Back to Journals » ClinicoEconomics and Outcomes Research » Volume 16
Estimating Costs Associated with Adverse Events in Patients with Advanced Lung Cancer
Authors Lin CY, Wu TI, Yang SC ![]()
Received 2 August 2024
Accepted for publication 17 October 2024
Published 19 October 2024 Volume 2024:16 Pages 761—769
DOI https://doi.org/10.2147/CEOR.S489783
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Samer Hamidi
Chien-Yu Lin,1 Tzu-I Wu,1,2 Szu-Chun Yang1
1Division of Thoracic Medicine, Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 2Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan
Correspondence: Szu-Chun Yang, Email [email protected]
Purpose: This study aimed to estimate the costs associated with adverse events (AEs) in advanced lung cancer patients treated with first-line therapies.
Subjects and Methods: All patients with advanced lung cancer diagnosed between 2011 and 2019 were identified from the Taiwan National Cancer Registry. First-line treatment was defined as a therapy that began within 30 days before and 90 days after the diagnosis. We defined a newly-developed AE as one established after first-line treatment had commenced, with the contingency that the patient had not been diagnosed with the AE within one year prior to the outset of therapy. One patient with a specific AE was matched on age, sex, and regimens with four patients without the AE. Payments incurred over the same period of time in the two groups were compared to estimate the AE-related costs.
Results: A total of 27,376 patients receiving first-line targeted therapy, immunotherapy, or chemotherapy were identified. Clinical characteristics of 15,454 treatment episodes with a specific AE and 61,816 treatment episodes without the AE were well balanced. The costliest AEs of any severity were sepsis/septicemia, neuropathy, and acute kidney injury, with the respective average incremental costs of 10101, 9982, and 7839 USD. The costliest severe AEs requiring hospitalization were sepsis/septicemia, interstitial lung disease/pneumonitis, and neuropathy, with mean incremental costs of 22483, 10645, and 10120 USD, respectively.
Conclusion: Costs associated with AEs in advanced lung cancer patients treated with first-line therapies were substantial. These estimates could be adopted for future cost-effectiveness analyses of new lung cancer treatments.
Keywords: adverse event, side effect, cost, lung cancer, utilization
Introduction
Lung cancer is the leading cause of cancer death in the world. More than half of all lung cancer patients are diagnosed in the advanced stage. For patients with advanced lung cancer who harbor actionable gene alterations, targeted therapies are the front-line treatment, whereas platinum-doublet chemotherapy has historically been the standard first-line treatment for patients whose tumors lack actionable gene alterations. Immunotherapy has changed the landscape of treatment for such patients. Given the increasing use and rising costs of lung cancer treatments, there is a growing demand for studies on cost-effectiveness which help thoracic oncologists move towards value-based practice when treating patients with advanced lung cancer.1–5
To study the cost-effectiveness of lung cancer treatments, costs associated with adverse events (AEs) need to be evaluated. Although several previous studies have used real-world data and expert appraisals to estimate AE-related costs,6–13 some of them have restricted the calculation of such costs to certain AEs or specific regimens.9,10,13 Additionally, the use of immune checkpoint inhibitors has not typically been taken into consideration. The majority of studies on the costs associated with AEs have come from North America or Europe. To date, no study has been conducted in East Asian countries. Values based on populations from Western nations might not be applicable to patients with advanced lung cancer in Taiwan.
We hypothesized that the costs associated with AEs were substantial for advanced lung cancer patients treated with first-line therapies. Based on an incremental approach to eliminating effects other than AEs, we attempted to estimate the AE-related costs of common first-line regimens and verify our hypothesis. These estimates could be adopted for future cost-effectiveness analyses of new lung cancer treatments in Taiwan.
Subjects and Methods
Data Source
We used the Taiwan National Cancer Registry database to identify all patients diagnosed with advanced lung cancer between 2011 and 2019. Lung cancer diagnosis was established according to the International Classification of Diseases for Oncology, third edition codes of C34.0-C34.3 and C34.8-C34.9, which included small cell lung cancer, squamous non-small cell lung cancer (NSCLC), and non-squamous NSCLC. Every patient was newly-diagnosed at stage IV according to the classification provided by the American Joint Committee on Cancer, seventh edition.14 Their baseline characteristics including age, sex, and Eastern Cooperative Oncology Group (ECOG) performance status were abstracted. Survival statuses of patients were verified by interlinking the data with the Taiwan National Mortality Registry database and following up until the end of 2020. We linked each patient’s identifying information to the Taiwan National Health Insurance (NHI) reimbursement database (2010–2020) for scoring prior 1-year comorbidities according to the Charlson Comorbidity Index15 and assessing first-line treatment regimens and associated AEs. Notably, Taiwan NHI reimbursed single-agent pembrolizumab as the first-line treatment for patients with NSCLC and programmed death-ligand 1 (PD-L1) expression levels ≥ 50% from April 1, 2019.
These databases capture the claims data of 99% of Taiwan’s inhabitants and are representative of the nationwide population. The Institutional Review Board of National Cheng Kung University Hospital approved the study before its commencement (A-EX-111-021). Informed consent was waived because of the use of de-identified information.
Defining First-Line Treatment
We used NHI codes to identify the first-line treatment regimens (Supplementary Table 1). Following the algorithm demonstrated by Davidoff et al,16 first-line treatment was defined as a therapy that began within 30 days before and 90 days after the diagnosis date of lung cancer. It included all regimens received from the first date of therapy to 30 days after the first date of therapy. We determined the final date of therapy as the point when a different drug began being administered after 30 days following the first date of therapy, when a 42-day period with no treatment was observed after the last administration of the regimens, the date when the patient died, or the date when data became unavailable (ie, December 31, 2020). Discontinuation of part of the first-line treatment did not constitute an end to the treatment. By using this algorithm, maintenance therapy could be captured as first-line treatment, whereas any switch therapy would be identified as second-line treatment.
We broadly categorized first-line treatments into targeted therapy, immunotherapy, and intravenous chemotherapy. Oral chemotherapy was excluded from the analysis. As anti-angiogenesis agents were not reimbursed by the NHI, we could not identify these drugs. Additionally, the NHI did not reimburse targeted therapy or immunotherapy in combination with chemotherapy doublet or single-agent chemotherapy. We were thus unable to capture these combination regimens.
Identifying Adverse Events
Adverse events selected for the analysis were those with an expected incidence rate of ≥ 10% after any first-line regimens according to UpToDate Clinical Decision Support.17 The NHI reimbursement data retain five main diagnoses for inpatient visits and three main diagnoses for outpatient or emergency visits. Using the codes of the International Classification of Disease, ninth and tenth editions (Supplementary Table 2), we identified AEs according to the presence of any diagnoses. We defined a newly-developed AE as a diagnosis which was established after first-line treatment had commenced and had experienced no previous AE within one year prior to the outset of therapy (Supplementary Figure 1). Severe AE denotes an AE identified from inpatient diagnoses.
Matching of Treatment Episodes for Incremental Costs
We estimated the costs associated with AEs by using an incremental approach which has been widely used in health services research18,19 and was adopted by a previous study in estimating AE-related costs.8 That is, one patient with a specific AE newly-developed during the first-line treatment period was completely matched on age and sex with four patients who underwent the same regimens but did not encounter the AE during the same length of observation period nor during the one-year period preceding the first date of therapy. All payments during the same length of observation periods in the two groups were totaled and converted to US dollars (USD) according to the exchange rate from the year 2020. After subtracting all costs incurred on the first-line treatment regimens, surgery, and radiation therapy, incremental costs associated with a specific AE was determined to be the remaining cost difference between the two groups.
It should be noted that the duration of first-line treatment in the matched treatment episode needed to be longer than that in treatment episode with a specific AE. Moreover, a patient could be counted multiple times because of their experience of having more than one AE. Although a treatment episode without the AE was matched once for a specific AE, it could be matched multiple times across different AEs.
Statistical Analysis
The balances of patient characteristics between a treatment episode with a specific AE and matched treatment episodes without the AE were measured using standardized differences and expressed as percentages. An absolute value of less than 10 suggested the two groups were well balanced. We evaluated the time spent on first-line treatment and overall survival of targeted therapy, immunotherapy, and chemotherapy using the Kaplan-Meier method and made comparisons using the Log rank test. The means and 95% confidence intervals of the cost differences were obtained. All the analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC) and P values were based on two-tail tests.
Results
Patient Characteristics
Among the 61,727 patients with advanced lung cancer diagnosed between 2011 and 2019, a total of 27,376 patients were identified as receiving targeted therapy, immunotherapy, or chemotherapy (Figure 1). Supplementary Figure 2 shows the time on first-line treatment and overall survival rate of patients who underwent targeted therapy, immunotherapy, and chemotherapy. Patients receiving targeted therapy experienced a longer time in first-line treatment and higher overall survival rates when compared with the others. After matching one patient having an AE on age, sex, and regimens with four patients without the AE, a total of 15,454 treatment episodes with a specific AE and 61,816 treatment episodes without the AE were compared (Table 1). The regimens of first-line treatment between the two groups were completely matched, leading to a balance of pathological subtypes. ECOG performance status and Charlson Comorbidity Index scores were also well balanced with absolute values of standardized differences (%) less than 10.
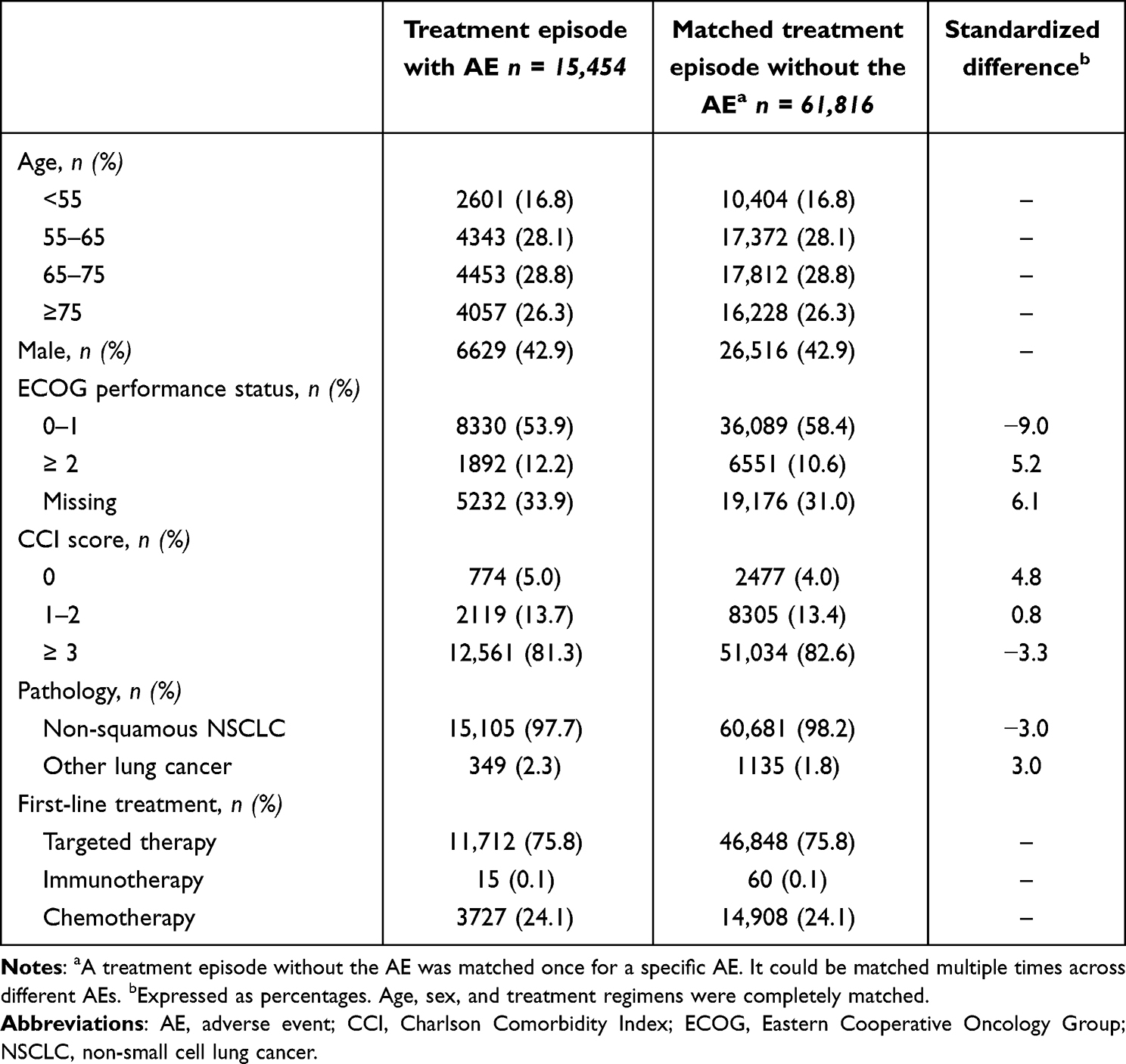 |
Table 1 Characteristics of Patients Across Treatment Episodes |
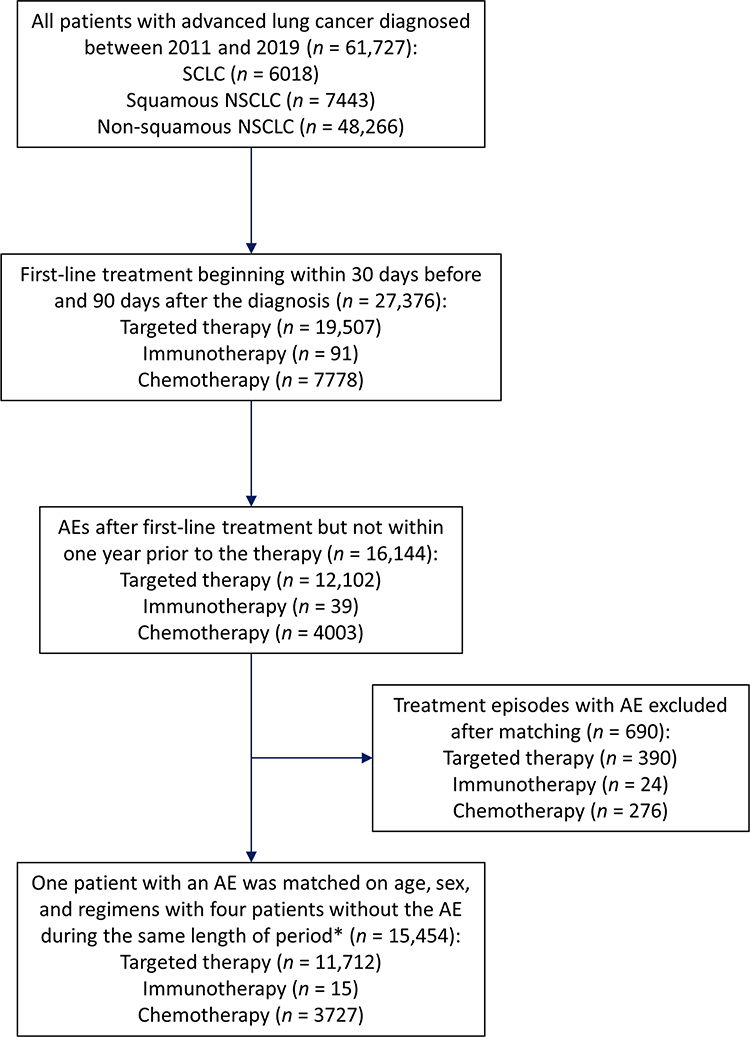 |
Figure 1 Flow diagram of identifying treatment episodes with adverse events (AEs). *A treatment episode without the AE was matched once for a specific AE. It could be matched multiple times across different AEs. NSCLC: non-small cell lung cancer. |
Prevalence and Duration of Treatment
The prevalence rates of patients with AE of any severity ranged from 0.1% for alopecia to 10.0% for constipation, with the median durations of treatment ranging from 8.5 months for neutropenia/febrile neutropenia to 33.9 months for neuropathy (Table 2). The other most common AEs of any severity included mucositis/stomatitis (8.7%) and musculoskeletal pain (7.0%). Conversely, the prevalence rates of patients with severe AE requiring hospitalization ranged from 0.0% for visual disturbance to 3.6% for sepsis/septicemia, with the median durations of treatment ranging from 7.0 months for interstitial lung disease/pneumonitis to 19.3 months for neuropathy. The other most common severe AEs included anemia (3.3%) and electrolyte imbalance (2.4%).
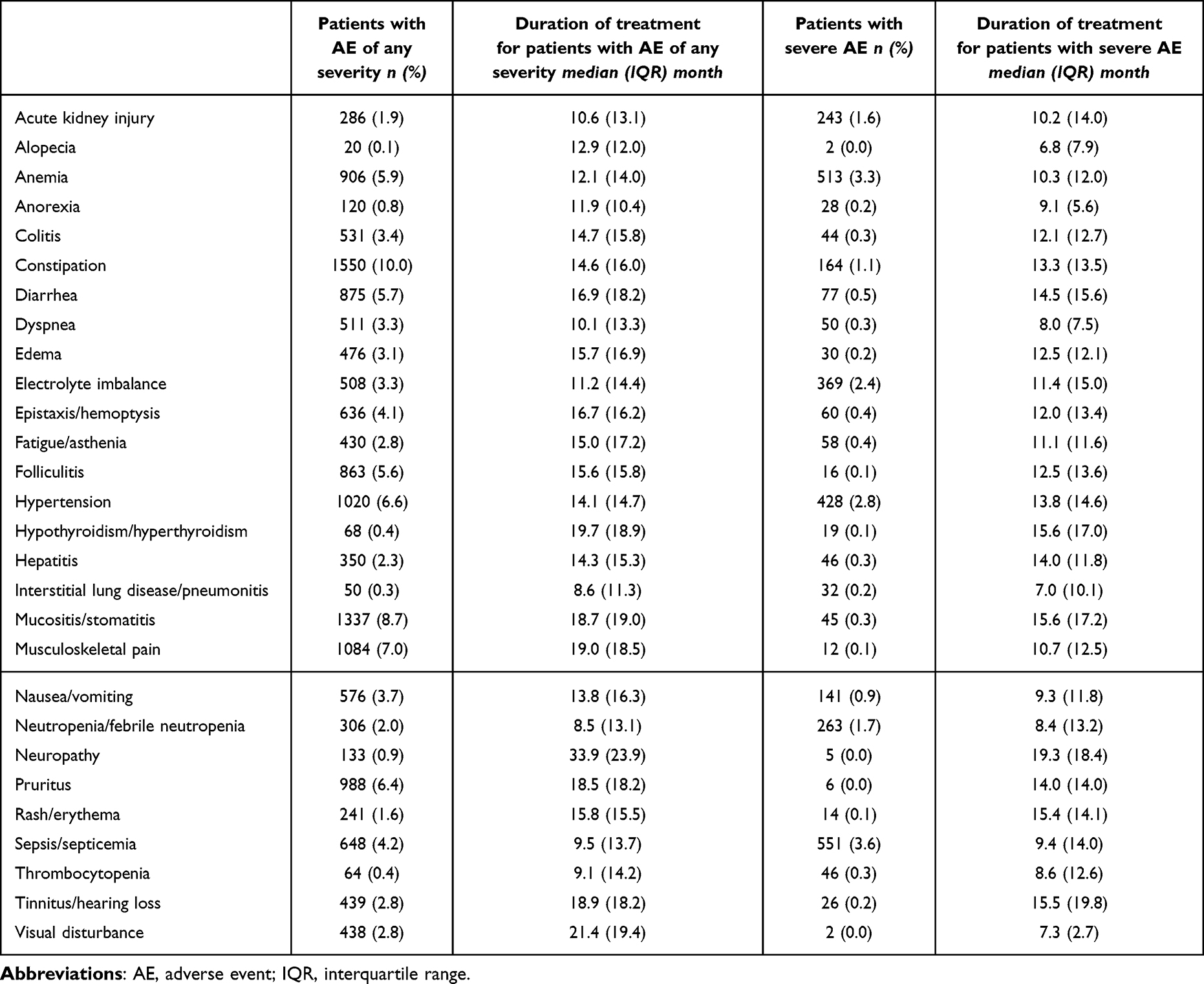 |
Table 2 Prevalence and Duration of Treatment for Patients with AE |
Costs Associated with Adverse Events
Incremental costs of AEs are shown in Table 3. Mean incremental costs associated with AE of any severity ranged from −3412 USD for folliculitis to 10,101 USD for sepsis/septicemia. Other costliest AEs of any severity included neuropathy (9982 USD) and acute kidney injury (7839 USD). Moreover, mean incremental costs associated with severe AE requiring hospitalization ranged from 2919 USD for visual disturbance to 22,483 USD for sepsis/septicemia. The other costliest severe AEs included interstitial lung disease/pneumonitis (10,645 USD) and neuropathy (10,120 USD).
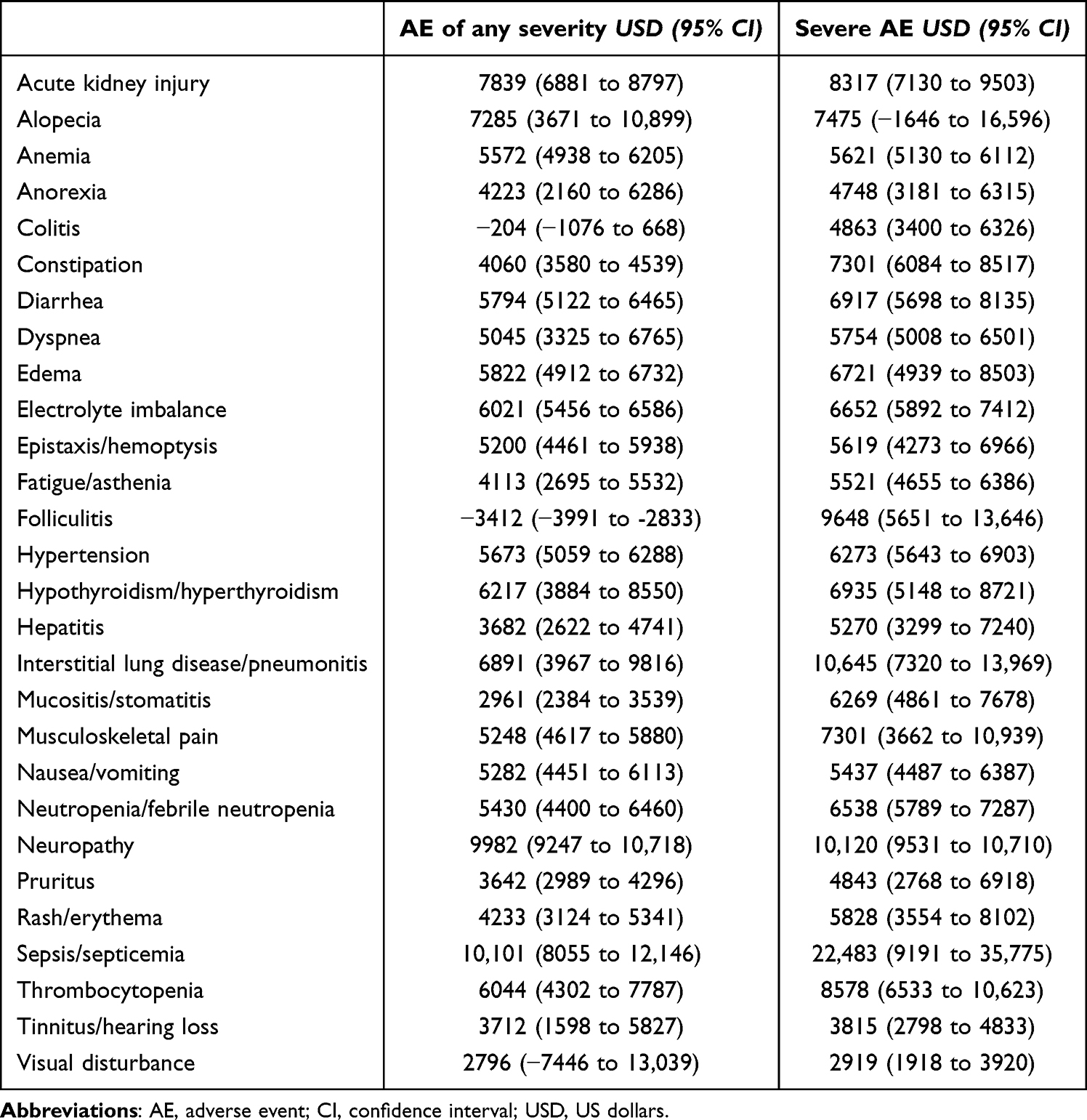 |
Table 3 Incremental Cost of AE |
Discussion
Several previous studies have estimated the costs associated with AEs for lung cancer patients.6–13 Some of them focused on AEs of specific regimens such as erlotinib, afatinib, and pemetrexed; others simply looked at the costs associated with certain AEs.9,10,13 Furthermore, no study has of yet been conducted in Asian countries.20 Our study used Taiwan NHI reimbursement data and followed up on lung cancer patients until the end of 2020, by which time pembrolizumab had already been reimbursed. We were thus able to capture the costs associated with AEs of this new therapy. Unlike previous research which did not consider differences in tumor stage across treatment episodes with and without an AE,8 this study limited its qualified patients to those newly diagnosed with advanced lung cancer and comprehensively matched the regimens of first-line treatment (Table 1). The costliest AEs of any severity in Taiwan were sepsis/septicemia (10,101 USD), neuropathy (9982 USD), and acute kidney injury (7839 USD), whereas the costliest severe AEs were sepsis/septicemia (22,483 USD), interstitial lung disease/pneumonitis (10,645 USD), and neuropathy (10,120 USD) (Table 3). These findings may help thoracic oncologists move towards value-based practice and evaluate the cost-effectiveness of new lung cancer treatments.
Prior research disclosed that anemia and dyspnea were the most commonly encountered AEs in patients with advanced lung cancer who underwent first-line treatments.6 In contrast, we found that mucositis/stomatitis, pruritus, diarrhea, and folliculitis were more commonly encountered than the aforementioned symptoms (Table 2). Such a phenomenon could be explained by the following reason: prior research was restricted to those patients who received platinum-based chemotherapy, yet did not include subjects undergoing targeted therapies. In Taiwan, more than half of patients with non-squamous NSCLC harbor EGFR mutations and receive targeted therapies in their front-line treatment. The AEs resulting from targeted therapies are quite different from those of platinum-based chemotherapy. Nevertheless, our study corroborated the results of prior research,6 where interstitial lung disease/pneumonitis was one of the AEs associated with the highest costs (Table 3). We further found that neutropenia/febrile neutropenia and sepsis/septicemia requiring hospitalization also resulted in high AE-associated costs. These findings are supported by the clinical experience in administering cytotoxic agents for patients with small cell lung cancer, a cohort not included in prior research.6
Although previous studies have estimated the costs of immunotherapy-related AEs, the estimates were simply based on experts’ opinions12 or calculated as the sum of costs on claims associated with the AE.11 Our study used an incremental approach to subtract the effects other than AEs, the costs would less likely to be overestimated compared with the aforementioned studies. However, the NHI only reimbursed pembrolizumab as monotherapy for patients with PD-L1 expression levels ≥ 50%. Patients whose PD-L1 expression levels < 50%, or those who were administered other immune checkpoint inhibitors, could not be identified in our study.
We strictly defined our usage of first-line treatment and the duration of treatment. To be specific, patients’ adherences to therapy were taken into consideration and all AEs must have been newly developed during the period when the patient was still undergoing the therapy. Nevertheless, the reduction of drug dosage and prolongation of drug interval could not be addressed in this study. As the costs of first-line treatment regimens were not counted while calculating the incremental costs, the reduction of drug dosage and prolongation of drug interval would not confound the results too much. Notably, patients with severe AEs had shorter durations of treatment when compared to those with AEs of any severity (Table 2). This emphasizes that greater effort should be made to prevent severe AEs requiring hospitalization, as it not only necessitates substantial costs but may also lead to poor prognosis.
Several limitations must be acknowledged in our study. First, caution is necessary when using claims data to draw any causal inference of a downstream AE from the preceding first-line treatment. However, we restricted the AEs in this study to those occurring after first-line treatment, but not within the preceding one year. Further, a patient with a specific AE was completely matched on age and sex with four referents who underwent the same regimens but did not experience the AE. Other clinical characteristics were also well balanced between the two groups. The incremental cost estimates could be attributed to the AE. Prospective collections of the cost data of predefined AEs merit future research. Second, some cost estimates were negative when using the incremental approach. Nevertheless, the costs of severe AE requiring hospitalization were all positive. Applying the results of severe AEs to cost-effectiveness analysis is still feasible. Third, we aimed to estimate the costs associated with different AEs and did not categorize the occurrences and costs of AEs by different first-line treatments. If we categorized them by different first-line therapies, the number of episodes in each category would become too small, preventing us from obtaining a conceivable estimate. Finally, to reduce the complexity of regimens, use of oral vinorelbine was not considered in the analysis, leading to a reduced number of patients in the chemotherapy groups. Carboplatin was not reimbursed by the NHI in patients with normal serum creatinine levels; therefore, it might not be captured in the analysis. Likewise, other out-of-pocket drugs such as anti-angiogenesis agents, targeted therapies, or immunotherapies in combination with chemotherapy could not be identified.
Conclusion
Costs associated with AEs were substantial for patients with advanced lung cancer who were treated with first-line therapy in Taiwan. These estimates could be used for evaluating the cost-effectiveness of new lung cancer treatments.
Data Sharing Statement
The datasets generated and/or analyzed during this study are not publicly available due to confidentiality reasons, but the sufficiently aggregated data used for analyses are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The Institutional Review Board of National Cheng Kung University Hospital approved the study before its commencement (A-EX-111-021). Informed consent was waived because of the use of de-identified information. Study methods were performed in accordance with the STROBE guidelines.
Acknowledgments
We thank both the Health and Welfare Data Science Center and the Health Data Science Center of National Cheng Kung University Hospital for providing administrative and technical support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Science and Technology Council (112-2314-B-006-013-MY2) and National Cheng Kung University Hospital (NCKUH-11303046). The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Yang SC, Lai WW, Hsu JC, Su WC, Wang JD. Comparative effectiveness and cost-effectiveness of three first-line EGFR-tyrosine kinase inhibitors: analysis of real-world data in a tertiary hospital in Taiwan. PLoS One. 2020;15(4):e0231413. doi:10.1371/journal.pone.0231413
2. Yang SC, Kunst N, Gross CP, Wang JD, Su WC, Wang SY. Cost-effectiveness of nivolumab plus ipilimumab with and without chemotherapy for advanced non-small cell lung cancer. Front Oncol. 2021;11:760686. doi:10.3389/fonc.2021.760686
3. Yang SC, Yeh YC, Chen YL, Chiu CH. Economic analysis of exclusionary EGFR test versus up-front NGS for lung adenocarcinoma in high EGFR mutation prevalence areas. J Natl Compr Canc Netw. 2022;20(7):774–782. doi:10.6004/jnccn.2021.7120
4. Yang SC, Lin CC, Chen YL, Su WC. Economic analysis of tissue-first, plasma-first, and complementary NGS approaches for treatment-naïve metastatic lung adenocarcinoma. Front Oncol. 2022;12:873111. doi:10.3389/fonc.2022.873111
5. Yang SC, Ou HT, Su WC, Wang SY. Cost-effectiveness of first-line immunotherapies for advanced non-small cell lung cancer. Cancer Med. 2023;12(7):8838–8850. doi:10.1002/cam4.5632
6. Bittoni MA, Arunachalam A, Li H, et al. Real-world treatment patterns, overall survival, and occurrence and costs of adverse events associated with first-line therapies for medicare patients 65 years and older with advanced non-small-cell lung cancer: a retrospective study. Clin Lung Cancer. 2018;19(5):e629–e645. doi:10.1016/j.cllc.2018.04.017
7. Arunachalam A, Li H, Bittoni MA, et al. Real-world treatment patterns, overall survival, and occurrence and costs of adverse events associated with second-line therapies for Medicare patients with advanced non-small-cell lung cancer. Clin Lung Cancer. 2018;19(5):e783–e799. doi:10.1016/j.cllc.2018.05.016
8. Wong W, Yim YM, Kim A, et al. Assessment of costs associated with adverse events in patients with cancer. PLoS One. 2018;13(4):e0196007. doi:10.1371/journal.pone.0196007
9. Subramanian J, Fernandes AW, Laliberte F, Pavilack M, DerSarkissian M, Duh MS. The rate of occurrence, healthcare resource use and costs of adverse events among metastatic non-small cell lung cancer patients treated with first- and second-generation epidermal growth factor receptor tyrosine kinase inhibitors. Lung Cancer. 2019;138:131–138. doi:10.1016/j.lungcan.2019.07.021
10. Isla D, De Castro J, Juan O, et al. Costs of adverse events associated with erlotinib or Afatinib in first-line treatment of advanced EGFR-positive non-small cell lung cancer. Clinicoecon Outcomes Res. 2017;9:31–38. doi:10.2147/CEOR.S121093
11. Engel-Nitz NM, Johnson MP, Bunner SH, Ryan KJ. Real-world costs of adverse events in first-line treatment of metastatic non-small cell lung cancer. J Manag Care Spec Pharm. 2020;26(6):729–740. doi:10.18553/jmcp.2020.26.6.729
12. Chouaid C, Loirat D, Clay E, et al. Cost analysis of adverse events associated with non-small cell lung cancer management in France. Clinicoecon Outcomes Res. 2017;9:443–449. doi:10.2147/CEOR.S138963
13. Banz K, Bischoff H, Brunner M, et al. Comparison of treatment costs of grade 3/4 adverse events associated with erlotinib or pemetrexed maintenance therapy for patients with advanced non-small-cell lung cancer (NSCLC) in Germany, France, Italy, and Spain. Lung Cancer. 2011;74(3):529–534. doi:10.1016/j.lungcan.2011.04.010
14. Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–1474. doi:10.1245/s10434-010-0985-4
15. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
16. Davidoff AJ, Tang M, Seal B, Edelman MJ. Chemotherapy and survival benefit in elderly patients with advanced non-small-cell lung cancer. J Clin Oncol. 2010;28(13):2191–2197. doi:10.1200/JCO.2009.25.4052
17. UpToDate. Available from: https://www.wolterskluwer.com/en/solutions/uptodate/clinical-decision-support.
18. Yabroff KR, Lamont EB, Mariotto A, et al. Cost of care for elderly cancer patients in the United States. J Natl Cancer Inst. 2008;100(9):630–641. doi:10.1093/jnci/djn103
19. Yang SC, Lai CH, Kuo CW, Lin CC, Lai WW, Wang JD. Downstream complications and healthcare expenditure after invasive procedures for lung lesions in Taiwan. Int J Environ Res Public Health. 2021;18(8):4040. doi:10.3390/ijerph18084040
20. Pearce A, Haas M, Viney R. Are the true impacts of adverse events considered in economic models of antineoplastic drugs? A systematic review. Appl Health Econ Health Policy. 2013;11(6):619–637. doi:10.1007/s40258-013-0058-5
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.