Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Erectile Dysfunction: Expert Panel Recommendations for Evaluation and Management in the United Arab Emirates
Authors Haddad A, Alzarooni A, Kassem HH, El Khoury J, Hussein S, Hassan T, Vignesh SO, Siddiqui U, Zubaidi OS ![]()
Received 18 September 2025
Accepted for publication 8 November 2025
Published 10 December 2025 Volume 2025:18 Pages 7949—7960
DOI https://doi.org/10.2147/JMDH.S554974
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pavani Rangachari
Anis Haddad,1 Abdulqadir Alzarooni,2 Hussien Heshmat Kassem,3 Joseph El Khoury,4 Saeed Hussein,5 Tarek Hassan,6 Shivani Ohri Vignesh,7 Urooj Siddiqui,8 Osman Saleh Zubaidi8
1Department of Urology, Dubai London Clinic, Dubai, United Arab Emirates; 2Department of Urology, Emirates Urology Society, Dubai, United Arab Emirates; 3Department of Cardiology, Cairo University and Tadawi Specialty Hospital, Dubai, United Arab Emirates; 4The Valens Clinic, One by Omniyat, Dubai, United Arab Emirates; 5Emirates Pharmacy Society, Dubai, United Arab Emirates; 6Global Specialty Excellence, Viatris Inc., Pittsburgh, PA, USA; 7Medical Affairs, Viatris, Bangalore, India; 8Medical Affairs, Viatris, Dubai, United Arab Emirates
Correspondence: Anis Haddad, Department of Urology, Dubai London Clinic, Jumeirah Road, 3, Dubai, 102565, United Arab Emirates, Email [email protected]
Abstract: Erectile dysfunction (ED) is one of the most common sexual disorders in men, and its effective management requires a holistic approach involving the collaboration of healthcare professionals from various specialties. There is a reluctance to seek treatment despite the high prevalence. In the UAE, there are no region-specific guidelines to guide physicians about its management. To address this need, a panel comprising experts from urology, psychiatry, interventional cardiology, and clinical pharmacy convened in Dubai from 19 to 21 May 2023 to provide recommendations for the management of ED in the UAE. The panel reviewed the currently available data and international guidelines to formulate recommendations for managing the condition in the UAE. The panel recommended recognizing ED as an early sign of cardiovascular disease, addressing psychological concerns, and involving multidisciplinary collaboration for managing the condition. Patients with ED should be screened for other comorbidities. There is a need for a well-connected network of healthcare providers comprising psychologists, gynecologists, urologists, dieticians, physical therapists, pharmacists, yoga instructors, and nurses to treat patients with ED, and timely referrals within this network are necessary. Recognizing the psychological impact of the condition, providing counseling to couples and psychological support to the patient is critical. Shared decision-making about treatment, based on open and meaningful conversations is the need of the hour. Technology can be used for awareness and patient education. Understanding the burden of ED and developing a patient-centric collaborative framework involving various specialists is important for the early diagnosis and effective management of ED. These expert recommendations aim to standardize ED management in the UAE and enhance multidisciplinary collaboration.
Keywords: erectile dysfunction, sexual dysfunction, male sexual disorders, holistic health
Introduction
Erectile dysfunction (ED) is one of the most common sexual disorders in men, with millions affected worldwide.1,2 The estimated prevalence is expected to be 322 million worldwide by 2025.3 The prevalence is about 20% at age <30 years, 25% at 30–39 years, 40% at 40–49 years, 60% at 50–59 years, 80% at 60 to 69 years, and 90% at > 70 years.4,5 Other than age, the major risk factors independently associated with ED include diabetes, cardiovascular disease (CVD), and depression.3 Conversely, ED itself is a predictor of CVD, dementia, and all-cause mortality.3 Other conditions associated with ED include obstructive sleep apnea6 and gastrointestinal disorders;7 however, this association is not widely known among clinicians. Hence, ED must be considered a symptom or indicator of other comorbidities rather than a primary condition.8 Evidence indicates that CVD can occur within two to three years of ED diagnosis.9 Individuals with ED have a higher risk of negative impact on their psychological, social, and physical well-being than those without ED.1, Effective management of ED requires a holistic approach involving the multidisciplinary collaboration of healthcare professionals from a range of relevant specialties. For successful management of ED, early recognition of the psychological impact of ED, early screening, and addressing the psychological issues in a culturally sensitive manner are critical.10 However, in clinical practice, the psychological aspects of ED receive little attention.1 Most clinical guidelines on ED focus on the assessment and treatment of ED only from a medical perspective, and the psychosocial aspects of ED are often ignored.2
The prevalence of ED in Arab countries is high; however, many patients feel embarrassed to discuss the problem and refrain from seeking treatment, although this has been improving in the last few years with the exposure to information over the internet and other platforms.11 There are no UAE-specific guidelines to guide physicians on the management of this condition. Hence, an expert panel was constituted to provide recommendations specific to the UAE, based on the best practices from existing international guidelines for the management of ED. The objectives of the panel discussion were to:
- Understand the health burden of ED and its underlying comorbidities in the UAE.
- Explore the current practice and gaps in managing ED in the UAE.
- Develop a patient-centric collaborative framework around management.
- Emphasize the role of open communication in the effective management of ED.
- Recommend effective strategies for patient referral.
Materials and Methods
A panel of 10 experts from urology, psychiatry, interventional cardiology, and clinical pharmacy convened in Dubai from 19 to 21 May 2023. Before the meeting, a structured discussion plan was created. It included 1) the available epidemiological data and the panel’s insights on ED in the UAE, 2) the current challenges in treating the condition in the UAE according to the panel, 3) the specialties that need to be involved in managing the condition, 4) international guidelines for the management of ED, and 5) formulating recommendations for managing the condition in the UAE. The current evidence-based international guidelines on the treatment of ED, particularly the EAU Guidelines on Sexual and Reproductive Health 202512 and the 2018 Revision to the Process of Care Model for Evaluation of Erectile Dysfunction,8 as well as the epidemiological data on ED in Arab countries, were reviewed by the panel. These guidelines and their own clinical experiences regarding the challenges in managing ED in the UAE were discussed. The published data of studies from the UAE on ED regarding the epidemiology and the challenges in treatment were also reviewed. Based on these, the panel arrived at protocols for screening, early diagnosis, and management of ED. No voting process was followed to arrive at the recommendations, as grading was not possible due to inadequate data on ED from the UAE. Statements were framed largely based on the panel’s clinical insights and international guidelines.
Results and Discussion
The Current Landscape of ED in the UAE
There is a lack of data about the prevalence and epidemiology of ED in the UAE. In fact, there is no robust data from the Arab region as a whole on the true prevalence of ED. Nevertheless, anecdotal reports and studies from Saudi Arabia have shown a high incidence of ED across different age groups and in those with comorbidities.13 A cross-sectional survey in 2022 among more than 300 married men in Saudi Arabia reported that the overall prevalence of ED was 10.45%. The prevalence among those aged >55 years was 32.43%. Medical conditions like diabetes mellitus, hypertension, hypercholesterolemia, hypogonadism (metabolic syndrome in general), lower education level, and sedentary lifestyle were associated with a higher prevalence.14 In another study during the same year, among 194 men in Saudi Arabia, mild ED was reported among 66.5% of subjects, while 2.6% and 1% had moderate and severe ED, respectively. The subjects were aged between 20 and 64 years. Severe ED was more prevalent among non-occupied men (6.9%), and 18.2% of people with chronic comorbidities had severe ED.15 Smoking was associated with a higher prevalence of ED in a study in southwestern Saudi Arabia in 2022.16 A previous study in 2017 among 230 subjects in Saudi Arabia reported the prevalence of ED as 15%. While patients in the age group of 20 to 30 years were willing to discuss the problem with their physician, those aged 41 to 50 years were reluctant. Overall, 28% of the participants were unwilling to discuss the problem with their physician.17 In a 2011 study among 804 subjects in the Middle East region, the prevalence of ED was 45.1% and was strongly correlated with the presence of risk factors such as age, diabetes, hypertension, depression, hormonal disturbance, and other sexual disorders.18 In a meta-analysis of 102 studies from the Arab countries from 2000 to 2011, the prevalence of ED was as high as >40% in some studies.13 In a cross-sectional study among 100 patients with diabetes aged ≥30 years in Bahrain in 2013, the overall prevalence of ED was 74.4%. The prevalence and severity of ED increased with age, from 55.6% in patients <40 years of age to 83.3% in patients aged 60–69 years. A significant relationship was found between ED and the duration of diabetes, hypertension, and coronary heart disease.19 These data show that the prevalence has remained high over the last decade and is particularly high among those with comorbidities. The expert panel shared that patients suffering from ED in the UAE tend to be younger compared to those in other regions. There is a high prevalence of low testosterone levels, which has led to an increase in the prevalence of ED in recent years. The decrease in testosterone levels is a global phenomenon that is related to the modern lifestyle and its challenges. These include stress, unhealthy diet, sedentary lifestyle, smoking, alcoholism, and substance abuse, along with comorbidities like hypertension, diabetes, anxiety, depression, and external factors such as pollution, radiation, and less healthy food intake.20
A survey highlighted the irrational use of Phosphodiesterase type 5 inhibitors (PDE5i), which are used to treat ED, among men in Saudi Arabia. Of the 1008 men in the survey, 37.5% reported using the drugs. However, among the users, only 38.1% had ED, and 84.1% bought these drugs without a medical prescription. This indicates poor awareness about the potentially dangerous effects of these drugs taken without medical supervision.21 Moreover, a study found that there is wide dissemination of misleading or incorrect information about ED in Arabic-language on social media, and the content has very high viewership. A larger concern is that 84% of the content was not based on scientific evidence.22
Protocols for the Management of ED in the UAE
Most patients with ED usually approach the general practitioner or a family physician for the first consultation about the problem. The modern management of ED requires a holistic approach involving the collaboration of healthcare professionals (HCPs) from a range of relevant specialties. There is a need for an integrated and coordinated approach, including physical, psychological, psychosexual, and bio-psycho-social evaluations during the early screening phase. The medical treatment of ED requires a stepwise approach, beginning with non-invasive treatments such as lifestyle changes and medication, followed by more invasive modalities such as mechanical devices, intracavernous injections, and penile prosthesis, if necessary.2 A multidisciplinary approach, combining medical and psychological treatment, has been shown to be more effective.2 The expert panel shared that there are no holistic guidelines nor a dedicated medical society for sexual health in the UAE. There is a strong social stigma surrounding visits to mental health professionals, particularly in relation to men’s health. There is also a general reluctance to have open conversations about men’s health, including mental health concerns in the broader medical community.
The following protocols for the management of ED in the UAE were suggested by the expert panel:
Screening for ED and Comorbidities
In recent times, ED has been considered an indicator of other metabolic or neurologic diseases rather than a primary condition alone. It is an independent risk factor for CVD, with the risk being 25% higher in those with ED.23 Thus, a patient presenting with ED should be considered an opportunity to screen for other comorbid conditions. ED diagnosis is an opportunity for lifestyle improvements that could prevent the development of a future cardiovascular (CV) event.8
Screening for CVD in men presenting with ED is also cost-effective for secondary prevention of CVD.12 The panel experts explained that endothelial dysfunction manifests first in the penile artery as ED, since it is a narrower artery, while it is still subclinical in larger arteries like the coronary and carotid. A significant number of patients (but not all) with ED should undergo a cardiovascular risk assessment and be treated accordingly. While there are many available tools, the Q-Risk questionnaire offers a simple method for assessing risk to estimate the 10-year risk of CVD, as it has been validated in patients aged 25–84 years while most other tools focus on people aged >40 years. Moreover, the Q-risk questionnaire comprises additional clinical variables, including ED.23
The presence of ED increases the risk of future myocardial infarction, cerebrovascular events, and CV as well as all-cause mortality.24,25 In patients with coronary artery disease (CAD), ED is seen to occur an average of 2 to 3 years before CAD detection.26 Other risk factors associated with ED include atherosclerosis, hyperlipidemia, diabetes mellitus, smoking, obesity, sedentary lifestyle, chronic alcohol use, and benign prostate hyperplasia. However, in real-world cardiology practice, sexual dysfunction is not routinely discussed.27 ED patients with a positive exercise stress test should be considered as having an extremely high risk for future CV events.12 ED is also an independent predictor for atrial fibrillation.28 Patients not diagnosed with diabetes but having impaired glucose tolerance or impaired fasting glucose may also be at risk for endothelial dysfunction and ED.29 Nevertheless, most of these patients remain undiagnosed and are unaware of ED.27 In a patient presenting with ED, blood pressure and heart rate should be measured if they have not been assessed in the previous 3–6 months. Body-mass index (BMI) calculation or waist circumference measurement should be undertaken to assess patients for comorbid conditions.12 Fasting blood glucose or HbA1c, lipid profile, and total testosterone should also be measured.12
Conversely, patients presenting with comorbidities should be screened for ED.8 A patient visiting a cardiologist and complaining of dyspnea should be questioned about the symptoms of ED. Similarly, a patient visiting an endocrinologist for diabetes or a psychologist/psychiatrist for depression may also have an undiagnosed ED.8 A suggested protocol for screening for ED and comorbidities is shown in Figure 1.
 |
Figure 1 Protocol for screening patients complaining of or diagnosed with ED. |
Evaluating a Patient with ED
The first step in evaluating ED is a detailed medical and sexual history of patients and their partners if feasible. The sexual history must include questions about past and current sexual relationships, sexual habits, onset and duration of ED, stress factors in life, previous consultations and treatments taken by the patient, and the patient’s thoughts about sexual performance. The current mental state should also be assessed.12 Discussing sexual history is an important first step in managing ED.8 Sexual habits that the patient should be asked about, include frequency of intercourse, predictability, timing, masturbation habits, use of pornography, desire, orgasm, ejaculation, relationship satisfaction, and sexual pain in either partner.8 The presence of nocturnal and/or morning erections indicates a possible psychogenic component to ED symptoms.30
Other important questions during history taking include age, medical and psychological comorbidities, history of surgery and previous medication, recreational substance use, smoking, and lower urinary tract symptoms.8 Medication history is important because many prescription medications have been associated with ED, including antidepressants, beta-blockers, diuretics, tricyclic antidepressants, benzodiazepines, anti-psychotics, anti-epileptics, and others. Recreational substance use is also associated with ED.8
Psychometric analyses should be done using validated psychometric questionnaires.12 Physical examination should focus on the genitourinary, endocrine, vascular, and neurological systems.12 Serum total testosterone should be measured in all men with ED to rule out testosterone deficiency (TD), defined as total testosterone <300 ng/dL.30 A suggested protocol for the evaluation of a patient with ED is shown in Figure 2.
 |
Figure 2 Protocol for evaluating a patient with ED.12 |
Timely Referrals and Multidisciplinary Approach
Collaboration between different specialists can be useful in patients with ED having many risk factors and comorbidities, for which they might be taking multiple drugs.27 However, the expert panel shared that in current primary practice, there is a low rate of cardiovascular referrals for patients with ED. Physicians should know when to refer a patient with ED to an appropriate specialist.10 Patients with any abnormalities detected in screening tests should be referred to the appropriate subspecialist for additional tests for vascular, neurologic, or endocrinologic abnormalities.8 The clinician should emphasize the importance of consulting other specialists with the patient and his partner.30 High-risk individuals (patients with diabetes, hypertension, family history of cardiovascular disease, patients who complain of dyspnea or chest pain during intercourse) should be referred for cardiac assessment and treatment.12 Referral to a mental health professional should be considered for treatment compliance, addressing performance anxiety, and integrating treatments into a sexual relationship.30
It has been demonstrated that a multidisciplinary team consisting of psychologists, gynecologists, urologists, dieticians, physical therapists, yoga instructors, and nurses in treating patients with sexual dysfunction has a positive impact on the patient and the couple.31 The expert panel suggested that recognizing that ED can be an early sign of cardiovascular disease, addressing psychological concerns, and involving endocrinologists are crucial components of a comprehensive approach to managing this condition. If the underlying causes of ED are not managed, there might be a further progression of underlying pathologies, and the risk of fatal events associated with undiagnosed and untreated secondary disease. The indications for referral are shown in Box 1.10
 |
Box 1 Indications for Specialist Referral in Patients with ED10 |
The 2018 Revision to the Process of Care Model for Evaluation of Erectile Dysfunction recommends psychological referral if there are indications of (1) depressive illness, (2) performance anxiety, and (3) couple dysfunction. It provides a list of questions that can help physicians identify the symptoms; these are presented in Figure 3.8 Experts at the meeting suggested that there is a need for a well-connected network of healthcare providers, addressing cultural barriers, promoting couple counseling, enhancing healthcare professionals’ knowledge, advocating for licensed sexologists, considering the impact of sexual performance anxiety, and providing psychological support to individuals with ED.
 |
Figure 3 Questions to detect the need for a psychological referral in patients with ED according to the Process of Care Model for Evaluation of Erectile Dysfunction.6 |
Psychosexual Assessment and Counseling
Physical, psychological, and social factors interact and influence the behavioral expression of ED.2 ED can affect the psychosocial health and quality of life (QoL) of the patient and his partner.12 It also affects self-confidence and is associated with a negative body image.2 According to the expert panel, psychiatric conditions such as depression and anxiety are strongly associated with ED. While ED itself might cause anxiety and depression, many psychiatric medications can negatively impact sexual health and performance. Questioning one’s abilities and self-doubt are common among individuals with ED, which is likely to negatively impact both mental and sexual well-being- a common example is sexual performance anxiety. Unfortunately, most available psychiatric assessment tools do not address sexual function.
A relaxed atmosphere during history-taking is important to facilitate conversations about erectile function and to explain the diagnosis and treatment approach to the patient and his partner. Validated psychometric questionnaires can be used to assess the various sexual function domains.12 While early assessment of psychological functioning is critical, the experts agreed that it is uncommon for someone to initially seek help from a psychologist or psychiatrist when experiencing ED. Psychosexual counseling is also often underutilized once a diagnosis has been made. The components that should be considered during the psychosocial assessment are shown in Box 2. The sexual partner should be included during the assessment.2
 |
Box 2 Components That Should Be Considered During Psychosocial Assessment2 |
The panel experts shared that recognizing the psychological aspects and integrating the expertise of psychologists is crucial for effectively addressing the multifaceted nature of this condition. Open and meaningful conversations are critical, as they play a vital role in addressing the concerns of patients with ED. In addition, there is a need for a diagnostic and therapeutic approach that addresses the sexual health needs of aging couples as a whole, rather than treating the man in isolation. Psychosexual counseling is crucial and often underutilized, and involving couples in the discussion should be considered. Couple therapy and counseling are recommended for specific cases where there is a need for intervention in relationship dynamics, although it may not be necessary for all patients. Dealing with cultural stigma affecting ED patients requires a tactful and patient-centered approach. It is important to create a safe and non-judgmental environment and provide culturally sensitive care. Confidentiality and privacy during the discussion about ED help patients feel more secure in seeking help.
Psychoeducation is the critical first step for increasing the patient’s knowledge about sexual response and ED and making him comfortable talking openly about sex.2 Psychological treatment programs commonly include psychoeducation for reducing anxiety, cognitive therapy, and sexual fantasy training; increasing sexual stimulation; and couple interventions.2 Cognitive behavior therapy should be combined with medical treatment to maximize treatment outcomes.12 Psychological treatment can improve treatment compliance, amalgamate the therapy into the sexual relationship, and help in resolving issues such as anxiety, negative thoughts, distress, self-confidence, intimacy, and communication problems between partners. Moreover, psychological treatment can prevent the recurrence of sexual problems after treatment because the patient learns to manage his dysfunctional response patterns associated with ED.2 It is also important to address unrealistic treatment expectations to prevent treatment discontinuation and dissatisfaction.
Pharmacological Treatment of ED
The choice of treatment should involve a shared decision between the patient, partner, and healthcare professional. Shared decision-making leads to better compliance and in turn, better outcomes because patients have more realistic treatment expectations.2 Clinician-patient communication can begin with a discussion of the patient’s goals and expectations in seeking treatment and include the goals of the couple. Clinicians can then emphasize the importance of evaluating and addressing any underlying comorbidities rather than only treating the symptoms of ED. During the initial and subsequent visits, the clinician should explain the effect of comorbidities, age, and factors like sexual history, relationship, and anxiety on sexual health, and suggest the option of including the sexual partner in discussions of ED treatment.8 Experts shared that in the UAE, phosphodiesterase type 5 inhibitor (PDE5i) inhibitors such as sildenafil and tadalafil are commonly used. Both are perceived to have comparable efficacy and tolerability. The choice between them, as well as on-demand vs daily dosing, depends on the patient’s preferences. Experts suggested that it is important to clarify that sexual dysfunction medications like PDE5i do not increase the risk of myocardial infarction in the vast majority of patients.
Modifiable or reversible risk factors, including lifestyle or drug-related factors, may be modified either before or at the same time as pharmacological treatment for ED. Underlying comorbidities should be well-controlled as the first step in ED treatment.12 Patients should be advised that a healthy diet and increased physical activity improve overall health and may improve erectile function.30 A treatment option of an oral PDE5i should be offered unless contraindicated, after discussing the benefits and risks. The currently approved PDE5is include sildenafil, tadalafil, vardenafil, and avanafil.30 Clinical trial results for the four PDE5is and post-marketing data of sildenafil, tadalafil, and vardenafil showed no increase in myocardial infarction rates in those taking PDE5is. The adverse events due to PDE5i are not aggravated even when the patient is taking several antihypertensive medications.12 Patients should also be informed of other options such as vacuum erection device, intracavernosal injection, LI-SWT (low-intensity shockwave therapy), and intra-urethral alprostadil, including discussion of benefits and risks/burdens.12,30 Studies have shown that topical testosterone therapy in hypogonadal men improves sexual function.29,30 However, clinicians are often concerned about the cardiovascular risk associated with testosterone replacement therapy. In a recent study, 5246 men aged 45 to 80 years with pre-existing or a high risk of cardiovascular disease and symptoms of hypogonadism, subjects received transdermal 1.62% testosterone gel (dose adjusted to maintain testosterone levels between 350 and 750 ng per deciliter) or placebo. Results showed that testosterone-replacement therapy did not lead to an increased incidence of major adverse cardiac events compared to placebo during a mean 22-month follow-up.31
Despite several claims of improvement in ED with medicinal herbs and natural supplements, robust scientific data are lacking. A recent Cochrane review showed that ginseng has only inconsequential effects on erectile function compared to placebo when assessed using validated tools.32 Another study reported that low serum levels of folic acid and vitamin B12 can lead to ED.33 The major challenge in treatment identified by the experts is that insurance companies in the UAE do not cover ED treatment. They recommended involving decision-makers and policymakers in the UAE to advocate for changes in insurance policies to ensure coverage for ED management. A suggested protocol for the management of ED is shown in Figure 4.
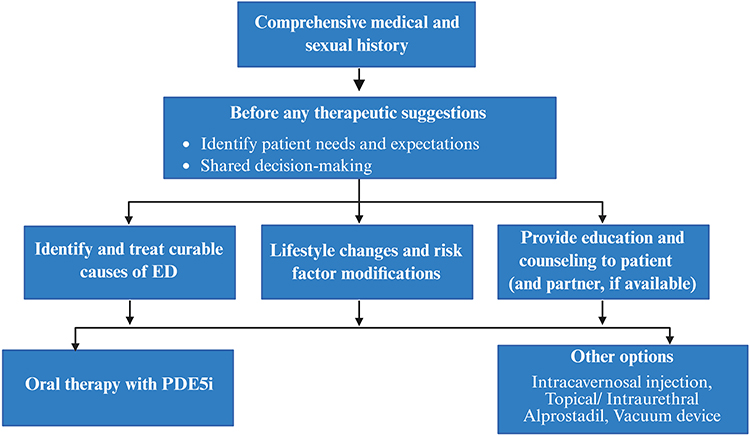 |
Figure 4 Protocol for the management of ED.12 |
Role of Pharmacists in the Management of ED
Experts at the meeting discussed the key role of pharmacists in providing appropriate guidance to patients with ED, as patients often approach pharmacists for counseling. This is because patients are inclined to pursue over-the-counter options such as herbal extracts and dietary supplements, rather than seek medical consultation.
Pharmacists can play a key role in patient communication and education. Their role can encompass several key areas as discussed below.
Patient Education and Counseling
Pharmacists can counsel patients about the various treatment options available for ED. They can explain how these medications work, how they should be taken, their potential side effects, and the importance of adherence to the prescribed treatment. Pharmacists can also provide lifestyle advice, such as the benefits of weight management, smoking cessation, and reducing alcohol consumption, which can improve ED symptoms.
Screening and Referral
Pharmacists can play a role in identifying patients who are likely to have ED through routine health screenings or during medication reviews. They can assess the presence of risk factors and comorbid conditions, such as diabetes, cardiovascular disease, and hypertension, which are often associated with ED. Based on the assessment, pharmacists can refer patients to their primary care provider or a specialist for further evaluation and treatment.
Medication Management
Pharmacists can review if a patient’s current medications, such as antihypertensives, antidepressants, or antipsychotics, can be a cause of ED. They can suggest alternative medications or dosages that may have a lower risk of causing or exacerbating ED. They can ensure that PDE5i is being used safely by a patient by enquiring about any adverse effects.
Support and Follow-Up
Pharmacists can offer ongoing support to patients by following up with them to assess the effectiveness of treatment and make any necessary adjustments in collaboration with the prescribing physician. Pharmacists can also address patients’ concerns or questions, ensuring that they feel comfortable and informed about their treatment.
Public Health and Advocacy
Pharmacists can contribute to public health efforts by increasing awareness about ED, reducing the stigma around it, and encouraging men to seek help. They can advocate for better access to ED treatment. Thus, pharmacists can play an integral role in the holistic management of ED, ensuring that patients receive comprehensive care addressing both physical and psychological aspects of the condition.
However, there is a knowledge gap among pharmacists about when patients should be referred to various specialists. They need to be provided with more education about ED and its comorbidities to equip them with effective counseling and referral. Efforts should be made to enhance their knowledge and improve communication.
Use of Technology for Education to Optimize Screening, Diagnosis, and Management of ED
There has been an increase in the use of technology-based sexual health education in recent years. Various digital technology tools, such as television, computers, tablets, smartphones, mobile apps, online educational games, or online collaborative learning environments, are being used for education.34 Digital sexual health education should focus on the importance of screening, diagnosis, and management of ED. The need for more widespread and easily accessible sex education is evident, and technology can offer cost-effective and longer-term sustainable educational solutions.35 Sexual health education programs can provide information and support to improve knowledge, attitudes, and behaviors related to sexual health.36 Technology-based interventions also allow increased privacy and more flexibility in customizing messages, as well as provide self-help support.35,36 Several digital strategies, such as web-based training modules, virtual videos, and simulated videos, can be used along with information dissemination/awareness campaigns.35 Digital health technologies have shown higher efficacy and greater engagement compared with traditional behavioral interventions.36
Conclusion
The modern management of ED in the UAE requires a holistic approach involving the multidisciplinary collaboration of HCPs from a range of relevant specialties. Recognizing that ED can be an early sign of cardiovascular disease, addressing psychological concerns, and involving endocrinologists are crucial components of a comprehensive approach to managing this condition. By screening patients with ED for other comorbidities, the risk of future cardiovascular events can be detected early, and such events can be effectively prevented. There is a need for a well-connected network of healthcare providers, consisting of psychologists, gynecologists, urologists, dieticians, physical therapists, yoga instructors, and nurses to treat patients with sexual dysfunction, and timely referrals within this network are important. Couple counseling and providing psychological support to individuals with ED is critical, considering that ED is strongly associated with anxiety and depression. Recognizing the psychological aspects and integrating the expertise of psychologists is crucial for effectively addressing the multifaceted nature of this condition. Open and meaningful conversations are critical, as they play a vital role in addressing the concerns of patients with ED. Shared decision-making between the patient, partner, urologist, and other specialists is an important part of patient-centered collaborative care in ED.
Statements for the Recommended Management of ED in the UAE Agreed Upon by the Expert Panel
- The management of ED in the UAE requires collaboration between HCPs across a range of specialties. There is a need for an integrated and coordinated approach, including physical, psychological, psychosexual, and bio-psycho-social evaluations during the early screening phase.
- A patient presenting with ED should be screened for other comorbid conditions. Similarly, patients presenting with comorbidities should be screened for ED.
- The first step in evaluating ED is a detailed medical and sexual history of patients and their partners.
- The current mental state should also be assessed at the first visit. Psychometric analyses should be done using validated psychometric questionnaires.
- Examination at first presentation with ED should include blood pressure, heart rate, BMI, waist circumference, fasting blood glucose or HbA1c, lipid profile, and total testosterone.
- The Q-Risk questionnaire offers a simple method for assessing risk to estimate the 10-year risk of cardiovascular disease.
- Patients with any abnormalities in screening tests should be referred to the appropriate subspecialist for additional tests for vascular, neurologic, or endocrinologic abnormalities.
- High-risk individuals (patients with diabetes, hypertension, family history of cardiovascular disease, patients who complain of dyspnea or chest pain during intercourse) should be referred for cardiac assessment and treatment.
- Referral to a mental health professional, psychosexual counseling, including couple therapy and counselling, should be considered.
- A multidisciplinary team consisting of psychologists, gynecologists, urologists, dieticians, physical therapists, yoga instructors, and nurses in treating patients with sexual dysfunction should manage a patient with ED.
- The medical treatment of ED should begin with lifestyle changes and medication.
- The choice of treatment should involve a shared decision between the patient, partner, and healthcare professional.
- It is important to clarify that sexual dysfunction medications like PDE-5 inhibitors do not increase the risk of myocardial infarction in the vast majority of patients.
- Underlying comorbidities should be well-controlled as the first step of any ED treatment.
- There is no scientific data about the improvement in ED with medicinal herbs and natural supplements.
- Cognitive behavior therapy should be combined with medical treatment to maximize treatment outcomes.
- Invasive modalities such as mechanical devices, intracavernous injections, and penile prosthesis, if necessary, should be used only after the failure of lifestyle changes and medication.
Abbreviations
CAD, coronary artery disease; CVD, cardiovascular disease; ED, Erectile dysfunction; LI-SWT, low-intensity shockwave therapy; PDE5i, Phosphodiesterase type 5 inhibitors; QOL, quality of life; TD, testosterone deficiency.
Acknowledgments
Medical writing assistance was provided by Dr. Sangeeta Dhanuka. Editorial assistance was provided by Dr. Shantha Kumar V from Viatris.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Medical writing assistance was funded by Viatris.
Disclosure
AH and SH have consulted for Viatris and have received honoraria as speakers. HHK has been a speaker for Boehringer Ingelheim, Viatris, Novartis, Bayer, Amgen, and Servier. JEK received a support grant from Janssen in 2017. He has been a consultant for some pharmaceutical companies and has received honoraria. He has been a regular speaker for Viatris, Janssen, Lundbeck, Pfizer, Newbridge, Hikma, and others. TH and US are employees of Viatris and hold shares of Viatris. SOV and OZ are employees of Viatris. AQA has no conflicts of interest to report.
References
1. Allen MS, Wood AM, Sheffield D. The psychology of erectile dysfunction. Curr Dir Psychol Sci. 2023;32(6):487–493. doi:10.1177/09637214231192269
2. Dewitte M, Bettocchi C, Carvalho J, et al. A psychosocial approach to erectile dysfunction: position statements from the European society of sexual medicine (ESSM). Sex Med. 2021;9(6):100434. doi:10.1016/j.esxm.2021.100434
3. Kessler A, Sollie S, Challacombe B, Briggs K, Van Hemelrijck M. The global prevalence of erectile dysfunction: a review. BJU Int. 2019;124(4):587–599. doi:10.1111/bju.14813
4. Allen MS, Walter EE. Erectile dysfunction: an umbrella review of meta-analyses of risk-factors, treatment, and prevalence outcomes. J Sex Med. 2019;16(4):531–541. doi:10.1016/j.jsxm.2019.01.314
5. Geerkens MJM, Al-Itejawi HHM, Nieuwenhuijzen JA, et al. Sexual dysfunction and bother due to erectile dysfunction in the healthy elderly male population: prevalence from a systematic review. Eur Urol Focus. 2020;6(4):776–790. doi:10.1016/j.euf.2019.03.004
6. Cantone E, Massanova M, Crocetto F, et al. The relationship between obstructive sleep apnoea and erectile dysfunction: an underdiagnosed link? A prospective cross‐sectional study. Andrologia. 2022;54(9). doi:10.1111/and.14504
7. Romano L, Zagari RM, Arcaniolo D, et al. Sexual dysfunction in gastroenterological patients: do gastroenterologists care enough? A nationwide survey from the Italian society of gastroenterology (SIGE). Digestive Liver Dis. 2022;54(11):1494–1501. doi:10.1016/j.dld.2022.05.016
8. Mulhall JP, Giraldi A, Hackett G, et al. The 2018 revision to the process of care model for evaluation of erectile dysfunction. J Sex Med. 2018;15(9):1280–1292. doi:10.1016/j.jsxm.2018.06.005
9. Hadisuyatmana S, Malik G, Efendi F, Reisenhofer S, Boyd J. The experiences and barriers in addressing type 2 diabetes mellitus-associated erectile dysfunction: a mixed method systematic review. Syst Rev BioMed Central Ltd. 2023;12(1):138. doi:10.1186/s13643-023-02303-4
10. Al-Shaiji TF. Breaking the ice of erectile dysfunction taboo: a focus on clinician–patient communication. J Patient Exp. 2022;9. doi:10.1177/23743735221077512
11. Almigbal TH, Schattner P. The willingness of Saudi men with type 2 diabetes to discuss erectile dysfunction with their physicians and the factors that influence this. PLoS One. 2018;13(7):e0201105. doi:10.1371/journal.pone.0201105
12. Salonia A, Boeri L, Capogrosso P, et al. EAU Guidelines.
13. El-Sakka AI. Erectile dysfunction in Arab countries. Part I: prevalence and correlates. Arab J Urol. 2012;10(2):97–103. doi:10.1016/j.aju.2012.01.004
14. Alenezi TM, Ahamed SS, Almutairi HR, et al. Prevalence and the associated factors of erectile dysfunction among saudi married males. Cureus. 2022. doi:10.7759/cureus.30998
15. Almarzouq Y, Altheneyan M, Alhazzani N, Almarzouq A, Sammour M. Please cite this article in press Yousef almarzouq et al, Prevalence of erectile dysfunction in young Saudi population. Indo Am J P Sci. 2022;2022(8):9. doi:10.5281/zenodo.7037305
16. Alamri AA, Al-Qahtani FS, Alsamghan AS, et al. Prevalence of erectile dysfunction among smokers in southwestern Saudi Arabia. J Mens Health. 2022;18(4):92. doi:10.31083/j.jomh1804092
17. Attaky A. HP-07-001 the prevalence of sexual dysfunction among Arab males living in Saudi Arabia. J Sex Med. 2017;14(Supplement_4a):e156–e156. doi:10.1016/j.jsxm.2017.03.056
18. Shaeer O, Shaeer K. The global online sexuality survey (GOSS): erectile dysfunction among Arabic‐speaking internet users in the middle east. J Sex Med. 2011;8(8):2152–2163. doi:10.1111/j.1743-6109.2011.02297.x
19. AlGhanem, Amal, Al Zayani, Ghada Prevalence and risk factors associated with erectile dysfunction among Bahraini men with diabetes mellitus. Journal of the Bahrain Medical Society. 2018; 30 (1): 27–34.
20. Joshi OV, Savale RR, Nalage D, Biradar A, Sontakke T. Lifestyle in flux: urbanization, dietary shifts, and endocrine health in emerging adulthood. Reprod Biol Endocrinol. 2025;23(1):118. doi:10.1186/s12958-025-01442-8
21. Alshahrani S, Ahmed AF, Gabr AH, Al Ansari A, El-Feky M, Elbadry MS. Phosphodiesterase type 5 inhibitors: irrational use in Saudi Arabia. Arab J Urol. 2016;14(2):94–100. doi:10.1016/j.aju.2016.03.003
22. Alzahrani MA, Khan MA, Hakami BO, et al. Is Arabic information on YouTube about erectile dysfunction based on scientific evidence? Res Rep Urol. 2023;15:261–272. doi:10.2147/RRU.S410127
23. Hippisley-Cox J, Coupland C, Brindle P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: prospective cohort study. BMJ. 2017;j2099. doi:10.1136/bmj.j2099
24. Weber MF, Smith DP, OˈConnell DL, et al. Risk factors for erectile dysfunction in a cohort of 108 477 Australian men. Med J Aust. 2013;199(2):107–111. doi:10.5694/mja12.11548
25. Gazzaruso C, Coppola A, Montalcini T, et al. Erectile dysfunction can improve the effectiveness of the current guidelines for the screening for asymptomatic coronary artery disease in diabetes. Endocrine. 2011;40(2):273–279. doi:10.1007/s12020-011-9523-9
26. Montorsi P, Ravagnani PM, Galli S, et al. Association between erectile dysfunction and coronary artery disease. Role of coronary clinical presentation and extent of coronary vessels involvement: the COBRA trial. Eur Heart J. 2006;27(22):2632–2639. doi:10.1093/eurheartj/ehl142
27. Cirillo L, Fusco GM, Di Bello F, et al. Sexual dysfunction: time for a multidisciplinary approach? Archivio Italiano di Urologia e Andrologia. 2023. doi:10.4081/aiua.2023.11236
28. Tanaka Y, Bundy JD, Allen NB, et al. Association of erectile dysfunction with incident atrial fibrillation: the multi-ethnic study of atherosclerosis (Mesa). Am J Med. 2020;133(5):613–620.e1. doi:10.1016/j.amjmed.2019.08.052
29. Corona G, Rastrelli G, Balercia G, et al. Hormonal association and sexual dysfunction in patients with impaired fasting glucose: a cross-sectional and longitudinal study. J Sex Med. 2012;9(6):1669–1680. doi:10.1111/j.1743-6109.2012.02717.x
30. Burnett AL, Nehra A, Breau RH, et al. Erectile dysfunction: AUA Guideline. J Urol. 2018;200(3):633–641. doi:10.1016/j.juro.2018.05.004
31. Lynn M, Iftekhar N, Mumby P, Hakimi M, Adam W. A multidisciplinary approach to the treatment of sexual dysfunction in couples. J Sex Med. 2022;19(Supplement_3):S6–S7. doi:10.1016/j.jsxm.2022.05.017
32. Lee HW, Lee MS, Kim TH, et al. Ginseng for erectile dysfunction: a cochrane systematic review. World J Mens Health. 2022;40(2):264. doi:10.5534/wjmh.210071
33. Xu J, Xu Z, Ge N, et al. Association between folic acid, homocysteine, vitamin B12 and erectile dysfunction—A cross‐sectional study. Andrologia. 2021;53(11). doi:10.1111/and.14234
34. Decker MJ, Harrison S, Price M, Gutmann-Gonzalez A, Yarger J, Tenney R. Educators’ perspectives on integrating technology into sexual health education: implementation study. JMIR Hum Factors. 2022;9(1):e31381. doi:10.2196/31381
35. Huang KY, Kumar M, Cheng S, Urcuyo AE, Macharia P. Applying technology to promote sexual and reproductive health and prevent gender based violence for adolescents in low and middle-income countries: digital health strategies synthesis from an umbrella review. BMC Health Serv Res. 2022;22(1):1373. doi:10.1186/s12913-022-08673-0
36. Brayboy LM, McCoy K, Thamotharan S, Zhu E, Gil G, Houck C. The use of technology in the sexual health education especially among minority adolescent girls in the United States. Curr Opin Obstet Gynecol. 2018;30(5):305–309. doi:10.1097/GCO.0000000000000485
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relationship Between Hypertension, Antihypertensive Drugs and Sexual Dysfunction in Men and Women: A Literature Review
Lou IX, Chen J, Ali K, Chen Q
Vascular Health and Risk Management 2023, 19:691-705
Published Date: 3 November 2023