Back to Journals » Nursing: Research and Reviews » Volume 16
Establishing an ED Dedicated Trauma Nurse Program to Improve Trauma Care: Insights from Our Trauma Center
Authors Aftab N, Maxson MR, Halalmeh DR, Harden E, Bains KK, Hussein MA, Cranford JA, Wong KR, Beer PR, Howell AC, Huber GA ![]() , Rieck LD, McCann ML, Sachwani-Daswani GR
, Rieck LD, McCann ML, Sachwani-Daswani GR
Received 25 December 2025
Accepted for publication 16 April 2026
Published 24 May 2026 Volume 2026:16 580023
DOI https://doi.org/10.2147/NRR.S580023
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ferry Efendi
Neha Aftab,1,2 Michelle R Maxson,1 Dia R Halalmeh,1,2 E’Lise Harden,1,2 Keerat K Bains,1,2 Mohamed A Hussein,3 James A Cranford,1,4 Kristoffer Ryan Wong,1,2 Patrick R Beer,1,2 Adam C Howell,1,2 Gavin A Huber,1,2 Lindsey D Rieck,1,2 Michael L McCann,1,2 Gul R Sachwani-Daswani1,2
1Department of Trauma and Acute Care Surgery, Hurley Medical Center, Flint, MI, USA; 2Department of Surgery, Michigan State University, Flint, MI, USA; 3Departmenr of Emergency Medicine, Western Michigan University, Homer Stryker MD School of Medicine, Kalamazoo, MI, USA; 4Department of Emergency Medicine, University of Michigan, Ann Arbor, MI, USA
Correspondence: Neha Aftab, Department of Trauma and Acute Care Surgery, Hurley Medical Center, 1 Hurley Plaza, Flint, MI, USA, Tel +1 (517)512-3389, Email [email protected]; [email protected]
Background: Delays in patient flow within the trauma system can be attributed to a lack of familiarity, disorganization, and failure to prioritize complex injuries. Due to these concerns and occasional inefficiencies during patient resuscitation, we evaluated the efficacy of a dedicated trauma nurse (DTN) model in improving efficiency.
Objective: To investigate DTN in improving the following efficiency measures: time to vitals, time to CT scan, time to intervention and ED dwell time.
Methods: Eligibility for DTN required nurses to have at least three-years of experience in the ED and to hold current Trauma Nursing Core Course (TNCC) or Advanced Trauma Care for Nurses (ATCN) certification. Candidates were required to pass a written examination and participate in mock scenarios. Completion of a mandatory eight-hour trauma course, including hands-on training, was required. Four efficiency measures were evaluated over a ten-year period (2012– 2022) using electronic health records from trauma patients presenting to the ED who required class-I or II trauma activations.
Results: The study included 5,438 trauma patients. They were divided into a pre-implementation group (Group-I) and a post-implementation group (Group-II), which was further split into pre-COVID (Group-IIa) and post-COVID (Group-IIb) subgroups. The time to vital signs dropped from an average of 4.2 minutes in Group-I to 3.6 minutes in Group-IIa and 3.9 minutes in Group-IIb (p< 0.001). The average time to CT scan was 35.9 minutes in Group-I, 25.4 minutes in Group-IIa, and 29 minutes in Group-IIb (p< 0.001). The time to intervention averaged 2.3 minutes in Group-I, 1.7 minutes in Group-IIa, and 3.1 minutes in Group-IIb (p< 0.001). ED dwell time decreased from 4.3 hours in Group-I to 3.7 hours in Group-IIa, but then increased to 5.8 hours in Group-IIb (p< 0.001).
Conclusion: DTN team can enhance efficiency during trauma resuscitation by reducing ED time and time to definitive care. On some measures, the impact of COVID-19 was substantial and led to a decrease in our efficiency measures.
Keywords: dedicated trauma nurse program, emergency department, trauma nursing
Introduction
Nurses play a crucial role in trauma resuscitation. Trauma nursing is a rapidly advancing and complex field. Trauma nurses must possess a strong knowledge base focusing on the mechanism of injury, critical thinking skills, and rapid assessment abilities. While specialized nursing care is key to caring for trauma patients, conventional workforce structures do not accommodate the individual strengths of nurses, resulting in ED nurses having sporadic exposure to trauma activations. The inexperience concerning trauma resuscitation and care can lead to ineffective teamwork and communication failures.1 Trauma teamwork training has been shown to improve team performance, patient outcomes, and overall quality of care.
Delays in patient flow in trauma setup can be due to a lack of familiarity with the trauma setting, disorganization, and failure to prioritize the complexity of injuries. Research on the impact of focused trauma education on patient outcomes suggested that overall mortality decreased after implementation, however, it was not statistically significant.2 Martin RN observed that their institute’s dedicated trauma nurse (DTN) program was associated with a decreased length of ED stay with a subsequent decrease in time to diagnosis and treatment due to standardization and continuity of trauma care.3 The implementation of the DTN program increased efficiency during trauma resuscitation and directly improved patient care by establishing clear, predefined goals for emergency department nurses. Additionally, the program enhanced time management by facilitating anticipation of necessary equipment, reducing treatment delays, and ensuring effective transfer of care from the emergency department to the operating room, interventional radiology, surgical intensive care unit, or inpatient floor.
The coronavirus (COVID-19) pandemic caused an unparalleled strain on healthcare due to a lack of resources and severe patient morbidity. Healthcare workers, particularly nurses, were vulnerable due to direct contact when caring for patients. Multiple studies have also emphasized that nurses experienced increased workload and psychological stress secondary to the nature of the pandemic.4,5
This retrospective pre-post implementation study aims to investigate the impact of implementing a dedicated trauma nurse program on trauma resuscitation and other ED efficiency measures at a level 1 trauma center. We also assessed the impact of the COVID-19 pandemic on our DTN program.
Methods
This study was conducted at Hurley Medical Center (HMC), a level-I American College of Surgeons (ACS) verified adult trauma center and an ACS verified level-II pediatric trauma center. HMC is a community-based, university-affiliated hospital with 443 beds. The trauma registry was reviewed to compare efficiency measures, including time to vitals, time to CT scan, time to intervention (defined as the interval from emergency department presentation to the operating room or interventional radiology procedure), and ED dwell time before and after implementation of the DTN program. Inclusion criteria comprised level 1 and level 2 adult and pediatric trauma activations (see Table 1 for criteria of level I and II activations at our institute). Both level-1 and level-2 activations were included in the analysis to evaluate the efficiency of the DTN program. The DTN group included 30 nurses, each with at least 3 years of emergency department experience, who completed a trauma training course. We developed our DTN program in-house, drawing on prior literature and input from ED staff and management. We identified training gaps through surveys and one-on-one feedback. Patient demographics from 2012 to 2022 were also analyzed to characterize the study population, including Injury Severity Score (ISS), discharge disposition, and mortality (Table 2).
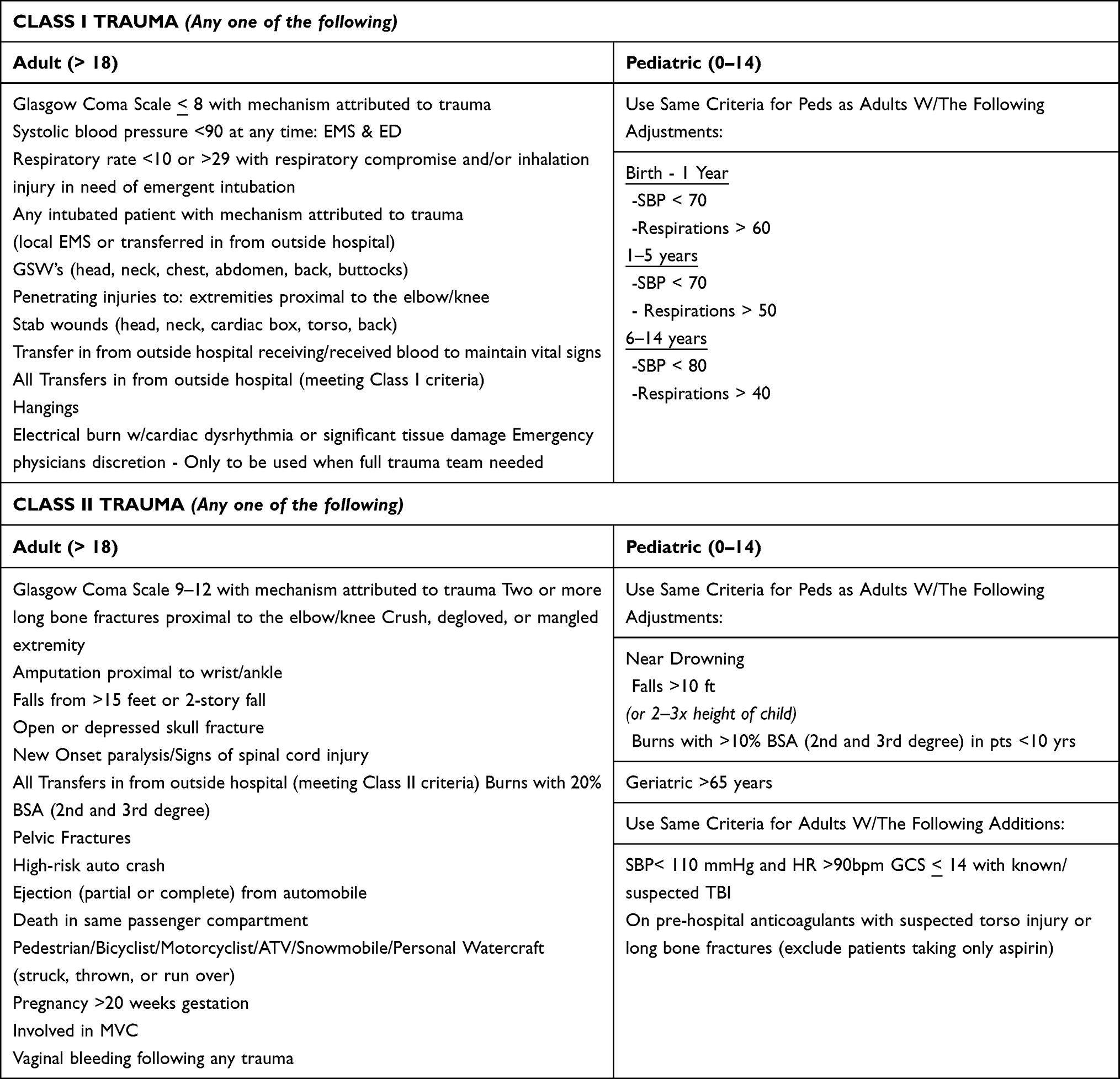 |
Table 1 Criteria for Adult and Pediatric Trauma Activations at Our Institute |
 |
Table 2 Patient Demographics and Clinical Data (N=5,438) |
Recruitment
Prior to having a dedicated trauma nurse team, 130 nurses were working in the ED who randomly rotated through the trauma bay. At times, nurses would have an extended period in which they were not assigned to the trauma bay, over 6 months in some instances. Maintaining consistency was a considerable challenge due to scheduling practices.
Implementation of Program
Inclusion Criteria for Nurses
Trauma services established minimum entrance requirements for applying to the dedicated ED trauma nurse group in collaboration with ED leadership. Nurses who were entered in the program were required to have a minimum of 3 years of experience in ED, successful completion of Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS), current certification in either Trauma Core Course for Nurses (TNCC) or Advanced Trauma Care for Nurses (ATCN), successful completion of the trauma class, and appropriate competency displayed during a mock trauma scenario. Being a member of the ED trauma nurse group was voluntary.
Implementation of the Program
All nurses interested in applying for the DTN group took the ED Basic Knowledge Assessment Tool (BKAT) exam. Candidates were required to pass BKAT and participate in mock scenarios. Completion of a mandatory eight-hour trauma course, including hands-on training, was required. The BKAT exam is an 85-item test that measures basic knowledge in critical care nursing in emergency departments. Those scoring 80% or higher could participate in a mock trauma scenario. The mock trauma scenarios were conducted by the trauma medical director and the trauma program manager with each nurse individually, each lasting approximately 30 minutes. The scenarios were used not only for evaluation purposes but also for education. Time was spent at the end of each scenario reviewing concepts the nurse had not appropriately identified.
After completing the testing process, 30 nurses were chosen to form the ED trauma nurse. A lecture was provided by the trauma medical director each month for continued education, including trauma topics and case reviews. These lectures initially consisted of topics identified as common weaknesses from the mock trauma scenarios. The nurses were required to attend 70% of the monthly trauma lectures to remain in the dedicated group. Failure to meet these requirements resulted in removal from the group. Individual evaluations were periodically performed with each nurse by the trauma medical director and the trauma program manager to identify strengths and opportunities for improvement.
To sustain this change, we continued to monitor the efficiency measures on a monthly basis to ensure forward progression. We continue to provide monthly education offerings for our ED Trauma Nurses to expand their knowledge base. The Trauma Medical Director, Trauma Program Manager, and the ED Nurse Educator provide individual performance evaluations to each dedicated trauma nurse every 6 months to identify strengths, weaknesses, and opportunities for improvement. Moving forward, any nurse joining the group needed to undergo the same testing and mock trauma scenario process.
Measure of Efficiency and Statistical Analyses and Group Implementation
Data were categorized into pre-implementation (group I) data from the year 2012 and post-implementation (group II); group II was further divided into group IIa implementation and pre-COVID data (2013–02/2020), and group IIb included the data from post-implementation post-coved (2020–03/2022). We used one-way analyses of variance (ANOVAs) to test for between-group differences in 4 continuous outcomes: 1) time to vital signs, 2) time to computed tomography (CT) scan, 3) time to the intervention, and 4) total ED dwell time, with Tukey HSD post-hoc tests where appropriate. An alpha level of.05 was used for all analyses. Analyses were conducted with the SPSS statistical software package (version 29.0, IBM, 2022).
Overall Monitoring of the Program
The DTN program has been ongoing since 2013. Variables are documented monthly using a continuous trauma registry. The trauma department conducts monthly meetings to review these variables and investigate any deviations or system delays. Additionally, the department organizes monthly lectures and collects feedback from nursing staff.
Results
The sample consisted of 5,438 trauma patients. Table 1 outlines the criteria for level 1 and level 2 trauma for both adult and pediatric populations at our institute. Table 2 describes the demographic characteristics of the study sample before and after implementation of our DTN program. The mean age of patients remained similar (pre: 35.4 ± 18.4, post: 35.8 ± 18.8; p=0.57). There were no statistically significant differences in gender distribution from pre- to post-implementation (male 75.2% vs 75.1% and female 24.8% vs 24.9%; p=0.96). Racial distribution differed statistically significantly in the pre- and post-implementation groups (p=0.04), with an increase in Caucasian patients (49.9% vs 63.1%), a slight decrease in Black patients (42.6% vs 39.6%), and an increase in Hispanic patients (0.8% vs 1.7%). The type of insurance also showed statistically significant differences in the pre and post-implementation phase, with increases in Medicaid patients (4.9% vs 40.9%), and in privately insured patients (11.9% vs 23.8%), and decreases in self-pay patients (1.3% vs 0%) and other/unknown (82% vs 35.2%). Mechanism of injury and level of activation were also statistically significantly different in the pre-implementation and post-implementation phase (p=0.02 and p<0.001). There was an increase in blunt trauma (60.2% vs 65.4%), a decrease in penetrating injury (35.5% vs 30.8%) and a slight increase in burn patients (4.3% vs 3.8%). Class I trauma activations increased in the post-implementation phase (42.2% vs 52.7%) and class II trauma showed a decrease in post-implementation phase (57.8% vs 47.3%). Injury severity score (ISS) showed a statistically significant change from pre- to post-implementation (p<0.01); ISS less than 15 (72.3 vs 67.1%), ISS 15–24 (18.1% vs 17.4%) and ISS greater than 25 (9.5% vs 15.5%). The patients who underwent intervention were further divided into emergent and non-emergent interventions; each intervention was further divided into interventional radiology intervention (IR) and operating room (OR). Emergent IR increased (0.8% vs 1.1%) and emergent OR increased as well (18.4% vs 30.9%). Nonemergent IR remained the same (3.6%) in both pre-implementation or post-implementation phase and nonemergent OR decreased in post-implementation (77.2% vs 64.3%). Discharge disposition to home or home with care decreased in post-implementation phase (73.5% vs 66.2%) and this difference was statistically significant (p<0.001). Discharge disposition to rehabilitation increased, and this increase was statistically significant (8.6% vs 11.9%, p<0.007). Mortality remained the same pre-implementation and post-implementation (11.3% vs 11.7%, p=0.75).
Four measures of efficiency were analyzed in the pre-implementation and post-implementation phase, including time to vital signs, time to CT scan, time to intervention and ED dwell time (Table 3). Data was categorized further in the following three groups: Group I, Pre-Implementation (n=799, 14.7%); Group IIa, Post-Implementation Pre-Covid (n=3215, 59.1%); and Group IIb, Post-Implementation Post-COVID (n=1,424 26.2%). These groups are analyzed together in Table 4. We further expanded our analyses in Table 4 (group I vs group IIa+IIIb) to determine the impact of our program post-implementation by combining group II and III. Table 5 represents subgroup analysis of the post-implementation phase comparing the efficiency measures in pre-covid phase vs the post-covid phase and explains the immediate effect of COVID 19 on our program.
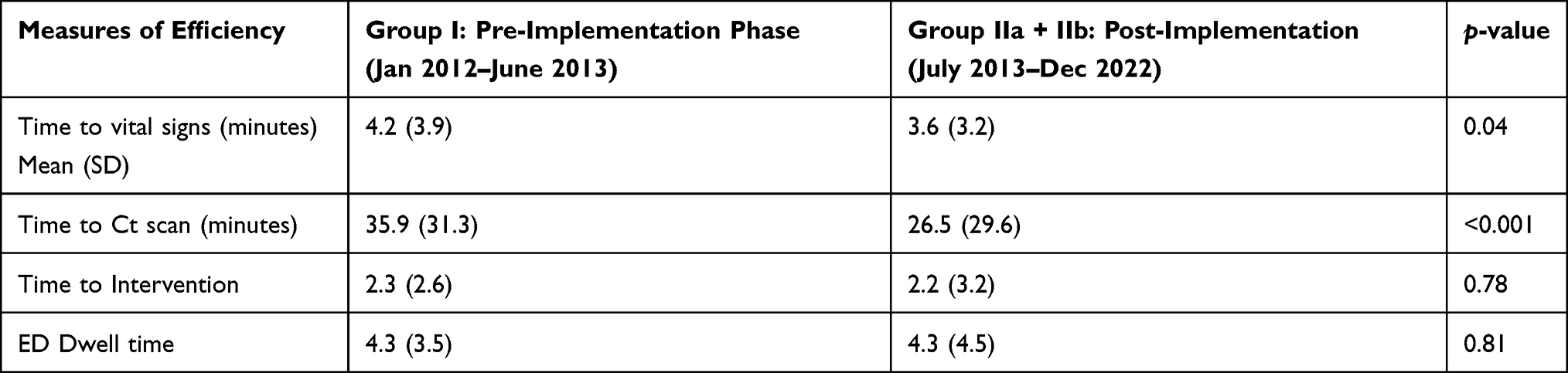 |
Table 3 Comparison of Efficiency Measures for Pre-Implementation vs. Post-Implementation Phases |
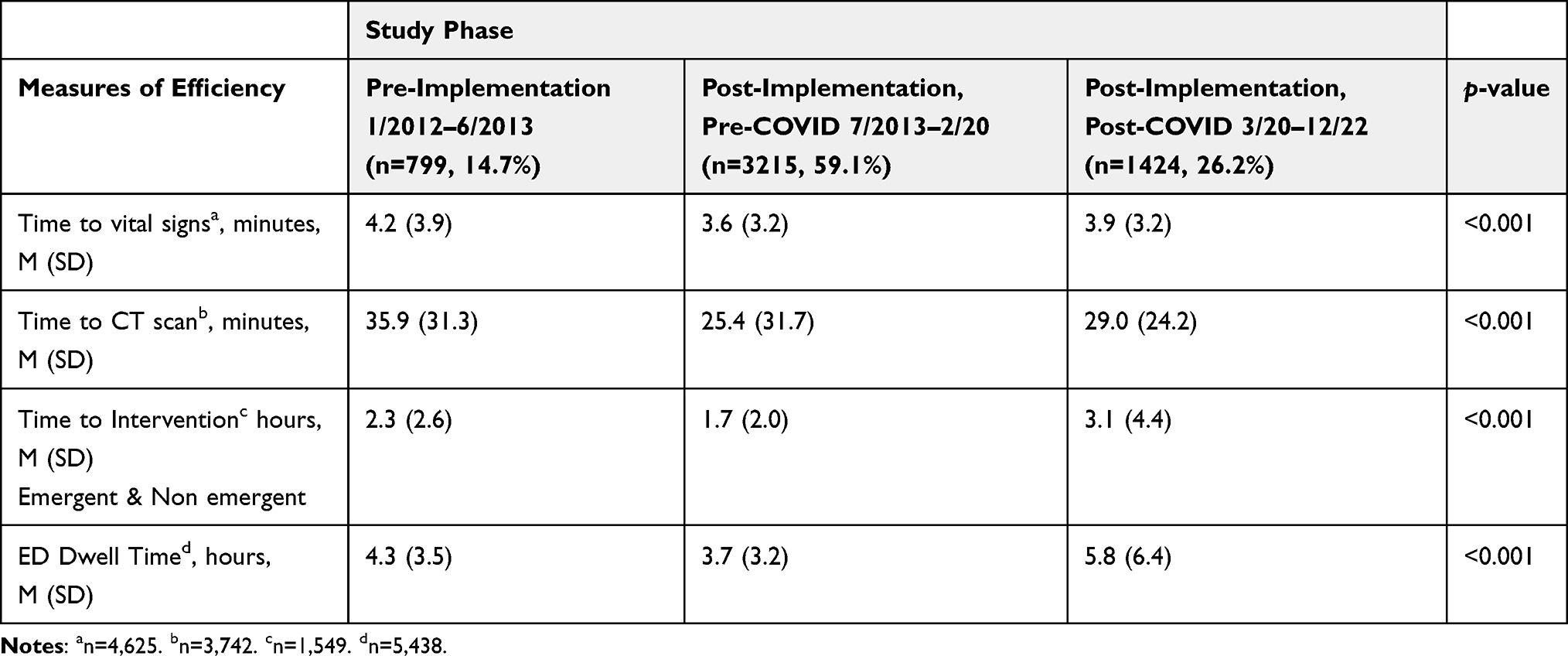 |
Table 4 ED Efficiency During Pre-Implementation, Post-Implementation Pre-COVID, and Post-Implementation Post-COVID Phases (N=5,438) |
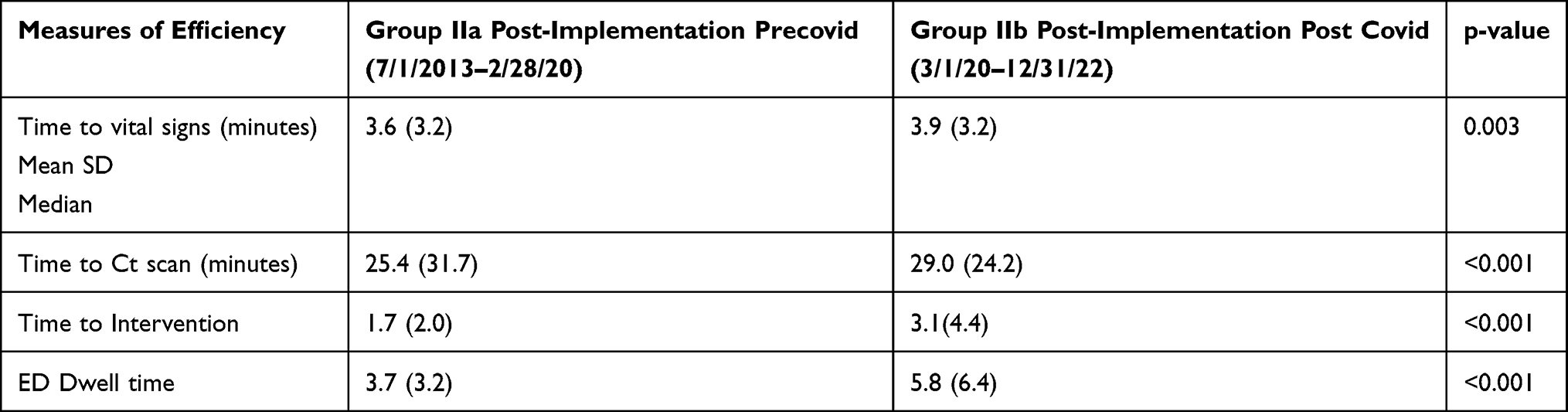 |
Table 5 Subgroup Analysis of Post-Implementation Phase of Measures of Efficiency: Pre-COVID vs. Post-COVID |
Time to Vital Signs
As shown in Table 3, overall comparison between the pre-implementation and post-implementation phases showed a reduction in time to vitals (M=4.2 vs M=3.6, p<0.04). In the sub-group analysis there was a difference between pre covid post covid (vs SD) representing an increase in time to vital signs. Figure 1 graphically represents initial decrease and subsequent increase in time to vital signs. Before the implementation of our DTN program our mean time to vitals was 4.2 minutes, decreased in our post-implementation group II to 3.6 minutes, and increased in our post-implementation post COVID group III to 3.9 minutes. The difference between the groups was statistically significant (p<0.001). However, when comparing the difference between group I (pre-implementation) and group II+III (post-implementation pre-covid + post-implementation post-COVID) time to vital signs was decreased overall to 3.6 (p<0.04).
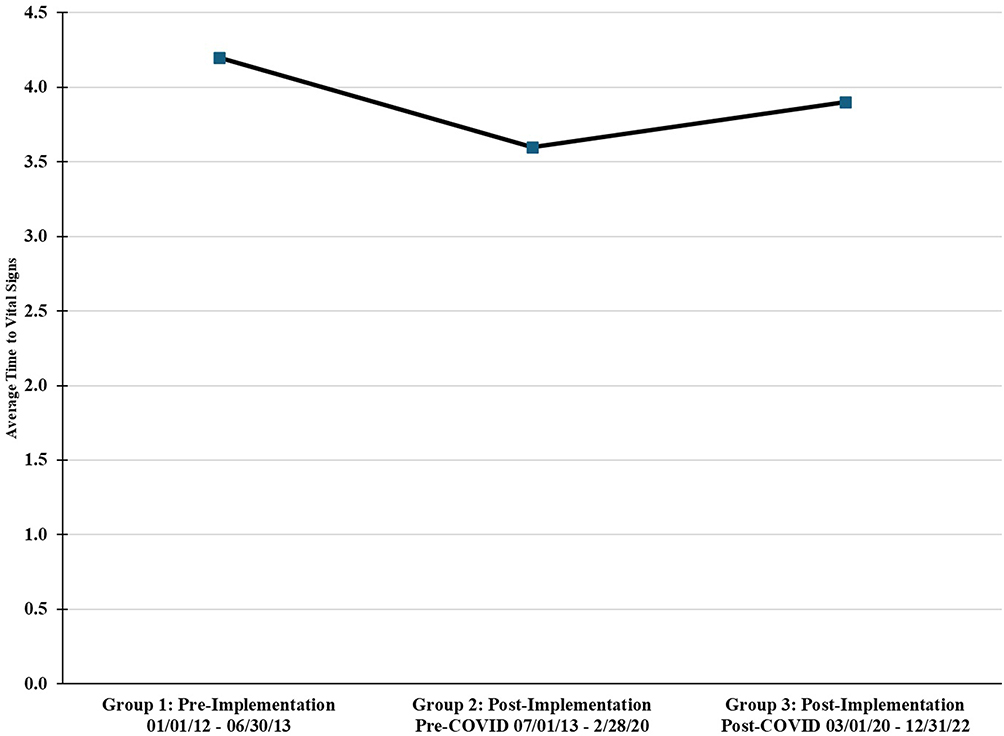 |
Figure 1 Time to Vital Signs During Pre-Implementation, Post-Implementation Pre-COVID, and Post-Implementation Post-COVID Phases. |
Time to Computed Tomography (CT) Scan
Time to CT scan (Figure 2) in group I was 35.9 minutes, which decreased after implementation in our post-implementation pre-COVID group II to 25.4 minutes, and then increased in our post-implementation post COVID group III to 29 minutes. The difference between the groups was statistically significant (p<0.001). When comparing the difference between group I (pre-implementation) and group II+III (post-implementation pre-covid + post-implementation post-COVID), time to CT scan decreased to 26.5 minutes (p<0.01). There was also a statistically significant increase in time to CT scan in group III post-implementation post-covid to 29 minutes vs 25.4 minutes in group II (p<0.001). Figure 2 graphically represents the initial decrease and subsequent increase in time to CT scan.
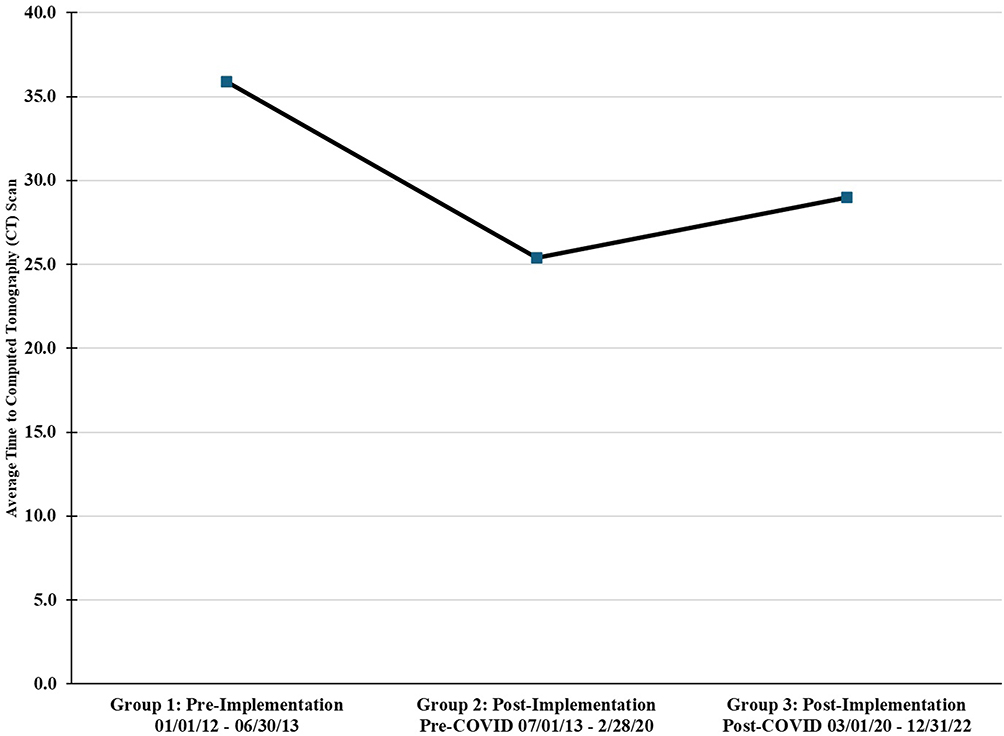 |
Figure 2 Time to CT Scan During Pre-Implementation, Post-Implementation Pre-COVID, and Post-Implementation Post-COVID Phase. |
Time to Intervention
Time to the intervention was measured in hours. Figure 3 shows that time to intervention decreased in group II and increased in group III (M=2.3, M=1.7, and M=3.1 respectively, p<0.001). This time the intervention included class I and class II emergent as well as non-emergent cases. The difference between the three groups was statistically significant (p<0.01). Time to intervention was decreased overall in the post-implementation group pre-COVID and post-COVID (group II+III) to 2.2 from 2.3 hours in group I, however this difference was not statistically significant. Time to intervention showed a statistically significant increase after the pandemic in group III (3.1 vs 1.7 in group II, p<0.001).
 |
Figure 3 Time to Intervention (OR and IR) During Pre-Implementation, Post-Implementation Pre-COVID, and Post-Implementation Post-COVID Phase. |
ED Dwell Time
As shown in Figure 4, ED dwell time in group I was 4.3 hours, decreased in group II to 3.7 hours, and increased in group III to 5.8 hours (p<0.001). Even though ED dwell time initially decreased after implementation and pre-COVID in group II to 3.7 hours, it did not change when group II and III were combined (p=0.81, Table 3). ED dwell time increased from 3.7 hours in group II to 5.8 hours in group III (p<0.001).
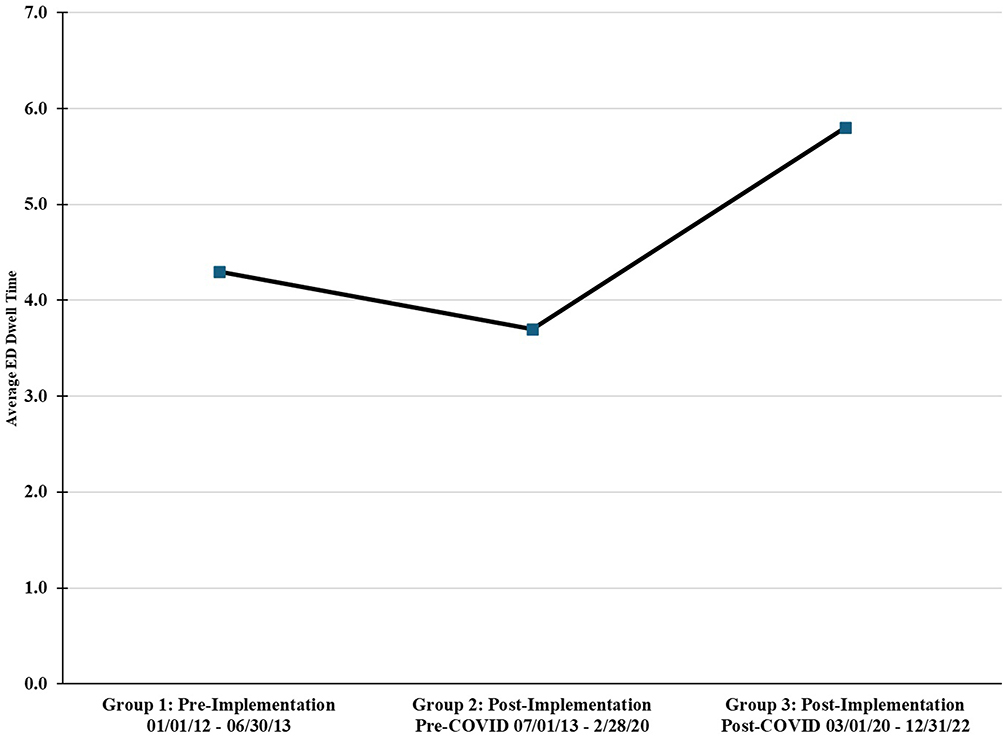 |
Figure 4 ED Dwell Time During Pre-Implementation, Post-Implementation Pre-COVID, and Post-Implementation Post-COVID Phases. |
Discussion
The proficiency of nurses is vital for improving the efficacy of ED services. Trauma resuscitation acts as an essential connection between injury and management. Ineffective communication accounts for most of the errors in high-risk settings, especially trauma resuscitation settings.1 Lacerenza et al emphasized that team-building interventions across multiple domains produce effective outcomes.6 The findings of our study provide valuable insights into developing a team of dedicated trauma nurses trained in trauma scenarios with designated roles and responsibilities to optimize trauma resuscitation.7,8 Metrics such as time to OR, time to CT, time to vital signs, time to labs, and ED dwell time are key indicators of patient outcomes. Although previous studies have examined the impact of trauma-specific programs, they have not evaluated these metrics to assess long-term system efficacy.
The variables evaluated after our DTN program’s implementation, including time to vital signs and CT scan, showed a statistically significant decrease after our implementation phase and before the COVID-19 pandemic.
Our findings are consistent with previous studies demonstrating the importance of a specialized trauma nursing program. Polovitch et al reported that their trauma nurse leadership program (TNL) led to a more efficient ER and not only improved patient outcomes significantly, but overall physician and staff satisfaction increased, and a decrease in the risk of ED nursing burnout was also reported.9 After implementing a DTN program, our time to CT scan, intervention, and ED dwell time decreased. This finding aligns with another study that observed reduced ED, CT scan, and intervention times within the first two hours after introducing a trauma resuscitation emergency care (TREC) nurse.7 While we observed a decrease in time to intervention after implementing our DTN program (Figure 3); however, the difference among groups did not reach statistical significance. Our mean time to intervention is expressed in hours, and we did not differentiate between our highest level of activation (Level I) and our Level 2 activations. The time to intervention ranged from 7 minutes to 9 hours, but a detailed analysis of the type of procedure was not performed. Murao et al observed that early CT scan examinations improved 24-hour mortality, suffering severe blood loss, but did not affect overall survival.10 A study by Lin Hsieh et al stated that a shorter time for definitive care led to a higher rate of survival.11 There has also been a decrease in hospital length of stay and ICU length of stay after adding an experienced trauma nurse.8,12
The inability to sustain these changes after 2020 is primarily attributed to the COVID-19 pandemic. The effect of COVID-19 cannot be understated, as the enormity of the pandemic was not fully understood until the following years. These results are consistent with those from previous studies; for example, Mulyadi et al reported on nurses’ experience and exhaustion of ED nurses during emergency triage after the first wave of COVID-19.13 All variables in our study were increased during and after the pandemic. ED nurses experienced extreme ordeals in triaging ED patients due to unmet demand and insufficient understanding of the disease. Another survey-based study also emphasized the delay in triage, stating that screening for COVID-19 and/or positive COVID-19 tests also led to delays in treatment.14 Our ED nurses faced the same challenges as many others throughout the world, which led to substantial burnout and subsequently staffing shortages. Due to inadequate onboarding of ED nurses with the trauma education program, there was a worsening in our efficiency variables during the COVID-19 pandemic.
The findings from our study have several implications for ED efficiency. Our study highlights the importance of introducing a team of DTNs to provide comprehensive trauma care. It also signifies the importance of defining roles in the emergency department, ensuring clarity in responsibilities while promoting effective teamwork. Although operational metrics are essential, trauma care, especially in pediatric populations, encompasses psychological safety and trauma-related stress outcomes for patients, as well as the overall well-being of emergency department nurses. Designated Trauma Nurses (DTNs) can directly benefit patients by ensuring organized care from the outset, reducing emotional stress for nurses through adequate preparation, and, in pediatric cases, helping to maintain an emotionally safe environment for children. Additionally, DTNs help prevent overcrowding in the trauma bay and facilitate clear communication with trauma providers. While our outcomes improved during the first phase of implementation, the decline during the COVID-19 pandemic cannot be overlooked.
Our study has several limitations. First, data were collected from a single Level 1 trauma center, which restricts the generalizability of our findings to other institutions with different management protocols. We also did not conduct subgroup analyses based on the mechanism of injury or type of operative intervention, such as thoracoabdominal, neurosurgical, or orthopedic procedures. Furthermore, data collection and charting may have omitted certain variables, particularly during the COVID-19 pandemic. Finally, the observed time to the operating room was longer, potentially because not all Level 1 trauma activations required immediate surgery, and our analysis combined Level 1 and Level 2 activations, which may have contributed to this finding. Additionally, analysis of pediatric trauma and future studies involving pediatric trauma patients could provide greater insight into communication consistency, emotional containment, and caregiver support.
In summary, this study demonstrates that a dedicated team of trauma nurses enhances efficiency during trauma resuscitation. DTN programs and structured trauma care, achieved through clearly defined nursing roles, may contribute to sustained professional competence and trauma-informed care in adult and pediatric trauma patients. Future research should prioritize developing guidelines and examining additional factors influencing trauma bay efficiency, such as workforce composition and leadership practices that facilitate effective teamwork.
Ethical Statement
The study has been conducted in accordance with the Declaration of Helsinki. Hurley Medical Center Institutional Review Board (IRB) approval was obtained prior to initiation of the study. IRB approval number is 1501215-4. Appropriate consent/waiver of consent was also obtained wherever needed.
Acknowledgments
The authors would like to thank trauma services, ED nurses and ED staff members for their assistance on this project.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Peters VK, Harvey EM, Wright A, Bath J, Freeman D, Collier B. Impact of a TeamSTEPPS trauma nurse academy at a level 1 trauma center. J Emerg Nurs. 2018;44(1):19–12. doi:10.1016/j.jen.2017.05.007
2. Petroze RT, Byiringiro JC, Ntakiyiruta G, et al. Can focused trauma education initiatives reduce mortality or improve resource utilization in a low‐resource setting? World J Surg. 2015;39(4):926–933. doi:10.1007/s00268-014-2899-y
3. Martin S. Designated Trauma nurses in the emergency department: do they impact patient outcomes? J Emerg Nurs. 2011;37(4):413–416. doi:10.1016/j.jen.2010.11.018
4. Galanis P, Vraka I, Fragkou D, Bilali A, Kaitelidou D. Nurses’ burnout and associated risk factors during the COVID‐19 pandemic: a systematic review and meta‐analysis. J Adv Nurs. 2021;77(8):3286–3302. doi:10.1111/jan.14839
5. Lavoie‐Tremblay M, Gélinas C, Aubé T, et al. Influence of caring for COVID‐19 patients on nurse’s turnover, work satisfaction and quality of care. J Nurs Manag. 2022;30(1):33–43. doi:10.1111/jonm.13462
6. Lacerenza CN, Marlow SL, Tannenbaum SI, Salas E. Team development interventions: evidence-based approaches for improving teamwork. Am Psychol. 2018;73(4):517–531. doi:10.1037/amp0000295
7. Holder MW, Leonard MA, Collins HW, Brogan AA, Burns JB. Impact of trauma resuscitation emergency care nurse deployment in trauma activations in a rural trauma center. J Trauma Nurs. 2023;30(4):228–234. doi:10.1097/JTN.0000000000000733
8. Geyer R, Kilgore J, Chow S, Grant C, Gibson A, Rice M. Core team members’ impact on outcomes and process improvement in the initial resuscitation of trauma patients. J Trauma Nurs. 2016;23(2):83–88. doi:10.1097/JTN.0000000000000191
9. Polovitch S, Muertos K, Burns A, Czerwinski A, Flemmer K, Rabon S. Trauma nurse leads in a level i trauma center: roles, responsibilities, and trauma performance improvement outcomes. J Trauma Nurs. 2019;26(2):99–103. doi:10.1097/JTN.0000000000000431
10. Murao S, Yamakawa K, Kabata D, et al. Effect of earlier Door-to-CT and Door-to-Bleeding control in severe blunt trauma: a retrospective cohort study. J Clin Med. 2021;10(7):1522. doi:10.3390/jcm10071522
11. Hsieh S-L, Hsiao CH, Chiang WC, et al. Association between the time to definitive care and trauma patient outcomes: every minute in the golden hour matters. Eur J Trauma Emerg Surg. 2022;48(4):2709–2716. doi:10.1007/s00068-021-01816-8
12. Flood R, Szwargulski P, Qureshi N, et al. Immediate bedding and patient satisfaction in a pediatric emergency department. J Emerg Med. 2016;50(5):791–798. doi:10.1016/j.jemermed.2015.10.008
13. Mulyadi M, Dedi B, Hou W, Huang I, Lee B. Nurses’ experiences of emergency department triage during the COVID‐19 pandemic in Indonesia. J Nurs Scholarsh. 2022;54(1):15–23. doi:10.1111/jnu.12709
14. Blakeman JR, DeVon HA, Stapleton SJ, Kim M, Eckhardt AL. Effects of the COVID-19 pandemic on emergency department triage nurses’ response to patients with potential acute coronary syndrome. J Cardiovasc Nurs. 2024;39(4):371–378. doi:10.1097/JCN.0000000000001008
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.