Back to Journals » Journal of Pain Research » Volume 11
Epidemiological profiles of chronic low back and knee pain in middle-aged and elderly Japanese from the Murakami cohort
Authors Takahashi A, Kitamura K, Watanabe Y, Kobayashi R, Saito T, Takachi R, Kabasawa K, Oshiki R, Tsugane S ![]() , Iki M
, Iki M ![]() , Sasaki A, Yamazaki O, Nakamura K
, Sasaki A, Yamazaki O, Nakamura K ![]()
Received 21 August 2018
Accepted for publication 9 November 2018
Published 12 December 2018 Volume 2018:11 Pages 3161—3169
DOI https://doi.org/10.2147/JPR.S184746
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Akemi Takahashi,1 Kaori Kitamura,2 Yumi Watanabe,2 Ryosaku Kobayashi,3 Toshiko Saito,4 Ribeka Takachi,5 Keiko Kabasawa,6 Rieko Oshiki,1 Shoichiro Tsugane,7 Masayuki Iki,8 Ayako Sasaki,9 Osamu Yamazaki,10 Kazutoshi Nakamura2
1Department of Rehabilitation, Niigata University of Rehabilitation, Niigata, Japan; 2Division of Preventive Medicine, Niigata University Graduate School of Medical and Dental Sciences, Niigata, Japan; 3Department of Physical Therapy, Niigata University of Health and Welfare, Niigata, Japan; 4Department of Health and Nutrition, Niigata University of Health and Welfare, Niigata, Japan; 5Department of Food Science and Nutrition, Nara Women’s University Graduate School of Humanities and Sciences, Nara, Japan; 6Department of Health Promotion Medicine, Niigata University Graduate School of Medical and Dental Sciences, Niigata, Japan; 7Center for Public Health Sciences, National Cancer Center, Tokyo, Japan; 8Department of Public Health, Kindai University Faculty of Medicine, Osaka, Japan; 9Murakami Public Health Center, Niigata, Japan; 10Niigata Prefectural Office, Niigata, Japan
Purpose: Epidemiological profiles of chronic low back and knee pain have not been studied extensively. This study aimed to determine the prevalence of and potential risk factors associated with chronic low back and knee pain in middle-aged and elderly Japanese.
Methods: This cross-sectional study involved 14,217 community-dwelling individuals aged 40–74 years living in the Murakami area of Japan. A self-administered questionnaire was used to obtain information regarding marital status, education level, occupation, household income, and body size. Participants also reported current chronic pain, if any, by site and degree of severity, using the verbal rating scale of the Short Form 36.
Results: The prevalence of moderate–very severe chronic pain was 9.7% in the low back, 6.7% in the knee, 13.9% in either the low back or knee, and 2.6% in both the low back and knee. Multivariate analysis revealed that lower education level, lower income, and manual occupation in men and older age and higher body mass index in women were significantly associated with a higher prevalence of chronic low back pain. In both sexes, older age, lower education level, and higher body mass index were significantly associated with a higher prevalence of knee pain. Regarding sex differences, adjusted ORs of chronic pain of the low back and knee for women were 0.85 (95% CI 0.75–0.97) and 1.27 (95% CI 1.09–1.49), respectively.
Conclusion: Nearly 14% of middle-aged and elderly individuals had moderate–very severe chronic pain of the low back or knee, and this pain was associated with many demographic factors, including sex, age, education level, household income, occupation, and body size.
Keywords: body mass index, chronic pain, demography, knee pain, low back pain, prevalence
Introduction
Pain is defined as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage”, and chronic pain is considered pain that persists for >3–6 months.1 Chronic pain causes suffering and affects an individual’s daily life. It also has major economic implications on society.2 Therefore, epidemiological studies are needed to characterize basic factors associated with chronic pain, in order to control it. Chronic pain is an important public health issue worldwide. Epidemiological studies on chronic pain have reported a prevalence of 10%–50%.3,4 In Japan, three epidemiological studies on chronic pain reported a prevalence of 15%–39%5–7 in adult populations.
Chronic low back and knee pain are relevant because they are very common types of musculoskeletal pain, and commonly cause disability and reduce quality of life.8,9 Compared to studies on overall chronic pain, few chronic pain studies have focused on the low back and knee. In this context, the National Health and Nutrition Examination Survey in the US recently described epidemiological characteristics of chronic low back pain.10 In Japan, a cross-sectional study8,11 reported on relationships between chronic low back and knee pain, physical activity, and body mass index (BMI). However, no other studies have systematically examined the epidemiological profiles of chronic low back and knee pain.
We previously initiated a large-cohort study on age-related musculoskeletal diseases in 2011 in the Murakami area (Niigata Prefecture) of Japan.12 Within this framework, we conducted a survey of chronic pain in the baseline study, which enabled us to clarify basic characteristics of chronic pain in detail. Although there are many published epidemiological studies on low back and knee pain, few of these employed the definition of “chronic” pain in their analyses. The present study aimed to determine the prevalence of and potential risk factors (eg, demographic factors and body size) associated with chronic low back and knee pain.
Methods
Subjects
The Murakami cohort is a population-based cohort established by the authors in cooperation with the three local governments of Sekikawa, Awashimaura, and Murakami, northern Niigata.12 All individuals aged 40–74 years who were subjects of the medical check-up program provided by the local governments were invited to participate in the cohort study. Of all 34,802 residents targeted, 14,364 (41.3%) participated in the baseline survey. Of these, 144 did not answer questions about chronic low back or knee pain. Accordingly, 14,217 individuals were analyzed in the present study. Written informed consent was obtained from all subjects, and the study was conducted in accordance with the Declaration of Helsinki. The protocol of this study was approved by the Ethics Committee of Niigata University School of Medicine.
Procedure
In the 2011–2012 baseline survey, a self-administered questionnaire in paper format was distributed to subjects and collected through a community-based communication network. The questionnaire was used to obtain information regarding marital status, education level, household income, occupation, body weight, height, and current chronic pain. Marital status was categorized as married, never married, and divorced, separated, or bereaved. Educational level was categorized as junior high school, high school, junior/vocational college, and university or higher. Household income (JP¥) per year was categorized as 0–2,999,000, 3,000,000–5,999,000, 6,000,000–8,999,000, and ≥9,000,000 (¥110 ≈ US$1 in 2017). BMI was calculated by dividing weight by height squared and categorized into four groups: <18.5, 18.5–21.9, 22.0–24.9, and ≥25.0 kg/m2. In the multivariate analysis, covariates included age (continuous variable), sex, marital status (categorical variable), education level, household income, occupation (categorical variable), and BMI (continuous variable). Details of the baseline survey have been published elsewhere.12
Chronic pain is considered pain that persists >3–6 months.1 Herein, we conservatively defined chronic pain as pain persisting ≥6 months. This definition has been used in previous epidemiological studies.13,14 Subjects were requested to report current chronic pain, if any, by site and degree of severity using the schematic shown in Figure 1. Degree of pain was self-evaluated with the verbal rating scale of Short Form 36:15 1, no pain; 2, very mild; 3, mild; 4, moderate; 5, severe; 6, very severe pain. In the present study, subjects with moderate–very severe chronic pain were allocated to the pain group and all others to the no-pain group when calculating ORs for presence of chronic pain. This categorization has been validated and used previously.13,16
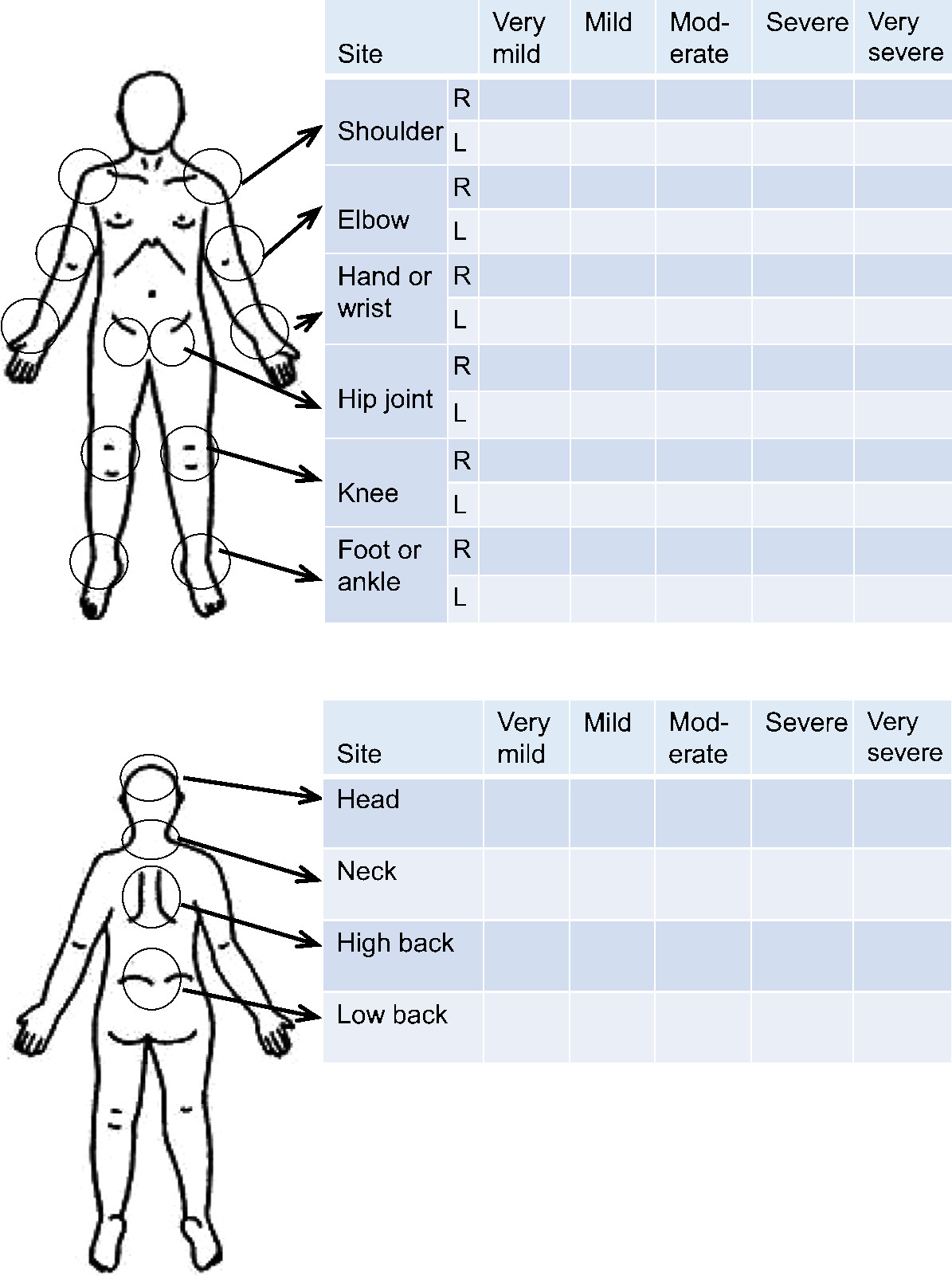 | Figure 1 Schematic in the questionnaire for reporting chronic pain, if any, by site and degree of severity. |
Statistical methods
Mean and SD were calculated to characterize continuous variables. The frequency of chronic pain was tabulated by site and degree of severity. Unadjusted and adjusted ORs for moderate–very severe chronic pain of the low back and knee, the outcome measures of this study, were computed according to age group, marital status, education level, household income, occupation, and BMI by sex using simple and multiple logistic regression analyses. In assigning reference subgroups for OR calculations, the probable lowest-risk subgroup was set as the reference. For the qualitative variable of occupation, although “office work” was the subgroup with the lowest OR for chronic pain, the number of office workers was too small (n=287 in men), suggesting that office work was unsuitable as a reference. Accordingly, “sales and service” was set as the reference. Ptrend values were calculated with simple or multiple logistic regression analysis. SAS 9.13 (SAS Institute Inc., Cary, NC, USA) was used for statistical analyses. P<0.05 was considered statistically significant.
Results
The mean age of subjects (n=14,217) was 59.1 (SD 9.3) years. Numbers of subjects with chronic pain in the low back and knee are shown in Table 1. The prevalence of moderate–very severe chronic pain was 9.7% in the low back and 6.7% in the knee. The prevalence of moderate–very severe chronic severe pain at either the low back or knee was 13.9% (1,970 of 14,217), and that at the low back and knee was 2.6% (364 of 14,217).
 | Table 1 Participants with chronic low back and knee pain (n=14,217) |
Prevalence and ORs of chronic low back pain according to levels of potential predictors are shown in Table 2. The multivariate model showed that lower education level, lower income, and manual occupation in men and older age and higher BMI in women were significantly associated with higher prevalence of chronic low back pain.
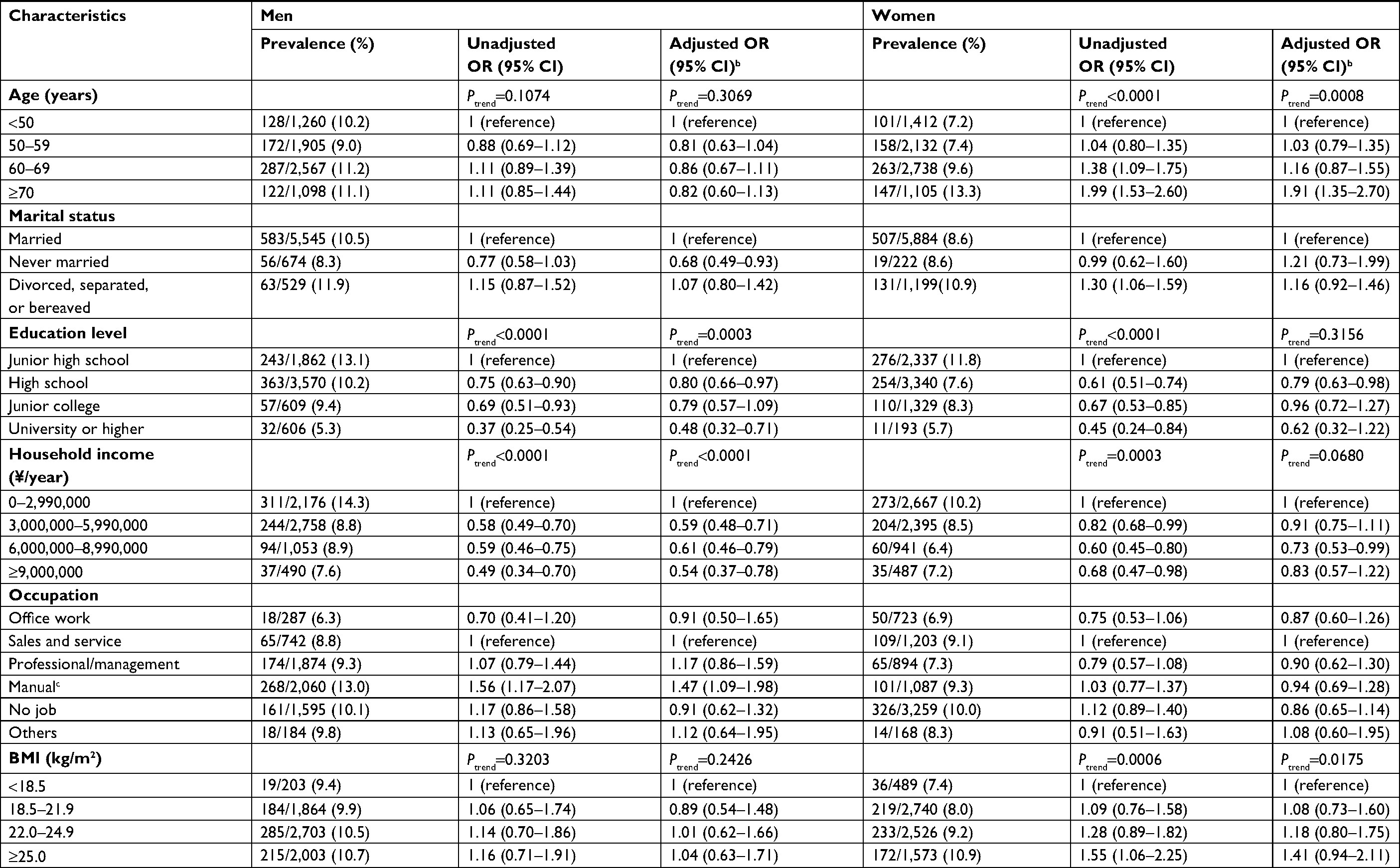 | Table 2 Chronic paina in the low back according to demographic factors and body mass index (BMI) Notes: aModerate, severe, or very severe chronic pain as outcome; badjusted for all other variables. cIncludes security, farming/forestry/fishery, transportation, and labor services. |
Prevalence and ORs of chronic knee pain according to levels of potential predictors are shown in Table 3. The multivariate model showed that older age, lower education, and higher BMI were significantly associated with higher prevalence of chronic knee pain in both sexes. In addition, office work was associated with lower prevalence of chronic knee pain in men.
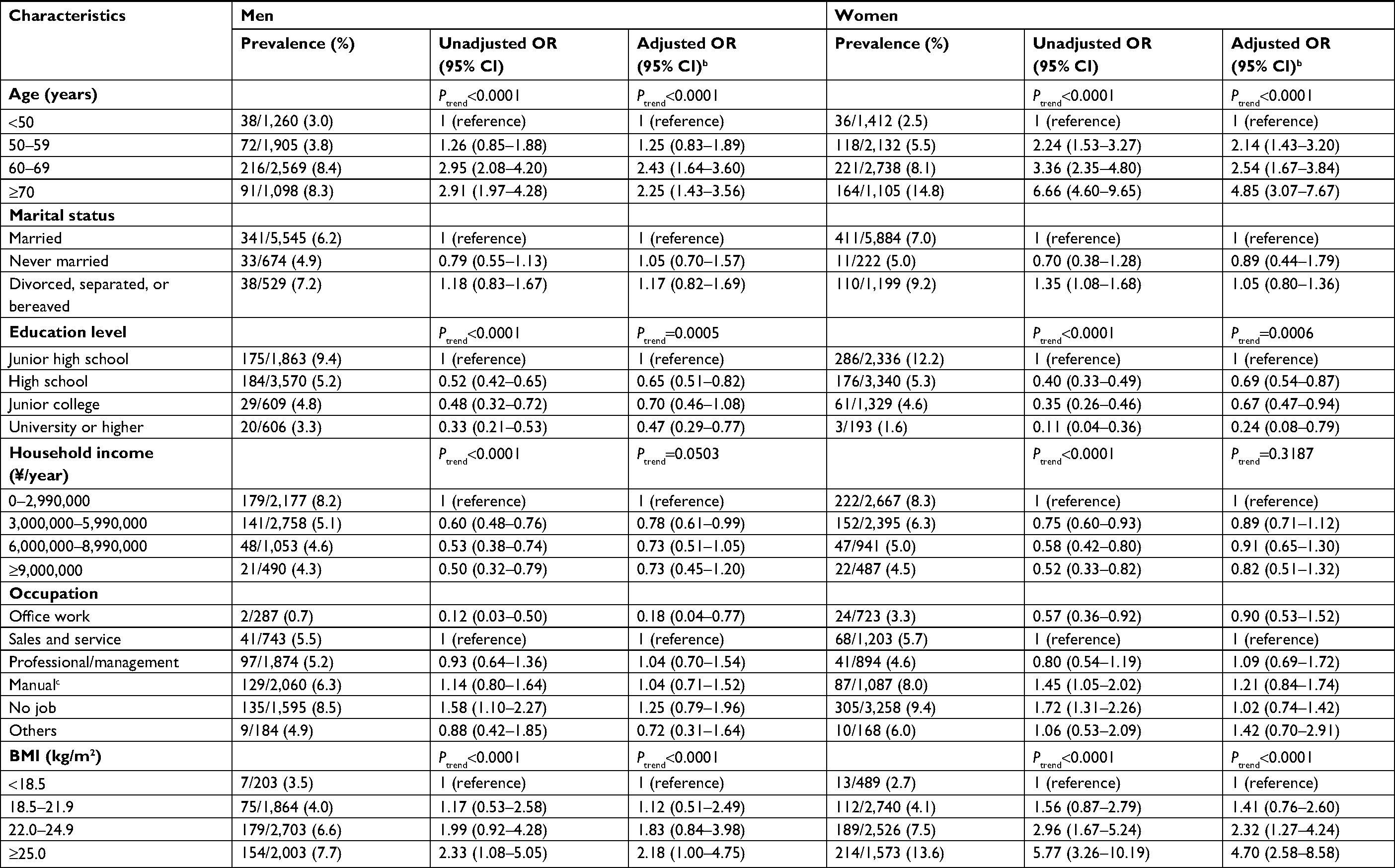 | Table 3 Chronic paina in the knee according to demographic factors and body mass index (BMI) Note: aModerate, severe, or very severe chronic pain as outcome; badjusted for all other variables; cincludes security, farming/forestry/fishery, transportation, and labor services. |
Subgroup analyses by middle-aged (<60 years) and elderly (≥60 years) populations were conducted, yielding differences in the strength of association between predictor and outcome variables. For low back pain, a higher risk was found in male manual workers aged <60 years (adjusted OR 1.73, 95% CI 1.12–2.67), but not in those aged ≥60 years (OR 1.24, 95% CI 0.83–1.87). Moreover, higher BMI were associated with higher adjusted ORs in both men and women aged ≥60 years (Ptrend=0.0092 and 0.0221, respectively), but not in men and women aged <60 years (Ptrend=0.2476 and 0.3506, respectively). For knee pain, higher education levels were associated with lower adjusted ORs in men aged ≥60 years (Ptrend<0.0001), but not in men aged <60 years (Ptrend=0.7306). With regard to sex differences, multivariable adjusted ORs of chronic low back and knee pain for women were 0.85 (95% CI 0.75–0.97) and 1.27 (95% CI 1.09–1.49), respectively.
Discussion
Prevalence
A systematic review reported that the prevalence of chronic low back pain is globally estimated to be 19.6% in those aged 20–59 years, although prevalence rates differed by definition, age, and other factors.17 In contrast, little is known about the prevalence of chronic knee pain, although some prevalence studies on knee osteoarthritis have been carried out.18 Kamada et al11 reported that prevalence rates of chronic low back and knee pain were 14.1% and 10.7%, respectively, in a Japanese population aged 40–79 years. These prevalence rates are slightly higher than those of the present study. This discrepancy may partly be due to differences in pain-assessment tools and age distribution of subjects.
The prevalence of musculoskeletal pain in global populations has been reported. For example, according to the World Health Organization’s Community Oriented Program for Control of Rheumatic Diseases project conducted mostly in developing countries,19 overall prevalence rates of low back and knee pain were 13% (n=66,543 in total) and 14% (n=47,888 in total), respectively. In contrast, three epidemiological studies in European countries (n=13,774 in total)20–22 showed higher overall prevalence of low back and knee pain (26% and 18%, respectively) in middle-aged individuals. Although these rates cannot directly be compared to our data, low back and knee pain appear to be a global health problem. In the paragraphs that follow, we discuss factors associated with the prevalence of chronic low back and knee pain. Comparisons between chronic low back and knee pain in relation to correlating factors identified in the present study are summarized in Table 4.
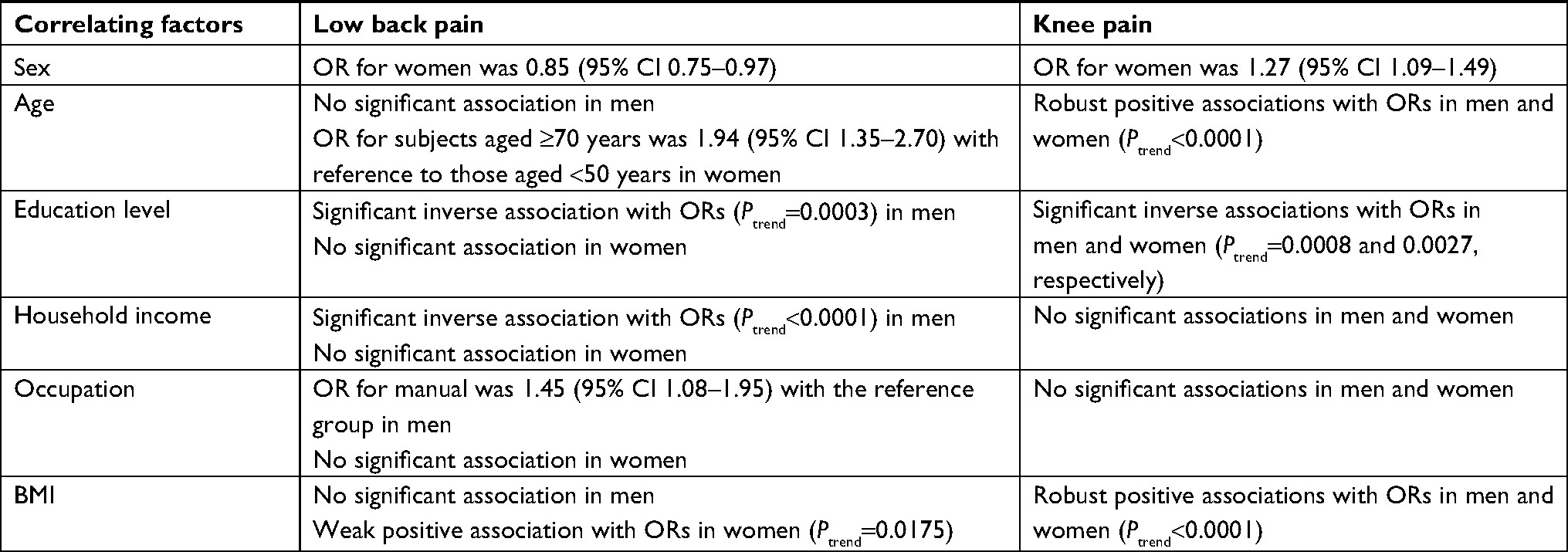 | Table 4 Summary of comparison between chronic low back and knee paina in relation to correlating factors of adjusted ORs Notes: ORs adjusted for all other variables. aModerate, severe, or very severe chronic pain as outcome. Abbreviation: BMI, body mass index. |
Age and sex
Older age was robustly associated with chronic knee pain in both sexes (Ptrend<0.0001) in the present study. This association is consistent with results of a previous report.23 However, age was not significantly associated with chronic low back pain in men. Dionne et al24 reported that the prevalence of chronic low back pain was generally high in working ages and tended to decrease thereafter. Therefore, the lack of association in the present study is in line with this phenomenon. In women, we found a significant increase in low back pain in the ≥70-year-old group. One possible explanation is that their low back pain was derived from farmwork, because many older women living in suburban, farming areas in Japan (including much of the Murakami region) do farm work,25 which is a risk factor of chronic low back pain.26 Chronic low back pain is a multifactorial disorder with possible etiologies other than physical factors, including psychological distress, anxiety, and depression,27 and thus should be further investigated in older women. In addition, we found a sex-based difference in the prevalence of chronic low back and knee pain, ie, prevalence of chronic low back pain was higher in men and prevalence of chronic knee pain was higher in women. This finding warrants sex-specific preventive measures and management of chronic pain.
Occupation
The prevalence of chronic low back pain in the manual-job group in men was significantly higher (adjusted OR 1.45) than the reference in the present study. This finding agrees with current knowledge that a heavy physical workload, such as heavy lifting, is a predictor of back pain.27 In contrast, we did not find a specific association between occupation and chronic knee pain, except in the male office-worker group, which had a small sample. Occupation has generally been considered a factor associated with knee pain or knee osteoarthritis.28 Recent evidence suggests that a heavy physical workload is not always a risk factor, but kneeling is an important element of physical work that can be a risk factor for knee pain and knee osteoarthritis.29 The present study did not find occupation to be a risk factor of chronic knee pain, and thus work posture should be taken into account in future studies.
Education level
We found that lower education level was significantly associated with prevalence of chronic low back and knee pain (except for female low back pain). Similarly, the 2009–2010 National Health and Nutrition Examination Survey conducted in the US found a dose-dependent, inverse association between education level and chronic low back pain.10 Leclerc et al30 also found such an association, and suggested that it could be explained by an intermediate effect of physical occupation as a pathway, ie, lower-education groups have occupations associated with a higher risk of chronic low back pain. The present study did not obtain detailed occupational information as a confounder, and consequently did not detect the confounding effect of this pathway. For association between education level and chronic knee pain, we found a robust link in both sexes. This is consistent with the results of a large Danish cohort study showing a dose-dependent, inverse association between education level and incidence of knee osteoarthritis.31 Similarly to chronic low back pain, factors related to occupation could potentially confound the association between education level and chronic knee pain.
Income
Household income level was inversely associated with chronic low back pain in men. Income is considered another sociodemographic characteristic, and a similar pathway as education may be involved. In addition to occupational factors, impaired psychological status, a risk factor of chronic low back pain,27 in low-income groups may be involved.
BMI
A large body of evidence has shown that overweight/obese status is associated with chronic knee pain and/or knee osteoarthritis,32–34 and our findings are consistent with this. Overweight/obese status is also reportedly associated with chronic low back pain.32,35 However, in the present study, there was no such association in men and only a weak association in women. This finding may be explained by the fact that Japanese individuals, including the present cohort, are slimmer and have a relatively lower prevalence of overweight/obese individuals compared to European and North American countries.36 This is supported by an international study showing the lack of an association between obesity and chronic low back pain in slimmer populations, including those in China, Ghana, and India.37 Nonetheless, our subgroup analyses demonstrated that BMI was associated with the prevalence of low back pain in elderly men and women (aged ≥60 years), suggesting that BMI may be a risk factor for low back pain only in older Japanese individuals.
Strengths and limitations
The present study is the first to report epidemiological profiles of chronic low back and knee pain in a large East Asian population. However, the study has some limitations. First, despite the large sample, the participation rate was not very high (41.3%). As such, the results may not be representative of the entire Japanese population. Second, profiles of chronic pain were based on a cross-sectional design, and thus should be confirmed with further cohort studies. Third, only anterior knee pain is shown as an option in Figure 1, suggesting that those with predominantly posterior knee pain may have not reported “having knee pain”. Therefore, the prevalence of knee pain may have been underestimated in this study. Finally, other confounding factors for chronic pain may exist, and these should be considered in future studies.
Conclusion
Nearly 14% of middle-aged and elderly individuals of the present cohort had chronic moderate–very severe pain of the low back or knee, and many demographic factors and body size were associated with the pain. This information could be useful in the development of a population-based preventive strategy for chronic low back and knee pain.
Acknowledgments
The authors acknowledge the Murakami Public Health Center, Murakami City Government, Sekikawa Village Government, and Awashimaura Village Government for their valuable support in data collection. This work was supported by JSPS Kakenhi grants JP23249035 and JP23790708, and the National Cancer Center Research and Development Fund (23-A31[toku]; since 2010).
Disclosure
The authors report no conflicts of interest in this work.
References
Unruh AM, Strong J, van Griensven H. Introduction to pain. In: van Griensven H, Strong J, Unruh AM, editors. Pain. 2nd ed. Edinburgh: Churchill Livingstone (Elsevier); 2014:1–7. | ||
Andrew R, Derry S, Taylor RS, Straube S, Phillips CJ. The costs and consequences of adequately managed chronic non-cancer pain and chronic neuropathic pain. Pain Pract. 2014;14(1):79–94. | ||
Goldberg DS, McGee SJ. Pain as a global public health priority. BMC Public Health. 2011;11:770. | ||
Fayaz A, Croft P, Langford RM, Donaldson LJ, Jones GT. Prevalence of chronic pain in the UK: a systematic review and meta-analysis of population studies. BMJ Open. 2016;6(6):e010364. | ||
Nakamura M, Nishiwaki Y, Ushida T, Toyama Y. Prevalence and characteristics of chronic musculoskeletal pain in Japan. J Orthop Sci. 2011;16(4):424–432. | ||
Takura T, Ushida T, Kanchiku T, et al. The societal burden of chronic pain in Japan: an internet survey. J Orthop Sci. 2015;20(4):750–760. | ||
Inoue S, Kobayashi F, Nishihara M, et al. Chronic pain in the Japanese community–prevalence, characteristics and impact on quality of life. PLoS One. 2015;10(6):e0129262. | ||
Hamano T, Kamada M, Kitayuguchi J, Sundquist K, Sundquist J, Shiwaku K. Association of overweight and elevation with chronic knee and low back pain: a cross-sectional study. Int J Environ Res Public Health. 2014;11(4):4417–4426. | ||
Kim W, Jin YS, Lee CS, Bin SI, Lee SY, Choi KH. Influence of knee pain and low back pain on the quality of life in adults older than 50 years of age. Pm R. 2015;7(9):955–961. | ||
Shmagel A, Foley R, Ibrahim H. Epidemiology of chronic low back pain in US adults: data from the 2009-2010 National Health and Nutrition Examination Survey. Arthritis Care Res (Hoboken). 2016;68(11):1688–1694. | ||
Kamada M, Kitayuguchi J, Lee IM, et al. Relationship between physical activity and chronic musculoskeletal pain among community-dwelling Japanese adults. J Epidemiol. 2014;24(6):474–483. | ||
Nakamura K, Takachi R, Kitamura K, et al. The Murakami cohort study of vitamin D for the prevention of musculoskeletal and other age-related diseases: a study protocol. Environ Health Prev Med. 2018;23(1):28. | ||
Eriksen J, Ekholm O, Sjøgren P, Rasmussen NK. Development of and recovery from long-term pain. A 6-year follow-up study of a cross-section of the adult Danish population. Pain. 2004;108(1–2):154–162. | ||
Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287–333. | ||
Ware JE Jr., Gandek B. The SF-36 health survey: development and use in mental health research and the IQOLA project. Int J Ment Health. 1994;23(2):49–73. | ||
Jensen MK, Sjøgren P, Ekholm O, Rasmussen NK, Eriksen J. Identifying a long-term/chronic, non-cancer pain population using a one-dimensional verbal pain rating scale: an epidemiological study. Eur J Pain. 2004;8(2):145–152. | ||
Meucci RD, Fassa AG, Faria NM. Prevalence of chronic low back pain: systematic review. Rev Saude Publica. 2015;49:73. | ||
Pereira D, Peleteiro B, Araújo J, Branco J, Santos RA, Ramos E. The effect of osteoarthritis definition on prevalence and incidence estimates: a systematic review. Osteoarthritis Cartilage. 2011;19(11):1270–1285. | ||
Davatchi F, Jamshidi AR, Tehrani Banihashemi A, et al. Effect of ethnic origin (Caucasians versus Turks) on the prevalence of rheumatic diseases: a WHO-ILAR COPCORD urban study in Iran. Clin Rheumatol. 2009;28(11):1275–1282. | ||
Picavet HS, Schouten JS. Musculoskeletal pain in the Netherlands: prevalences, consequences and risk groups, the DMC(3)-study. Pain. 2003;102(1–2):167–178. | ||
MacFarlane GJ, Norrie G, Atherton K, Power C, Jones GT. The influence of socioeconomic status on the reporting of regional and widespread musculoskeletal pain: results from the 1958 British Birth Cohort Study. Ann Rheum Dis. 2009;68(10):1591–1595. | ||
Hartvigsen J, Davidsen M, Hestbaek L, Sogaard K, Roos EM. Patterns of musculoskeletal pain in the population: a latent class analysis using a nationally representative interviewer-based survey of 4817 Danes. Eur J Pain. 2013;17(3):452–460. | ||
Noormohammadpour P, Mansournia MA, Koohpayehzadeh J, et al. Prevalence of chronic neck pain, low back pain, and knee pain and their related factors in community-dwelling adults in Iran: a population-based national study. Clin J Pain. 2017;33(2):181–187. | ||
Dionne CE, Dunn KM, Croft PR. Does back pain prevalence really decrease with increasing age? A systematic review. Age Ageing. 2006;35(3):229–234. | ||
Nakamura K, Kitamura K, Oshiki R, Kobayashi R, Saito T, Nishiwaki T. Prolonged occupational activity and 6-year changes in postural sway in elderly women. J Musculoskelet Neuronal Interact. 2015;15(1):78–82. | ||
Holmberg S, Thelin A, Stiernstrom E, Svardsudd K. The impact of physical work exposure on musculoskeletal symptoms among farmers and rural non-farmers. Ann Agric Environ Med. 2003;10(2):179–184. | ||
Manchikanti L, Singh V, Falco FJ, Benyamin RM, Hirsch JA. Epidemiology of low back pain in adults. Neuromodulation. 2014;17(Suppl 2):3–10. | ||
McWilliams DF, Leeb BF, Muthuri SG, Doherty M, Zhang W. Occupational risk factors for osteoarthritis of the knee: a meta-analysis. Osteoarthritis Cartilage. 2011;19(7):829–839. | ||
Silverwood V, Blagojevic-Bucknall M, Jinks C, Jordan JL, Protheroe J, Jordan KP. Current evidence on risk factors for knee osteoarthritis in older adults: a systematic review and meta-analysis. Osteoarthritis Cartilage. 2015;23(4):507–515. | ||
Leclerc A, Gourmelen J, Chastang JF, Plouvier S, Niedhammer I, Lanoë JL. Level of education and back pain in France: the role of demographic, lifestyle and physical work factors. Int Arch Occup Environ Health. 2009;82(5):643–652. | ||
Jørgensen KT, Pedersen BV, Nielsen NM, et al. Socio-demographic factors, reproductive history and risk of osteoarthritis in a cohort of 4.6 million Danish women and men. Osteoarthritis Cartilage. 2011;19(10):1176–1182. | ||
Anandacoomarasamy A, Caterson I, Sambrook P, Fransen M, March L. The impact of obesity on the musculoskeletal system. Int J Obes. 2008;32(2):211–222. | ||
Jinks C, Jordan KP, Blagojevic M, Croft P. Predictors of onset and progression of knee pain in adults living in the community. A prospective study. Rheumatology (Oxford). 2008;47(3):368–374. | ||
Zheng H, Chen C. Body mass index and risk of knee osteoarthritis: systematic review and meta-analysis of prospective studies. BMJ Open. 2015;5(12):e007568. | ||
Hussain SM, Urquhart DM, Wang Y, et al. Fat mass and fat distribution are associated with low back pain intensity and disability: results from a cohort study. Arthritis Res Ther. 2017;19(1):26. | ||
Zheng W, McLerran DF, Rolland B, et al. Association between body mass index and risk of death in more than 1 million Asians. N Engl J Med. 2011;364(8):719–729. | ||
Koyanagi A, Stickley A, Garin N, et al. The association between obesity and back pain in nine countries: a cross-sectional study. BMC Public Health. 2015;15:123. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.