Back to Journals » Drug, Healthcare and Patient Safety » Volume 17
Establishing of a National Diagnostic Reference Level for Radiation Dose in Digital Paediatric Pelvic X-Rays in Jordan: A Multicenter Retrospective Study
Authors AlHawadi M ![]() , Ayasrah M
, Ayasrah M ![]()
Received 21 November 2024
Accepted for publication 29 August 2025
Published 3 October 2025 Volume 2025:17 Pages 197—207
DOI https://doi.org/10.2147/DHPS.S507740
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Siew Siang Chua
Malak AlHawadi, Mohammad Ayasrah
Department of Allied Medical Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid, 22110, Jordan
Correspondence: Mohammad Ayasrah, Department of Allied Medical Sciences Faculty of Applied Medical Sciences, Jordan University of Science and Technology, P.O. Box 3030, Irbid, 22110, Jordan, Tel +96227201000-26939, Fax +96227201087, Email [email protected]
Background: Paediatric pelvic X-rays are essential for diagnosing injuries and developmental abnormalities but pose radiation risks to sensitive children. Dose Reference Levels (DRLs) play a critical role in optimising radiographic procedures, ensuring both safety and high-quality imaging.
Objective: This research aimed to establish a National Dose Reference Level (NDRL) for digital paediatric pelvic X-rays in Jordan to optimise radiation doses, improve diagnostic accuracy, and minimise risks.
Methods: A Multicenter retrospective analysis was performed on paediatric Anterior-Posterior (AP) digital pelvic X-rays from various 12 Jordanian healthcare institutions. Parameters including Kilovoltage peak (kVp), milli Ampere second (mAs), and Focal to Skin Distance (FSD) were collected. Entrance Surface Dose (ESD) was indirectly calculated following international guidelines.
Results: The study analysed 1,674 paediatric pelvic X-rays, finding a mean ESD of 0.69 milli-Gray (mGy). The 75th percentile ESD, or (DRL), was 0.612 mGy overall, with age-specific DRLs of 0.265 mGy (0 to < 1 year), 0.382 mGy (1 to < 5 years), 0.704 mGy (5 to < 10 years), and 0.995 mGy (10 to ≤ 15 years).
Conclusion: The study revealed age-dependent variations and notable disparities in radiation doses among various healthcare institutions in Jordan. Establishing the NDRL of 0.612 mGy provides a benchmark for dose optimisation and aligns Jordan’s practices with international standards. The findings can guide national radiation protection policies and clinical guidelines, enhance paediatric imaging practices, and minimise unnecessary radiation exposure.
Keywords: radiation safety, paediatric radiography, dose reference levels, DRLs, dose optimisation, medical imaging, Jordan
Introduction
Medical imaging (MI) is vital in modern healthcare, providing essential diagnostic information across a wide range of conditions.1 Many MI procedures utilise ionising radiation, including conventional radiography, which remains prevalent in developing countries due to its affordability and accessibility.2,3 Notably, radiologic medical procedures are the main cause of radiation exposure for the public in numerous countries and are the largest contributor to the applications of ionising radiation in the medical domain.3,4 The evolution of X-ray technology and increasing examination complexities have led to higher patient radiation doses.3 Diagnostic X-ray exams account approximately for about 80% of the general population’s radiation exposure.5
Although ionising radiation facilitates accurate diagnoses, it concurrently introduces considerable risks, especially for vulnerable populations like paediatric patients.6 Paediatric pelvic radiography is routinely employed for the assessment of traumatic and congenital injuries, in addition to developmental abnormalities. However, the radiosensitivity of children’s pelvic regions necessitates distinct challenges for radiation management.8 Female paediatric patients exhibit particular vulnerability, given the anatomical location of their ovaries within the radiation field, which leads to a comparatively greater exposure than that experienced by males.9
The use of radiation shielding in paediatric imaging underscores the ongoing debate between protecting patients and maintaining diagnostic image quality. Evidence-based protocols are necessary to reconcile these objectives.6
Establishing DRLs represents an important benchmark for optimising radiation doses in medical imaging procedures, helping identify and reduce unnecessarily high exposure while maintaining diagnostic quality.7,8 The International Commission on Radiological Protection (ICRP) and other international organisations advocate for DRLs to standardise radiation doses and identify unnecessarily high exposures while maintaining diagnostic efficacy.9 ESD is recognised as the primary used for basic radiography evaluations due to its ease of measurement, comparability with international studies, and strong correlation with effective dose.10
Research from the Middle East and North Africa (MENA) region reveals significant discrepancies in reported paediatric DRLs, stemming from variations in imaging techniques, equipment, and procedural protocols. Reported DRLs for paediatric pelvic X-rays range from 1.88 mGy in Iraq11 to 0.63 mGy in Saudi Arabia,12 highlighting the need for standardised national guidelines to ensure paediatric radiation safety and dose optimisation. Iran documented a DRL of 0.59 mGy for children’s pelvis X-rays, reflecting discrepancies even within the region.13
Global variations in DRLs are evident: In Korea, the DRL for pelvic AP projection in 10-year-old patients was set at 1.0 mGy, with a reported range of 0.1 to 5.26 mGy.14 In Kenya, values demonstrated variation from 0.1 mGy for toddlers under one year to 0.36 mGy for children aged 10 to 15 years.15 Portugal’s DRLs ranged from 0.098 mGy for infants to 0.573 mGy for older adolescents,16 while Ethiopia recorded values of 1.05 mGy for younger children and 25.03 mGy for older paediatric cohorts.17 These inconsistencies underscore the necessity for customised national guidelines to ensure paediatric patients’ safety and dose optimisation in paediatric imaging.
Despite the significance of DRLs, Jordan lacks NDRLs for paediatric pelvic X-rays. This deficiency may contribute to substantial variances in radiation doses among healthcare facilities raising concerns about patient overexposure and associated radiation risks, as well as underexposure that could compromise diagnostic accuracy.18
This study aims to establish NDRLs for paediatric pelvic X-rays in Jordan, investigating variations caused by imaging equipment, procedures, and operator training.
In this study, age-based DRLs were selected in preference to weight or height, primarily for their clinical practicality and consistency with global dose assessment procedures. This age-based grouping facilitates the implementation of DRLs in clinical settings, particularly where weight or height data might be inconsistent or unavailable across various institutions.19 Moreover, age groups more precisely reflect skeletal and tissue development, establishing them as a reliable metric for dose optimisation in paediatric imaging.20
The establishment of NDRLs in Jordan is anticipated to significantly impact policy and clinical practice. It will facilitate the reduction of excessive radiation exposure by providing standardised dose benchmarks, thereby ensuring diagnostic efficacy. The findings will align of Jordan’s radiology practices with international standards, improving radiation safety and advancing best practices in paediatric imaging. The implementation of NDRLs can inform national healthcare policies, directing future initiatives to enhance dose monitoring, training, and equipment optimisation within Jordanian medical institutions.17 All abbreviations used throughout this manuscript are defined in Supplementary Material Table S1.
Methods
Study Design
This multicenter retrospective study aimed to establish an NDRL for digital paediatric pelvic X-rays in Jordan. The inclusion criteria for this study comprised paediatric patients 15 years old and below who underwent AP digital pelvic X-ray examinations from June 2022 to June 2023 within any of the participating healthcare institutions, provided their imaging records were complete with all essential exposure parameters such as kVp, mAs, and FSD. Patients were excluded if they were over 15 years of age, had imaging performed for non-pelvic conditions, had incomplete exposure data, were imaged outside the participating centers, or if their images were of poor quality or contained technical errors.
The study was conducted across 12 healthcare institutions in Jordan, which were strategically chosen to encompass regional variation and differing capacities of healthcare service provision. This cohort included six governmental hospitals (MOH), one university hospital (UNIV), three Royal Medical Services hospitals (RMSH), and two private hospitals (PRIV).
Equipment and Quality Control Measures
The study used a variety of digital X-ray machines, including Digital Radiography (DR) and Computed Radiography (CR) systems, from different manufacturers and models, as detailed in Supplementary Table S2.
The retrospective nature of the study precluded the application of direct quality control (QC) procedures. However, the large sample size and the inclusion of several institutions enhanced the representativeness of the findings for paediatric pelvic X-rays performed in Jordan.
Sample Size and Technique
The sample population was sourced from the Jordan Bureau of Statistics. The sample size was calculated using Daniel’s formula (1).

where:
n = sample size,
Z = the level of confidence of 95%, which is conventional; the Z value is 1.96
P = expected prevalence or proportion (in proportion of one; if 20%, P = 0.2)
d = precision (5%, d = 0.05).
An initial sample size of 346 was derived; however, to address concerns regarding missing data and to achieve greater statistical power, the final sample size was augmented to 1,674. This expansion enabled precise evaluations of radiation exposure in paediatric pelvic X-rays, contributing to the formulation of a NDRL in Jordan. To guarantee proportional representation, institutions were selected using a stratified random method, categorised by healthcare facility type (MOH, UNIV, RMS, PRIV) and geographic location.
To minimise potential bias from missing data, available-case analysis was performed, allowing for the inclusion of all available information without discarding complete cases. Additionally, missing exposure parameters were retrieved from Digital Imaging and Communications in Medicine (DICOM) metadata and manually verified against hospital records, thereby reducing data loss.
Data Collection and ESD Calculation
DICOM tags were used to extract the data from the X-ray images, or the patient’s age at the time of the request, gender, and exposure factors like kVp, mA, exposure time, and FSD were collected manually through the electronic healthcare medical system.
Paediatric patients, from newborn to 15 years, were categorised into four non-overlapping age groups: 0 to <1 year, 1 to <5 years, 5 to <10 years, and 10 to ≤15 years. This classification was based on developmental stages, institutional imaging protocols, and the Jordanian Bureau of Statistics’ demographic standards. Age-based grouping was chosen over weight or height for its practicality in clinical environments, alignment with international guidelines (eg, ICRP and the European Commission), and strong correlation with skeletal maturation, making it a reliable criterion for dose assessment in paediatric X-ray imaging.21 Additionally, this approach ensures comparability with local and regional dose surveys and reflects actual imaging practices across Jordan.
The DRL paediatric pelvic radiography was determined based on European Commission and ICRP guidelines.9,22 The ESD was computed utilising the exposure parameters documented for each patient. Hospitals where FSD data could not be collected due to time constraints were classified as having no data availability. However, all participating institutions included in the study routinely collect FSD from imaging services. The ESD was calculated using the following equation 2:23

ESD = skin dose in mGy,
c = a constant with a value of 0.2775
kVp =Kilo volts peak
FSD = Focus skin distance in m
mA = Milliampere
mm.Al = the total filtration Aluminum in mm
All calculations were automated in Excel, allowing for efficient computation of patient-specific radiation doses.
Data Analysis
Continuous variables were presented as mean ± standard deviation (SD), and categorical variables were illustrated through counts and corresponding percentages. Following the ICRP 135 recommendations, the NDRLs were determined as the 75th percentile (third quartile) of the mean distribution in the sample.9 The Shapiro–Wilk test was employed to evaluate the normality of continuous variables, ascertaining if the data satisfied the prerequisites for parametric tests. Since the study included a large sample size, analysis of variance (ANOVA) was used to examine potential differences in ESD across different groups or categories, with statistical significance established at p < 0.05.
The pairwise deletion method was used to deal with missing data, ensuring that available data were preserved for analysis while avoiding the exclusion of entire cases. All data analyses were performed using IBM SPSS software, version 26.0.
Ethical Consideration
Ethical approval for the study was obtained from the Institutional Review Board (IRB) at Jordan University of Science and Technology, with approval granted on 1/11/2023 No. 34/164/2023.
Results
Demographic Profile
The study included a total of 1,674 paediatric patients with a virtually balanced gender distribution: 49.6% (n=831) female and 50.4% (n=843) male. The age distribution showed a relatively balanced profile, with a greater proportion of younger patients. The 0– <1 year cohort constituted 28.9% (n=483), succeeded by the 1– <5 year cohort at 27.7% (n=463), the 5– <10 year cohort at 22.5% (n=376), and the 10 – ≤15 year cohort at 21.0% (n=352). The detailed demographic distribution across healthcare institutions is presented in Table 1.
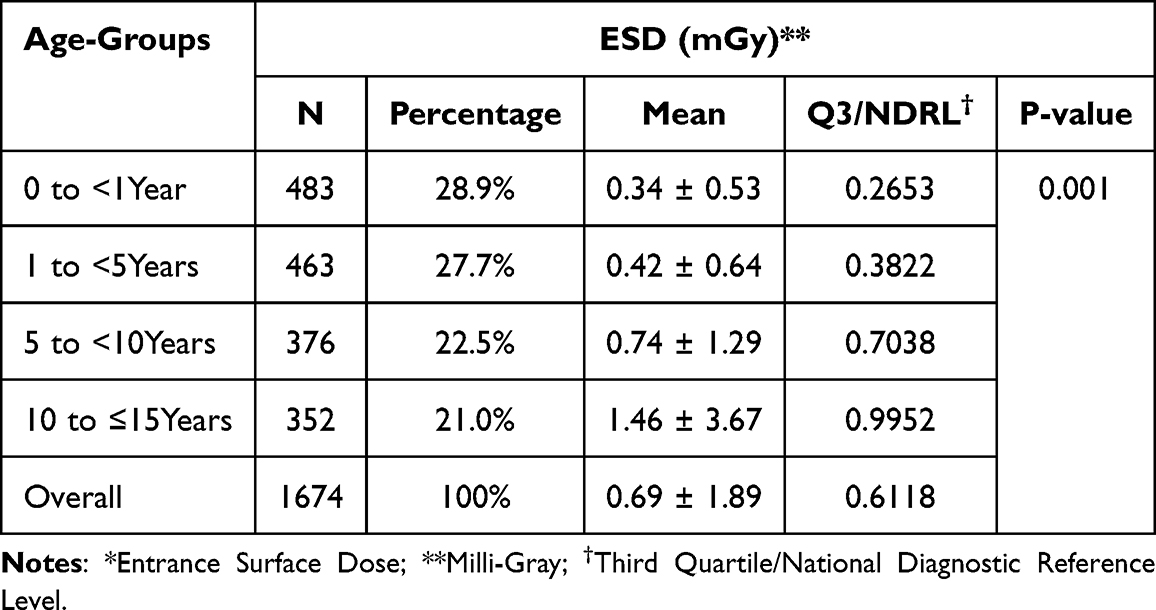 |
Table 1 Descriptive Statistics and ANOVA Results for ESD* by Age Groups |
Technical Parameters
Preliminary assessment of data distribution was performed using the Shapiro–Wilk test to inform the selection of appropriate descriptive statistics for the technical parameters. The results showed statistically significant deviations from normality for all variables: kVp (p < 0.001), mAs (p < 0.001), FSD (p < 0.001), and ESD (p < 0.001). Although kVp and FSD showed near-normal distribution visually, the statistical tests indicated non-normality. Accordingly, descriptive statistics are presented using mean ± SD for consistency and interpretability.
The average kVp was 68.41 ± 8.48, the average mAs was 6.12 ± 9.53, the average FSD was 88.48 cm ± 4.41, and the average ESD was 0.69 mGy ± 1.89. As shown in Table 2, exposure factors such as kVp, mAs, and FSD vary across paediatric age groups. These variations reflect clinical practice adjustments based on patient size and imaging needs. Table 2 also presents the variations in mean kVp, mAs, and FSD values among different age groups, including the overall means. The overall mean and SD for ESD are presented in Table 1.
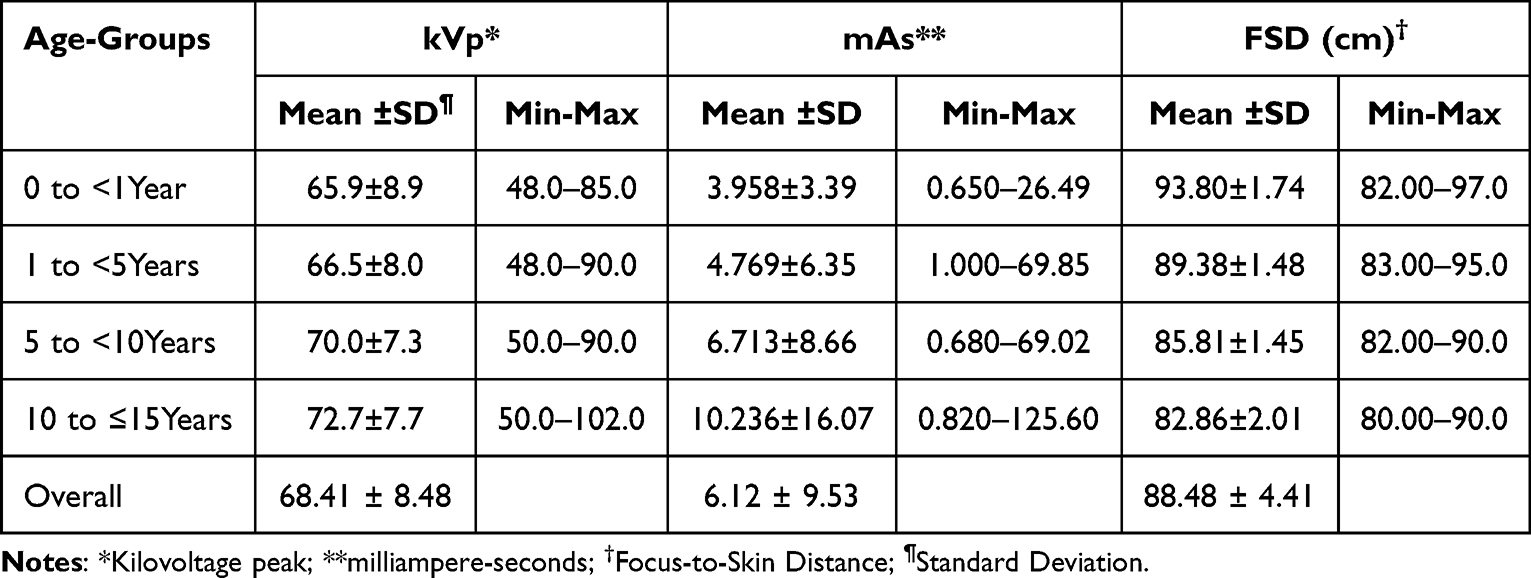 |
Table 2 kVp, mAs, and FSD by Age Group |
Diagnostic Reference Level
The evaluation of ESD across different age groups in Jordan demonstrated inconsistencies related to differences in patient size and imaging protocols. The mean ESD demonstrated an increasing trend with age, beginning at 0.35 mGy for the 0 – <1 year cohort (SD 0.53 mGy) and rising to 1.46 mGy in the 10 – ≤15-year cohort (SD 3.67 mGy). The youngest group exhibited minimal variability, whereas the 10–15-year cohort demonstrated the greatest variability, with Q3/DRL values attaining 0.995 mGy.
The ANOVA conducted on age groups and ESD revealed statistically significant differences in mean ESD across the age groups (P-value = 0.001), as shown in Table 1. This analysis was essential in assessing whether radiation dose levels differed significantly with patient age, thereby ensuring the appropriate establishment of age-based DRLs. These findings underscore the importance of modifying exposure parameters according to patient age to enhance radiation safety and reduce unnecessary exposure in paediatric imaging.
Hospital-Specific ESD Analysis
Table 3 shows notable differences in ESD values amongst hospitals. Hospitals like UNIV1 and PRIV2 recorded the lowest mean ESDs, indicating compliance with dose optimisation protocols. In contrast, MOH5 and RMSH2 demonstrated the highest mean ESDs, with MOH5 showing the widest range (0.413–55.260 mGy), reflecting significant variability in imaging practices that requires further investigation.
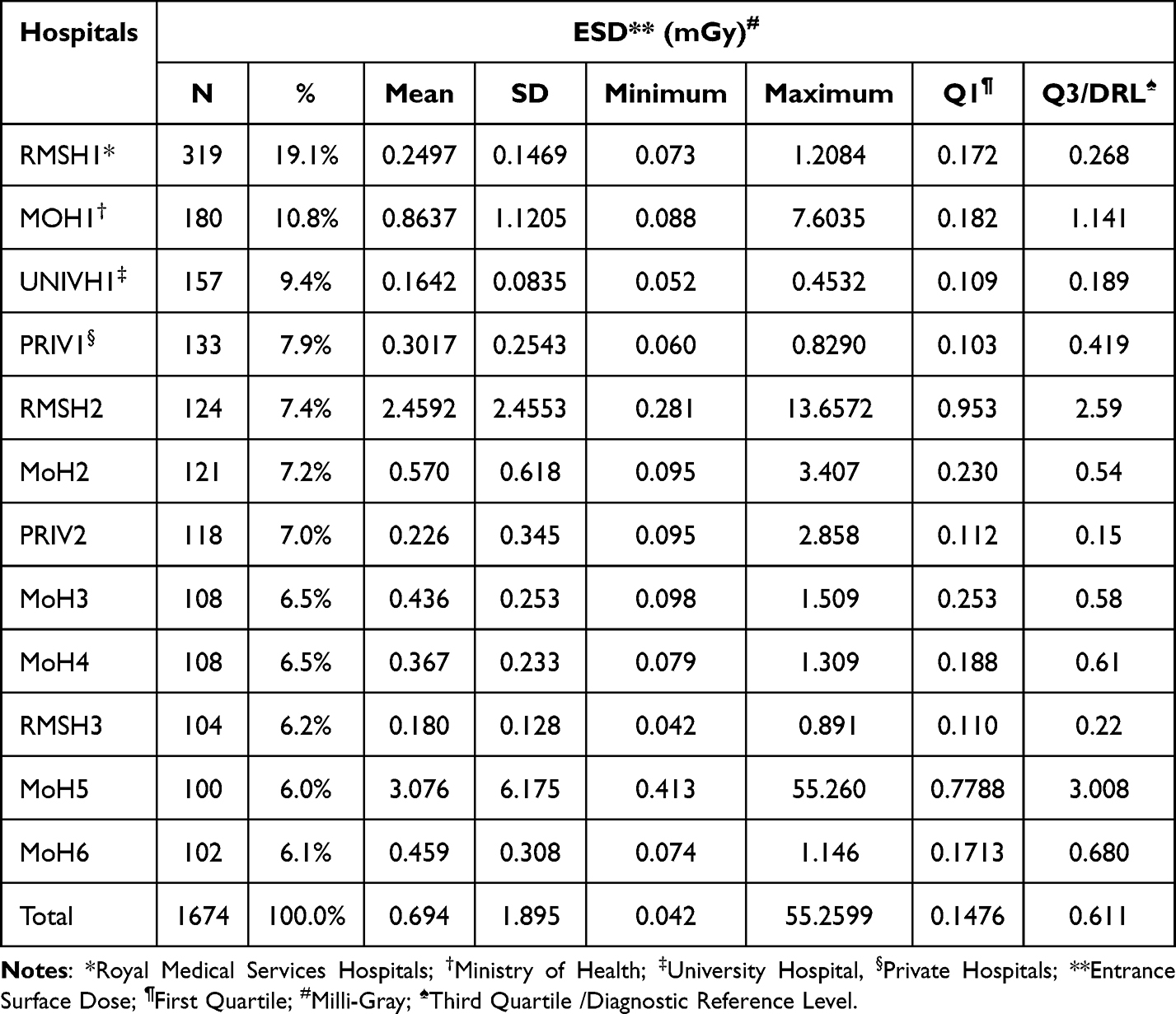 |
Table 3 Demographic and Dose Distribution by Hospital |
Discussion
Accurate establishment of NDRLs requires surveying diverse healthcare institutions to ensure data representation.24 This study examined the ESD received by 1,674 paediatric patients, categorised into four non-overlapping age groups: 0 to <1 year, 1 to <5 years, 5 to <10 years, and 10 to ≤ 15 years.
International and national authorities advocate for compliance with the DRLs as a key tool for enhancing patient outcomes by minimising unnecessary radiation exposure while ensuring diagnostic consistency.9 Paediatric patients demonstrate increased radiosensitivity attributed to their developing tissues and extended life expectancy, which requires careful dose optimisation.25 DRLs offer a framework for recognising and managing excessively high doses, ensuring that radiation exposure remains at levels essential for meeting clinical goals while maintaining safety standards.17,26 Minimising variability in imaging practices enhances diagnostic confidence and consistency across institutions. Furthermore, compliance with NDRLs guarantees that all healthcare sectors have equitable access to optimal radiation doses.27
This study is the first nationwide endeavor in Jordan to establish NDRLs based on ESD values and assess DRLs for paediatric pelvic X-rays. The findings indicate an ESD third quartile (Q3/DRL) of 0.612 mGy and a mean ESD of 0.694 mGy. Comparing Jordanian DRLs with international benchmarks reveals both similarities and discrepancies, as shown in Table 4. The DRL established in this study is lower than those reported in Iraq (1.88 mGy) 34 and Nigeria (0.85 mGy),17,28 yet they are comparable to Saudi Arabia (0.63 mGy)23 and Iran (0.59 mGy).3 In contrast, Jordanian DRLs exceed those recorded in Portugal (0.192–0.573 mGy)26 and Kenya (0.1–0.36 mGy).28 The large variety of ESD values (0.04–55.26 mGy) in this study is due to the bigger sample size of 1,674 compared to 240 to 450 in Ademola’s study and the broad range of digital radiography.11
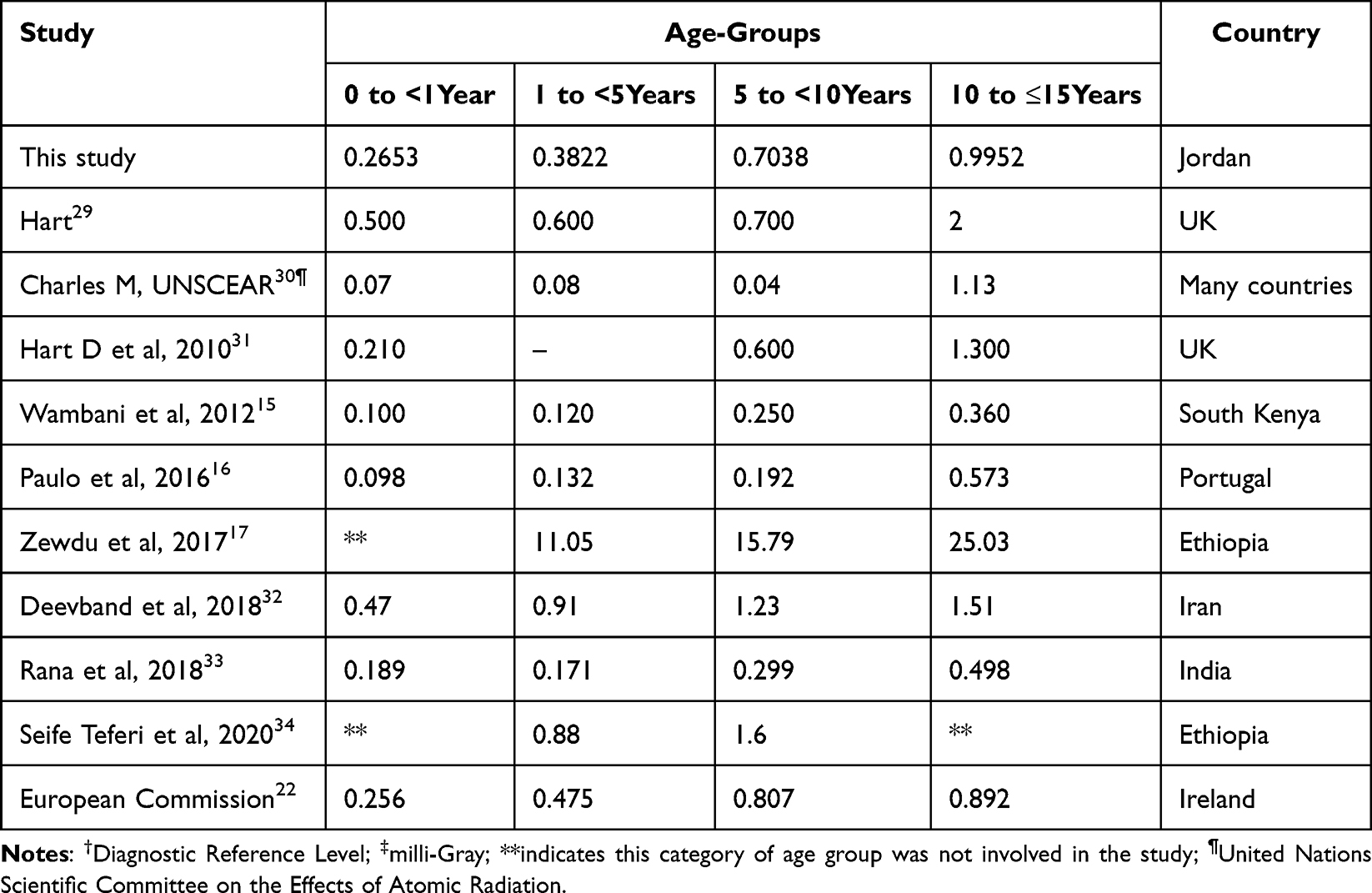 |
Table 4 Comparison of DRL† Values (mGy) ‡in Jordan with Internationally Published DRLs |
The variations in DRLs among different studies and countries arise from disparities in healthcare infrastructure, imaging techniques, patient demographics, radiographic protocols, equipment calibration, and regulatory standards.35 This study used digital radiography, which normally reduces radiation doses as compared to traditional techniques.36 Research involving smaller sample sizes may yield elevated DRLs due to patient variability, while larger datasets, as used in this study, offer more accurate dose estimates.28 Exposure parameters, including kVp, mA, and FSD, significantly affect radiation dose levels.37 Countries with established NDRLs frequently report lower DRLs as a result of strict compliance with international radiation safety standards.38,39 Higher DRLs in Iraq and Ethiopia (15.79–25.03 mGy for older paediatric patients) indicate challenges including limited access to advanced radiographic equipment, inconsistent protocols, and insufficient training. To align Jordanian practices with global standards, investment in infrastructure, regulatory oversight, and improved radiology training programs is necessary.
As depicted in Figure 1, the ESD demonstrates an increase with age, suggesting that greater radiation doses are required for older patients due to anatomical differences.
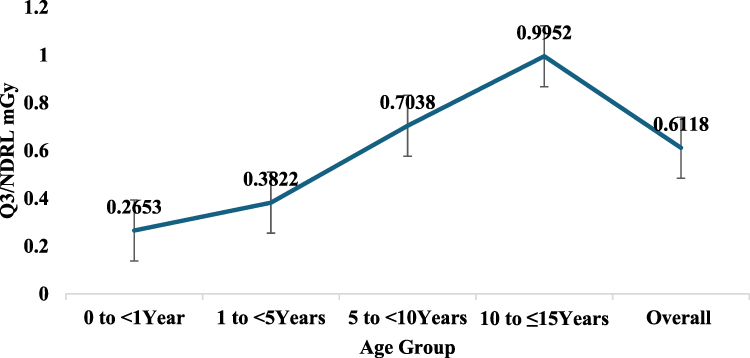 |
Figure 1 The (Q3/DRL) for (ESD) across paediatric age groups and the total population in Jordan. |
Statistical analysis using ANOVA (P-value = 0.001; Table 1) revealed significant variations in average ESD across different age groups, a crucial insight for the accurate determination of age-based DRLs. This trend aligns with findings from the majority of DRL studies.15–17,26,31–34 Furthermore, the DRL values presented in this study are lower than those documented by Zewdu et al,17 Deevband et al,32 the National Radiological Protection Board (NRPB)-W14 report,29 and Seife Teferi et al,34 yet they exceed those reported by Wambani et al,15 Paulo et al,16 and Rana et al.33
In contrast, the DRL values in this study are mostly higher than those in the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) report, except for the age group of 10 to 15 years, where this study shows a lower value of 0.9952 mGy compared to 1.13 mGy in the UNSCEAR report.
This variation in DRL values across age groups is also apparent in similar studies conducted in European countries.9
A comparison of the ESD values across healthcare sectors reveals substantial differences in radiation exposure practices from the NDRL of 0.611 mGy, as illustrated in Figure 2.
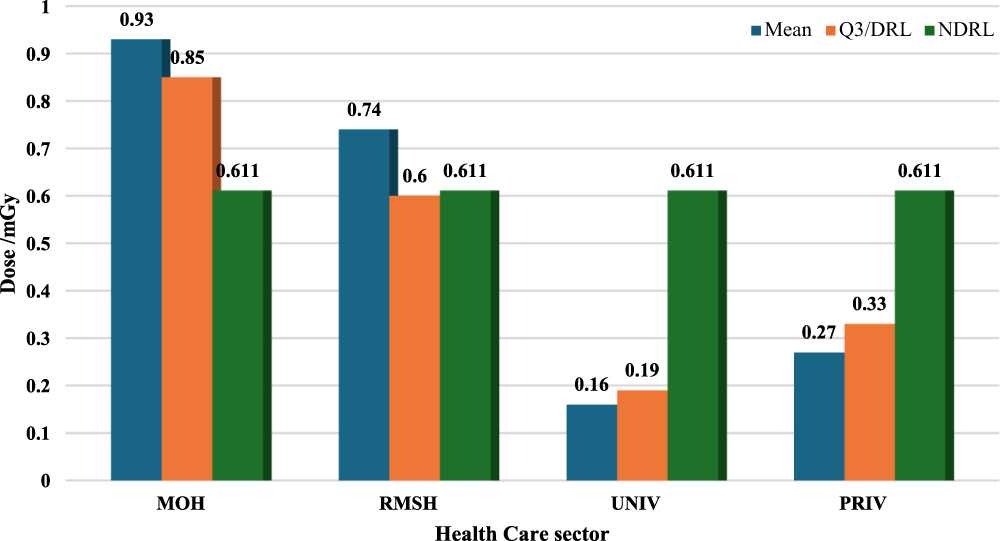 |
Figure 2 Comparison of the ESD, (Q3/DRL), and (NDRL) across healthcare sectors in Jordan. |
The observed variations in DRLs among healthcare sectors underscore the necessity for standardised equipment and protocols.33 Such differences frequently stem from variations in imaging parameters like kVp and filtration, patient habits, equipment calibration, operator proficiency, and institutional protocols. The inconsistent use of Automatic Exposure Control (AEC) and the absence of dedicated paediatric radiology units in numerous facilities further amplify these discrepancies.11,17,28
Mitigating these issues necessitates regulatory supervision, specialised training, and investments in contemporary radiography technology to guarantee adherence to national and international standards.11 Institutions such as MOH and RMSH had considerable ESD variability, with MOH surpassing the national DRL by 52%. Conversely, UNIV and PRIV exhibited superior dose optimisation. Improving training and performing regular audits are crucial for aligning practices with NDRLs and ensuring uniform radiation safety across the nation.11,17
Considerable variability in radiation doses among hospitals was observed in this study, stemming from differences in exposure parameters including kVp, mAs, and FSD. A key finding was that kVp values for younger age groups frequently did not align with European Commission recommendations (60–80 kVp for 0–1 year; 100–120 kVp for 5 years and older).9,24,32 This discrepancy is likely due to the lack of a standardised NDRL, inconsistent quality control, and operator-dependent practices. Implementing kVp settings according to these guidelines could standardise dose levels and minimise unnecessary radiation exposure.40 Although FSD values were consistently 100 cm, optimising other parameters such as filtration and AEC remains crucial for improving dose uniformity and reducing overall variability.9,31,41
The study’s findings reveal significant challenges in paediatric radiology, such as insufficient training for imaging personnel and the lack of specialised paediatric radiology units.17 Many Jordanian facilities utilise general X-ray equipment, which may not be optimised for paediatric imaging, resulting in inconsistent radiation doses. These disparities underscore the need for dedicated paediatric imaging departments and continuous educational initiatives for radiology staff.11 These initiatives are vital for achieving compliance with NDRLs and guaranteeing equitable access to safe, high-quality imaging for all paediatric patients, thereby meeting international radiation protection requirements.
Apart from infrastructure development and training monitoring, adherence to NDRLs is vital for their effective implementation.39 These systems aggregate dose data from multiple healthcare institutions and generate reports for regulatory oversight, facilitating continuous evaluation and refinement of NDRLs. Additionally, automated dose monitoring software, when integrated with imaging equipment, offers real-time feedback to radiology teams, facilitating adherence to dose thresholds and highlighting areas for improvement.15 Routine audits and institutional dose reviews would enhance compliance with NDRLs, reduce variability in exposure levels, and improve overall patient safety within Jordanian healthcare sectors.37 These regulatory measures, when implemented effectively, would enhance adherence to NDRLs, decrease variability, and strengthen patient safety across the nation.
This study establishes a benchmark for paediatric pelvic X-ray radiation doses in Jordan, though its generalisability beyond the sample should be acknowledged. The inclusion of multiple healthcare sectors—public, university, military, and private hospitals—enhances the findings’ relevance to the broader Jordanian healthcare system. However, variations in imaging protocols, equipment calibration, and operator experience among institutions may limit direct extrapolation to other countries or regions with different healthcare infrastructures. Despite this, the study’s adherence to international dose assessment methodologies makes it a valuable reference for establishing NDRLs in similar contexts, particularly in Middle Eastern or developing nations facing comparable radiographic practices and healthcare challenges. Future research incorporating additional regions and larger datasets could further validate these findings globally.
Limitations of the Study
This study, despite extensive data gathering and analysis, is subject to certain limitations. The retrospective nature of the research could have introduced biases during data collection. Moreover, the sample size may not fully represent the Jordanian paediatric population, which limits the generalisability of the findings. Additionally, variations in imaging equipment and techniques across healthcare facilities might have impacted the accuracy and reliability of the study’s outcomes.
Conclusion
This study established an NDRL of 0.6118 mGy for paediatric pelvic X-rays in Jordan, illustrating that radiation dose is age-dependent and varies among healthcare facilities. This variation stems from factors including exposure settings, technician proficiency, and quality control protocols. The study’s retrospective methodology and inherent data variability constitute its primary limitations. Future research should prioritise longitudinal DRL studies, concerted quality control initiatives, and the refinement of paediatric imaging techniques. These endeavours are essential for augmenting radiation safety and informing national guidelines to foster consistent and safer imaging practices.
Data Sharing Statement
The data that supports the findings of this study is available from the corresponding author upon reasonable request.
Ethical Approval
This retrospective study received approval from the IRB at Jordan University of Science and Technology (Approval No. 34/164/2023, dated 1/11/2023), confirming adherence to ethical standards. The study aimed to establish DRLs for radiation exposure from digital paediatric pelvic X-rays in Jordan, utilising anonymised, pre-existing healthcare data without direct patient involvement. Parental consent was waived by the IRB due to the absence of patient interaction and identifiable information. Data management followed stringent confidentiality protocols, ensuring patient privacy and upholding the ethical principles of the Declaration of Helsinki.
Author Contributions
The authors collectively made significant contributions to this work, from its initial conception and study design through execution, data acquisition, analysis, and interpretation. They were all involved in drafting, revising, or critically reviewing the article, granted final approval for the version to be published, agreed on the journal for submission, and assume joint accountability for all aspects of the work.
Funding
This research was funded by the Deanship of Research at Jordan University of Science and Technology (JUST) No. 20230660.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. European Society of Radiology. 2009 The future role of radiology in healthcare. Insights Imaging. 2010;1(1):2–11. doi:10.1007/s13244-009-0007-x.
2. Hussain S, Mubeen I, Ullah N, et al. Modern diagnostic imaging technique applications and risk factors in the medical field: a review. Biomed Res. Int. 2022;2022:1–19. doi:10.1155/2022/5164970
3. Shamsi K, Monfared AS, Deevband MR, et al. Evaluation of effective dose and entrance skin dose in digital radiology. Pol. J. Med. Phys. Eng. 2020;26(2):119–125. doi:10.2478/pjmpe-2020-0013
4. Ogundare FO, Ajibola CL, Balogun FA. Survey of radiological techniques and doses of children undergoing some common x-ray examinations in three hospitals in Nigeria. Med Phys. 2004;31(3):521–524. doi:10.1118/1.1644671
5. Sonawane AU, Shirva VK, Pradhan AS. Estimation of skin entrance doses (SEDs) for common medical X-ray diagnostic examinations in India and proposed diagnostic reference levels (DRLs). Radiat Prot Dosimetry. 2010;138(2):129–136. doi:10.1093/rpd/ncp235
6. Samara ET, Saltybaeva N, Sans Merce M, Gianolini S, Ith M. Systematic literature review on the benefit of patient protection shielding during medical X-ray imaging: towards a discontinuation of the current practice. Phys Med. 2022;94:102–109. doi:10.1016/j.ejmp.2021.12.016
7. Harrison JD, Balonov M, Bochud F, et al. The use of dose quantities in radiological protection: ICRP publication 147 Ann ICRP 50(1) 2021. J Radiol Prot. 2021;41(2):410–422. doi:10.1088/1361-6498/abe548
8. Vassileva J, Rehani M. Diagnostic Reference Levels. Am J Roentgenol. 2015;204(1):W1–W3. doi:10.2214/AJR.14.12794
9. Vañó E, Miller DL, Martin CJ, et al. ICRP publication 135: diagnostic reference levels in medical imaging. Ann ICRP. 2017;46(1):1–144. doi:10.1177/0146645317717209
10. Ahmed NA, Basheir EH, Farah AB, Mohammedzein TS, Suliman II. Proposed national diagnostic reference levels for standard radiographic x-ray procedures in Sudan. Radiat Prot Dosimetry. 2020;190(4):419–426. doi:10.1093/rpd/ncaa114
11. Ali RMKM, Mraity HAAB, Hadi BH, Dana SH. Estimation of skin radiation dose from common radiographic examinations: a preliminary study to establish diagnostic reference levels (DRLs). Medico Legal Update. 2020;20(4):431–437. doi:10.37506/mlu.v20i4.1854
12. Abdallah Y. Measurement of entrance skin dose in radiographic examinations of paediatric patients. CMIR. 2021;17(11):1385–1389. doi:10.2174/1573405617666210628162238
13. Karami V, Zabihzadeh M, Keshtkar M. Evaluation of the Entrance Surface Dose (ESD) and radiation dose to the radiosensitive organs in paediatric pelvic radiography. ijp. Int J Pediatr. 2017. doi:10.22038/ijp.2017.22364.1873
14. Lee SY, Park SM. DBpia. Available from: https://www.dbpia.co.kr.
15. Wambani JS, Korir GK, Korir IK, Kilaha S. Establishment of local diagnostic reference levels in paediatric screen-film radiography at a children’s hospital. Radiat Prot Dosimetry. 2013;154(4):465–476. doi:10.1093/rpd/ncs270
16. Paulo G, Vaño E, Rodrigues A. Diagnostic reference levels in plain radiography for paediatric imaging: a Portuguese study. Radiography. 2016;22(1):e34–e39. doi:10.1016/j.radi.2015.07.002
17. Zewdu M, Kadir E, Berhane M. Assessment of paediatrics radiation dose from routine x-ray examination at jimma university hospital, Southwest Ethiopia. Ethiop J Health Sci. 2017;27(5):481–490. doi:10.4314/ejhs.v27i5.6
18. Health C for D and R. White Paper. Initiative to reduce unnecessary radiation exposure from medical imaging. FDA. Available from: https://www.fda.gov/radiation-emitting-products/initiative-reduce-unnecessary-radiation-exposure-medical-imaging/white-paper-initiative-reduce-unnecessary-radiation-exposure-medical-imaging.
19. Agency IAE. Radiation protection in paediatric radiology.Int Atomic Energy Agency.2013;1–111.
20. Guo H, Liu WY, He XY, Zhou XS, Zeng QL, Li BY. Optimising imaging quality and radiation dose by the age-dependent setting of tube voltage in paediatric chest digital radiography. Korean J Radiol. 2013;14(1):126–131. doi:10.3348/kjr.2013.14.1.126
21. Alhailiy A, Alkhybari E, Alghamdi S, Fisal N, Aldosari S, Albeshan S. Reporting diagnostic reference levels for paediatric patients undergoing brain computed tomography. Tomography. 2023;9(6):2029–2038. doi:10.3390/tomography9060159
22. European Commission. Directorate General for Energy. European Study on Clinical Diagnostic Reference Levels for X-Ray Medical Imaging:EUCLID. 2021. Available from: https://data.europa.eu/doi/10.2833/031357.
23. Eljak SNA, Ayad CE, Abdalla EA. Evaluation of entrance skin radiation exposure dose for pediatrics examined by digital radiography at Asser Central Hospital-KSA. OJRad. 2015;05(03):125–130. doi:10.4236/ojrad.2015.53019
24. Olarinoye OI, Ibrahim S. A protocol for setting dose reference level for medical radiography in Nigeria: a review. Bayero J Pure Appl Sci. 2010;3. doi:10.4314/bajopas.v3i1.58748
25. Ababneh ZQ, Ababneh AM, Bani Hani MS, Ababneh RS, Aljarrah KM. Assessment of patient radiation dose during conventional diagnostic x-ray examinations in three public hospitals in northern jordan using TLDs. Health Physics. 2020;118(6):593. doi:10.1097/HP.0000000000001155
26. Olowookere CJ. A preliminary radiation dose audit in some nigerian hospitals: need for determination of National Diagnostic Reference Levels (NDRLs). Pac J Sci Technol. 2012;13:9.
27. Thomas P. National diagnostic reference levels: what they are, why we need them and what’s next. J Med Imaging Radiat Oncol. 2022;66(2):208–214. doi:10.1111/1754-9485.13375
28. Ademola AK, Obed RI, Adejumobi CA, Abodunrin OP, Alabi OF, Oladapo M. Assessment of entrance skin dose in routine x-ray examinations of chest, skull, abdomen and pelvis of children in five selected hospitals in nigeria. IOSR J Applied Physics. 2013;5(2):47–50. doi:10.9790/4861-0524750
29. Hart D, Hillir M, Wall B. BRPB-W14: Doses to Patients From Medical X-Ray Examinations in the UK. 2000 Review. UK: NRPB-National Radiological Protection Board; 2002. Available from: https://assets.publishing.service.gov.uk/media/5a80aaa6ed915d74e33fbb84/2002_NrpbW14.pdf.
30. Charles M. UNSCEAR report 2000: sources and effects of ionizing radiation. united nations scientific committee on the effects of atomic radiation. J Radiol Prot. 2001;21(1):83–86. doi:10.1088/0952-4746/21/1/609
31. Wall BF, Haylock R, Jansen JT, Hillier MC, Hart D, Shrimpton PC. Radiation Risks From Medical X-Ray Examinations as a Function of the Age and Sex of the Patient. Didcot: Health Protection Agency; Oct 2011.
32. Deevband M. The national diagnostic reference level in routine digital radiography examinations in Iran. BJSTR. 2018;7(5). doi:10.26717/BJSTR.2018.07.001578
33. Rana BS, Kumar S, Sandhu IS, Singh NP. Dosimetry of adult and pediatric patients for common digital radiography examinations. Radiat Prot Dosimetry. 2018;179(4):349–357. doi:10.1093/rpd/ncx293
34. Teferi S, Zewdeneh D. Variation of paediatric doses undergoing digital and computed radiography examination in Addis Ababa, Ethiopia. Ethiop J Health Sci. 2020;30(2):269–276. doi:10.4314/ejhs.v30i2.15
35. Malik MMUD, Alqahtani M, Hadadi I, AlQhtani AGM, Alqarni A. An analysis of computed tomography diagnostic reference levels in India compared to other countries. Diagnostics. 2024;14(15):1585. doi:10.3390/diagnostics14151585
36. Dudhe SS, Mishra G, Parihar P, Nimodia D, Kumari A. Radiation dose optimisation in radiology: a comprehensive review of safeguarding patients and preserving image fidelity. Cureus. 16(5):e60846. doi:10.7759/cureus.60846
37. Suliman II. Estimates of patient radiation doses in digital radiography using DICOM information at a large teaching hospital in Oman. J Digit Imaging. 2020;33(1):64–70. doi:10.1007/s10278-019-00199-y
38. Clerkin C, Brennan S, Mullaney LM. Establishment of national diagnostic reference levels (DRLs) for radiotherapy localisation computer tomography of the head and neck. Rep Pract Oncol Radiother. 2018;23(5):407–412. doi:10.1016/j.rpor.2018.07.012
39. Rao S, Sharan K, Sukumar S, et al. Systematic review on diagnostic reference levels for computed tomography examinations in radiation therapy planning. Diagnostics. 2023;13(6):1072. doi:10.3390/diagnostics13061072
40. Lakhwani OP, Dalal V, Jindal M, Nagala A. Radiation protection and standardization. J Clin Orthop Trauma. 2019;10(4):738–743. doi:10.1016/j.jcot.2018.08.010
41. Schibilla (CEC), K. Schneider (D). European Guidelines On Quality Criteria For Diagnostic Radiographic Images In Paediatrics. Available from: https://www.sprmn.pt/pdf/EuropeanGuidelinesEur16261.pdf.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.