")
Back to Journals » Clinical Interventions in Aging » Volume 11
European Society for Swallowing Disorders – European Union Geriatric Medicine Society white paper: oropharyngeal dysphagia as a geriatric syndrome
Authors Baijens LW, Clavé P, Cras P, Ekberg O, Forster A, Kolb GF, Leners JC, Masiero S , Mateos-Nozal J, Ortega O , Smithard DG , Speyer R, Walshe M
Received 4 March 2016
Accepted for publication 27 April 2016
Published 7 October 2016 Volume 2016:11 Pages 1403—1428
DOI https://doi.org/10.2147/CIA.S107750
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Laura WJ Baijens,1 Pere Clavé,2,3 Patrick Cras,4 Olle Ekberg,5 Alexandre Forster,6 Gerald F Kolb,7 Jean-Claude Leners,8 Stefano Masiero,9 Jesús Mateos-Nozal,10 Omar Ortega,2,3 David G Smithard,11 Renée Speyer,12 Margaret Walshe13
1Department of Otorhinolaryngology – Head and Neck Surgery, Maastricht University Medical Center, Maastricht, the Netherlands; 2Gastrointestinal Physiology Laboratory, Department of Surgery, Hospital of Mataró, Autonomous University of Barcelona, Mataró, 3CIBERehd, Instituto de Salud Carlos III, Barcelona, Spain; 4Department of Neurology, Antwerp University Hospital, University of Antwerp, Born Bunge Institute, Edegem, Belgium; 5Department of Translational Medicine, Division of Medical Radiology, Skåne University Hospital, Malmö, Sweden; 6Clinique Bois-Bougy, Nyon, Switzerland; 7Department of Geriatrics and Physical Medicine, Bonifatius Hospital, Lingen, Germany; 8Long Term Care and Hospice, Ettelbruck, Luxembourg; 9Rehabilitation Unit, Department of Neuroscience, University of Padua, Padova, Italy; 10Department of Geriatric Medicine, Hospital Ramón y Cajal, Madrid, Spain; 11Clinical Gerontology, Princess Royal University Hospital, King’s College Hospital Foundation Trust, London, UK; 12College of Healthcare Sciences, James Cook University, Townsville, QLD, Australia; 13Department of Clinical Speech and Language Studies, Trinity College Dublin, Dublin, Ireland
Abstract: This position document has been developed by the Dysphagia Working Group, a committee of members from the European Society for Swallowing Disorders and the European Union Geriatric Medicine Society, and invited experts. It consists of 12 sections that cover all aspects of clinical management of oropharyngeal dysphagia (OD) related to geriatric medicine and discusses prevalence, quality of life, and legal and ethical issues, as well as health economics and social burden. OD constitutes impaired or uncomfortable transit of food or liquids from the oral cavity to the esophagus, and it is included in the World Health Organization’s classification of diseases. It can cause severe complications such as malnutrition, dehydration, respiratory infections, aspiration pneumonia, and increased readmissions, institutionalization, and morbimortality. OD is a prevalent and serious problem among all phenotypes of older patients as oropharyngeal swallow response is impaired in older people and can cause aspiration. Despite its prevalence and severity, OD is still underdiagnosed and untreated in many medical centers. There are several validated clinical and instrumental methods (videofluoroscopy and fiberoptic endoscopic evaluation of swallowing) to diagnose OD, and treatment is mainly based on compensatory measures, although new treatments to stimulate the oropharyngeal swallow response are under research. OD matches the definition of a geriatric syndrome as it is highly prevalent among older people, is caused by multiple factors, is associated with several comorbidities and poor prognosis, and needs a multidimensional approach to be treated. OD should be given more importance and attention and thus be included in all standard screening protocols, treated, and regularly monitored to prevent its main complications. More research is needed to develop and standardize new treatments and management protocols for older patients with OD, which is a challenging mission for our societies.
Keywords: Swallowing disorders, malnutrition, aged, frail elderly, quality of life, healthy aging, sarcopenia
Introduction: what is a geriatric syndrome?
The term “geriatric syndrome” was first defined in 1909,1 and became a key concept in geriatrics in the 20th century. The first geriatric syndromes to be defined, often called “the four geriatric giants”, were immobility, instability, incontinence, and intellectual impairment. Other syndromes, such as sarcopenia2 and frailty,3 have since been added. Teachers of gerontology have pointed out that the presence of geriatric syndromes is one of the criteria used to select patients for geriatric care.4 Dysphagia is a frequent and severe condition among older persons to the extent that the question has arisen over whether dysphagia should be classified as a geriatric syndrome.
Evolution and definition of the term “geriatric syndrome”
The original definition of a geriatric syndrome was “conditions experienced by older persons that occur intermittently, may be triggered by acute insults and often are linked to subsequent functional decline”.5 However, at the beginning of the 21st century, several authors modified this concept and defined geriatric syndromes as: Conditions in which symptoms develop when the accumulated effect of the several impairments in multiple domains compromise compensatory ability and reserve and the final outcome is a single phenomenology.6–8
One of the latest definitions of the term “geriatric syndrome” is
Clinical conditions in older persons that do not fit into disease categories but are highly prevalent in old age, multifactorial, associated with multiple co-morbidities and poor outcomes and are only treatable when a multidimensional approach is used.9
Oropharyngeal dysphagia as a geriatric syndrome
Oropharyngeal dysphagia (OD) is a condition involving perceived or real difficulty in forming or moving a bolus safely from the oral cavity to the esophagus.10 OD is classified as a digestive condition in the International Classification of Diseases (ICD) promoted by the World Health Organization ICD-9 (787.2) and ICD-10 (R13).11 OD should be differentiated from feeding disorders and associated imbalances in the normal feeding habits (ICD-9 783.3 and ICD-10 R63.3). Finally, globus pharyngis is the persistent sensation of having a “lump in one’s throat”, phlegm, or some other sort of obstruction when there is none (ICD-9-CM 306.4).
OD has already been proposed as a geriatric syndrome in a study that suggested that OD matched all the requirements for being considered a geriatric giant.12 The following are the criteria needed for a condition to be considered as a geriatric syndrome and the corresponding data regarding dysphagia.
High prevalence in older persons
The prevalence of OD has been calculated in older persons across different settings, with rates between 30% and 40% in independently living older people,13 44% in those admitted to geriatric acute care,14 and 60% in institutionalized older patients.15
Combination of symptoms
OD includes a group of symptoms and signs which refers to difficulty in forming or moving a bolus safely from the oral cavity to the esophagus.10 OD is included in the ICD-10 R13 and International Classification of Functioning, Disability and Health code B5105 of the World Health Organization. Prominent among the main symptoms are aspiration, residue, excessive throat clearing, coughing, hoarse voice, atypical ventilation periods, and repetitive swallowing. An added risk is that many older people are unaware of their swallowing dysfunction.14,15
Common risk factors
Five geriatric syndromes (pressure ulcers, incontinence, falls, functional decline, and delirium) have been shown to share at least two risk factors: functional dependency and cognitive dependency.7 OD has been shown to be more prevalent in hospitalized older patients with functional or cognitive impairments,16 and in independently living older persons with functional or mobility impairments.17 OD is closely associated with age, functional capacity, frailty, polymedication, and multimorbidity.18
Interactions with other geriatric syndromes
The highest prevalence of dysphagia has been observed in neurological patients, in 29%–64% of those with stroke19 and over 80% of those with dementia, especially at advanced stages of the disease.20,21 One study demonstrated a close interrelation between OD and malnutrition (MN).18 Other common geriatric complications like sarcopenia are also considered major sources of reduced reserve capacity due to an age-related diminishment of muscle mass and strength which contributes to dysphagia.22,23
Impaired outcomes
Geriatric syndromes have an impact on the prognosis of older persons; in the case of dysphagia, one research group demonstrated higher short- and long-term mortality associated with OD,16 and recently identified it as a risk factor for hospital readmission for pneumonia in the very old.24 Another study associated dysphagia with MN in independently living older people.25 A recent study related OD, institutionalization, and 1-year mortality in patients 70 years and older discharged from an acute care hospital.18
Multicomponent intervention
These syndromes benefit from multidisciplinary treatment. It is generally accepted that OD should be managed by a multidisciplinary team and its treatment should include different strategies, including compensatory and rehabilitative approaches.12,26,27
According to all the literature mentioned, OD clearly fulfills the criteria of a geriatric syndrome and thus receives the necessary attention not only for diagnosis but also for treatment and prevention of its main complications. Interventions aimed at reducing risk factors will improve incidence and severity rates of OD.8
Populations: age, setting, and condition
Etiology by age
“Any disruption in the swallowing process may be defined as dysphagia”.28 However, the anatomical, physiological, psychological, and functional changes that contribute to alterations in swallowing as part of “aging” are called presbyphagia, and involve natural diminishment of functional reserve.29,30 Though these progressive alterations put older adults at risk for dysphagia, swallowing in healthy older adults is not necessarily impaired.29 But the prevalence of disease increases with age, and likewise the prevalence of dysphagia. OD is one of the comorbidities of many age-related neurological and neurodegenerative diseases (NDDs) and/or their subsequent treatments.30
In persons younger than 60 years, it is mostly associated with oncologic and neurologic pathologies, whereas in older people, it is related to aging itself or to stroke and NDDs.
Prevalence of OD by age-group
Prevalence data in the literature vary as a result of participant selection, screening or assessment tools, and the definition of OD (Table 1). Among the general population, prevalence of OD varies between 2.3% and 16%.31–36 These data are based on self-reported questionnaires or surveys. The prevalence of OD in a random selection of the general population in the Netherlands was 8.4%, as found in a study that used the Eating Assessment Tool (EAT-10)37 in a telephone survey. Prevalence increases with age, with up to 26.7% for participants above the age of 76 years. Using the Standardized Swallowing Assessment by Perry,38 a Korean longitudinal study described a prevalence of OD of 33.7% (95% confidence interval, 29.1%–38.4%) in people over 65 years living independently.39 Another study on independently living older persons found a clinical prevalence of OD of 27%.17 In specific settings, such as hospitals and nursing homes, the prevalence of OD is even higher. Prevalence rates of over 40% have been described in institutionalized people.40 Cabre et al found a prevalence of OD of 44% in older persons in a geriatric acute care unit,41 and Lin et al described a prevalence rate over 60% in people living in institutionalized settings.13
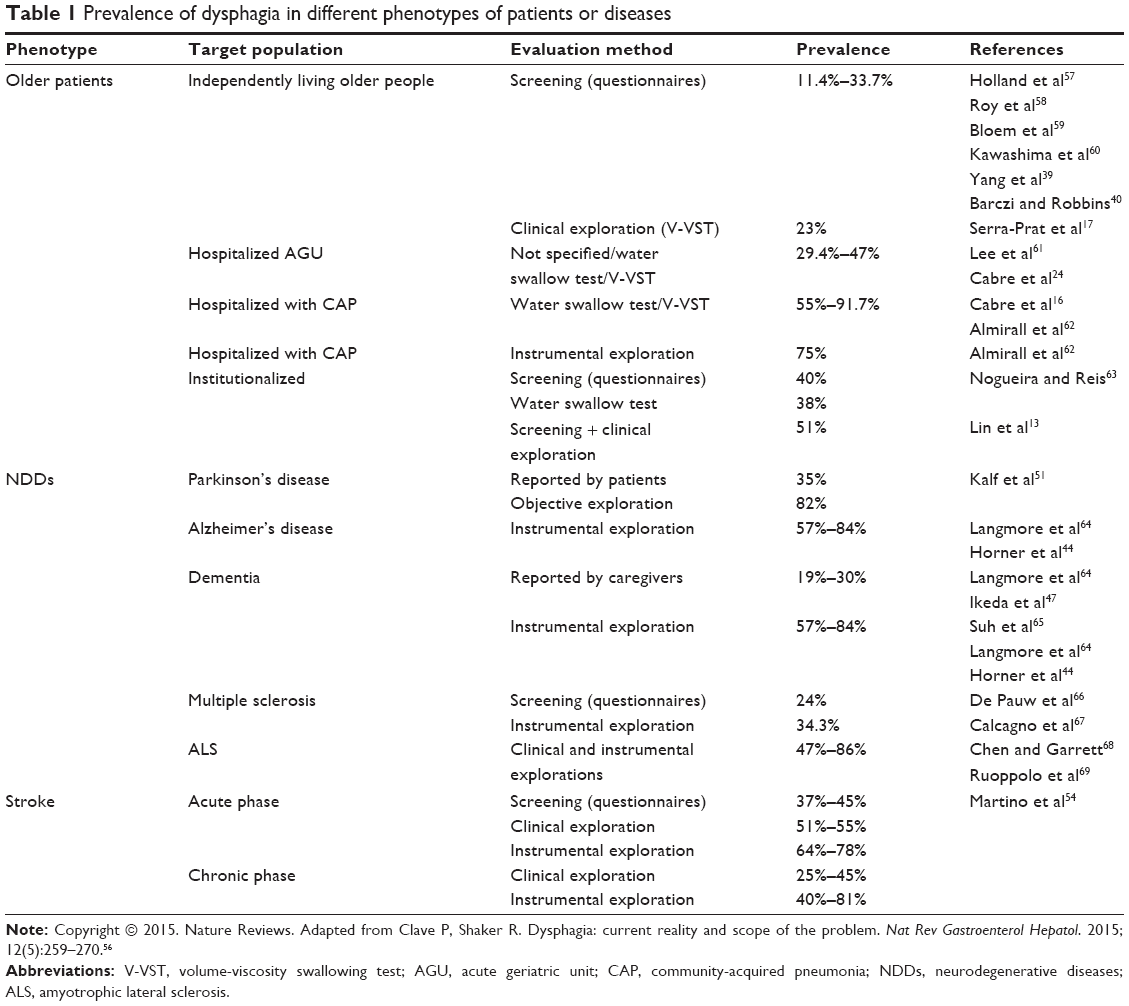 | Table 1 Prevalence of dysphagia in different phenotypes of patients or diseases |
Prevalence of OD in frail older patients
Frail older patients (FOPs) are at greater risk of OD compared to robust or independently living older people. FOPs have many risk factors associated with OD and its complications such as vulnerability, impaired functionality and nutritional status, sarcopenia, and comorbidities.24,42 One study found that the clinical prevalence of OD in FOPs admitted to an acute geriatric unit (AGU) was 47.4%,18 while in FOPs admitted for community-acquired pneumonia, it was even higher at 55%.16
Prevalence of dysphagia in neurological diseases
Dementia, including Alzheimer’s disease
The prevalence of swallowing disorders in patients with dementia can reach up to 93%,43 with 28% suffering from aspiration identified by videofluoroscopy (VFS).43,44 A meta-analysis performed by Affoo et al showed a combined prevalence of dysphagia of 32%–45% in Alzheimer’s disease (AD) patients when clinically assessed, and 84%–93%, when instrumentally assessed.45 Logemann et al found a 55% prevalence of aspiration in AD patients using VFS and the three ingestion methods (chin-down posture, nectar-thickened liquids, or honey-thickened liquids).46
In patients with dementia, the prevalence of swallowing disorders and appetite habits varies according to the type of the dementia. Using a questionnaire, Ikeda et al47 showed significantly higher prevalence among those with frontotemporal dementia (26%) and semantic dementia (20%) compared to AD patients (7%). These percentages also varied according to the stage of the dementia. A study found that the probability of having eating problems over a period of 18 months in patients with advanced dementia was 85.8%.21 Another study with the same kind of patients showed a 35% prevalence of clinical signs of aspiration.48 Up to 45% of patients with dementia in nursing homes have been shown to have some level of swallowing impairment.27
Parkinson’s disease
Using VFS, Logemann et al46 found a 39% prevalence of aspiration in patients with Parkinson’s disease (PD). Using a swallow speed test, Miller et al49 showed that 23% of patients with PD could not finish the test and 80% showed a slower swallowing rate compared to healthy controls. A self-administered questionnaire for PD patients, the Unified Parkinson’s Disease Rating Scale,50 found a prevalence of 32%, independent of the stage of PD, in clear correlation with reduced motor skills. A meta-analysis carried out in 2011 found a rate of 35% in studies checking subjective outcomes, but 82% in studies using objective measurements.51 In a French cohort study that used the Unified Parkinson’s Disease Rating Scale questionnaires in 419 patients with PD, Perez-Lloret et al52 showed that 20% were suffering from dysphagia alone or dysphagia combined with dysarthria and/or sialorrhea. The higher the Hoehn and Yahr score of PD progression, the greater the prevalence of dysphagia (8%–46%).
Stroke
As early as 1997, Smithard et al studied the progression and incidence of OD and risk of aspiration pneumonia (AP) in poststroke patients.53 From the acute stage on admission to 1 month later, the risk diminished from 51% to 15%. Through clinical or VFS assessment in stroke patients, the prevalence of dysphagia was found to vary from 51% to 64% and that of aspiration from 22% to 49%.19
In a meta-analysis by Martino et al,54 similar prevalence rates of dysphagia were found in those with recent stroke: 37%–45% using screening assessment, 51%–55% by clinical assessment, and 64%–78% through instrumental techniques. In a study by Sura et al,27 a general estimation in these patients showed that the prevalence ranged from 30% to 65%, and based on the Canadian Stroke Registry, Flowers et al55 reported an incidence of 44% in 250 stroke patients.
OD – pathophysiology in older persons
The upper aerodigestive tract performs two functions through the same anatomic pathway: breathing and swallowing. The oropharyngeal swallow response (OSR) depends on the configuration of oropharyngeal structures that change from a respiratory to a digestive pathway, the passing of the bolus from the oral cavity to the esophagus, and the reconfiguration to the respiratory pathway.70,71 This complex process involves many interacting sensory, motor, and psychological components, including >40 muscles.72
The deglutition process can be described in three sequential phases.73,74
- The oral phase involves voluntary and reflex actions. During the oral preparatory phase, a homogeneous bolus is made and then collected on the anterior tongue and directed toward the posterior part of the mouth by a posterior and superior lingual movement.
- In the involuntary pharyngeal phase, the soft palate rises to close the nasopharynx and prevent nasal regurgitations. The hyoid bone rises, bringing the larynx up, while the epiglottis closes the entrance to the larynx. The base of the tongue contacts the pharyngeal wall, at the same time as the hyoid moves forward, coinciding with the relaxation of the cricopharyngeus muscle and the opening of the upper esophageal sphincter (UES).
- Once the bolus passes through the UES, the involuntary esophageal phase begins, moving the bolus to the stomach with peristaltic movements.
The neuroanatomy of swallowing implicates cerebral cortical areas like the precentral and inferior frontal gyrus and other regions adjacent to the sylvian fissure and the lateral precentral cortex, all essential for voluntary control of the oral and parts of the pharyngeal phase described later. The motor nuclei of most muscles involved and the pattern generators responsible for reflex initiation of deglutition are located in the brainstem, especially in the nucleus tractus solitarius and the nucleus ambiguous.74
Afferent sensory input sending information of the physicochemical properties of the bolus triggers and modulates the OSR. Somatic stimuli from the oropharynx and larynx, including taste, pressure, temperature, and nociceptive stimuli, are sent via the V, VII, IX, and X cranial nerves to the central pattern generator within the nucleus tractus solitarius, where they join and are processed along with information from the cortex. Swallowing cerebral representation involves the caudal sensorimotor and lateral premotor cortex, insula, temporopolar cortex, amygdala, and cerebellum, which are multiregional and asymmetric. Once activated, the central pattern generator triggers an OSR, including motor neurons in the brainstem and axons traveling through the cervical spinal cord (C1–C2) and cranial nerves (V, VII, IX–XII).70 Older people use more areas of the cortex during swallowing, suggesting that this is necessary for the same swallowing function.75–77 Healthy older adults have prolonged oropharyngeal phase with aging,78,79 delay before the pharyngeal swallow response is triggered, increased residue in the pharynx,72 and higher proportion of silent aspirations or penetrations.80 Overall, oral transit time is significantly prolonged and UES opening is significantly delayed in older people.79,81,82
OD can cause bolus, liquid, or saliva to enter into the larynx. When the bolus remains above the glottis level, it is defined as a penetration, and when it moves below the vocal folds, an aspiration. In the absence of cough, it is defined as silent. Structural alterations in older people may cause OD as they may impair bolus transit. The most frequent ones are esophageal and ear–neck–throat tumors, neck osteophytes, postsurgical esophageal stenosis, and Zenker’s diverticulum.83 OD may be a complication of radiotherapy in patients with head and neck cancer.84 However, OD is more frequently a result of altered physiology of deglutition caused by aging, stroke, or systemic or neurological diseases. In addition, iatrogenic causes like intubation, tracheotomy, surgery, radiation treatments, and the use of some drugs can lead to OD.85–87
OD in older people is related to impaired swallow efficacy and/or safety due to weak tongue propulsion and prolonged and delayed OSR. Impaired swallow safety is caused by delayed physiological protective reflexes during the reconfiguration of the oropharynx (particularly the laryngeal vestibule closure [LVC]) and is associated with various risk factors (aging, NDDs, confusion, and medication). Impaired swallow efficacy is associated with reduced bolus propulsion due to weak muscular tongue force related to sarcopenia.88
Length of swallow in healthy persons is 600–1,000 ms70 characterized by short trigger time in submental muscles,89 short OSR (<740 ms), fast LVC (<160 ms), and fast UES opening (<220 ms).90 However, OSR is altered in older persons, particularly those with neurogenic dysphagia.89–91 Reaction time in the submental muscles is prolonged,89 and duration of the OSR is longer compared with healthy volunteers.90 Likewise, bolus velocity diminished (<10 cm/s) and bolus propulsion forces are weaker (<0.14 mJ)90 in older persons with OD compared with healthy adults (>35 cm/s and >0.33 mJ, respectively).90 In older patients with neurological diseases, delayed LVC and UES opening are the main alterations of the OSR, taking twice as long as that of healthy controls, which leads to unsafe swallow and aspiration.90,91 This delayed OSR in older persons and in patients with neurogenic OD can be attributed to an impairment of oropharyngeal sensitivity,92,93 a reduced number of neurons in the brain, and delayed synaptic conduction of afferent inputs to the central nervous system caused by risk factors such as aging,89 NDDs, and/or stroke.86,88
Screening and clinical assessment of dysphagia
Due to the complexity of older persons’ conditions, a comprehensive geriatric assessment (CGA) is recommended for these kinds of patients. A different diagnostic and therapeutic approach is needed for older persons due to physiological and anatomical changes associated with aging, the atypical presentation of illnesses, and the high frequency of several geriatric syndromes. CGA, as defined by Stuck et al,
Is a multidimensional, interdisciplinary diagnostic process to determine the medical, psychological, and functional capabilities of a frail older person in order to develop a coordinated and integrated plan for treatment and long-term follow-up.94
The positive effects of the CGA on older patients in hospital have been demonstrated, including reduced mortality or rate of institutionalization and improved physical function.94
Despite the high prevalence of OD and its severe complications, it is underexplored and frequently undetected, and the majority of patients with OD are not diagnosed or treated. Diagnosis of OD requires a three-step approach consisting of clinical screening and clinical and instrumental assessment.
The goal of screening is to identify patients at risk of OD early. These patients should be referred for swallowing assessment to prevent aspiration or MN.95 The goal of clinical swallowing assessment is to establish a clinical diagnosis by assessing the pathophysiology of OD, and identifying the main signs and symptoms and the mechanism of the impaired swallow, to select the corresponding treatment for those patients (such as institutionalized patients) who cannot easily undergo instrumental explorations such as VFS.95,96
- The aim of the clinical screening is to detect the majority of patients at risk of OD particularly at the primary-care level. It should therefore be easy to perform, quick, and cheap and of low risk, facilitating its use by general practitioners (GPs), nurses, and other health care providers without specific training in OD. High sensitivity at this point is more valuable than high specificity due to risks involved in undetected OD.96 The aim of the screening process is to select patients who have “failed” the screening test and are at risk of OD and need further clinical and/or instrumental assessment. Three deglutition-specific questionnaires are good examples of screening tools for OD: 1) The EAT-10 is a self-reported questionnaire, on the symptoms associated with OD. It has been shown to be internally consistent, reproducible, and valid. An EAT-10 score of ≥2 is considered abnormal and offers 89% sensitivity and 82% specificity for OD according to a recent study.96 2) There is also a validated specific symptom questionnaire (Sydney Swallowing Questionnaire) which assesses the severity of OD in patients with neuromyogenic dysphagia.97 Patients are asked to grade 17 questions on a visual analog scale. It has shown good psychometric properties.97 Face, content, and construct validity and score also correlated closely with an independent global assessment severity score.97 3) Finally, the Swallowing Disturbance Questionnaire is a self-administered 15-item “yes/no” questionnaire on swallowing disturbances showing good sensitivity (79.7%) and specificity (73%) in identifying patients with swallowing disorders coming from several etiologies.98
- The aim of clinical assessment is to evaluate the safety and efficacy of swallowing, and detect silent aspirations at the bedside. It should have good psychometric properties, reliability, and be easy and safe to perform.95,96 Clinical assessment should be performed by specialists and regularly repeated according to progression of the disease. The objective of OD assessment is to evaluate the two components of swallow: 1) efficacy, a patient’s capacity to consume the necessary amount of calories and water to be well nourished and hydrated; and 2) safety, a patient’s capacity to consume all the required calories and water without respiratory complications occurring.15 There are many swallowing evaluation tests, and the sensitivity or specificity among them varies.99 Traditional clinical assessment tests for OD include Burke’s 3-oz water swallow test,100 the timed swallow test,100 and the standardized bedside swallow assessment.101 Patients are asked to swallow 50, 150, or 60 mL (3 oz)101–103 water in one go. Abnormal swallow is identified by coughing during or after swallow, wet/hoarse voice quality, or slow swallow (<10 mL/s). Burke’s 3-oz water swallow test presented a sensitivity of 76% and a specificity of 59% in detecting aspiration,100 and the standardized bedside swallow assessment showed a sensitivity of 47%–68% and a specificity of 67%–86% according to whether the administrator was a doctor or speech–language pathologist.101–103 These clinical tests involve continuous swallowing of quite large quantities of liquid, which puts the patient at risk of aspiration. Furthermore, several of these studies on bedside tests for OD lacked methodological quality, so the psychometric properties of the procedures under study could not be determined accurately.102
Two recent systematic reviews,95,104 following the design and quality criteria of the Cochrane Collaboration for reviewing test accuracy of diagnostic tools, recommended the following: 1) bedside clinical tests with water or other liquids together with oximetry, to look for coughing, choking, voice changes, and desaturation, thereby identifying patients with OD;95 and 2) minimum required psychometric characteristics including sensitivity of >70% and specificity of >60%. Two bedside clinical methods were indicated: the volume-viscosity swallow test (V-VST), and the Toronto Bedside Swallowing Screening Test (TOR-BSST). The V-VST involves the sequential administration of 5–20 mL boluses at three viscosities (nectar, liquid, and pudding) to explore both safety and efficacy of swallowing.96,105 Clinical signs of impaired safety include cough, fall in oxygen saturation ≥3%, and voice changes; and signs of impaired efficacy include impaired labial seal, piecemeal deglutition, and oral and pharyngeal residue. V-VST showed a sensitivity of 94% and a specificity of 88% for OD, 91% sensitivity for aspiration, and 79% sensitivity for impaired efficacy, and is thus safe, quick, and accurate.96 The use of several viscosities can provide more information than a water test and protects patients from aspiration.96,105 The TOR-BSST is a two-step test.106,107 The first step involves an oral exam, and the second step involves swallowing 10×1 teaspoons of water. The test is only administered if the patient is alert. At the first sign of abnormal swallow, the test is suspended.96,105 Sensitivity of the TOR-BSST for OD is 80%–96%, and specificity is 64%–68%.95
Patients with positive tests should undergo instrumental explorations (VFS or fiberoptic endoscopic evaluation of swallowing [FEES]), or for those who cannot easily undergo these explorations (such as older patients admitted to nursing homes), the most appropriate compensatory therapy can be decided according to the results of the V-VST.96
Instrumental assessment
Clinical decision making is the process of reaching an informed judgment necessary to plan treatment or rehabilitation for a patient. Are instrumental evaluations helpful in orienting the clinical decision making of a dysphagia treatment plan? When dealing with OD, decision making may not be straightforward. An instrumental examination may be indicated in order to confirm the diagnosis and/or plan treatment for patients suspected of having dysphagia following clinical observation/examination. Findings from instrumental assessments of OD are helpful in understanding the pathophysiology of deglutition disorders and in evaluating the natural progression of the disease and the response to therapy. Indications and contraindications, including cognitive-linguistic status and overall health status of the patient, should be taken into consideration when selecting instrumental assessment. As described in the literature, instrumental assessment includes VFS of swallowing, FEES, ultrasound, and manometry.108–111 Structural and functional assessment of the muscles and structures used in swallowing including the esophagus, and the pathophysiology of airway protection and coordination of respiration and swallowing are recommended points of interest in the instrumental assessment of swallowing.112 The effects of bolus modification, changes in bolus delivery, and therapeutic postural or airway protection maneuvers can also be evaluated during instrumental assessment if deemed safe for the patient.113 Some instrumental procedures provide specific information about a particular aspect of swallowing. Multidimensional swallowing assessment is recommended, using different assessment tools, to provide complimentary information on the swallowing pathophysiology and to support the decision making of the treatment plan.113–115 However, access to dysphagia health care and instrumental swallowing assessment varies across European countries, groups, and individuals, influenced by social and economic conditions as well as the existing health policies. The current position statements of the European Society for Swallowing Disorders (ESSD) state that patients who suffer from dysphagia or impaired airway protection during clinical assessment should have an instrumental assessment such as VFS or FEES.116 These examinations should be performed in a standardized way by experienced personnel, but there are several different protocols and there is no consensus on the number of swallow trials, bolus volumes, and bolus consistencies to include in an FEES or VFS examination. As described earlier, the instrumental tests should assess the impaired physiology and methods by which the impairment might be remedied.
FEES enables the pharynx and larynx and their function to be directly visualized, during and after the swallow. FEES is able to visualize manifestations such as vallecular and pyriform sinuses residue, uncontrolled bolus or premature loss of liquid, penetration, aspiration, and piecemeal deglutition.117,118 In addition, it is well tolerated, easy to perform, and repeatable, and the clinician is able to perform it at the bedside.118
The aim of VFS is to evaluate the safety and efficacy of swallowing, to characterize the swallowing impairments in terms of VFS manifestations, and to assist in the selection and evaluation of treatments. VFS videos should be examined in a dark room to reduce interpretation mistakes. VFS should be performed in a lateral projection, and images should show the lips, mouth, pharynx, cervical spine, and the esophagus (with dental prosthesis in place). Furthermore, VFS and FEES examinations should be viewed several times at normal speed and then frame by frame, as needed. The interpretation of exams improves with clinicians’ experience and training.114,119 The use of standardized checklists to assess VFS and FEES exams can be helpful as a format for the final clinical report and for future comparison of results between patients.108,120
Complications of dysphagia in older persons
OD in older people causes severe complications that have great impact on patients’ health, nutritional status, functionality, morbimortality, and quality of life (QoL). Impaired efficacy of swallow or the inefficient ingestion of nutrients and liquids leads to MN and/or dehydration. Impaired safety of swallow with penetrations and aspirations causes respiratory infections, hospital readmissions, and AP. All these complications lead to frailty and institutionalization, increasing morbimortality in this population.12,15,82,121
MN and dehydration
MN in patients with OD is associated with overall oral intake and impaired bolus propulsion forces82 caused by weakness of muscular neck and tongue strength and decreased tongue volume through sarcopenia and frailty.122,123 OD is associated with three types of MN: 1) starvation-related MN (ie, OD in older patients), 2) chronic disease-related MN (ie, OD in patients with neurological and neurodegenerative and head and neck diseases), and 3) acute disease-related MN (ie, AP). Starvation-related MN develops in situations of chronic energy and protein deficiency and is characterized by decreased muscle mass, decreased subcutaneous fat, and no inflammation. Chronic disease-related MN, the most common type of MN in hospitals, is characterized by reduced food intake due to disease-associated anorexia and chronic inflammation. Finally, acute disease-related MN is characterized by acute and severe inflammation that impairs the ability to use oral or infused nutrients.124
MN is highly prevalent in several phenotypes of older patients with OD. A study on independently living older persons with OD showed that the percentage of patients with or at risk of MN was 21.7%. Moreover, prevalence of MN at 1-year follow-up rose to 26% in patients with OD.25 Another publication showed that prevalence of MN in older patients with OD and pneumonia was 37%, and also found that MN correlated with lower functional capacity and higher 1-year mortality after hospital discharge.16 Among older patients with OD from an AGU, the percentage of malnourished patients or those at risk of MN was 61.5%.125 A European Council resolution has recognized the correlation between dysphagia and MN recommending to improve the diagnosis and treatment of MN in OD patients.126
Dehydration, also caused by impaired efficacy of swallow, is a major problem in older people. Restricted fluid intake due to dysphagia causes an imbalance of body fluids, which leads to increased mortality in hospitalized older adults.127 Dehydration is one of the ten most common diagnoses on hospital admission of older persons.128 Furthermore, its prevalence in older people from the community is as high as 60%.129 Dehydration has been directly related to OD,130 and a study found that daily oral thickened fluid intake in patients with OD was only 22% of the recommended daily amount.131 The hydration status of older patients with OD must be monitored to avoid additional complications.132
MN and dehydration as complications of impaired efficacy of swallow can lead to sarcopenia, decreased functionality, reduced immunity, impaired wound healing, hypovolemia, frailty, and higher morbimortality.15 Sarcopenic dysphagia has been defined as “the difficulty of swallowing due to sarcopenia of generalized skeletal and swallowing muscles”. Tongue force, which plays a key role in bolus propulsion, is impaired in older adults. This finding has been related to weakness of the head and neck muscles and general frailty.122 This kind of dysphagia is closely related to MN, and FOPs can experience activity-, disease-, and/or nutritional-related sarcopenia that results in the development of sarcopenic dysphagia. Nutritional-related sarcopenia treatment should involve correct nutritional intake and management with the aim of increasing muscle mass.133
Respiratory infections and AP
OD is associated with lower respiratory tract infections in independently living older people.25 One study on this population showed that annual incidence of lower respiratory tract infections was higher in patients presenting impaired safety of swallow than in patients without (40% vs 21.8%; P<0.05).25 AP is defined as a pulmonary infection with radiological evidence of condensation in patients with swallowing disorders. AP is caused when liquid, saliva, or food containing oropharyngeal microorganisms and respiratory pathogens is aspirated into the airways.134–136 AP can occur in up to 50% of aspirations in older people with an associated mortality of 50%.10 One publication showed that the number of admissions caused by AP among all admissions for pneumonia increases gradually with age, from 0% in those patients 50 years or younger to as high as 90% in those 90 years or older.136 Up to 10% of independently living older patients admitted to a general hospital with a diagnosis of pneumonia are diagnosed with AP, and the prevalence increases to 30% in nursing home residents.137 Up to 20% of patients with cerebrovascular disease have AP in the first days after stroke, and it is the first cause of death 1 year following discharge.10,138 A study found a high rate of AP in nursing homes (43%–50%) with a mortality of up to 45%.10 Two studies on hospitalized older patients with community-acquired pneumonia found that the prevalence of OD, measured with a clinical test during hospitalization, was very high (>50%). In addition, at 1 year follow-up, the patients who had presented OD on admission had significantly increased mortality compared with patients who had not.16,134
The physiopathology of AP is explained by three main risk factors: 1) OD with impaired safety of swallow and aspiration; 2) a vulnerable status with MN, frailty, comorbidity, reduced functionality, and impaired immunity; and 3) deficient oral health and hygiene, presenting bacterial colonization by potential respiratory pathogens.20,135 AP is closely related to patients’ oral health and hygiene status because the quantity and quality of germs in the mouth are determined by the conditions of the oral niche.139,140 In addition, caries, the number of functional teeth, periodontitis, and the presence of dental plaque were correlated with the incidence, severity, and death rate of AP in older patients.139,141 One study assessing the oral health and hygiene status of older people with dysphagia found high prevalence of periodontitis, caries, and poor oral hygiene status.142 In addition, according to a meta-analysis, a positive correlation between OD and AP in FOPs with stroke was found, also showing that good oral dental care reduced this risk significantly.143 A review described AP as a frequent complication of OD, the major risk factors being age, poor dental hygiene (colonized dental plaque), MN, smoking, use of some antibiotics, inhalers (for COPD patients), dehydration, and reduced immunity.144
Hospital readmissions and institutionalization
OD is a very frequent, independent, and important risk factor correlated with hospital readmission for pneumonia in older persons.138 A study found a hospital readmission rate for pneumonia of 3.67 readmissions per 100 person-years in individuals without OD and 6.7 in those with OD, with a rate ratio of 1.82.138 This study also found that ~5% of all hospital readmissions and 80% of those due to AP were attributable to OD, showing the relevance of dysphagia regarding health resource consumption.24 In addition, OD leads to frailty, which is associated with higher institutionalization rates, hospitalization, and deaths.42 One study found that institutionalization rate after discharge in patients with OD admitted to an AGU was higher than those without OD (52.4% vs 28.5%; P<0.001).18
QoL and psychological burden
Several studies have suggested that there is significant psychological and social impact associated with dysphagia with negative consequences for individuals’ psychological well-being.145,146 One study, which analyzed QoL while eating in older nursing home residents, found that 84% said that eating should be enjoyable, but only 45% expressed that it was. An important 41% experienced anxiety and panic during eating, while 36% avoided eating with other people because of OD.145 In addition, anxiety and depression are associated with OD.147–149 In an outpatient clinic for OD, the prevalence of associated anxiety was 37%, and of depression, 32%.149 Functional changes in eating, often associated with OD, have a negative impact on QoL.150 Research on dysphagia associated with oropharyngeal and laryngeal cancer84,151 and progressive neurological disease148 suggests that negative change in QoL is strongly associated with both oropharyngeal and esophageal dysphagia. Complications of OD have a great impact on QoL of patients and national health budgets because they induce frailty, institutionalization, comorbidities, decreased functionality, readmissions, higher drug intake, and increased length of hospitalization.
Treatment
Treatment for OD is usually divided into compensatory measures that aim to compensate the effects of impaired OSR by avoiding or reducing them, and rehabilitative interventions that improve swallow on a biomechanical level. A recent review explored the level of evidence and classified the types of interventions into the following categories: 1) bolus modifications and management, 2) swallow postures and maneuvers, 3) other interventions, and 4) facilitation techniques.113 There is no specific strategy that fits all older patients with OD,27 but some strategies are useful for many as described by Ney et al:30
- Eat slowly with intent to implement control of bolus flow and allow enough time for a meal.
- Do not eat or drink when rushed or tired.
- Put small amounts of food or liquid into the mouth (use a teaspoon).
- Concentrate only on swallowing – eliminate distractions.
- Avoid mixing food and liquid in the same mouthful.
- Place the food on the stronger side of the mouth if there is unilateral weakness.
- Alternate liquids and solids to “wash down” residue.
- Use sauces, condiments, and gravies to facilitate cohesive bolus formation.
Older dementia and stroke patients might not be independent and may require the help of others for feeding due to physical and/or cognitive limitations,27 so caregivers need training.
Bolus modifications
The modification of the consistency of solids and/or liquids is the main element of compensatory treatment for patients suffering from OD,27 and the therapeutic effect of this strategy is very high. The therapeutic effect of thickening agents is viscosity-dependent, and these agents are frequently used in hospitals and nursing homes.152 The level of evidence with this treatment is A (randomized controlled trials) and B (non-randomized controlled trials).113 Several studies have shown that these products reduce laryngeal vestibule penetrations and tracheobronchial aspirations,82,90,153 but compliance with treatment is low, 48%–56%,154 due to the dislike of bolus organoleptic properties (texture and taste), greater effort needed to swallow, and increased difficulty of meal preparation.155 Some studies reported that thickeners increased the risk of dehydration,27,154 probably due to greater swallowing difficulty and lower compliance at high viscosity levels. The lower the viscosity, the higher the compliance, as patients tolerate thinner viscosities like nectar better.156 Treatment compliance is important as it correlates with incidence of respiratory infections, AP, and hospital readmissions.157
Solid food modification can improve the safety of swallow and nutrition in patients with OD and/or deficient chewing.27,113 There are several recommended diets which detail the kinds and textures of alimentary products needed by patients with OD, but the descriptors vary and scientific evidence in this field is limited.158 Some of the most frequently used descriptors in Europe are those of the British Dietetic Association and the Royal College of Speech and Language Therapists which are based on consensus of expert opinion. As research provides more evidence, these descriptors should be updated.159
Swallow postures and maneuvers
Postures are easy to learn, do not require great effort, and are able to redirect bolus flow through biomechanical adjustments. A general directive is to swallow in an upright position (90° seated)27 and to maintain this posture after the meal for at least 30 minutes. Some examples include tucking chin toward the chest,27 or turning the head toward the hemiparetic side (for hemiparetic patients) to effectively close that side to bolus entrance, thus facilitating bolus transport through the non-paretic side of the pharynx. Chin-down posture is easy to perform and helps patients close the respiratory airway, and it has maximal level of evidence (A).113,160 There are also specific maneuvers to compensate swallow alterations, which should be learnt and performed automatically. Each specific maneuver is used to compensate a particular biomechanical alteration.88,161 Generally, level of evidence for maneuvers and other postures is B.113
Some of the most used ones are the following:
- Double deglutition is used to reduce post-swallow residue before next inspiration.161
- Mendelsohn maneuver, aimed at treating reduced laryngeal excursion and impaired cricopharyngeal opening, promotes higher extent and duration of larynx elevation, and consequently, increases amplitude and duration of UES opening.161 It consists of maintaining the larynx at the highest position for a few seconds by voluntary muscular contraction during swallowing.
- Effortful, forceful, or hard swallow aims at increasing the tongue base movement during swallowing to enhance bolus propulsion.88,161 It consists of making a swallow hard by squeezing all the deglutition muscles.
- Supraglottic and super supraglottic swallow is useful in patients who have impaired safety of swallow during the pharyngeal phase or in patients with a slow OSR. It consists of breathing deeply and holding the breath during swallowing and coughing just after swallow to eliminate any residue. The maneuver aims at protecting the airways by closing the vocal folds before and during swallowing. The difference between supraglottic and super supraglottic swallow is the effort level in the pre-swallow breath-hold.12,110
Other interventions
Oral hygiene
Deficient oral hygiene is a risk factor for pneumonia in older patients with OD and is very common in this population.135,142 The prevalence and quantity of potential respiratory pathogens in the mouth are very high in older patients with OD compared to those without.162 Thus, patients should be told to perform daily oral hygiene measures and perform periodic professional dental examinations.30 One systematic review found that:
Oral health care consisting of tooth brushing after each meal, cleaning dentures once a day, and regular professional oral health care seemed the best intervention to reduce the incidence of aspiration pneumonia.163
In addition, oral cleaning with mouthwashes (especially with chlorhexidine without ethanol) has shown good results.163,164 Edentulous patients should clean mouth surfaces and dentures every day and use mouthwashes to avoid bacterial colonization.163 Another systematic review, based on randomized clinical trials, found a preventive effect of oral care on respiratory infections and pneumonia and showed that mechanical toothbrushing decreased risk of mortality from pneumonia (one out of every ten cases) and had a preventive effect on nonfatal pneumonia in dependent older individuals.165
Minimal oral hygiene should be performed every 12 hours to avoid dental plaque formation.166,167 Mouthwashes should be used at least every 3 days, chlorhexidine being the most effective but it should not be used for >15 days.168,169 Phenolic derivatives should be used for maintenance.170,171
Swallow rehabilitation
Swallowing rehabilitation involves exercises that train specific muscles or muscular groups.12,161,172 Generally, swallowing interventions based on exercise have proved to ameliorate functional deglutition, enhance impaired swallowing physiology, and reduce or avoid OD-related comorbidities.27 They are often exercises to improve tongue and lip muscle function, improving bolus formation (homogeneity of the bolus) in the oral cavity just before deglutition.12,161,172 Tongue isometric pressure decreases with aging.173,174 One study showed that progressive lingual exercises (8 weeks) improved isometric and swallowing pressures and tongue volume, suggesting that this approach would help to prevent OD due to sarcopenia, common in FOPs.123 Scientific evidence of this exercise corresponds to level B.113 Moreover, there are additional swallowing rehabilitation techniques such as expiratory muscle strength training that increases the strength of submental muscles and improves expiratory pressures and therefore airway protection,175 and exercises to ameliorate laryngeal excursion and pharyngeal contraction.12,161,172 The Shaker exercise, which aims to strengthen suprahyoid muscles, is an isometric–isotonic anterior flexion of the neck with the patient laying in decubitus. This exercise has shown changes in oropharyngeal physiology and has a therapeutic effect on patients with OD, increasing UES opening and the anterior movement of the larynx, and reducing post-deglutitive residue and aspirations.176 Scientific evidence of this exercise is maximal (A) from a randomized crossover study.113
Surgical treatment
Surgical treatment can be applied in specific situations, such as patients with an UES obstructive pattern, with surgical cricopharyngeal section177 or botulin toxin injection.178 In addition, patients with Zenker’s diverticulum can be operated (diverticulum resection) with good results.179
Facilitation techniques
In recent years, new treatments based on stimulation of sensorial and motor pathways are being assessed. These new therapeutic strategies aim to improve swallowing physiology by recovering swallowing function rather than compensating for swallowing impairments. Some examples are intrapharyngeal or transcutaneous electrical stimulation, repetitive transcranial magnetic stimulation (rTMS), transcranial direct current stimulation, and chemical stimulation with molecules that can stimulate swallowing, such as TRPV1 agonists. Scientific evidence of these therapeutic strategies is limited to patients with stroke; there are no studies as yet on older patients.113
Pharmacological treatment
There are many drugs with detrimental effects on consciousness or OSR which are frequently used by older patients, such as serotonin reuptake inhibitors, benzodiazepines, risperidone, and haloperidol.16 One study found a 60% greater risk of pneumonia in patients using antipsychotics.180 Moreover, extrapyramidal signs and dry mouth are frequent side effects of these medications and ones clearly associated with OD.181,182 On the other hand, the use of pharmacological stimulants to improve OSR has shown promising results.183 TRPV1 agonists such as capsaicin and piperine have been shown to stimulate the sensorial afferent pathways of deglutition and improve OSR.184–188 In addition, heat and acids, which are also stimulants of TRPV1 receptors, have also been shown to improve deglutition.161,189,190
Electrical stimulation
Neuromuscular electrical stimulation (NMES) therapy stimulates deglutition nerves and muscles to improve OSR. NMES requires innervation of the muscle and facilitates muscular contraction through healthy muscular fibers, recruiting motor units to enhance muscular force.191 In addition, electrical stimulation on a sensory level is another strategy to treat patients with OD.192 The main target nerves are the superior laryngeal nerve, the pharyngeal branch of the glossopharyngeal nerve, and two branches of the vagus nerve, the pharyngeal branch and the maxillary branch of the trigeminal nerve. Transcutaneous NMES is applied by placing electrodes on the neck of the patient at specific locations, while intrapharyngeal sensorial stimulation is applied with an intrapharyngeal probe.191 Guidelines on NMES have been published by the British National Institute for Health and Care Excellence giving recommendations, indications, description of the procedures, and efficacy and safety revisions of NMES. The report suggested that current evidence on the efficacy of NMES for OD is limited in quality and that the evidence on safety is limited in quality and quantity although with no major concerns on safety. Thus, NMES should only be used with special adjustments for clinical management, consent, and audit or research.193 In patients with poststroke OD, treatment with transcutaneous NMES increased prevalence of safe swallows and reduced the time of LVC.192,194
Repetitive transcranial magnetic stimulation
rTMS is a noninvasive technique that delivers electrical stimulation through a coil to the brain to generate a magnetic field.195 This therapeutic approach is being assessed for the treatment of patients with OD and has shown good results in poststroke OD patients, improving swallowing safety196 and laryngeal elevation time.197
Transcranial direct current stimulation
Transcranial direct current stimulation is a safe and well-tolerated neurorehabilitation therapy which uses electric current (normally from 1 to 2 mA) passing through the brain. A combination of several variables (current strength, duration of stimuli, and electrode placement) will determine the effects of the therapy.198
Feeding
Nutritional status is basic to good health and an important part of treatment of many chronic diseases, MN being considered a geriatric giant. Food and meals are important elements of all cultures and are closely linked to a person’s lifestyle.199 Nutritional intake is often compromised in older persons with OD. The relationship between MN and OD has already been established,18,25 so nutritional status of older patients with OD must be assessed, taking into consideration that OD can be the underlying diagnosis of this common complication. If MN is present, an individualized nutritional program should be developed, and different aspects of old age should be taken into consideration, including beliefs, attitudes, preferences, expectations, and aspirations.200 A recent position statement of the ESSD claimed that swallowing efficacy and safety must be regularly assessed in malnourished patients with OD in order to choose the best method of providing specialized nutritional support.116 It was also recommended that patients following modified texture diets or being given enteral feeding for OD should have their swallowing and nutritional status regularly assessed, after the first week and then every 2 or 3 months for the first year and then every 6 months, although dysphagia severity and recovery rate may influence the reassessment schedule.116
Dysphagia diets and adaptation of fluids to improve nutritional outcomes are not standardized among the medical community. In addition, due to the multiple fields that deal with the diagnosis, treatment, and management of OD, the intervention of a multidisciplinary team of health care professionals is needed to properly prevent and/or solve OD-associated complications.12,201 However, there is a lack of training in many medical disciplines in the management and care of older patients with OD. The ESSD is trying to correct this with an international multidisciplinary postgraduate diploma for all health care providers working in the field of dysphagia. The ESSD also provides workshops and other courses during the year and has developed an online introductory course available on the Univadis medical education platform and in the ESSD website member section.
Impaired masticatory function
Masticatory function is very important for efficient swallow in older people.202 Chewing reduces food bulk and moisturizes it with saliva, the lips, tongue, and jaws working together with cyclic movements of the jaws. This action is synchronized with the passing of the food by the tongue and cheeks to the molars (stage I).203 There, food is further chewed and mixed with saliva and passed (stage II) through the fauces to the oropharynx or vallecula and formed into a bolus before being swallowed.203 The condition of the mouth, including number of teeth, strength of bite, and flow of saliva, will affect mastication,202 which is inevitably impaired in older persons with edentulism, chewing weakness and longer chewing cycles, and xerostomia.204 Several studies have shown that mastication is impaired in people who wear removable dentures205–207 and this can increase the risk of aspiration.208,209 Implanted prostheses improve masticatory function in edentulous patients.210–212 Nevertheless, studies that focus on nutritional status, dysphagia, and denture function or chewing efficacy are rare.213 Bedside testing procedures or assessment tools which allow geriatricians to screen masticatory function and chewing efficiency are not well accepted or used in current clinical practice.214,215 Objective masticatory performance is generally measured by assessing the ability to crush food into a pulp in a certain number of chews.202
Nutritional support
Due to the complexity of MN in older people and the difference of nutritional parameters between older and young adults, specific guidelines on nutrition have been developed by several organizations, including the European Society for Clinical Nutrition and Metabolism (ESPEN) Guidelines on Enteral Nutrition in Geriatrics that supports that nutritional interventions (mainly oral supplements or tube feeding) can provide sufficient energy, protein, and micronutrients and have an impact on the functional status and on the survival and include specific situations that benefit from them.216
The need of ensuring safe oral feeding and specific situations where nutritional interventions may have a role are pointed out in this guideline. Oral feeding is usually feasible with adaptation of the diet or oral nutritional supplements (ONSs), taking into account the pleasure and social aspects of eating, but some patients present such severe deglutition impairment that compensatory measures are useless and alternative methods of nutritional intake like enteral nutrition (EN) must be provided in order to avoid MN or respiratory complications.
Nutritional interventions includes different strategies such as adaptation of the diet, ONSs, and EN administered by nasogastric tube (NGT) or percutaneous endoscopic gastrostomy (PEG) and should be based on the nutritional needs that change along with time due to aging and many prevalent diseases in old age. The main differences between NGT and PEG are presented in the following subsections.
Oral nutritional supplements
The main goal of ONSs is to increase total nutrient consumption, maintain or recover nutritional status and functional capacity, maintain or improve QoL, and reduce morbimortality.216 A recent position paper of the ESPEN recommends ONSs for old patients at risk of MN, those with multimorbidity and frailty, and those who have undergone orthopedic surgery.216 Among older patients with OD, ONSs are provided as follows: 1) ONSs should be provided as long as appetite and oral nutrition with traditional food are not compromised; 2) ONSs should be provided in patients with anorexia, dietary restriction due to chronic diseases, nutritional intake <75% of their nutritional requirements, or involuntary weight loss; 3) ONSs (standard, hyperproteic, hypercaloric, hypercaloric–hyperproteic, and specific) should be given to patients according to their specific needs; 4) ONS prescriptions should be recorded precisely in order to monitor and manage patients’ nutritional status.217
Enteral nutrition
Nasogastric tube
NGT is the most commonly used type of probe and is recommended for short periods of time (<2 months) and when there is no risk of gastroesophageal reflux (GERD). It is recommended for patients with acute dysphagia that has favorable prognosis.218 Some of its disadvantages are enhanced risk of GERD, accidental extraction, and nasal and esophageal lesions.219,220
Percutaneous endoscopic gastrostomy
Percutaneous tube is placed directly to the stomach through the wall of the abdomen. The PEG is most commonly used, and it can be inserted by radioscopy or surgery. It is recommended in patients who need long-term EN (>4–6 weeks) such as those with chronic or progressive diseases.221,222 Geriatric patients with dysphagia after stroke and with dementia are most indicated for PEG. There is currently a controversial discussion over whether PEG can prevent AP especially when aspiration during feeding is minor or micro.223 In addition, PEG may cause an enhanced risk of GERD with increased risk of aspiration.224 Finally, decision over indication for PEG in geriatrics is a challenge to the interdisciplinary team and includes the patient and the caregiver.
The continued need for adapted nutritional support should be reviewed regularly.116 Ongoing, unintentional loss of weight in older adults is related to increased mortality,30,225 making the evaluation of nutrition and nutritional adaptation a key element in management of older adults with OD.
Specific indications
The main indication for EN (PEG or NGT) is severe neurological dysphagia, for which EN should be started as soon as possible, accompanied by intensive swallowing therapy. EN administration in patients with severe dysphagia may reduce nutritional complications, but NGT has not been shown to prevent AP.216 In dementia, ONSs or NGT may improve nutritional status, but the stage of dementia must be taken into consideration:
- Early- and middle-stage dementia: ONSs and sometimes NGT can be considered to provide sufficient calories and nutrition and prevent undernutrition.216
- Terminal dementia: The ESPEN guidelines recommend avoiding tube feeding in this population.216 The American Society for Clinical Nutrition and Metabolism published a guideline on the use of PEG in patients with advanced dementia which provides a checklist and an algorithm that should be consulted before placing G-tubes or any long-term enteral feeding devices and counsels against them in patients with advanced dementia or other end-stage diseases.226 In addition, there are several studies that showed a morbidity and mortality associated with NGT or PEG in advanced dementia which should be taken into account.227–231 Finally, there are two documents that should be mentioned: first, the prospective study of Mitchel et al which showed an association between eating problems including OD and mortality, considering them bad prognosis criteria,21 and the Cochrane review that found poor-quality studies and no evidence in this population.232
Health economics, social burden, and impact on QoL of OD in older people
OD can occasionally increase financial costs to older patients, their carers, and health service providers.27,201 OD is recognized as carrying a significant physical burden with the presence of drooling, chewing and swallowing difficulty, coughing, choking, and aspiration. Knowledge of these physical impairments is insufficient to understand the consequences of OD for older persons, their families, and other key stakeholders. OD has a serious impact on patients’ social life because eating is compromised and treatment with compensatory measures is not well accepted by patients. The social burden of OD and its impact on QoL must be evaluated to facilitate a holistic approach to management of OD in older persons.
The purpose of this section is to review the evidence on the impact of OD on the domains of health economics (HE) and social burden.
HE of OD in older persons
HE “is concerned with the optimum use of scarce economic resources for the care of the sick and the promotion of health, taking into account competing uses of these resources”.233
HE on swallowing disorders in older persons has not been studied in depth despite causing increased financial costs to patients, carers, and national health care systems. Apart from the cost of home and hospital care and rehabilitation, OD causes other social costs such as loss of productivity and formal and informal care. One possible reason for this lack of knowledge on the economic impact of OD is that it is difficult to place a monetary value on its physical, psychological, and social consequences, particularly as they coexist with underlying medical conditions and comorbidities. A further challenge is that health care systems vary from country to country.234 Nevertheless, dysphagia is known to impact on length of hospital stay,235,236 thereby increasing costs. A study examined the cost of poststroke OD in the US and found that the cost for patients with OD was US$4,510 more per patient than for those without OD.236 People with dysphagia were more likely to be discharged to nursing homes than to their own home and had longer hospital stays than patients without dysphagia when age, comorbidities, ethnicity, and proportion of time alive were controlled in the analysis.236
OD gives rise to MN and dehydration, a possible important predictor of MN in older persons.18,25,237,238 Investigators and economists have attempted to measure the cost of MN and dehydration on health services across the world. Hospital admission rates and mortality have been found to increase in people with low (<20 kg/m2) body mass index levels and compromised nutritional states such as MN and dehydration.239 With data collected in 2003, the British Association for Parenteral and Enteral Nutrition estimated that the cost of disease-associated MN in the UK was >£7.3 billion (~€10.5 billion) per year240 or ~10% of health care costs in the UK at that time.234 There were increased costs for adults over 65 years of age in both hospital and long-term care settings. But it has been suggested that these results were conservative as they did not include costs of house calls by health care workers, visits to GPs and outpatient clinics by adults <65 years, or the costs of private health care.241
OD patients have increased length of hospital stay; one study found an average of 1.64 days increased length of stay and conservatively calculated the annual economic impact of OD in the hospital setting at US$547 million (~€505 million).235 Regarding respiratory infections, the cost of AP was also estimated in the US in 1995 to be US$26,618 (~€24,590) per patient, with a mean hospital stay of 16.1 days.242 Another study performed in Canada calculated a mean cost of AP per patient of CAD$17,000 (~€12,410), but it ranged from CAD$11,000 to CAD$94,000 (approximately from €8,030 to €68,620) depending on the comorbidities the patients presented.243 A study also showed that specialized care of patients with OD and chest infection reduced the costs of hospital stay from £48.2 million to £26.1 million (approximately from €65.8 to €35.6 million) when speech–language pathologists were involved.244 In order to reduce health-associated expenses, preventive strategies are needed. OD is an easy and inexpensive complication to treat. Minimal care should be aimed at early screening of patients, adaptation of liquids and food to select the appropriate volume and viscosity to avoid penetrations and aspirations, screening and treatment of MN and dehydration with nutritional supplements, and screening and promotion of good oral health practices among these patients to reduce bacterial colonization by respiratory pathogens.
Social burden
The concept of “social burden” is poorly defined in the literature. The social burden of a condition should be understood in the context of social organization, cultural roles, and cultural beliefs. Religious, cultural, and family traditions all play a role in eating, drinking, and swallowing,245 which are affected when OD arises. Issues such as food preferences, social roles, family roles in feeding, and the role of tube feeding must be considered when interpreting the social burden of OD on the individual. Eating practices and mealtime regimes become disrupted when a person develops OD. Fear of choking, altered diets, slow eating and drinking, fatigue, and embarrassment of eating in public all affect participation in social events.145 Preparation of special diets can add to financial burden and stress on older carers and families. Lack of compliance with diet and swallowing regimes can cause tension and conflict within families.246
Further research on the HE and social burden of OD is needed to calculate the real cost of this disease and the potential economic benefits from the interventions. Once we can measure these benefits, we will be able to convince decision makers of the importance of improving screening, diagnosis, treatment, follow-up, and prevention of the condition.
The legal framework of swallowing disorders
Patients with oral feeding difficulties make health care workers face legal, moral, and ethical challenges. Feeding difficulties can arise in persons with physical or cognitive impairments at any stage of life including end of life. Treatment for dysphagia by artificial hydration and nutrition is a medical intervention and an ethical issue. As a general rule, any health care intervention is preceded by assessment and an informed consent (IC) by the patient or a proxy, consent that can be implicit or explicit in nature. Yet, there are some forms of care that seem so self-evident that one would hardly consider obtaining an IC. When a medical center admits a patient, this center as a general rule has the obligation of providing basic health care. This includes several measures such as heating, refuge, relief from pain and distressing symptoms, hygiene measures, and oral nutrition and hydration which could include, if conditions require, their provision by artificial means. Some patients will be confronted with swallowing disorders and will need assessment and treatment, either by modification of nutrient selection or texture or by administration of artificial nutrition and hydration by nasogastric or percutaneous gastrostomy tube. Furthermore, there are instances where nutrition becomes an intervention that is no longer defendable and is not adding to the comfort of the patient. At the end of life, many patients will refrain from eating and drinking and will eventually die due to dehydration among other causes. The discussion on providing nutrition by tube feeding as an obligatory basic life support or a medical intervention that needs consent and can be withheld in some conditions has a long history. The former refers to nutrition as a symbolic gesture, as a sign of compassion and care, the latter is contingent with patient autonomy and emphasis on quality rather than quantity of life.
Nutrition as a fundamental human right
It is important to note that two relevant articles in the European Convention on Human Rights (1950) can apply to the situations of food intake.247 Article 2 refers to the right to life and states that “Everyone’s right to life shall be protected by law”. The article has been used in relation to providing or withholding artificial nutrition and hydration. Article 3 of the European Convention refers to prohibition of torture and states that “No one shall be subjected to torture or to inhuman or degrading treatment or punishment”. Forced tube feeding without consent could be considered an assault, and this has been the subject of debate in cases of hunger strike by political activists and prisoners.
Whether withholding nutrition can be considered an infraction on human dignity is the subject of continuous debate. The Roman Catholic Church has considered tube feeding a medical intervention that can be withheld under particular circumstances.248 However, in 2004, at a 4-day conference by the Pontifical Academy for Life, Pope John Paul II addressed participants and stated that: “artificial nutrition and hydration, was “normal care” and “a natural means of preserving life, not a medical act,” and, therefore, morally obligatory, independent of an assessment of benefits and burdens to the patient, the patient’s family and the community”.248
This position that seemed to be more conservative created an intense discussion in ecclesiastic circles and beyond. It has been argued later that the statement was taken out of context and indeed Pope John Paul II refused hospitalization and tube feeding when confronted with end of life. The provision of a treatment (in this case nutrition) that is not beneficial to a patient is morally and ethically wrong and may result in more harm than good.
Vulnerable populations
In general, an enhanced duty of protection should apply to the frailest older persons with dementia but also prematurely born babies or individuals otherwise incapacitated. The notion of duty of care has always to be balanced with the best interest of the patient. Medical decisions should take into consideration evidence-based medicine and guidelines. A legal guide for practitioners in the UK gives clear indications concerning unsafe care, nutrition, and infection.249
Consent and the right to refuse treatment
Informed consent
Health care workers have an ethical and legal responsibility to obtain a patient’s IC before any procedure or treatment. However, legislation governing the conditions under which IC is required and the format it is obtained varies from country to country.250 In general, IC is of an oral nature and should be documented in the medical file. Formal IC can also be obtained in writing.251 There should be proportionality in the risk incurred and the method of IC. Before consenting, the patient has to be informed and needs to be competent to reach a decision. Competency or mental capacity is contextual and is not immediately lost after a diagnosis of dementia is made. An IC is always willingly given and without coercion, as determined in Article 6 of the Universal Declaration of Bioethics and Human Rights. Under common law, patients have the right to give or withhold consent before examinations or treatments, irrespective of the medical practitioner’s view of that decision. Capacity to provide consent is essential. The capacity of a person to understand a situation and to act reasonably must be present. The process of assessing mental capacity is important in the context of providing care for persons suffering from dementia or impaired consciousness.
Information and disclosure
The information provided should be essentially neutral, but when a choice of treatments exists, health care professionals might recommend a treatment to the patient and give the reasons for following it. Sufficient information must be given to ensure that patients are able to understand the procedure, effects and any side effects of the therapy recommended, and the effects of refusal of treatment. When written material is offered, it should be adapted to the age, mental development, and any language impairment of the patient. As a general rule, legibility of printed information should be at the level of a 16-year-old. Patients can decide at any time to accept or refuse a particular treatment or to withdraw the consent. The consequences of refusing treatment should also be made clear.
Proxy consent
In persons with dementia, autonomy in understanding and making a decision about medical recommendations or treatments is lost. This loss of autonomy or competence in the ability to consent makes the patient’s management with respect to his/her self-determination more difficult.252 Consent to a treatment for a patient without mental capacity requires nomination of a legal substitute. Making decisions on terminal care is likely to cause psychosocial stress to close relatives. Health care workers have to be cautious in imposing the burden of important decisions with regard to end of life on next of kin and should make an effort to share responsibilities.
Advance directives and refusal of treatment
Advance care planning is a dialogue between patients and their health care providers on their future care. Advance directives allow autonomous decisions to be taken by patients for their own future in the case they become incapable of making that decision later on. The right of competent adults to reject medical therapy, even if that rejection may result in their death, is well established in law. Management of refusals of treatment raises ethical concerns regarding informed refusal, patients’ mental and legal capacity to make their decisions, and whether refusals may be overridden by parental or other authority or courts of law.253 A valid and applicable advance refusal of treatment has the same effect as a refusal of treatment by a patient who has the ability to take the decision. Health care workers can be faced with a conflict of values when an intervention such as tube feeding is expected to be of short duration and advance directives were not intended to deny acute interventions with a reasonably good prognosis. It is broadly recognized that there is no intrinsic moral difference between withholding and withdrawing treatment.
In general, the Roman Catholic Church is in favor of advance directives as long as they do not contradict Church teachings. If a person, in order not to prolong a patient’s suffering, carries out an advance directive which indicates the patient does not want tube feeding and hydration if ever in a state of post-coma unresponsiveness, no member of the Catholic Church would consider this wrong.
Consent for nasogastric or percutaneous gastric tube feeding
IC should be obtained before nasogastric or percutaneous (PEG) tube feeding is commenced. Patients should be offered alternatives, such as continued and adapted oral feeding, if well informed of the risks involved. Many older patients will refuse tube feeding if alternatives are discussed. In the event of emergency or incapacity of patients, and in the absence of advance directives, health care workers will have to decide autonomously. Deferred consent will often be provided by a legal representative or family member.254 A legal representative may also ask to stop tube feeding if this is no longer in the interest of the patient or if not in line with values and beliefs of the patient.
Swallowing disorders make health care workers face ethical, moral, and legal dilemmas. Patients’ autonomy should be enhanced through provision of information and shared decision making of diagnostic procedures and artificial nutrition and hydration by means of nasogastric or percutaneous gastrostomy tube. IC is only valid if obtained from a competent patient or legal representative.
Ethical issues
There are several ethical and moral issues involved in the management of dysphagia. Indeed, nutrition is a basic human right that simply cannot be denied. The human right to food is stated in the Universal Declaration of Human Rights,255 Article 25, which states, “Everyone has the right to a standard of living adequate for the health and well-being of himself and his family, including food”. Adequate nutrition provides sufficient calories and essential nutrients necessary to support human life and health. The World Food Programme estimates that >800 million people are barred from adequate food intake. In some African and Asian countries, starvation is an important determinant of child mortality and life expectancy in general. In conditions of disease or rehabilitation, calorie and protein intake has to be increased. An insufficient diet will have a deleterious impact on health outcomes resulting in increased stress, impaired wound healing, and loss of rehabilitation potential. MN in patients admitted to hospital is associated with increased morbidity and mortality.256
The culture of food preparation and eating and the communal aspect involved is an important part of our daily life. A person’s experience and culture help to mold the nutritional and eating activity, from the vegetable garden to cleaning up after a meal. Taking meals together increases family enjoyment and strengthens bonds.257 Some authors have even claimed that communal feeding has an intrinsic moral value. Oral feeding also has a libidinous dimension: Freud assumed that a child experiences pleasure in connection with erogenous zones such as mouth and anus by the process of feeding and defecation.258 The pleasure of delicious smells, inviting plate presentation, and food taste together with a chance to socialize with family and friends contribute to the holistic experience of oral feeding.
In health care, MN is a major problem in geriatric wards and nursing homes.259 Estimates of MN in hospitals are in the range of 35% depending on the population studied.256 MN results in prolonged hospitalization, higher readmissions rates, increased health care resource consumption, and higher risk of mortality. Feeding difficulties can result from loss of appetite, generalized weakness, swallowing disorders, and decreased gastrointestinal motility. People tend to lose interest in intake of fluids and food, especially at the end of life, and cachexia and dehydration are common causes of death. A recent European Council resolution has recognized the association between dysphagia and MN and recommends improving diagnosis and treatment of MN in OD patients.126
Conditions with impairment of oral nutrition
Swallowing disorders are the consequence of structural or motor abnormalities. Structural disorders include deformities of the mouth and pharynx, diverticula, and stenosis caused by intrinsic and extrinsic processes. Motor disorders include paresis, sphincteric dysfunction, and other disorders. In addition, loss of interest in eating and cachexia due to cancer and other disorders can also result in poor oral nutrition. Reduced fluid and food intake can be favored by the development of dementia due to a reduced recognition of thirst and hunger, poor smell and taste perception, deglutition difficulties, incapacity to distinguish and properly use eating utensils, physical control loss, and depression.
Ethical principles as applied to swallowing disorders
Four principles characterize the majority of ethical decisions in clinical practice: beneficence (Latin: benefacere), nonmaleficence (Latin: non malefacere or non nocere), respect for patient autonomy, and justice.260 Beneficence refers to the clinician’s obligation to act in the patient’s interests, while nonmaleficence refers to the obligation to prevent or do no damage. In the treatment of swallowing disorders, this would result in offering the patient effective treatment for dysphagia. On the other hand, when outcomes are uncertain and harm is likely to be caused, abstention of treatment is justifiable on both moral and ethical grounds. Respect for the patients’ autonomy refers to the obligation to respect patients, their health care-associated values, preferences, and goals, and their rights of self-determination. Respect for the patient’s autonomy confers a duty to support the patient’s decision-making capacity. In addition, patients can refuse treatment or ask for it to be removed whether or not they are at the end of life, irrespective of whether the treatment would extend their life. Patients must be treated evenly and fairly, without discrimination on the basis of social status, race, ethnicity, or religious belief. In practice, health care workers have to develop sensitivity for diversity of opinion.
To treat or not to treat?
The major ethical issues revolve around who should be treated, when, and how? The simple answer is that there is no answer. In order to develop a treatment plan, two major factors should be taken into account, one being the individual values and expectations of the patient, and the second, the cost-benefit (pain, discomfort, and distress vs recovery, nutrition, well-being, and QoL). It is frequently difficult to predict the long-term outcome, while discomfort and complications are immediately evident. Furthermore, what might be a favorable outcome for one person might not be acceptable for another. A percutaneous gastrostomy (PEG) may be a burden for one person and his/her family, a comfort for another.
The greatest dilemmas frequently occur in those people where the outcome is the most uncertain. Should enteral feeding be provided or not? Can it be tried and then removed? Is it a medical treatment or an inalienable right?
By common law, enteral feeding is a medical treatment, and as such, it can be prescribed, started, and subsequently stopped.261 Often, it is easier to never start than to provide a glimmer of hope to a family, only to remove those hopes soon after. If enteral feeding (nasogastric feeding) is to be attempted, the decision needs to be made clear at the beginning of treatment about the length of time the trial will continue for, the outcome that is being sought/measured, and how it is to be assessed.
When coming to a decision, communication is key. Communication starts between members of the multidisciplinary team, then communication with the family, and if possible, communication with the patient. Once the decision is made, it is just as important to communicate that decision; otherwise, there will be confusion, blame, and possible harm to the patient. It must be remembered that no one dies in 24–48 hours because of lack of food or liquid.
There are two other major ethical dilemmas: one, the patient who can swallow but refuses to eat, and the other, the patient who is at risk when he/she swallows but insists on eating an unmodified diet or refuses to use any techniques to increase the safety of the swallow.
It has to be remembered that the patient has the right to refuse treatment and not to eat or to eat when advised otherwise or decide what course of treatment is best.262 To be able to make such decisions, it is essential that health staff and family are clear regarding the patient’s capacity to make the decision.
Assessment of the patients’ mental capacity may be required to ensure that they have the capacity to make a decision of this magnitude. There may need to be the involvement of an independent advocate, particularly when there is no legal representative to make decisions regarding health care matters.
Sometimes, the decisions people come to are hard to accept, but if patients’ autonomy and the right to refuse are accepted and they have the capacity to make decisions, health staff, carers, and family have to accept them.
However, if capacity to make a major decision is impaired due to illness (dementia, depression, sepsis, conscious level), what should be done if there is a refusal to eat? Force feeding may constitute assault; restraint needs to be carefully considered in any shape or form. Is it safe to use a securing device with an NGT? Can “boxing gloves” or web spacers be applied to prevent NGTs being pulled out? What are the aims? Often in nonreversible situations, all that happens is that the final decision is postponed and not changed. The difficulty in those who can but will not eat is that the ultimate outcome is death.
Continued hazardous oral feeding
Patients who are deemed to swallow unsafely but have mental capacity should be encouraged to follow medical advice but should also be allowed to eat. A proportion will have no ill effects from this approach. Those who do not have capacity and eat when carers are not looking are more difficult, especially if they refuse modified diets because of texture or presentation or taste. All that can be done in this situation is to remove food from their reach, to ensure that eating and hence swallowing is undertaken in as safe an environment as possible.
Terminal dehydration
The final ethical dilemma is the role of nutrition and hydration in end-of-life care. The major decision in this scenario is determining what the role of parenteral fluids and nutrition is, what gains there are to be had, and what the benefit to the patient is compared with the pain and distress of tube feeding.254 A study has shown that most patients do not become significantly thirsty when artificial hydration is withdrawn, and if they do, this situation can be remedied with simple topical measures.263
Conclusion and need for research
The white paper “Oropharyngeal dysphagia as a geriatric syndrome” has been developed by the Dysphagia Working Group, a committee formed by five members from the ESSD and five members from the European Union Geriatric Medicine Society, plus three invited experts. The document consists of 12 sections that were written and revised by the committee and covers all aspects of OD related to geriatric medicine: diagnosis, prevalence, physiopathology, complications, management, treatment, and legal and ethical issues. The document has been approved by the boards of the two societies. This last section summarizes the main aspects of each part of the document.
Swallowing is a complex process essential for life. Not only is it essential for existence, but it also plays an important role in happiness and socialization. With increasing age, changes in the swallowing process begin to manifest themselves. Some of these changes are subtle, leading to changes in the consistency, volume, and speed that food is eaten. OD refers to difficulty or discomfort during the progression of the alimentary bolus from the mouth to the esophagus and is included in the ICD-10 R13 and International Classification of Functioning, Disability and Health code B5105 of the World Health Organization. It is very prevalent among older patients because of aging itself, coexistent medical problems, neurological diseases and NDDs (stroke, PD, AD, all forms of dementia), non-neurological diseases (heart failure, rheumatoid arthritis, etc), and frailty and sarcopenia. Its prevalence goes from 23% in independently living older people, to 51% in institutionalized patients to as high as 84% in patients with AD or other forms of dementia (Table 1). This prevalence increases with disease burden and is very common in long-stay institutions. Frail adults may have a “safe” swallow that becomes unsafe when their homeostasis is perturbed, either by illness or by medication changes. In addition, OD can cause severe complications such as MN, dehydration, respiratory infections, AP, and increased readmissions, institutionalization, and morbimortality. Despite its prevalence and severity, it is still underdiagnosed and untreated in many medical centers and suffers from a lack of a universal framework to ensure that there is a consistency of terminology around diagnosis and treatment/management. Moreover, diagnosis and treatment of OD are not standardized, and consensus documents like the present one are of great value in establishing procedures to treat patients with that disorder.
There is no universal standard tool for screening or clinical assessment of OD. Most recognized tools have similar items, the commonest of which are cough, altered voice, and a slow swallow. Consensus should be reached in order to standardize clinical diagnosis process. Moreover, OD needs to be documented in medical records, to raise its profile and encourage research. Further investigation and assessment of OD is dependent on available resources but should include VFS or FEES. More work needs to be undertaken on the utility of these assessments. Should they be undertaken routinely or only when clinically indicated?
When someone is unable to swallow or is unable to support his/her nutritional needs, nutritional support is required. This support is important to maintain independence and avoid unnecessary hospital admissions. Although studies have provided some answers to questions of feeding, many other questions remain unanswered. What are the best viscosities for fluids and consistencies for solids for these patients? When is the optimum time to commence enteral feeding? How early should a percutaneous tube be placed? Where water intake is a problem, should we use other ways of administration? Should we explore different ways such as subcutaneous fluid intake (hypodermoclysis) or rectal feeding? How should OD be managed in advanced dementia?
Current treatment of OD is usually compensatory, rehabilitative, or a combination of the two. Many of these simple therapies (viscosities, chin tuck against resistance, Shaker maneuver, etc) have been proved to be effective but are not standardized, and as a consequence, it is not possible to indicate the optimal length of time or how a particular intervention will benefit individuals. Actually, minimal-massive interventions like the integration of these classical treatments with simple strategies like screening and treatment of MN and oral hygiene to reduce bacterial colonization of the oral cavity are helping to reduce or avoid major complications of OD, but larger randomized clinical trials should be undertaken. In addition, treatments that stimulate recovery of swallow and function are under research, and there are several publications with positive results and a good level of evidence (NEMS, pharmacological treatments with stimulants like TRPV1 receptor agonists, rTMS, etc).
OD is frequently a terminal phase in many neurological conditions but also in the dying patient. The presence of OD will often result in distress for family members rather than the patient themselves. The section on nutritional support and feeding, and the ethical and legal issues has provided a good summary of the present understanding. Simply to say, if there is no benefit accruing to the patient, then it is unethical to provide intervention. Research in this area is difficult but needs to be undertaken. More innovative and imaginative approaches may be required to provide answers to these vexed issues.
Throughout the document, OD has been proposed as a geriatric syndrome because it is a highly prevalent clinical condition in old age, multifactorial, associated with multiple comorbidities and bad prognosis, and is only treatable when a multidimensional approach is used. This white paper has reviewed the case and found that OD fulfills the criteria to be recognized as a geriatric syndrome. We feel that dysphagia in older people is a forgotten “geriatric giant” and fulfills all the criteria to be considered a syndrome, as are falls and confusion. OD should be given more importance and attention and thus be included in all standard screening protocols, treated, and regularly monitored to prevent its main complications. Interventions aimed at reducing the contributing factors will result in a reduction in the incidence and severity of OD in this population at risk. We need more studies, clinical trials, HE studies, clinical evidence, and clear guidelines to manage this condition, and this is one of the challenging missions for our societies.
Acknowledgment
The authors would like to thank Mrs Jane Lewis for English revision.
Disclosure
The authors report no conflicts of interest in this work.
References
Nascher IL. Geriatrics. The Diseases of Old Age and Their Treatment. Philadelphia: University of California Libraries; 1914. | ||
Cruz-Jentoft AJ, Michel JP. Sarcopenia: a useful paradigm for physical frailty. Eur Geriatr Med. 2013;4(2):102–105. | ||
Ahmed N, Mandel R, Fain MJ. Frailty: an emerging geriatric syndrome. Am J Med. 2007;120(9):748–753. | ||
Wharsaw GA. Which patients benefit the most from a geriatrician’s care? Consensus among directors of geriatrics academic programs. J Am Geriatr Soc. 2008;56(10):1796–1801. | ||
Reuben DB. Geriatrics syndromes. In: Beck AC, editor. Geriatrics Review Syllabus. 2nd ed. New York: American Geriatrics Society; 1991:117–231. | ||
Olde-Rikkert MG, Rigaud AS, van Hoeyweghen RJ, de Graff J. Geriatric syndromes: medical misnomer or progress in geriatrics? Neth J Med. 2003;61:83–87. | ||
Inouye SK, Studenski S, Tinetti ME, Kuchel GA. Geriatric syndromes: clinical, research, and policy implications of a core geriatric concept. J Am Geriatr Soc. 2007;55(5):780–791. | ||
Flacker JM. What is a geriatric syndrome anyway? J Am Geriatr Soc. 2003;51(4):574–576. | ||
Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis. Age Ageing. 2010;39(4): 412–423. | ||
Cook IJ, Kahrilas PJ. AGA technical review on management of oropharyngeal dysphagia. Gastroenterology. 1999;116(2):455–478. | ||
World Health Organization. International Classification of Diseases (ICD). Geneva: World Health Organization; 2010. | ||
Rofes L, Arreola V, Almirall J, et al. Diagnosis and management of oropharyngeal dysphagia and its nutritional and respiratory complications in the elderly. Gastroenterol Res Pract. 2011;2011:818979. | ||
Lin LC, Wu SC, Chen HS, Wang TG, Chen MY. Prevalence of impaired swallowing in institutionalized older people in Taiwan. J Am Geriatr Soc. 2002;50(6):1118–1123. | ||
Logemann JA. Evaluation and Treatment of Swallowing Disorders. Austin, TX: College-Hill Press; 1983. | ||
Clave P, Rofes L, Carrión S, et al. Pathophysiology, relevance and natural history of oropharyngeal dysphagia among older people. Nestle Nutr Inst Workshop Ser. 2012;72:57–66. | ||
Cabre M, Serra-Prat M, Palomera E, Almirall J, Pallares R, Clave P. Prevalence and prognostic implications of dysphagia in elderly patients with pneumonia. Age Ageing. 2010;39(1):39–45. | ||
Serra-Prat M, Hinojosa G, Lopez D, et al. Prevalence of oropharyngeal dysphagia and impaired safety and efficacy of swallow in independently living older persons. J Am Geriatr Soc. 2011;59(1):186–187. | ||
Carrion S, Cabre M, Monteis R, et al. Oropharyngeal dysphagia is a prevalent risk factor for malnutrition in a cohort of older patients admitted with an acute disease to a general hospital. Clin Nutr. 2015;34(3):436–442. | ||
Mann G, Hankey GJ, Cameron D. Swallowing disorders following acute stroke: prevalence and diagnostic accuracy. Cerebrovasc Dis. 2000;10(5):380–386. | ||
Kikawada M, Iwamoto T, Takasaki M. Aspiration and infection in the elderly – epidemiology, diagnosis and management. Drugs Aging. 2005;22(2):115–130. | ||
Mitchel S, Teno JM, Kiely DK, et al. The clinical course of advanced dementia. N Engl J Med. 2009;361:1529–1538. | ||
Robbins J. Old swallowing and dysphagia: thoughts on intervention and prevention. Nutr Clin Pract. 1999;14(5):21–26. | ||
Robbins J. Normal swallowing and aging. Semin Neurol. 1996;16(4):309–317. | ||
Cabre M, Serra-Prat M, Force LL, Almirall J, Palomera E, Clave P. Oropharyngeal dysphagia is a risk factor for readmission for pneumonia in the very elderly persons: observational prospective study. J Gerontol A Biol Sci Med Sci. 2014;69(3):330–337. | ||
Serra-Prat M, Palomera M, Gomez C, et al. Oropharyngeal dysphagia as a risk factor for malnutrition and lower respiratory tract infection in independently living older persons: a population-based prospective study. Age Ageing. 2012;41(3):376–381. | ||
Puisieux F, d’Andrea C, Baconnier P, et al. Troubles de la déglutition du sujet âgé et pneumopathies en 14 questions/réponses. [Swallowing disorders, pneumonia and respiratory tract infectious disease in the elderly]. Rev Mal Respir. 2009;26(6):587–605. French. | ||
Sura L, Madhavan A, Carnaby G, Crary MA. Dysphagia in the elderly: management and nutritional considerations. Clin Interv Aging. 2012;7:287–297. | ||
Crary MA, Groher ME. Introduction to Adult Swallowing Disorders. Philadelphia, PA: Butterworth Heinemann; 2003. | ||
Humbert IA, Robbins J. Dysphagia in the elderly. Phys Med Rehabil Clin N Am. 2008;19(4):853–866. | ||
Ney DM, Weiss JM, Kind AJH, Robbins J. Senescent swallowing: impact, strategies, and interventions. Nutr Clin Pract. 2009;24(3):395–413. | ||
Chiocca JC, Olmos JA, Salis GB, Soifer LO, Higa R, Marcolongo M. Prevalence, clinical spectrum and atypical symptoms of gastro-oesophageal reflux in Argentina: a nationwide population-based study. Aliment Pharmacol Ther. 2005;22(4):331–342. | ||
Cho YS, Choi MG, Jeong JJ, et al. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Asan-si, Korea. Am J Gastroenterol. 2005;100(4):747–753. | ||
Eslick GD, Talley NJ. Dysphagia: epidemiology, risk factors and impact on quality of life – a population-based study. Aliment Pharmacol Ther. 2008;27(10):971–979. | ||
Ruth M, Mansson I, Sandberg N. The prevalence of symptoms suggestive of esophageal disorders. Scand J Gastroenterol. 1991;26(1):73–81. | ||
Watson DI, Lally CJ. Prevalence of symptoms and use of medication for gastroesophageal reflux in an Australian community. World J Surg. 2009;33(1):88–94. | ||
Ziolkowski BA, Pacholec A, Muszynski JT. Objawy alarmowe, czynniki ryzyka wystąpienia raka przewodu pokarmowego i gotowość do udziału w endoskopowych badaniach przesiewowych. [Alarm symptoms, risk factors for digestive tract cancer and readiness to participate in an endoscopic screening program]. Prz Gastroenterol. 2013;8(2):108–114. Polish. | ||
Belafsky PC, Mouadeb DA, Rees CJ, et al. Validity and reliability of the Eating Assessment Tool (EAT-10). Ann Otol Rhinol Laryngol. 2008;117(12):919–924. | ||
Perry L. Screening swallowing function of patients with acute stroke. Part two: detailed evaluation of the tool used by nurses. J Clin Nurs. 2001;10(4):474–481. | ||
Yang EJ, Kim MH, Lim JY, Paik NJ. Oropharyngeal dysphagia in a community-based elderly cohort: the Korean longitudinal study on health and aging. J Korean Med Sci. 2013;28(10):1534–1539. | ||
Barczi SR, Robbins J. How should dysphagia care of older adults differ? Establishing optimal practice patterns. Semin Speech Lang. 2000;21(4):347–361. | ||
Cabre M, Almirall J, Clave P. Aspiration pneumonia: management in Spain. Eur Geriatr Med. 201;2(3):180–183. | ||
Bergman H, Ferrucci L, Guralnik J, et al. Frailty: an emerging research and clinical paradigm – issues and controversies. J Gerontol A Biol Sci Med Sci. 2007;62(7):731–737. | ||
Feinberg MJ, Ekberg O, Segall L, Tully J. Deglutition in elderly patients with dementia – findings of videofluorographic evaluation and impact on staging and management. Radiology. 1992;183(3):811–814. | ||
Horner J, Alberts MJ, Dawson DV, Cook GM. Swallowing in Alzheimer’s disease. Alzheimer Dis Assoc Disord. 1994;8(3):177–189. | ||
Affoo RH, Foley N, Rosenbek J, Shoemaker JK, Martin RE. Swallowing dysfunction and autonomic nervous system dysfunction in Alzheimer’s disease: a scoping review of the evidence. J Am Geriatr Soc. 2013;61(12):2203–2213. | ||
Logemann JA, Gensler G, Robbins J, et al. A randomized study of three interventions for aspiration of thin liquids in patients with dementia or Parkinson’s disease. J Speech Lang Hear Res. 2008;51(1):173–183. | ||
Ikeda M, Brown J, Holland AJ, Fukuhara R, Hodges JR. Changes in appetite, food preference, and eating habits in frontotemporal dementia and Alzheimer’s disease. J Neurol Neurosurg Psychiatry. 2002;73(4):371–376. | ||
Rosler A, Pfeil S, Lessmann H, Hoder J, Befahr A, von Renteln-Kruse W. Dysphagia in dementia: influence of dementia severity and food texture on the prevalence of aspiration and latency to swallow in hospitalized geriatric patients. J Am Med Dir Assoc. 2015;16(8):697–701. | ||
Miller N, Allcock L, Hildreth AJ, Jones D, Noble E, Burn DJ. Swallowing problems in Parkinson disease: frequency and clinical correlates. J Neurol Neurosurg Psychiatry. 2009;80(9):1047–1049. | ||
Walker RW, Dunn JR, Gray WK. Self-reported dysphagia and its correlates within a prevalent population of people with Parkinson’s disease. Dysphagia. 2011;26(1):92–96. | ||
Kalf JG, de Swart BJM, Bloem BR, Munneke M. Prevalence of oropharyngeal dysphagia in Parkinson’s disease: a meta-analysis. Parkinsonism Relat Disord. 2012;18(4):311–315. | ||
Perez-Lloret S, Negre-Pages L, Ojero-Senard A, et al. Oro-buccal symptoms (dysphagia, dysarthria, and sialorrhea) in patients with Parkinson’s disease: preliminary analysis from the French COPARK cohort. Eur J Neurol. 2012;19(1):28–37. | ||
Smithard DG, Oneill PA, England RE, et al. The natural history of dysphagia following a stroke. Dysphagia. 1997;12(4):188–193. | ||
Martino R, Foley N, Bhogal S, Diamant N, Speechley M, Teasell R. Dysphagia after stroke – incidence, diagnosis, and pulmonary complications. Stroke. 2005;36(12):2756–2763. | ||
Flowers HL, Silver FL, Fang JM, Rochon E, Martino R. The incidence, co-occurrence, and predictors of dysphagia, dysarthria, and aphasia after first-ever acute ischemic stroke. J Commun Disord. 2013;46(3):238–248. | ||
Clave P, Shaker R. Dysphagia: current reality and scope of the problem. Nat Rev Gastroenterol Hepatol. 2015;12(5):259–270. | ||
Holland G, Jayasekeran V, Pendleton N, Horan M, Jones M, Hamdy S. Prevalence and symptom profiling of oropharyngeal dysphagia in a community dwelling of an elderly population: a self-reporting questionnaire survey. Dis Esophagus. 2011;24(7):476–480. | ||
Roy N, Stemple J, Merrill RM, Thomas L. Dysphagia in the elderly: preliminary evidence of prevalence, risk factors, and socioemotional effects. Ann Otol Rhinol Laryngol. 2007;116(11):858–865. | ||
Bloem BR, Lagaay AM, Vanbeek W, Haan J, Roos RAC, Wintzen AR. Prevalence of subjective dysphagia in community residents aged over 87. BMJ. 1990;300(6726):721–722. | ||
Kawashima K, Motohashi Y, Fujishima I. Prevalence of dysphagia among community-dwelling elderly individuals as estimated using a questionnaire for dysphagia screening. Dysphagia. 2004;19(4): 266–271. | ||
Lee A, Sitoh YY, Lieu PK, Phua SY, Chin JJ. Swallowing impairment and feeding dependency in the hospitalised elderly. Ann Acad Med Singapore. 1999;28:371–376. | ||
Almirall J, Rofes L, Serra-Prat M, et al. Oropharyngeal dysphagia is a risk factor for community-acquired pneumonia in the elderly. Eur Respir J. 2013;41(4):923–928. | ||
Nogueira D, Reis E. Swallowing disorders in nursing home residents: how can the problem be explained? Clin Interv Aging. 2013;8:221–227. | ||
Langmore SE, Olney RK, Lomen-Hoerth C, Miller BL. Dysphagia in patients with frontotemporal lobar dementia. Arch Neurol. 2007;64(1):58–62. | ||
Suh MK, Kim HH, Na DL. Dysphagia in patients with dementia Alzheimer versus vascular. Alzheimer Dis Assoc Disord. 2009;23(2):178–184. | ||
De Pauw A, Dejaeger E, D’hooghe B, Carton H. Dysphagia in multiple sclerosis. Clin Neurol Neurosurg. 2002;104(4):345–351. | ||
Calcagno P, Ruoppolo G, Grasso MG, De Vincentiis M, Paolucci S. Dysphagia in multiple sclerosis – prevalence and prognostic factors. Acta Neurol Scand. 2002;105(1):40–43. | ||
Chen A, Garrett CG. Otolaryngologic presentations of amyotrophic lateral sclerosis. Otolaringol Head Neck Surg. 2005;132(3):500–504. | ||
Ruoppolo G, Schettino I, Frasca V, et al. Dysphagia in amyotrophic lateral sclerosis: prevalence and clinical findings. Acta Neurol Scand. 2013;128(6):397–401. | ||
Jean A. Brain stem control of swallowing: neuronal network and cellular mechanisms. Physiol Rev. 2001;81(2):929–969. | ||
Kahrilas PJ, Lin SZ, Chen J, Logemann JA. Oropharyngeal accommodation to swallow volume. Gastroenterology. 1996;111(2):297–306. | ||
Suzuki M, Asada Y, Ito J, Hayashi K, Inoue H, Kitano H. Activation of cerebellum and basal ganglia on volitional swallowing detected by functional magnetic resonance imaging. Dysphagia. 2003;18(2):71–77. | ||
Daniels SK, Brailey K, Foundas AL. Lingual discoordination and dysphagia following acute stroke: analyses of lesion localization. Dysphagia. 1999;14(2):85–92. | ||
Schindler JS, Kelly JH. State of the art review: swallowing disorders in the elderly. Laryngoscope. 2002;112(4):589–602. | ||
Humbert IA, Fitzgerald ME, McLaren DG, et al. Neurophysiology of swallowing: effects of age and bolus type. Neuroimage. 2009;44(3):982–991. | ||
Martin R, Barr A, MacIntosh B, et al. Cerebral cortical processing of swallowing in older adults. Exp Brain Res. 2007;176(1):12–22. | ||
Teismann IK, Steinstraeter O, Schwindt W, Ringelstein EB, Pantev C, Dziewas R. Age-related changes in cortical swallowing processing. Neurobiol Aging. 2010;31(6):1044–1050. | ||
Mendell DA, Logemann JA. Temporal sequence of swallow events during the oropharyngeal swallow. J Speech Lang Hear Res. 2007;50(5):1256–1271. | ||
Shaw DW, Cook IJ, Gabb M, et al. Influence of normal aging on oral-pharyngeal and upper esophageal sphincter function during swallowing. Am J Physiol. 1995;268(3 Pt 1):G389–G396. | ||
Butler SG, Stuart A, Leng XY, Rees C, Williamson J, Kritchevsky SB. Factors influencing aspiration during swallowing in healthy older adults. Laryngoscope. 2010;120(11):2147–2152. | ||
Nicosia MA, Hind JA, Roecker EB, et al. Age effects on the temporal evolution of isometric and swallowing pressure. J Gerontol A Biol Sci Med Sci. 2000;55(11):M634–M640. | ||
Rofes L, Arreola V, Romea M, et al. Pathophysiology of oropharyngeal dysphagia in the frail elderly. Neurogastroenterol Motil. 2010;22(8):851–858. | ||
Clave P, Terre R, De Kraa M, Serra M. Approaching oropharyngeal dysphagia. Rev Esp Enferm Dig. 2004;96(2):119–126. | ||
Garcia-Peris P, Paron L, Velasco C, et al. Long-term prevalence of oropharyngeal dysphagia in head and neck cancer patients: impact on quality of life. Clin Nutr. 2007;26(6):710–717. | ||
Cook IJ. Oropharyngeal dysphagia. Gastroenterol Clin North Am. 2009;38(3):411–431. | ||
Turley R, Cohen S. Impact of voice and swallowing problems in the elderly. Otolaryngol Head Neck Surg. 2009;140(1):33–36. | ||
Wieseke A, Bantz D, Siktberg L, Dillard N. Assessment and early diagnosis of dysphagia. Geriatr Nurs. 2008;29(6):376–383. | ||
Clave P, Verdaguer A, Arreola V. Disfagia orofaríngea en el anciano. [Oral-pharyngeal dysphagia in the elderly]. Med Clin (Barc). 2005; 124(19):742–748. Spanish. | ||
Nagaya M, Sumi Y. Reaction time in the submental muscles of normal older people. J Am Geriatr Soc. 2002;50(5):975–976. | ||
Clave P, De Kraa M, Arreola V, et al. The effect of bolus viscosity on swallowing function in neurogenic dysphagia. Aliment Pharmacol Ther. 2006;24(9):1385–1394. | ||
Kahrilas PJ, Lin S, Rademaker AW, Logeman JA. Impaired deglutitive airway protection: a videofluoroscopic analysis of severity and mechanism. Gastroenterology. 1997;113:1457–1464. | ||
Teismann IK, Steinstraeter O, Stoeckigt K, et al. Functional oropharyngeal sensory disruption interferes with the cortical control of swallowing. BMC Neurosci. 2007;8:62. | ||
Teismann IK, Steinstrater O, Warnecke T, et al. Tactile thermal oral stimulation increases the cortical representation of swallowing. BMC Neurosci. 2009;10:71. | ||
Stuck AE, Siu AL, Wieland GD, Adams J, Rubenstein LZ. Comprehensive geriatric assessment – a metaanalysis of controlled trials. Lancet. 1993;342(8878):1032–1036. | ||
Kertscher B, Speyer R, Palmieri M, Plant C. Bedside screening to detect oropharyngeal dysphagia in patients with neurological disorders: an updated systematic review. Dysphagia. 2014;29(2):204–212. | ||
Rofes L, Arreola V, Mukherjee R, Clave P. Sensitivity and specificity of the Eating Assessment Tool and the Volume-Viscosity Swallow Test for clinical evaluation of oropharyngeal dysphagia. Neurogastroenterol Motil. 2014;26(9):1256–1265. | ||
Wallace AL, Middleton S, Cook IJ. Development and validation of a self-report symptom inventory to assess the severity of oral-pharyngeal dysphagia. Gastroenterology. 2000;118(4):678–687. | ||
Cohen JT, Manor Y. Swallowing disturbance questionnaire for detecting dysphagia. Laryngoscope. 2011;121(7):1383–1387. | ||
Wilkinson AH, Burns SL, Witham MD. Aspiration in older patients without stroke: a systematic review of bedside diagnostic tests and predictors of pneumonia. Eur Geriatr Med. 2012;3(3):145–152. | ||
DePippo KL, Holas MA, Reding MJ. Validation of the 3-oz water swallow test for aspiration following stroke. Arch Neurol. 1992;49(12):1259–1261. | ||
Nathadwarawala KM, Nicklin J, Wiles CM. A timed test of swallowing capacity for neurological patients. J Neurol Neurosurg Psychiatry. 1992;55(9):822–825. | ||
Smithard DG, O’Neill PA, Park C, et al. Can bedside assessment reliably exclude aspiration following acute stroke? Age Ageing. 1998;27(2):99–106. | ||
Westergren A. Detection of eating difficulties after stroke: a systematic review. Int Nurs Rev. 2006;53(2):143–149. | ||
Bours GJ, Speyer R, Lemmens J, Limburg M, de Wit R. Bedside screening tests vs videofluoroscopy or fibreoptic endoscopic evaluation of swallowing to detect dysphagia in patients with neurological disorders: systematic review. J Adv Nurs. 2009;65(3):477–493. | ||
Clave P, Arreola V, Romea M, Medina L, Palornera E, Serra-Prat M. Accuracy of the volume-viscosity swallow test for clinical screening of oropharyngeal dysphagia and aspiration. Clin Nutr. 2008;27(6):806–815. | ||
Martino R, Silver F, Teasell R, et al. The Toronto Bedside Swallowing Screening Test (TOR-BSST): development and validation of a dysphagia screening tool for patients with stroke. Stroke. 2009;40(2):555–561. | ||
Martino R, Maki E, Diamant N. Identification of dysphagia using the Toronto Bedside Swallowing Screening Test (TOR-BSST ©): are 10 teaspoons of water necessary? Int J Speech Lang Pathol. 2014;16(3):193–198. | ||
Rosenbek JC, Robbins JA, Roecker EB, Coyle JL, Wood JL. A penetration aspiration scale. Dysphagia. 1996;11(2):93–98. | ||
American Speech-Language-Hearing Association. Clinical indicators for instrumental assessment of dysphagia. 2000. Available from: http://www.asha.org/policy/GL2000-00047.htm. Accessed March 18, 2016. | ||
Logemann JA. Evaluation and Treatment of Swallowing Disorders. Austin, TX: Pro-Ed; 1998. | ||
Langmore SE. Evaluation of oropharyngeal dysphagia: which diagnostic tool is superior? Curr Opin Otolaryngol Head Neck Surg. 2003;11:485–489. | ||
American Speech-Language-Hearing Association. Guidelines for speech-language pathologists performing videofluoroscopic swallowing studies. Available from: http://www.asha.org/policy/GL2004-00050.htm. Accessed March 18, 2016. | ||
Speyer R, Baijens L, Heijnen M, Zwijnenberg I. Effects of therapy in oropharyngeal dysphagia by speech and language therapists: a systematic review. Dysphagia. 2010;25(1):40–65. | ||
Baijens L, Barikroo A, Pilz W. Intrarater and interrater reliability for measurements in videofluoroscopy of swallowing. Eur J Radiol. 2013;82(10):1683–1695. | ||
Kelly AM, Drinnan MJ, Leslie P. Assessing penetration and aspiration: how do videofluoroscopy and fiberoptic endoscopic evaluation of swallowing compare? Laryngoscope. 2007;117(10):1723–1727. | ||
European Society for Swallowing Disorders. Position statements and meeting abstracts. Uniting Europe against dysphagia, Barcelona, Spain, October 25–27, 2012. Dysphagia. 2013;28(2):280–335. | ||
Kelly AM, Leslie P, Beale T, Payten C, Drinnan MJ. Fibreoptic endoscopic evaluation of swallowing and videofluoroscopy: does examination type influence perception of pharyngeal residue severity? Clin Otolaryngol. 2006;31(5):425–432. | ||
Langmore SE, Aviv JE. Endoscopic Evaluation and Treatment of Swallowing Disorders. New York: Thieme Medical Publishers; 2001. | ||
Hind JA, Gensler G, Brandt DK, et al. Comparison of trained clinician ratings with expert ratings of aspiration on videofluoroscopic images from a randomized clinical trial. Dysphagia. 2009;24(2):211–217. | ||
Logemann JA. Manual for the Videofluoroscopic Study of Swallowing. 2nd ed. Austin, TX: Pro-Ed; 1993. | ||
Ortega O, Cabre M, Clave P. Oropharyngeal dysphagia: aetiology and effects of ageing. J Gastroenterol Hepatol Res. 2014;3(5):1049–1054. | ||
Robbins J, Langmore S, Hind JA, Erlichman M. Dysphagia research in the 21st century and beyond: proceedings from Dysphagia Experts Meeting, August 21, 2001. J Rehabil Res Dev. 2002;39(4):543–547. | ||
Robbins J, Gangnon RE, Theis SM, Kays SA, Hewitt AL, Hind JA. The effects of lingual exercise on swallowing in older adults. J Am Geriatr Soc. 2005;53(9):1483–1489. | ||
Jensen GL, Mirtallo J, Compher C, et al. Adult starvation and disease-related malnutrition: a proposal for etiology-based diagnosis in the clinical practice setting from the International Consensus Guideline Committee. Clin Nutr. 2010;29(2):151–153. | ||
Carrión S, Arreola V, Roca M, Palomera E. Study of the body composition and nutritional status of elderly patients with oropharyngeal dysphagia. Clin Nutr. 2012;7(1):172. | ||
Council of Europe Committee of Ministers. Resolution ResAP (2003) on food and nutritional care in hospitals. Strasbourg: Council of Europe; 2003 [updated March 18, 2016]. Available from: https://search.coe.int/cm/Pages/result_details.aspx?ObjectID=09000016805de833. Accessed November 17, 2013. | ||
Warren JL, Bacon WE, Harris T, Mcbean AM, Foley DJ, Phillips C. The burden and outcomes associated with dehydration among US elderly, 1991. Am J Public Health. 1994;84(8):1265–1269. | ||
Xiao H, Barber J, Campbell ES. Economic burden of dehydration among hospitalized elderly patients. Am J Health Syst Pharm. 2004;61(23):2534–2540. | ||
Stookey JD, Pieper CF, Cohen HJ. Is the prevalence of dehydration among community-dwelling older adults really low? Informing current debate over the fluid recommendation for adults aged 70+ years. Public Health Nutr. 2005;8(8):1275–1285. | ||
Vivanti AP, Campbell KL, Suter MS, Hannan-Jones MT, Hulcombe JA. Contribution of thickened drinks, food and enteral and parenteral fluids to fluid intake in hospitalised patients with dysphagia. J Hum Nutr Diet. 2009;22(2):148–155. | ||
Whelan K. Inadequate fluid intakes in dysphagic acute stroke. Clin Nutr. 2001;20(5):423–428. | ||
Stanga Z, Baldinger SH, Clave P. Dehydration and dysphagia. In: Ekberg O, editor. Dysphagia. Diagnosis and Treatment. Berlin: Springer; 2012:601–610. | ||
Wakabayashi H. Transdisciplinary approach for sarcopenia. Sarcopenic dysphagia. Clin Calcium. 2014;24(10):1509–1517. | ||
Almirall J, Cabre M, Clave P. Complications of oropharyngeal dysphagia: aspiration pneumonia. Nestle Nutr Inst Workshop Ser. 2012;72; 67–76. | ||
Ortega O, Clavé P. Oral hygiene, aspiration, and aspiration pneumonia: from pathophysiology to therapeutic strategies. Curr Phys Med Rehabil Rep. 2013;1:292–295. | ||
Teramoto S, Fukuchi Y, Sasaki H, Sato K, Sekizawa K, Matsuse T. High incidence of aspiration pneumonia in community- and hospital-acquired pneumonia in hospitalized patients: a multicenter, prospective study in Japan. J Am Geriatr Soc. 2008;56(3):577–579. | ||
Shariatzadeh MR, Huang JQ, Marrie TJ. Differences in the features of aspiration pneumonia according to site of acquisition: community or continuing care facility. J Am Geriatr Soc. 2006;54(2): 296–302. | ||
Ickenstein GW, Clave P, Dziewas R, et al. Diagnosis and Treatment of Neurogenic Dysphagia. 1st ed. Bremen: Uni-Med Verlag AG; 2011. | ||
Awano S, Ansai T, Takata Y, et al. Oral health and mortality risk from pneumonia in the elderly. J Dent Res. 2008;87(4):334–339. | ||
Marik PE, Kaplan D. Aspiration pneumonia and dysphagia in the elderly. Chest. 2003;124(1):328–336. | ||
Terpenning MS, Taylor GW, Lopatin DE, Kerr CK, Dominguez BL, Loesche WJ. Aspiration pneumonia: dental and oral risk factors in an older veteran population. J Am Geriatr Soc. 2001;49(5):557–563. | ||
Ortega O, Parra C, Zarcero S, Nart J, Sakwinska O, Clave P. Oral health in older patients with oropharyngeal dysphagia. Age Ageing. 2014;43(1):132–137. | ||
van der Maarel-Wierink CD, Vanobbergen JNO, Bronkhorst EM, Schols JMGA, de Baat C. Meta-analysis of dysphagia and aspiration pneumonia in frail elders. J Dent Res. 2011;90(12):1398–1404. | ||
Almirall J, Cabre M, Clave P. Aspiration pneumonia. Med Clin. 2007;129(11):424–432. | ||
Ekberg O, Hamdy S, Woisard V, Wuttge-Hannig A, Ortega P. Social and psychological burden of dysphagia: its impact on diagnosis and treatment. Dysphagia. 2002;17(2):139–146. | ||
Tibbling LGB. Dysphagia and its consequences in the elderly. Dysphagia. 1991;6(4):200–202. | ||
Han M, Ohnishi H, Nonaka M, et al. Relationship between dysphagia and depressive states in patients with Parkinson’s disease. Parkinsonism Relat Disord. 2011;17(6):437–449. | ||
Leow LP, Huckabee ML, Anderson T, Beckert L. The impact of dysphagia on quality of life in ageing and Parkinson’s disease as measured by the swallowing quality of life (SWAL-QOL) questionnaire. Dysphagia. 2010;25(3):216–220. | ||
Verdonschot RJCG, Baijens LWJ, Serroyen JL, Leue C, Kremer B. Symptoms of anxiety and depression assessed with the Hospital Anxiety and Depression Scale in patients with oropharyngeal dysphagia. J Psychosom Res. 2013;75(5):451–455. | ||
Hickson M, Frost G. An investigation into the relationships between quality of life, nutritional status and physical function. Clin Nutr. 2004;23(2):213–221. | ||
Nguyen NP, Frank C, Moltz CC, et al. Impact of dysphagia on quality of life after treatment of head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2005;61(3):772–778. | ||
Rofes L, Arreola V, Mukherjee R, Swanson J, Clavé P. The effects of a xanthan gum-based thickener on the swallowing function of patients with dysphagia. Aliment Pharmacol Ther. 2014;39(10):1169–1179. | ||
Bhattacharyya N, Kotz T, Shapiro J. The effect of bolus consistency on dysphagia in unilateral vocal cord paralysis. Otolaryngol Head Neck Surg. 2003;129(6):632–636. | ||
Rosenvinge SK, Starke ID. Improving care for patients with dysphagia. Age Ageing. 2005;34(6):587–593. | ||
Shim JS, Oh BM, Han TR. Factors associated with compliance with viscosity-modified diet among dysphagic patients. Ann Rehabil Med. 2013;37(5):628–632. | ||
Matta Z, Chambers E, Garcia JM, Helverson JM. Sensory characteristics of beverages prepared with commercial thickeners used for dysphagia diets. J Am Diet Assoc. 2006;106(7):1049–1054. | ||
Low J, Wyles C, Wilkinson T, Sainsbury R. The effect of compliance on clinical outcomes for patients with dysphagia on videofluoroscopy. Dysphagia. 2001;16(2):123–127. | ||
Steele CM, Alsanei WA, Ayanikalath S, et al. The influence of food texture and liquid consistency modification on swallowing physiology and function: a systematic review. Dysphagia. 2015;30(1):2–26. | ||
National Patient Safety Agency, Royal College of Speech & Language Therapists, The British Dietetic Association, National Nurses Nutrition Group, Hospital Caterers Association. Dysphagia diet food texture descriptors. 2011. | ||
Terre R, Mearin F. Effectiveness of chin-down posture to prevent tracheal aspiration in dysphagia secondary to acquired brain injury. A videofluoroscopy study. Neurogastroenterol Motil. 2012;24(5):414–419. | ||
Logemann JA. Dysphagia – evaluation and treatment. Folia Phoniatr Logop. 1995;47(3):140–164. | ||
Ortega O, Sakwinska O, Combremont S, et al. High prevalence of colonization of oral cavity by respiratory pathogens in frail older patients with oropharyngeal dysphagia. Neurogastroenterol Motil. 2015;27(12):1804–1816. | ||
van der Maarel-Wierink CD, Vanobbergen JN, Bronkhorst EM, Schols JMGA, de Baat C. Oral health care and aspiration pneumonia in frail older people: a systematic literature review. Gerodontology. 2013;30(1):3–9. | ||
Scannapieco FA, Yu J, Raghavendran K, et al. A randomized trial of chlorhexidine gluconate on oral bacterial pathogens in mechanically ventilated patients. Crit Care. 2009;13(4):R117. | ||
Sjogren P, Nilsson E, Forsell M, Johansson O, Hoogstraate J. A systematic review of the preventive effect of oral hygiene on pneumonia and respiratory tract infection in elderly people in hospitals and nursing homes: effect estimates and methodological quality of randomized controlled trials. J Am Geriatr Soc. 2008;56(11):2124–2130. | ||
Loe H, Theilade E, Jensen SB. Experimental gingivitis in man. J Periodontol. 1965;36(3):177–187. | ||
Page RC, Schroeder HE. Pathogenesis of inflammatory periodontal-disease – summary of current work. Lab Invest. 1976;34(3):235–249. | ||
Berchier CE, Slot DE, Van der Weijden GA. The efficacy of 0.12% chlorhexidine mouthrinse compared with 0.2% on plaque accumulation and periodontal parameters: a systematic review. J Clin Periodontol. 2010;37(9):829–839. | ||
Strydonck DAC, Slot DE, Van der Velden U, Van der Weijden F. Effect of a chlorhexidine mouthrinse on plaque, gingival inflammation and staining in gingivitis patients: a systematic review. J Clin Periodontol. 2012;39(11):1042–1055. | ||
Stoeken JE, Paraskevas S, Van der Weijden GA. The long-term effect of a mouthrinse containing essential oils on dental plaque and gingivitis: a systematic review. J Periodontol. 2007;78(7):1218–1228. | ||
Van Leeuwen MPC, Slot DE, Van der Weijden GA. Essential oils compared to chlorhexidine with respect to plaque and parameters of gingival inflammation: a systematic review. J Periodontol. 2011;82(2):174–194. | ||
Schindler A, Vincon E, Grosso E, Miletto AM, Rosa R, Schindler O. Rehabilitative management of oroopharyngeal dysphagia in acute care settings: data from a large Italian teaching hospital. Dysphagia. 2008;23(3):230–236. | ||
Robbins J, Levine R, Wood J, Roecker EB, Luschei E. Age effects on lingual pressure generation as a risk factor for dysphagia. J Gerontol A Biol Sci Med Sci. 1995;50(5):M257–M262. | ||
Todd JT, Lintzenich CR, Butler SG. Isometric and swallowing tongue strength in healthy adults. Laryngoscope. 2013;123(10):2469–2473. | ||
Schindler O, Ruoppolo A, Schindler A. Deglutologia. 2nd ed. Torino: Omega; 2011:947–957. | ||
Shaker R, Easterling C, Kern M, et al. Rehabilitation of swallowing by exercise in tube-fed patients with pharyngeal dysphagia secondary to abnormal UES opening. Gastroenterology. 2002;122(5):1314–1321. | ||
Shaw DW, Cook IJ, Jamieson GG, Gabb M, Simula ME, Dent J. Influence of surgery on deglutitive upper oesophageal sphincter mechanics in Zenker’s diverticulum. Gut. 1996;38(6):806–811. | ||
Ravich WJ. Botulinum toxin for UES dysfunction: therapy or poison? Dysphagia. 2001;16(3):168–170. | ||
Clave P, Arreola V, Velasco M, et al. Diagnóstico y tratamiento de la disfagia orofaríngea funcional. Aspectos de interés para el cirujano digestivo. [Diagnosis and treatment of functional oropharyngeal dysphagia. Features of interest to the digestive surgeon]. Cir Esp. 2007;82(2):62–76. Spanish. | ||
Knol W, Van Marum RJ, Jansen PAF, Souverein PC, Schobben AFAM, Egberts ACG. Antipsychotic drug use and risk of pneumonia in elderly people. J Am Geriatr Soc. 2008;56(4):661–666. | ||
Dziewas R, Warnecke T, Schnabel M, et al. Neuroleptic-induced dysphagia: case report and literature review. Dysphagia. 2007;22(1):63–67. | ||
Sokoloff LG, Pavlakovic R. Neuroleptic-induced dysphagia. Dysphagia. 1997;12(4):177–179. | ||
Loeb MB, Becker M, Eady A, Walker-Dilks C. Interventions to prevent aspiration pneumonia in older adults: a systematic review. J Am Geriatr Soc. 2003;51(7):1018–1022. | ||
Ebihara T, Sekizawa K, Nakazawa H, Sasaki H. Capsaicin and swallowing reflex. Lancet. 1993;341(8842):432. | ||
Ebihara T, Takahashi H, Ebihara S, et al. Capsaicin troche for swallowing dysfunction in older people. J Am Geriatr Soc. 2005;53(5):824–828. | ||
Ebihara T, Ebihara S, Maruyama M, et al. A randomized trial of olfactory stimulation using black pepper oil in older people with swallowing dysfunction. J Am Geriatr Soc. 2006;54(9):1401–1406. | ||
Ebihara T, Ebihara S, Yamazaki M, Asada M, Yamanda S, Arai H. Intensive stepwise method for oral intake using a combination of transient receptor potential stimulation and olfactory stimulation inhibits the incidence of pneumonia in dysphagic older adults. J Am Geriatr Soc. 2010;58(1):196–198. | ||
Rofes L, Arreola V, Martin A, Clave P. Natural capsaicinoids improve swallow response in older patients with oropharyngeal dysphagia. Gut. 2013;62(9):1280–1287. | ||
Hamdy S, Jilani S, Price V, Parker C, Hall N, Power M. Modulation of human swallowing behaviour by thermal and chemical stimulation in health and after brain injury. Neurogastroenterol Motil. 2003;15(1):69–77. | ||
Watando A, Ebihara S, Ebihara T, et al. Effect of temperature on swallowing reflex in elderly patients with aspiration pneumonia. J Am Geriatr Soc. 2004;52(12):2143–2144. | ||
Rofes L, Clave P, Ouyang A, et al. Neurogenic and oropharyngeal dysphagia. Ann N Y Acad Sci. 2013;1303:1–10. | ||
Rofes L, Arreola V, Lopez I, et al. Effect of surface sensory and motor electrical stimulation on chronic poststroke oropharyngeal dysfunction. Neurogastroenterol Motil. 2013;25(11):888–e701. | ||
National Institute for Health and Care Excellence, UK. Transcutaneous neuromuscular electrical stimulation for oropharyngeal dysphagia. NICE interventional procedure guidance [IPG490]. 2014. | ||
Gallas S, Marie JP, Leroi AM, Verin E. Sensory transcutaneous electrical stimulation improves post-stroke dysphagic patients. Dysphagia. 2010;25(4):291–297. | ||
Hallett M. Transcranial magnetic stimulation: a primer. Neuron. 2007;55(2):187–199. | ||
Michou E, Mistry S, Rothwell J, Hamdy S. Priming pharyngeal motor cortex by repeated paired associative stimulation: implications for dysphagia neurorehabilitation. Neurorehabil Neural Repair. 2013;27(4):355–362. | ||
Momosaki R, Masahiro A, Wataru K. Bilateral repetitive transcranial magnetic stimulation combined with intensive swallowing rehabilitation for chronic stroke dysphagia: a case series study. Case Rep Neurol. 2014;6(1):60–67. | ||
Adeyemo BO, Simis M, Macea DD, Fregni F. Systematic review of parameters of stimulation, clinical trial design characteristics, and motor outcomes in non-invasive brain stimulation in stroke. Front Psychiatry. 2015;3:88. | ||
Sánchez García E, Montero Errasquín B, Sánchez Castellano C, Cruz-Jentoft AJ. Importance of nutritional support in older people. Nestle Nutr Inst Workshop Ser. 2012;72:101–108. | ||
Cruz-Jentoft AJ, Franco A, Sommer P, et al. European silver paper on the future of health promotion and preventive actions, basic research and clinical aspects of age-related diseases. Aging Clin Exp Res. 2009;21(6):376–385. | ||
Forster A, Samaras N, Gold G, Samaras D. Oropharyngeal dysphagia in older adults: a review. Eur Geriatr Med. 2011;2(6):356–362. | ||
van der Bilt A. Assessment of mastication with implications for oral rehabilitation: a review. J Oral Rehabil. 2011;38(10):754–780. | ||
Matsuo K, Palmer JB. Coordination of mastication, swallowing and breathing. Jpn Dent Sci Rev. 2009;45(1):31–40. | ||
Kohyama K, Mioche L, Bourdiol P. Influence of age and dental status on chewing behaviour studied by EMG recordings during consumption of various food samples. Gerodontology. 2003;20(1):15–23. | ||
Helkimo E, Carlsson GE, Helkimo M. Bite force and state of dentition. Acta Odontol Scand. 1977;35:297–303. | ||
Kapur KK, Soman SD. Masticatory performance + efficiency in denture wearers. J Prosthet Dent. 1964;14(4):687–694. | ||
Slagter AP, Bosman F, Vanderbilt A. Comminution of 2 artificial test foods by dentate and edentulous subjects. J Oral Rehabil. 1993;20(2):159–176. | ||
Hiiemae KM, Palmer JB. Food transport and bolus formation during complete feeding sequences on foods of different initial consistency. Dysphagia. 1999;14(1):31–42. | ||
Leonard R, McKenzie S. Hyoid-bolus transit latencies in normal swallow. Dysphagia. 2006;21(3):183–190. | ||
Fontijn-Tekamp FA, Slagter AP, van der Bilt A, et al. Biting and chewing in overdentures, full dentures, and natural dentitions. J Dent Res. 2000;79(7):1519–1524. | ||
Kapur KK, Garrett NR, Hamada MO, et al. A randomized clinical trial comparing the efficacy of mandibular implant-supported overdentures and conventional dentures in diabetic patients. Part I: methodology and clinical outcomes. J Prosthet Dent. 1998;79(5):555–569. | ||
Tang L, Lund JP, Tache R, Clokie CML, Feine JS. A within-subject comparison of mandibular long-bar and hybrid implant-supported prostheses: evaluation of masticatory function. J Dent Res. 1999;78(9):1544–1553. | ||
Kolb G. Why do we need cooperation between the geriatrician and the dentist? Z Gerontol Geriatr. 1999;32(2):150. | ||
Wickop H, Woestmann B, Ferger P, Kolb G. Correlation of dental and nutritional status in elderly patients. Z Gerontol Geriatr. 1999;32(2):167. | ||
Woestmann B, Wickop H, Nguyen CT, Ferger P, Kolb G. Correlation between chewing efficiency, dental and nutritional status in elderly patients. Z Gerontol Geriatr. 1999;32(2):168. | ||
Volkert D, Berner YN, Berry E, et al. ESPEN guidelines on enteral nutrition: geriatrics. Clin Nutr. 2006;25(2):330–360. | ||
Clave P, Garcia-Peris P. Guía de Diagnóstico y de Tratamiento Nutricional y Rehabilitador de la Disfagia Orofaríngea [Guide of Diagnostic and Nutritional and Reabilitation Treatment of Oropharyngeal Dysphagia]. Barcelona: Nestlé Nutrition; 2011. Spanish. | ||
Miller RG, Rosenberg JA, Gelinas NF, et al. Practice parameter: the care of the patient with amyotrophic lateral sclerosis (an evidence-based review) – report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 1999;52(7):1311–1323. | ||
Baeten C, Hoefnagels J. Feeding via nasogastric tube or percutaneous endoscopic gastrostomy – a comparison. Scand J Gastroenterol. 1992;27:95–98. | ||
Dwolatzky T, Berezovski S, Friedmann R, et al. A prospective comparison of the use of nasogastric and percutaneous endoscopic gastrostomy tubes for long-term enteral feeding in older people. Clin Nutr. 2001;20(6):535–540. | ||
Carrau RL, Pou A, Eibling DE, Murry T, Ferguson BJ. Laryngeal framework surgery for the management of aspiration. Head Neck. 1999;21(2):139–145. | ||
Mazzini L, Corra T, Zaccala M, Mora G, Delpiano M, Galante M. Percutaneous endoscopic gastrostomy and enteral nutrition in amyotrophic-lateral-sclerosis. J Neurol. 1995;242(10):695–698. | ||
Groher ME. Determination of the risks and benefits of oral feeding. Dysphagia. 1994;9(4):233–235. | ||
Shailesh LTC, Kadakia C, Sullivan HO, Starnes E. Percutaneous endoscopic gastrostomy or jejunostomy and the incidence of aspiration in 79 patients. Am J Surg. 1992;164(2):114–118. | ||
Guidelines for the use of parenteral and enteral nutrition in adult and pediatric patients. JPEN J Parenter Enteral Nutr. 2002;26(Suppl 1):S1–S138. | ||
Schwartz DB, Barrocas A, Wesley JR, et al. Gastrostomy tube placement in patients with advanced dementia or near end of life. Nutr Clin Pract. 2014;29(6):829–840. | ||
Abuksis G, Mor M, Segal N, et al. Percutaneous endoscopic gastrostomy: high mortality rates in hospitalized patients. Am J Gastroenterol. 2000;95(1):128–132. | ||
Gillick MR. Sounding board – rethinking the role of tube feeding in patients with advanced dementia. N Engl J Med. 2000;342(3):206–210. | ||
Pearce CB, Duncan HD. Enteral feeding. Nasogastric, nasojejunal, percutaneous endoscopic gastrostomy, or jejunostomy: its indications and limitations. Postgrad Med J. 2002;78(918):198–204. | ||
Perona F, Castellazzi G, De Iuliis A, Rizzo L. Percutaneous radiologic gastrostomy: 12-year series. Gut Liver. 2010;4(Suppl 1):S44–S49. | ||
Potack JZ, Chokhavatia S. Complications of and controversies associated with percutaneous endoscopic gastrostomy: report of a case and literature review. Medscape J Med. 2008;10(6):142. | ||
Sampson EL, Candy B, Jones L. Enteral tube feeding for older people with advanced dementia. Cochrane Database Syst Rev. 2009;2:CD007209. | ||
Mushkin SJ. Toward a definition of health economics. Public Health Rep. 1958;73(9):785–793. | ||
Elia M. Nutrition and health economics. Nutrition. 2006;22(5):576–578. | ||
Altman KW, Yu GP, Schaefer SD. Consequence of dysphagia in the hospitalized patient impact on prognosis and hospital resources. Arch Otolaryngol Head Neck Surg. 2010;136(8):784–789. | ||
Bonilha HS, Simpson AN, Ellis C, Mauldin P, Martin-Harris B, Simpson K. The one-year attributable cost of post-stroke dysphagia. Dysphagia. 2014;29(5):545–552. | ||
Cowan DT, Roberts JD, Fitzpatrick JM, While AE, Baldwin J. Nutritional status of older people in long term care settings: current status and future directions. Int J Nurs Stud. 2004;41(3):225–237. | ||
Takeuchi K, Aida J, Ito K, Furuta M, Yamashita Y, Osaka K. Nutritional status and dysphagia risk among community-dwelling frail older adults. J Nutr Health Aging. 2014;18(4):352–357. | ||
Martyn CN, Winter PD, Coles SJ, Edington J. Effect of nutritional status on use of health care resources by patients with chronic disease living in the community. Clin Nutr. 1998;17(3):119–123. | ||
Elia M, Stratton R, Russel C, Green C, Pang F. The Cost of Disease-Related Malnutrition in the UK and Economic Considerations for the Use of Oral Nutritional Supplements (ONS) in Adults. Redditch: Health Economic Group of the British Association for Parenteral and Enteral Nutrition (BAPEN); 2005. | ||
Russell CA. The impact of malnutrition on healthcare costs and economic considerations for the use of oral nutritional supplements. Clin Nutr. 2007;2(1):25–32. | ||
Siddique R, Neslusan CA, Crown WH, Crystal-Peters J, Sloan S, Farup C. A national inpatient cost estimate of percutaneous endoscopic gastrostomy (PEG)-associated aspiration pneumonia. Am J Manag Care. 2000;6(4):490–496. | ||
Sutherland JM, Hamm J, Hatcher J. Adjusting case mix payment amounts for inaccurately reported comorbidity data. Health Care Manag Sci. 2010;13(1):65–73. | ||
Marsh K, Bertanou E, Suominen H, Venkatachalam M. An Economic Evaluation of Speech and Language Therapy. London: Royal College of Speech and Language Therapists; 2010. | ||
Riquelme LF. The role of cultural competence in providing services to persons with dysphagia. Top Geriatr Rehabil. 2007;23(3):228–239. | ||
Davis LA. Quality of life issues related to dysphagia. Top Geriatr Rehabil. 2007;23(4):352–365. | ||
European Convention on Human Rights. Available from: www.echr.coe.int/Documents/Convention_ENG.pdf. Accessed April 26, 2015. | ||
Hamel R. The Catholic Health Association’s response to the papal allocution on artificial nutrition and hydration. Virtual Mentor. 2015;9(5):388–392. | ||
Social care institute for excellence [homepage on the Internet]. Available from: www.scie.org.uk. Accessed April 26, 2015. | ||
Nys H, Stultiens L, Borry P, Goffin T, Dierickx K. Patient rights in EU member states after the ratification of the convention on human rights and biomedicine. Health Policy. 2007;83(2–3):223–235. | ||
Souza MK, Jacob CE, Gama-Rodrigues J, Zilberstein B, Ceconnello I, Habr-Gama A. The written informed consent form (WICF): factors that interfere with acceptance. Arg Bras Cir Dig. 2013;26(3):200–205. | ||
de Vries R, Ryan KA, Stanczyk A, et al. Public’s approach to surrogate consent for dementia research: cautious pragmatism. Am J Geriatr Psychiatry. 2013;21(4):364–372. | ||
Dickens BM, Cook RJ. Adolescents and consent to treatment. Int J Gynaecol Obstet. 2005;89(2):179–184. | ||
Brett AS, Rosenberg JC. The adequacy of informed consent for placement of gastrostomy tubes. Arch Intern Med. 2001;161(5):745–748. | ||
The Universal Declaration of Human Rights [webpage on the Internet]. Available from: www.un.org/en/documents/udhr. Accessed July 1, 2016. | ||
Barker LA, Gout BS, Crowe TC. Hospital malnutrition: prevalence, identification and impact on patients and the healthcare system. Int J Environ Res Public Health. 2011;8(2):514–527. | ||
Weinstein M. The Surprising Power of Family Meals. How Eating Together Makes Us Smarter, Stronger, Healthier and Happier. Hannover: Steerforth Press L.C.; 2005. | ||
Freud S. On Sexuality. London: Penguin; 1991. | ||
Correia MITD, Hegazi RA, Higashiguchi T, et al. Evidence-based recommendations for addressing malnutrition in health care: an updated strategy from the feed M.E. Global Study Group. J Am Med Dir Assoc. 2014;15(8):544–550. | ||
Beuchamps T, Childress J. Principles of Biomedical Ethics. New York: Oxford University Press; 2009. | ||
Stroud M, Duncan H, Nightingale J. Guidelines for enteral feeding in adult hospital patients. Gut. 2003;52:1–12. | ||
Dickens B. Patients’ refusal of recommended treatment. Int J Gynaecol Obstet. 2015;131(1):105–108. | ||
Bernat JL, Gert B, Mogielnicki RP. Patient refusal of hydration and nutrition – an alternative to physician-assisted suicide or voluntary active euthanasia. Arch Intern Med. 1993;153(24):2723–2728. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.