Back to Journals » Journal of Multidisciplinary Healthcare » Volume 10
Establishing community-based integrated care for elderly patients through interprofessional teamwork: a qualitative analysis
Authors Asakawa T, Kawabata H, Kisa K, Terashita T ![]() , Murakami M, Otaki J
, Murakami M, Otaki J
Received 21 June 2017
Accepted for publication 5 August 2017
Published 11 October 2017 Volume 2017:10 Pages 399—407
DOI https://doi.org/10.2147/JMDH.S144526
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Tomohiro Asakawa,1 Hidenobu Kawabata,1 Kengo Kisa,2 Takayoshi Terashita,3 Manabu Murakami,4 Junji Otaki1
1Department of Medical Education and General Medicine, Graduate School of Medicine, Hokkaido University, Sapporo, 2Kutchan-Kosei General Hospital, Kutchan, Hokkaido, 3Graduate School of Radiological Technology Gunma Prefectural College of Health Sciences, Kamioki-machi, Maebashi, Gunma, 4International Relations Office, Graduate School of Medicine, Hokkaido University, Sapporo, Hokkaido, Japan
Background: Working in multidisciplinary teams is indispensable for ensuring high-quality care for elderly people in Japan’s rapidly aging society. However, health professionals often experience difficulty collaborating in practice because of their different educational backgrounds, ideas, and the roles of each profession. In this qualitative descriptive study, we reveal how to build interdisciplinary collaboration in multidisciplinary teams.
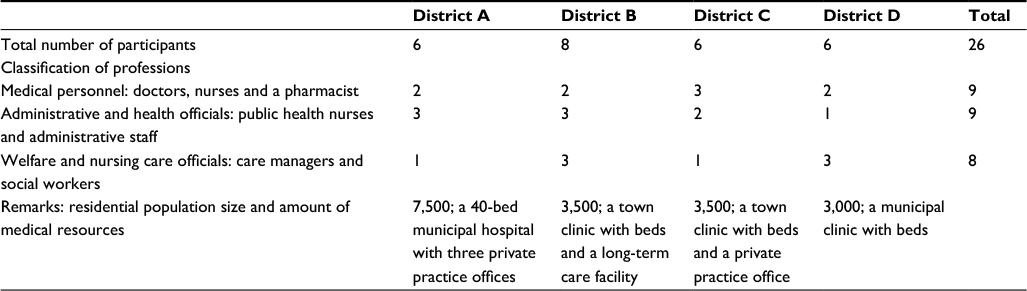
Methods: Semi-structured interviews were conducted with a total of 26 medical professionals, including physicians, nurses, public health nurses, medical social workers, and clerical personnel. Each participant worked as a team member of community-based integrated care. The central topic of the interviews was what the participants needed to establish collaboration during the care of elderly residents. Each interview lasted for about 60 minutes. All the interviews were recorded, transcribed verbatim, and subjected to content analysis.
Results: The analysis yielded the following three categories concerning the necessary elements of building collaboration: 1) two types of meeting configuration; 2) building good communication; and 3) effective leadership. The two meetings described in the first category – “community care meetings” and “individual care meetings” – were aimed at bringing together the disciplines and discussing individual cases, respectively. Building good communication referred to the activities that help professionals understand each other’s ideas and roles within community-based integrated care. Effective leadership referred to the presence of two distinctive human resources that could coordinate disciplines and move the team forward to achieve goals.
Conclusion: Taken together, our results indicate that these three factors are important for establishing collaborative medical teams according to health professionals. Regular meetings and good communication facilitated by effective leadership can promote collaborative practice and mutual understanding between various professions.
Keywords: interprofessional education, multidisciplinary collaboration, integrated primary and community care, qualitative research, interdisciplinary communication, geriatric health services, Japan
Introduction
Patient-centered communication has gained attention as a viable way to engage patients with their health care.1 Call light systems are the primary means of patients to initiate communication with their health care providers.2,3 Previous studies have shown that the use of call lights can positively contribute to patient outcomes by improving safety and satisfaction measures.4,5 Therefore, it is imperative to understand how call lights are used to communicate in order to bolster their effective utility and improve care delivery. Patak et al advocated that health care providers perform patient communication assessments (ie, literary, cultural, behavioral, and physical barriers) to ensure effective patient–provider communication. In addition to these communication assessments, understanding call light use from the patient perspective contributes to knowledge about patient and provider communication.6
Although there is a vast literature describing patient communication with their health care providers, few studies have discussed patients’ perceptions concerning call light use and communication.7 Deitrick et al utilized ethnographic qualitative methods and found that communication using the call light consisted of three interrelated components (namely answering the call light, communicating the patient’s request, and following through on the request), but used primarily observation analysis and did not directly incorporate patient perspectives.8 Montie et al explored the perceptions of Spanish-speaking patients with limited English language skills regarding call light use and found that participants had a number of concerns that contributed to health care disparities, some of which involved communication and call lights.9 In addition, nurses’ perceptions regarding call light communication have recently been investigated.4,10 The patients’ perceptions and perspectives regarding their call light use and their communication with their nurses and the effect of these two factors on their health care are missing in the literature.
The purpose of this qualitative study was to report patients’ perceptions of using their call light as part of a National Institutes of Health (NIH)-funded parent study on “Advancing Patient Call Light Systems to Achieve Better Outcomes” (R42MD006149).9–11 The specific aim of this component of the study was to solicit patients’ perceptions regarding the use of their call light and communication with nursing staff.
Methods
Design and sample
The research team used a qualitative descriptive approach to explore patients’ perceptions. The goals of qualitative descriptive studies include the comprehensive summarization of the experiences by the research participants (eg, patient participants and their perceptions). The study was conducted in an academic medical center located in Michigan. Study team members recruited patient participants from four adult medical–surgical units. Patients invited to the study met the following inclusion criteria: proficient in English, been hospitalized for at least 24 hours, aged ≥21 years, and able to communicate verbally (eg, not intubated).
Qualitative studies utilize theoretical sampling so that participants’ perspectives can validate emerging theories and/or phenomena. Thirty participants who provided written informed consent were enrolled in the study, and all thirty completed the interviews.
Instrumentation
A semi-structured interview guide (Table 1) included open-ended questions and probes. The interview guide helped to ensure the capture of participants’ perceptions regarding the use of their call light and communication with nurses.
 | Table 1 Participant interview guide |
Data collection procedures
Institutional review board approval was required and was provided by the University of Michigan prior to the start of any research-related activities. A trained graduate student research assistant (GSRA) received lists of potential participants from the units’ respective nurse managers. The GSRA met the potential participants in their hospital rooms to determine their interest in participation, obtain informed consent, and conduct the interview. The same GSRA conducted all the interviews. All the interviews were audio-recorded, took place in patients’ rooms without the presence of nurses or other health care providers, and did not last longer than an hour. Upon the completion of the interview, the participants received a $50.00 gift card as compensation for their time and effort.
Analysis
The same trained GSRA transcribed the interview audio-recordings verbatim. Team members checked the transcriptions for accuracy, and three members of the research team initially read the transcripts and coded the data independently. The review of three researchers helped to identify and correct individual biases.
Data analysis utilized the constant comparative methods of Glaser and Strauss.12,13 During discussion, team members compared codes, sorted, and rearranged the codes until common themes emerged based on the consensus of the research team investigators. Salient categories of meaning and relationships between themes were derived from the data itself through a process of inductive reasoning. During this process, minor and major themes emerged. The constant comparative method and qualitative content analysis described the phenomena.13 Taylor and Bogdan summarized that with the constant comparative method researchers simultaneously code and analyze data in order to develop concepts/themes, continually compare and refine these concepts, identify the concepts’ properties, explore their relationships to one another, and lastly integrate these concepts into a coherent explanatory model.14 This qualitative study achieved rigor by cross-checking transcripts with the audio-recordings.15
Results
Patient participants included thirteen women and seventeen men. The majority of participants self-identified as Caucasian (80%). Other participants self-identified as African American (17%) and American Indian/Alaskan Native (3%).
The participants discussed their overall perceptions of the call light and its usage. Some participants reported experiences that were favorable.
[…] I always got it to work. They were here as soon as I pushed it”; “Yes. It works. I have hit the button. [P21]
Other participants reported experiences that were unfavorable.
[…] the problem is the response time … It’s not quick enough in a lot of cases…; [P14]
[…] The nurse call system it seems like it could be better, if you’re in somewhat of an emergency that they’re not aware of, you know, it kinda seems like a long time before somebody shows up. [P4]
Whether favorable or unfavorable, participants’ perceptions described the call light device as a direct conduit to their care, as they associated response time with not only receiving care, but also the timeliness of the fulfillment of their requests.
Themes
Five major themes emerged during data analysis: establishing connectivity, participant safety concerns, no separation: health care and the call light device; issues with the current call light, and participants’ perceptions of “nurse work.” Multiple minor themes supported these major themes (Table 2).
 | Table 2 Table of results |
Establishing connectivity
Participants were very specific about the importance of using the call light for connectivity and to serve their needs.
“[…] For anything that I need to make me comfortable,” [P2] and “It’s just a lifeline”; [P12] and “… To me, that call light is the first point of order in everything starting to come back together.” [P5]
Participants described four primary reasons why they used the call light system: assistance, requests, medication, and connectivity to nursing staff. At the time of our study, the patients were using the Rauland Responder® 5 (pillow-speaker; Mount Prospect, IL, USA) call light device. This simplistic call light device allows the patient to request their caregivers (red button) and controls the television, lights, and audio (blue buttons).16
Assistance
Participants stated that they used the call light to request assistance:
Pretty much if I need something because it’s hard to get out of bed. I’m hooked up to these machines with suction, IV, the IV can run out or the morphine can run out … [P21]
For that alarm system [IV pump] and for getting up out of bed. My first couple days out were hard. I had to have a nurse come help me out. I would push the button and they would be here. [P9]
Requests
In addition to assistance, participants remarked that they used the call light system as the primary means of making requests. Requests varied from general to very specific:
Mostly for water and maybe help in the bathroom. [P29]
[…] You need help or because you just can’t get up and take off. They’ll bring it right to you. It comes in handy. [P29]
Medication
Lastly, participants stated that they also used the call light specifically to obtain medication:
I ask for pain medicine. [P24]
Earlier I had some heartburn, so I had to call for medicine. [P24]
Connectivity to nurse staff
More importantly, participants reiterated that the call light is an inseparable link to their specific nursing staff:
I think the biggest thing is that somebody responds to you personally to see what your issue is. You just push the button and someone will come, either tech or nurse. [P7]
Oh, yes! It’s detrimental to your health. If you are in pain, to have somebody there right away or if something major is going on. It’s comforting to know I can push a button and in a couple of minutes somebody will be here. [P30]
Yes. Oh, yes. It gets me what I need. Not what I want, it gets me what I need. [P26]
Participants used the call light to establish “connectivity” with nursing staff. They described using the call light as a catalyst for getting their needs met, namely communicating their need for assistance, making requests, and getting medication. This “connectivity” alluded to the direct dependence patient participants had on the call light for their health care needs.
Participant safety concerns
Participants described safety concerns about call light use. Real-life experiences and “hypothetical” safety concerns comprised these experiences:
Participant safety experiences
Participants stated real-life safety experiences:
If I sit here and I can’t get them [by using the call light], first off I get cold, I get sick […] I couldn’t get the help I needed … [P5]
[…] This call light does not let them know what I want and who I need … I’ve been in respiratory distress. They had me on the phone and the nurse was like, “Can’t you breathe?” I was like saying, no. The next thing I know I was being life-flighted … If they waited any longer, I very well could have been dead. [P25]
Like when I was having that anxiety attack. There were just extenuating things that brought the call down. I had to wait 1½ hours … [P30]
[…] I tried to get out of bed to go to move to answer the phone, not realizing all the tubes and wires I had. I ended up falling and hitting my head. I laid there, a good hour … [P4]
Safety concerns as discussed by participants involved real-life situations directly related to the call light.
Participants’ “hypothetical” safety concerns
Participants described “hypothetical” safety concerns about their call light use. They described detailed vignettes of situations that posed great concern:
[…] Since I have a chest tube and all this stuff, they like to help me in case I rip something out. They prefer to help me, but I’m not going to stand in the bathroom for 10 minutes when I can help myself … Waiting 10 minutes [for call light response] would be pretty upsetting; or, if I did fall … [P20]
It is [a lifeline]. Like if I can’t breathe, 40 minutes would be too long and I can’t reach the cord … [P12]
[…] I understand the nurses have quite a few patients at one time and they’re trying to give everybody equal care … [call light does not tell them] if you’re having a heart attack or something is happening, or can’t breathe … [P28]
Although these concerns were hypothetical, participants nevertheless expressed anxiety regarding their safety and the potential of compromised care with the current call light system.
In summation, participants described safety concerns from not only their lived experiences, but also their perceptions regarding hypothetical safety situations that caused anxiety to participants. In addition, participants also described the call light and their health care as a singular entity, rather than separate modes for getting their health care needs met.
No separation: health care and the call light device
Participants viewed the call light and their care as synonymous. Rather than viewing the call light separately as a device for their care and assistance, they described a direct link between the call light device and their care that was inseparable, describing a system of care that included security, versatility, and linkage to the nursing staff.
Security
Participants stressed the fact that the call light brought them feelings of security concerning their care:
It [call light] gets me the people that can get me better, that nurse. She’s [nurse] a powerful lady. [P26]
I think it [call light] just gives you the security to know that someone is going to take care of you, that they’re going to help you out. [P6]
Versatility
Participants also remarked that the call light was versatile when it comes to their care. For example, participants remarked about the call light as follows:
It [call light] controls everything. It controls your nurse getting to you, it controls the light, and it controls the TV. [P26]
It [call light] works out real good. To get the nurse, all you have to do is push that. If you want the lights on, you do that. [P14]
The TV worked great and I didn’t have any issues. You have a wide variety of channels to meet most people. If you need testing done, they use the call light for the food if you need testing done. [P17]
Participants clearly relied solely on the call light for care and viewed the call light and their care synonymously.
Issues with the current call light
Participants remarked that there were some problematic issues with the current call light system. Lack of privacy, communication barriers, and the location of the current call light were key sources of stressors when it came to their health care. Participants suggested that the two-way communication functionality would mitigate these concerns.
Lack of privacy
Participants stated that they felt that the current call light posed a privacy concern:
[…] Some things you don’t want people to know, especially in the hospital. You don’t want people to know your chronic illness or whatever it may be. [P26]
It may be disruptive to your neighbor. Because you’re having a conversation over the intercom. [P24]
It depends on my situation. If I don’t like talking around other people … [P26]
Communication barriers
Participants stated that they felt that there were some barriers to communication with the current call light system. For example, they thought that it was important to separate the nurse requests from nurse technician requests and highly advocated for this logistical change:
I think having a tech button would be a good idea. For people who just needed juice or help going to the bathroom. You know, things that the tech can help with. Maybe they need their own button themselves … [P25]
Maybe if you had two buttons that would solve that problem, whether it’s a real emergency or if you just need a glass of water. The difference between something simple and something that’s real. [P28]
Location of current call light device
Participants also stated that the location of the current call light was problematic for a variety of reasons:
[…] If you don’t have the TV on, you can’t hear it and you don’t really know where it’s at. I guess that’s why I think the call button should be someplace, not where you could rest your hand and accidentally set it off … [P8]
Try to get it where you want it before you lie down. You have to turn your body towards it so you can reach it. Wrap it around the rail so it doesn’t fall. [P24]
Participants described the location of the call light device and its storage as key issues that contributed to their stress as it is related to the call light system. In addition, participants stated specifically that they wanted two-way communication with their nurses.
Wanted: two-way communication
Participants stated that they would prefer two-way communication with their nurses (ie, nurses could respond through the call light device when they initially used the call light) in order to 1) specify needs; 2) establish acknowledgment; 3) improve efficiency in fulfillment of participant requests and nursing care; and 4) potential impact of two-way communication.
Specify needs
Participants expressed the importance of two-way communication with their nurses as it enables them to specify their needs:
It [would be] a lot better than a button, I mean, because you’re defining your wants and needs and everything by a system like this … [P4]
It would actually be nice if you push it [call light], if they could say, “What do you need?” Then, for example, I could say, “My IV’s loose.” Then they would know … [P11]
I think you could give specific directions when the nurse is out of the room so she knows what to do when she comes in here. Hitting a general button, the nurse has to come in here to see what you need, then leave, then come back. It’s gotta be more efficient for the nurses. They wouldn’t have to make three trips in here to take care of one problem. [P6]
Establish acknowledgment
In addition, participants stated that they thought that two-way communication would not only provide acknowledgment for their needs, but also be reflective of a prioritizing system of answering call light requests:
You’re getting confirmation. They already know what you want or what you need, not just, the light went off … [P21]
[…] It would be nice to not make somebody wait 20 minutes, 10 minutes, and 5 minutes. If you can’t get to me, you could let me know. It’s an open line of communication between patient and nurse. Because sometimes they [nurses] get overwhelmed and sometimes they get busy in a hospital … [P12]
Like I said, they [nurses] would know who to go to first. And not just I have to get somebody up in bed, they could tell them, “I’ll be with you in a minute.” I have another patient with urgent needs that I have to see first. [P11]
Improve efficiency with patient requests
Likewise, participants felt that a two-way communication call light system would improve efficiency.
They say, “Can I help you?” and you can just talk through it to them so they don’t have to physically walk down the hall … If you just wanted water, they would have to come down here to see what you wanted, go to the other end of the hallway to get the water, and then bring it back down here. If you could’ve told ‘em, they could have just brought the water with them. [P24]
I would think, for efficiency’s sake, you should be able to tell the nurse what you want. The poor [nurses] have to run around to find out what you want. It would be more effective if you could tell them what you need. [P13]
It would be better for the nurses too. If they had a serious patient and I just needed a juice, they wouldn’t have to come running in here. They can finish with the serious patient and then maybe come in here and check on me to make sure I’m okay. [P20]
Participants discussed suggestions for two-way communication with their health care nurses as not only beneficial for their care (ie, describing what they specifically need), but also a way to improve their health care (ie, prioritizing the call light system by the importance or relevance of requests).
Participants’ perceptions of “nurse work”
Participants described their perceptions of “nurse work.” “Nurse Work” as defined by participants included perceptions and evaluation of how they viewed nursing duties and how these perceptions affected their call light request fulfillment.
Perceptions of nurse “time”
Participants described their feelings regarding the time that nurses allocated to answering their call lights, and they understood that nursing duties included caring for other patients:
[…] Because you never know which nurse is tied to what room. I don’t want to add anything … They got enough to do, having to add that much to each shift when they set up, that would be a pain. [P8]
If they [nurses] didn’t come promptly, at first I got a little agitated. Then I said, well, they may be busy. Be patient. I’m not the only one in here … [P2]
When you only have one nurse and she has five rooms and they’re kinda randomly spread out. I turn my light on and she may be in somebody’s room and not even know my light is on. So, she may be taking somebody to the restroom and that may take 5 or 10 minutes … [P20]
Understanding nurses’ challenges with prioritizing patient call light requests
Participants also expressed understanding that nurses must prioritize their patients’ needs:
Well, I figure that people out there are sicker than I am. Pillow fluffing is nothing compared to somebody who’s having a hard time breathing … [P30]
[…] They sometimes rush in here from another room, thinking it’s really important and all you needed was a cup of ice. The assistant ran in here all out of breath and saying, “I’m sorry you had to wait.” I felt bad because all I needed was sugar and she was changing somebody. I don’t want her to rush and possibly end up hurting somebody because I need sugar … [P18]
Depending on who gets the call. Like the techs would get the comfort related items. Then the nurse would get more of the medication calls and assistance calls. You don’t feel bad pushing a button that’s already there for you to push. [P7]
Participants understood the importance of nurses’ prioritization of call light responses and addressing patient needs accordingly, and they clearly understood “nurse work” and respected the work that nurses do.
Discussion
The findings of this study revealed that participants perceived the call light as more than merely a device to initiate communication, but also as a direct conduit to their health care and its delivery. As direct conduits to care, call lights are a reflection of cooperation, communication, and safety as evidenced by participants’ perceptions. Understanding how patients use call lights bolsters the effective utility of call lights, lends information to improve care delivery, and contributes to knowledge regarding patient and provider communication.
There are few studies investigating patients’ perceptions regarding their call light use and its communication. Previous research4,10 focused on nurse perceptions of call light communication, but no study has solicited patients’ perceptions regarding call light communication with nurses or the use of call light technology. Findings from this study suggest that the patient participants not only relied on the call light for their health care needs, but also described the call light device as a direct conduit to their care. Despite reporting that nurse response time to call light initiation was prompt, participants believed that the call light response time impacted when they would receive their care. Delayed or missed call light responses led to safety incidents and safety concerns. In regard to safety, some participants’ concerns were hypothetical, which nonetheless caused participants’ angst and stress. These findings differ from previously published research due primarily to the inclusion of participants’ perceptions. Patients’ perceptions provide salient communication clues between their health care providers and the call light device.
Participants discussed various experiences with the current call light device in use, both favorable and unfavorable. They thought that favorable experiences with the call light device were directly related to the nursing staff and their subsequent care. Further reinforcement of this idea was supported by the minor theme “nurses are prompt.” Participants’ unfavorable experiences with the call light were directly related to the device itself. Participants stated that the device was technologically “outdated,” lacked user-friendliness, and influenced the response time. In addition, participants understood nurse work and that nurses must prioritize both call light requests and patients’ needs. In summary, participants found the call light favorable when thinking about their nursing care and unfavorable when thinking about it as a communication device. Therefore, to improve communication access, initiation, and utility of call light technology, additional work on this topic should continue so that patients are involved in the design of these important devices.
Because in this study participants did not perceive the device as separate from their care or nurses, the results also suggest that the call light is more than merely a means of communication. Call light use also influences the quality of care they receive according to the respondents. Participants expressed interest and investment with their health care not only by continually suggesting improvements for the call light, but also by providing suggestions for nurses with regard to how to better deliver health care, eg, by advocating for two-way communication systems or for separate “nurse” and “tech” buttons. It is imperative that we improve the call light device to improve communication and to improve patients’ perception of care. Updates to the call light device may also improve patient satisfaction, mitigate patient safety concerns, and improve nursing workflow.
Limitations
The study has some limitations. It consisted of a single site, including only those participant perspectives from the single site. In addition, the study involved only perceptions in regard to one particular call light device. Although qualitative research does not seek generalizability as a viable research outcome, we do acknowledge the potential value of replicating this study at other study sites.
Perhaps the strongest implication for clinical practice from this study is the safety concerns with the call light device itself and nurses’ response time. Participants described incidents where delay in answering or failure to answer the call light resulted in compromised care. Another implication involves the current state of health care technology, which requires updated technology to reflect not only patients’ needs, but also the needs of nurses.
Research implications
The study informs many potential avenues for additional research. Future efforts to include the development and testing of more advanced call light technology should take into account and address patients’ perspectives about their health care and its delivery. Participants in this study did not differentiate the delivery of their health care from the call light device request. This lack of differentiation warrants further exploration in future research. The results from this study indicate that further research is needed about how to improve call light capabilities to increase patient communication and how nurses could benefit from an improved call light system for patient-centered care delivery.
Acknowledgments
This research was supported by Small Business Technology Transfer Program of the NIH under award number R42MD006149. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Disclosure
The authors report no conflicts of interest in this work.
References
Paget L, Han P, Nedza S, et al. Patient-Clinician Communication: Basic Principles And Expectations. Washington, DC: IOM Working Group Report, Institute of Medicine; 2011. | ||
Vandenkerkhof EG, Hall S, Wilson R, Gay A, Duhn L. Evaluation of an innovative communication technology in an acute care setting. Comput Inform Nurs. 2009;27(4):254–262. | ||
Kuruzovich J, Angst CM, Faraj S, Agarwal R. Wireless communication role patient response time: a study of vocera integration with a nurse call system. Comput Inform Nurs. 2008;26(3):159–166. | ||
Tzeng HM. Perspectives of staff nurses toward patient- and family-initiated call light usage and response time to call lights. Appl Nurs Res. 2011;24(1):59–63. | ||
Tzeng HM, Yin CY. Are call light use and response time correlated with inpatient falls and inpatient dissatisfaction? J Nurs Care Qual. 2009;24(3):232–242. | ||
Patak L, Wilson-Stronks A, Costello J, et al. Improving patient-provider communication: a call to action. J Nurs Adm. 2009;39(9):372–376. | ||
Shuman C, Liu J, Montie M, et al. Patient perceptions and experiences with falls during hospitalization and after discharge. Appl Nurs Res. 2016;31:79–85. | ||
Deitrick L, Bokovoy J, Stern G, Panik A. Dance of the call bells: using ethnography to evaluate patient satisfaction with quality of care. J Nurs Care Qual. 2006;21(4):316–324. | ||
Montie M, Galinato JG, Patak L, Titler M. Spanish speaking limited English proficiency patients and call light use. Hisp Health Care Int. 2016;14(2), 65–72. | ||
Galinato J, Montie M, Shuman C, Patak L, Titler M. Perspectives of nurses on patients with limited English proficiency and their call light use. Glob Qual Nurs Res. 2016;3:1–9. | ||
Galinato J, Montie, M, Patak L, Titler M. Perspectives of nurses and patients on call light technology. Comput Inform Nurs. 2015;33(8):359–367. | ||
Strauss A, Corbin J. Basics of Qualitative Research. Newbury Park, CA: Sage; 1990. | ||
Glaser BG, Strauss, A. The Discovery of Grounded Theory. Chicago, IL: Aldine; 1967. | ||
Taylor SJ, Bogdan R. Introduction to Qualitative Research Methods: The Search for Meaning. New York, NY: Wiley; 1984. | ||
Lincoln YS, Guba EG. Naturalistic Inquiry. Los Angeles, CA: Sage; 1985. | ||
Rauland Responder ®5. Critical clinical communications. AMETEK, Inc.; 2017. Available from: https://www.rauland.com/healthcare/responder-5. Accessed June 12, 2016. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.