Back to Journals » Clinical Epidemiology » Volume 12
Estimating the Fraction of First-Year Hemodialysis Deaths Attributable to Potentially Modifiable Risk Factors: Results from the DOPPS
Authors Karaboyas A ![]() , Morgenstern H, Li Y, Bieber BA
, Morgenstern H, Li Y, Bieber BA ![]() , Hakim R, Hasegawa T, Jadoul M, Schaeffner E, Vanholder R, Pisoni RL, Port FK, Robinson BM
, Hakim R, Hasegawa T, Jadoul M, Schaeffner E, Vanholder R, Pisoni RL, Port FK, Robinson BM
Received 2 October 2019
Accepted for publication 12 December 2019
Published 16 January 2020 Volume 2020:12 Pages 51—60
DOI https://doi.org/10.2147/CLEP.S233197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eyal Cohen
Angelo Karaboyas, 1 Hal Morgenstern, 2 Yun Li, 3 Brian A Bieber, 1 Raymond Hakim, 4 Takeshi Hasegawa, 5 Michel Jadoul, 6 Elke Schaeffner, 7 Raymond Vanholder, 8 Ronald L Pisoni, 1 Friedrich K Port, 9 Bruce M Robinson 1
1Arbor Research Collaborative for Health, Ann Arbor, MI, USA; 2Departments of Epidemiology and Environmental Health Sciences, School of Public Health, and Department of Urology, Medical School, University of Michigan, Ann Arbor, MI, USA; 3Department of Biostatistics, University of Michigan School of Public Health, Ann Arbor, MI, USA; 4Vanderbilt University Medical Center, Nashville, TN, USA; 5Division of Nephrology, Department of Medicine, Showa University Fujigaoka Hospital, Yokohama, Japan, and Showa University Research Administration Center (SURAC), Showa University, Tokyo, Japan; 6Cliniques universitaires St Luc, Université Catholique de Louvain, Brussels, Belgium; 7Institute of Public Health, Charité – Universitätsmedizin Berlin, Berlin, Germany; 8Department of Nephrology, University Hospital Ghent, Ghent, Belgium; 9Department of Epidemiology, University of Michigan School of Public Health, and Department of Internal Medicine-Nephrology, University of Michigan Medical School, Ann Arbor, MI, USA
Correspondence: Angelo Karaboyas
Arbor Research Collaborative for Health, 3700 Earhart Drive, Ann Arbor, MI 48105, USA
Tel +1 734 665-4108
Fax +1 734 665-2103
Email [email protected]
Purpose: Mortality among first-year hemodialysis (HD) patients remains unacceptably high. To address this problem, we estimate the proportions of early HD deaths that are potentially preventable by modifying known risk factors.
Methods: We included 15,891 HD patients (within 60 days of starting HD) from 21 countries in the Dialysis Outcomes and Practice Patterns Study (1996– 2015), a prospective cohort study. Using Cox regression adjusted for potential confounders, we estimated the fraction of first-year deaths attributable to one or more of twelve modifiable risk factors (the population attributable fraction, AF) identified from the published literature by comparing predicted survival based on risk factors observed vs counterfactually set to reference levels.
Results: The highest AFs were for catheter use (22%), albumin < 3.5 g/dL (19%), and creatinine < 6 mg/dL (12%). AFs were 5%-9% for no pre-HD nephrology care, no residual urine volume, systolic blood pressure < 130 or ≥ 160 mm Hg, phosphorus < 3.5 or ≥ 5.5 mg/dL, hemoglobin < 10 or ≥ 12 g/dL, and white blood cell count > 10,000/μL. AFs for ferritin, calcium, and PTH were < 3%. Overall, 65% (95% CI: 59%-71%) of deaths were attributable to these 12 risk factors. Additionally, the AF for C-reactive protein > 10 mg/L was 21% in facilities where it was routinely measured.
Conclusion: A substantial proportion of first-year HD deaths could be prevented by successfully modifying a few risk factors. Highest priorities should be decreasing catheter use and limiting malnutrition/inflammation whenever possible.
Keywords: hemodialysis, incidence, mortality, attributable fraction, cohort study
Introduction
Mortality risk during the first year of chronic hemodialysis (HD) remains high worldwide, including 21% in the US, and is especially high in the first few months after initiating HD.1–5 Several findings support the possibility that improvements in care may improve outcomes for incident HD patients. Clinical practices that may positively influence first-year mortality, such as pre-end-stage renal disease (ESRD) nephrology care and use of arteriovenous fistula (AVF) for dialysis, have been recognized for some time.3,6–8 However, in many countries, a large proportion of patients start dialysis only a few months after first seeing a nephrologist, too soon to establish surgical vascular access for use at dialysis initiation.6,9 The mean eGFR at dialysis start has until recently been rising in the US and elsewhere, despite a lack of evidence for clinical benefit of earlier dialysis treatment.10−14 Patients often start dialysis several months before needed, missing the opportunity to be adequately prepared to start dialysis. As one mitigating strategy, multidisciplinary programs to optimize preparation for dialysis may help limit urgent or unnecessarily early dialysis starts and, in turn, improve patient outcomes,15–17 but structural barriers and policy misalignments limit their wider implementation in many countries.18,19
Prior studies have identified risk factors for early dialysis mortality, but they have not incorporated prevalence to quantify the impact of these risk factors at the population level, i.e., to estimate the proportions of early HD deaths that are potentially preventable. The population attributable fraction (AF) approach is an appealing solution, but is rarely used in the context of time-to-event outcomes, presumably due to challenges in estimation. Given the urgent need to appropriately direct resources to improve outcomes for patients in the first year of dialysis, it is imperative to identify the most important risk factors for early dialysis mortality at the population level. To this end, our study aim was to quantify the impact – considering both prevalence and effects on mortality – of potentially modifiable patient and treatment risk factors on first-year HD mortality using a population AF approach suitable for a time-to-event outcome.
Methods
Data Source
The Dialysis Outcomes and Practice Patterns Study (DOPPS) is an ongoing international prospective cohort study of HD patients designed to identify links between modifiable practices and outcomes in HD patients, with the goal of extending survival and improving quality of life; the DOPPS helps researchers and clinicians better understand differences in practice patterns and factors associated with patient outcomes. This analysis includes data from 21 countries across DOPPS phases 1–5 (1996–2015). Participating countries included France, Germany, Italy, Japan, Spain, United Kingdom, and United States (US) in DOPPS phases 1–5; Australia and New Zealand (ANZ), Belgium, Canada, and Sweden in DOPPS phases 2–5; and the Gulf Cooperation Council (GCC, including Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, United Arab Emirates), China, Russia, and Turkey in DOPPS Phase 5. At the beginning of each study phase (~3 years each), DOPPS participants were randomly selected from national samples of HD facilities within each country to achieve representative samples of the age ≥18 in-center HD population within each country.20,21 The DOPPS Program is coordinated by Arbor Research Collaborative for Health. Study approval was obtained by a central institutional review board (Ethical & Independent Review Services, Independence, MO). Additional study approval and patient consent were obtained as required by national and local ethics committee regulations. All data are housed at Arbor Research Collaborative for Health and available internally for research purposes. Data on demographics, comorbid conditions, laboratory values, and prescriptions were abstracted from medical records at DOPPS enrollment using uniform data collection tools. Mortality events were collected during study follow-up. The population of interest for this study was patients who enrolled in DOPPS within 60 days after initiating maintenance HD therapy. Participants with unknown vintage (time since dialysis initiation) at DOPPS enrollment (baseline) were excluded; no other exclusions were made.
Variables
Twelve known risk factors for dying (Table 2) were chosen from variables measured at baseline. To estimate associations with mortality, we categorized risk factors into two groups (high vs low risk) or three groups (if hypothesized U-shaped association). Cutpoints were based principally on previous research demonstrating adjusted associations with mortality.
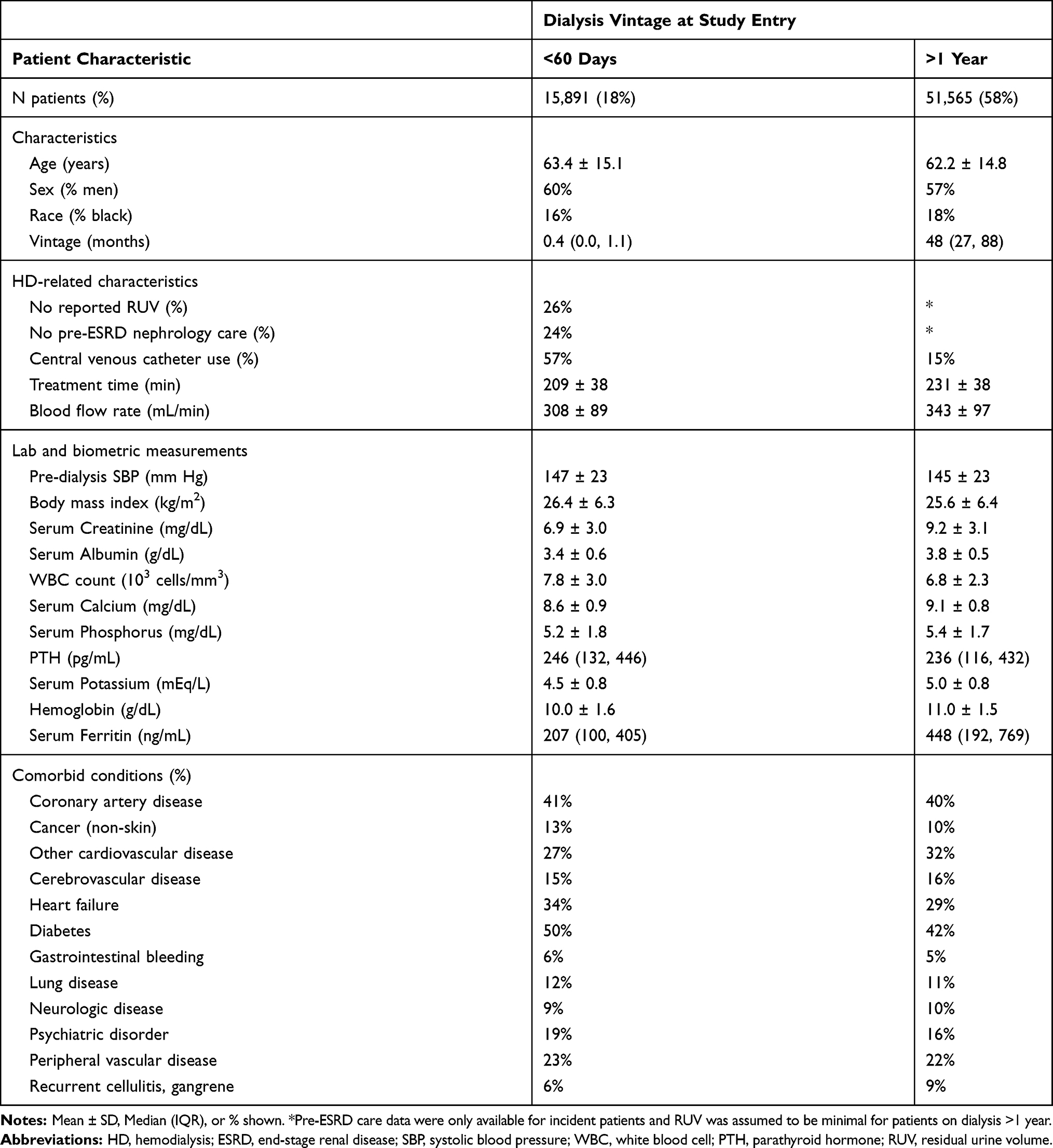 |
Table 1 Patient Characteristics by Time on Dialysis (Vintage) |
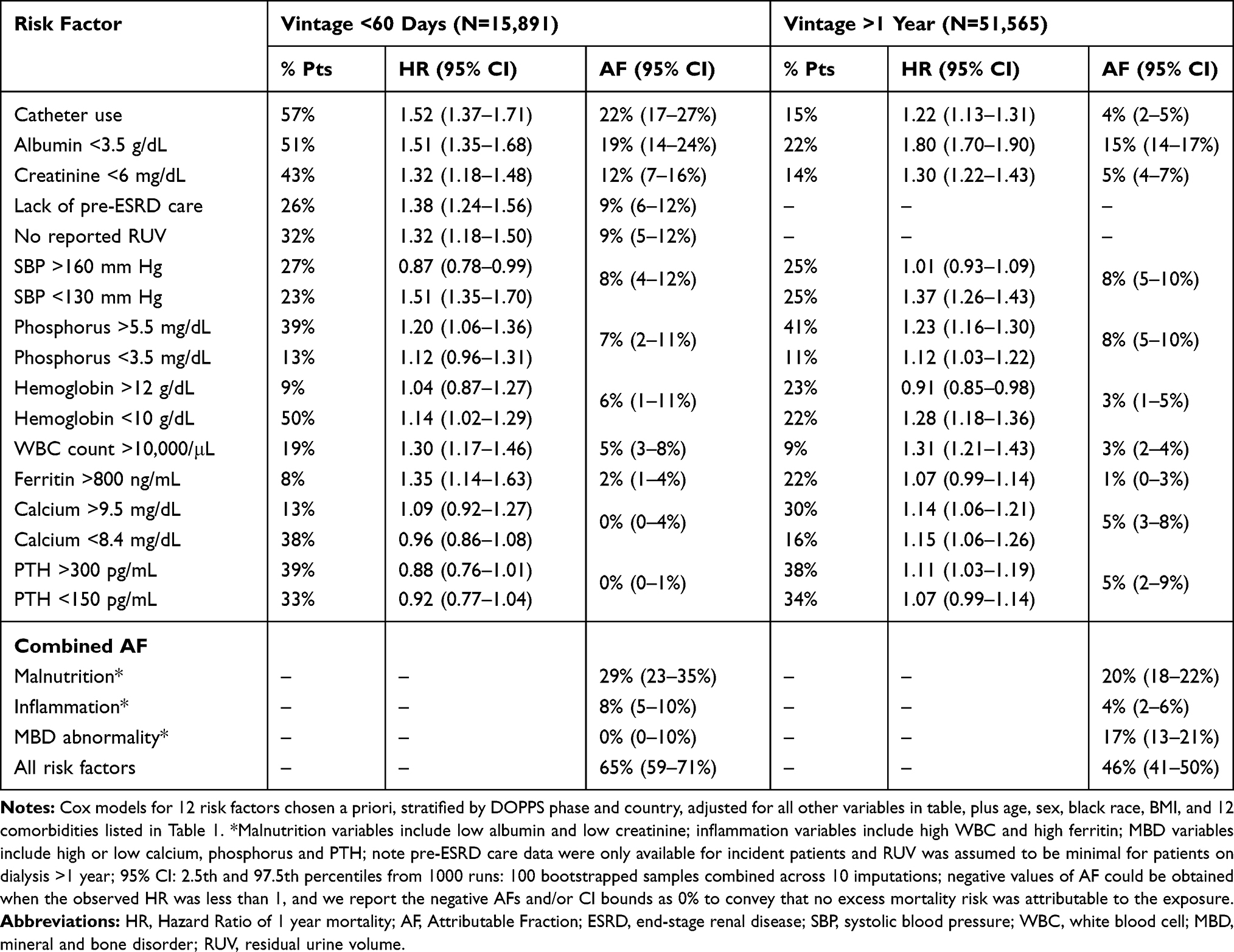 |
Table 2 Attributable Fractions for Mortality Risk-Factors, by Baseline Vintage |
Statistical Analysis
We used Cox regression, stratified by DOPPS phase and country, and accounted for within-facility clustering, to estimate the association between each risk factor and 1-year mortality among patients with vintage <60 days at DOPPS entry. Models included all risk factors plus adjustments for age, sex, black race, body mass index, and 12 comorbidities (Table 1). Time at risk extended from study enrollment to the day of death, 7 days after transition to home dialysis, or facility departure due to transfer or kidney transplantation, loss to follow-up, end of the study phase, or 1 year after enrollment. Because we focus on assessing risk factors with potential interventions at or near HD initiation, we utilized exposure variables measured at baseline only.
The proportion of observed first-year deaths in the study population attributable to each risk factor was estimated using the method of Samuelsen and Eide.22 The population AF for deaths occurring before time t, labeled “AFB(t),” depends on both the strength of the association (hazard ratio; HR) and prevalence of the risk factor. The AF is the estimated percentage of deaths that would not have occurred if every patient’s baseline risk-factor value had been in the reference category (e.g., if no patients dialyzed with a catheter; no catheter use); this is the maximum potential impact of eliminating each risk factor and does not necessarily reflect what is achievable in clinical practice.23 From the fitted Cox model, we calculated predicted 1-year survival using each patient’s observed value of the risk factor (PredSurv_Obs) and with that risk factor counterfactually set to the reference value (PredSurv_CF). We then estimated AFB (t=1 year), hereafter referred to as AF, by (i) summing (PredSurv_CF – PredSurv_Obs) across all patients, (ii) summing (1 – PredSurv_Obs) across all patients, and (iii) dividing the result from (i) by the result from (ii). The AF was estimated for each risk factor and for all risk factors combined. For 3-level factors, we estimated the HR for low and high levels (vs the “normal” referent) and summed contributions from both categories. To estimate the combined AF, we counterfactually set all tested risk factors to the reference level concurrently. We similarly estimated a combined AF for each of the three groups of variables related to malnutrition, inflammation, and mineral and bone disorder (MBD) abnormalities.
Analyses were repeated by DOPPS region and study phase, and by black race within North America. Analyses within Japan and countries new to DOPPS in phase 5 were not feasible due to the very small number of deaths. C-reactive protein (CRP) was not collected in DOPPS Phase 1 and was not measured in the majority of facilities – particularly in North America (1% of facilities). CRP >10 mg/L was thus investigated as a risk factor in a subset of facilities that routinely measured CRP (in ≥50% of patients). To compare HD patients at different stages of their dialysis treatment, we performed secondary analyses to estimate AFs for other cohorts of patients with baseline vintage >1 year, and 60 days to 1 year.
We used multiple imputation to deal with missing covariate data using the Sequential Regression Multiple Imputation Method by IVEware.24 The proportion of missing data was below 20% for all model covariates, with the exception of PTH (42%), no residual urine volume (RUV; urine output <200 mL/day, 41%), ferritin (36%), pre-ESRD nephrology care (30%), and albumin (25%). Confidence intervals (CIs) for HRs and AFs were estimated using clustered bootstrapped re-sampling. Within each DOPPS phase-country combination, we resampled patients 100 times and repeated the AF analyses. This process was repeated for 10 imputations, resulting in 1000 datasets. We then derived the 95% CI as the 2.5th and 97.5th percentile of these datasets based on the “MI boot (pooled sample)” procedure described by Schomaker and Heumann.25 All analyses were conducted using SAS software, version 9.4 (SAS institute, Cary, NC).
Results
Patient Characteristics
Our primary analyses focused on 15,891 incident patients with vintage <60 days at DOPPS enrollment. Table 1 compares characteristics of these patients to those on dialysis for >1 year (average 5.9 years) at enrollment. Incident patients were more likely to dialyze using a catheter and to have RUV, shorter treatment time, higher white blood cell (WBC) count, lower hemoglobin, and lower serum values of albumin, creatinine, calcium, potassium, and ferritin. Over the 1 year follow-up period, the mortality rate was 0.165/year (1937 deaths) among 15,891 patients with baseline vintage <60 days, and 0.131/year (5759 deaths) among 51,565 patients with vintage >1 year.
Attributable Fractions for Mortality Risk Factors
In our primary analysis, the risk factors for 1-year mortality with the largest AF were catheter use (22%; 95% CI: 17–27%) and albumin <3.5 g/dL (19%; 95% CI: 14-24%) (Table 2, left panel). Other risk factors with AF >5% were serum creatinine <6 mg/dL (AF=12%), lack of pre-ESRD nephrology care (AF=9%), lack of RUV (AF=9%), pre-dialysis systolic blood pressure (SBP) out-of-range 130–160 mm Hg (AF=8%), serum phosphorus out-of-range 3.5–5.5 mg/dL (AF=7%), and hemoglobin out-of-range 10–12 g/dL (AF=6%). Serum calcium and PTH were weakly associated with mortality, and their estimated AFs were not positive. The combined AF was higher for malnutrition (low albumin and/or low creatinine; AF=29%) than for inflammation (high ferritin and/or high WBC; AF=8%) or MBD abnormalities (serum calcium, phosphorus, and/or PTH out-of-range; AF=0%). Overall, 65% (95% CI: 59-71%) of first-year HD deaths were attributable to the risk factors in Table 2.
Compared to this “incident” cohort of vintage <60 days, the proportion of deaths attributed to all combined risk factors was lower among patients with baseline vintage >1 year (AF=46%; 95% CI: 41-50%; Table 2, right panel). Low albumin had the largest AF (15%). For catheter use, both the prevalence (15% vs 57%) and magnitude of the association (HR = 1.22 vs 1.52) were smaller among patients with baseline vintage >1 year vs <60 days, resulting in a much smaller AF (4% vs 22%). In contrast, the AF for MBD abnormalities was larger in the cohort with baseline vintage >1 year vs <60 days (17% vs 0%), driven by stronger associations of calcium and PTH abnormalities with mortality. The combined AF (95% CI) was 62% (56%-67%) among patients with baseline vintage 60 days to 1 year (Supplementary Table 1).
Among incident HD patients, we found a similar combined AF in North America (AF=66%) and Europe/ANZ (AF=62%) (Table 3). The AFs for individual risk factors were most different between regions for no RUV (11% in North America vs 3% in Europe/ANZ), due to higher prevalence of no RUV in North America, and out-of-range hemoglobin (3% in North America vs 14% in Europe/ANZ), due to stronger HR for Hgb <10 g/dL in Europe/ANZ. When further stratifying the North America results by race, we found that the combined AF was 77% (95% CI: 62%-87%) among black patients and 64% (95% CI: 54%-72%) among non-black patients; the AF for most individual risk factors was larger among black patients (Supplementary Table 3). The combined AF (95% CI) was 65% (57%-72%) in DOPPS phases 1–2 (1996–2004) and 68% (56%-76%) in DOPPS phases 3–5 (2005–2015) (Supplementary Table 2). Notable differences included a greater contribution of catheter use (AF=29% vs 19%) and high ferritin (AF=6% vs 1%) and a smaller contribution of phosphorus abnormalities (AF=3% vs 9%) using more recent data (phases 3–5 vs phase 1–2).
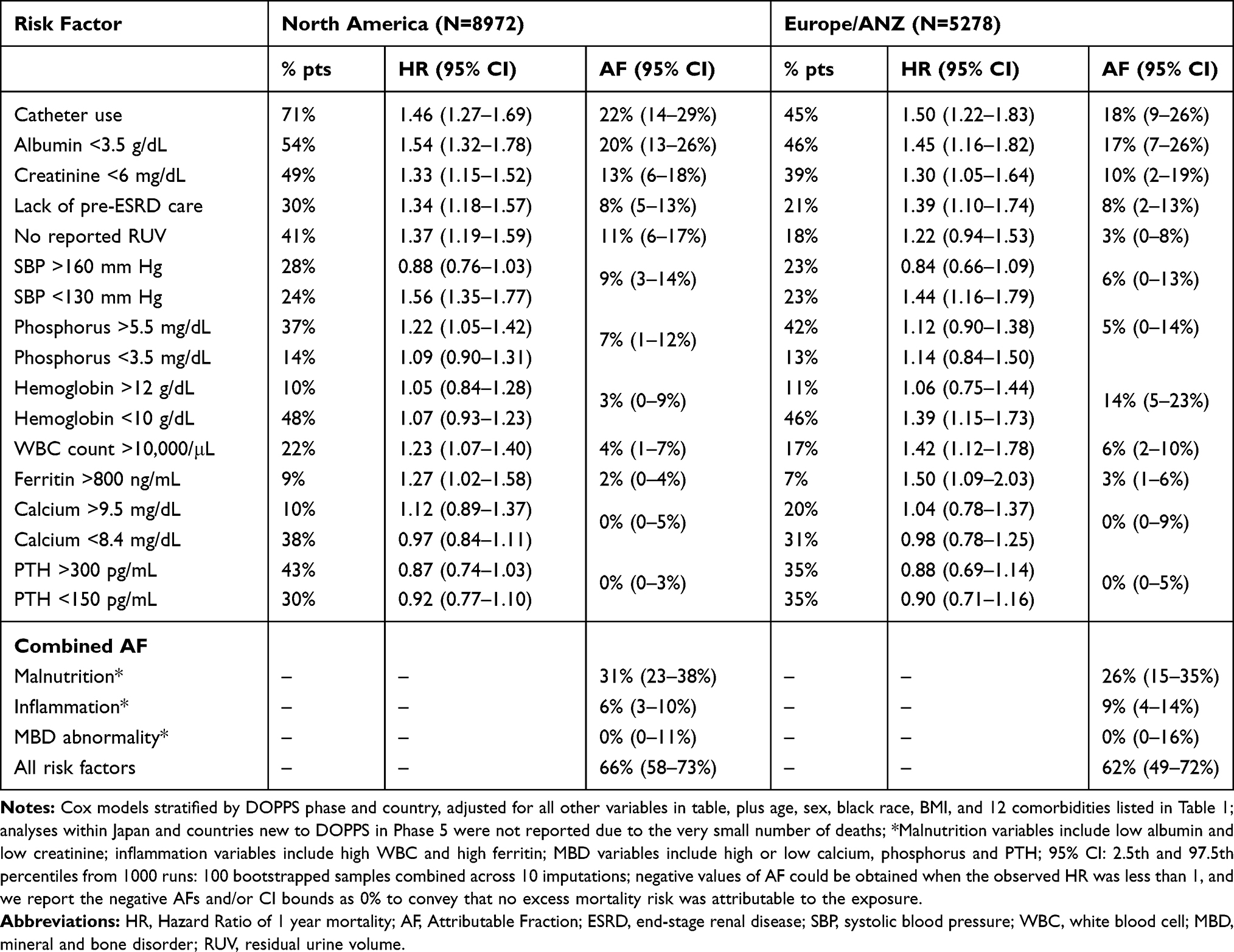 |
Table 3 Attributable Fractions for Mortality Risk-Factors Among Incident (<60 Days Vintage) Patients, by Region |
In a subset of facilities where CRP was routinely measured, 40% of the 3,596 incident HD patients had high CRP (>10 mg/L), and the HR (95% CI) for high (vs low) CRP was 1.64 (1.21–2.22). The AF for high CRP was 21%, and the inclusion of CRP increased the “Inflammation” AF from 7% to 26% and the overall AF from 59% to 62% in this cohort (Supplementary Table 4).
Discussion
We estimated attributable fractions to identify the most important clinical risk factors that may potentially be modified to reduce the very high mortality rates in the months soon after dialysis start. Extending beyond existing literature reliant on strength of association (e.g., hazard ratio), the most important risk factors have both relatively strong associations with mortality and are relatively common (i.e., high prevalence). As such, estimates of attributable fractions provide information about potential impact of interventions that are more useful to clinical care and policy decisions. Among generally modifiable risk factors, the most important were catheter use, nutritional/inflammatory markers (serum albumin, creatinine, and CRP), lack of pre-dialysis nephrology care, and lack of RUV. Other common dialysis measures (SBP, Hgb, and phosphorus) contributed to lesser extents.
In prior DOPPS work,2 we showed that mortality is highest in the first 4 months of dialysis internationally. The mortality rate in the US still exceeds 0.25/year during the first 4 months of dialysis despite improvements over the past two decades.1 This study is, to our knowledge, the first to quantify the potential for lowering first-year HD mortality by modifying known risk factors for mortality among HD patients, using a measure of the AF appropriate for survival data.21 Risk factors with the largest AFs are both strongly associated with mortality and highly prevalent in this population.
Among practices evaluated, the largest fraction of early dialysis mortality was attributed to catheter use (AF=22%). There is widespread recognition of the dangers of catheter use,3,26 and substantial reductions in catheter use have been made and sustained over time in several countries, e.g., through programs such as the Fistula First Breakthrough Initiative (FFBI) and the CMS ESRD Quality Incentive Program in the US.27,28 Among patients with vintage >1 year, the AF for catheter use was only 4% because of much lower prevalence and a weaker association with mortality than in the early dialysis period. Nevertheless, successes targeting chronic HD patients highlight the need for practice and policy changes to promote reductions in catheter use among new dialysis starts. Catheter use in the US is remarkably high, at 80% at dialysis initiation1 and 67% in the first 60 days of HD.29 Catheter use within 60 days of HD start is also high in the GCC (81%), Belgium (71%), and Canada (68%), while low catheter use has been achieved in other countries, including Japan (11%), Italy (42%), and Germany (42%).29 In this context, our findings highlight that, in many countries, initiatives to reduce catheter use may be the most important means to improve outcomes in new dialysis patients, and that reduction among incident patients should be prioritized over much smaller gains that may be realized in longer-term patients.
Lack of pre-ESRD nephrology care had an AF of 9%, highlighting the need to improve access to care for patients at high risk for ESRD. Both longer pre-ESRD nephrology care and greater frequency of patient-nephrologist contact prior to ESRD have been linked to lower first-year mortality.6,30 The proportion of patients starting dialysis with little or no pre-ESRD nephrology care remains high in the US, at 26% in 2015, though improved from 32% in 2011.5,31 The true AF for absent pre-ESRD nephrology care is likely higher than our estimate of 9%, because the statistical model included potential mediators on the causal pathway between pre-ESRD nephrology care and clinical outcomes, such as AV access use and nutritional markers.
AFs for low serum albumin and creatinine levels were 19% and 12%, respectively, highlighting the need to optimize nutrition and physical condition for patients approaching kidney failure and after starting dialysis.32 The prevalence, and consequently the AF, of these risk factors was lower among patients on dialysis >1 year, likely due to early death of older and frail patients.
We found an AF of 21% for CRP >10 mg/L, higher than for other inflammatory indicators (5% for WBC >10,000/μL, 2% for ferritin >800 ng/mL). These results highlight the importance of inflammation, and suggest the value of measuring CRP in the clinic. In contrast to North America, many nephrologists in Europe and Japan appear to have incorporated CRP years ago into the panel of data that routinely inform decision-making in clinical dialysis practice.
Non-monotonic associations of several laboratory and biometric measures with mortality have been reported previously and merit mention in the context of this study. Both low and high pre-dialysis SBP are common (>20%), but the association with elevated mortality is much clearer for low than high SBP.2,33 Though confounding due to poor health status partly explains the association at lower SBP levels, greater emphasis on limiting treatment-related hypotension appears warranted; doing so soon after HD initiation can have additional value by preserving RUV. Other potential interventions to preserve RUV include starting patients on incremental dialysis and avoiding hemodynamic instability by managing the ultrafiltration volume on HD. While it is not realistic to restore RUV to prevalent HD patients, these potential steps can be taken at or around the time of dialysis initiation.
While both low and high phosphorus are associated with elevated mortality, high phosphorus (>5.5 mg/dL) is exceptionally common at ~40% across dialysis vintages, so therapy directly targeting hyperphosphatemia should be a priority before and after initiating HD.34 Management of low phosphorus (<3.5 mg/dL, prevalence ~10%) is part of broader nutritional interventions targeting low serum albumin, low serum creatinine, and other measures. The AF for other MBD markers – PTH and serum calcium – was larger in the vintage >1 year cohort than during the first year of dialysis, potentially explained in part by the accumulation of calcium leading to vascular calcification. Consensus regarding hemoglobin targets has settled generally in the 10–12 g/dL range.35,36 In our analysis, the AF for hemoglobin is highest in the first year of HD (6%), driven by an excess of patients (50%) with hemoglobin <10 g/dL at or near HD initiation. Anemia of kidney disease tends to be undertreated in the non-dialysis setting, with “catch up” treatment after dialysis start.1 The current analysis supports the potential value of treating patients earlier in the transition to kidney failure.
Consideration of our findings is warranted in the context of real-world efforts to improve outcomes. Over a decade ago, the RightStart program was a US-based systematic case management approach during the first three months of dialysis that achieved reductions in first-year mortality, though it was unclear which of the program’s interventions were most effective.15,16 Focus in the US in recent years has been on ESRD Seamless Care Organizations (ESCO), which carry accountability for clinical and financial outcomes for Medicare dialysis beneficiaries as part of Medicare’s accountable care organization demonstration projects.37 To increase their impact, some ESCOs have been moving “upstream” to provide education and other services for CKD patients not yet on dialysis,18,19 reflecting the recognition that improving outcomes on dialysis necessitates adequate preparation prior to dialysis. However, policy changes may be warranted to directly promote accountability for adequate preparation for dialysis.
Strengths of this study include uniform data collection in 21 countries. We also used state-of-the-art statistical methods for estimating AFs in a survival context and calculating confidence intervals using bootstrapped imputations. This study has some limitations. While qualitative interpretation by ranking AFs may identify highest priority targets to improve survival, the AFs should be interpreted cautiously as the maximum potential impact of eliminating each risk factor; the expected impact of doing so in practice is uncertain and is likely less than the estimated AFs.23 For example, if catheter use cannot realistically be reduced to zero because some catheter patients may not be candidates for AV access, then the expected impact of practice changes will be less than the estimated AF of 22%. Further, our AF estimates for individual risk factors may be biased due to lack of control for unmeasured risk factors, measurement error, or over-adjustment for mediators. In addition, AF estimates for continuous risk factors depend on how cutpoints are defined. We relied on previous findings and guidelines for target values to categorize these risk factors.
The goal of this study was not to identify interventions that most effectively reduce or eliminate key risk factors; these are important next steps. In some cases, directed treatments merit study, such as preserving RUV by minimizing exposure to intradialytic hypotension and nephrotoxic agents. To reduce catheter use, multilevel interventions may be required, including optimizing technical approaches, facility practices and services, patient and family education, and promoting a “culture” of fistula use.17,29,38,39 Risk factors such as low serum albumin and creatinine levels, reflecting poor nutrition and frailty, can have socioeconomic as well as medical determinants, and reducing disparities related to social support, access to care, and health care coverage (in the US and certain other countries) merits attention.18,19
The key innovation of this study was to identify the most important clinical risk factors for first-year dialysis mortality from a population health perspective, doing so using attributable fractions that incorporate risk-factor prevalence rather than strength of association alone. Our findings indicate that a substantial proportion of the first-year deaths among HD patients could be potentially prevented by favorably altering the distribution of several modifiable risk factors, prioritizing attention to risk factors that have the greatest impact. These include reducing catheter use, raising pre-ESRD nephrology care, avoiding or treating malnutrition/inflammation, and preserving RUV. Focus on interventions that most effectively reduce these key risk factors may impact mortality in the first year of hemodialysis and beyond.
Acknowledgments
Jennifer McCready-Maynes, an employee of Arbor Research Collaborative for Health, provided editorial assistance for this paper. The results presented in this paper have not been published previously in whole or part, except in abstract format. The abstract was presented as part of ASN’s Kidney Week 2018. The citation is: Robinson BM, Morgenstern H, Karaboyas A, Li Y, Bieber B, Hakim RM, Hasegawa T, Jadoul M, Schaeffner E, Vanholder R, Pisoni RL. Estimating the fraction of first-year hemodialysis deaths attributable to potentially modifiable risk factors: results from the DOPPS [abstract]. J Am Soc Nephrol. 2018;29: 629-630.
Disclosure
Friedrich K Port has a consultancy contract with Arbor Research Collaborative for Health. Hal Morgenstern is consultant at Arbor Research Collaborative for Health. Takeshi Hasagawa has consulted for Kyowa Hakko Kirin, received research funding from JSPS KAKENHI (Grant Number 15K00877) and received speaker honoraria from Kyowa Hakko Kirin, Chugai Pharmaceutical, Torii Pharmaceutical, and Daiichi-Sankyo Pharmaceutical. Raymond Vanholder has received travel support and speaker’s honoraria from B. Braun and Nikisho. Michel Jadoul has served as a consultant for Astellas, MSD, Vifor Fresenius Medical Care Renal Pharma, received grant/research support from Amgen, Astra-Zeneca, Janssen-Cilag, MSD, Otsuka, Roche, been a speaker for AbbVie, Amgen, Menarini, MSD, Vifor Fresenius Medical Care Renal Pharma, received travel compensation from Amgen; all monies paid to institution including non-financial support from Sanofi-Genzyme, outside the submitted work. Elke Schaeffner reports speaker honorarium from Fresenius Medical Care, Fresenius Kabi, Siemens healthineers and grants from E.N.D.I foundation and DDnÄ, outside the submitted work. Angelo Karaboyas, Bruce M. Robinson, Ronald L Pisoni, Brian A. Bieber are employees of Arbor Research Collaborative for Health, which administers the DOPPS. Angelo Karaboyas reports grants from Akebia Therapeutics, Amgen, AstraZeneca, Bard Peripheral Vascular, Baxter Healthcare, Bayer Yakuhin, Chugai Pharmaceutical, Fresenius Medical Care Asia-Pacific, Japanese Society for Peritoneal Dialysis, JMS Co, Kidney Research UK, Kidney Foundation Japan, Kissei Pharmaceutical Co, Kyowa Kirin Co, MEDICE Arzneimittel Pütter GmbH & Co KG, Nikkiso, ONO Pharmaceutical Co, Sanofi-Aventis Deutschland GmbH, Terumo Corporation, Torii Pharmaceutical Co, Vifor-Fresenius Medical Care Renal Pharma Ltd, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. United States Renal Data System. 2017 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. Bethesda, MD; 2017.
2. Robinson BM, Zhang J, Morgenstern H, et al. Worldwide, mortality risk is high soon after initiation of hemodialysis. Kidney Int. 2014;85(1):158–165. doi:10.1038/ki.2013.252
3. Bradbury BD, Fissell RB, Albert JM, et al. Predictors of early mortality among incident US hemodialysis patients in the dialysis outcomes and practice patterns study (DOPPS). Clin J Am Soc Nephrol. 2007;2(1):89–99. doi:10.2215/CJN.01170905
4. Foley RN, Chen SC, Solid CA, Gilbertson DT, Collins AJ. Early mortality in patients starting dialysis appears to go unregistered. Kidney Int. 2014;86:392–398. doi:10.1038/ki.2014.15
5. United States Renal Data System. 2017 USRDS Annual Data Report: Reference table – 2017 – vol 2, table c, patient characteristics.
6. Hasegawa T, Bragg-Gresham JL, Yamazaki S, et al. Greater first-year survival on hemodialysis in facilities in which patients are provided earlier and more frequent pre-nephrology visits. Clin J Am Soc Nephrol. 2009;4(3):595–602. doi:10.2215/CJN.03540708
7. Slinin Y, Guo H, Gilbertson DT, et al. Meeting KDOQI guideline goals at hemodialysis initiation and survival during the first year. Clin J Am Soc Nephrol. 2010;5(9):1574–1581. doi:10.2215/CJN.01320210
8. Hwang SJ, Yang WC, Lin MY, Mau LW, Chen HC. Impact of the clinical conditions at dialysis initiation on mortality in incident haemodialysis patients: a national cohort study in Taiwan. Nephrol Dial Transplant. 2010;25(8):2616–2624. doi:10.1093/ndt/gfq308
9. Gillespie BW, Morgenstern H, Hedgeman E, et al. Nephrology care prior to end-stage renal disease and outcomes among new ESRD patients in the USA. Clin Kidney J. 2015;8:772–780. doi:10.1093/ckj/sfv103
10. Cooper BA, Branley P, Bulfone L, et al. A randomized, controlled trial of early versus late initiation of dialysis. N Engl J Med. 2010;363:609–619. doi:10.1056/NEJMoa1000552
11. Mehrotra R, Rivara M, Himmelfarb J. Initiation of dialysis should be timely: neither early nor late. Semin Dial. 2013;26:644–649.
12. National Kidney Foundation. NKF-DOQI clinical practice guidelines for peritoneal dialysis adequacy. Am J Kidney Dis. 1997;30(3Suppl 2):S67–136. doi:10.1016/S0272-6386(97)70028-3
13. National Kidney Foundation. KDOQI clinical practice guideline for hemodialysis adequacy: 2015 update. Am J Kidney Dis. 2015;66:884–930. doi:10.1053/j.ajkd.2015.07.015
14. Rosansky S, Glassock RJ, Clark WF. Early start of dialysis: a critical review. Clin J Am Soc Nephrol. 2011;6(5):1222–1228. doi:10.2215/CJN.09301010
15. Wingard RL, Pupim LB, Krishnan M, et al. Early intervention improves mortality and hospitalization rates in incident hemodialysis patients: rightStart program. Clin J Am Soc Nephrol. 2007;2(6):1170–1175. doi:10.2215/CJN.04261206
16. Lacson E
17. Watanabe Y, Yamagata K, Nishi S, et al. Hemodialysis initiation for maintenance hemodialysis” Guideline Working Group, Japanese Society for Dialysis Therapy: Japanese Society for Dialysis Therapy Clinical Guideline for Hemodialysis Initiation for Maintenance Hemodialysis. Ther Apher Dial. 2015;19:93–107. doi:10.1111/tap.2015.19.issue-s1
18. Johnson DS, Kapoian T, Taylor R, Meyer KB. Going upstream. Semin Dial. 2016;29(2):125–134. doi:10.1111/sdi.12461
19. Berns JS, Glickman JD, Reese PP. Dialysis payment model reform: managing conflicts between profits and patient goals of care decision making. Am J Kidney Dis. 2018;71(1):133–136. doi:10.1053/j.ajkd.2017.04.024
20. Young EW, Goodkin DA, Mapes DL, et al. The Dialysis Outcomes and Practice Patterns Study (DOPPS): an international hemodialysis study. Kidney Int. 2000;57(suppl74):
21. Pisoni RL, Gillespie BW, Dickinson DM, et al. The Dialysis Outcomes and Practice Patterns Study (DOPPS): design, data elements, and methodology. Am J Kidney Dis. 2004;44(Suppl 2):7–15. doi:10.1016/S0272-6386(04)01099-6
22. Samuelsen SO, Eide GE. Attributable fractions with survival data. Stat Med. 2008;27(9):1447–1467. doi:10.1002/(ISSN)1097-0258
23. Morgenstern H. Attributable fractions. In: Boslaugh S, editor. Encyclopedia of Epidemiology. Vol. 1. Thousand Oaks, CA: Sage Publications; 2008:55–63.
24. Raghunathan TE, Solenberger PW, Van Hoewyk J. IVEware: Imputation and Variance Estimation Software: User Guide. Ann Arbor, MI: Institute for Social Research, University of Michigan; 2002.
25. Schomaker M, Heumann C. Bootstrap inference when using multiple imputation. Statistics in medicine. 2018;37(14):2252–2266.
26. Ng LJ, Chen F, Pisoni RL, et al. Hospitalization risks related to vascular access type among incident US hemodialysis patients. Nephrol Dial Transplant. 2011;26(11):3659–3666. doi:10.1093/ndt/gfr063
27. Centers for Medicare & Medicaid Services. ESRD Quality Incentive Program. Available from: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/ESRDQIP/index.html.
28. ESRD National Coordinating Center. Fistula first catheter last. Available from: https://esrdncc.org/en/fistula-first-catheter-last/.
29. Pisoni RL, Zepel L, Port FK, Robinson BM. Trends in US vascular access use, patient preferences, and related practices: an update from the US DOPPS practice monitor with international comparisons. Am J Kidney Dis. 2015;65(6):905–915. doi:10.1053/j.ajkd.2014.12.014
30. Kausz AT, Guo H, Pereira BJ, Collins AJ, Gilbertson DT. General medical care among patients with chronic kidney disease: opportunities for improving outcomes. J Am Soc Nephrol. 2005;16(10):3092–3101. doi:10.1681/ASN.2004110910
31. Mendelssohn DC, Curtis B, Yeates K, et al. Suboptimal initiation of dialysis with and without early referral to a nephrologist. Nephrol Dial Transplant. 2011;26(9):2959–2965. doi:10.1093/ndt/gfq843
32. Fink JC, Burdick RA, Kurth SJ, et al. Significance of serum creatinine values in new end-stage renal disease patients. Am J Kidney Dis. 1999;34(4):694–701. doi:10.1016/S0272-6386(99)70395-1
33. Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Work Group. KDIGO clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Inter. 2012;2:337–414.
34. Tentori F, Blayney MJ, Albert JM, et al. Mortality risk for dialysis patients with different levels of serum calcium, phosphorus, and PTH: the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis. 2008;52(3):519–530. doi:10.1053/j.ajkd.2008.03.020
35. US Food and Drug Administration; US Department of Health and Human Services: FDA Drug Safety Communication: Modified Dosing Recommendations to Improve the Safe Use of Erythropoiesis-Stimulating Agents (ESAs) in Chronic Kidney Disease. Safety Announcement 6/24/2011. Available from: http://www.fda.gov/drugs/drugsafety/ucm259639.htm.
36. Kidney Disease: Improving Global Outcomes (KDIGO) Anemia Work Group. KDIGO clinical practice guideline for anemia in chronic kidney disease. Kidney Inter. 2012;2:279–335.
37. ESCO. Available from: https://innovation.cms.gov/initiatives/comprehensive-esrd-care/.
38. Pisoni RL, Zepel L, Fluck R, et al. International differences in the location and use of arteriovenous accesses created for hemodialysis: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis. 2018;71(4):469–478. doi:10.1053/j.ajkd.2017.09.012
39. Woodside KJ, Bell S, Mukhopadhyay P, et al. Arteriovenous fistula maturation in prevalent hemodialysis patients in the United States: a national study. Am J Kidney Dis. 2018;71(6):793–801. doi:10.1053/j.ajkd.2017.11.020
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.