")
Back to Journals » Clinical Ophthalmology » Volume 18
Etiology and Characteristics of Patients Presenting with Eyelid Lacerations at a Level 1 Trauma Center
Authors Awidi AA , Zhao J, Li X, Rajaii F , Ahmad M, Jensen A , Woreta FA
Received 11 November 2023
Accepted for publication 29 February 2024
Published 23 March 2024 Volume 2024:18 Pages 929—935
DOI https://doi.org/10.2147/OPTH.S447452
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Abdelhalim A Awidi,1 Jiawei Zhao,2 Ximin Li,1 Fatemeh Rajaii,1 Meleha Ahmad,3 Adrianna Jensen,4 Fasika A Woreta1
1Wilmer Eye Institute, Johns Hopkins Medicine, Baltimore, MD, USA; 2Plastic Surgery Department, The University of Texas MD Anderson Cancer Center, Houston, TX, USA; 3Ophthalmic Plastic and Reconstructive Surgery Department, University of California, San Francisco, CA, USA; 4Ophthalmic Plastic and Reconstructive Surgery Department, Pacific Center for Oculofacial and Aesthetic Plastic Surgery, San Francisco, CA, USA
Correspondence: Fasika A Woreta, Ophthalmology Department, Wilmer Eye Institute, Baltimore, MD, USA, Tel +1 410 955 5650, Email [email protected]
Purpose: To investigate the etiology and demographic associations of patients presenting with eyelid lacerations to a US level 1 trauma center emergency department (ED).
Patient and Methods: A retrospective chart review of all patients with eyelid lacerations presenting to the ED at a single level 1 trauma center was performed. Eyelid lacerations were categorized as simple eyelid lacerations, eyelid lacerations with eyelid margin involvement, and eyelid lacerations with nasolacrimal system involvement. Data on demographics and clinical characteristics were analyzed.
Results: A total of 303 eyelid laceration cases were identified, 56% were simple eyelid lacerations, followed by 24% with nasolacrimal involvement and 20% involving the eyelid margin. Sixty percent of animal bites/scratches resulted in a nasolacrimal system involving laceration, most commonly affecting children. Falls were the most common etiology in children and patients over the age of 60. Black patients, patients presenting with concomitant ophthalmic injuries, and those with Medicaid insurance were more likely to have an assault etiology (p < 0.05 for all).
Conclusion: Falls were the most common etiology for eyelid lacerations in children and the elderly, while assault was the most common in adults. Identifying the most common etiology by demographic factors can help raise awareness regarding targeted prevention strategies for high-risk populations.
Keywords: eyelid lacerations, ocular trauma, eye injury, emergency department
Introduction
Eyelid lacerations are a commonly reported cause of emergency department (ED) visits in the United States (US), representing approximately 10% of all ED visits.1,2 Eyelid lacerations are also a frequently encountered type of ophthalmic injury with over 2.4 million eye-related injuries reported annually in the US.2 Mechanisms of ophthalmic injuries are usually dependent on the age of the affected individual, with the younger population commonly presenting due to dog bites, sports injuries, and being struck by an object.3–6 Conversely, the elderly population present with ocular injuries due to falls, accidents due to use of consumer products such as chemicals and household tools, as well as motor-vehicle accidents.7–9
Although the demographics and etiology of ophthalmic injuries have been reported extensively, the demographics and etiology of eyelid lacerations have not been as clearly identified.1–5 The only eyelid lacerations clinical study found in the literature was a case series from Iran that reported assault, accidents, and falls as the leading causes of eyelid lacerations in 98 patients.10
The objective of this study was to investigate the etiology, sociodemographic factors, and clinical characteristics of patients presenting to the ED with eyelid lacerations at a level 1 trauma center in the US. A comprehensive understanding of the epidemiology, etiology, and impact of eyelid lacerations may help raise awareness regarding targeted prevention strategies for high-risk populations.
Materials and Methods
A retrospective chart review was conducted on patients with eyelid lacerations presenting to our level 1 trauma center ED from April 2018 through December 2020. The study was conducted in accordance with the tenets of the Declaration of Helsinki. Due to the retrospective nature of the study and minimal risk involved to the privacy of individual participants, a waiver for written informed consent was approved by the Johns Hopkins Medicine Institutional Review Board and all data were deidentified and kept confidential.
The location of our ED is in Baltimore, Maryland, within a large, urban environment where 61% of the population is Black.11 Patients were included in the study if they presented to the ED with a diagnosis of eyelid laceration. Eyelid lacerations were defined as simple eyelid lacerations (ones that do not involve either the eyelid margin or the nasolacrimal system), eyelid lacerations with eyelid margin involvement, and eyelid lacerations nasolacrimal system involvement. The decision regarding surgical repair of the eyelid laceration was made by either the ophthalmology team, plastic surgeons, head and neck surgeons, or emergency medicine physicians. A total of 303 patients were included, and data was collected on demographics (age, sex, race, and insurance status) and baseline features (mechanism of injury, visual acuity, intraocular pressure, location and depth of eyelid laceration, external and slit-lamp examination findings, and imaging evidence of orbital fractures). Information on race/ethnicity was captured through electronic health records, with patients of Hispanic ethnicity being categorized as Hispanic, regardless of their race (White or Black patients could be in the Hispanic category). Other insurance category included Medicare, Workers’ compensation insurance, and military insurance.
As the International Classification of Diseases, Tenth Revision (ICD-10) codes combine eyelid laceration with all lacerations in the periocular region, patient records were individually reviewed to include only those with laceration to the eyelid.
Age was categorized into the following categories according to date of presentation to the ED: children (≤10 years), adolescents (11–20 years), adults (21–60 years), and elderly (≥61 years). Etiology of eyelid laceration injury were categorized as assault, falls, sports and recreational activity, animal bite/scratch, and motor-vehicle related.
Our primary outcome variable was eyelid laceration injury etiology. Descriptive analysis was performed on patient characteristics and demographics. We constructed a multivariable logistic regression model that adjusted for the covariates sex, age, race/ethnicity, insurance status, and concomitant ophthalmic injuries, to investigate the association between these variables and the specific etiology of the eyelid laceration (assault, falls, and motor-vehicle related injuries). Odds ratio (OR) and 95% confidence intervals (CIs) were computed. All statistical analyses was conducted with STATA version 14 (StataCorp, College Station, TX, USA). Statistical significance was defined as p < 0.05.
Results
Baseline demographics and clinical characteristics of patients according to the etiology of their eyelid laceration injury are demonstrated in Table 1. After excluding 750 patients due to injuries that did not meet our criteria for eyelid lacerations, we identified 303 eyelid laceration cases that presented to the ED between April 2018 and December 2020. Mean follow-up duration was 4 months (SD= 6.9 months) and 68% of patients were male. A large percentage of patients presenting to our ED with eyelid lacerations were of Black race (44.2%). Our cohort comprised of 52% adults (21–60 years), followed by 26% children (≤ 10 years), 13% adolescents (11–20 years), and 10% elderly patients (> 61 years) [p < 0.001]. Overall, the top two most frequent insurance categories were Medicaid insurance (39%) followed by private insurance (28%) [p = 0.04]. The majority of falls (33%) and animal bite/scratch (66%) injuries occurred in the children population (≤ 10 years). Conversely, 81% of patients who presented due to assaults and 59% of patients who presented due to motor-vehicle accidents were adults (21–60 years).
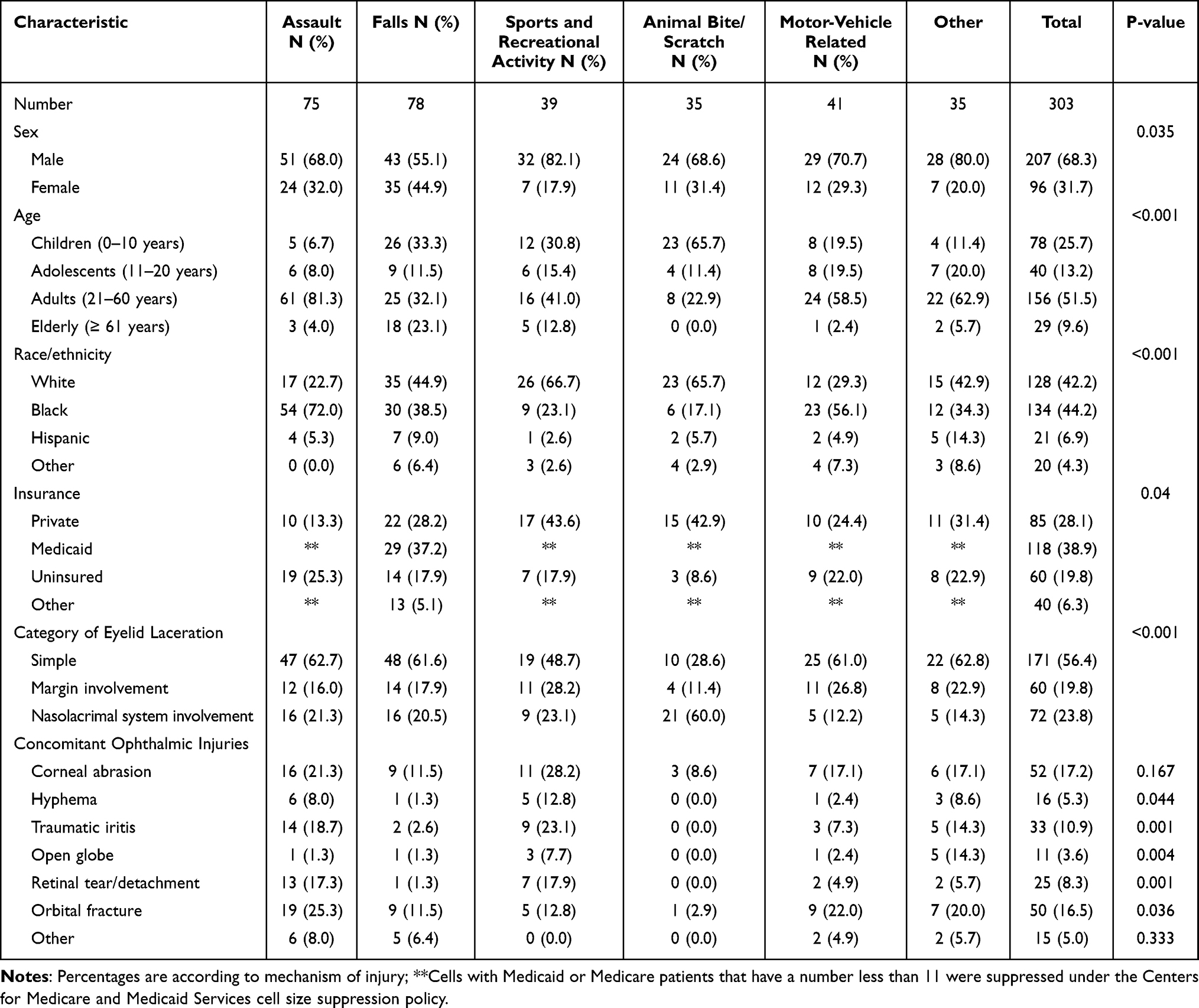 |
Table 1 Characteristics of Patients with Eyelid Lacerations According to Mechanism of Injury |
Assaults occurred more frequently in the Black population (72%), compared to patients in the White (23%) and Hispanic (5%) populations. The majority of sports and recreational activity injuries occurred in the White population (67%).
Simple eyelid lacerations (56%) were the most common type of eyelid laceration among all etiologies, followed by eyelid lacerations with nasolacrimal system involvement (24%) and eyelid lacerations with eyelid margin involvement (20%). Nasolacrimal involving eyelid lacerations were the most common category of eyelid lacerations (60%) in patients presenting secondary to an animal bite/scratch etiology. The majority of fall-related eyelid lacerations (74.4%) resulted from falls that occurred indoors. A higher percentage of males experienced falls outdoors (60.3%) compared to females (39.7%), while a higher percentage of those in the elderly population fell indoors (78.2%) compared to those in the adult population (57.7%). Seventy percent of eyelid lacerations involved the upper eyelid compared to 30% involving the lower eyelid. Additionally, 85% of nasolacrimal system involving lacerations involved the medial punctum.
Corneal abrasions (17%) and orbital fractures (17%) were the most common concomitant ophthalmic injuries across all etiologies, followed by traumatic iritis (11%). Among those who presented with an assault etiology, 25% had orbital fractures, 21% had corneal abrasions, while 19% had traumatic iritis. Patients who were assaulted had a higher frequency of each category of concomitant ophthalmic and orbital injuries (except open globe injuries) compared to other mechanisms of injury.
The management strategy of our patient population is shown in Table 2. In total, 57% of patients underwent surgical eyelid laceration repair, 23% had surgical repair of the canaliculus, followed by 13% of patients that had superficial lacerations and were observed.
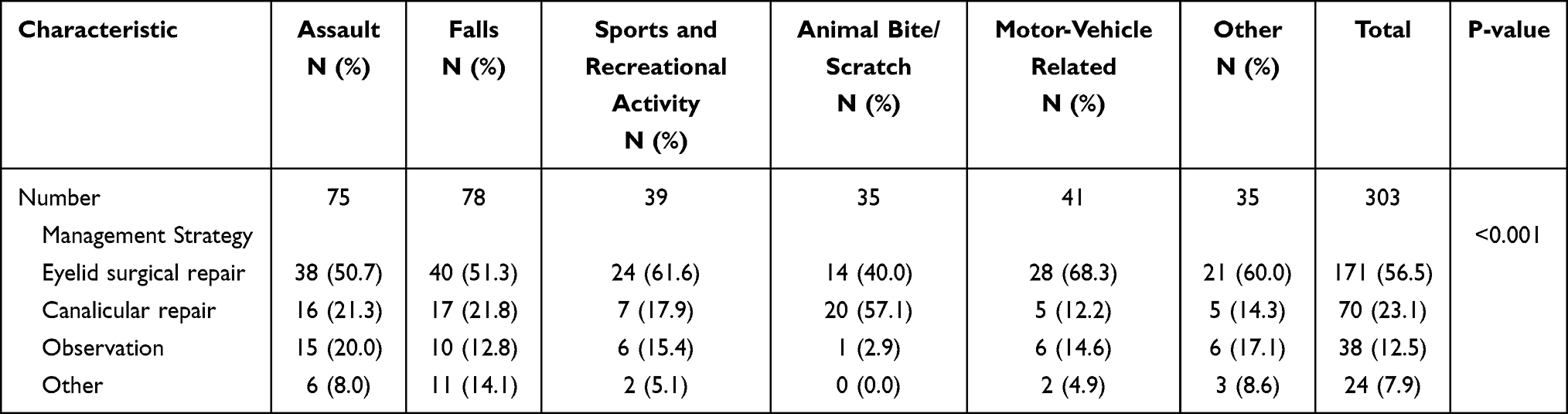 |
Table 2 Management Strategy of Patients Presenting with Eyelid Lacerations |
A multivariable regression analysis model (Table 3) showed that female patients had a higher risk of falls compared to males (OR 2.32 [95% CI 1.27–4.23]; p = 0.006). Children, adolescents, and adults (OR 0.15 [95% CI 0.04–0.48], p = 0.002; OR 0.12 [95% CI 0.03–0.43], p = 0.015; OR 0.08 [95% CI 0.02–0.24]; p < 0.001, respectively) were less likely to present due to a fall compared to elderly patients. Black individuals were more likely to present to the ED with injuries due to assault than White individuals (OR 3.57 [95% CI 1.78–7.41]; p <0.001). Patients who had Medicaid insurance had a higher risk of presenting to the ED with eyelid lacerations due to assault when compared to patients with private insurance (OR 2.66 [95% CI 1.14–6.57]; p = 0.03). Patients presenting with concomitant ophthalmic injuries were more likely to have an assault etiology when compared to those with no concomitant ophthalmic injuries (OR 2.25 [95% CI 1.20–4.29]; p = 0.01).
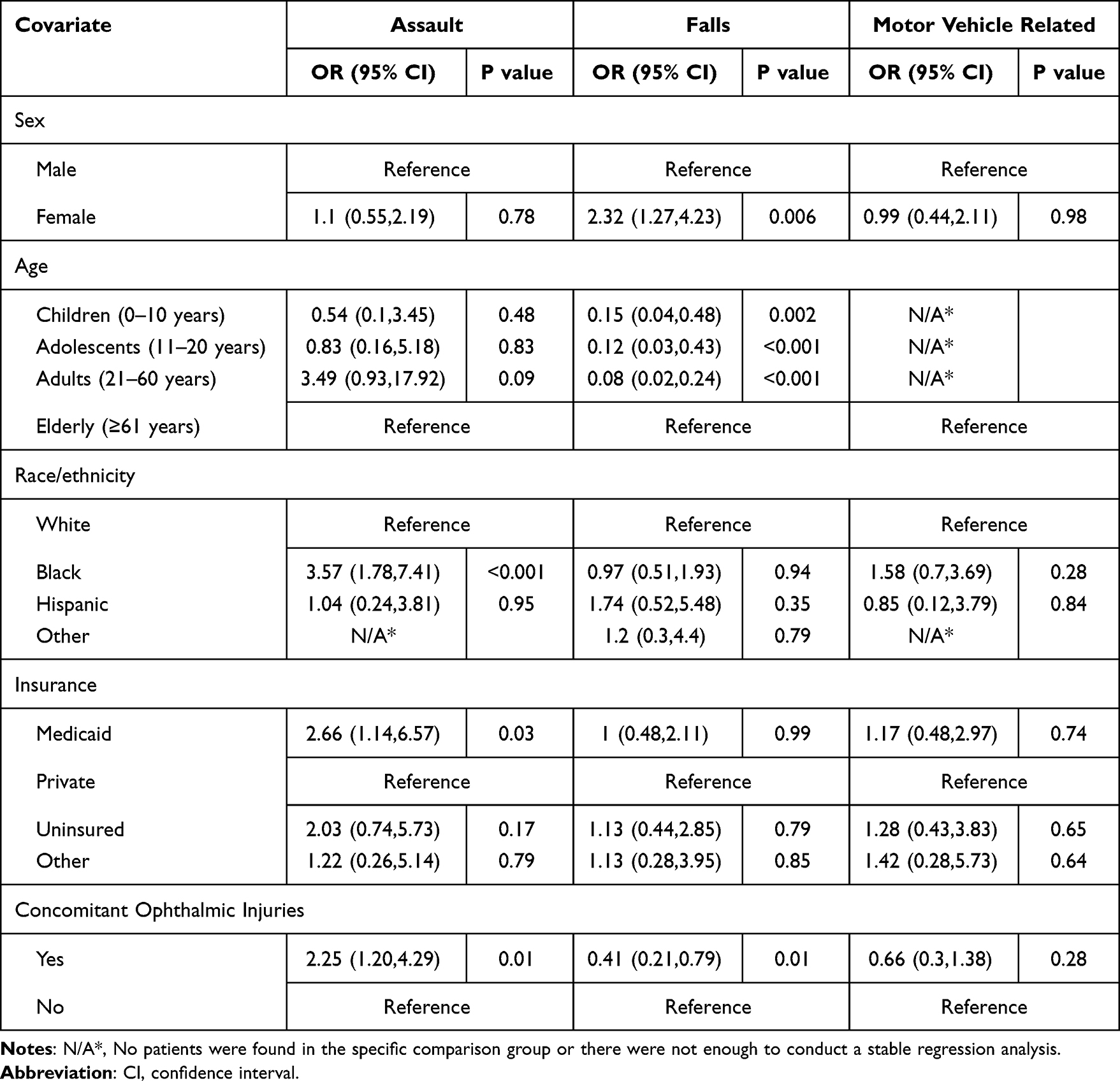 |
Table 3 Multivariable Logistic Regression Analysis Investigating Factors Associated with the Three Most Common Mechanisms of Injury (Assault, Falls, Motor Vehicle Related) |
Discussion
Although causes of ophthalmic trauma in patients presenting to the ED have been previously reported, there is limited literature focusing on eyelid lacerations. We investigated the various etiologies and sociodemographic factors of patients presenting to the ED with eyelid lacerations at a level 1 trauma center in the US. Falls were the most common etiology for eyelid lacerations in children and the elderly populations, while assault was most common in adults. Additionally, patients who presented with concomitant ophthalmic injuries, were Black, or had Medicaid insurance were more likely to present with eyelid lacerations secondary to assault.
Males represented the majority of patients with eyelid lacerations, more than double the number of females in our cohort. This is consistent with prior literature that showed higher rates of ocular trauma in males, irrespective of age of presentation.4,12–14 Black patients were more likely to present with eyelid lacerations secondary to assault compared to White patients. In a study investigating the characteristics of ocular trauma in the US, Black patients were three times more likely to present due to an assault etiology compared to White patients.15 Additionally, a study investigating the incidence of ED–treated eye injuries in the US found that the eye injury rates were highest among Black patients.16 Another finding from our study was that those who had Medicaid insurance were 2.7 times more likely to present with eyelid lacerations due to an assault etiology when compared to those who had private insurance. We hypothesize that this is due to living in socioeconomically disadvantaged neighborhoods that may have higher rates of violent crimes, such as assault.17 Medicaid insurance has been associated with worse trauma outcomes, as shown in a study by Chun et al who investigated the correlation between insurance status and trauma etiology.18 They also found that patients with Medicaid insurance were more likely to suffer from violent crime etiologies, such as gunshot wounds.
The elderly population in our patient cohort were more likely to present with eyelid lacerations secondary to falls compared to other age groups. This is consistent with a study by Usmani et al that reported falls as the leading cause of ophthalmic trauma presenting to the ED in the elderly population from 2006 to 2015.19 In a study that analyzed the characteristics of eyelid lacerations in the ED from 2006 to 2014 using the Nationwide Emergency Department Sample data set, falls were found to cause 74% of all primary eyelid lacerations in the elderly population.20 Falls are well-recognized as one of the leading causes of injuries in the elderly population, and studies focusing on ophthalmic trauma in the elderly have also highlighted the extensive damage that falls carry with them. In our study, 50% of the elderly population who presented with eyelid lacerations due to falls had a concomitant orbital fracture, highlighting the high impact damage that is associated with a fall, not limited to just eyelid lacerations. This was similar to a study investigating fall-related ophthalmic trauma diagnoses in the ED, which found incidence of orbital fractures to be significantly higher in elderly patients when compared to other age groups.21 These findings point to the important role that targeted fall risk mitigations interventions and comprehensive fall risk assessments can play in fall prevention in the elderly population, as falls can have considerable long-term consequences.
In our study, those who presented to the ED with eyelid lacerations and concomitant ophthalmic injuries were more likely to have been assaulted than those who presented with no concomitant ophthalmic injuries. We also noted that 38% of patients who arrived in the ED with concomitant orbital fractures had an assault etiology. A similar finding was reported by a study that investigated the characteristics of orbital floor fractures presenting to the ED in the US over a 12-year period, and found that assaults were the most common mechanism of injury.21 Another study also found assaults to be the most common cause of eye injury in those presenting to the ED with severe eye trauma requiring evisceration or enucleation surgery.22 These studies highlight the long term sequelae of ophthalmic trauma secondary to assaults, and the integral part that a focused ophthalmologic assessment and examination play. Early assessment of extraocular movements and gaze restriction following orbital floor fracture can help prevent the consequences associated with prolonged muscle entrapment such as fibrosis and permanent dysfunction.23
Another important finding of this study was that with the exception of one patient, all those who presented to the ED due to an animal bite/scratch required a form of surgical repair, either eyelid (40%) or canalicular repair (57%). These findings underline the tendency of animal bite/scratch injuries to affect the canalicular system in comparison to other causes of eyelid lacerations, which was also shown in the study by Sadiq et al.24 As the involvement of eyelid structures is likely to be extensive in animal bite/scratch etiologies, consulting an ophthalmologist when treating these injuries could be crucial. Children constituted the majority of patients in the group with an animal bite/scratch etiology, a finding that was similar to other studies.25,26 A study investigating ocular trauma in dog bite victims in a level 1 trauma center over 11 years showed that children with dog bite injuries were 4.2 times more likely to sustain ocular injuries than adults.27 They also found that 40% of those who suffered from periocular injuries due to dog bites had a canalicular laceration injury. Children are particularly vulnerable to animal injuries as they lack situational awareness and are thus likely to encroach on an animal’s territory with provocative interactions. This should also emphasize the prompt assessment of the canalicular system in children who present to the ED with eyelid lacerations caused by animal bites/scratch due to the high frequency of concomitant injury.
The strengths of this study include the extensive assessments of patients presenting with eyelid lacerations, including demographics, clinical characteristics, and management strategy. In addition, these evaluations were performed by ophthalmologists or ophthalmology trainees. The study was also conducted at a level 1 trauma center, which allowed for a diverse, integrated patient population in terms of racial/ethnic background, socioeconomic status, and varying etiologies of eyelid laceration injuries. The main limitations of this study are its retrospective nature and being conducted in a single-center. Another limitation was the low number of patients with certain demographics in some trauma etiologies that limited our power calculations in identifying all relevant risk factors. Despite the strength of the study being conducted at a level 1 trauma center, it was still a single-center study. Future multi-center institute studies investigating the etiology and characteristics of patients presenting to the ED with eyelid lacerations to investigate the generalizability of our results are warranted.
Conclusion
Prompt consultation and management of eyelid lacerations can be crucial as they commonly present with a varying range of concomitant ophthalmic injuries, such as orbital fracture, open globe, hyphema, and traumatic iritis. In addition, we noted that with the exception of one patient, all those who presented with eyelid lacerations due to animal-related injuries required a form of surgical repair, thus emphasizing the need for a timely consult and operation. Finally, as eyelid lacerations secondary to falls were most commonly seen in elderly patients, future targeted fall risk mitigations interventions and comprehensive fall risk assessments may play a role in prevention.
Abbreviations
ED, Emergency department; US, United States; ICD-10, International Classification of Diseases, Tenth Revision (ICD-10); OR, Odds ratio; CI, confidence interval.
Acknowledgments
This work was supported by the Wilmer Biostatistics Core Grant P30EY001765. The funding source was not involved in any part of the study.
The abstract of this paper was presented at the 2022 Association for Research in Vision and Ophthalmology as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in the Investigative Ophthalmology & Visual Science Journal https://iovs.arvojournals.org/article.aspx?articleid=2780571.
Disclosure
Dr Fatemeh Rajaii reports personal fees for consulting and stock ownership (sold) from Horizon Therapeutics, principal investigator in sponsored research for Immunovant, personal fees for consulting from Acelyrin, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Channa R, Zafar SN, Canner JK, Haring RS, Schneider EB, Friedman DS. Epidemiology of eye-related emergency department visits. JAMA Ophthalmol. 2016;134(3):312–319. doi:10.1001/jamaophthalmol.2015.5778
2. Owens PL, Mutter R. Emergency department visits related to eye injuries, 2008: statistical brief #112. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006.
3. Iftikhar M, Junaid N, Lemus M, et al. Epidemiology of primary ophthalmic inpatient admissions in the United States. Am J Ophthalmol. 2018;185:101–109. doi:10.1016/j.ajo.2017.10.014
4. Avraham JB, Bhandari M, Frangos SG, Levine DA, Tunik MG, DiMaggio CJ. Epidemiology of paediatric trauma presenting to US emergency departments: 2006–2012. Inj Prev. 2019;25(2):136–143. doi:10.1136/injuryprev-2017-042435
5. Matsa E, Shi J, Wheeler KK, McCarthy T, McGregor ML, Leonard JC. Trends in US emergency department visits for pediatric acute ocular injury. JAMA Ophthalmol. 2018;136(8):895–903. doi:10.1001/jamaophthalmol.2018.2062
6. Bratton EM, Golas L, Wei LA, Davies BW, Durairaj VD. Ophthalmic manifestations of facial dog bites in children. Ophthalmic Plast Reconstr Surg. 2018;34(2):106–109. doi:10.1097/iop.0000000000000875
7. Halawa O, Mitchell W, Zebardast N. Fall-related eye injury among older adults in the United States. Am J Ophthalmol. 2021;229:82–89. doi:10.1016/j.ajo.2021.03.063
8. Chen AJ, Kim JG, Linakis JG, Mello MJ, Greenberg PB. Eye injuries in the elderly from consumer products in the United States: 2001–2007. Graefes Arch Clin Exp Ophthalmol. 2013;251(3):645–651. doi:10.1007/s00417-012-2004-x
9. Sheng I, Bauza A, Langer P, Zarbin M, Bhagat N. A 10-year review of open-globe trauma in elderly patients at an urban hospital. Retina. 2015;35(1):105–110. doi:10.1097/iae.0000000000000261
10. Tabatabaei A, Kasaei A, Nikdel M, et al. Clinical characteristics and causality of eye lid laceration in Iran. Oman Med J. 2013;28(2):97–101. doi:10.5001/omj.2013.26
11. U.S. Census Bureau. Population estimates, July 1, 2023 -- Baltimore city, MD [data table]. Quick Facts; 2023. Available from: https://www.census.gov/quickfacts/fact/table/baltimorecitymaryland/PST045223.
12. Özer Ö, Güçiü E. Etiology, clinical characteristics and surgical indications in traumatic eyelid injuries: experience of a tertiary referral center, 18 September 2023, PREPRINT (Version 1) available at Research Square. 2023.
13. Oiticica-Barbosa MM, Kasahara N. Eye trauma in children and adolescents: perspectives from a developing country and validation of the ocular trauma score. J Trop Pediatr. 2015;61(4):238–243. doi:10.1093/tropej/fmv010
14. Gervasio KA, Weinstock BM, Wu AY. Prognostic value of ocular trauma scores in patients with combined open globe injuries and facial fractures. Am J Ophthalmol. 2015;160(5):882–888.e882. doi:10.1016/j.ajo.2015.08.007
15. He CH, Poulsen DM, Parsikia A, Mbekeani JN. Characteristics of ocular trauma in the United States. Arq Bras Oftalmol. 2022;85(3):240–248. doi:10.5935/0004-2749.20220035
16. McGwin G Jr, Owsley C. Incidence of emergency department-treated eye injury in the United States. Arch Ophthalmol. 2005;123(5):662–666. doi:10.1001/archopht.123.5.662
17. Chong VE, Lee WS, Victorino GP. Neighborhood socioeconomic status is associated with violent reinjury. J Surg Res. 2015;199(1):177–182. doi:10.1016/j.jss.2015.03.086
18. Chun M, Zhang Y, Nguyen A, et al. How does insurance status correlate with trauma mechanisms and outcomes? A retrospective study at a level 1 trauma center. Am Surg. 2022;88(5):859–865. doi:10.1177/00031348211032592
19. Usmani B, Latif A, Iftikhar M, et al. Eye trauma in falls presenting to the emergency department from 2006 through 2015. Br J Ophthalmol. 2021;105(2):198–204. doi:10.1136/bjophthalmol-2019-314669
20. Cade KL, Taneja K, Jensen A, Rajaii F. Incidence, characteristics, and cost of eyelid lacerations in the United States from 2006 to 2014. Ophthalmol Ther. 2023;12(1):263–279. doi:10.1007/s40123-022-00605-9
21. Iftikhar M, Canner JK, Hall L, Ahmad M, Srikumaran D, Woreta FA. Characteristics of orbital floor fractures in the United States from 2006 to 2017. Ophthalmology. 2021;128(3):463–470. doi:10.1016/j.ophtha.2020.06.065
22. Gauthier AC, Oduyale OK, Fliotsos MJ, et al. Clinical characteristics and outcomes in patients undergoing primary or secondary enucleation or evisceration after ocular trauma. Clin Ophthalmol. 2020;14:3499–3506. doi:10.2147/opth.S273760
23. Joseph JM, Glavas IP. Orbital fractures: a review. Clin Ophthalmol. 2011;5:95–100. doi:10.2147/opth.S14972
24. Sadiq MA, Corkin F, Mantagos IS. Eyelid lacerations due to dog bite in children. J Pediatr Ophthalmol Strabismus. 2015;52(6):360–363. doi:10.3928/01913913-20150901-02
25. Kaye AE, Belz JM, Kirschner RE. Pediatric dog bite injuries: a 5-year review of the experience at the children’s hospital of Philadelphia. Plast Reconstr Surg. 2009;124(2):551–558. doi:10.1097/PRS.0b013e3181addad9
26. Boyd LC, Chang J, Ajmera S, Wallace RD, Alvarez SM, Konofaos P. Pediatric dog bites: a review of 1422 cases treated at a level one regional pediatric trauma center. J Craniofac Surg. 2022;33(4):1118–1121. doi:10.1097/scs.0000000000008209
27. Prendes MA, Jian-Amadi A, Chang SH, Shaftel SS. Ocular trauma from dog bites: characterization, associations, and treatment patterns at a regional level i trauma center over 11 years. Ophthalmic Plast Reconstr Surg. 2016;32(4):279–283. doi:10.1097/iop.0000000000000501
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.