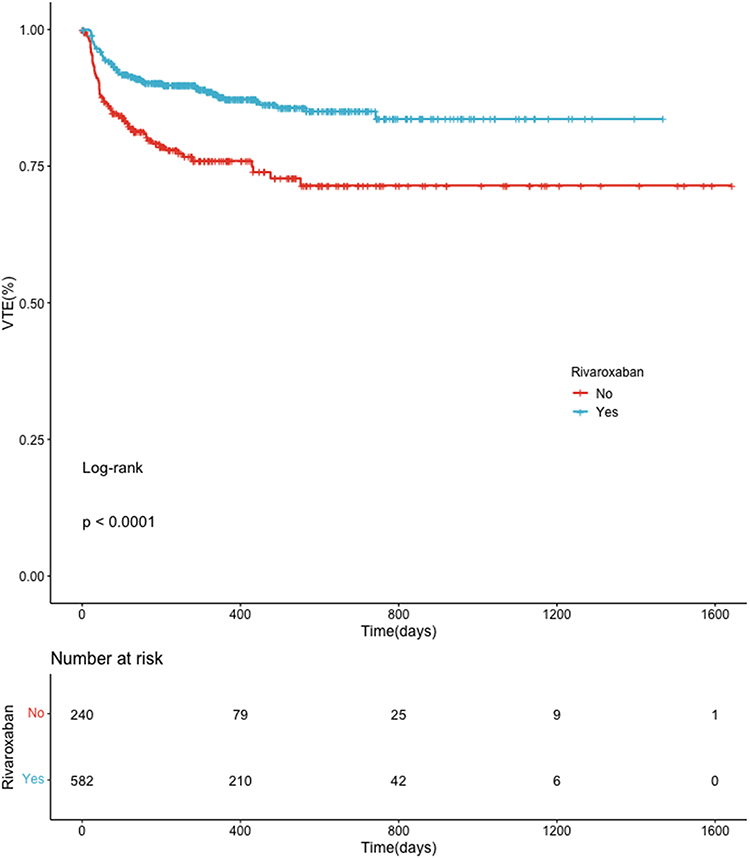 |
Figure 3 Rivaroxaban Prophylaxis Significantly Reduces CRT Risk in Cancer Patients With Long-Term Central Venous Access Devices (PICC and PORT). Kaplan–Meier curves showing the cumulative incidence of CRT, stratified by prophylactic use of rivaroxaban. Patients receiving rivaroxaban showed significantly lower CRT incidence (log-rank p < 0.0001). Number of patients at risk are shown below. |
Subgroup analyses further elucidated the impact of rivaroxaban across various patient characteristics, showing that the drug provided significant prophylactic benefits in most groups (Table 1), such as the PICC group (HR = 0.49, 95% CI: 0.26–0.91; p=0.024).
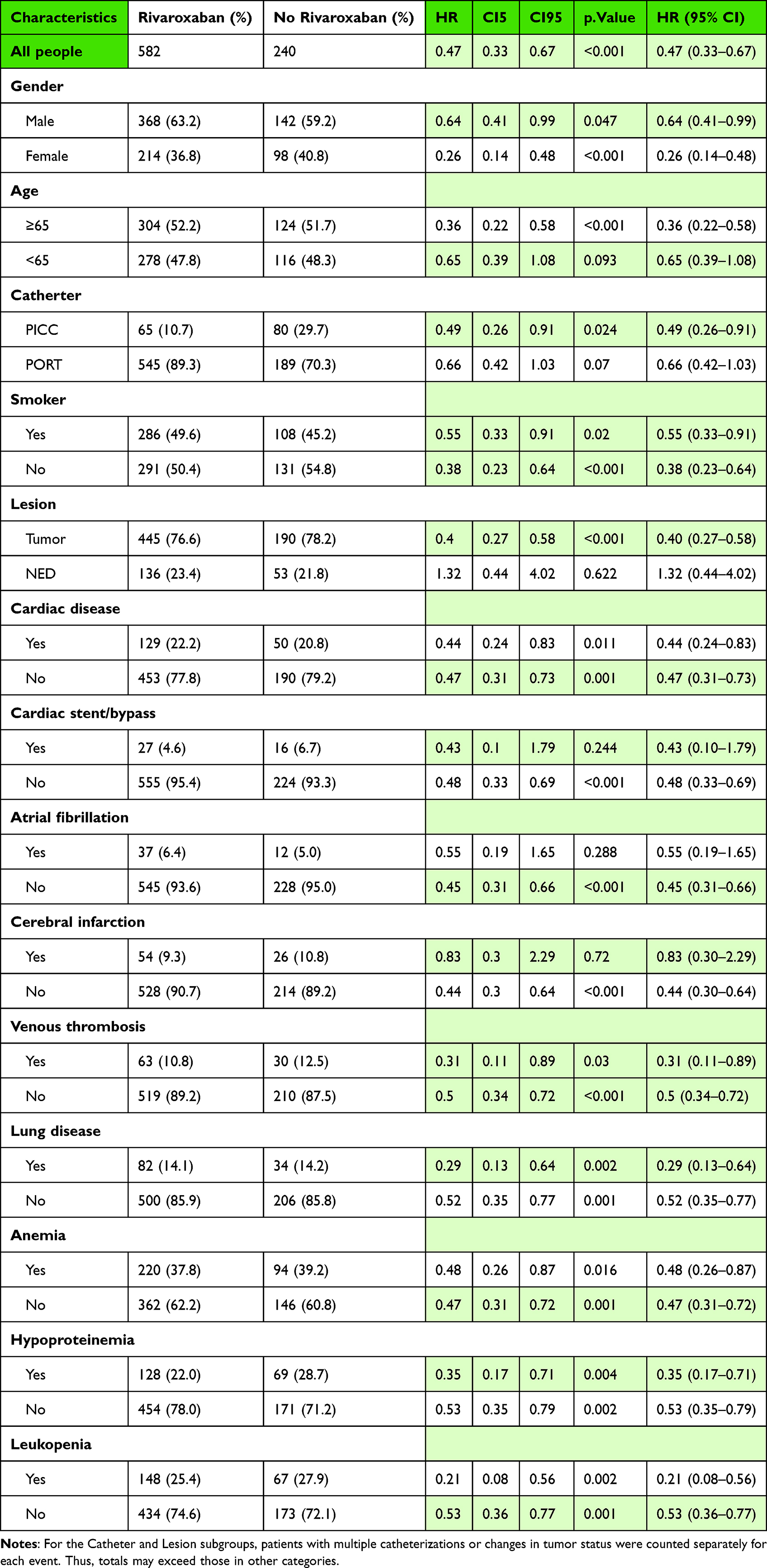 |
Table 1 Subgroup Analysis of the Effect of Rivaroxaban Prophylaxis on CRT in Cancer Patients With Long-Term Central Venous Access Devices (PICC and PORT) |
However, there were a few notable exceptions where rivaroxaban did not significantly reduce the risk of CRT. In the NED group, where patients had no active cancer, rivaroxaban did not provide a significant reduction in CRT risk (HR = 1.32, 95% CI: 0.44–4.02; p = 0.622). Additionally, patients with cardiac stent/bypass (HR = 0.43, 95% CI: 0.10–1.79; p = 0.244), atrial fibrillation (HR = 0.45, 95% CI: 0.31–0.66; p < 0.001), and cerebral infarction (HR = 0.44, 95% CI: 0.30–0.64; p < 0.001) did not show significant reductions in CRT risk, potentially due to the confounding effect of other anticoagulants or antiplatelet therapies commonly used in these patients, such as aspirin or clopidogrel.
Although PORT patients did not show a statistically significant reduction in the risk of CRT with rivaroxaban (HR = 0.66, 95% CI: 0.42–1.03; p = 0.07), a trend in favor of rivaroxaban use was observed. To further refine our analysis and minimize potential confounding factors, we focused on a subset of the PORT group that had a tumor burden and no other anticoagulant therapies, by excluding patients with NED, cardiac stents, atrial fibrillation, and cerebral infarction, as these conditions often involve concurrent anticoagulant or antiplatelet therapy (Figure 4). The results of this analysis revealed that rivaroxaban did demonstrate significant prophylactic efficacy in this adjusted cohort (HR = 0.52, 95% CI: 0.31–0.90; p = 0.0195).
 |
Figure 4 Effect of Rivaroxaban Prophylaxis in PORT Patients Before and After Risk-Based Subgroup Refinement. (A) Kaplan–Meier analysis of CRT–free survival in cancer patients with PORT. No statistically significant difference between rivaroxaban and non-rivaroxaban groups (cox model p = 0.07). (B) After excluding low-risk individuals, rivaroxaban was associated with improved CRT-free survival (p = 0.0195). |
Discussion
The need for prophylactic anticoagulation in cancer patients with peripherally inserted central catheters (PICC) or implantable ports (PORT) remains controversial. Current international guidelines, including those from the ISTH, do not recommend routine pharmacologic prophylaxis or screening for CRT, primarily due to the low incidence of symptomatic events and lack of clear benefit in unselected populations.6 Meta-analyses of LMWH trials suggest limited efficacy in preventing symptomatic CRT despite reducing asymptomatic events, and without increasing major bleeding risk. A Cochrane review13 of 12 studies including 3611 cancer patients found no statistically significant reduction in either symptomatic or asymptomatic CRT from prophylactic unfractionated heparin or LMWH, nor did vitamin K antagonists demonstrate a clear advantage.
Nevertheless, patients with cancer represent a distinctly prothrombotic population. Central venous catheterization, a common intervention for chemotherapy, adds an additional risk factor. Some guidelines (ASCO, ITAC) now suggest that prophylaxis with LMWH or DOACs like rivaroxaban may be considered in high-risk patients. Indeed, out of seven investigations evaluating anticoagulation’s role in reducing CRT risk, one retrospective case-control study reported a positive association.5 There remain no large randomized controlled trials specifically assessing novel oral anticoagulants (eg, dabigatran, rivaroxaban, or apixaban) for primary thromboprophylaxis in patients with indwelling central venous catheters.
Our real-world study focused on cancer patients with PICC or PORT placement and found that rivaroxaban prophylaxis significantly reduced the risk of CRT. The benefit was most pronounced in patients with PICC and active malignancy, whereas those with no evidence of disease (NED) or on concurrent antiplatelet therapy derived little to no benefit. These findings support a risk-adapted approach rather than universal prophylaxis.
Notably, the overall CRT rate in our cohort was 8.52% (17.1% in PICC cases; 6.6% in PORT cases), consistent with published rates ranging from 0.3% to 28.3%.2,14–17 Subgroup analysis showed that in NED patients, rivaroxaban conferred no protective effect, likely due to a diminished hypercoagulable state. Conversely, in patients with active disease, the prothrombotic burden- driven by tumor-derived tissue factor, cancer procoagulant, and altered fibrinolytic balance- may justify prophylaxis. Although tumor burden was not quantitatively assessed, existing tools like the Khorana score18 or the Vienna CATS score19 may assist in future risk stratification.
Our study also found that patients with cardiovascular comorbidities (eg, coronary artery stents, atrial fibrillation, or stroke) did not benefit from rivaroxaban, probably due to concomitant antiplatelet use, such as aspirin and/or clopidogrel.20,21 These observations are aligned with the cohort data showing that ongoing antiplatelet therapy is protective against CRT,22 and highlight the importance of considering background antithrombotic regimens when prescribing additional anticoagulation.
Interestingly, the median time to CRT was 55 days, with over two-thirds of events occurring within 90 days post-catheterization, consisted with the randomized clinical trial by Young et al.23 This supports a 3-month prophylaxis window, which may offer optimal protection during the high-risk period. While PORT patients did not reach statistical significance overall, exclusion of low-risk individuals revealed a protective effect, suggesting that selection criteria strongly influence outcomes. Prior studies have similarly noted lower CRT incidence in PORT vs PICC users,24–26 likely due to anatomical and mechanical differences in catheter design and placement. PICC lines, which are inserted through peripheral veins and extended into the central veins, tend to have longer catheter lengths and require smaller diameter of arm veins, which may cause greater irritation to the blood vessel endothelium.25,27,28
Our study has limitations. It was retrospective, with potential confounding and incomplete documentation of bleeding outcomes due to outpatient rivaroxaban use. Also, it was conducted at a single center, limiting generalizability. Although detailed data on adverse events such as bleeding were not systematically recorded, rivaroxaban is a well-established anticoagulant with a safety profile that has been thoroughly evaluated in multiple large-scale clinical trials and real-world studies, providing a valuable reference for clinical practice.29–32
Conclusion
In summary, our findings suggest that tailored rivaroxaban prophylaxis may be effective in select high-risk cancer patients with long-term central venous access devices, particularly those with PICCs or active malignancy. In contrast, no significant benefit was observed in patients with NED or those with major cardiovascular or cerebrovascular comorbidities already requiring long-term antiplatelet therapy. Further prospective, multicenter trials are warranted to confirm these observations and to define the optimal patient population for prophylactic anticoagulation.
Ethical Approval Statement
This study was approved by Ethical Committee of Tianjin Medical University General Hospital (approval number: IRB2025-YX-001-01), and was conducted in accordance with the ethical principles of the Declaration of Helsinki. Due to the retrospective nature of the study and the use of anonymized patient data, the requirement for informed consent was waived by the ethics committee.
Acknowledgments
We thank the members of Intravenous Therapy Team in Tianjin Medical University General Hospital.
Author Contributions
Bin Jia and Hui Lv contributed equally to this work and share first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Tianjin Municipal Education Commission (2020KJ156).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kearon C, Kahn SR. Long-term treatment of venous thromboembolism. Blood. 2020;135(5):317–325. doi:10.1182/blood.2019002364
2. Verso M, Agnelli G. Venous thromboembolism associated with long-term use of central venous catheters in cancer patients. J Clin Oncol. 2003;21(19):3665–3675. doi:10.1200/JCO.2003.08.008
3. Liu F, Zhang Q, Rao L, Song J. Relationship between ABO blood group and risk of venous thrombosis in cancer patients with peripherally inserted central catheters: a protocol for systematic review and meta-analysis. Medicine. 2020;99(45):e23091. doi:10.1097/MD.0000000000023091
4. Huang X, Xie M, Zhao S, Chen Y, Wu L, Zeng X. Benefits of an online multimodal nursing program among patients with peripherally inserted central catheter-related thrombosis. Front Public Health. 2022;10:971363. doi:10.3389/fpubh.2022.971363
5. Leung A, Heal C, Perera M, Pretorius C. A systematic review of patient-related risk factors for catheter-related thrombosis. J Thromb Thrombolysis. 2015;40(3):363–373. doi:10.1007/s11239-015-1175-9
6. Debourdeau P, Farge D, Beckers M, et al. International clinical practice guidelines for the treatment and prophylaxis of thrombosis associated with central venous catheters in patients with cancer. J Thromb Haemost. 2013;11(1):71–80. doi:10.1111/jth.12071
7. Key NS, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2020;38(5):496–520. doi:10.1200/JCO.19.01461
8. Farge D, Frere C, Connors JM, et al. 2022 International clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer, including patients with COVID-19. Lancet Oncol. 2022;23(7):e334–e347. doi:10.1016/S1470-2045(22)00160-7
9. Falanga A, Ay C, Di Nisio M, et al. Venous thromboembolism in cancer patients: ESMO clinical practice guideline. Ann Oncol. 2023;34(5):452–467. doi:10.1016/j.annonc.2022.12.014
10. Xing J, Yin X, Chen D. Rivaroxaban versus enoxaparin for the prevention of recurrent venous thromboembolism in patients with cancer: a meta-analysis. Medicine. 2018;97(31):e11384. doi:10.1097/md.0000000000011384
11. Rosencher N, Albaladejo P. A new approach with anticoagulant development: tailoring anticoagulant therapy with dabigatran etexilate according to patient risk. Expert Opin Pharmacother. 2012;13(2):217–226. doi:10.1517/14656566.2012.648614
12. Becattini C, Pace U, Pirozzi F, et al. Rivaroxaban vs placebo for extended antithrombotic prophylaxis after laparoscopic surgery for colorectal cancer. Blood. 2022;140(8):900–908. doi:10.1182/blood.2022015796
13. Akl EA, Vasireddi SR, Gunukula S, et al. Anticoagulation for patients with cancer and central venous catheters. Cochrane Database Syst Rev. 2011;(2):CD006468. doi:10.1002/14651858.CD006468.pub3
14. Gaddh M, Antun A, Yamada K, et al. Venous access catheter-related thrombosis in patients with cancer. Leuk Lymphoma. 2014;55(3):501–508. doi:10.3109/10428194.2013.813503
15. Wu S, Huang J, Jiang Z, et al. Internal jugular vein versus subclavian vein as the percutaneous insertion site for totally implantable venous access devices: a meta-analysis of comparative studies. BMC Cancer. 2016;16(1):747. doi:10.1186/s12885-016-2791-2
16. Kansu E. Thrombosis in stem cell transplantation. Hematology. 2012;17 Suppl 1:S159-62. doi:10.1179/102453312x13336169156735
17. Drugeon B, Guenezan J, Pichon M, et al. Incidence, complications, and costs of peripheral venous catheter-related bacteraemia: a retrospective, single-centre study. J Hosp Infect. 2023;135:67–73. doi:10.1016/j.jhin.2023.02.012
18. Huang X, Chen H, Meng S, et al. External validation of the khorana score for the prediction of venous thromboembolism in cancer patients: a systematic review and meta-analysis. Int J Nurs Stud. 2024;159:104867. doi:10.1016/j.ijnurstu.2024.104867
19. Verzeroli C, Giaccherini C, Russo L, et al. Utility of the khorana and the new-vienna CATS prediction scores in cancer patients of the HYPERCAN cohort. J Thromb Haemost. 2023;21(7):1869–1881. doi:10.1016/j.jtha.2023.03.037
20. Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation. 2024;149(1):e1–e156. doi:10.1161/CIR.0000000000001193
21. Valgimigli M, Landi A, Angiolillo DJ, et al. Demystifying the Contemporary role of 12-month dual antiplatelet therapy after acute coronary syndrome. Circulation. 2024;150(4):317–335. doi:10.1161/CIRCULATIONAHA.124.069012
22. BLOOD-Cancer-associated.
23. Young AM, Billingham LJ, Begum G, et al. Warfarin thromboprophylaxis in cancer patients with central venous catheters (WARP): an open-label randomised trial. Lancet. 2009;373(9663):567–574. doi:10.1016/S0140-6736(09)60205-1
24. Wang P, Soh KL, Ying Y, Liu Y, Huang X, Huang J. Risk of VTE associated with PORTs and PICCs in cancer patients: a systematic review and meta-analysis. Thromb Res. 2022;213:34–42. doi:10.1016/j.thromres.2022.02.024
25. Taxbro K, Hammarskjold F, Thelin B, et al. Clinical impact of peripherally inserted central catheters vs implanted port catheters in patients with cancer: an open-label, randomised, two-centre trial. Br J Anaesth. 2019;122(6):734–741. doi:10.1016/j.bja.2019.01.038
26. Moss JG, Wu O, Bodenham AR, et al. Central venous access devices for the delivery of systemic anticancer therapy (CAVA): a randomised controlled trial. Lancet. 2021;398(10298):403–415. doi:10.1016/S0140-6736(21)00766-2
27. Forauer AR, Theoharis CG, Dasika NL. Jugular vein catheter placement: histologic features and development of catheter-related (fibrin) sheaths in a swine model. Radiology. 2006;240(2):427–434. doi:10.1148/radiol.2402031129
28. Wang G, Li Y, Wu C, et al. The clinical features and related factors of PICC-related upper extremity asymptomatic venous thrombosis in cancer patients: a prospective study. Medicine. 2020;99(12):e19409. doi:10.1097/MD.0000000000019409
29. Hill NR, Sandler B, Bergrath E, et al. A systematic review of network meta-analyses and real-world evidence comparing apixaban and rivaroxaban in nonvalvular atrial fibrillation. Clin Appl Thromb Hemost. 2020;26:1076029619898764. doi:10.1177/1076029619898764
30. Yang Z, Wang J, Yuan Y, et al. Application of rivaroxaban in patients with non-valvular atrial fibrillation and end-stage kidney disease: a systematic review and meta-analysis. Front Cardiovasc Med. 2023;10:1021959. doi:10.3389/fcvm.2023.1021959
31. Ageno W, Lopes RD, Goldin M, et al. Rivaroxaban for extended thromboprophylaxis in acutely ill medical patients 75 years of age or older. J Thromb Haemost. 2021;19(11):2772–2780. doi:10.1111/jth.15477
32. Maura G, Blotière PO, Bouillon K, et al. Comparison of the short-term risk of bleeding and arterial thromboembolic events in nonvalvular atrial fibrillation patients newly treated with dabigatran or rivaroxaban versus vitamin K antagonists: a French nationwide propensity-matched cohort study. Circulation. 2015;132(13):1252–1260. doi:10.1161/circulationaha.115.015710
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Multicenter Study Assessing the Optimal Anticoagulation Strategies in COVID-19 Critically Ill Patients with New-Onset Atrial Fibrillation: Balancing Effectiveness and Safety
Al Sulaiman K, Aljuhani O, Korayem GB, Altebainawi AF, Alharbi A, Alalawi M, Joharji H, Almohsen RA, Faden RM, Alotaibi N, Alshalawi BS, Alkhushaym N, Alanazi FF, Alharbi A, Alqarni A, Samkari S, Alharbi B, Alshehab N, Alshehri RA, Vishwakarma R
International Journal of General Medicine 2024, 17:5611-5622
Published Date: 28 November 2024