Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 14
Evaluating Gender Differences in Egyptian Fibromyalgia Patients Using the 1990, 2011, and 2016 ACR Criteria
Authors Moshrif A ![]() , Shoaeir MZ, Abbas AS, Abdel-Aziz TM
, Shoaeir MZ, Abbas AS, Abdel-Aziz TM ![]() , Gouda W
, Gouda W ![]()
Received 13 January 2022
Accepted for publication 30 March 2022
Published 23 April 2022 Volume 2022:14 Pages 67—74
DOI https://doi.org/10.2147/OARRR.S358255
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Abdelhfeez Moshrif, Mohamed Z Shoaeir, Awad Saad Abbas, Tarek M Abdel-Aziz, Wesam Gouda
Rheumatology Department, Faculty of Medicine, Al Azhar University, Assiut, Egypt
Correspondence: Abdelhfeez Moshrif, Rheumatology Department, Faculty of Medicine, Al Azhar University, Assiut, 71524, Egypt, Tel +201062930120, Email [email protected]
Background: Fibromyalgia (FM) is a common rheumatic illness distinguished by chronic pain, fatigue, cognitive problems, and functional disability. However, the differences between men and women have not yet been comprehensively studied, especially after the development of the last 2016 American College of Rheumatology (ACR) criteria. The aim of this study was to evaluate the gender differences in symptom characteristics, cognitive dysfunction, and disease severity in Egyptian FM patients considering both the ACR 1990, 2011, and the last 2016 ACR diagnostic criteria.
Methods: This is a prospective cross-sectional study that was carried out on 352 patients with FM in the Rheumatology Department, Al-Azhar University Hospital in Egypt, in the period between January 1, 2020, and June 1, 2021. In addition to the number of tender points (TPC), data was collected on age, gender, body mass index (BMI), marital status, disease onset, duration, and diagnostic delay. The widespread pain index (WPI), the symptom severity scale (SSS), fatigue, cognitive dysfunction, sleep disturbance, awakening unrefreshed, headache, abdominal pain, and depression were evaluated and scored according to 2010 and 2016 ACR criteria. A visual analog scale (VAS) for pain, fatigue, stiffness, anxiety, and depression is included in the questionnaire. The total score ranges were produced using total score ranges ranging from 0 to 80 (excluding job items), with higher scores indicating a stronger negative effect and/or intensity of symptoms. The polysymptomatic distress scale (PDS) has been calculated by the summation of the SSS with the WPI. The Revised FM impact questionnaire (FIQR) has also been evaluated.
Results: The study shows that females have a significantly higher prevalence of fatigue, cognitive dysfunction, sleep disturbance, headache, and abdominal pain (p < 0.05). Also, females showed significantly higher scores than males regarding WPI, SSS, and mean TPC (p = 0.004, 0.027, and 0.001, respectively). While there was no difference regarding the FIQR (p=0.93), PDS was significantly higher in women (p= 0.001).
Conclusion: Female patients with FM had greater disease severity scores, symptomatology, and number of tender points. Whatever the criteria applied, the prevalence and intensity of the disease features are higher in females, which may underestimate the disease in male patients.
Keywords: fibromyalgia, gender differences, chronic pain, diagnostic criteria
Introduction
Fibromyalgia (FM) is a rheumatic illness that is characterized by chronic pain in many sites, fatigue, cognitive problems, sleep disturbances, and functional disability.1
The global FM incidence ranges from 0.2% to 8%.2 During the last decade, the number of cases diagnosed with FM has risen.2,3 Although the etiology of FM is unknown, research shows that central nervous system neurochemical imbalances may intensify or enhance pain perception.4
There is a controversial and unclear relationship between FM and sex. FM has traditionally been thought to be a female-predominant disorder. The consensus is that at least 90% of FM diagnoses are present in females.5,6 However, two major epidemiological studies show that 60.8% of people with FM are females.7,8
Several diagnostic criteria have been evolved throughout time. The American College of Rheumatology (ACR) published the first-time FM criteria in 1990.9 These classification criteria, which have been commonly used in clinical practice, require a history of widespread pain for at least 3 months and tenderness on digital palpation in at least 11 of 18 defined tender points.9 The ACR published another version of the diagnostic criteria in 2010 that removed the tender point examination requirement. It was solely based on the usage of two scales: the Widespread Pain Index (WPI) and the symptom severity scale (SSS). The presence of symptoms for at least three months is required.10 This criteria set has been later validated in the French and Spanish populations.11,12
The 2010 ACR diagnostic criteria were updated and adjusted for use in research by Wolfe et al in 2011.13 The 2011 criteria were only slightly different from the 2010 criteria. The FM symptom scale has been renamed the polysymptomatic distress scale (PDS).
The FM diagnostic criteria were updated in 2016.14 The earlier requirement that the patient have no other ailments that may explain the discomfort was eliminated. These criteria were reviewed to ensure that they could be utilized not only as diagnostic criteria in clinical practice but also as classification criteria in research.14 The criteria added the “generalized pain” criterion to overcome the inclusion of regional pain syndrome as a limitation of the previous one.14,15
Notably, the sex ratio varies greatly depending on the criterion used. When the 2010 ACR criteria are utilized, a larger proportion of men are diagnosed with FM.16
So far, little research has looked at gender differences in the FM patient group, and the results have been contentious and inconclusive, with female patients showing more tender points and more pain intensity than males in most studies.17–19
With the elimination of the tender points from the recent criteria, gender differences in prevalence tend to be far smaller than previously reported.20,21
However, the impact of gender on the construct of the old and new criteria has not yet been systematically evaluated. We thought that addressing this point may enhance the early diagnosis of FM, especially in men, which leads to proper management and decreases the health care utilization and cost previously reported in the disease management.22,23 Furthermore, gender differences would affect different gender-targeted treatment and follow-up strategies.
In this cross-sectional prospective analysis, we aimed to evaluate the gender differences in symptom characteristics, cognitive dysfunction, and disease severity in Egyptian FM patients considering both ACR 1990, 2011 and the last 2016 ACR diagnostic criteria.
Materials and Methods
Study Design and Patients
This is a prospective cross-sectional study that was carried out on 352 patients with FM in the Rheumatology Department, Al-Azhar University Hospital in Egypt, in the period between January 1, 2020, and June 1, 2021.
Inclusion Criteria
Patients were included if they had been diagnosed with FM by rheumatologists as fulfilling all the ACR criteria (1990, 2011 and 2016) were included.9,13,14
Exclusion Criteria
Patients under the age of 18 and beyond the age of 70 were excluded from the research, as were those with any inflammatory rheumatic diseases (eg, rheumatoid arthritis or psoriatic arthritis), active malignancy, fractures, or other non-rheumatic sources of pain. Patients who refused to participate in the study.
Ethical Considerations
The study was approved by the ethical committee of Al Azhar University School of Medicine (Az 062-11-012, December 2019). All participants were informed about the study procedures and signed an informed consent form. The study was carried out in compliance with the competent committee on human experimentation’s ethical criteria, as well as the Helsinki Declaration of 1975, as updated in 1983. No financial support was received for this study.
Demographics, Clinical Characteristics, and Clinical Outcomes
Data collected included: age, gender, body mass index (BMI), marital status, disease onset, duration, and diagnostic delay, which has been defined as the time period from the start of symptoms until the diagnosis of FM by a rheumatologist. All patients were assessed using the 1990,19 2011 modification13 of 2010 criteria,10 and 201614 ACR criteria. In addition to the number of tender points (TPC), WPI, SSS, fatigue, cognitive dysfunction, sleep disturbance, awakening unrefreshed, headache, abdominal pain, and depression were evaluated and scored according to the above-mentioned criteria as follows:
-1990 ACR criteria require a history of generalized pain for at least 3 months and tenderness on digital palpation of at least 11 out of 18 specified tender points.9
–2011 ACR modification of the 2010 criteria: “A patient satisfies modified ACR 2010 FM diagnostic criteria if the following 3 conditions are met: (1) WPI ≥ 7 and SSS ≥ 5 or WPI between 3–6 and SSS > 9. (2) Symptoms have been present at a similar level for at least 3 months. (3) The patient does not have a disorder that would otherwise sufficiently explain the pain.13
WPI (0–19): The widespread pain index is a count of 19 painful locations from the Regional Pain Scale (RPS), a self-reported list of painful sites.
SSS (0–12): The symptom severity scale is the total of the severity grades (0–9) of three symptoms (fatigue, waking unrefreshed, and cognitive symptoms) plus the sum (0–3) of the number of the following symptoms experienced by the patient in the preceding six months:
(1) Headaches (0–1), (2) Lower abdominal pain or cramps (0–1), and (3) depression (0–1).- PDS has been evaluated as a measure of disease severity. It is calculated by adding the WPI and SSS (0–31).24–2016 ACR criteria: A patient is diagnosed with FM (satisfies modified 2016 FM criteria) if all three of the following characteristics are met: (1) WPI ≥ 7 and SSS score ≥ 5 OR WPI of 4–6 and SSS score ≥ 9. (2) There must be generalized pain, defined as pain in at least four of the five areas. The generalized pain definition excludes jaw, chest, and abdominal discomfort. Symptoms have typically been present for at least three months.14
The revised FM impact questionnaire (FIQR) was evaluated using a previously validated Arabic version.25
The questionnaire includes a visual analog scale (VAS) for pain, fatigue, stiffness, anxiety, depression, physical function, and well-being. Total score ranges were calculated with total score ranges between 0 and 80 (without job items), where high scores indicated a higher negative impact and/or a greater severity of symptoms.26
Statistical Analysis
The collected data was reviewed, coded, and tabulated using the Statistical Package for Social Science (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.). The mean and standard deviation (mean ± SD) were used to describe the parametric numerical data. The frequency and percentage were used to describe the non-numerical data. An independent sample t-test was used to detect significant differences between men and women for continuous variables and a chi-square test or Fisher’s exact test was used to determine gender-related differences for qualitative variables. P<0.05 was considered statistically significant.
Results
This study included 352 FM patients; most patients were females, 281 (79.8%), while males were 71 (20.2%), and the female/male ratio was 3.96:1. There was a statistically significant difference between females and males regarding age, marital status, and BMI (Table 1).
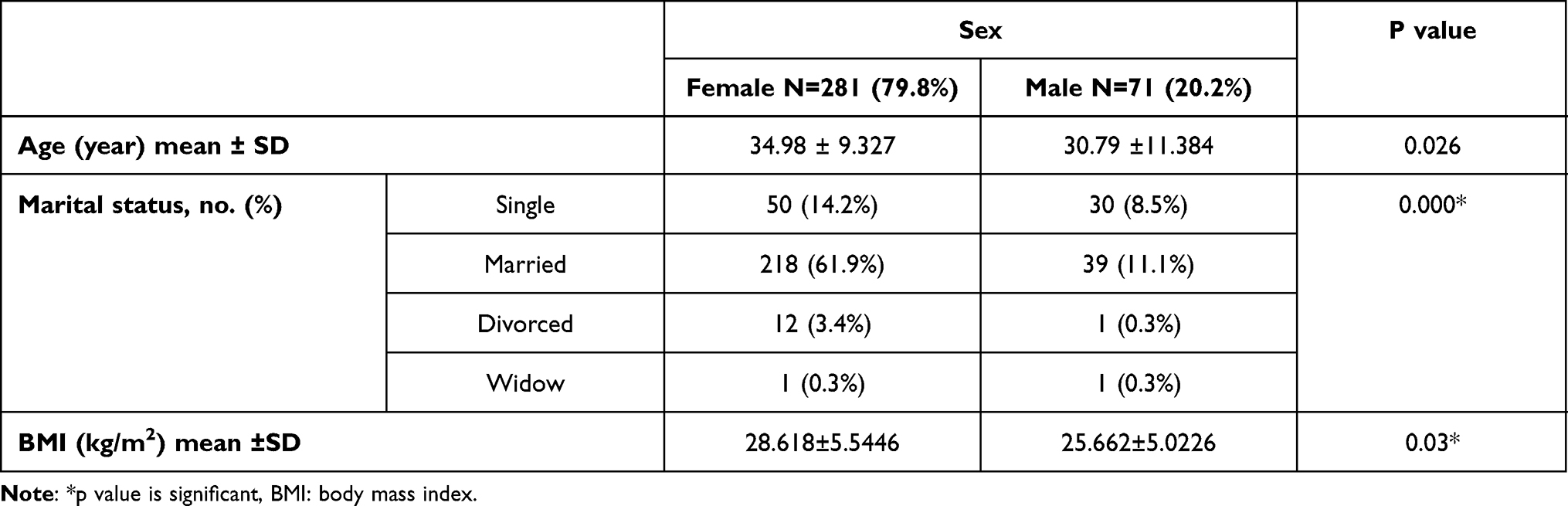 |
Table 1 Demographic Features of FM Patients According to Gender |
Females had a significantly higher incidence of fatigue, cognitive dysfunction, sleep disturbance, headache, and abdominal pain (p < 0.05) while there was no significant difference between females and males considering awakened unrefreshed and depression (Table 2).
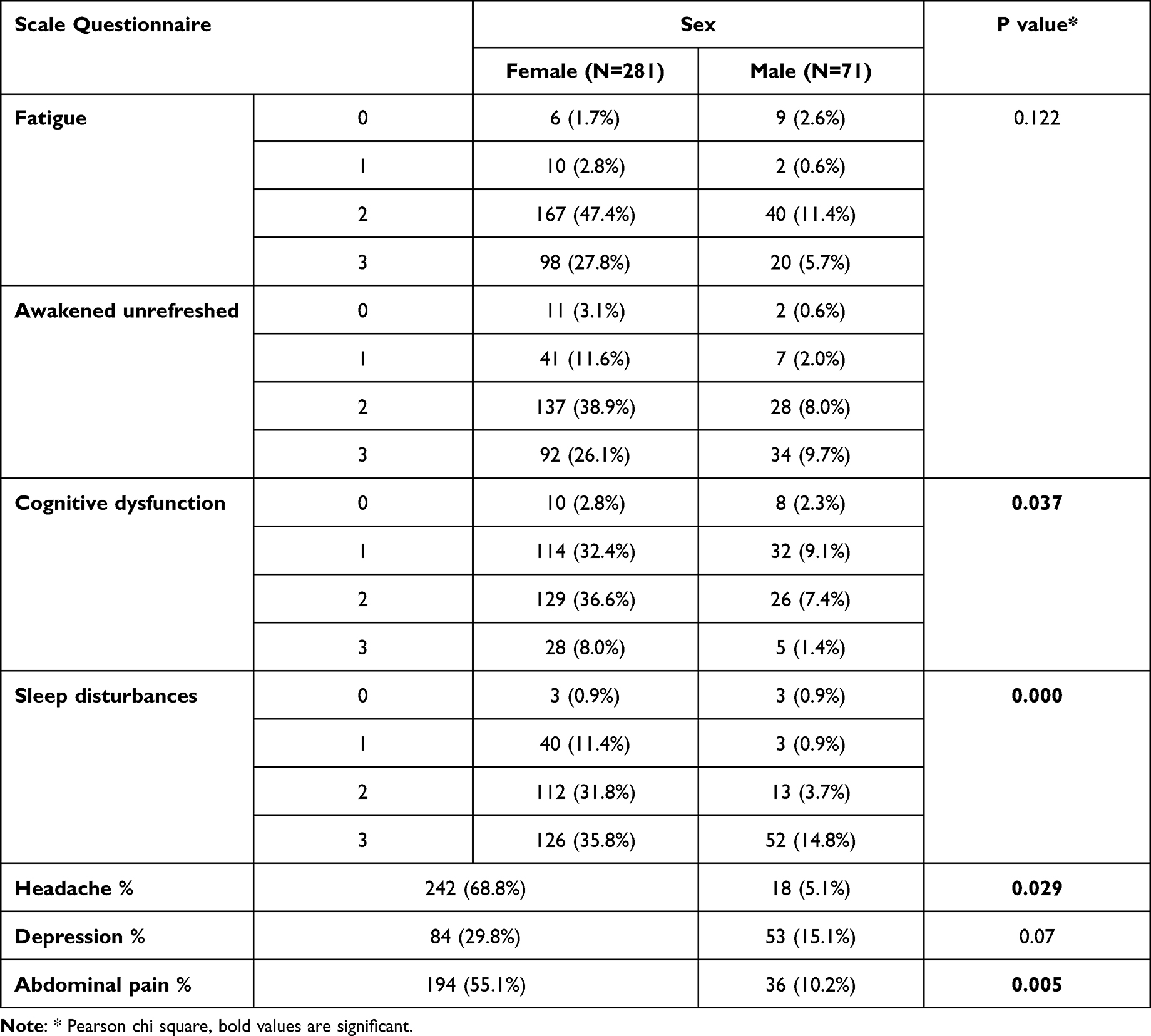 |
Table 2 Qualitative Symptoms of FM According to Gender |
Females showed a significantly higher score than males regarding WPI, SSS, and TPC (p = 0.004, 0.027, and 0.001, respectively), while there was no significant difference between females and males considering disease duration, diagnostic delay, and FIQR (Table 3).
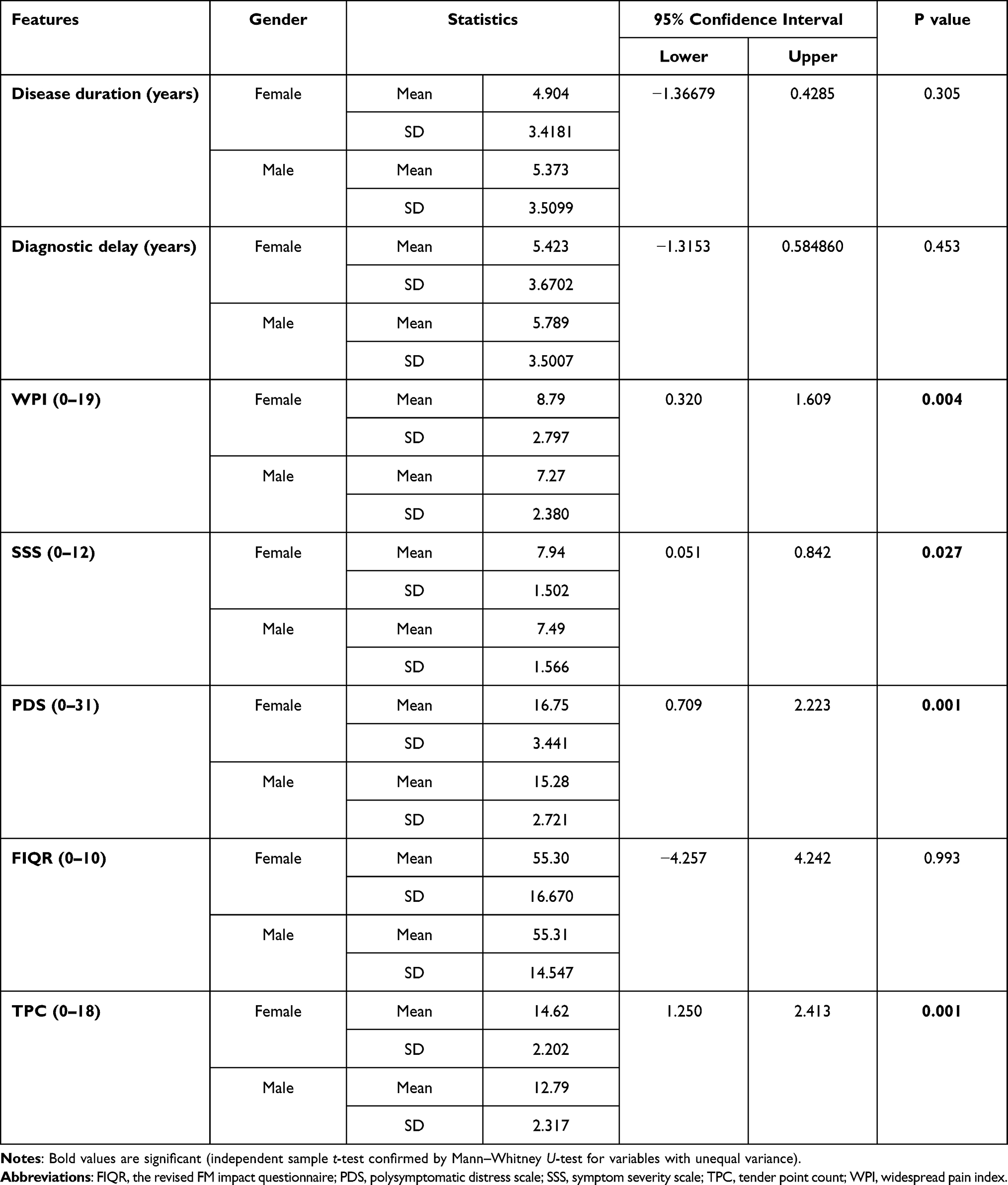 |
Table 3 FM Disease Duration, Diagnostic Delay, and Severity Parameters According to Gender |
Discussion
The relationship between gender and FM is still debatable, confusing, and underestimated despite the development of many diagnostic criteria over the past three decades.5,19,27
FM has always been seen as a major women’s disease. However, according to the parameters applied, the sex ratio differs significantly. When the 2010 ACR criteria are applied, more males are identified with FM; the 1990 ACR criteria showed that the ratio of women to men was 13.7:1, whereas the ratio was 4.8:1 using the 2010 ACR criteria and even less with the 2011 modification (2.3:1).16 When applying the three criteria sets in this study, we found a female to male ratio of 3.96:1.
The perception of FM as primarily a female illness (the traditionally assumed female ratio was 90%) is not supported by data from objective research. As previously stated, the female percentage of cases was 60% based on established criteria and fair patient selection.7,8 Wolfe and others are recommending the application of the 2016 clinical and epidemiological study criteria for FM due to its revised score and widespread pain.14,15
In the current study, we found a significantly higher incidence of fatigue, cognitive dysfunction, sleep disturbance, headache, and abdominal pain in females compared with males, in accordance with established greater values on the biological and social levels of female symptoms and pain reporting.28,29
These differences may make the diagnosis of FM more difficult in men, especially with the less prevalent “generalized pain criterion” and a lesser degree of cognitive dysfunction. Yunus et al30 observed higher levels of fatigue and morning tiredness in the female FM group. However, other studies contrarily observed higher levels of fatigue in male patients19 or reported no gender differences.31,32
The rise in FM in females has been associated with and explained by the variance in the intensity of symptoms in general and in PSD scores in particular.15,17 In the same line, our results showed that females had a significantly higher score than males regarding the WPI and SSS. In accordance with our findings, Wolfe et al reported a difference between women and men with FM regarding the mean PSD (10.2 vs 8.2). They also found a linear relation between the probability of being female and FM and the degree of severity when applying the 2016 criteria.5,14
Regarding the tender point count, we observed that women have a mean tender point much greater than men. However, the points of tenderness are not easy to evaluate, and women are often affected by divergent pain conditions compared to males.28 Newer research reflecting the 2010 elimination of tender points as a criteria for diagnosis of FM has shown gender equality rates.33
In an Italian study based on the 1990 criteria, the authors found no difference between men and women regarding the age at the onset of symptoms, the number of tender points, fatigue, and sleep disturbance. They stated that hyperalgesia is more frequent in women. However, the sample size was very small for both genders, and they recommended further studies on gender differences applying 2010 criteria.34
In a study by Sánchez et al 2012, they reported duration of symptoms and disability in men than in women, while this could not be observed in our study as there were no differences between the sexes regarding the disease duration or the diagnostic delay. It is noteworthy that they depended only on the old (1990) criteria.35 In the same context, Huser et al in 2011 reported a longer disease duration in women but no gender differences regarding the age, sites of pain, somatic symptoms, or features of depression.36
In the current study, we found no significant difference between men and women regarding the FIQR. However, we did not compare our patients on the basis of the individual variables in the questionnaire. Some features are compared separately, such as fatigue and sleep disturbances, which were more prevalent and intense in females.
Aparicio et al investigated the gender differences in quality of life and FIQR in a small cohort of FM patients in Spain.They reported that the overall FIQR is higher in men, while the individual features of the questionnaire showed a higher prevalence of fatigue and morning tiredness in female patients. The quality of life measured by the SF-36 was lower in women with FM. However, they considered their results preliminary given the small sample size (only 20 men) and the consequent low statistical power.37
Although this study evaluated gender differences for the first time through the application of the old and last 2016 ACR diagnostic criteria, there are numerous limitations to the present study. First, because the study was prospective and cross-sectional, selection bias cannot be ruled out. Second, numerous comparisons can raise the chance of a type I error in this relatively small sample. Third, the differences in the current treatments were not evaluated. Nevertheless, these results provide significant data that may help guide future research on the foundation and impact of gender disparities among FM patients.
Conclusion
Female patients with FM had greater disease severity scores, symptomatology, and number of tender points. Whatever the criteria applied, the prevalence and intensity of the disease features are higher in females, which may underestimate the disease in male patients. Future studies with a larger male FM sample size will need to identify why males with fibromyalgia have a distinct clinical profile in terms of symptoms, which may be due to physiological differences.
Data Sharing Statement
The datasets used in this work are available upon reasonable request from the corresponding author.
Ethical Approval
The study was approved by the ethical committee of Al Azhar University School of Medicine in Egypt (Az 062-11-012, December 2019).
Consent for Publication
Consent for publication was obtained.
Disclosure
There are no conflicts of interest reported by the authors in this study.
References
1. Skaer TL. Fibromyalgia: disease synopsis, medication cost effectiveness and economic burden. Pharmacoeconomics. 2014;32(5):457–466. doi:10.1007/s40273-014-0137-y
2. Marques AP, Santo AD, Berssaneti AA, Matsutani LA, Yuan SL. Prevalence of fibromyalgia: literature review update. Rev Bras Reumatol. 2017;57:356–363. doi:10.1016/j.rbr.2016.10.004
3. Clauw DJ. Fibromyalgia: a clinical review. JAMA. 2014;311(15):1547–1555. doi:10.1001/jama.2014.3266
4. Foerster BR, Petrou M, Edden RA, et al. Reduced insular γ‐aminobutyric acid in fibromyalgia. Arthritis Rheum. 2012;64(2):579–583. doi:10.1002/art.33339
5. Wolfe F, Walitt B, Perrot S, Rasker JJ, Häuser W. Fibromyalgia diagnosis and biased assessment: sex, prevalence and bias. PLoS One. 2018;13(9):e0203755. doi:10.1371/journal.pone.0203755
6. Nakamura I, Nishioka K, Usui C, et al. An epidemiologic internet survey of fibromyalgia and chronic pain in Japan. Arthritis Care Res. 2014;66(7):1093–1101. doi:10.1002/acr.22277
7. Shipley M. Chronic widespread pain and fibromyalgia syndrome. Medicine. 2018;46(4):252–255. doi:10.1016/j.mpmed.2018.01.009
8. Galvez-Sánchez CM, Reyes Del Paso GA. Diagnostic criteria for fibromyalgia: critical review and future perspectives. J Clin Med. 2020;9(4):1219. doi:10.3390/jcm9041219
9. Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum. 1990;33(2):160–172. doi:10.1002/art.1780330203
10. Wolfe F, Clauw DJ, Fitzcharles MA, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010;62(5):600–610. doi:10.1002/acr.20140
11. Fitzcharles MA, Ste-Marie PA, Panopalis P, Ménard H, Shir Y, Wolfe F. The 2010 American college of rheumatology fibromyalgia survey diagnostic criteria and symptom severity scale is a valid and reliable tool in a French speaking fibromyalgia cohort. BMC Musculoskelet Disord. 2012;13(1):1–6. doi:10.1186/1471-2474-13-179
12. Casanueva B, García-Fructuoso F, Belenguer R, et al. The Spanish version of the 2010 American College of Rheumatology preliminary diagnostic criteria for fibromyalgia: reliability and validity assessment. Clin Exp Rheumatol. 2016;34(2 Suppl):S55–8.
13. Wolfe F, Clauw DJ, Fitzcharles MA, et al. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: a modification of the ACR preliminary diagnostic criteria for fibromyalgia. J Rheumatol. 2011;38(6):1113–1122. doi:10.3899/jrheum.100594
14. Wolfe F, Clauw DJ, Fitzcharles MA, et al. 2016 revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. 2016;46. 319–329.
15. Ablin JN, Wolfe F. A comparative evaluation of the 2011 and 2016 criteria for fibromyalgia. J Rheumatol. 2017;44(8):1271–1276. doi:10.3899/jrheum.170095
16. Jones GT, Atzeni F, Beasley M, Flüß E, Sarzi‐Puttini P, Macfarlane GJ. The prevalence of fibromyalgia in the general population: a comparison of the American College of Rheumatology 1990, 2010, and modified 2010 classification criteria. Arthritis Rheumatol. 2015;67(2):568–575. doi:10.1002/art.38905
17. Arout CA, Sofuoglu M, Bastian LA, Rosenheck RA. Gender differences in the prevalence of fibromyalgia and in concomitant medical and psychiatric disorders: a National Veterans Health Administration Study. J Womens Health. 2018;27(8):1035–1044. doi:10.1089/jwh.2017.6622
18. Wolfe F, Cathey MA. The epidemiology of tender points: a prospective study of 1520 patients. J Rheumatol. 1985;12(6):1164–1168.
19. Buskila D, Neumann L, Alhoashle A, Abu-Shakra M Fibromyalgia syndrome in men. Semin Arthritis Rheum. 2000;30:47–51.
20. Häuser W, Ablin J, Perrot S, Fitzcharles MA. Management of fibromyalgia: practical guides from recent evidence-based guidelines. Pol Arch Intern Med. 2017;127(1):47–56. doi:10.20452/pamw.3877
21. Yunus MB. The role of gender in fibromyalgia syndrome. Curr Rheumatol Rep. 2001;3(2):128–134. doi:10.1007/s11926-001-0008-3
22. Wolfe F, Anderson J, Harkness D, et al. A prospective, longitudinal, multicenter study of service utilization and costs in fibromyalgia. Arthritis Rheum. 1997;40(9):1560–1570. doi:10.1002/art.1780400904
23. Moshrif A, Gouda W, Abu-Zaid MH. THU0466 Early diagnosis is associated with less disease severity and better outcome in fibromyalgia syndrome: a tricentric prospective analysis of a cohort of 370 patients. Ann Rheum Dis. 2020;79:470. doi:10.1136/annrheumdis-2020-eular.5504
24. Wolfe F, Walitt BT, Rasker JJ, Katz RS, Häuser W. The use of polysymptomatic distress categories in the evaluation of fibromyalgia (FM) and FM severity. J Rheumatol. 2015;42(8):1494–1501. doi:10.3899/jrheum.141519
25. Abd El-Naby M, Hefny MA, Fahim AE, Awadalla MA. Validation of an adapted Arabic version of fibromyalgia syndrome impact questionnaire. Rheumatol Int. 2013;33(10):2561–2567. doi:10.1007/s00296-013-2779-z
26. Bennett R. The Fibromyalgia Impact Questionnaire (FIQ): a review of its development, current version, operating characteristics and uses. Clin Exp Rheumatol. 2005;23(5):S154.
27. Katz JD, Mamyrova G, Guzhva O, Furmark L. Gender bias in diagnosing fibromyalgia. Gend Med. 2010;7(1):19–27. doi:10.1016/j.genm.2010.01.003
28. Hurley RW, Adams MC. Sex, gender, and pain: an overview of a complex field. Anesth Analg. 2008;107(1):309. doi:10.1213/01.ane.0b013e31816ba437
29. Conversano C, Ciacchini R, Orru G, Bazzichi ML, Gemignani A, Miniati M. Gender differences on psychological factors in fibromyalgia: a systematic review on male’s experience. Clin Exp Rheumatol. 2020;2. doi:10.55563/clinexprheumatol/73g6np
30. Yunus MB, Inanici FA, Aldag JC, Mangold RF. Fibromyalgia in men: comparison of clinical features with women. J Rheumatol. 2000;27(2):485–490.
31. Pérez R, Linares U, Perez MB, et al. Differences in sociodemographic, clinical, psychosocial and health care characteristics between men and women diagnosed with fibromyalgia. Rev Clin Esp. 2007;207(9):433–439. doi:10.1157/13109832
32. Yunus MB, Celiker R, Aldag JC. Fibromyalgia in men: comparison of psychological features with women. J Rheumatol. 2004;31(12):2464–2467.
33. Wolfe F, Brähler E, Hinz A, Häuser W. Fibromyalgia prevalence, somatic symptom reporting, and the dimensionality of polysymptomatic distress: results from a survey of the general population. Arthritis Care Res. 2013;65(5):777–785. doi:10.1002/acr.21931
34. Guzzo MP, Iannuccelli C, Gerardi MC, Lucchino B, Valesini G, Di Franco M. AB0925 gender difference in fibromyalgia: comparison between male and female patients from an Italian monocentric cohort Annals of the Rheumatic Diseases. J Womens Health. 2017;76:1379.
35. Castro-Sánchez AM, Matarán-Peñarrocha GA, López-Rodríguez MM, Lara-Palomo IC, Arendt-Nielsen L, Fernández-de-las-peñas C. Gender differences in pain severity, disability, depression, and widespread pressure pain sensitivity in patients with fibromyalgia syndrome without comorbid conditions. Pain Med. 2012;13(12):1639–1647. doi:10.1111/j.1526-4637.2012.01523.x
36. Häuser W, Kühn-Becker H, von Wilmoswky H, Settan M, Brähler E, Petzke F. Demographic and clinical features of patients with fibromyalgia syndrome of different settings: a gender comparison. Gend Med. 2011;8(2):116–125. doi:10.1016/j.genm.2011.03.002
37. Aparicio VA, Ortega FB, Carbonell-Baeza A, et al. Are there gender differences in quality of life and symptomatology between fibromyalgia patients? Am J Mens Health. 2012;6(4):314–319. doi:10.1177/1557988312436872
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.