")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 15
Estimating the Cost of Spinopelvic Complications After Adult Spinal Deformity Surgery
Authors Zuckerman SL, Cher D , Capobianco R, Sciubba D, Polly DW
Received 20 September 2023
Accepted for publication 1 November 2023
Published 9 November 2023 Volume 2023:15 Pages 765—772
DOI https://doi.org/10.2147/CEOR.S437202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Samer Hamidi
Scott L Zuckerman,1 Daniel Cher,2 Robyn Capobianco,2 Daniel Sciubba,3 David W Polly4
1Department of Neurological Surgery, Vanderbilt University Medical Center, Nashville, TN, USA; 2SI-BONE, Inc, Santa Clara, CA, USA; 3Department of Neurosurgery, Zucker School of Medicine at Hofstra, Long Island Jewish Medical Center and North Shore University Hospital, Northwell Health, Manhasset, NY, USA; 4Department of Orthopaedic Surgery, University of Minnesota, Minneapolis, MN, USA
Correspondence: Scott L Zuckerman, Department of Neurological Surgery, Vanderbilt University Medical Center, Nashville, TN, USA, Email [email protected]
Objective: Reoperations for spinopelvic failure after adult spinal deformity (ASD) surgery are common. We sought to determine the added costs of ASD surgery attributable to reoperations for spinopelvic construct failures.
Methods: We constructed a Markov process model to calculate the expected discounted 5-year costs of spinopelvic construct failures after ASD surgery. The Nationwide Inpatient Sample (NIS) was queried to estimate the number of ASD surgeries. Model inputs were based on literature review and expert opinion. ASD surgery was defined as thoracolumbar fusion of 4 or more levels with pelvic fixation. The following pelvic fixation failures were included: 1) rod fracture or pseudarthrosis from L4-S1, 2) iliac screw failure or set plug dislodgment, 3) iliac screw prominence, and 4) sacroiliac (SI) joint pain. The number of patients undergoing ASD surgery annually in the US was determined using a commercial claims database.
Results: The net present value 5-year cost per patient for spinopelvic complications was $35,265, equal to 29% of index surgery costs. Given an estimated 27,580 cases annually in the US, the additional cost to address spinopelvic complications reach nearly $1 billion over 5-years. A sensitivity analysis showed that these costs were most sensitive to the rate of rod fracture/pseudarthrosis, iliac screw prominence, and reoperation.
Conclusion: A conservative estimate of the cost of spinopelvic failures after ASD surgery is substantial, nearly $1 billion over 5-years. We propose a method of capturing spinopelvic fixation failures for use in future clinical studies and cost analyses.
Keywords: spinopelvic, sacroiliac, deformity surgery
A Letter to the Editor has been published for this article.
Introduction
Though adult spinal deformity surgery (ASD) has potential to provide major improvements in quality of life,1 complications and healthcare costs surgery remain high.1–3 Complication rates have been reported to be as high as 60–70%,4,5 with approximately 20% requiring reoperation.6 Even after a successful perioperative recovery, the risk of longer-term complications such as proximal junctional kyphosis (PJK), implant failure, pseudarthrosis, and rod fracture lingers.
The number of ASD surgeries performed each year is rising, which in turn increases healthcare spending associated with ASD surgery.7 The mean cost of an index ASD surgery ranges from approximately $60-80,000, with revision surgeries adding on approximately $50,000.3,8 Surgery for degenerative scoliosis has been described as the most expensive type of ASD surgery at $85,010, followed closely by idiopathic scoliosis at $70,531 and sagittal plane deformities $70,776.3,9 While PJK is a common complication after ASD surgeries, failure at the spinopelvic region encompasses a range of pathologies that are less described and often require reoperation.
Several aspects of spinopelvic constructs can fail, and reoperations to address such failures are common. Failures span L4 to the sacrum and include rod fracture, iliac screw breakage, iliac screw pullout or prominence, set screw dislodgement, and sacroiliac joint (SIJ) pain. Together these can result in high overall rates of failure, as high as 24% in a recent multicenter study.10 Revision surgeries to address spinopelvic failure can be very expensive, totaling as high as $86,673.2 We sought to better understand the economic impact of spinopelvic failures after ASD surgery, both on a per-patient basis and from an overall US healthcare perspective.
Methods
Study Design
We combined literature-based estimates of probabilities of various types of spinopelvic fixation failures after ASD surgery with expert opinion in a Markov model to estimate expected costs over a 5-year postoperative time period. We then used the number of surgeries derived from the Nationwide Inpatient Sample (NIS) database to calculate the total national economic impact of spinopelvic failures after ASD surgery. The NIS, available through the Healthcare Research and Quality (AHRQ), is a publicly available all-payer inpatient care database in the United States. This limited dataset does not include physician or patient identifiers and its use does not meet the criteria for research involving human subjects. The database was only queried for the number of surgeries; no further analysis was performed. Finally, as this is a cost estimate study and not an evaluation of a device or drug, it is not covered under US 21 CFR Part 56. Therefore, the performed analysis is exempt from Institutional Review Board review.
Modeled Spinopelvic Complications
We sought to comprehensively describe all possible spinopelvic complications after ASD surgery. Several reports have been written on spinopelvic failure, yet the literature is heterogenous, and most studies include different types of spinopelvic complications. Due to the relatively non-specific nature of available published reports, we modeled one set of acute complications and three long-term complications.
Acute Spinopelvic Complications
- Iliac screw/set screw failure. In a single-center study,2 Martin et al reported a 5% rate of acute complications consisting of rod slippage with and without set screw dissociation, and often associated with caudal sacral fracture. In a subsequent multicenter report on the same topic, Martin et al11 reported a similar 5% acute failure rate consisting of rod slippage or set screw loosening (17 cases, 2.2%), screw shaft breakage (9 cases, 1.2%), screw loosening (9 cases, 1.2%) and sacral fracture (6 cases, 0.8%). All cases in both studies underwent revision surgery. We modeled these findings generally as acute fixation failures (ie, set screw dislodgement with or without rod slippage, screw breakage, lumbosacral rod breakage, or sacral/iliac fracture). We assumed a $40,000 surgical cost for revision surgery associated with acute spinopelvic failures; this was based on a figure reported by Yermaneni.2
Long-Term Spinopelvic Complications
Representative cases for each of these complications are provided in Figures 1–4.
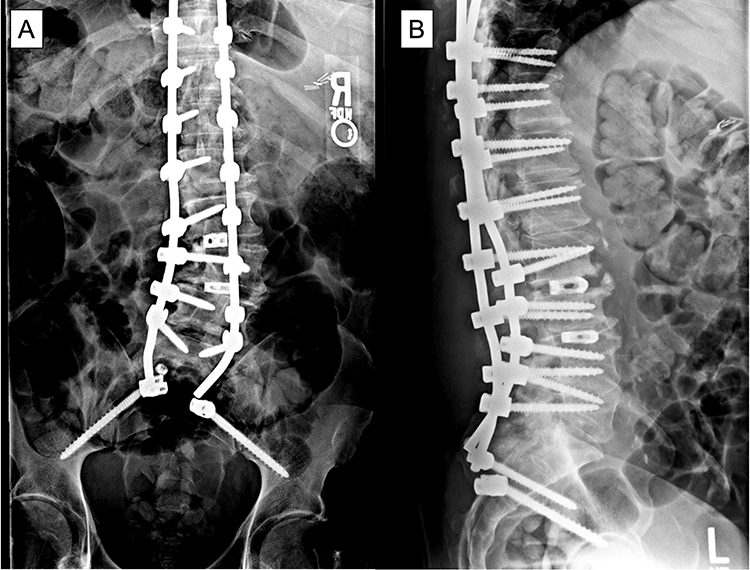 |
Figure 1 Patient underwent T10-ilium PSIF. Two weeks postoperatively, he experienced acute onset of low back pain while getting up from chair. (A) PA and (B) lateral x-rays showed pullout of right rod from S2AI screw and set screw popped off from R S2AI screw. Of note, S1 screws are missing, which may have led to the acute iliac screw failure. |
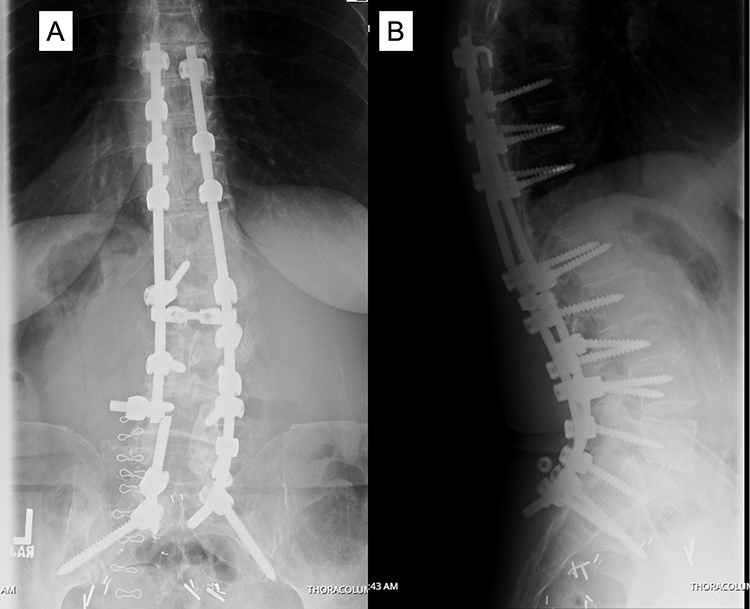 |
Figure 2 (A) PA and (B) lateral x-ray of patient who underwent T8-pelvis fusion and 2-years postoperatively experienced rod fracture at L4/5 on the left and pseudoarthrosis requiring reoperation. Of note, the right iliac set screw has also popped off. |
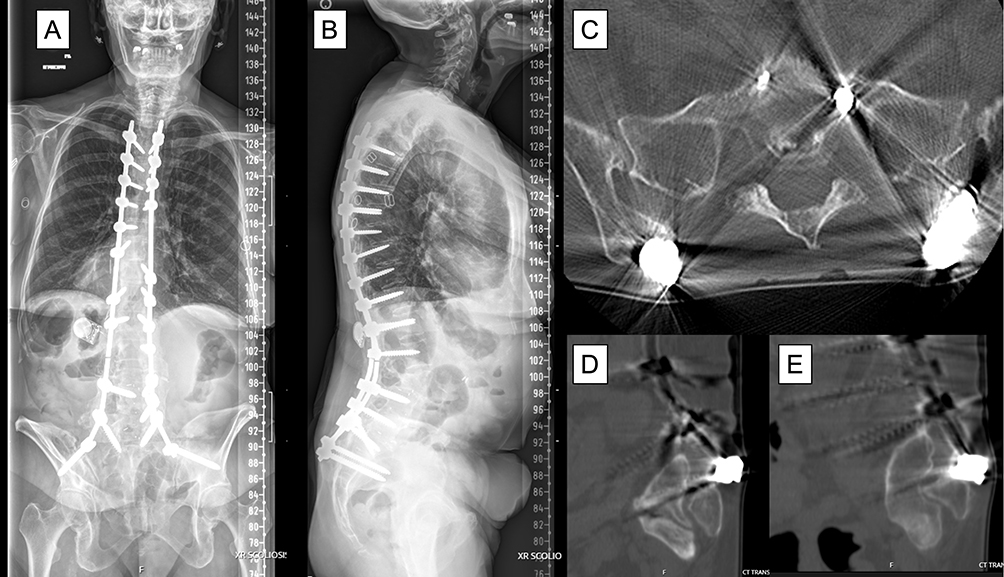 |
Figure 3 (A and B) Patient who underwent a T5-ilium PSIF in 2013 with solid fusion. Nine years later she experienced prominence of her iliac instrumentation and skin breakdown. (C) Axial CT scan shows iliac screws close to the skin, with sagittal CT scans of the (D) right and (E) left screws eroding through the skin. The rods were cut proximal the screw, the screws were removed, and plastic surgery rotated paraspinal muscle flaps for closure. Of note, the unilateral left L3 rod fracture was asymptomatic. |
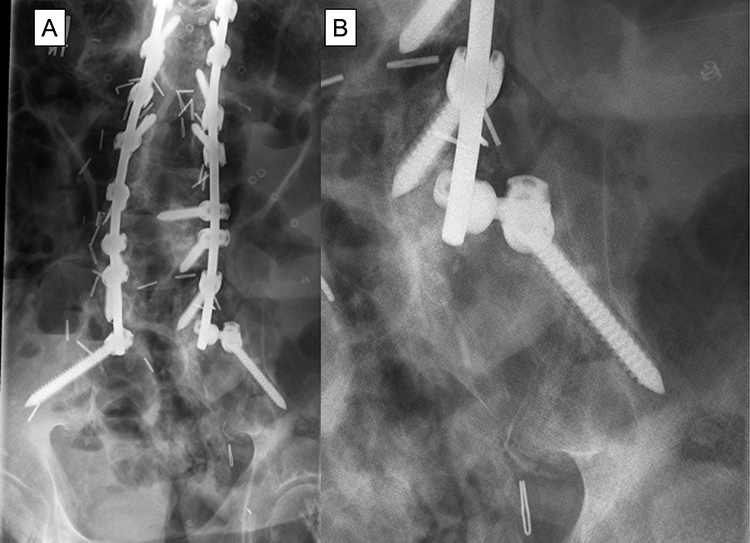 |
Figure 4 (A) PA x-ray in patient who underwent lumbosacral deformity surgery showing radiolucency in the right iliac screw. (B) Enlarged view of the right iliac screw lucency. This patient developed sacroiliac joint (SIJ) pain that was improved with SIJ injections. |
For each of the above health transitions, we included a transition cost, based on expert opinion, representing expected costs of diagnosis, which can include physician visits, radiographic studies and, for SI joint pain, diagnostic SI joint block.
Patient Population
The National Inpatient Sample (NIS) publicly available database was queried to estimate the number of ASD operations performed annually in the US. MS-DRGs 456, 457, and 458 were selected as these denote spinal curvature and complex spinal fusion surgery, typically for deformity. These DRGs comprise 74 deformity-related ICD-10 codes. This query returned 27,885 and 27,560 surgeries for the years 2019 and 2020, respectively. For the purposes of modeling, we assumed 27,580 ASD surgeries annually. The NIS database contains no personally identifiable information or patient outcomes; it consists of codes for procedures. Institutional review board approval was not required given the public nature of the database.
Statistical Analysis
We created a Markov model in Microsoft Excel. The model includes a transition probability matrix, costs associated with diagnosis of the failure of interest and a vector of costs associated with treatment of each failure. Future costs were discounted by 3% per year. Model parameters were adjusted so that cumulative rates of each event matched those reported in Table 1. We report cumulative 5-year discounted costs. One-way sensitivity analysis was performed using ranges based on either literature review or expert opinion.
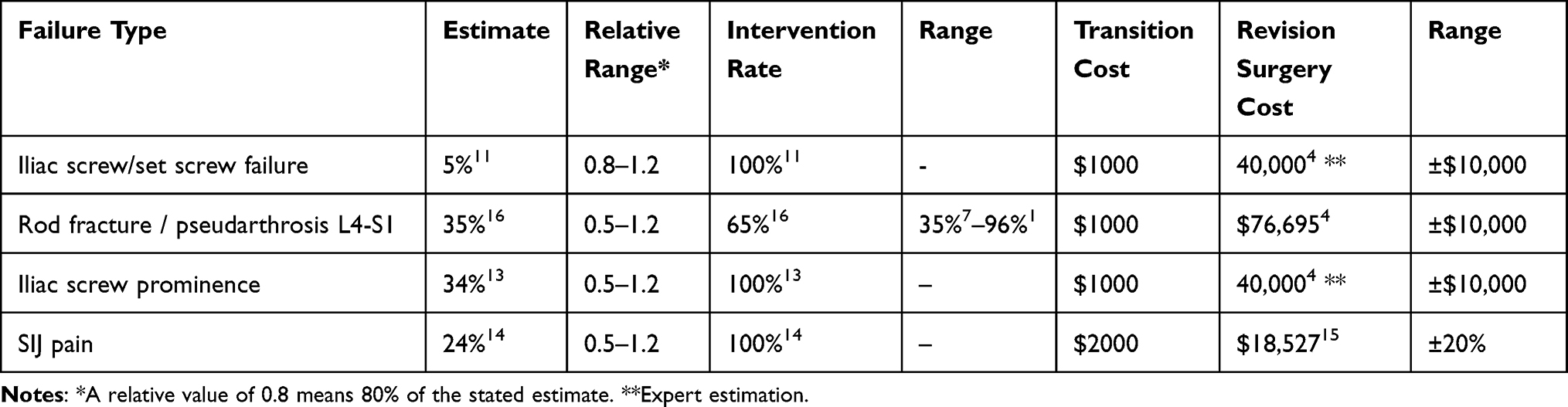 |
Table 1 Incidence, Intervention Rate, and Cost of Four Modes of Spinopelvic Failure |
Results
The base case cumulative per-patient discounted 5-year costs of spinopelvic fixation failures was $34,177. Assuming ASD surgery incurs costs of $123,000,14 the additional costs represent 28% of index surgery costs. Assuming approximately 27,580 patients undergoing ASD surgery annually in the US, the 5-year discounted costs represent $0.94 billion per year.
One-way sensitivity analysis was performed using the ranges listed in Table 1. The model was sensitive to several assumptions (Figure 5). Expected costs ranged from slightly less than $30,000 to slightly more than $40,000. Expressed as a percentage, the lowest additional excess cost due to postoperative complications was 23% of the cost of index surgery; the highest additional excess cost was 33%.
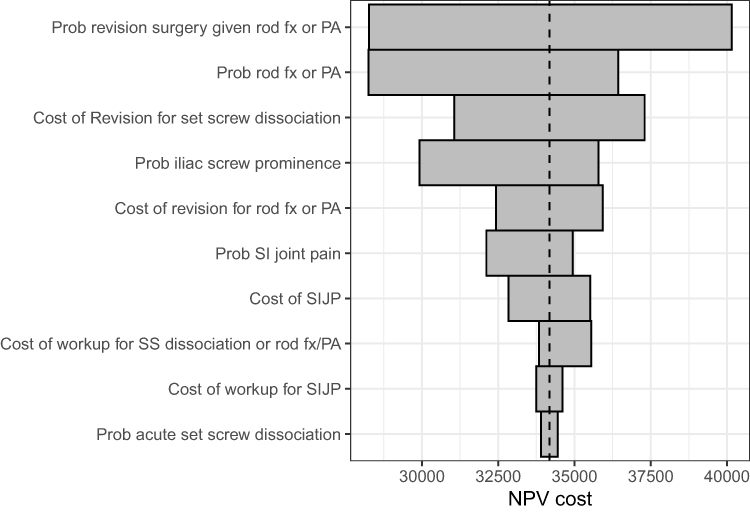 |
Figure 5 Tornado plot illustrating model sensitivities. Abbreviations: NPV, Net Present Value; PA, pseudarthrosis; Prob, probability; SS, set screw; fx, fracture. |
Discussion
Spinopelvic complications after ASD surgery are common. Our model indicates that these complications represent a substantial portion of index surgery costs (28%) and account for very high US healthcare expenditures (~$1 billion). The magnitude of estimated costs for spinopelvic fixation failures was not a surprise; however, these costs are concerning given the increasing use of surgery for ASD and the increasing age of patients undergoing ASD surgery, who are presumably at higher risk for complications. Techniques and technologies to reduce the risk of spinopelvic complications are in high need. Due to the variable and insufficient reporting of outcomes in published literature, our model was necessarily relatively simplistic. Moreover, sensitivity analysis showed that the model was sensitive to estimates of key input parameters. These findings highlight the importance of both improved reporting of spinopelvic failure outcomes and more precise definitions of failure types.
Spinopelvic failure after ASD surgery is an understudied complication that often requires reoperation. One potential barrier to further study is the heterogenous definition of these complications. Several prior studies have defined spinopelvic failures, in slightly different ways.10,12 Some studies have focused on iliac fixation failure,10 whereas others have focused on rod fracture16 or SIJ pain.14 Cho et al12 defined major lumbopelvic failure as rod breakage between L4-S1, failure of S1 screws (breakage, halo, pullout), and prominent iliac screws requiring removal, which occurred in 12% of their 67 patient series. Minor failures did not require surgery and included rod breakage between S1 and iliac screws and failure of iliac screws, occurring in 22% of patients. A multicenter study by Martin et al11 reported a rate of 5% for catastrophic iliac screw failure, which included set screw dislodgment and acute iliac screw failure. Regarding L4-S1 rod fracture or pseudarthrosis, Sardi et al16 reported 39% rod fracture rate in 160 patients; 72% of rod fractures occurred at L3 or below.17 Specific to sacral and iliac fixation, Eastlack et al10 reported a 24% complication rate involving iliac or S1 screws after ASD surgery. Lastly, with respect to iliac screw prominence, though these are more common with classically described iliac bolts rather than S2-alar-iliac screws or medial iliac screws, Tsuchiya et al13 reported that 23% of patients required iliac screw removal.
While complications after ASD surgery have been reported to add considerable financial burden to healthcare systems, cost studies remain sparse. McCarthy et al3 estimated the direct costs of four types of ASD surgery – revision 38%, idiopathic 32%, degenerative 19%, sagittal 12%. Costs ranged from $10,000 to $187,000 with a mean of $72,000. Degenerative etiology was the most expensive, and surgery with fusion to the pelvis were significantly more costly ($84,735 vs $56,106, p < 0.01). Moreover, fusion to the pelvis was associated with a $60,935 increase in expected costs for an average patient 18–29 years old. In a similar paper by the same authors,9 the cost of a readmission/reoperation was $67,000 in 27% of patients, and the total costs of patients with no reoperation was approximately $100,000 versus $174,000 in patients requiring reoperation. In perhaps the most cited cost paper in ASD surgery, Yeramaneni et al2 conducted a systematic review and calculated the following cost estimates per specific complication: pseudarthrosis $84,985, PJK/F $67,420, and infection $40,765. The most expensive complication was pseudarthrosis, which also represent the majority type of complication amongst all spinopelvic failures.
Spinopelvic complications are costly due to the complexity of addressing them. Not only do most spinopelvic complications require reoperation, but these reoperations are challenging. Most involve opening the entire wound. To replace a rod that has broken or pulled out of an iliac screw, the surgeon must reopen the entire wound and replace the rods and screws. It may also include placing additional instrumentation to secure multiple points of fixation within the sacrum and ilium.
Because of the high economic and health consequences of spinopelvic failures, the pursuit of techniques and devices/procedures to reduce failure rates is critical. To better address spinopelvic failures, methods of reporting need to be improved. We propose investigators reporting spinopelvic failures use the reporting rubric presented (Table 2). Incidence rates can be calculated as proportions when follow-up rates at fixed time points are high (>95%) and with Kaplan–Meier methods when long-term follow-up is variable and subject to patient dropout. We believe it is important to report not only the occurrence of the failure but also how the failure was treated, since surgical interventions are typically far more expensive than non-surgical treatment. Finally, because each of the complications listed in the table may have multiple-risk factors, reporting such risk factors (eg, age, body mass index, bone mineral density, sagittal and coronal pelvic alignment, use of osteotomies during surgery, and degree of restoration of normal spinopelvic alignment) should also be reported.
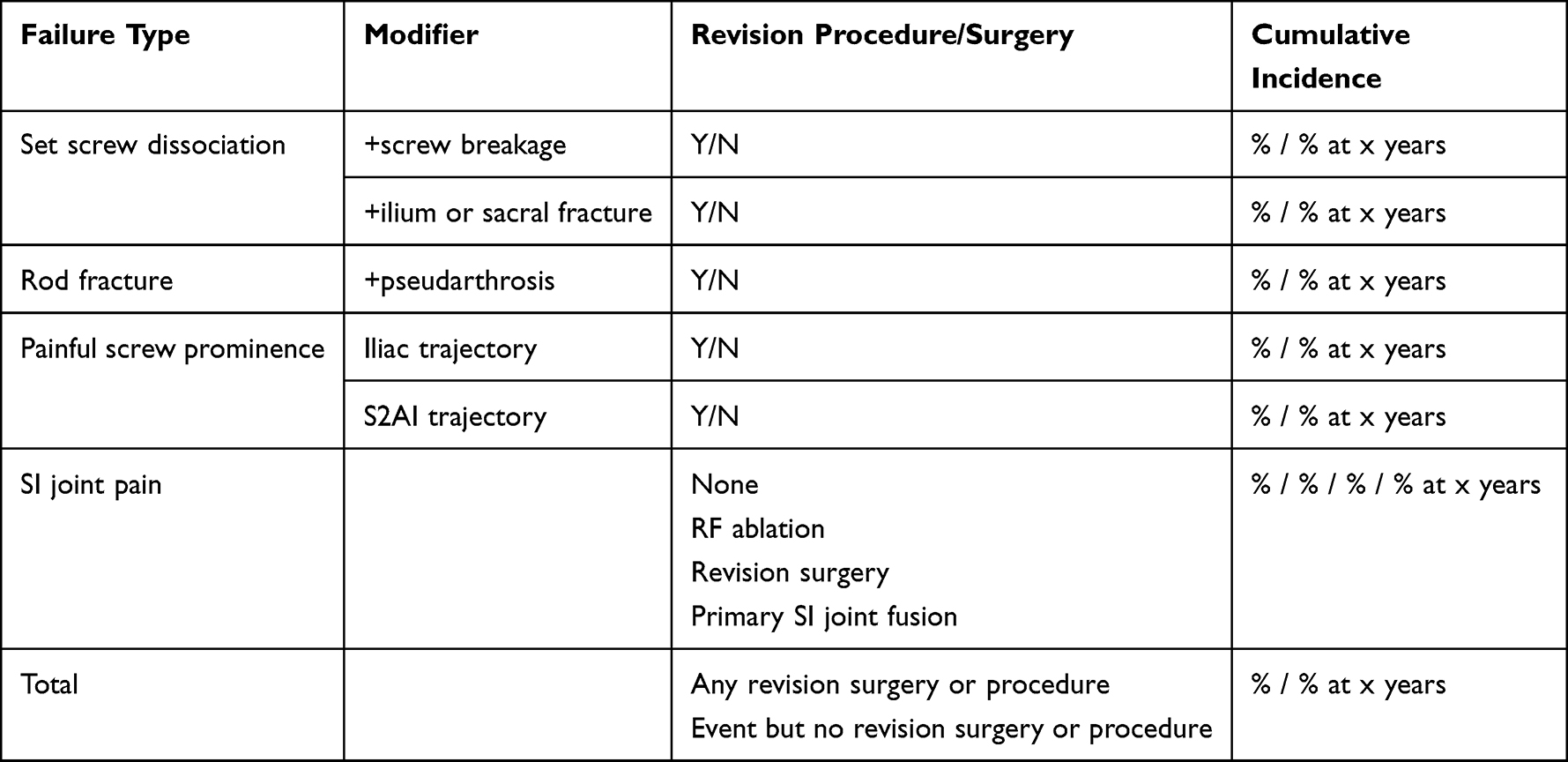 |
Table 2 Proposed Reporting Guideline for Studies of Spinopelvic Fusion Complications |
Our analysis was limited by the sparseness and variable reporting of spinopelvic failures in published reports. To date, there is no clear definition of what constitutes spinopelvic failure. In light of this heterogeneity, we have used our own definition based on prior literature as a guide. It is our hope that future papers will build upon our proposed definition to standardize how we define spinopelvic failure after ASD surgery. In addition, the sensitivity analysis performed suggests that key parameters need more precise study to improve the accuracy of our estimates. Nonetheless, because of the relatively high frequency of spinopelvic failures and their high associated treatment costs, our model results suggest that treatment strategies to prevent such failures may have marked positive economic and health consequences.
Conclusions
Spinopelvic failures after ASD surgery may add 28% over index surgery costs to overall treatment costs. The impact of spinopelvic failures on the US healthcare system is substantial.
Disclosure
Dr Daniel Cher and Dr Robyn Capobianco are employees of SI-BONE. SI-BONE manufactures devices used in spine surgery. The manuscript does not discuss these devices. Dr Daniel Sciubba reports personal fees from DePuy, Medtronic, Stryker, Nuvasive, Baxter, and SI Bone, outside the submitted work. Dr David Polly reports personal fees from SI Bone and Globus, during the conduct of the study; grants from Medtronic and MizuhoOSI, outside the submitted work. In addition, Dr David Polly has patents US 11,571,245 B2. February 7, 2023, US 11,234,830 B2. February 1, 2022, and US 11,369,419 B2. June 28, 2022 with royalties paid to SI Bone. The authors report no other conflicts of interest in this work.
References
1. Smith JS, Klineberg E, Lafage V, et al. Prospective multicenter assessment of perioperative and minimum 2-year postoperative complication rates associated with adult spinal deformity surgery. J Neurosurg Spine. 2016;25(1):1–14. doi:10.3171/2015.11.SPINE151036
2. Yeramaneni S, Robinson C, Hostin R. Impact of spine surgery complications on costs associated with management of adult spinal deformity. Curr Rev Musculoskelet Med. 2016;9(3):327–332. doi:10.1007/s12178-016-9352-9
3. McCarthy IM, Hostin RA, O’Brien MF, et al. Analysis of the direct cost of surgery for four diagnostic categories of adult spinal deformity. Spine J. 2013;13(12):1843–1848. doi:10.1016/j.spinee.2013.06.048
4. Yadla S, Maltenfort MG, Ratliff JK, Harrop JS. Adult scoliosis surgery outcomes: a systematic review. Neurosurg Focus. 2010;28(3):E3. doi:10.3171/2009.12.FOCUS09254
5. Passias PG, Soroceanu A, Yang S, et al. Predictors of revision surgical procedure excluding wound complications in adult spinal deformity and impact on patient-reported outcomes and satisfaction: a two-year follow-up. J Bone Joint Surg Am. 2016;98(7):536–543. doi:10.2106/JBJS.14.01126
6. Scheer JK, Tang JA, Smith JS, et al. Reoperation rates and impact on outcome in a large, prospective, multicenter, adult spinal deformity database: clinical article. J Neurosurg Spine. 2013;19(4):464–470. doi:10.3171/2013.7.SPINE12901
7. Zygourakis CC, Liu CY, Keefe M, et al. Analysis of national rates, cost, and sources of cost variation in adult spinal deformity. Neurosurgery. 2018;82(3):378–387. doi:10.1093/neuros/nyx218
8. Theologis AA, Miller L, Callahan M, et al. Economic impact of revision surgery for proximal junctional failure after adult spinal deformity surgery: a cost analysis of 57 operations in a 10-year experience at a Major Deformity Center. Spine. 2016;41(16):E964–E972. doi:10.1097/BRS.0000000000001523
9. McCarthy IM, Hostin RA, Ames CP, et al. Total hospital costs of surgical treatment for adult spinal deformity: an extended follow-up study. Spine J. 2014;14(10):2326–2333. doi:10.1016/j.spinee.2014.01.032
10. Eastlack RK, Soroceanu A, Mundis GM, et al. Rates of loosening, failure, and revision of iliac fixation in adult deformity surgery. Spine. 2022;47(14):986–994. doi:10.1097/BRS.0000000000004356
11. Martin CT, Holton KJ, Elder BD, et al. Catastrophic acute failure of pelvic fixation in adult spinal deformity requiring revision surgery: a multicenter review of incidence, failure mechanisms, and risk factors. J Neurosurg Spine. 2022;38(1):1–9.
12. Cho W, Mason JR, Smith JS, et al. Failure of lumbopelvic fixation after long construct fusions in patients with adult spinal deformity: clinical and radiographic risk factors: clinical article. J Neurosurg Spine. 2013;19(4):445–453. doi:10.3171/2013.6.SPINE121129
13. Tsuchiya K, Bridwell KH, Kuklo TR, Lenke LG, Baldus C. Minimum 5-year analysis of L5-S1 fusion using sacropelvic fixation (bilateral S1 and iliac screws) for spinal deformity. Spine. 2006;31(3):303–308. doi:10.1097/01.brs.0000197193.81296.f1
14. Manzetti M, Ruffilli A, Barile F, et al. Sacroiliac joint degeneration and pain after spinal arthrodesis: a systematic review. Clin Spine Surg. 2022;36(4):169–182. doi:10.1097/BSD.0000000000001341
15. Ackerman SJ, Deol GS, Polly DW. Cost-utility analysis of sacroiliac joint fusion in high-risk patients undergoing multi-level lumbar fusion to the sacrum. Clinicoecon Outcomes Res. 2022;14:523–535. doi:10.2147/CEOR.S377132
16. Sardi JP, Lazaro B, Smith JS, et al. Rod fractures in thoracolumbar fusions to the sacrum/pelvis for adult symptomatic lumbar scoliosis: long-term follow-up of a prospective, multicenter cohort of 160 patients. J Neurosurg Spine. 2023;38(2):217–229. doi:10.3171/2022.8.SPINE22423
17. Smith JS, Shaffrey E, Klineberg E, et al. Prospective multicenter assessment of risk factors for rod fracture following surgery for adult spinal deformity. J Neurosurg Spine. 2014;21(6):994–1003. doi:10.3171/2014.9.SPINE131176
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.