Back to Journals » Risk Management and Healthcare Policy » Volume 18
Epidemiology, Risk Factors, and Predictive Modelling of Post-Traumatic Sepsis: A Retrospective Cohort Study
Authors Fu X, Wang ZY, Qin YJ, Cao XX, Deng WS, Dai C, Hu DZ, Dong SM
Received 22 May 2025
Accepted for publication 27 September 2025
Published 23 October 2025 Volume 2025:18 Pages 3449—3464
DOI https://doi.org/10.2147/RMHP.S542208
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Xue Fu,1,* Zhen-Yi Wang,2,* Yan-Jun Qin,1 Xue-Xia Cao,1 Wang-Sheng Deng,2 Chen Dai,1 De-Zheng Hu,1 Shi-Min Dong1
1Department of Emergency Medicine, Hebei Medical University Third Hospital, Shijiazhuang, Hebei, 050011, People’s Republic of China; 2Department of Emergency Medicine, Shenzhen Longhua District People’s Hospital, Shenzhen, Guangdong, 518000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shi-Min Dong, Department of Emergency Medicine, Hebei Medical University Third Hospital, 139 Ziqiang Road, Shijiazhuang, Hebei, 050011, People’s Republic of China, Tel +86031188602330, Email [email protected]
Objective: This study aimed to evaluate the distribution spectrum and epidemiological characteristics associated with post-traumatic sepsis and to identify associated risk factors.
Methods: This retrospective study analyzed data from 722 patients with traumatic injuries admitted to the Emergency Department of the Hebei Medical University Third Hospital between January 1, 2021, and November 30, 2023. Participants were categorized into two groups: those who developed sepsis and those who did not. Patients diagnosed with sepsis were further categorized into survival and non-survival subgroups. Patient demographics, injury characteristics, and clinical variables were collected. Sepsis occurrence was assessed within the first week post-injury. Multivariate logistic regression analysis was performed to identify independent risk factors for post-traumatic sepsis.
Results: Among 722 trauma patients, 189 developed sepsis. In the sepsis cohort, injuries were mainly from traffic accidents (54.5%), falls from heights (17.46%), crush injuries (13.76%), and falls/collisions (11.64%). In contrast, non-sepsis cases (n=533) were predominantly due to falls/collisions (43.15%) and traffic accidents (36.02%). Pulmonary infection was the leading site in both survivors (95.62%) and non-survivors (100%), with some patients presenting multiple infection sites. A predictive model for post-traumatic sepsis, incorporating 10 variables such as hospitalization length and injury site number, achieved excellent performance (AUROC 0.998). A sepsis mortality model, based on five variables including age and injury sites, also showed high accuracy (AUROC 0.969).
Conclusion: Traffic accidents were the primary cause of post-traumatic sepsis. Key risk factors included injury severity, CRP level, and hospitalization duration. Independent predictors of 28-day mortality included age, organ failure score, and vasoactive drug use.
Keywords: epidemiological characteristics, ISS, post-traumatic sepsis, predictive modelling, risk factor, receiver operating characteristic curve, ROC curve, SOFA score
Introduction
Trauma represents a significant global health challenge, particularly affecting individuals in young and middle adulthood. In the United States, trauma is the leading cause of mortality among individuals under 45 years of age, accounting for over half of all deaths within this demographic and resulting in an estimated annual economic burden of up to $600 billion.1 The severity of trauma lies in its association with high rates of disability, mortality, and disease burden. Despite advancements in medical technology and management, including early hemorrhage control, which has improved survival, approximately two-thirds of patients with severe trauma continue to succumb to secondary complications. Although the restoration of blood pressure is crucial, the subsequent trauma-induced systemic inflammatory response can result in functional impairment of multiple organs. This dysfunction may be exacerbated by concurrent infections, often resulting in adverse outcomes, including death.2
With the evolution of modern medicine, the management of patients with traumatic injuries has become increasingly systematic and standardized, contributing to improved survival rates in patients with severe trauma.3 Once stabilized, these patients are typically transferred to the intensive care unit for ongoing treatment. However, during this phase, they remain at risk for complications such as sepsis, septic shock, and multiorgan failure. In healthcare systems with advanced diagnostic capabilities and access to life -sustaining interventions, the incidence of direct trauma-related deaths has declined. However, the incidence of mortality related to trauma-associated complications remains substantial, with post-traumatic sepsis emerging as one of the most prevalent and critical complications.4–6
Post-traumatic sepsis constitutes a leading cause of death in individuals with traumatic injuries.7 The incidence rate of post - traumatic sepsis can reach up to 10% among patients with severe trauma, and its mortality rate cannot be ignored. According to multiple studies, the case - fatality rate of trauma - related sepsis is close to 30%.8 A retrospective analysis conducted by Wafaisade et al in Germany, involving 29,829 individuals with polytrauma reported that approximately 10% developed sepsis during hospitalization.6 The infection risk among trauma patients stems from the disruption of mechanical barriers, the invasion of external bacteria, local wound factors, and invasive diagnostic and therapeutic procedures. The pathogenesis of sepsis involves multiple factors, including wound contamination, invasive surgical procedures, massive blood transfusion, tissue ischemia - reperfusion, mechanical ventilation, and immune system disorders.9 The onset of post-traumatic sepsis exhibits considerable heterogeneity, and a uniform timeline for its occurrence has not been definitively established. The coexistence of trauma and sepsis gives rise to complex pathophysiological mechanisms, necessitating ongoing research focused on early identification and optimized therapeutic approaches. Several predictive tools have been proposed for sepsis risk assessment, such as the Sequential Organ Failure Assessment (SOFA) score, the quick SOFA (qSOFA), and other clinical prediction models. However, these tools were primarily designed for general sepsis populations and may have limited applicability to trauma-specific settings. Importantly, only a few models have been tailored to post-traumatic sepsis, and their predictive accuracy and external validation remain limited. Moreover, the incidence of trauma-related sepsis demonstrates substantial global variability, ranging from approximately [10.2%] in high-income countries to over [26.9%] in certain low- and middle- income regions.6,10 Such differences reflect disparities in trauma epidemiology, healthcare resources, and infection control practices, underscoring the need for context-specific data and predictive approaches.
Against this background, our study aimed to investigate the epidemiology and risk factors of post-traumatic sepsis in adult patients and to develop a predictive model that integrates demographic, clinical, laboratory, and interventional data. By addressing the limitations of existing tools, this work seeks to provide new insights into the early identification of high-risk trauma patients and contribute to improved prevention and management strategies.
Methods
Study Participants
Patients admitted to the Emergency Department of the Hebei Medical University Third Hospital between January 1, 2021, and November 30, 2023, were selected for inclusion in the study. A total of 722 patients met the eligibility criteria and were enrolled. According to the Sepsis 3.0 diagnostic criteria, patients who developed sepsis within one week following trauma were assigned to the sepsis group, while those who did not were categorized into the non-sepsis group. Among patients in the sepsis group, those who died within 28 days of the sepsis diagnosis were classified into the non-surviving group, while those who survived beyond this period were included in the surviving group.
This study was approved by the Ethics Committee of the Hebei Medical University Third Hospital (Approval No. W2022-044-1). All data were de-identified prior to analysis to protect patient confidentiality. As this was a retrospective study using existing medical records, the requirement for informed consent was waived in accordance with the Declaration of Helsinki and its amendments.
Inclusion Criteria
- Patients meeting the following criteria were included:
- Admission to the Emergency Department of the Hebei Medical University Third Hospital for trauma due to mechanical injury between January 1, 2021, and November 30, 2023.
- Aged between 18 and 75 years.
- No signs or suspicion of infection prior to trauma.
- Admitted within one week of injury.
Exclusion Criteria
Patients were excluded if they met any of the following:
- Aged below 18 or above 75 years.
- Evidence or suspicion of pre-trauma infection.
- Preexisting immune dysfunction (eg, malignancy, AIDS, tuberculosis, or recent immunotherapy).
- End-stage hepatic or renal failure.
- Incomplete clinical data (>20% missing).
Diagnostic Criteria
Sepsis was diagnosed in patients with confirmed or suspected infection if the SOFA score increased by ≥2 points from baseline.11
Definition of Infection
Infection types were categorized according to the International Sepsis Forum guidelines,12 including pulmonary, bloodstream, endocardial, abdominal, urinary, catheter-associated, and skin/soft tissue infections. Hospital-related complications were considered as potential contributors.
Collection of Indicators
- General Information: Age, sex, BMI, and comorbidities.
- Vital Signs (within 24 hours of admission): Temperature, respiratory rate, heart rate, systolic and diastolic blood pressure, and mean arterial pressure.
- Laboratory Tests (within 24 hours): Routine blood work, liver and kidney function, coagulation, blood gases, and inflammatory markers.
- Scoring Systems (within 24 hours): GCS, APACHE II, SOFA, and ISS scores.
- Trauma, Infection, and Organ Dysfunction During Hospitalization:
1) Injury sites (head/neck, face, chest, abdomen, limbs, body surface)
2) Infection sites (lung, abdomen, blood, urinary tract, nervous system, bone/soft tissue)
3) Organ dysfunction (respiratory, cardiac, hepatic, renal, circulatory)
4) Number of infections and organ failures
6. Treatment During Hospitalization: Surgery, mechanical ventilation, CRRT, anti-infective therapy, blood transfusion, vasoactive drugs, and invasive procedures.
Statistical Methods
Statistical analysis was performed using SPSS version 21.0. Continuous variables were expressed as medians with interquartile ranges [M (QL, QU)], and categorical variables as frequencies and percentages (%). The rank-sum test was used for continuous variables, and the chi-square test for categorical variables. Variables with P < 0.05 in univariate analysis were entered into multivariate logistic regression to develop predictive models. Model performance was evaluated using receiver operating characteristic (ROC) curves, and the area under the ROC curve (AUC) was calculated. We reported odds ratios (OR = exp(β)) with 95% confidence intervals (CIs) from logistic regression.
Missing values in key clinical predictors were addressed using multiple imputation by chained equations (MICE) under a missing-at-random assumption. Imputation models included all variables used in the multivariable analyses and clinically plausible auxiliary variables; the outcome was not imputed. Continuous variables were imputed using predictive mean matching, binary variables using logistic regression, and ordinal variables using proportional-odds models. If transformations were used, variables were imputed on the analysis scale with passive back-transformation. We generated m = 20 imputed datasets and combined estimates using Rubin’s rules. Pooled MI estimates are reported as the primary results.
This analysis represents model development. We did not perform internal resampling (eg, bootstrap or cross-validation) or external validation due to resource constraints. Therefore, discrimination is reported as the apparent AUC in the development dataset. Calibration and external transportability require assessment in future studies.
Results
Epidemiological Characteristics of Patients with Trauma and Risk Factors
Baseline Characteristics
Baseline demographic and clinical characteristics are summarized in Table 1. The cohort included 722 patients, 513 (71.05%) were male. The median age in the sepsis group was 55.5 years (interquartile range [IQR]: 46–65). The leading causes of trauma were [traffic accidents (40.86%), Collisions (34.90%), falls (12.33%)]. The overall incidence of post-traumatic sepsis was [26.18%]. Patients who developed sepsis tended to have more severe injuries compared with those without sepsis.
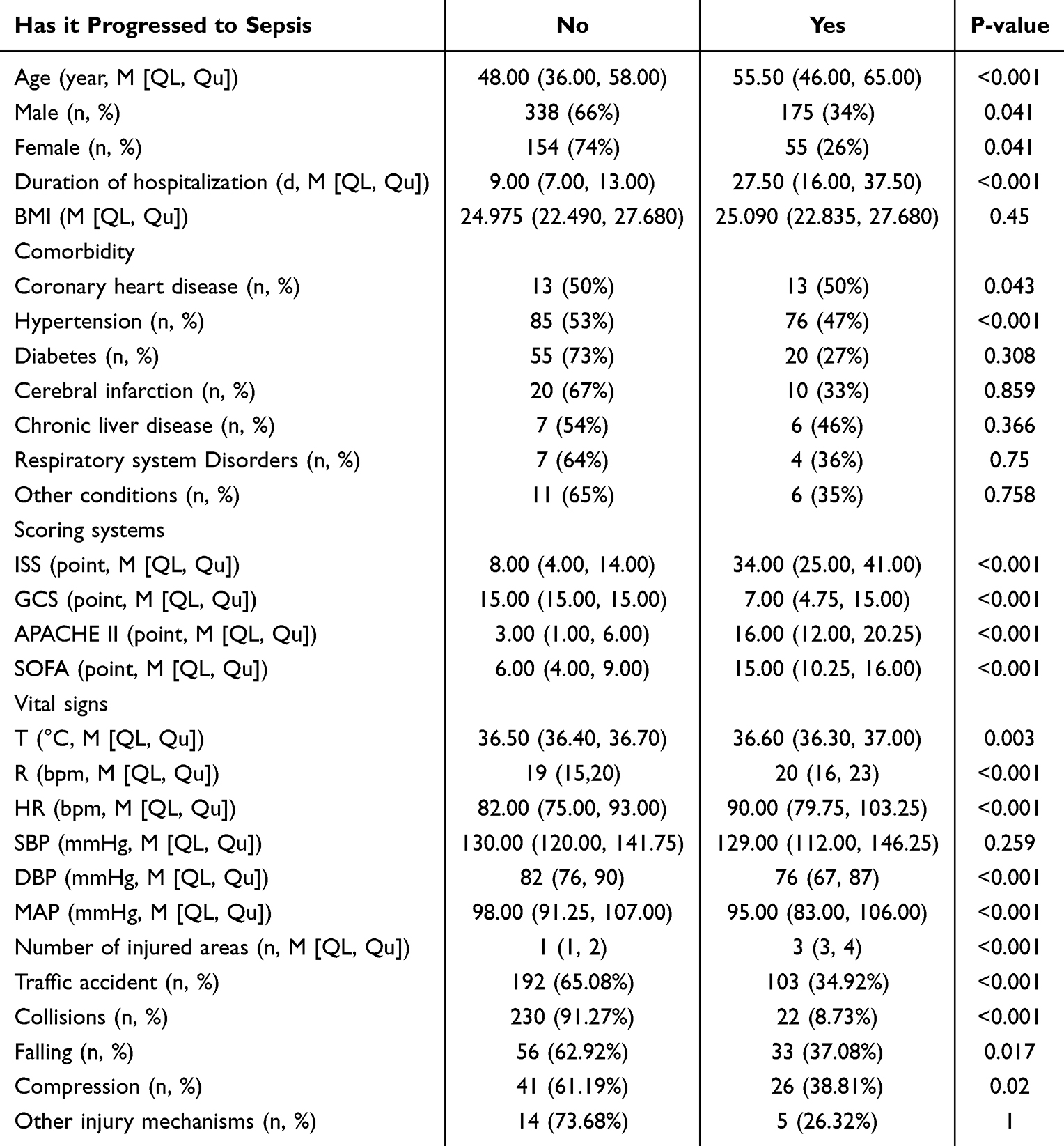 |
Table 1 Comparison of Baseline Demographic and Clinical Characteristics Between the Sepsis Group and the Non-Sepsis Group |
Laboratory and Interventional Data
Laboratory and interventional findings are presented in Table 2. Patients with sepsis exhibited significantly higher inflammatory markers (eg, [WBC, CRP]) and prolonged prothrombin time (PT) compared with non-septic patients. Invasive interventions, including [eg Emergency surgery, mechanical ventilation, blood transfusion], were more frequently performed in the sepsis group. These hospital-related complications contributed to the increased risk of infection during hospitalization.
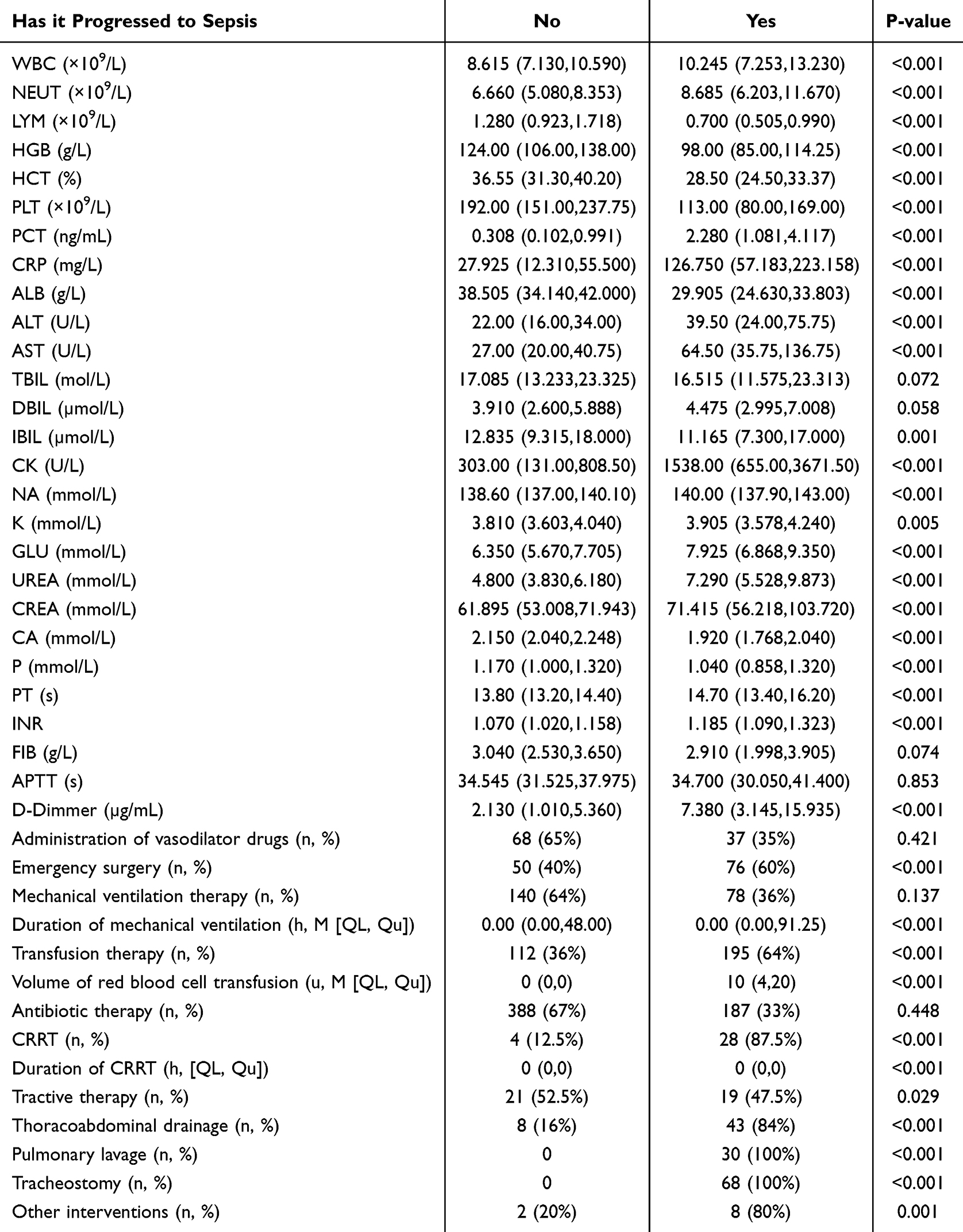 |
Table 2 Comparison of Laboratory and Interventional Findings Between the Sepsis Group and the Non-Sepsis Group |
Risk Factor Analysis
All effect estimates and inference reported below are pooled across the imputed datasets using Rubin’s rules. In univariate analysis, several variables were significantly associated with post-traumatic sepsis, including [length of hospitalization, number of injury sites, ISS, GCS, neutrophil count, CRP, creatine kinas, CRRT treatment, duration of CRRT, tracheotomy treatment]. After adjustment in multivariate logistic regression, [length of hospitalization, number of injury sites, ISS, GCS, NEUT, CRP, creatine kinase, Na, and duration of CRRT] remained independent predictors of sepsis (all P < 0.05), as presented in Table 3.
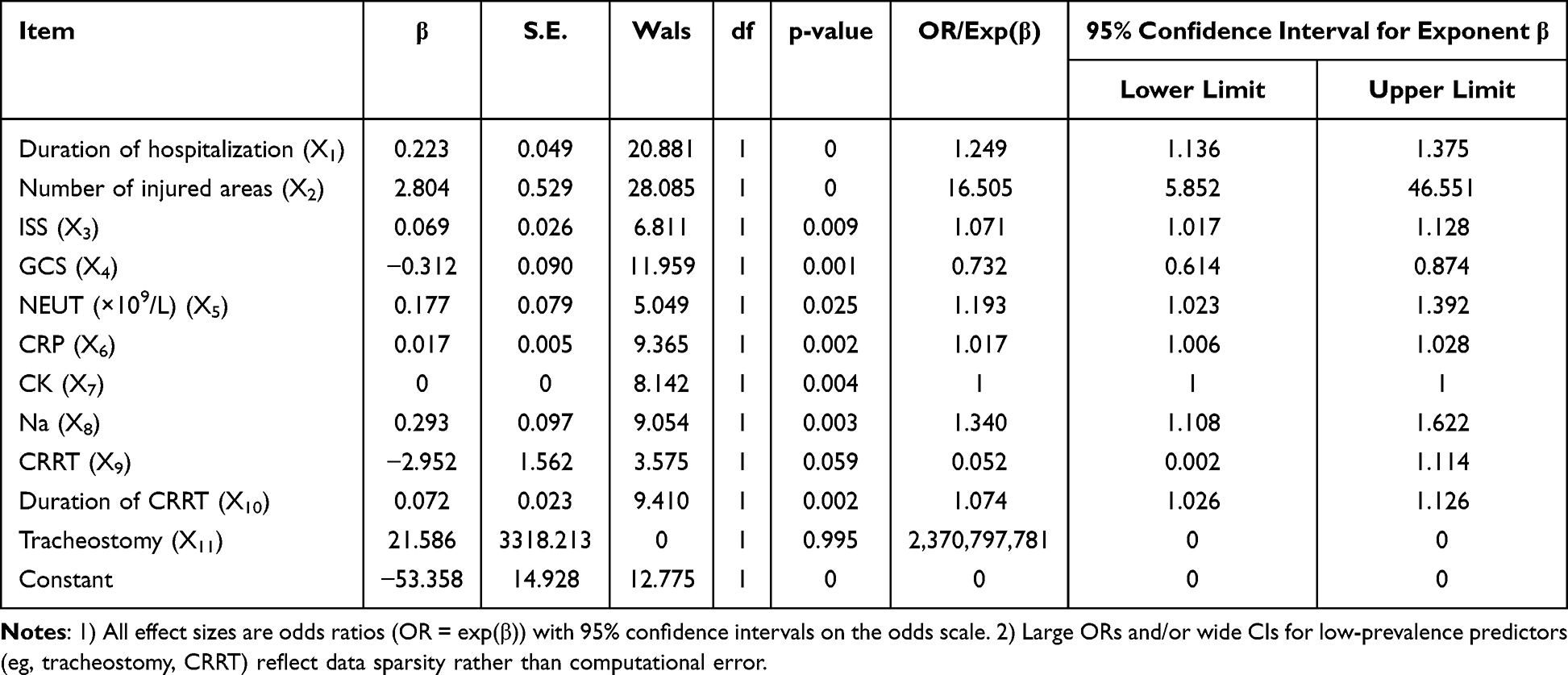 |
Table 3 Multivariate Logistic Regression Analysis of Risk Factors Associated with the Risk of Developing Post-Traumatic Sepsis |
To our knowledge, this study is among the first to integrate demographic, clinical, laboratory, and interventional variables in a single model to identify independent risk factors for post-traumatic sepsis. ISS and GCS were retained without indications of problematic collinearity.
Based on these findings, the following risk prediction model was constructed: logit (P)=0.223X1+2.804X2+0.069X3-0.312X4+0.177X5+0.017X6+0.293X8-2.952X9+0.072X10+21.586X11-53.358.
ROC Curve Analysis of the Post-Traumatic Sepsis Risk Prediction Model
The predictive performance of the constructed post-traumatic sepsis risk model was evaluated using ROC curve analysis. The following performance relates to the development dataset. The apparent AUC was 0.998, reflecting high discrimination in the development dataset. Given the absence of internal/external validation, clinical application should be cautious until validated (Figure 1).
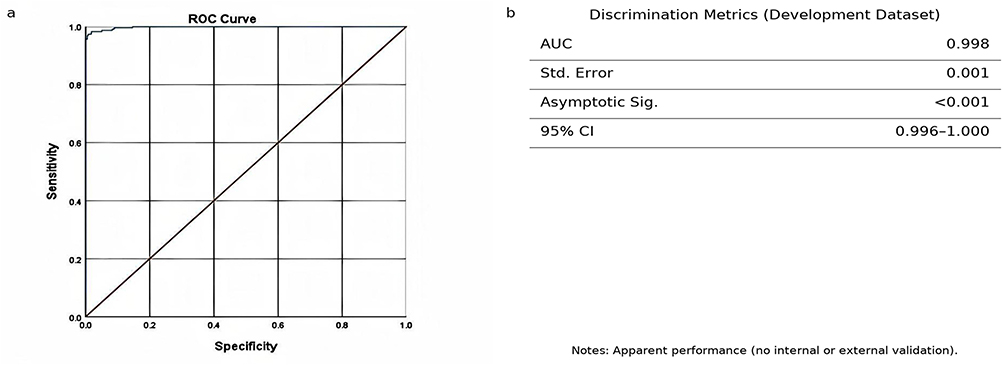 |
Figure 1 Model discrimination in the development dataset: (a) ROC curve; (b) discrimination metrics (apparent performance: AUC 0.998, 95% CI 0.996–1.000). |
Epidemiologic Characteristics and Risk Factors for Mortality in Patients with Post-Traumatic Sepsis
Baseline Characteristics Between Surviving and Non-Surviving Patients
Baseline demographic and clinical characteristics are summarized in Table 4. Patients who developed post-traumatic sepsis were generally older, had more injury sites, and exhibited higher severity scores (ISS, APACHE II, SOFA) compared with non-septic patients (P < 0.05). Among septic patients, non-survivors demonstrated significantly higher APACHE II and SOFA scores, lower admission blood pressure, and more frequent multi-organ dysfunction than survivors.
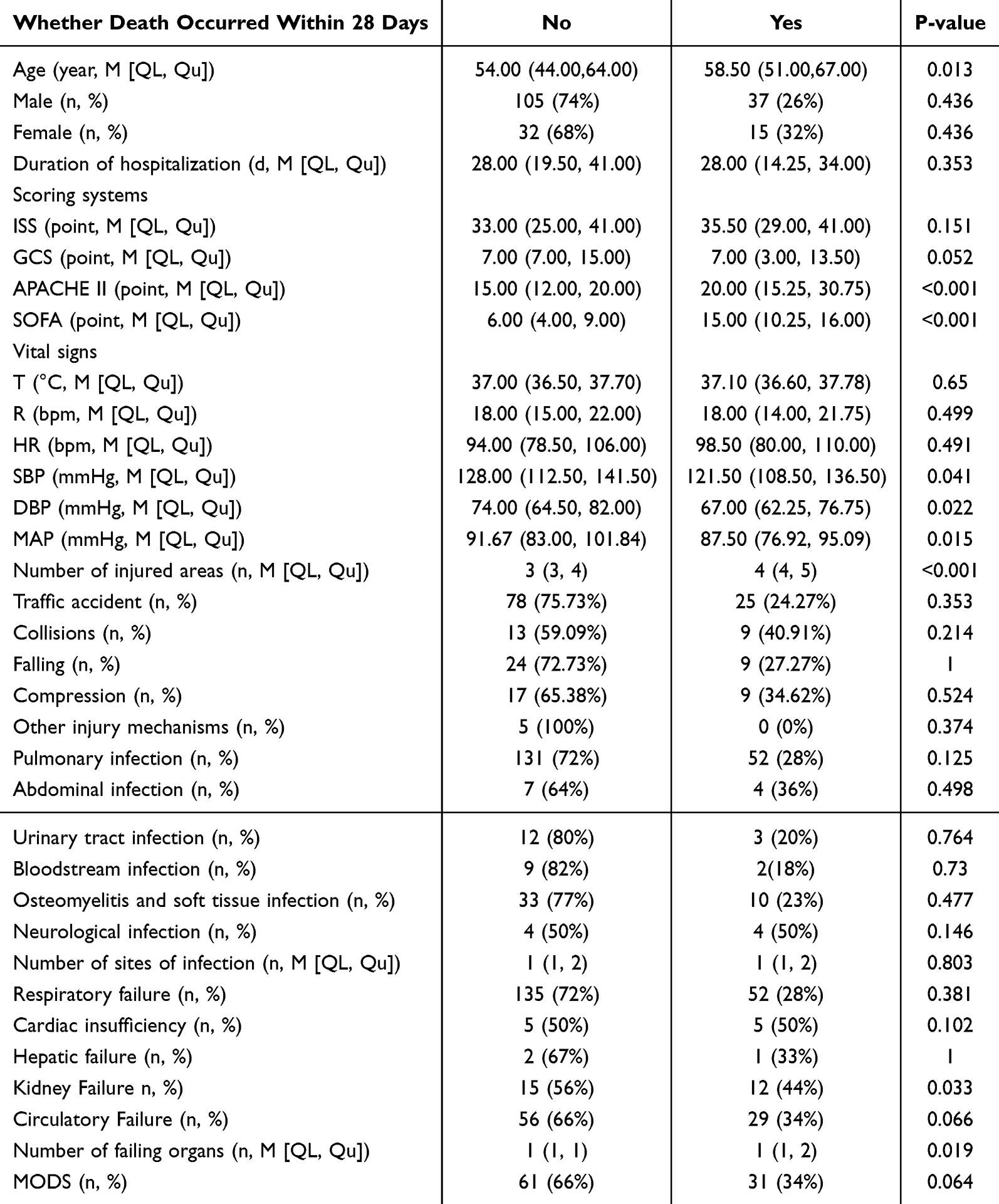 |
Table 4 Baseline Demographic and Clinical Characteristics of Patients with Post-Traumatic Sepsis Between Survivors and Non-Survivors |
The onset of post-traumatic sepsis predominantly occurred within the first three days following trauma. Specifically, sepsis occurred on the day of injury in 13 cases (6.88%), on the first day post-injury in 61 cases (32.28%), on the second day in 40 cases (21.16%), and on the third day in 28 cases (14.81%), as illustrated in Figure 2.
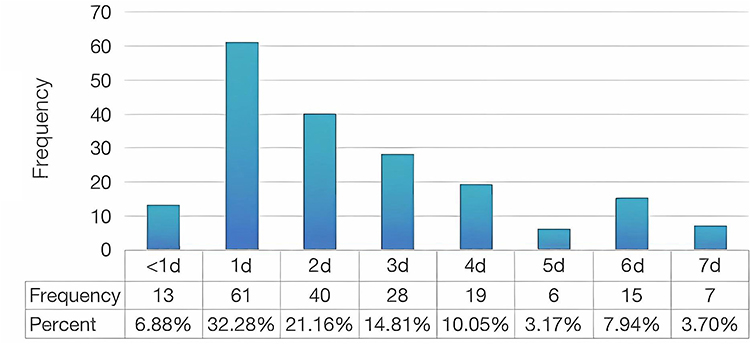 |
Figure 2 Schematic diagram of the onset time of post-traumatic sepsis. |
Laboratory and Interventional Data Between Surviving and Non-Surviving Patients
Laboratory and treatment-related data are presented in Table 5. Compared with survivors, non-survivors had higher CRP, sodium, and lactate levels. Interventional measures such as mechanical ventilation, vasoactive drug administration, and continuous renal replacement therapy (CRRT) were significantly more frequent in the sepsis group, particularly among non-survivors.
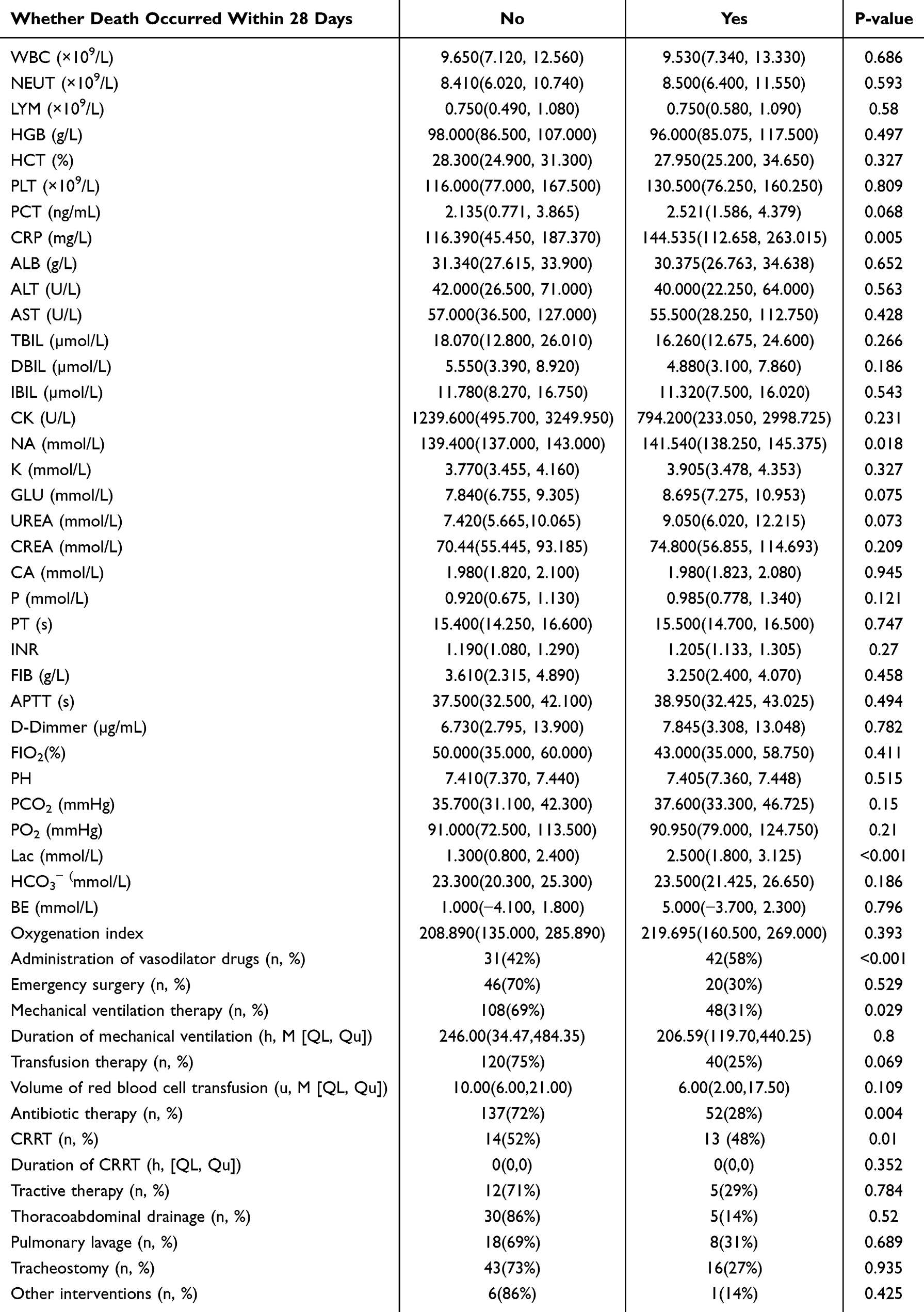 |
Table 5 Laboratory and Treatment-Related Data in Patients with Post-Traumatic Sepsis Between Survivors and Non-Survivors |
Risk Factors for Mortality in Post-Traumatic Sepsis
Development of a Predictive Model for 28 Days Mortality
All effect estimates and inference reported below are pooled across the imputed datasets using Rubin’s rules. Multivariate logistic regression analysis reveals that age, the number of injury sites, Sequential Organ Failure Assessment (SOFA) score, C-reactive protein (CRP), and the use of vasoactive drugs are independent risk factors for the progression of traumatic sepsis to death within 28 days, as shown in the Table 6. In the final multivariable models, SOFA was included as the global severity score, while APACHE II was omitted to avoid redundancy/collinearity between global scores.
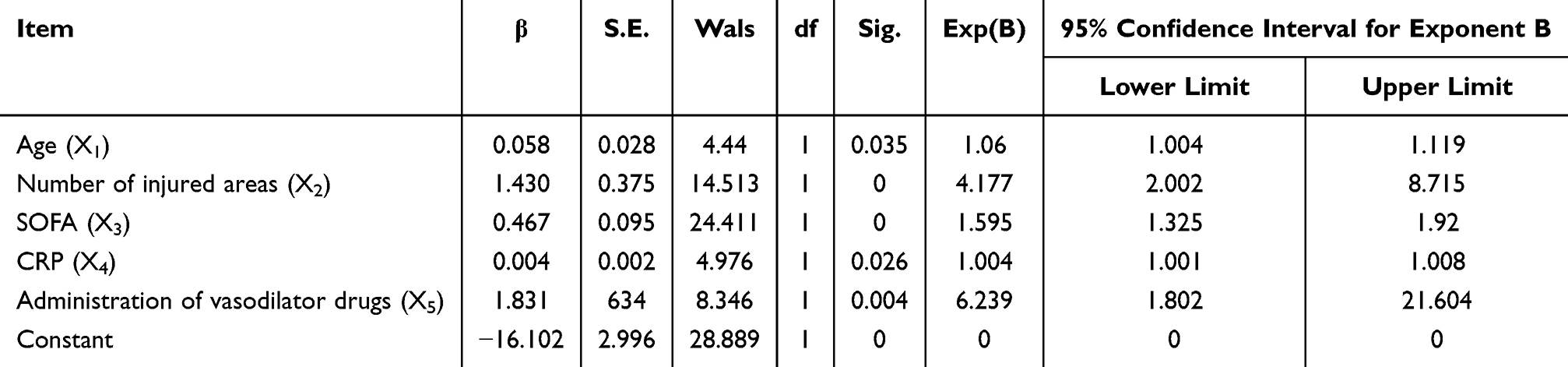 |
Table 6 Logistic Regression Analysis of Risk Factors Associated with Death From Post-Traumatic Sepsis |
Based on these variables, the following logistic regression equation was derived: Logit (P) = 0.058X1 + 1.43X2 + 0.467X3 + 0.004X4 + 1.831X5-16.102.
Evaluation of the Post-Traumatic Sepsis Mortality Prediction Model Using ROC Curve Analysis
The predictive performance of the post-traumatic sepsis mortality risk model was evaluated using ROC curve analysis. The apparent AUC was calculated to be 0.969, showing high apparent discrimination in the development dataset for 28-day mortality. Detailed results are presented in Figure 3.
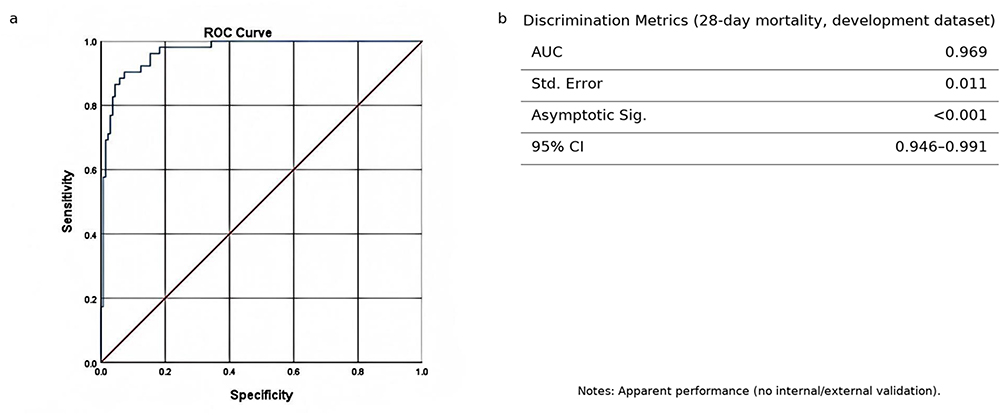 |
Figure 3 Model discrimination for 28-day mortality (development dataset): (a) ROC curve; (b) discrimination metrics (AUC 0.969, 95% CI 0.946–0.991). |
Discussion
In this study, we found that the incidence of post-traumatic sepsis among adult trauma patients was 26.18%. This incidence is within the range reported in previous studies (10%–30%), highlighting that sepsis remains a frequent and life-threatening complication of major trauma.8,9,13 Compared with earlier reports, the incidence observed in our cohort was slightly higher, which may be explained by differences in patient demographics, injury severity, treatment protocols, or infection control measures across institutions. In the 1980s, Trunkey proposed the three-peak model of trauma-related mortality, proposing that most trauma deaths occur at the scene of the incident. The primary causes of mortality in the early phase include hemorrhagic shock resulting from severe brain injury or substantial blood loss following major trauma.14 In contrast, mortality associated with post-traumatic sepsis typically manifests at a later stage, characterized by life-threatening organ dysfunction caused by infection-induced dysregulation of the physiological responses.15 During this third peak of mortality, significant improvements in patient outcomes were achieved through advancements such as prompt hemorrhage control, early fluid resuscitation, development of innovative antibiotic therapies, and comprehensive support for vital organ function. Despite these advancements, survival outcomes for patients with post-traumatic infections have not improved at a comparable rate.3,5,6
The present study found that patients with post-traumatic sepsis were primarily between the ages of 46 and 65 years. This finding differs from national and international epidemiological data, which generally indicate that post-traumatic sepsis predominantly affects individuals aged 45 years or younger.1,16 Consistent with the findings of a Korean study, the present analysis demonstrated that age is an independent risk factor for 28-day mortality in individuals with post-traumatic sepsis.17
A domestic study conducted using data from the Medical Information Mart for Intensive Care III reported that age, respiratory rate, mechanical ventilation, and the use of vasoactive drugs were independent risk factors associated with in-hospital mortality in patients with post-traumatic sepsis.7 These findings contrast with the results of several other national and international studies. Several factors may account for these inconsistencies. One explanation may involve differences in the distribution of injuries within the local population. Another contributing factor could be the increased average age of the primary working population in the local area. Lastly, the single-center design of this study may have introduced selection bias, limiting the generalizability of the findings. To address these limitations, future studies should incorporate data from multiple centers, and larger, more diverse cohorts. Such efforts could mitigate biases and improve the generalizability of the findings.
The present study identified a significantly higher prevalence of hypertension and coronary artery disease among individuals with post-traumatic sepsis compared to those without sepsis. These findings are consistent with a single-center prospective cohort study conducted in China, which reported hypertension as an independent risk factor for the development of sepsis.18 Furthermore, a national study reported that diabetes mellitus (DM), hypertension, coagulation disorders, elevated creatinine levels, increased urea nitrogen levels, higher body mass index (BMI), and lower initial GCS scores were independent risk factors for post-traumatic sepsis. Notably, the incidence of sepsis was significantly higher among individuals with glycated hemoglobin levels exceeding 6.5%.19
Similar associations have been reported internationally, where hypertension, DM, and sepsis often share geographic distributions. The findings of the current study, along with numerous other investigations, indicates a potential shared pathophysiological mechanism linking sepsis, hypertension, and DM. However, further research is needed to elucidate this relationship.20
This study also identified a significant difference in the distribution of injury mechanisms between the sepsis and non-sepsis groups. However, no statistically significant difference was observed between the surviving and non-surviving subgroups within the sepsis group. In the sepsis group, traffic accident injuries were the most common cause (54.50%), while fall or collision injuries were predominant in the non-sepsis group (43.15%).
These findings are consistent with international data indicating that traffic accidents are a major contributor to trauma-related mortality, and that infections are among the most frequent complications following traumatic injuries.21 In China, the widespread adoption of motorization and industrialization has resulted a substantial increase in road traffic injuries, which have become the leading cause of injury-related deaths since 2000.22 A regional study conducted by Li et al in Suining, Sichuan, involving 500 cases of unintentional injuries, also identified traffic accidents as the primary cause.23
In terms of injury mechanisms, traffic accidents are more likely to result in multiple severe trauma types, whereas fall or collision injuries tend to involve single-site trauma with a higher severity level.13
Several scoring systems are routinely used in the diagnosis and management of trauma and sepsis, playing a key role in assessing injury severity and guiding treatment decisions. Common trauma assessment tools include the Abbreviated Injury Scale, Injury Severity Score, Trauma Injury Severity Score, and the Approach to Characteristic Severity of Trauma. In the context of sepsis, widely used scoring systems include the SOFA score, the Systemic Inflammatory Response Syndrome diagnostic criteria, and the Quick SOFA score.
Eguia et al analyzed clinical data from patients with trauma between 2014 and 2016 and demonstrated a correlation between the SOFA score at admission, the presence of severe trauma, and the incidence of post-traumatic sepsis.13 Similarly, a randomized controlled trial involving 869 patients conducted by Campwala et al identified multiple organ failure and nosocomial infections as common complications among patients with trauma.24 These complications were associated with increased injury severity, elevated shock indices, and reduced GCS scores.
The findings of this study align with previous research, indicating that the ISS, GCS, and the number of injury sites are independent risk factors for post-traumatic sepsis. Furthermore, the SOFA score and the number of injury sites were identified as independent risk factors for 28-day mortality in patients with post-traumatic sepsis.
Although the APACHE-II score is one of the most widely applied tools for assessing disease severity and predicting prognosis among patients who are critically ill, its use in this study indicated a significant covariance with the SOFA score during multifactorial logistic regression. This covariance may explain the association between the APACHE-II score and the 28-day mortality rate in patients with post-traumatic sepsis.
In clinical settings, the objective is to use concise and contextually relevant scoring systems to assess disease severity and predict prognosis. Although dynamic assessment allows for a more precise understanding of patient status, it also imposes a considerable statistical workload. Therefore, further research is needed to develop intelligent dynamic assessment models for clinical applications, enabling more efficient and accurate patient monitoring.
The findings of this study indicate that the onset of post-traumatic sepsis typically occurred within three days following injury. This observation is consistent with established concepts regarding the host’s immunological response to trauma, particularly the “two-hit” or “second blow” theory.25 In individuals with trauma, the shock resulting from injury often leads to organ and soft tissue damage or fractures. The initial result, or the “first blow” —typically involving hemorrhagic shock, soft tissue damage, or bone fractures—activates complex systemic inflammatory responses.25–27 The “second blow” is introduced by additional endogenous or exogenous factors that exacerbate the initial response, thereby contributing to the onset and progression of post-traumatic complications, including sepsis.28,29
Typical endogenous factors contributing to the “second blow” include acute respiratory distress, metabolic acidosis, recurrent blood pressure fluctuations, and ischemia/reperfusion injury.30,31 In contrast, exogenous factors encompass severe tissue damage, hypothermia, and substantial blood loss.32,33 Although post-traumatic sepsis can be predicted through the development of risk models, the specific mechanisms underlying the progression from trauma to sepsis remain under investigation. Various internal and external stimuli may accelerate the progression of sepsis, aside from instances such as gastrointestinal perforation due to abdominal trauma and infections resulting from contaminated injury sites.
Sepsis-related biomarkers: In recent years, the investigation of sepsis-related biomarkers has gained significant attention. In the present study, neutrophil count, CRP level, creatine kinase, and Na were identified as independent risk factors for the development of post-traumatic sepsis. Additionally, the CRP level was identified as an independent risk factor for 28-day mortality in patients with post-traumatic sepsis.
Although the PCT level, commonly used in clinical settings, differed significantly between the sepsis and non-sepsis groups, PCT did not emerge as an independent risk factor in the multivariate logistic regression model. This discrepancy may be attributed to the timing of data collection, as laboratory indicators were obtained at the time of admission, possibly before the progression to infection and sepsis. Although PCT is continuously secreted during noninfectious processes, its peak level typically appears during active infection.34
A national study reported that the CRP/albumin ratio serves as an independent risk factor for the development of sepsis.35 In a comprehensive analysis conducted by Pierrakos et al in 2020, a total of 5,367 publications were reviewed, identifying 258 candidate biomarkers for sepsis diagnosis.36 Among these, 44 biomarkers exhibited low specificity for diagnosing sepsis. Various biomarkers, including PCT, CRP, the neutrophil-to-lymphocyte ratio, the monocyte-to-lymphocyte ratio, the platelet-to-lymphocyte ratio, and the ratio of mean platelet volume (MPV) to platelet count (MPV/PLT), have been evaluated for their prognostic value in sepsis onset and mortality. However, apart from PCT and interleukin-6 (IL-6), which are increasingly applied to monitor sepsis progression, the clinical use of other biomarkers requires further investigation.37
Consistent with previous studies, the present analysis identified the lungs as the most common site of infection in patients with post-traumatic sepsis.38 This predominance may be attributed to compromised thoracic integrity resulting from direct chest injury, as well as the development of acute respiratory distress syndrome (ARDS) as a result of direct or indirect lung injury.39 ARDS is a frequent complication in sepsis, characterized by diffuse alveolar damage, severe hypoxemia, and respiratory distress. Despite ongoing research, the pathogenesis of ARDS remains unclear, and the condition continues to be associated with a high mortality rate, ranging from 30% to 40%.40 The presence of pulmonary involvement—whether due to primary mechanical trauma or secondary systemic inflammatory responses—significantly increases the risk of sepsis in patients with trauma.38
Therapeutic interventions and risk of mortality: This study also demonstrated that the use of vasoactive medications was an independent risk factor for 28-day mortality in patients with post-traumatic sepsis. Vasoactive medications play a key role in managing shock, particularly in cases of traumatic, hemorrhagic, or septic shock.41 The timely and appropriate administration of these drugs ensures adequate blood distribution and helps mitigate the risk of organ failure.11
Predictive models for sepsis progression and mortality: Two logistic regression-based predictive models were developed in this study: one for identifying the risk of developing post-traumatic sepsis and another for predicting 28-day mortality in affected patients. The model for sepsis progression identified several independent risk factors, including length of hospital stay, number of injury sites, ISS, NEUT, CRP level, serum sodium concentration, duration of CRRT, and duration of tracheotomy. A separate predictive model for 28-day mortality in patients with post-traumatic sepsis identified age, number of injury sites, SOFA score, CRP level, and vasoactive drug use as significant risk factors. Tempering accuracy claims. Reported discrimination is apparent and likely optimistic; clinical utility and generalizability require validation.
The ISS is extensively applied in clinical practice for assessing trauma severity. An ISS score of 25 or higher typically indicates severe trauma and correlates with significantly reduced survival prospects. When the ISS exceeds 50, the survival rates are extremely low, making the score a valuable predictor of mortality in patients with trauma.42,43 In this study, the ISS was significantly higher in the sepsis group compared to the non-sepsis group.
Inflammatory markers and biomarkers: Recent research has increasingly focused on the diagnostic and prognostic value of inflammatory markers. Jekarl et al investigated various cytokines and found that both PCT and CRP have diagnostic value in sepsis, while PCT, IL-6, and interleukin-5 are useful for assessing sepsis severity.44 In the present study, CRP emerged as an independent risk factor for both the onset of post-traumatic sepsis and 28-day mortality in affected patients.
Elevation of creatine kinase is often observed due to mechanical disruption of rhabdomyocytes following trauma. Forouzan et al reported a significant association between creatine kinase BB isoenzyme levels and intracranial damage.45 Additionally, serum creatine kinase has been linked to BMI and the occurrence of acute kidney injury in patients with severe trauma, as reported in a prospective cohort study.46
Several limitations should be acknowledged in this study. The retrospective, single-center design may introduce a selection and information bias. External validation through large-scale, prospective studies is necessary to confirm the robustness and applicability of the developed models. Certain key clinical indicators were not included due to a high proportion of missing data. Notably, variables such as hydrogen ion concentration, blood lactate levels, and the oxygenation index were not included, potentially limiting the comprehensiveness of the study. Although the study incorporated a broad range of clinical parameters collected at admission, it did not evaluate the dynamic changes in these indicators during the course of hospitalization. Further research is necessary to assess the prognostic value of longitudinal changes in key clinical and biochemical parameters. Although hospital-related complications were considered, the available data were limited, and their role in the development of post-traumatic sepsis warrants further investigation in larger cohorts. A few predictors exhibited large ORs and wide CIs due to low exposure counts (data sparsity). This statistical imprecision does not alter the direction of associations nor our main conclusions. This study reports a developmental model without internal resampling or external validation; consequently, the reported AUC likely overestimates performance due to optimism. Generalizability beyond this cohort remains uncertain and requires bootstrap- or CV-based internal validation and external validation in independent populations. If validated, the model could support triage workflows as follows: (i) When: compute risk at ED/trauma admission (0–6 h) with routine labs; re-assess at 24–48 h when new data become available. (ii) How: implement risk stratification with thresholds chosen to prioritize sensitivity for early rule-in (final thresholds to be locally validated). (iii) What to do: high-risk flags could trigger closer monitoring, repeat CRP/sodium, blood cultures/infection screen, and early sepsis bundle per local guidelines; intermediate-risk prompts repeat labs and reassessment; low-risk supports routine care with vigilance. (iv) Integration: embed as an EHR calculator/alert, restrict inputs to readily available variables, and record reasons for overrides. (v) Governance: deploy in a silent-mode pilot to audit performance and fairness, followed by local recalibration and periodic monitoring before widespread use. Until such validation is completed, the model should be considered an exploratory decision-support tool, not a stand-alone diagnostic.
Conclusions
This study characterizes the epidemiology of post-traumatic sepsis and reports a multivariable model with good discrimination in the development dataset, highlighting potentially actionable markers. Given the lack of internal/external validation and the potential for optimism/sparsity-related instability, the model should not be used for clinical decision-making at this stage. Future work should include resampling-based internal validation, external validation in prospective multicenter cohorts, recalibration, and impact assessment. Until then, the model may serve as an exploratory decision-support tool in silent pilots. Nonetheless, they outline a pragmatic pathway for integrating early risk stratification into trauma triage.
Abbreviations
ISS, Injury Severity Score; GCS, Glasgow Coma Score; CRP, reactive protein; CRRT, Continuous blood purification; SOFA, Sequential Organ Failure Assessment; ROC curve, Receiver Operating Characteristic Curve; ICU, Intensive care unit; AUC, Area under the ROC curve; APACHE-II, Acute Physiology and Chronic Health Score; HCT, Erythrocyte pressure volume; PLT, Platelet count; PCT, Procalcitonin; ALT, Alanine aminotransferase; AST, Aspartate aminotransferase; Na, Sodium ion concentration; K, Potassium ion concentration; GLU, Random blood glucose; Ca, Calcium ion concentration; P, Phosphorus ion concentration; PT, Prothrombin time; INR, Internationalization ratio; FIB, Fibrinogen; APTT, Activated partial thromboplastin time; NEUT, Neutrophil count; MIMIC-III, Medical Information Mart for Intensive Care III; AIS, Abbreviated Injury Scale; TRISS, Trauma Injury Severity Score; ASCOT, Approach to Characteristic Severity of Trauma; SIRS, Systemic Inflammatory Response Syndrome; qSOFA, Quick SOFA; CAR, CRP/albumin ratio; NLR, Neutrophil-to-lymphocyte ratio; MLR, Monocyte-to-lymphocyte ratio; PLR, Platelet-to-lymphocyte ratio; MPV, Mean platelet volume; IL-6, Interleukin-6; ARDS, Acute respiratory distress syndrome; IL-5, Interleukin-5; CK-BB, Creatine kinase BB isoenzyme; BMI, Body Mass Index; AKI, Acute Kidney Injury; pH, Power of hydrogen.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The retrospective study was approved by ethics committee of the Hebei Medical University Third Hospital (Approval No. W2022-044-1). This study was conducted in accordance with the declaration of Helsinki. Informed consent was waived due to the retrospective nature of the study, which involved the analysis of existing clinical data with no direct patient contact or intervention.
Funding
No external funding was received to conduct this study.
Disclosure
The authors declare that they have no conflict of interests.
References
1. Leonardo P. Trauma: a neglected US public health emergency. Lancet. 2016;388(10056):2058. doi:10.1016/S0140-6736(16)32057-8
2. Lord JM, Midwinter MJ, Chen Y-F, et al. The systemic immune response to trauma: an overview of pathophysiology and treatment. Lancet. 2014;384(9952):1455–1465. doi:10.1016/S0140-6736(14)60687-5
3. Oyeniyi BT, Fox EE, Scerbo M, Tomasek JS, Wade CE, Holcomb JB. Trends in 1029 trauma deaths at a level 1 trauma center: impact of a bleeding control bundle of care. Injury. 2017;48(1):5–12. doi:10.1016/j.injury.2016.10.037
4. Eriksson J, Lindström A-C, Hellgren E, et al. Postinjury sepsis-associations with risk factors, impact on clinical course, and mortality: a retrospective observational study. Crit Care Explor. 2021;3(8):e0495. doi:10.1097/CCE.0000000000000495
5. Eguia E, Bunn C, Kulshrestha S, et al. Trends, cost, and mortality from sepsis after trauma in the United States: an evaluation of the national inpatient sample of hospitalizations, 2012–2016. Crit Care Med. 2020;48(9):1296–1303. doi:10.1097/CCM.0000000000004451
6. Wafaisade A, Lefering R, Bouillon B, et al. Trauma registry of the german society for trauma surgery. epidemiology and risk factors of sepsis after multiple trauma: an analysis of 29,829 patients from the trauma registry of the german society for trauma surgery. Crit Care Med. 2011;39(4):621–628. doi:10.1097/CCM.0b013e318206d3df
7. Qi J, Xie Q, Li Z, Sun C, Hostiuc S. A nomogram to better predict the in-hospital mortality of trauma patients with sepsis in the intensive care unit. Int J Clin Pract. 2022;2022(1):4134138. doi:10.1155/2022/4134138
8. Mas-Celis F, Olea-López J, Parroquin-Maldonado JA. Sepsis in trauma: a deadly complication. Arch Med Res. 2021;52(8):808–816. doi:10.1016/j.arcmed.2021.10.007
9. Stengel D, Bauwens K, Sehouli J, Ekkernkamp A, Porzsolt F. Systematic review and meta-analysis of antibiotic therapy for bone and joint infections. Lancet Infect Dis. 2001;1(3):175–188. doi:10.1016/S1473-3099(01)00094-9
10. Tong Y, Zhang J, Fu Y, He X, Feng Q, Adnan M. Risk factors and outcome of sepsis in traumatic patients and pathogen detection using metagenomic next-generation sequencing. Can J Infect Dis Med Microbiol. 2022;2022:2549413. doi:10.1155/2022/2549413
11. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
12. Calandra T, Cohen J. International sepsis forum definition of infection in the ICU consensus conference. The international sepsis forum consensus conference on definitions of infection in the intensive care unit. Crit Care Med. 2005;33(7):1538–1548. doi:10.1097/01.ccm.0000168253.91200.83
13. Eguia E, Cobb AN, Baker MS, et al. Risk factors for infection and evaluation of Sepsis-3 in patients with trauma. Am J Surg. 2019;218(5):851–857. doi:10.1016/j.amjsurg.2019.03.005
14. Demetriades D, Murray J, Charalambides K, et al. Trauma fatalities: time and location of hospital deaths. J Am Coll Surg. 2004;198(1):20–26. doi:10.1016/j.jamcollsurg.2003.09.003
15. Trunkey DD. Trauma. Accidental and intentional injuries account for more years of life lost in the U.S. than cancer and heart disease. Among the prescribed remedies are improved preventive efforts, speedier surgery and further research. Sci Am. 1983;249(2):28–35. doi:10.1038/scientificamerican0883-28
16. Bösch F, Angele MK, Chaudry IH. Gender differences in trauma, shock and sepsis. Mil Med Res. 2018;5(1):35. doi:10.1186/s40779-018-0182-5
17. Park JH, Choi SH, Yoon YH, Park SJ, Kim JY, Cho HJ. Risk factors for sepsis in Korean trauma patients. Eur J Trauma Emerg Surg. 2016;42(4):453–458. Epub 2015 Jul 23. PMID: 26201390. doi:10.1007/s00068-015-0552-6
18. Zhou J, Luo X-Y, Chen G-Q, et al. Incidence, risk factors and outcomes of sepsis in critically ill post-craniotomy patients: a single-center prospective cohort study. Front Public Health. 2022;10:895991. doi:10.3389/fpubh.2022.895991
19. Guo F, Shen H. Glycosylated hemoglobin as a predictor of sepsis and all-cause mortality in trauma patients. Infect Drug Resist. 2021;14:2517–2526. doi:10.2147/IDR.S307868
20. Ahlberg CD, Wallam S, Tirba LA, Itumba SN, Gorman L, Galiatsatos P. Linking sepsis with chronic arterial hypertension, diabetes mellitus, and socioeconomic factors in the United States: a scoping review. J Crit Care. 2023;77:154324. doi:10.1016/j.jcrc.2023.154324
21. Castro Appiani LM, Castro S, Romero B, et al. Upper extremity trauma in costa rica - evaluating epidemiology and identifying opportunities. Curr Orthop Pract. 2023;34(6):280–284. doi:10.1097/bco.0000000000001233
22. Ozanne-Smith J, Li Q. A social change perspective on injury prevention in China. Inj Prev. 2018;24(Suppl 1):i25–i31. doi:10.1136/injuryprev-2017-042712
23. Li YA, Hu KH, Wang M. Epidemiological characteristics of 500 cases of first-aid injuries outside hospital. J Pub Health Prev Med. 2023;34(6):85–88.
24. Campwala I, Guyette FX, Brown JB, et al. Evaluation of critical care burden following traumatic injury from two randomized controlled trials. Sci Rep. 2023;13(1):1106. doi:10.1038/s41598-023-28422-5
25. Rotstein OD. Modeling the two-hit hypothesis for evaluating strategies to prevent organ injury after shock/resuscitation. J Trauma. 2003;54(5 Suppl):S203–6. doi:10.1097/01.TA.0000064512.62949.92
26. Napolitano LM, Ferrer T, McCarter RJ Jr, Scalea TM. Systemic inflammatory response syndrome score at admission independently predicts mortality and length of stay in trauma patients. J Trauma. 2000;49(4):647–653. doi:10.1097/00005373-200010000-00011
27. Keel M, Trentz O. Pathophysiology of polytrauma. Injury. 2005;36(6):691–709. doi:10.1016/j.injury.2004.12.037
28. Smail N, Messiah A, Edouard A, et al. Role of systemic inflammatory response syndrome and infection in the occurrence of early multiple organ dysfunction syndrome following severe trauma. Intensive Care Med. 1995;21(10):813–816. doi:10.1007/BF01700964
29. Malone DL, Kuhls D, Napolitano LM, McCarter R, Scalea T. Back to basics: validation of the admission systemic inflammatory response syndrome score in predicting outcome in trauma. J Trauma. 2001;51(3):458–463. doi:10.1097/00005373-200109000-00006
30. Ertel W, Friedl HP, Trentz O. Multiple organ dysfunction syndrome (MODS) following multiple trauma: rationale and concept of therapeutic approach. Eur J Pediatr Surg. 1994;4(4):243–248. doi:10.1055/s-2008-1066112
31. Dunham CM, Damiano AM, Wiles CE, et al. Post-traumatic multiple organ dysfunction syndrome--infection is an uncommon antecedent risk factor [J]. Injury. 1995;26(6):373–378. doi:10.1016/0020-1383(95)00061-D
32. Haga Y, Beppu T, Doi K, et al. Systemic inflammatory response syndrome and organ dysfunction following gastrointestinal surgery. Crit Care Med. 1997;25(12):1994–2000. doi:10.1097/00003246-199712000-00016
33. Waydhas C, Nast-Kolb D, Trupka A, et al. Posttraumatic inflammatory response, secondary operations, and late multiple organ failure. J Trauma. 1996;40(4):624–630. doi:10.1097/00005373-199604000-00018
34. Mierzchała-Pasierb M, Lipińska-Gediga M. Sepsis diagnosis and monitoring - procalcitonin as standard, but what next? Anaesthesiol Intensive Ther. 2019;51(4):299–305. doi:10.5114/ait.2019.88104
35. Kang P, Kang W, Li Y, Li T. C-reactive protein-to-albumin ratio as an early biomarker to identify sepsis in neonates with pneumonia. Mediators Inflamm. 2022;2022:4711018. doi:10.1155/2022/4711018
36. Pierrakos C, Velissaris D, Bisdorff M, Marshall JC, Vincent JL. Biomarkers of sepsis: time for a reappraisal. Crit Care. 2020;24(1):287. doi:10.1186/s13054-020-02993-5
37. Djordjevic D, Rondovic G, Surbatovic M, et al. Neutrophil-to-lymphocyte ratio monocyte-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and mean platelet volume-to-platelet count ratio as biomarkers in critically ill and injured patients: which ratio to choose to predict outcome and nature of bacteremia? Mediators Inflamm. 2018;2018:3758068. doi:10.1155/2018/3758068
38. Dvorak JE, Ladhani HA, Claridge JA. Review of sepsis in burn patients in 2020. Surg Infect (Larchmt). 2021;22(1):37-43. doi: 10.1089/sur.2020.367. Surg Infect. 2021;22(9):989. doi:10.1089/sur.2020.367.correx
39. Jabaudon M, Blondonnet R, Constantin JM. ARDS in patients with chest trauma: better safe than sorry. Anaesth Crit Care Pain Med. 2019;38(3):221–222. doi:10.1016/j.accpm.2019.04.006
40. Li W, Li D, Chen Y, et al. Classic signaling pathways in alveolar injury and repair involved in sepsis-induced ALI/ARDS: new research progress and prospect. Dis Markers. 2022;2022:6362344. doi:10.1155/2022/6362344
41. Annane D, Ouanes-Besbes L, de Backer D, et al. A global perspective on vasoactive agents in shock. Intensive Care Med. 2018;44(6):833–846. doi:10.1007/s00134-018-5242-5
42. Mica L, Furrer E, Keel M, Trentz O. Predictive ability of the ISS, NISS, and APACHE II score for SIRS and sepsis in polytrauma patients. Eur J Trauma Emerg Surg. 2012;38(6):665–671. doi:10.1007/s00068-012-0227-5
43. Harwood PJ, Giannoudis PV, Probst C, Van Griensven M, Krettek C, Pape HC, Polytrauma Study Group of the German Trauma Society. Which AIS based scoring system is the best predictor of outcome in orthopaedic blunt trauma patients? J Trauma. 2006;60(2):334–340. doi:10.1097/01.ta.0000197148.86271.13
44. Jekarl DW, Kim JY, Lee S, et al. Diagnosis and evaluation of severity of sepsis via the use of biomarkers and profiles of 13 cytokines: a multiplex analysis. Clin Chem Lab Med. 2015;53(4):575–581. doi:10.1515/cclm-2014-0607
45. Forouzan A, Fahimi MA, Bastan ASI, Delirrooyfard A. Diagnostic competence of creatine kinase BB, in mild traumatic brain injury and its prognostic value. Adv Biomed Res. 2023;12(1):84. doi:10.4103/abr.abr_122_21
46. Vasquez CR, DiSanto T, Reilly JP, et al. Relationship of body mass index, serum creatine kinase, and acute kidney injury after severe trauma. J Trauma Acute Care Surg. 2020;89(1):179–185. doi:10.1097/TA.0000000000002714
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.