Back to Journals » OncoTargets and Therapy » Volume 10
Epidermal growth factor receptor T790M mutation-positive metastatic non-small-cell lung cancer: focus on osimertinib (AZD9291)
Authors Saad N, Poudel A, Basnet A, Gajra A
Received 29 August 2016
Accepted for publication 2 December 2016
Published 22 March 2017 Volume 2017:10 Pages 1757—1766
DOI https://doi.org/10.2147/OTT.S100650
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr XuYu Yang
Nibal Saad, Aarati Poudel, Alina Basnet, Ajeet Gajra
Internal Medicine Department, Division of Hematology and Oncology, Upstate Cancer Center, SUNY Upstate Medical University, Syracuse, NY, USA
Abstract: Adenocarcinoma is the most common type of non-small-cell lung cancer (NSCLC). Adenocarcinoma with epidermal growth factor receptor (EGFR) mutations accounts for 8%–30% of all cases of NSCLC depending on the geography and ethnicity. EGFR-mutated NSCLC usually responds to first-line therapy with EGFR tyrosine kinase inhibitors (TKIs). However, there is eventual loss of efficacy to TKIs due to development of resistance. The most frequent cause for resistance is a second EGFR mutation in exon 20 (T790M), which is encountered in up to 62% of patients. Osimertinib is one of the third-generation EGFR TKIs with a high selective potency against T790M mutants. In Phase I trial of osimertinib in advanced lung cancer after progression on EGFR TKIs, the response rate and disease control rate were 61% and 95%, respectively. A subsequent Phase II (AURA2) trial demonstrated a disease control rate of 92%, a response rate of 71%, a median duration of response of 7.8 months, and a median progression-free survival of 8.6 months. Osimertinib was approved by the US Food & Drug Administration in November 2015 for patients whose tumors exhibited T790M mutation and for those with progressive disease on other EGFR TKIs. In this review, we address the role of EGFR TKIs in the management of EGFR mutation lung cancer and the mechanisms of resistance to TKIs with a focus on the role of osimertinib. Data from completed trials of osimertinib, ongoing trials, as well as novel diagnostic methods to detect EGFR T790M mutation are reviewed.
Keywords: osimertinib, AZD9291, third-generation EGFR TKIs, EGFR T790M, lung adenocarcinoma, NSCLC
Epidermal growth factor receptor mutation (EGFRm) and tyrosine kinase inhibitors (TKIs) in non-small-cell lung cancer (NSCLC)
Lung cancer is one of the leading causes of cancer deaths, accounting for ~27% in males and 26% in females of all cancer deaths.1 The mortality rate from lung cancer exceeds that of breast, prostate, and colorectal cancers combined.1,2 In 2016, 224,390 new cases of lung cancer are estimated, with 158,0803 deaths being attributed to the disease. Only 17.7% of lung cancer patients are expected to be living 5 years after diagnosis.3
NSCLC accounts for 83% of lung cancers, and 50% of these are adenocarcinomas.2 The 5-year survival rates are 55%, 27%, and 4% in localized, regional, and metastatic diseases, respectively, and the median survival is between 10 months and 12 months in advanced NSCLC.2 EGFRm NSCLC accounts for 10%–15% of NSCLC patients in Europe, 30%–40% in Asia, and 7%–8% in North America.4 The incidence of EGFRm lung cancer is 22%–60% in women vs 8%–37% in men and 32%–64% in never smokers vs 6%–33% in smokers.4,5
Most of the EGFRms have been found to lie between exon 18 and exon 21. The most common mutations are in-frame deletions around the LREA motif of amino acid (leucine, arginine, glutamic acid, and alanine) sequences from 747 to 750, 9–24 base pairs in exon 19, and the L858R point mutation in exon 21, which occurs in 45% and 40% of cases, respectively. Together, the axon 19 and 21 mutations account for 85%–90% of all EGFRms.6
Metastatic lung cancer patients with activating EGFRm receive first-line therapy with epidermal growth factor receptor (EGFR) TKIs and generally experience an objective response rate (ORR) of ~70%–80% and a median progression-free survival (PFS) of 10–12 months.6,7 First-line TKI therapy provides a median PFS of 14.6 months and 9.7 months in patients with exon 19 deletions5 and L858R mutation, respectively.6,8
Till date, there exist three generations of TKIs. Erlotinib and gefitinib are the first-generation agents; afatinib, dacomitinib, and neratinib are the second-generation agents; and osimertinib, rociletinib, HM61713, and ASP8273 are the recently developed third-generation agents. The latter two are still in the development phase.
Gefitinib was the first EGFR TKI to be available. It was introduced in Japan in 2002 and then in the USA in 2003. Initial Phase II studies had shown objective response rate between 12% and 18% with median survival between 7 months and 8 months.9 This drug, which was restricted earlier in the USA, was reintroduced in the year 2015, after a Phase IV study demonstrating an ORR of 70%, a median PFS of 9.7 months, and a median OS of 19 months.10 Erlotinib was approved in 2004 for locally advanced and metastatic disease after the failure of at least one prior chemotherapy. In 2010, it received approval as maintenance therapy without disease progression after four cycles of platinum-based chemotherapy.6,8 In 2013, it was approved as first line in the metastatic setting. Based on LUX-Lung 3 and LUX-Lung 6 trials, the Food & Drug Administration approved afatinib as first-line treatment for metastatic EGFRm NSCLC in 2013 (Table 1).11,12
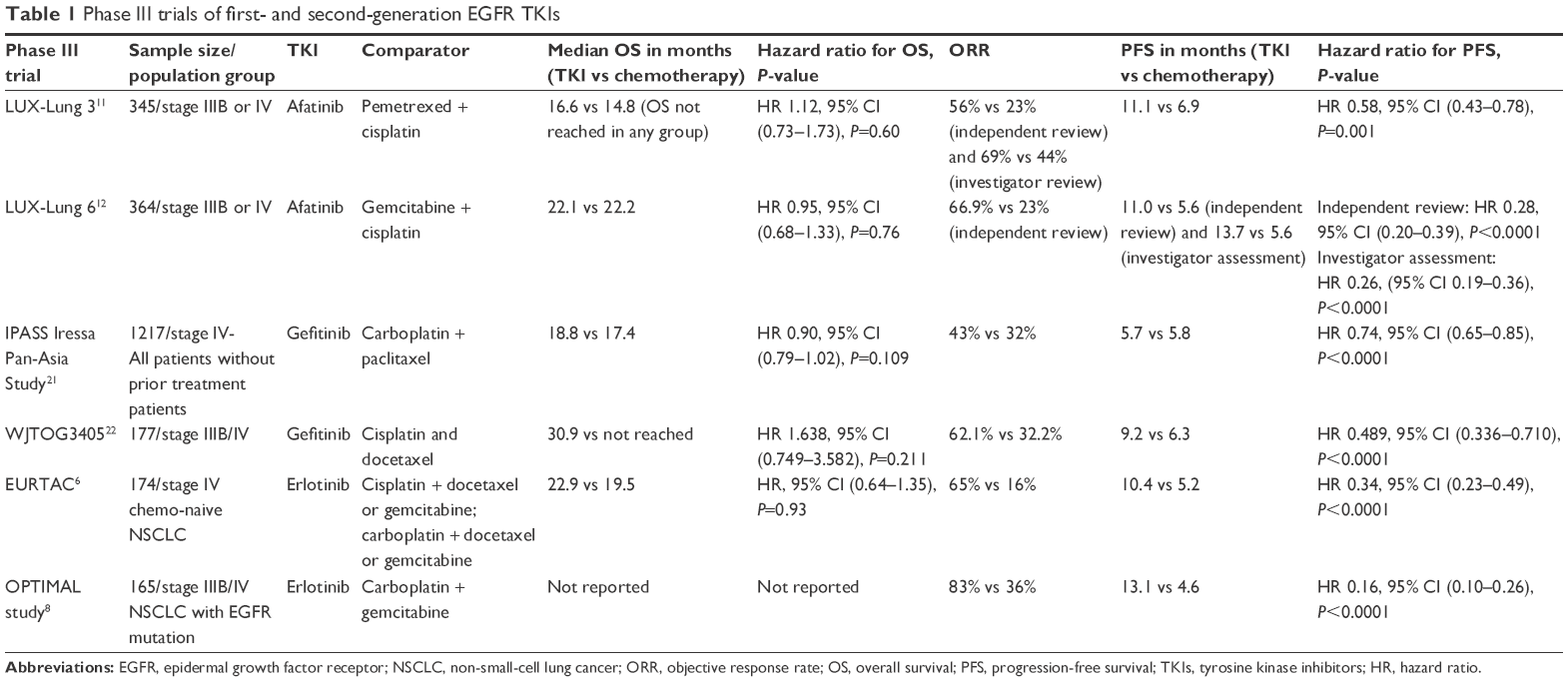 | Table 1 Phase III trials of first- and second-generation EGFR TKIs |
Resistance to TKI therapy can occur as secondary mutations in the EGFR gene, acquired mutations in other oncogenic genes, upregulation of signaling pathways, amplification of EGFR, or histological transformation to small-cell lung cancer. KRAS and ALK rearrangements, mutation with exon 20 insertion, are among the causes for resistance to TKI.13 Other rare and less studied mutations include exon 18 point mutations, exon 19 insertions, exon 21 L861Q, and exon 18 (G719X).5,13
Gatekeeper mutation in the EGFR kinase domain (EGFR T790M) of exon 20 accounts for 51%–68% of cases and is the most common resistance mechanism to first- and second-generation TKIs,13 followed by human epidermal growth factor receptor 2 (HER2) gene amplification (12%–15%), MET gene amplification (5%–11%), transformation to small-cell carcinoma (5%), phosphatidylinositide 3-kinase A (PIK3A) gene mutation (1%), or activating mutations in RAS or BRAF.14–17
T790M mutation leads to an enhanced affinity for adenosine triphosphate, thereby reducing the ability of reversible EGFR TKIs to bind to the tyrosine kinase domain of EGFR.14 Threonine amino acid replaces methionine at the T790M position of exon 20 and causes steric hindrance to bind the reversible TKIs and increases the affinity for ATP. This increases phosphorylation and reduce the potency of TKIs.14,18 Extracellular signal-regulated kinase (ERK) activation (via MEK1 amplification or mutation) and downstream inhibitors of this pathway are other resistant pathways detected on progression along with RET rearrangement.
Besides third-generation EGFR TKIs, several strategies are in clinical evaluation for reversal of acquired resistance to first- and second-generation EGFR TKIs. Second-generation EGFR TKIs such as afatinib, dacomitinib, and neratinib have been found to inhibit T790M in vitro, but the required doses are significantly higher in vivo, which limits their use due to unacceptable toxicity.19 Another strategy focuses on dual inhibition of EGFR.20 The combination of afatinib with cetuximab in a Phase II trial resulted in a response rate of 30% and a median PFS of 4.7 months in heavily pretreated patients.20 The clinical implication may be limited by severe gastrointestinal and skin toxicities. Furthermore, the combination of erlotinib and bevacizumab resulted in good outcome in the first-line treatment of patients with T790M-positive NSCLC in the BELIEF Phase II trial.21 The 1-year PFS rate was 72% without any unexpected toxicities.
Third-generation EGFR TKIs
Therapeutic approach to disease progressive on first- and second-generation TKIs depends on the severity of symptoms and the location of progression. National Comprehensive Cancer Network (NCCN) panel recommends to continue the same TKI with local treatment if there is local progression and to add chemotherapy to TKI or switch to third-generation TKI in case T790M mutation.22 Restarting the same TKI with or without everolimus was not beneficial and not recommended.23
Third-generation EGFR TKIs are more potent against T790M mutants, with higher selectivity for them over wild-type (WT) EGFR. While many such TKIs are being evaluated in preclinical and early-phase studies, such as HM61713 (BI 1482694),24 ASP8273,25 EGF816,26 and PF-06747775,27 two of these covalent EGFR inhibitors including CO-1686 (rociletinib) and AZD9291 (osimertinib) have made it through Phase I and II trials. Both drugs contain a distinctive aminopyrimidine scaffold that helps to avoid the steric interference with the mutant protein.28 Of these, osimertinib is the only agent currently approved for clinical use in the USA and Europe.
Rociletinib
Rociletinib (CO-1686; Clovis Oncology, Boulder, CO, USA) is an oral, covalent inhibitor of EGFRms. Like other third-generation EGFR TKIs, rociletinib has minimal activity against WT EGFR. It does not affect exon 20 insertions but inhibits exon 19 deletions, L858R, and T790M mutants as was evident in preclinical studies that confirmed its activity against EGFRm-positive tumors.29
Efficacy and dosage of rociletinib were studied in a Phase I/II study as second-line treatment in EGFR-mutated NSCLC.30 Doses of 500 mg, 625 mg, and 750 mg twice daily were used, with no maximum tolerated dose (MTD) identified after enrolling 130 patients. The ORR was 59% in patients with T790M-positive disease, and the ORR was 29% in patients with T790M-negative disease. The median age was 60 years; females comprised 77% of the patients, and only 15% of the patients were Asian. However, in a subsequent pooled TIGER-X phase1/2 and TIGER-2 analysis, the ORR with rociletinib (500–750 mg twice daily) among 325 patients with EGFR T790M-positive metastatic NSCLC who progressed on at least one EGFR inhibitor was lower at 30.2% (95% CI, 25.2–35.5).31 The manufacturer has terminated enrollment in all ongoing rociletinib studies, including the Phase III TIGER-3 trial (a Phase III trial, patients with EGFRm NSCLC who progressed on platinum-based regimen and one previous EGFR TKI were treated with either rociletinib or single-agent chemotherapy), and has withdrawn its application for regulatory approval in the European Union.
Osimertinib
Osimertinib (monoanilinopyrimidine AZD9291) is an irreversible TKI that targets T790M-resistant mutations as well as the sensitizing forms of the EGFR tyrosine kinase with selectivity over the WT form of the receptor. Osimertinib binds covalently to cysteine-797 residue in ATP-binding site, as confirmed by mass spectrometry of chymotrypsin digestion.32
Preclinical data of osimertinib
EGFR recombinant enzyme assay showed that AZD9291 is 200 times more potent against L858R/T790M than WT EGFR. Products of AZD9291 metabolism are mainly two products, AZ5104 and AZ7550. Biochemical assays in murine models show that AZ7550 has similar profile to the parent molecule, while AZ5104 has more potency against both mutant and WT EGFR.28 AZD9291 led to tumor shrinkage and resolution in mutant EGFR xenograft models after 14 days of 2.5 mg/kg/day dose.28 AZD9291 showed activity in two mouse tumor models (EGFRL858R and EGFRL858R/T790M) with lung adenocarcinoma, compared to afatinib, which was active on EGFRL858R only, and a control, which did not show activity in either type.28
Osimertinib in Phase I/II trials
Phases I and II AURA trial tested osimertinib as second line in patients with advanced lung cancer who progressed on EGFR TKI.33 The dose-escalating group included 31 patients using doses from 20 mg to 240 mg a day, and had no dose-limiting toxicities. An additional 222 patients were included in the expansion group. In this trial, 31% were men. Asian and Caucasian patients were 60% and 27%, respectively. The AURA2 Phase II trial abstract was presented at the 16th World Conference on Lung Cancer.34 In this trial, 70% of the population were females, 63% were Asian, and 76% were nonsmokers. Osimertinib was used as second line after NSCLC progression on frontline EGFR TKI.
The objective response rate (partial response [PR] and complete response [CR]) was 51%–71%. Stable disease and disease control (which included CR, PR, or stable disease) were achieved in 33% and 84%, respectively. Disease control rate in EGFR T790M-positive group was 92%–95% with a PFS of 8.6–9.6 months, while patients with negative EGFR T790M had a PFS of 2.8 months and a response rate of 21%. Response rate was similar among Asian and non-Asian patients. Response rate and PFS from AURA I–II and AURA2 trials are summarized in Table 2.
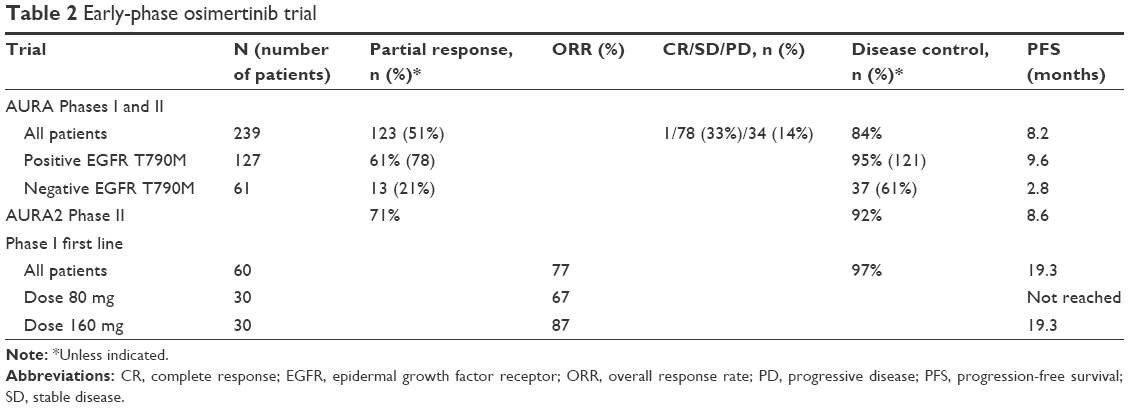 | Table 2 Early-phase osimertinib trial |
Grade III or higher side effects were observed in 32% of patients. Gastrointestinal symptoms were the most common side effects (diarrhea 47%, nausea 22%, and decreased appetite 21%), followed by dermatologic side effects (rash 40%, dry skin, and pruritus). Dose reduction and drug discontinuation due to side effects happened in 7% and 6%, respectively. Pneumonitis-like disease was observed in 2% of patients; all except one resolved after discontinuation of the drug. Fatal events were reported in 2.7% of patients, one of which (pneumonia) was reported as being possibly drug-related. Hyperglycemia and QT prolongation were seen in 2% and 4%, respectively, but they did not result in dose reduction.
FDA approval of osimertinib
On November 13, 2015, the FDA approved osimertinib for patients with (T790M) positive NSCLC whose disease had progressed on other EGFR TKIs. The European Commission approval was received on February 2, 2016. Based on FDA approval, the presence of the EGFR T790M mutation should be confirmed before starting therapy with osimertinib. The recommended dose is 80 mg, taken daily by mouth with or without food. Missed doses of osimertinib should not be made up.35 Osimertinib is available in two dosage strengths, including 40 mg and 80 mg tablets. Dose selection was based on pharmacokinetics analyses showing that the 80 mg dose ensured exposure levels greater than that observed for the 20 mg or 40 mg dose, which had also demonstrated clinical activity in the AURA Phase I study. The 80 mg dose provided substantial clinical efficacy and was associated with fewer dose reductions, lower incidence of skin disorders, nail effects, and diarrhea compared with 160 mg and 240 mg doses, which appeared unlikely to provide additional efficacy.36
NCCN guidelines to use osimertinib in EGFR-positive NSCLC22
On November 6, 2015, based upon review of the AURA and AURA2 data, NCCN panel consensus was to add osimertinib as a category 2A recommendation for the following indications: symptomatic progression with isolated systemic metastasis; symptomatic progression and multiple systemic metastasis; progression on subsequent therapy; asymptomatic and symptomatic progression, and brain metastases.
Ongoing trials using osimertinib
Based on Phase II trial results, osimertinib is being evaluated in multiple ongoing trials. Osimertinib is being evaluated as first-line treatment for patients with locally advanced or metastatic EGFRm NSCLC in a Phase I expansion cohort trial.37 Results were presented in abstract form in the Journal of Thoracic Oncology. A total of 80 mg and 160 mg daily doses were used. Five out of 60 patients were EGFR T790M positive. The ORR was 77% (67% at 80 mg dose and 87% at 160 mg dose). Overall PFS was 19.3 months. Dose reduction was needed in 10% and 47% of patients on 80 mg and 160 mg doses, respectively. Side effects were more prominent at 160 mg dose compared with 80 mg dose. Most common adverse events were diarrhea, stomatitis, and paronychia. Another ongoing Phase III trial compares gefitinib or erlotinib with or without osimertinib in EGFRm NSCLC.27 Transgenic models with EGFRm/T790M resistant to AZD9291 showed response after adding an MEK inhibitor such as selumetinib;38 thus, this combination is being tested in clinical trials as well. More combinations are under study, like AZD9291 with antibody to EGFR, such as necitumumab, navitoclax, which inhibits Bcl-2, or AZD6094, which is an MET inhibitor.27 Many other trials are summarized in Table 3 with their current accrual status.
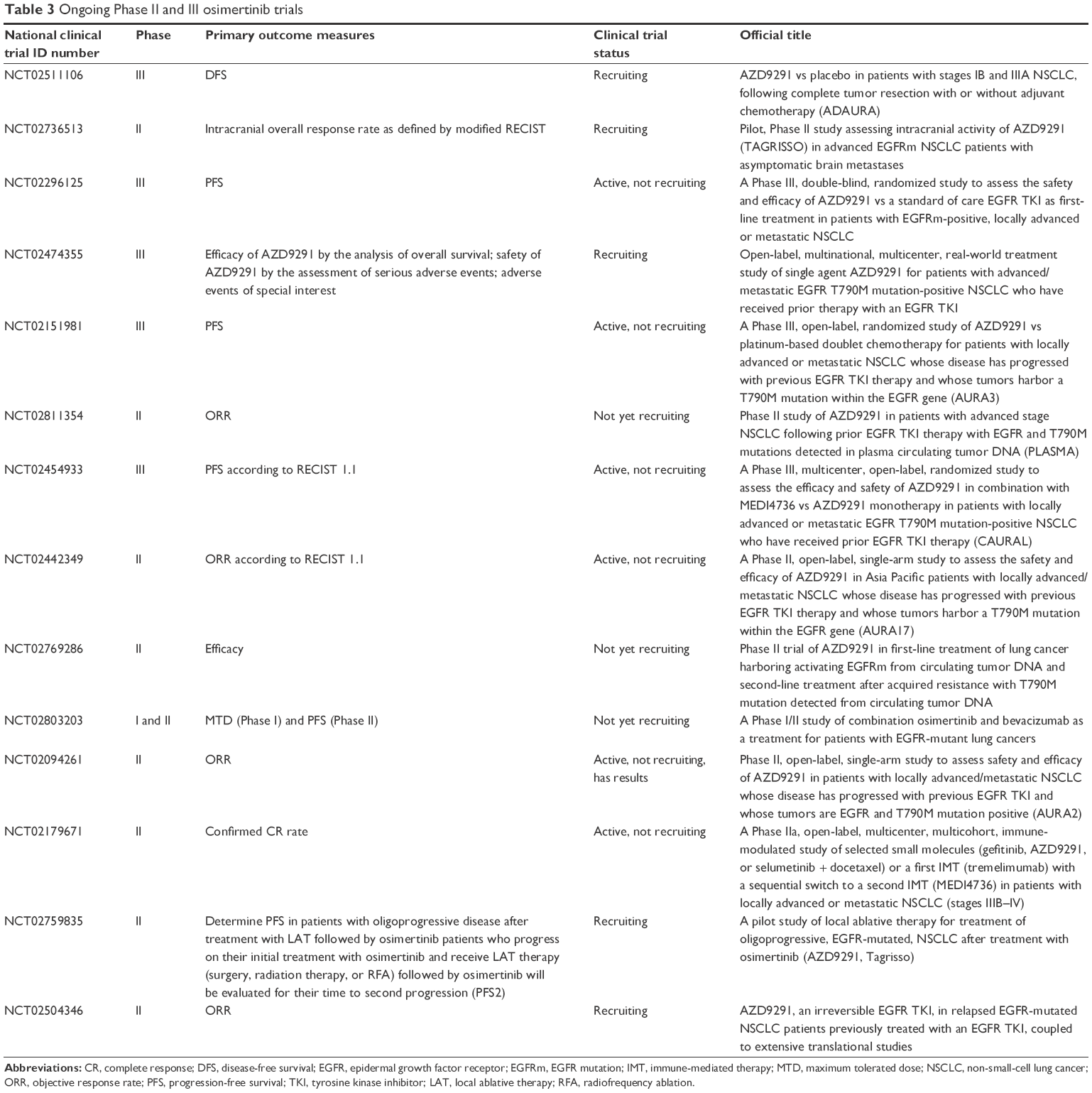 | Table 3 Ongoing Phase II and III osimertinib trials |
Osimertinib in EGFR-positive NSCLC with central nervous system (CNS) metastasis
Despite the fact that both third-generation EGFR TKIs target T790M mutant EGFR, the mechanism of action of rociletinib and osimertinib may be different. Sequist et al39 reported a case series of nine patients who progressed on rociletinib in the TIGER-X Phase I/II trial and then started on osimertinib in the AURA Phase I/II trial. Seven of them responded to osimertinib: three patients with PR and four patients with stable disease. Interestingly, three patients who developed CNS metastases on rociletinib responded to osimertinib. None of these CNS lesions underwent radiation. Two additional cases have been reported showing CNS metastasis response to osimertinib after progression on erlotinib or gefitinib.40 Another case report showed an improvement of brain lesions on osimertinib in EGFR T790M-positive adenocarcinoma of the lung with brain metastasis, which was refractory to radiation.41
The results of BLOOM trial (Phase I) were presented at the American Society of Clinical Oncology (ASCO) annual meeting. In this study, EGFRm-positive NSCLC patients with leptomeningeal (LM) disease had an improvement in MRI signal intensity on osimertinib.42 A total of 21 patients were treated with 160 mg once daily osimertinib. Seven of them had objective improvement in imaging: five patients had improved symptoms and two patients cleared their cerebrospinal fluid from tumor cells. None of those patients underwent radiotherapy treatment or received intrathecal chemotherapy. There is preclinical evidence that osimertinib crosses the blood brain barrier more efficiently that other TKIs.43
Diagnosis of EGFRm and liquid biopsies
Identification of mutations in the gene encoding for EGFR requires histological or cytological samples. However, it is not always feasible to get tumor samples. Frequently, tumor material is not adequate for molecular analyses44 and decalcification procedures in bone biopsies interfere with molecular testing and results.45 Thus, there was an urgent need to develop more accessible and less invasive methods for molecular alteration identification. A simple, validated, minimally invasive, blood/serum-based assay may also serve as a method to assess the response to EGFR TKI treatment.
Patients with EGFRm were found to have DNA fragments carrying the tumor-specific sequence (circulating cell-free tumor DNA [cftDNA]) in variable levels among their total plasma circulating DNA.46 Detecting these cftDNA showed a high specificity to EGFR gene mutations. The analysis of cftDNA, defined as “liquid biopsy”, could be potentially repeated every time via simple blood draw. To validate cftDNA analysis for the detection of EGFRms, Kimura et al47 compared results from cftDNA with results of tissue biopsies from the tumor. Report suggested a 92.9% concordance between serum and tissue.
Two meta-analyses of studies comparing tissues and plasma samples were published. They assessed the yield of cftDNA for EGFRms.48,49 Results showed a pooled sensitivity of 0.620–0.674 and a pooled specificity of 0.935–0.959. The area under the curve (AUC) resulted in high diagnostic accuracy (0.9–0.93). The results were more sensitive in poorly differentiated adenocarcinoma and in patients with advanced disease. In other words, the more aggressive the tumor and the bulkier the disease, the higher the levels of cftDNA and the higher the sensitivity to EGFRm.50 The optimal time of blood collection and the effect of chemotherapy on these results are to be defined.51
Therapeutic management of patients with EGFRm NSCLC after the progression on first- or second-generation TKIs makes it imperative to identify the molecular mechanisms of acquired resistance. Biopsy used to be necessary to do this molecular study, which could be invasive and confounded by intra tumor heterogeneity.52–54 Hence, cftDNA analysis becomes more interesting and more important. Furthermore, multiple studies demonstrated that an increase in levels of EGFR activating mutation after the initiation of an EGFR TKI is a relatively early phenomenon of T790M appearance. These changes might be detected several weeks before the progression is visible radiographically.
Resistance to third-generation EGFR inhibitors
Eventually, disease progresses on third-generation EGFR TKI, representing further resistance mechanisms. C797S mutation is one of the most common mechanisms of resistance.55,56 The loss of the potential for covalent bond formation at position 797 by the missense mutation C797S is located within the kinase-binding site. This results in a markedly reduced cellular potency of this class of TKIs.57 This mutation usually arises after 6–17 months of treatment in T790M-positive patients.55,56
Some patients with previous T790M mutation acquire resistance without having the C797S mutation. In these cases, the mechanisms of this resistance still need to be identified.58 Novel agents are needed to overcome the C797S tertiary EGFRm.
Disclosure
The authors report no conflicts of interest in this work.
References
Cancer.org [homepage on the Internet]. Cancer Facts & Figures 2016. American Cancer Society; 2016. Available from: http://www.cancer.org/research/cancerfactsstatistics/cancerfactsfigures2016/. Accessed October 22, 2016. | ||
Miller KD, Siegel RL, Lin CC, et al. Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin. 2016;66(4):271–289. | ||
SEER 18 [homepage on the Internet]. Available from: 1.http://seer.cancer.gov/statfacts/. Accessed December 2, 2016. | ||
Midha A, Dearden S, McCormack R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: a systematic review and global map by ethnicity (mutMapII). Am J Cancer Res. 2015;5(9):2892. | ||
Shigematsu H, Lin L, Takahashi T, et al. Clinical and biological features associated with epidermal growth factor receptor gene mutations in lung cancers. J Natl Cancer Inst. 2005;97(5):339–346. | ||
Rosell R, Carcereny E, Gervais R, et al; Spanish Lung Cancer Group in collaboration with Groupe Franais de Pneumo-Cancrologie and Associazione Italiana Oncologia Toracica. Erlotinib versus standard chemotherapy as rst-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13(3):239–246. | ||
Langer CJ. Epidermal growth factor receptor inhibition in mutation-positive non–small-cell lung cancer: is afatinib better or simply newer? J Clin Oncol. 2013;31(27):3303–3306. | ||
Zhou C, Wu Y, Chen G, et al. Final overall survival results from a randomised, phase III study of erlotinib versus chemotherapy as first-line treatment of EGFR mutation-positive advanced non-small-cell lung cancer (OPTIMAL, CTONG-0802). Ann Oncol. 2015;26(9):1877–1883. | ||
Ando M, Okamoto I, Yamamoto N, et al. Predictive factors for interstitial lung disease, antitumor response, and survival in non–small-cell lung cancer patients treated with gefitinib. J Clin Oncol. 2006;24(16):2549–2556. | ||
Douillard J, Ostoros G, Cobo M, et al. First-line gefitinib in Caucasian EGFR mutation-positive NSCLC patients: a phase-IV, open-label, single-arm study. Br J Cancer. 2014;110(1):55–62. | ||
Sequist LV, Yang JC-H, Yamamoto N, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol. 2013;31(27):3327–3334. | ||
Wu Y-L, Zhou C, Hu C-P, et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-lung 6): an open-label, randomised phase 3 trial. Lancet Oncol. 2014;15(2):213–222. | ||
Oxnard GR, Arcila ME, Sima CS, et al. Acquired resistance to EGFR tyrosine kinase inhibitors in EGFR-mutant lung cancer: distinct natural history of patients with tumors harboring the T790M mutation. Clin Cancer Res. 2011;17(6):1616–1622. | ||
Yun C-H, Mengwasser KE, Toms AV, et al. The T790M mutation in EGFR kinase causes drug resistance by increasing the affinity for ATP. Proc Natl Acad Sci U S A. 2008;105(6):2070–2075. | ||
Helena AY, Arcila ME, Rekhtman N, et al. Analysis of tumor specimens at the time of acquired resistance to EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers. Clin Cancer Res. 2013;19(8):2240–2247. | ||
Niederst MJ, Sequist LV, Poirier JT, et al. RB loss in resistant EGFR mutant lung adenocarcinomas that transform to small-cell lung cancer. Nat Commun. 2015;6:6377. | ||
Riely GJ, Marks J, Pao W. KRAS mutations in non–small cell lung cancer. Proc Am Thorac Soc. 2009;6(2):201–205. | ||
Kuiper J, Heideman D, Thunnissen E, et al. Incidence of T790M mutation in (sequential) rebiopsies in EGFR-mutated NSCLC-patients. Lung Cancer. 2014;85(1):19–24. | ||
Zou HY, Friboulet L, Kodack DP, et al. PF-06463922, an ALK/ROS1 inhibitor, overcomes resistance to first and second generation ALK inhibitors in preclinical models. Cancer Cell. 2015;28(1):70–81. | ||
Janjigian YY, Smit EF, Groen HJ, et al. Dual inhibition of EGFR with afatinib and cetuximab in kinase inhibitor–resistant EGFR-mutant lung cancer with and without T790M mutations. Cancer Discov. 2014;4(9):1036–1045. | ||
Seto T, Kato T, Nishio M, et al. Erlotinib alone or with bevacizumab as first-line therapy in patients with advanced non-squamous non-small-cell lung cancer harbouring EGFR mutations (JO25567): an open-label, randomised, multicentre, phase 2 study. Lancet Oncol. 2014;15(11):1236–1244. | ||
NCCN.org [homepage on the Internet]. National Comprehensive Cancer Network. Fort Washington, PA: 2016. Available from: http://www.nccn.org/. Accessed October 29, 2016. | ||
Riely GJ, Kris MG, Zhao B, et al. Prospective assessment of discontinuation and reinitiation of erlotinib or gefitinib in patients with acquired resistance to erlotinib or gefitinib followed by the addition of everolimus. Clin Cancer Res. 2007;13(17):5150–5155. | ||
Park K, Han J-Y, Kim D-W, et al. 190TiP: ELUXA 1: phase II study of BI 1482694 (HM61713) in patients (pts) with T790M-positive non-small cell lung cancer (NSCLC) after treatment with an epidermal growth factor receptor tyrosine kinase inhibitor (EGFR TKI). J Thorac Oncol. 2016;11(4):S139. | ||
Yu HA, Spira AI, Horn L, et al. Antitumor activity of ASP8273 300 mg in subjects with EGFR mutation-positive non-small cell lung cancer: interim results from an ongoing phase 1 study. Paper presented at: ASCO Annual Meeting Proceedings. 2016; Chicago, Illinois, USA. | ||
Jia Y, Juarez J, Li J, et al. EGF816 exerts anticancer effects in non–small cell lung cancer by irreversibly and selectively targeting primary and acquired activating mutations in the EGF receptor. Cancer Res. 2016; 76(6):1591–1602. | ||
Wang S, Cang S, Liu D. Third-generation inhibitors targeting EGFR T790M mutation in advanced non-small cell lung cancer. J Hematol Oncol. 2016;9:34. | ||
Cross DA, Ashton SE, Ghiorghiu S, et al. AZD9291, an irreversible EGFR TKI, overcomes T790M-mediated resistance to EGFR inhibitors in lung cancer. Cancer Discov. 2014;4(9):1046–1061. | ||
Walter AO, Sjin RTT, Haringsma HJ, et al. Discovery of a mutant-selective covalent inhibitor of EGFR that overcomes T790M-mediated resistance in NSCLC. Cancer Discov. 2013;3(12):1404–1415. | ||
Sequist LV, Soria J-C, Goldman JW, et al. Rociletinib in EGFR-mutated non–small-cell lung cancer. N Engl J Med. 2015;372(18):1700–1709. | ||
FDA. FDA Briefing Document Oncologic Drugs Advisory Committee Meeting NDA 208542 Rociletinib. FDA; Boulder, Colorado: 2016. | ||
Ward RA, Anderton MJ, Ashton S, et al. Structure-and reactivity-based development of covalent inhibitors of the activating and gatekeeper mutant forms of the epidermal growth factor receptor (EGFR). J Med Chem. 2013;56(17):7025–7048. | ||
Jänne PA, Yang JC-H, Kim D-W, et al. AZD9291 in EGFR inhibitor–resistant non–small-cell lung cancer. N Engl J Med. 2015;372(18):1689–1699. | ||
Mitsudomi T, Tsai C-M, Shepherd F, et al. AZD9291 in pre-treated T790M positive advanced NSCLC: AURA2 phase II study. J Thorac Oncol. 2015;10(9):S320. | ||
Tagrisso (osimertinib) tablet [prescribing information]. Wilmington: DAPN; 2015. | ||
Yver A. Osimertinib (AZD9291) – a science-driven, collaborative approach to rapid drug design and development. Ann Oncol. 2016;27(6):1165–1170. | ||
Ramalingam S, Yang J-H, Lee C, et al. LBA1_PR: osimertinib as first-line treatment for EGFR mutation-positive advanced NSCLC: updated efficacy and safety results from two phase I expansion cohorts. J Thorac Oncol. 2016;11(4):S152. | ||
Eberlein CA, Stetson D, Markovets AA, et al. Acquired resistance to the mutant-selective EGFR inhibitor AZD9291 is associated with increased dependence on RAS signaling in preclinical models. Cancer Res. 2015;75(12):2489–2500. | ||
Sequist LV, Piotrowska Z, Niederst MJ, et al. Osimertinib responses after disease progression in patients who had been receiving rociletinib. JAMA Oncol. 2016;2(4):541–543. | ||
Ricciuti B, Chiari R, Chiarini P, et al. Osimertinib (AZD9291) and CNS response in two radiotherapy-naïve patients with EGFR-mutant and T790M-positive advanced non-small cell lung cancer. Clin Drug Investig. 2016;36(8):683–686. | ||
Reichegger H, Jochum W, Förbs D, Hader C, Früh M. Rapid intracranial response to osimertinib in a patient with epidermal growth factor receptor T790M-positive adenocarcinoma of the lung. Oncol Res Treat. 2016;39(7–8):461–463. | ||
Yang JCH. Osimertinib activity in patients (pts) with leptomeningeal (LM) disease from non-small cell lung cancer (NSCLC): updated results from BLOOM, a phase I study. Abstract 9002 [Oral Presentation] presented at The annual meeting of the American Society of Clinical Oncology; 3–7 June 2016. Chicago: 2016:1. | ||
Ballard P, Yang P, Cross D, et al. Preclinical activity of AZD9291 in EGFR-mutant NSCLC brain metastases. Paper presented at: ESMO 2014. 27 September; 2014; Madrid, Spain. | ||
Vanderlaan PA, Yamaguchi N, Folch E, et al. Success and failure rates of tumor genotyping techniques in routine pathological samples with non-small-cell lung cancer. Lung Cancer. 2014;84(1):39–44. | ||
Singh VM, Salunga RC, Huang VJ, et al. Analysis of the effect of various decalcification agents on the quantity and quality of nucleic acid (DNA and RNA) recovered from bone biopsies. Ann Diagn Pathol. 2013;17(4):322–326. | ||
Bettegowda C, Sausen M, Leary RJ, et al. Detection of circulating tumor DNA in early-and late-stage human malignancies. Sci Transl Med. 2014;6(224):224ra24–224ra24. | ||
Kimura H, Suminoe M, Kasahara K, et al. Evaluation of epidermal growth factor receptor mutation status in serum DNA as a predictor of response to gefitinib (IRESSA). Br J Cancer. 2007;97(6):778–784. | ||
Luo J, Shen L, Zheng D. Diagnostic value of circulating free DNA for the detection of EGFR mutation status in NSCLC: a systematic review and meta-analysis. Sci Rep. 2014;4:6269. | ||
Qiu M, Wang J, Xu Y, et al. Circulating tumor DNA is effective for the detection of EGFR mutation in non–small cell lung cancer: a meta-analysis. Cancer Epidemiol Biomarkers Prev. 2015;24(1):206–212. | ||
Bordi P, Del Re M, Danesi R, Tiseo M. Circulating DNA in diagnosis and monitoring EGFR gene mutations in advanced non-small cell lung cancer. Transl Lung Cancer Res. 2015;4(5):584. | ||
Bai H, Wang Z, Chen K, et al. Influence of chemotherapy on EGFR mutation status among patients with non–small-cell lung cancer. J Clin Oncol. 2012;30(25):3077–3083. | ||
Diaz LA, Bardelli A. Liquid biopsies: genotyping circulating tumor DNA. J Clin Oncol. 2014;32(6):579–586. | ||
Gerlinger M, Rowan AJ, Horswell S, et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N Engl J Med. 2012;366(10):883–892. | ||
Vogelstein B, Papadopoulos N, Velculescu VE, Zhou S, Diaz LA Jr, Kinzler KW. Cancer genome landscapes. Science. 2013;339(6127):1546–1558. | ||
Niederst MJ, Hu H, Mulvey HE, et al. The allelic context of the C797S mutation acquired upon treatment with third-generation EGFR inhibitors impacts sensitivity to subsequent treatment strategies. Clin Cancer Res. 2015;21(17):3924–3933. | ||
Song H-N, Jung KS, Yoo KH, et al. Acquired C797S mutation upon treatment with a T790M-specific third-generation EGFR inhibitor (HM61713) in non–small cell lung cancer. J Thorac Oncol. 2016;11(4):e45–e47. | ||
Schwartz PA, Kuzmic P, Solowiej J, et al. Covalent EGFR inhibitor analysis reveals importance of reversible interactions to potency and mechanisms of drug resistance. Proc Natl Acad Sci U S A. 2014;111(1):173–178. | ||
Thress KS, Paweletz CP, Felip E, et al. Acquired EGFR C797S mutation mediates resistance to AZD9291 in non-small cell lung cancer harboring EGFR T790M. Nat Med. 2015;21(6):560–562. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.