Back to Journals » International Journal of General Medicine » Volume 18
Establishment and Evaluation of a Risk Prediction Model for Abnormal Circadian Rhythm of Blood Pressure in Young Hypertensive Patients
Authors Chen Q ![]() , Shi L, Li X, Wen J, Geng G, Jiang J, Yu H, Quan M
, Shi L, Li X, Wen J, Geng G, Jiang J, Yu H, Quan M
Received 6 July 2025
Accepted for publication 2 October 2025
Published 17 October 2025 Volume 2025:18 Pages 6301—6313
DOI https://doi.org/10.2147/IJGM.S551845
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Qinhao Chen,1 Lei Shi,2 Xiang Li,1 Jing Wen,1 Guangan Geng,1 Jinliang Jiang,1 Haiyang Yu,3 Mingzhu Quan1
1Department of Electrocardiogram, 901st Hospital of the Chinese People’s Liberation Army Joint Logistics Support Force, Hefei, Anhui Province, People’s Republic of China; 2The First Affiliated Clinical Medical College of Anhui University of Chinese Medicine, Hefei, Anhui Province, People’s Republic of China; 3Department of Clinical Oncology, The First Affiliated Hospital of USTC, Hefei, Anhui Province, People’s Republic of China
Correspondence: Mingzhu Quan, Department of Electrocardiogram, 901st Hospital of the Chinese People’s Liberation Army Joint Logistics Support Force, Hefei, Anhui Province, People’s Republic of China, Tel +8613349198759, Email [email protected]
Objective: This study aimed to develop and validate a simple and clinically applicable nomogram to predict abnormal circadian blood pressure rhythm in young hypertensive patients, enabling early detection and intervention.
Methods: A total of 211 young hypertensive patients were enrolled between January 2023 and June 2024, with an additional 203 patients from other hospitals included for external validation. Patients were categorized into dipper and non-dipper groups based on 24-hour ambulatory blood pressure monitoring. Independent risk factors for abnormal circadian blood pressure rhythms were identified using multivariate logistic regression analysis, which was subsequently used to construct and externally validate a nomogram model.
Results: Univariate analysis revealed significant differences (P< 0.05) in the lymphocyte-to-monocyte ratio (LMR), systemic inflammatory response index (SIRI), systemic immune-inflammatory index (SII), triglycerides (TG), high-density lipoprotein (HDL), low-density lipoprotein (LDL), and uric acid (UA) between the dipper and non-dipper groups. Multivariate analysis identified decreased LMR, increased SIRI, elevated TG, and elevated UA as independent risk factors for abnormal circadian blood pressure rhythms in young hypertensive patients. The risk nomogram model was established based on the variables filtered by the multi-factor Logistic regression model. The evaluation results showed that the area under the curve (AUC) was 0.883. External validation showed an AUC of 0.844, with calibration confirming excellent predictive performance.
Conclusion: LMR, SIRI, TG, and UA are independent predictors of abnormal circadian blood pressure rhythms in young hypertensive patients. The developed nomogram model is straightforward, rapid, and exhibits clinically relevant accuracy, providing valuable insights for clinical application.
Keywords: hypertension, systemic immune response index, lymphocyte-to-monocyte ratio, circadian rhythm of blood pressure, nomogram
Introduction
Hypertension is a significant independent risk factor for cardiovascular diseases (CVD), including cardiac death, coronary heart disease, heart failure, and stroke.1 Blood pressure in the human body follows a circadian rhythm regulated by the nervous and endocrine systems. Typically, blood pressure exhibits two peaks, occurring between 6:00 to 10:00 a.m. and 4:00 to 6:00 p.m., with the lowest levels observed between 2:00 and 3:00 a.m., often decreasing by 10–20%.2 These circadian variations can be monitored using 24-hour ambulatory blood pressure monitoring (ABPM). Based on nocturnal blood pressure decline, blood pressure rhythms are classified into dipper, non-dipper, anti-dipper, and super-dipper patterns. Dipper blood pressure represents the normal physiological pattern, whereas non-dipper, super-dipper, and anti-dipper patterns are associated with target organ damage and an increased risk of cardiovascular and cerebrovascular mortality.3
Previous studies have highlighted the critical role of inflammatory factors in the development of hypertension. Peripheral blood cell counts and derived indicators that assess inflammatory status have been widely employed in clinical research on chronic inflammation. Examples include the systemic immune-inflammatory index (SII), systemic inflammatory response index (SIRI), and lymphocyte-monocyte ratio (LMR). These indicators encompass different components of blood cells, reflecting various inflammatory pathways and mechanisms of immune regulation. As reliable, cost-effective, and easily obtainable markers of inflammation, their levels are closely linked to a range of cardiovascular and cerebrovascular diseases.4 Inflammatory state plays a key role in the pathogenesis of non-dipper blood pressure, and higher levels of inflammation may lead to impaired nighttime blood pressure drop by promoting endothelial dysfunction and sympathetic nervous system overactivity.5 Akyüz et al’s study showed that white blood cell counts and neutrophil levels were significantly higher in patients with non-dipper hypertension, highlighting the critical role of inflammation in mediating adverse outcomes associated with non-dipper hypertension.6
In recent years, there has been a concerning trend of hypertension manifesting at a younger age. A national survey conducted between 2012 and 2015 revealed a prevalence of 10.1% among individuals aged 18–35, a figure that continues to rise.7 Young hypertensive patients have a significantly increased lifetime cardiovascular risk due to prolonged exposure to hypertension.8 Early identification and treatment are key to reducing future cardiovascular risk, and strengthening blood pressure reduction early can reduce lifelong cardiovascular mortality.9
Consequently, early detection, prevention, and effective management of hypertension are crucial for safeguarding cardiovascular health. Predictive models are becoming increasingly pivotal in clinical decision-making, particularly for assessing early disease risks. Unfortunately, there are currently limited predictive tools available in clinical practice for assessing the risk of young hypertensive patients, especially for nomogram that have not been validated specifically for young hypertensive patients. Therefore, this study aimed to identify independent risk factors for abnormal circadian blood pressure rhythms in young patients with hypertension and to develop a predictive model. Such a model could facilitate the early identification of high-risk individuals and provide essential clinical guidance for the intervention and treatment of young hypertensive patients.10
Materials and Methods
Study Participants
This study included 327 young hypertensive patients who received treatment and evaluation at the 901st Hospital of the Chinese People’s Liberation Army Joint Logistics Support Force from January 2023 to June 2024 through consecutive sampling. After excluding patients with incomplete personal information, a total of 211 study subjects were ultimately included. Additionally, 203 hypertensive patients admitted to the First Affiliated Hospital of the University of Science and Technology of China during the same period were recruited for external validation. Based on the model area under the curve (AUC) value and predictor variables, and following the improved Events Per (EPV) criterion (EPV ≥ 7). To accurately estimate the confidence interval of AUC (target with ≤ 0.10) and ensure statistical performance (detecting AUC decrease ≥ 0.05, α=0.05, β=0.2). Hypertension in this study was defined according to the Guidelines for the Prevention and Treatment of Hypertension in China (Revised Edition 2018). Inclusion criteria were as follows: (1) Patients with a history of hypertension or currently using antihypertensive medications, with blood pressure consistently below 140/90 mmHg; (2) Diagnosis of hypertension based on ambulatory blood pressure monitoring (ABPM): average systolic/diastolic blood pressure ≥ 130/80 mmHg; daytime ≥ 135/85 mmHg; nighttime ≥ 120/70 mmHg; (3) Young hypertensive patients, Age range 15–35 years. Exclusion criteria were: (1) Secondary hypertension; (2) Systemic inflammatory diseases; (3) Malignant tumors; (4) Obstructive sleep apnea syndrome; (5) Severe impaired consciousness and/or mental symptoms precluding cooperation; (6) Recent use of glucocorticoids or immunosuppressants; (7) Active tumors, acute and chronic inflammation, blood system, and immune system diseases; (8) Severe liver and kidney failure.
All participants underwent 24-hour ABPM. Individuals showing a nighttime blood pressure decrease of 10%–20% compared to daytime levels were classified into the dipper group, while those without such a decrease were classified into the non-dipper group.
Research Methods and Grouping
General Information
Clinical demographic information was collected via a survey questionnaire, which included data on gender, age, height, weight, nocturnal sleep duration, and history of smoking and drinking.
Blood Pressure Measurement
Blood pressure was assessed according to WHO standards. Patients rested in a seated position for 30 minutes, avoiding any disruption to the measurement site and refraining from alcohol or stimulating beverages. Blood pressure was measured using the Korotkoff auscultatory method, with three measurements taken at 2-minute intervals. The average of the three readings was recorded as the final result. For the detection of dynamic blood pressure, the same brand and model of equipment are used.
24-Hour Ambulatory Blood Pressure Monitoring
ABPM was programmed to automatically measure blood pressure every 30 minutes during the day (8:00–22:00) and every hour at night (22:00–8:00). Patients were instructed to remain in a quiet state during measurements. Data not meeting predefined criteria—such as systolic blood pressure > 260 mmHg or < 60 mmHg, and diastolic blood pressure > 160 mmHg or < 40 mmHg—were excluded from the analysis. Participants wore the device for 24 hours, with data retention required to exceed 90% for inclusion; otherwise, measurements were repeated. The following blood pressure parameters were collected: 24-hour average systolic blood pressure (24h SBP), 24-hour average diastolic blood pressure (24h DBP), daytime average systolic blood pressure (DSBP), daytime average diastolic blood pressure (DDBP), nighttime average systolic blood pressure (NSBP), nighttime average diastolic blood pressure (NDBP), 24-hour systolic blood pressure load, 24-hour diastolic blood pressure load, 24-hour systolic blood pressure variability, 24-hour diastolic blood pressure variability, daytime systolic blood pressure load, daytime diastolic blood pressure load, daytime systolic blood pressure variability, daytime diastolic blood pressure variability, nighttime systolic blood pressure load, nighttime diastolic blood pressure load, nighttime systolic blood pressure variability, nighttime diastolic blood pressure variability, morning peak systolic blood pressure, and morning peak diastolic blood pressure. The nighttime blood pressure dip rate was calculated as follows: Nighttime blood pressure dip rate % = (average daytime blood pressure - average nighttime blood pressure) / average daytime blood pressure × 100%. This calculation typically refers to systolic blood pressure.
Laboratory Testing
For the detection of peripheral blood indicators, we used Ethylene Diamine Tetraacetic Acid (EDTA) anticoagulant tubes of the same specifications from the same manufacturer, using the same testing reagents and standard range. Fasting overnight for 6–8 hours, peripheral venous blood was collected in the morning. A fully automated biochemical analyzer was used to measure blood routine parameters, including fasting blood glucose (FBG), total cholesterol (TC), triglycerides (TG), high-density lipoprotein (HDL), low-density lipoprotein (LDL), creatinine (Cr), glomerular filtration rate (GFR), urea (UREA), uric acid (UA), aspartate aminotransferase (AST), and alanine aminotransferase (ALT).
Inflammatory indices were calculated as follows: Systemic Inflammatory Response Index (SIRI) = absolute neutrophil count (N) × absolute monocyte count (M) / absolute lymphocyte count (L); Systemic Immune-Inflammatory Index (SII) = peripheral platelet count (PLT) × absolute neutrophil count (N) / absolute lymphocyte count (L); Lymphocyte-to-Monocyte Ratio (LMR) = L / M; Neutrophil-to-Lymphocyte Ratio (NLR) = N / L; Platelet-to-Lymphocyte Ratio (PLR) = P / L; Neutrophil-to-Monocyte Ratio (NMR) = N / M.
Statistical Analyses
Statistical analyses were conducted using SPSS 25.0 and R software (version 4.2.1), incorporating the rms, Hmisc, pROC, and ggplot2 packages. Data conforming to normal distribution were presented as mean ± standard deviation (SD), and comparisons between groups were assessed using independent sample t-tests. Non-normally distributed data were expressed as median (interquartile range, IQR), and non-parametric tests were applied. Categorical data were presented as frequencies and analyzed using the Chi-square test. The binary logistic model was constructed using the glm function using R software, and the Nomogram correlation model was constructed and visualized using the rms package. For the inclusion criteria of variables in multivariate regression analysis, we included factors that were meaningful in univariate regression analysis, and combined with previous studies, included variables with strong clinical significance. Statistical significance was set at P < 0.05.
Results
Comparison of General Data Between the Two Groups of Hypertensive Patients
The study included a total of 211 patients, with 93 in the dipper group and 118 in the non-dipper group. A comparison between the groups revealed significant differences in TG, HDL, LDL, Cr, UA, AST, and ALT levels (P < 0.05). Specifically, the non-dipper group showed higher levels of TG, LDL, Cr, and UA, and lower levels of HDL, AST, and ALT compared to the dipper group. No significant differences were observed in gender, age, smoking history, drinking history, nighttime sleep duration, BMI, FBG, TC, GFR, or UREA between the groups (Table 1).
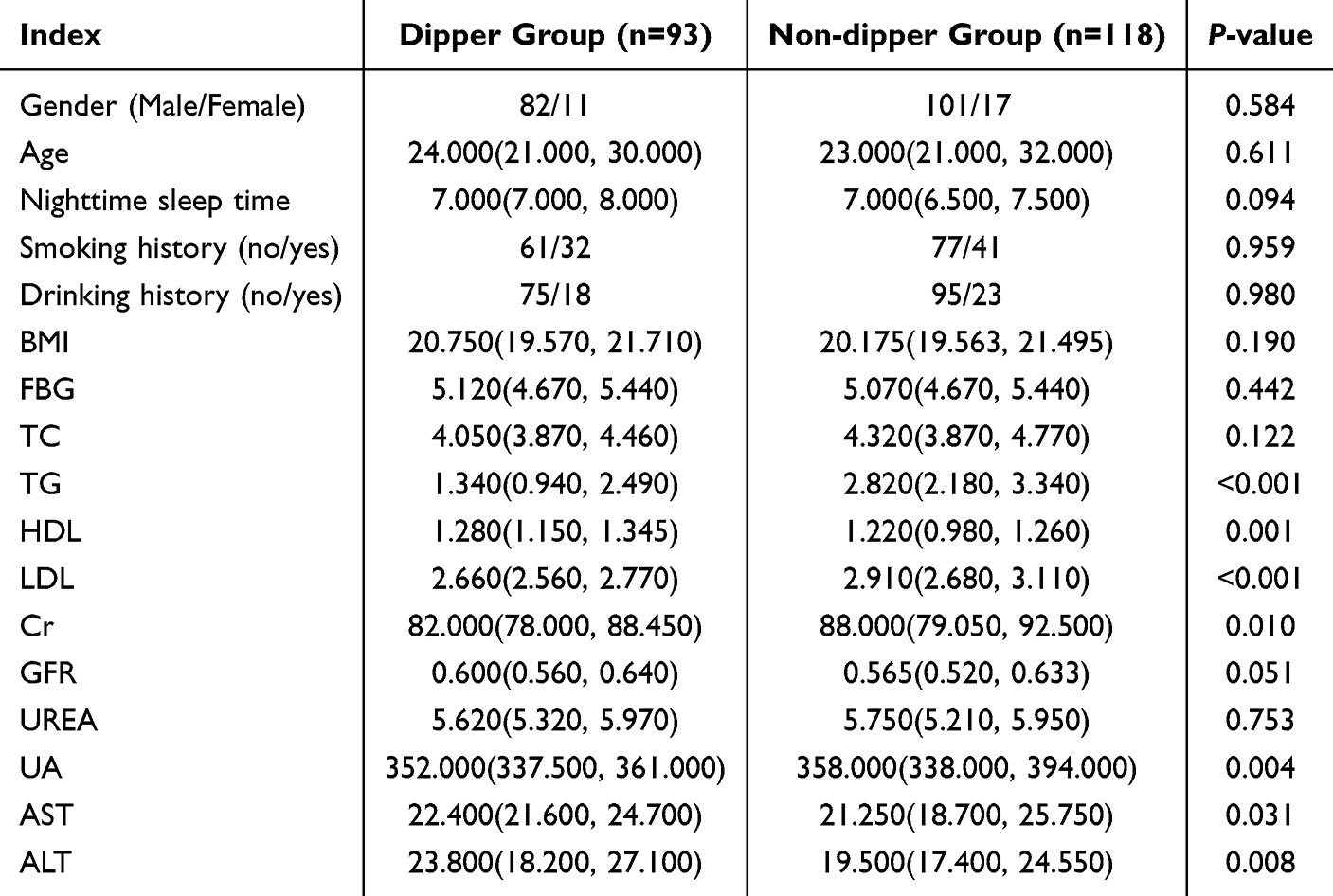 |
Table 1 Comparison of General Data Between the Two Groups |
Comparison of Inflammatory Indicators Between the Two Groups of Hypertensive Patients
A comparison between the two groups revealed significant differences in LMR, SIRI, and SII (P < 0.05). The non-dipper group exhibited higher SIRI and SII levels and lower LMR levels compared to the dipper group. However, no significant differences were found in WBC, N, NLR, PLR, or NMR between the groups (Table 2).
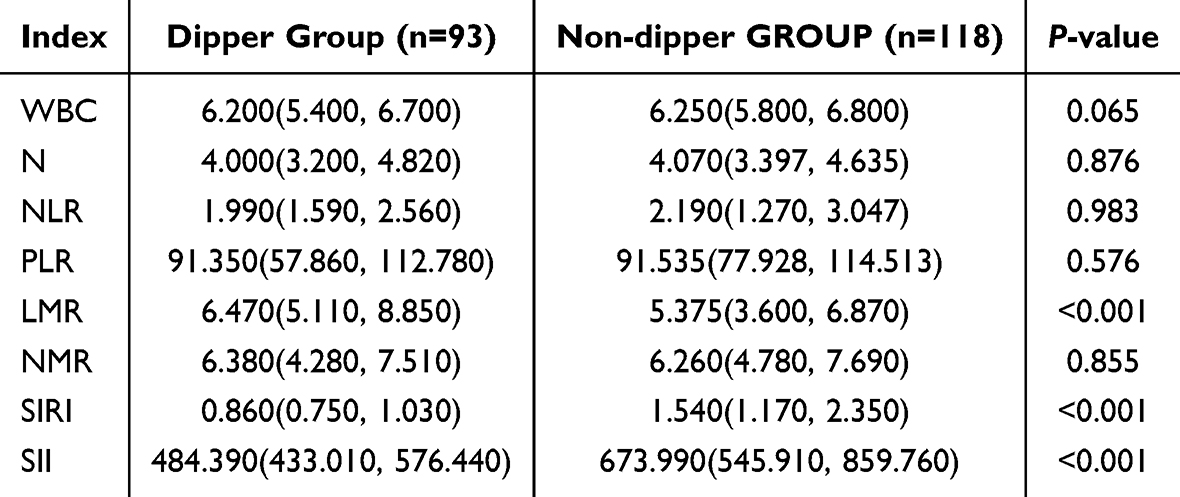 |
Table 2 Comparison of Inflammatory Indicators Between the Two Groups |
Comparison of Blood Pressure Levels and Rhythms Between the Two Groups of Hypertensive Patients
The nocturnal drop rate of blood pressure differed significantly between the dipper and non-dipper groups (P < 0.05). The non-dipper group exhibited a significantly lower nocturnal drop rate compared to the dipper group. No significant differences were observed in other blood pressure indicators (Table 3).
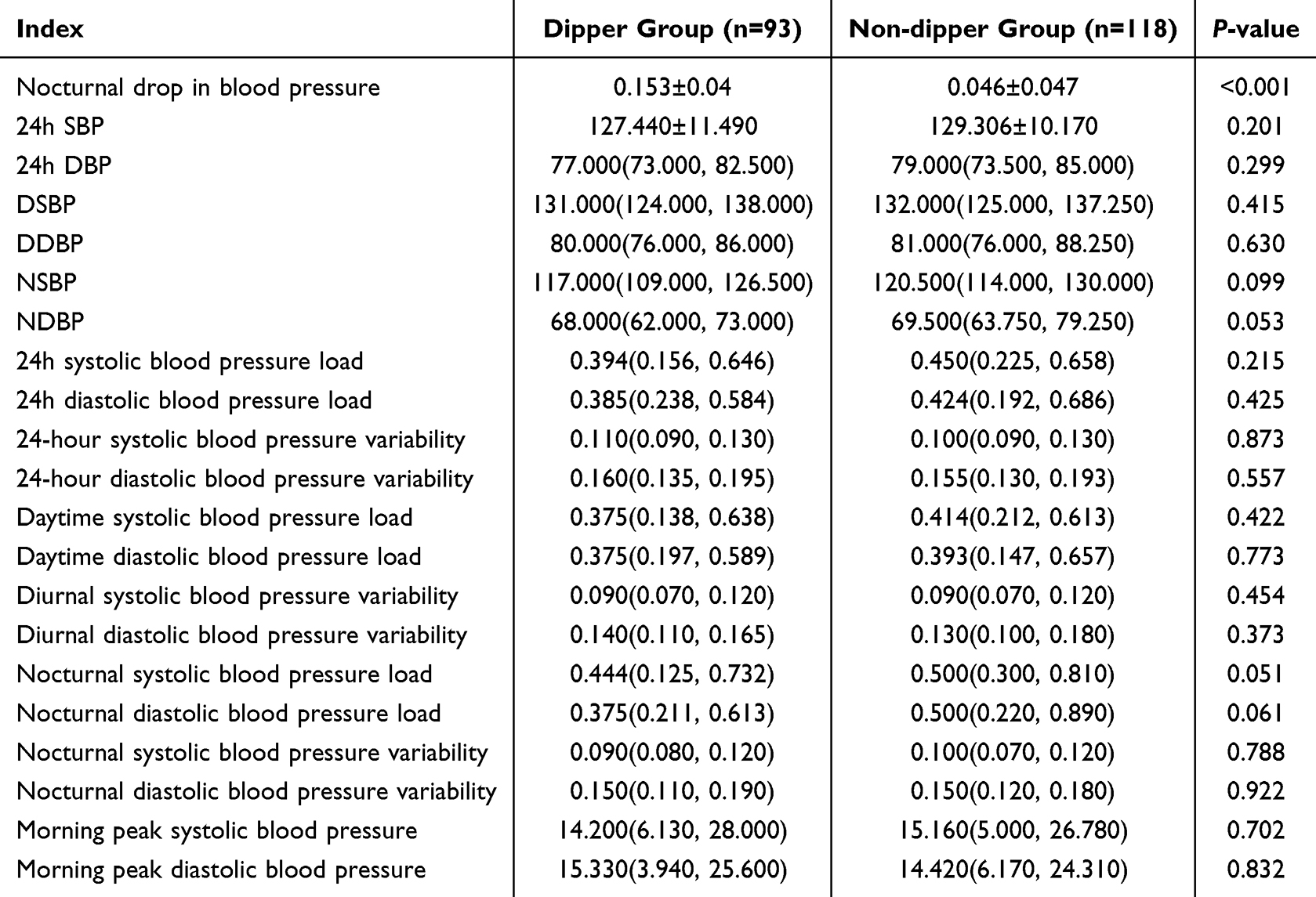 |
Table 3 Comparison of Blood Pressure Levels and Rhythms Between the Two Groups |
Univariate and Multivariate Logistic Regression Analysis of Abnormal Circadian Rhythm of Blood Pressure in Young Hypertensive Patients
Univariate Logistic regression analysis revealed significant differences in LMR, SIRI, SII, TG, HDL, LDL, and UA between the dipper and non-dipper groups (P < 0.05). Abnormal circadian rhythm of blood pressure in young hypertensive patients was set as the dependent variable (non-dipper group = 1, dipper group = 0), while significant variables from the univariate analysis were included as independent variables in the multivariate logistic regression model (Table 4). The results identified decreased LMR, increased SIRI, elevated TG, and elevated UA as independent risk factors for abnormal circadian rhythm of blood pressure in hypertensive patients.
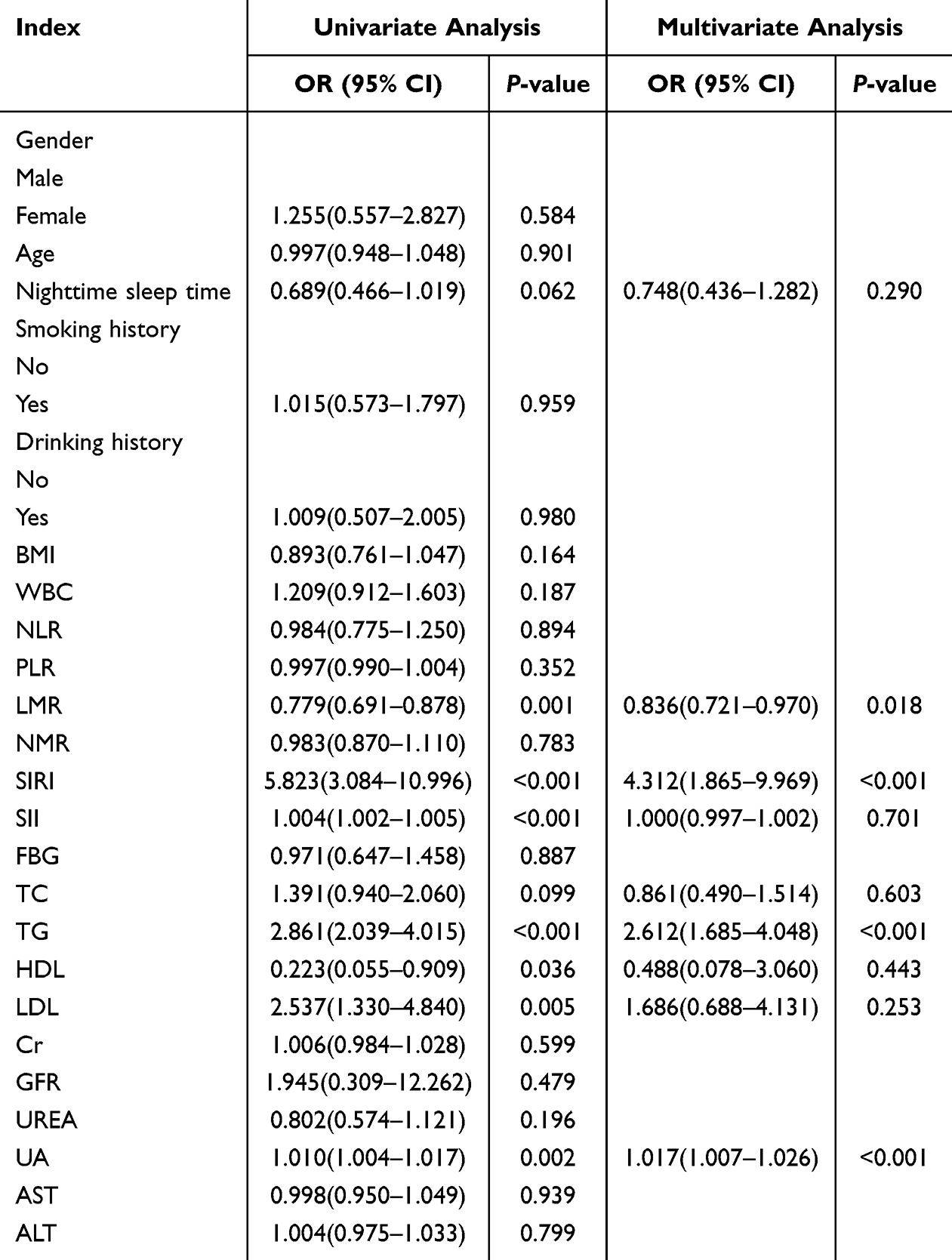 |
Table 4 Logistic Regression Analysis of Influencing Factors of Abnormal Circadian Rhythm of Blood Pressure |
Nomogram Prediction Model for the Risk of Abnormal Circadian Rhythm of Blood Pressure in Hypertensive Patients
A nomogram was developed based on the four independent risk factors identified through multivariate logistic regression analysis, as shown in Figure 1. Each factor corresponds to a score (Points) on the scale. The total score (Total Points) is calculated by summing these individual scores, corresponding to a specific value on the risk axis. This value represents the risk of abnormal circadian rhythm of blood pressure in hypertensive patients.
 |
Figure 1 Risk nomogram for abnormal circadian rhythm of blood pressure. |
Evaluation of Risk Nomogram
The discrimination ability of the model using Harrell concordance index analysis method. Similarly, the ROC curve analysis showed an AUC of 0.883, indicating high discrimination ability and accuracy. Calibration of the nomogram was evaluated using calibration curves, where the X-axis represents the predicted risk of abnormal circadian rhythm, and the Y-axis represents the actual occurrence. The Apparent curve reflects prediction performance, the Bias-corrected curve shows calibration accuracy, and the Ideal curve represents a perfect prediction. The model closely approximated the ideal prediction, demonstrating strong consistency with theoretical expectations (Figures 2 and 3).
 |
Figure 2 Area under the ROC curve of the risk nomogram. |
 |
Figure 3 Calibration curve of risk nomogram. |
External Validation of the Risk Prediction Model for Abnormal Circadian Rhythm of Blood Pressure in Hypertensive Patients
For external validation, 203 patients were included, with 99 in the dipper group and 104 in the non-dipper group. The ROC curve analysis yielded an AUC of 0.844, indicating strong discriminatory ability. Additionally, the calibration curve showed close alignment between predicted and actual values, highlighting the model’s high accuracy in predicting abnormal circadian rhythms of blood pressure in hypertensive patients (Figures 4 and 5).
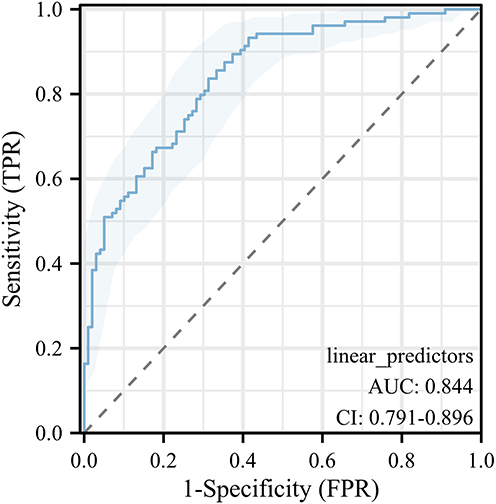 |
Figure 4 Area under the ROC curve of the external validation risk nomogram. |
 |
Figure 5 Calibration curve of the external validation risk nomogram. |
Discussion
Hypertension, a prevalent chronic condition, is strongly associated with an increased risks of heart attack, stroke, and damage to vital organs. Its incidence has been steadily rising, particularly among younger individuals. Effective management of hypertension is essential to prevent target organ damage and reduce the likelihood of adverse cardiovascular events. The circadian rhythm of blood pressure is recognized as an independent risk factor in the progression of hypertension. Abnormal blood pressure patterns throughout the day significantly heighten the risk of target organ damage, as well as cardiovascular and cerebrovascular complications.11 According to the 2011 guidelines from the British Hypertension Society, except for patients with stage 3 hypertension, antihypertensive treatment decisions should be guided by dynamic blood pressure monitoring results.
Prior studies have demonstrated that hypertensive patients with abnormal circadian blood pressure rhythms experience imbalances between sympathetic and vagal nerve activity.12 In particular, nocturnal non-dipping blood pressure pattern is closely associated with an increased risk of cardiovascular, cerebrovascular, and renal complications.13,14 While the precise mechanisms underlying non-dipping blood pressure patterns remain unclear, research suggests links to impaired autonomic nervous system function, heightened sympathetic nerve activity, and elevated levels of inflammatory markers.
The pathophysiology of hypertension involves endothelial damage, inflammatory activation, insulin resistance, and platelet activation. Hypertension is not merely characterized by elevated blood pressure but is a complex cardiovascular disorder. Increased blood pressure correlates with higher levels of systemic inflammation, and prolonged inflammatory responses play a critical role in the progression of hypertension. Circulating inflammatory factors are strongly associated with the severity of hypertension and the extent of target organ damage.
Neutrophils, the most abundant white blood cells, are pivotal in responding to inflammation. They release numerous cytokines in response to inflammatory stimuli, such as bacterial infection, cancer, or environmental exposure, thereby initiating and amplifying the inflammatory response. Neutrophils also promote the secretion of inflammatory mediators, including arachidonic acid, myeloperoxidase, superoxide radicals, interleukin-1β, and matrix metalloproteinases.15 Additionally, they activate the renin-angiotensin-aldosterone system and reduce levels of coenzyme II,16 contributing to endothelial dysfunction, arteriosclerosis, and an increased risk of hypertension and arrhythmias. Monocytes play a central role in vascular inflammation and tissue remodeling by secreting chemokines and cytokines, generating reactive oxygen species (ROS), expressing coagulation factors, and transforming into macrophages.17 Lymphocytopenia, a condition linked to blood pressure disorders, is associated with the activation of adaptive immunity and stress responses. Inflammatory responses may induce apoptosis of regulatory lymphocytes, inhibit the secretion of anti-inflammatory factors, and disrupt the balance between anti-inflammatory and pro-inflammatory systems.18 These processes affect vascular homeostasis and promote the development of hypertension. The inflammatory response progressively disrupts the circadian rhythm of blood pressure, increasing sympathetic nervous system activity during nighttime. This disruption exacerbates the release of inflammatory factors and causes further vascular endothelial damage. The interplay of these factors ultimately contributes to the progression of hypertension and increases the risk of target organ damage.
SIRI and LMR are emerging inflammatory markers derived from multiple blood cell components. In this study, SIRI and LMR were demonstrated to be independent risk factors for circadian rhythm abnormalities in young hypertensive patients. Evidence increasingly highlights the critical role of innate and adaptive immune responses in the inflammatory pathways of hypertension. Activated immune cells infiltrate target tissues, causing organ damage by excessively secreting cytokines and chemokines. Monocytes, which are integral to both SIRI and LMR, play a key role in hypertension pathogenesis. LMR, as a novel inflammatory parameter, has been widely studied in cardiovascular diseases. For example, in a small sample single center retrospective study, it was found that LMR is a novel marker of blood pressure variability, connected to target-organ damage, in children with primary and secondary renal hypertension.19 In addition, a retrospective study by Aky ü z, A et al found that SII was an independent predictor of non-dipper hypertension.6 The high SII value in hypertension patients can be used as an early warning parameter to identify non-dipper hypertension patients. Unlike our study, our research indicates that SII has certain predictive value in the single factor analysis stage, but further multivariate analysis has no significant significance. We speculate that besides queue differences, its collinearity with SIRI may also be a potential reason. Monocyte levels are positively correlated with all-cause mortality and cardiovascular disease risk, underscoring their clinical significance.20 Animal studies further support this, demonstrating the influence of inflammatory markers on hypertension outcomes.21,22 For instance, Wenzel et al showed that monocyte depletion reduced blood pressure and improved vascular function in mice.23 Similarly, mice deficient in tumor necrosis factor α (TNFα) or interleukin-6 (IL-6) exhibited lower blood pressure.24 These findings suggest that SIRI and LMR, as comprehensive inflammatory markers, have predictive value comparable to traditional markers.
We also observed significantly higher triglyceride levels in the non-dipper group compared to the dipper group, identifying triglycerides as an independent risk factor for abnormal circadian blood pressure rhythm. This finding suggests that disrupted circadian rhythms and nocturnal sympathetic nerve excitation contribute to elevated nighttime blood pressure and abnormal lipid metabolism. Previous studies have similarly linked elevated LDL levels to the progression of non-dipper hypertension. Hyperlipidemia can stimulate angiotensin-2 receptors, promoting hypertension development.25 Additionally, hyperlipidemia impairs vascular endothelial function and disrupts pressure sensory reflex pathways, further contributing to elevated blood pressure.26 Thus, in addition to managing blood pressure actively, it is crucial to address blood lipid metabolism in hypertensive patients. Prospective studies have established a strong relationship between blood lipids and the development of hypertension. Elevated blood lipid levels independently predict the future risk of hypertension, even in apparently healthy individuals, preceding its onset.27,28
This study found that UA levels were significantly higher in the non-dipper group than in the dipper group, identifying UA as an independent predictor of abnormal circadian blood pressure rhythms in hypertensive patients. Supporting this, a study involving adolescents with hypertension reported that nearly 90% of patients had elevated serum UA levels, a condition rare in healthy individuals.29 Animal studies have shown that elevated UA induces hypertension through mechanisms such as stimulating oxidative stress, impairing endothelial function, and activating the renin-angiotensin system.30 Elevated UA can also lead to renal microvascular disease (arteriosclerosis), contributing to salt-sensitive hypertension that may persist even after UA reduction.31
The subjects of this study were young hypertensive patients aged 18–35, who were significantly characterized by a low incidence of age-related comorbidities. In addition, this population has a single type of antihypertensive medication, a low rate of combination therapy, and minimal interference from non-cardiovascular drugs. The young cohort is not a limitation, but a scientific choice to enhance the intrinsic effectiveness of research. In addition, we found that gender, age, BMI, smoking history, and drinking history had no significant effect on the circadian rhythm of blood pressure. This may be attributed to the narrow age range of the participants and the fact that most subjects were young individuals without underlying diseases.
Nomograms are widely used in predictive models as visual tools to represent the relationships between variables. They graphically display the results of logistic regression analysis, enabling intuitive assessment of disease risk and prognosis based on statistically significant factors. In this retrospective study of 211 hypertensive patients from our hospital, a nomogram was developed to predict abnormal circadian blood pressure rhythms. Scores were assigned to LMR, SIRI, TG, and UA, with the total score reflecting the overall risk level. The predictive ability, consistency, and clinical utility of the model were evaluated and found to be favorable, offering valuable clinical insights. External validation, conducted using data from 203 hypertensive patients from other hospitals, confirmed the model’s reliability and robustness.
Previous studies have developed predictive models for spoon type hypertension based on inflammatory indicators, such as pan-immune-inflammation value (PIV)(AUC=0.725), uric acid/albumin ratio (UAR) (AUC=0.783 95% CI: 0.743–0.822).32,33 The model established in this study has higher predictive accuracy compared to previous studies (AUC=0.883 (95% CI: 0.835–0.931)), has been validated in an independent third-party cohort (AUC=0.844 (95% CI: 0.791–0.896)), making it more generalizable.
The inflammation integration model developed in this study provides a new tool for precise management of hypertension in young people. In the future, it is necessary to verify its generalization in multi center queues and explore the impact of genetic environmental interactions on predictive performance. More importantly, prospective intervention trials will determine whether individualized treatment based on this model can improve prognosis. If the verification is successful, the guideline committee may consider incorporating SIRI and other factors into the risk assessment process for non-dipper hypertension, to supplement the potential application value of inflammation assessment.
It cannot be denied that although we have reduced the impact of some diseases and comorbidities on the study through exclusion criteria, the factors that may cause inflammation and cardiovascular changes are complex and varied, and there may still be potential factors that could lead to model bias. In this study, our univariate analysis results showed that factors such as LDL, HDL, AST, ALT were significant in univariate analysis but not in multivariate analysis, and there may be a risk of overfitting or collinearity.
Conclusions
In conclusion, decreased LMR, increased SIRI, elevated TG, and higher UA levels were identified as independent risk factors for abnormal circadian blood pressure rhythms in young hypertensive patients. This study successfully developed a nomogram-based risk prediction model incorporating LMR, SIRI, TG, and UA as key indicators. The model is simple, rapid to apply, clinically accurate, and holds significant relevance for practical applications in hypertension management.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
All participants provided written informed consent prior to enrolment in this study. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All procedures performed in this study were in accordance with the Declaration of Helsinki (as revised in 2013) and this study was approved by the Ethics Committee of the 901st Hospital of the Chinese People’s Liberation Army Joint Logistics Support Force (No. LY2024YGYB15) and written informed consent for publication of the patients’ information and images was entirely obtained.
Acknowledgments
We would like to thank all the participants who contributed to our research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research, creation, and/or publication of this article was supported by the Hospital Management Project of the 901st Hospital of the Chinese People’s Liberation Army (No. 2024YGYB15). Funders only provide financial support.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Mills KT, Bundy JD, Kelly TN, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation. 2016;134(6):441–450. doi:10.1161/CIRCULATIONAHA.115.018912
2. Araújo S, Rouxinol-Dias A, Mesquita-Bastos J, Silva J, Barbosa L, Polónia J. Ambulatory blood pressure monitoring profiles in a cross-sectional analysis of a large database of normotensive and true or suspected hypertensive patients. Rev Port Cardiol. 2018;37(4):319–327. doi:10.1016/j.repc.2017.07.009
3. Yang WY, Melgarejo JD, Thijs L, et al. Association of office and ambulatory blood pressure with mortality and cardiovascular outcomes. JAMA. 2019;322(5):409–420. doi:10.1001/jama.2019.9811
4. Jin Z, Wu Q, Chen S, et al. The associations of two novel inflammation indexes, sii and siri with the risks for cardiovascular diseases and all-cause mortality: a ten-year follow-up study in 85,154 individuals. J Inflamm Res. 2021;14:131–140. doi:10.2147/JIR.S283835
5. Sarejloo S, Dehesh M, Fathi M, et al. Meta-analysis of differences in neutrophil to lymphocyte ratio between hypertensive and non-hypertensive individuals. BMC Cardiovasc Disord. 2023;23(1):283. doi:10.1186/s12872-023-03304-w
6. Akyüz A, Işık F. Systemic immune-inflammation index: a novel predictor for non-dipper hypertension. Cureus. 2022;14(8):e28176. doi:10.7759/cureus.28176
7. Wang Z, Chen Z, Zhang L, et al. Status of hypertension in China: results from the China Hypertension Survey, 2012–2015. Circulation. 2018;137(22):2344–2356. doi:10.1161/CIRCULATIONAHA.117.032380
8. Sundström J, Neovius M, Tynelius P, Rasmussen F. Association of blood pressure in late adolescence with subsequent mortality: cohort study of Swedish male conscripts. BMJ. 2011;
9. De Venecia T, Lu M, Figueredo VM. Hypertension in young adults. Postgrad Med. 2016;128(2):201–207. doi:10.1080/00325481.2016.1147927
10. Zhang Y, Shi R, Yu L, Ji L, Li M, Hu F. Establishment of a risk prediction model for non-alcoholic fatty liver disease in type 2 diabetes. Diabetes Ther. 2020;11(9):2057–2073. doi:10.1007/s13300-020-00893-z
11. Dai S, Huang B, Zou Y, Liu Y. Associations of dipping and non-dipping hypertension with cardiovascular diseases in patients with dyslipidemia. Arch Med Sci. 2019;15(2):337–342. doi:10.5114/aoms.2018.72609
12. Kohara K, Nishida W, Maguchi M, Hiwada K. Autonomic nervous function in non-dipper essential hypertensive subjects. Evaluation by power spectral analysis of heart rate variability. Hypertension. 1995;26(5):808–814. doi:10.1161/01.hyp.26.5.808
13. Tang A, Yang E, Ebinger JE. Non-Dipping Blood Pressure or Nocturnal Hypertension: does One Matter More? Curr Hypertens Rep. 2024;26(1):21–30. doi:10.1007/s11906-023-01273-1
14. Komori T, Hoshide S, Turana Y, Sogunuru GP, Kario K. HOPE Asia Network. Cognitive impairment in heart failure patients: association with abnormal circadian blood pressure rhythm: a review from the HOPE Asia Network. Hypertens Res. 2024;47(2):261–270. doi:10.1038/s41440-023-01423-7
15. Buso G, Faggin E, Rosenblatt-Velin N, et al. The role of neutrophils in lower limb peripheral artery disease: state of the art and future perspectives. Int J Mol Sci. 2023;24(2):1169. doi:10.3390/ijms24021169
16. Fernandez DM, Giannarelli C. Immune cell profiling in atherosclerosis: role in research and precision medicine. Nat Rev Cardiol. 2022;19(1):43–58. doi:10.1038/s41569-021-00589-2
17. Wenzel P. Monocytes as immune targets in arterial hypertension. Br J Pharmacol. 2019;176(12):1966–1977. doi:10.1111/bph.14389
18. Guzik TJ, Nosalski R, Maffia P, Drummond GR. Immune and inflammatory mechanisms in hypertension. Nat Rev Cardiol. 2024;21(6):396–416. doi:10.1038/s41569-023-00964-1
19. Musiał K, Bargenda-Lange A, Mazurkiewicz P, Gaik M, Gralec S, Zwolińska D. Lymphocyte to monocyte ratio and blood pressure variability in childhood hypertension-a pilot study. Pediatr Res. 2023;93(1):137–142. doi:10.1038/s41390-022-02056-1
20. Zhao S, Dong S, Qin Y, Wang Y, Zhang B, Liu A. Inflammation index SIRI is associated with increased all-cause and cardiovascular mortality among patients with hypertension. Front Cardiovasc Med. 2022;9:1066219. doi:10.3389/fcvm.2022.1066219
21. Maaliki D, Itani M, Jarrah H, et al. Dietary high salt intake exacerbates SGK1-mediated T cell pathogenicity in L-NAME/high salt-induced hypertension. Int J Mol Sci. 2024;25(8):4402. doi:10.3390/ijms25084402
22. Wu O, Wu Y, Zhang X, et al. Causal effect of interleukin (IL)-6 on blood pressure and hypertension: a mendelian randomization study. Immunogenetics. 2024;76(2):123–135. doi:10.1007/s00251-024-01332-0
23. Wenzel P, Knorr M, Kossmann S, et al. Lysozyme M-positive monocytes mediate angiotensin II-induced arterial hypertension and vascular dysfunction. Circulation. 2011;124(12):1370–1381. doi:10.1161/CIRCULATIONAHA.111.034470
24. Brands MW, Banes-Berceli AKL, Inscho EW, Al-Azawi H, Allen AJ, Labazi H. Interleukin 6 knockout prevents angiotensin II hypertension: role of renal vasoconstriction and janus kinase 2/signal transducer and activator of transcription 3 activation. Hypertension. 2010;56(5):879–884. doi:10.1161/HYPERTENSIONAHA.110.158071
25. Endrias EE, Tesfaye Mamito T, Geta Hardido T, Ataro BA. Prevalence of pre-hypertension/hypertension and its associated factors among adults in the Wolaita Zone of Southern Ethiopia: a cross-sectional study. Inquiry. 2024;61:469580241246968. doi:10.1177/00469580241246968
26. Siurana JM, Sabaté-Rotés A, Amigó N, et al. Different profiles of lipoprotein particles associate various degrees of cardiac involvement in adolescents with morbid obesity. Front Pediatrics. 2022;10:887771. doi:10.3389/fped.2022.887771
27. Yin X, Willinger CM, Keefe J, et al. Lipidomic profiling identifies signatures of metabolic risk. EBioMedicine. 2020;51:102520. doi:10.1016/j.ebiom.2019.10.046
28. Xie H, Zhuang Q, Mu J, et al. The relationship between lipid risk score and new-onset hypertension in a prospective cohort study. Front Endocrinol. 2022;13:916951. doi:10.3389/fendo.2022.916951
29. Viazzi F, Antolini L, Giussani M, et al. Serum uric acid and blood pressure in children at cardiovascular risk. Pediatrics. 2013;132(1):e93–99. doi:10.1542/peds.2013-0047
30. Yusnaini R, Nasution R, Saidi N, et al. Ethanolic extract from Limonia acidissima L. Fruit attenuates serum uric acid level via URAT1 in potassium oxonate-induced hyperuricemic rats. Pharmaceuticals. 2023;16(3):419. doi:10.3390/ph16030419
31. Watanabe S, Kang DH, Feng L, et al. Uric acid, hominoid evolution, and the pathogenesis of salt-sensitivity. Hypertension. 2002;40(3):355–360. doi:10.1161/01.hyp.0000028589.66335.aa
32. Ateş MS, Yıldırım A, Sökmen E. Association between pan-immune-inflammation value and dipper/non-dipper status in newly diagnosed hypertensive patients. J Inflamm Res. 2025;18:6217–6228. doi:10.2147/JIR.S522032
33. Toprak K, Özen K, Karataş M, Dursun A. Inflammation-based markers, especially the uric acid/albumin ratio, are associated with non-dipper pattern in newly diagnosed treatment-naive hypertensive patients. Blood Press Monit. 2024;29(5):221–231. doi:10.1097/MBP.0000000000000709
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.