Back to Journals » International Journal of Women's Health » Volume 18
Epidemiological Characteristics and Genotype Distribution of Human Papillomavirus Among Women of Different Ethnic Groups in the Yili Region: A Retrospective Study of 13,915 Women
Authors He H, Hou X, Bahtiyar H, Tuhetamishi M, Bian T ![]()
Received 10 April 2026
Accepted for publication 11 June 2026
Published 26 June 2026 Volume 2026:18 615155
DOI https://doi.org/10.2147/IJWH.S615155
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Huizi He,1,* Xiaoli Hou,1,* Hulkar Bahtiyar,1 Meier Tuhetamishi,1 Tingting Bian1,2
1Department of Pathology, Friendship Hospital of Ili Kazak Autonomous Prefecture, Yining, Xinjiang Uygur Autonomous Region, People’s Republic of China; 2Department of Pathology, Affiliated Hospital of Nantong University, Nantong, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tingting Bian, Email [email protected]
Objective: To analyze Human Papillomavirus (HPV) infection status and its association with cervical lesions among women of different ethnic groups in the Yili region (2021– 2023), providing evidence for local cervical cancer prevention.
Methods: Retrospective analysis of 13,915 women who underwent HPV genotyping and ThinPrep cytologic testing (TCT) at three hospitals. Among them, 1,240 with abnormal screening or clinical symptoms received cervical biopsy. SPSS 27.0 was used for statistical analysis.
Results: Overall HPV infection rate was 22.0% (3,068/13,915), with high-risk (HR-HPV) accounting for 87.2%. Age-specific rates showed a U-shaped pattern: highest in ≤ 24 years (39.3%), a second peak at 55– 64 years (27.9%), lowest at 45– 54 years (19.8%) (P< 0.001). Common genotypes: HPV16, 52, 42, 53, 51, 58. Among 7,490 women with ethnicity data, Kazakh women had the highest HPV infection rate (34.6%) and HR-HPV rate (30.1%), significantly higher than Han (27.7%), Uyghur (20.4%), and Hui (24.2%) (P< 0.001). However, after age adjustment, the difference was no longer statistically significant. Among 1,240 biopsy cases, HPV infection rates increased with lesion severity: chronic cervicitis (79.5%), cervical intraepithelial neoplasia (CIN) 1 (85.4%), CIN2 (97.3%), CIN3 (96.8%), cervical cancer (92.7%) (P< 0.001). HPV16 was the most common genotype in CIN2+ lesions, followed by HPV52 and HPV58.
Conclusion: HPV infection rate in Yili region is high (22.0%), predominantly HR-HPV (87.2%). The infection rate among Kazakh women was the highest, but the analysis adjusted by age showed no statistically significant difference. This suggests that they might be the key population for cervical cancer screening and prevention, but more evidence is needed to confirm this. Furthermore, hospital-based sampling may limit generalizability.
Keywords: human papillomavirus, genotype, Kazakh population, cervical lesions
Introduction
Cervical lesions primarily refer to epithelial abnormalities, including cervical intraepithelial neoplasia (CIN) and cervical cancer. Chronic cervicitis, an inflammatory condition rather than a true neoplastic lesion, was also included in this study for completeness. Cervical cancer ranks fourth among the most common cancers in women worldwide. In 2022 alone, there were approximately 661,000 new cases and over 348,000 deaths globally, with about 85% occurring in developing countries.1 In recent years, the incidence has continued to rise, posing a considerable threat to women’s health. Persistent infection with human papillomavirus (HPV) is recognized as the key factor in the development of cervical cancer, particularly high-risk HPV (HR-HPV) types.2 Across China, differences in economic conditions and ethnic composition vary widely from region to region, and so does the epidemiological pattern of HPV infection.3 Vaccination coverage also shows noticeable variation.4
Recent studies in Xinjiang have reported significant ethnic differences in HPV infection patterns. The Kazakh population showed distinct genotype distribution, with HPV53 as the major type, whereas HPV16 predominated in Uyghur, Han, and Hui groups5 Uyghur women exhibited lower HPV infection rates but higher cervical cancer incidence, possibly related to vaginal microecological imbalances.6 These ethnic-specific patterns highlight the need for targeted prevention strategies in the multi-ethnic Yili region.
Against this background, the present study focuses on a multi-ethnic population in the Yili region, examining HPV epidemiological characteristics from 2021 to 2023 and their association with cervical lesions. The aim is to provide evidence that may support the development of more tailored cervical cancer screening and vaccination strategies for women across different ethnic groups in this region.
Materials and Methods
Data Source
All included women underwent both HPV genotyping and ThinPrep cytologic testing (TCT), and had complete clinical records. A total of 13,915 cases were included in the analysis. Among them, 1,240 women with abnormal screening results or evident clinical symptoms underwent further evaluation by colposcopy and cervical histopathological biopsy.
Inclusion criteria: (1) no history of hysterectomy or gynecological malignancy; (2) not in menstruation, pregnancy, lactation, or acute genital tract inflammation; (3) no use of intravaginal medication within one week prior to testing; (4) informed consent obtained, with full cooperation throughout the study process.
Exclusion criteria: (1) no history of sexual activity; (2) prior history of cervical lesions, gynecological malignancy, or hysterectomy; (3) women in menstruation, pregnancy, or within 12 weeks postpartum (Royal College of Nursing (RCN)).
Among the 13,915 women, the racial data was complete for 7,490 individuals (accounting for 53.8%). The reasons for the missing racial information are as follows: (1) The local information system is not yet fully developed, and the correlation between racial information and treatment is not significant, so it was not continuously recorded; (2) Some data come from handwritten paper records, and the handwriting is difficult to read; (3) A small portion of electronic records have incomplete racial information entry. Therefore, when interpreting these results, consideration should be given to the possible selection bias caused by the missing data.
Reagents and Instruments
A 23-type human papillomavirus (HPV) genotyping detection kit (Yaneng Biotechnology [Shenzhen] Co., Ltd., China; registration No. 20193401918) was used in this study.7 The main instruments included a fully automated PCR gene amplification system (SLAN-96S, Shanghai Hongshi Medical Technology Co., Ltd.), an automated nucleic acid hybridization analyzer (YN-HR95, Yaneng Biotechnology [Shenzhen] Co., Ltd.), and an electronic colposcope (model SLC-2000B, Jinkewei, Shenzhen Huaxia Health Medical Technology Co., Ltd.).
HPV Genotyping
HPV genotyping was performed strictly according to the instructions of the 23-type detection kit, using a PCR-based reverse dot blot hybridization method. In brief—though the steps themselves are fairly standard—HPV DNA was first amplified in vitro and then hybridized for genotype identification.
High-risk HPV (HR-HPV) types are those with established or probable carcinogenic potential, which are associated with cervical cancer and high-grade cervical intraepithelial neoplasia, whereas low-risk HPV (LR-HPV) types are primarily associated with benign genital warts or mild cytological abnormalities. According to the International Agency for Research on Cancer (IARC) classification criteria,8 HR-HPV types included those classified as IARC Group 1 (carcinogenic to humans), Group 2A (probably carcinogenic), or Group 2B (possibly carcinogenic), specifically HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, and 82. LR-HPV types, which are not classified as carcinogenic by IARC, included HPV6, 11, 42, 43, 81, and 83. The procedure involved DNA extraction, hybridization, membrane washing, color development, and result interpretation. Based on the results, HPV genotypes were classified as negative, low-risk, or high-risk (HR-HPV).
Histopathological Examination
Cervical biopsy specimens obtained under colposcopy were fixed in neutral formaldehyde, followed by routine processing—tissue sampling, dehydration, embedding, sectioning, and hematoxylin–eosin (HE) staining. Slides were then reviewed by experienced pathologists at the attending physician level or above.
Histopathological diagnosis of cervical lesions was made in accordance with the World Health Organization (WHO) Classification of Female Genital Tumours (2020).9 The diagnostic categories included chronic cervicitis, CIN grades 1–3, and cervical cancer (including cervical adenocarcinoma and squamous cell carcinoma).
Statistical Analysis
All data were first entered and organized in Excel, where both general information—such as name, ethnicity, and age—and study-specific variables, including HPV genotypes, TCT results, and cervical histopathological findings, were compiled into a structured database. Based on this dataset, the results were subsequently summarized and presented in tables and figures.
For statistical processing, IBM SPSS Statistics 27.0 was used. Categorical variables were expressed as n (%), and group comparisons were performed using the chi-square test. To address potential confounding in ethnic comparisons, multivariable logistic regression was performed with HPV infection, HR-HPV infection, and LR-HPV infection as binary outcomes, ethnicity as the main independent variable, and age as an adjusted covariate. Multiple testing was corrected using the Benjamini–Hochberg false discovery rate (FDR) method, with Bonferroni correction provided as a conservative sensitivity approach. The significance level was set at α = 0.05, and a P value < 0.05 was considered statistically significant.
Results
Distribution of HPV Infection Across Different Age Groups
In this cohort of 13,915 cases, cervical HPV positivity was identified in 3,068 individuals, corresponding to an overall infection rate of 22.0% (3,068/13,915). Within the HPV-positive population, HR-HPV constituted 87.2% (2,676/3,068), whereas low-risk HPV (LR-HPV) accounted for 12.8% (392/13,915).
To look more closely at age-related patterns, the population was stratified into six groups (≤24, 25–34, 35–44, 45–54, 55–64, and ≥65 years). Across these groups, infection rates were 39.3% (116/295), 23.6% (776/3,285), 20.1% (915/4,556), 19.8% (823/4,147), 27.9% (353/1,263), and 23.0% (85/369), respectively. What stands out is not a steady decline or increase, but rather a U-shaped pattern.
The ≤24-year group showed the highest infection rate. Next came the 55–64-year group, followed—though not in a strictly linear order—by the 25–34, ≥65, and 35–44-year groups, while the lowest rate appeared in the 45–54-year group.
When these age groups were compared statistically, the overall difference proved significant (χ2 = 245.6, P < 0.001). After applying Bonferroni correction for multiple comparisons, no significant difference was found between the 35–44 and 45–54-year groups. Similarly, comparisons between the ≥65-year group and the 25–34, 35–44, and 45–54-year groups did not reach statistical significance. The remaining pairwise comparisons, however, were statistically significant (χ2 = 103.691, P < 0.001).
Turning to high-risk types, the highest HR-HPV infection rate was again observed in the ≤24-year group. In descending order, the proportions were: ≤24 years (34.6%, 102/295), 55–64 years (24.3%, 307/1,263), ≥65 years (21.1%, 78/369), 25–34 years (21.0%, 689/3,285), 35–44 years (17.3%, 787/4,556), and 45–54 years (17.2%, 713/4,147).
Across age groups, differences in HR-HPV infection were statistically significant (χ2 = 95.23, P < 0.001). In contrast, LR-HPV infection did not show a significant association with age (P > 0.05). See Table 1 and Figure 1.
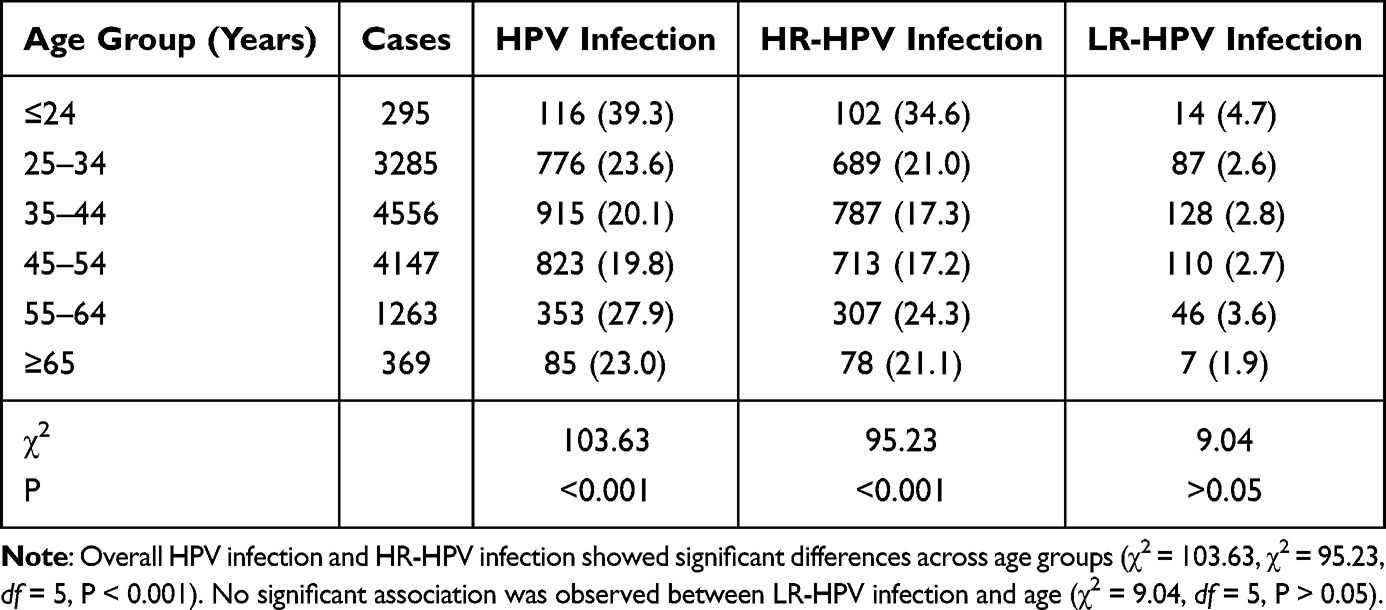 |
Table 1 Distribution of HPV Infection and Risk Types Across Different Age Groups [n (%)] |
 |
Figure 1 Age-specific distribution of HPV infection rates by risk type HPV positivity rate (%), high-risk HPV (HR-HPV) rate, and low-risk HPV (LR-HPV) rate across six age groups (≤24, 25–34, 35–44, 45–54, 55–64, ≥65 years). The highest overall infection rate was observed in the ≤24-year group (39.3%), followed by the 55–64-year group (27.9%). |
Ethnic Distribution of the Study Population and HPV Infection Status
Among the 13,915 cases included in the study, 6,425 cases with incomplete ethnic information were excluded. The remaining 7,490 cases were analyzed to assess differences in HPV infection among ethnic groups in this multi-ethnic region.
In terms of distribution, the largest proportion of HPV-infected individuals was found in the Han population (39.1%, 2,926/7,490), followed by the Uyghur population (34.2%, 2,564/7,490), the Kazakh population (15.3%, 1,144/7,490), the Hui population (6.9%, 516/7,490), and other ethnic minorities (4.5%, 340/7,490), including Mongolian, Xibe, Dongxiang, Kirgiz, Uzbek, Manchu, Russian, Zhuang, Tatar, and Tibetan populations. See Figure 2.
 |
Figure 2 Ethnic distribution of the study population Proportion of each ethnic group among the 7,490 women with complete ethnicity data. Han: 39.1% (2,926/7,490); Uyghur: 34.2% (2,564/7,490); Kazakh: 15.3% (1,144/7,490); Hui: 6.9% (516/7,490); other ethnic minorities: 4.5% (340/7,490). |
A further comparison focused on the four major ethnic groups in the Yili region—Han, Uyghur, Kazakh, and Hui—examining overall HPV infection, HR-HPV infection, and LR-HPV infection, as well as differences among these groups. The pattern is quite clear: both high-risk and LR-HPV infection rates were highest in the Kazakh population and lowest in the Uyghur population.
Specifically, HPV infection rates were 27.7% (812/2,926) in the Han population, 20.4% (524/2,564) in the Uyghur population, 34.6% (396/1,144) in the Kazakh population, and 24.2% (125/516) in the Hui population. The differences among ethnic groups were statistically significant (χ2 = 108.45, P < 0.001). After adjusting for age using multivariable logistic regression, compared with the Han population, the Uyghur population had a significantly lower odds of HPV infection (adjusted-OR = 0.65, 95% CI: 0.52–0.80, P < 0.001), and the Hui population also showed lower odds (adjusted-OR = 0.61, 95% CI: 0.38–0.95, P = 0.038). The Kazakh population showed higher odds, but the difference did not reach statistical significance (adjusted-OR = 1.47, 95% CI: 0.92–2.27, P = 0.094). The global P value for ethnicity was < 0.001, indicating overall significant differences across groups after age adjustment (Supplementary Table 1).
For HR-HPV, the corresponding infection rates were 25.0% (731/2,926) in Han, 18.0% (462/2,564) in Uyghur, 30.1% (344/1,144) in Kazakh, and 21.5% (111/516) in Hui populations, again showing statistically significant differences (χ2 = 94.72, P < 0.001).
As for LR-HPV, infection rates were 2.8% (81/2,926) in Han, 2.4% (62/2,564) in Uyghur, 4.5% (52/1,144) in Kazakh, and 2.7% (14/516) in Hui populations. Differences across ethnic groups remained statistically significant (χ2 = 20.15, P < 0.001). See Table 2.
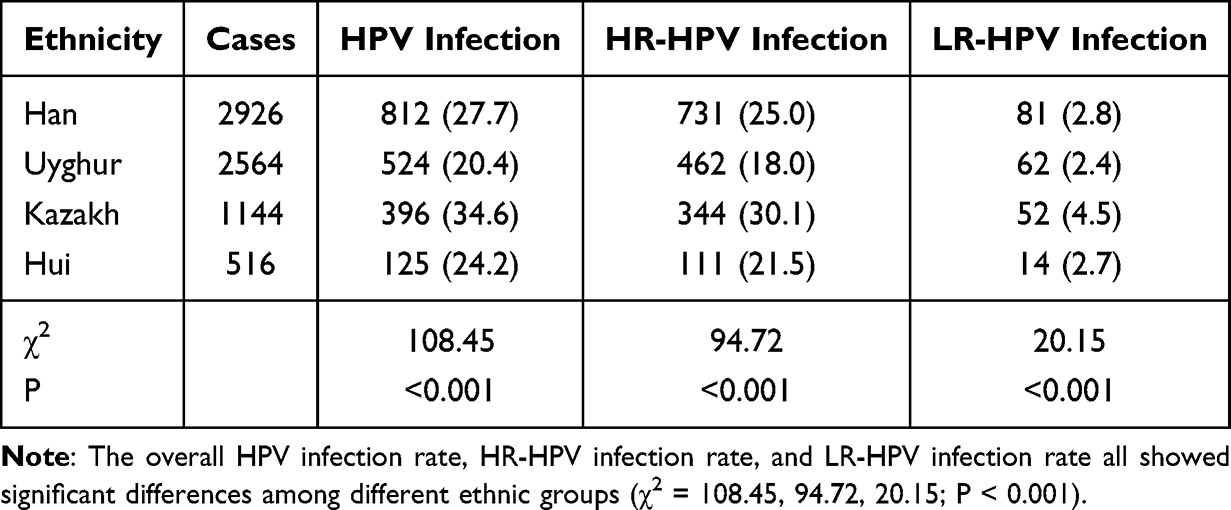 |
Table 2 Distribution of HPV Infection and Risk Types by Ethnicity [n (%)] |
Distribution of Single and Multiple HPV Infections Across Ethnic Groups
Among the 3,068 HPV-positive cases, single-type infection was observed in 2,246 cases, accounting for 73.21% of all positive cases. Multiple infections were less common, and when they did occur, double infection was the most frequent pattern, with 574 cases (18.71%). This was followed by triple infection (171 cases, 5.57%), quadruple infection (53 cases, 1.73%), quintuple infection (19 cases, 0.62%), sextuple infection (4 cases, 0.13%), and, rarely, ten-type infection (1 case, 0.03%). Single infection clearly predominated, while high-order multiple infections were uncommon. See Figure 3.
 |
Figure 3 Distribution of single and multiple HPV infections among 3,068 HPV-positive cases Single infection accounted for 73.21% (2,246/3,068). Among multiple infections, double infection was the most common (18.71%, 574/3,068), followed by triple (5.57%), quadruple (1.73%), quintuple (0.62%), sextuple (0.13%), and ten-type (0.03%) infections. |
Across the Han, Uyghur, Kazakh, and Hui populations, HPV infection was mainly in the form of single-type infection. The proportion of single infection was highest in the Han population at 74.8% (607/812), followed by the Uyghur population at 71.9% (377/524), the Kazakh population at 67.2% (266/396), and the Hui population at 66.7% (89/125).
As for multiple infection, the highest rate was observed in the Kazakh population at 32.8% (130/396), followed by the Hui population at 28.8% (36/125), the Uyghur population at 28.1% (147/524), and the Han population at 25.2% (205/812).
However, when comparing across ethnic groups, neither the distribution of single infection nor that of multiple infection showed statistically significant differences (χ2 = 7.69, P > 0.05). See Table 3.
 |
Table 3 Distribution of Single and Multiple HPV Infections Across Ethnic Groups [n (%)] |
Distribution of HPV Genotypes Across Different Age Groups and Ethnicities
As noted above, some HPV-positive cases involved multiple infections. In the genotype-specific analyses (Table 4 and Table 5), each HPV genotype detected in a woman with multiple infections was counted separately for that genotype. Consequently, a woman infected with more than one HPV type contributed to the count of each respective genotype. Thus, among the 13,915 cases included in this study, a total of 4,248 HPV genotype detections were recorded. Of these, 3,463 were high-risk types, accounting for 81.5% of all detected genotypes, while 785 were low-risk types (18.5%).
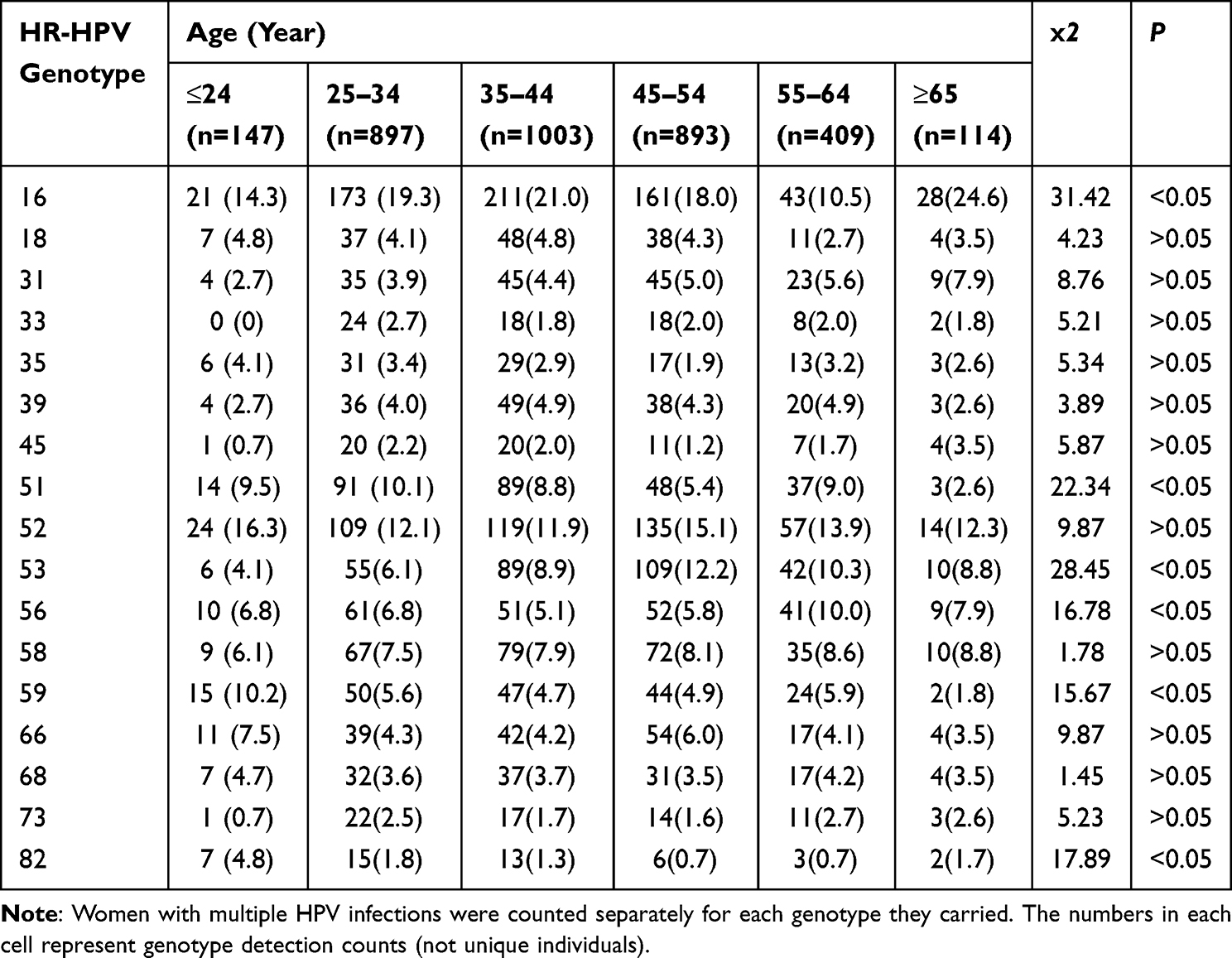 |
Table 4 Age-Specific Distribution of HR-HPV Genotypes [n (%)] |
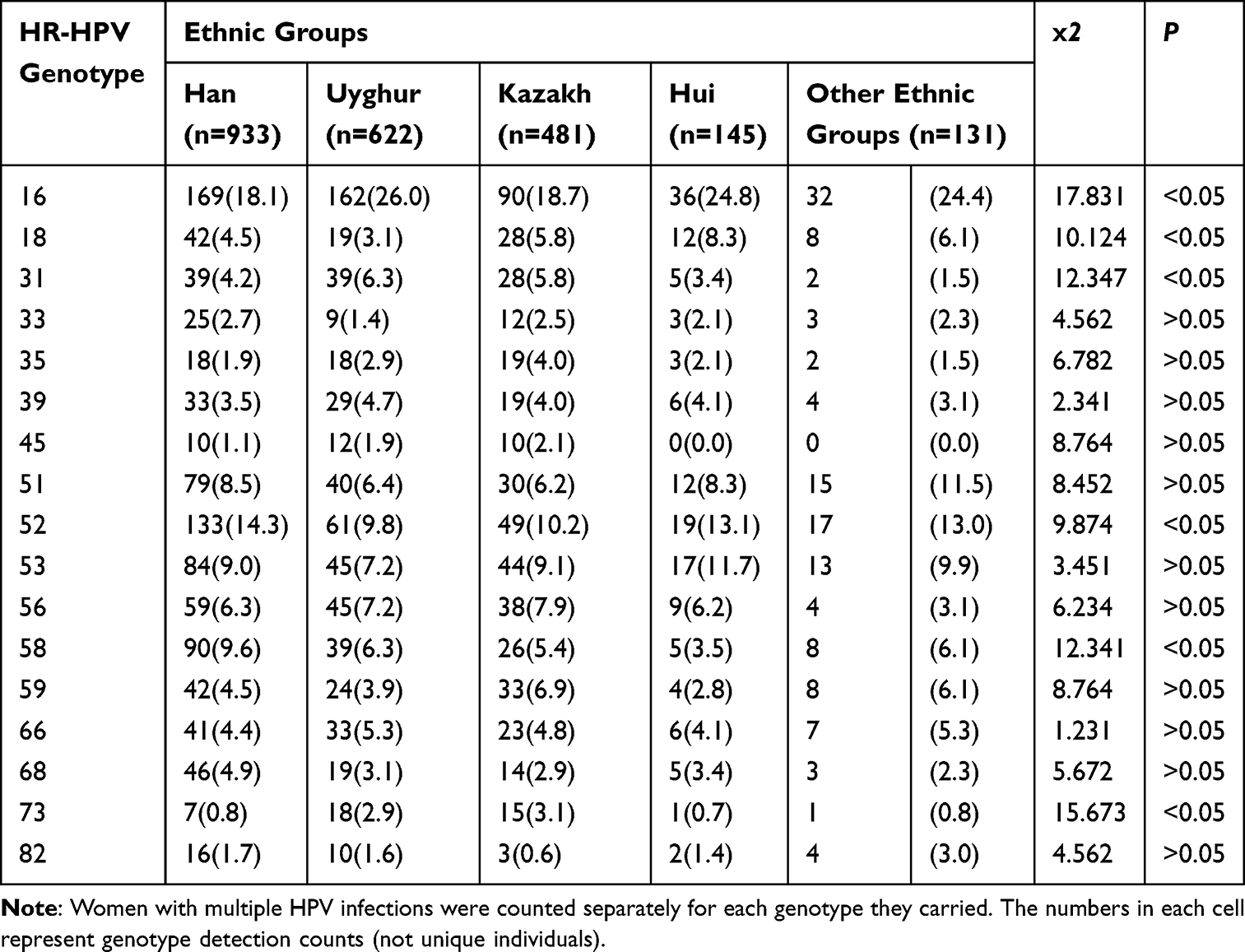 |
Table 5 Ethnic Distribution of HR-HPV Genotypes [n (%)] |
To further examine how HR-HPV genotypes were distributed across age groups, the data were organized and analyzed in tabular form. The dominant genotypes varied somewhat by age. In the ≤24-year group, HPV52, 16, and 59 were most common; in the 25–34-year group, HPV16, 52, and 51 predominated. For those aged 35–44 and 45–54 years, HPV16, 52, and 53 were the main types. In the 55–64-year group, HPV52, 16, and 53 were most frequently detected. Among individuals aged ≥65 years, HPV16, 52, and 53/58 (tied for third) were the principal types. See Table 4.
Across all detected genotypes, HPV16 was the most frequent, with 637 cases (15.0%). This was followed by HPV52 (458 cases, 10.8%), HPV42 (316 cases, 7.4%), HPV53 (311 cases, 7.3%), and HPV51 (282 cases, 6.6%).
Given that HR-HPV types accounted for a markedly higher proportion than low-risk types, further analysis was conducted to explore differences in HR-HPV genotype distribution across ethnic groups. The patterns were not identical. In the Han population, HPV16, 52, and 58 were most common; in the Uyghur population, HPV16, 52, and 53/56 (tied for third) predominated. In both the Kazakh and Hui populations, HPV16, 52, and 53 were the main genotypes, whereas in other ethnic groups, HPV16, 52, and 51 were most frequently observed.
Chi-square analysis showed that certain HR-HPV genotypes—specifically types 16, 18, 31, 52, 58, and 73—differed significantly in their distribution among ethnic groups (P < 0.05). However, to correct for multiple comparisons, we applied the Benjamini–Hochberg false discovery rate (FDR) correction. After FDR correction, only HPV16 (P = 0.023) and HPV73 (P = 0.030) remained statistically significant. Other genotypes, including HPV18, HPV31, HPV52, and HPV58, did not retain significance after correction (all adjusted P > 0.05) (Supplementary Table 2). For example, HPV16 infection was highest in the Uyghur population (26.0%) and lowest in the Han population (18.1%). HPV18 showed the highest rate in the Hui population (8.3%) and the lowest in the Uyghur population (3.1%). HPV31 was most frequent in the Uyghur population (6.3%) and least frequent in other ethnic groups (1.5%). HPV52 and HPV58 both reached their highest rates in the Han population (14.3%) and lowest in the Uyghur population (9.8%). HPV73 was most common in the Kazakh population (3.1%) and least common in the Hui population (0.7%).
By contrast, no statistically significant differences were observed among ethnic groups for HR-HPV types 33, 35, 39, 45, 51, 53, 56, 59, 66, 68, and 82 (P ≥ 0.05), suggesting that ethnic factors had limited influence on the distribution of these genotypes. See Table 5.
Association Between Cervical Lesion Grades and HPV Infection
Among the 13,915 participants included in this study, 1,240 women with abnormal screening results and/or obvious clinical symptoms underwent further examination by colposcopy and cervical histopathological biopsy. In these 1,240 biopsy cases, 586 cases of chronic cervicitis were identified (47.3%), along with 364 cases of CIN1 (29.4%), 111 cases of CIN2 (9.0%), 124 cases of CIN3 (10.0%), and 55 cases of cervical cancer (4.4%) (see Table 6). The occurrence of high-grade lesions (CIN2 and above, including CIN2, CIN3, and cervical cancer) showed a trend across age groups—highest in the ≥65-year group, followed by the 55–64, 25–34, 35–44, ≤24, and 45–54-year groups. The ≥65-year group had the highest rate (40.4%). In contrast, low-grade lesions (chronic cervicitis and CIN1) were more frequent than high-grade lesions in all age groups. See Figure 4. When the distribution of cervical lesion grades across age groups was analyzed using the chi-square test, the differences were statistically significant (χ2 = 84.68, P < 0.05).
 |
Table 6 Age-Specific Distribution of Cervical Lesions [n (%)] |
 |
Figure 4 Age-specific distribution of cervical lesion incidence Proportions of low-grade lesions (chronic cervicitis + CIN1) and high-grade lesions (CIN2 + CIN3 + cervical cancer) across age groups. High-grade lesions were most frequent in the ≥65-year group (40.4%). See Table 6 for detailed case numbers. |
Further analysis focused on HPV infection status in women with different cervical lesions (see Table 7). Among the 1,240 cases, HPV infection was detected in 1,056 cases, giving an infection rate of 85.2%. HR-HPV infection was present in 1,006 cases (81.1%), while LR-HPV infection was found in 50 cases (4.7%). As lesion severity increased—from chronic cervicitis to cervical cancer—the HPV infection rate showed an overall upward trend (from 75.5% to 97.3%), though a slight decrease was observed in CIN3 and cervical cancer (from 96.8% to 92.7%), possibly influenced by abnormal bleeding affecting result interpretation. A similar pattern was observed for HR-HPV infection, which increased with lesion severity (from 71.1% to 94.6%), reaching 90.9% in cervical cancer cases. In contrast, LR-HPV infection remained low across all groups (1.8%–5.5%) and did not show a clear trend. Chi-square analysis showed significant differences in overall HPV infection rates among different cervical lesion groups (χ2 = 43.44, P < 0.001), as well as in HR-HPV infection rates (χ2 = 41.23, P < 0.001). However, no significant association was found between LR-HPV infection and lesion severity (χ2 = 6.09, P > 0.05).
 |
Table 7 Distribution of HPV Infection and Risk Types in Different Cervical Lesions [n (%)] |
Further analysis was performed on the distribution of different cervical lesions across ethnic groups (see Table 8). Chi-square tests for each lesion type showed that chronic cervicitis, CIN1, CIN2, and CIN3 did not differ significantly among ethnic groups (P > 0.05). In contrast, cervical cancer showed a different pattern: the proportion was higher in the Han population (45.5%) and lower in other ethnic groups (for example, only 3.6% in other minorities), with a statistically significant difference among ethnic groups (P < 0.05).
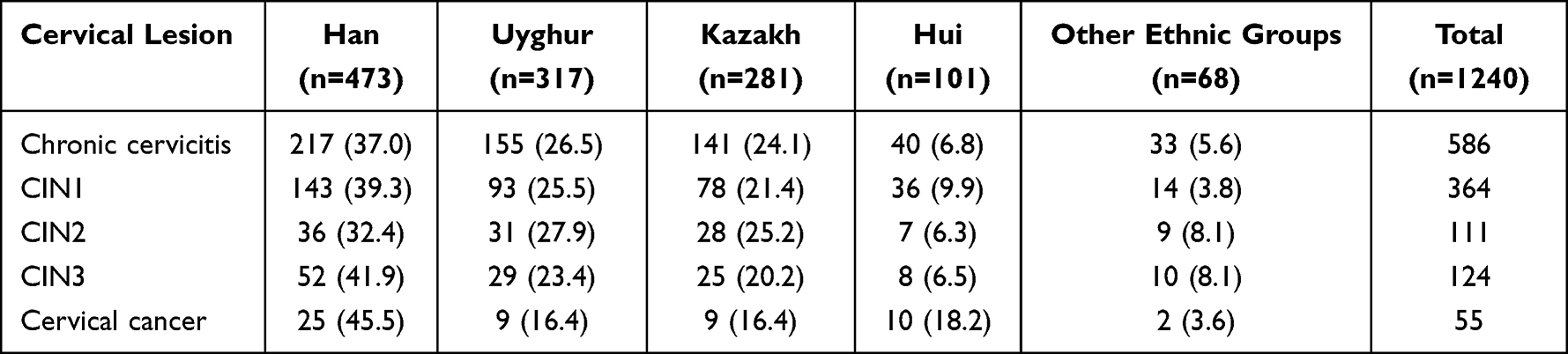 |
Table 8 Distribution of Cervical Lesions Across Ethnic Groups [n (%)] |
Discussion
Cervical cancer is a malignancy with a clearly defined etiology and, importantly, one that can be prevented and controlled. In practice, two pillars tend to be emphasized—HPV vaccination and standardized cervical cancer screening. As screening programs have become more widely implemented in recent years, both cervical cancer and its precancerous lesions are being detected earlier, allowing for earlier intervention; accordingly, both incidence and mortality have shown a noticeable decline.10 Epidemiological investigations of HPV infection suggest that its distribution is not uniform. Differences can be observed across regions and populations.11,12 Persistent infection with HR-HPV is generally considered a key driver of cervical carcinogenesis, and more than 90% of women with cervical cancer have a history of HPV infection.13 Based on a cross-sectional survey conducted among women of different ethnic groups in the Yili region from 2021 to 2023, the present study attempts—at least in part—to provide evidence that may inform local strategies for HPV vaccination and cervical cancer prevention.
HPV infection does not present identically across regions. In this study, the overall infection rate in the Yili region was 22.0%, with high-risk types accounting for 87.2% of HPV-positive cases. Compared with reports from other regions in China, these values appear somewhat higher: for example, Chengdu14 reported an HPV infection rate of 20.73% with 65.70% high-risk types, Xianyang15 21.55% with 83.78% high-risk types, and Guangzhou16 21.66% with 86.01% high-risk types. At the genotype level, previous global data have identified HPV16, 18, 31, 58, and 52 as the most common types,17 while a large-scale Chinese study involving 1.7 million individuals reported HPV16, 52, 58, 18, and 33 as the predominant types.18 In the present study, however, the most common genotypes in the Yili region were HPV16, 52, 53, 51, and 58. HPV16 remained the dominant type, consistent with earlier findings. What differs somewhat is the relatively high proportion of HPV52, 53, and 51. This discrepancy may relate to factors such as viral genetic diversity, ethnic composition, lifestyle patterns, and vaccination coverage. It also raises the hypothesis that, in this region, vaccines covering a broader range of high-risk types, such as quadrivalent or nonavalent vaccines, or even region-specific formulations, might provide broader coverage than bivalent vaccines targeting HPV16/18 alone, although further studies are needed to confirm this.
Age-related differences in HPV infection were also evident. In Guangzhou, for instance, the age distribution of cervical HPV infection has been described as bimodal.11 In contrast, the present study showed a U-shaped pattern across age groups. The highest HPV infection rate in the ≤24-year group (39.3%) aligns with recent national data. A nationwide study of 33.7 million Chinese women reported that participants under 20 years had the highest infection burden (81.46%).19 Another analysis of 2.7 million women confirmed a bimodal age distribution with the first peak in women under 21 years.20 Young women are at peak sexual activity, leading to increased HPV exposure, but most infections are transient and self-clear, which is why screening is recommended from age 25 years.21 These findings underscore the need to improve HPV vaccination coverage among adolescents in the Yili region. In contrast, although sexual activity tends to decrease in women aged 55–64 years, the risk of HPV infection appears to rise again. This secondary peak may be related to hormonal changes, alterations in the vaginal microenvironment, and reduced immune function, all of which may impair the clearance of HPV infection.22 From a clinical perspective, this underscores the need to strengthen screening and vaccination efforts in high-risk populations, as well as to emphasize regular follow-up to prevent persistent infection and subsequent lesion development.
Marked differences were also observed among ethnic groups. In the Yili region, the main ethnic populations—Han, Uyghur, Kazakh, and Hui—showed significantly different HPV infection rates. The Kazakh population had the highest rate (34.6%), exceeding that of Han (27.7%), Uyghur (20.4%), and Hui (24.2%) populations. These values are somewhat higher than those reported in previous studies, where HPV infection rates in the Kazakh population ranged from 12.88% to 27.89%.23–25 A similar pattern was observed for HR-HPV infection, with the Kazakh population again showing the highest rate (30.1%), compared with 25.0% in Han, 18.0% in Uyghur, and 21.5% in Hui populations. Differences were also noted in the distribution of specific HR-HPV genotypes: HPV16 showed the highest infection rate in the Uyghur population (26.0%) and the lowest in the Han population (18.1%); HPV52 and HPV58 were most frequent in the Han population (both 14.3%) and lowest in the Uyghur population (both 9.8%); HPV18 was highest in the Hui population (8.3%) and lowest in the Uyghur population (3.1%). These findings suggest that ethnicity may be associated with differences in genotype distribution, although residual confounding cannot be ruled out. Such differences are likely multifactorial. Genetic susceptibility may vary among ethnic groups.25 In addition, disparities in awareness of cervical health, participation in routine screening, and access to timely intervention may contribute. In rural and pastoral areas—where the Kazakh population is relatively concentrated—vaccination coverage tends to be lower. Cultural practices related to marriage and hygiene may also influence HPV exposure and clearance. Kazakh women showed the highest crude prevalence and may warrant further surveillance; however, age-adjusted analysis did not confirm ethnicity as an independent determinant of HPV infection. Public health strategies could therefore consider focusing on improving vaccination coverage and screening participation in this group, alongside culturally appropriate health education.
The relationship between HPV infection and cervical lesion severity was also evident. Among the 1,240 biopsy cases, the overall HPV infection rate was 85.2%, with HR-HPV accounting for 81.1% and LR-HPV for 4.0%. Infection rates across lesion grades were as follows: chronic cervicitis (79.5%), CIN1 (85.4%), CIN2 (97.3%), CIN3 (96.8%), and cervical cancer (92.7%). HPV infection, particularly with high-risk types, is closely linked to the development of CIN and cervical cancer.26 In this study, HR-HPV infection increased with lesion severity—from 74.1% in chronic cervicitis to 97.3% in cervical cancer—again supporting the role of persistent HR-HPV infection as a key driver of cervical lesion progression. Regarding genotype-specific associations with lesion severity, HPV16 was the most common genotype in high-grade lesions (CIN2+), followed by HPV52 and HPV58. These findings reinforce the central role of HR-HPV testing in cervical cancer screening in this region.
Within the framework of China’s national “Action plan for accelerating the elimination of cervical cancer (2023–2030)” action plan,27 one of the most pressing challenges in the Yili region remains the relatively low vaccination coverage. Although HPV vaccination was incorporated into the national immunization program in 2025, and efforts to strengthen the vaccination capacity at the primary level have been accelerated, significant disparities still persist at the local level. The present findings suggest that screening resources could be more strategically allocated, with particular attention to populations at higher risk—especially Kazakh women and those with a higher likelihood of lesion progression. Improving accessibility in remote areas and minority-dominated pastoral regions, while addressing vaccine hesitancy and enhancing screening awareness, might represent key steps toward more effective cervical cancer prevention, although further implementation research is needed.
Several limitations should be acknowledged. First, ethnicity data were incomplete: only 7,490 of 13,915 women (53.8%) had complete ethnicity information, which may introduce selection bias. Second, there is a validation bias. Only 1,240 women with abnormal screening results or clinical symptoms were subjected to cervical biopsies, while those with normal screening results did not undergo biopsies. This selective validation may lead to an overestimation of the HPV infection rate and the strength of the association between HPV infection and cervical lesions. Third, although age-adjusted multivariable logistic regression was performed, no adjustment was made for socioeconomic or other potential confounders. Therefore, the observed differences should be interpreted as associations rather than causal effects. Finally, the hospital-based sample may limit generalizability to the general population.
In conclusion, this retrospective study of 13,915 women in the Yili region reveals an overall HPV prevalence of 22.0% (2021–2023), with high-risk genotypes accounting for 87.2%. The most common genotypes were HPV16, 52, 42, 53, 51, and 58. The Kazakh population showed a higher HPV infection rate (34.6%) than the Han, Uyghur, and Hui populations. Although age-adjusted multivariable logistic regression was performed, no adjustment was made for socioeconomic or other potential confounders; therefore, these findings should be interpreted as associations rather than causal effects of ethnicity. Given the incomplete ethnicity data (7,490/13,915) and verification bias, future population-based studies with comprehensive multivariable adjustment (including socioeconomic factors) are needed to confirm these associations and guide targeted prevention strategies for the Kazakh population.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethical Statement
This study was approved by the Ethics Committee of Yili Kazakh Autonomous Prefecture Friendship Hospital (Approval No. RMB2024-26), and the data were confirmed to be reliable. All subjects signed the consent form before participation in the study. The study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study is supported by Science and Technology Program of Ili Kazakh Autonomous Prefecture(YJC2024B14).
Disclosure
Dr Huizi He reports Support for the manuscript from Science and Technology Program of Ili Kazakh Autonomous Prefecture (YJC2024B14), during the conduct of the study, outside the submitted work. The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–13. doi:10.3322/caac.21834
2. Karnik M, Tulimilli SV, Anantharaju PG, et al. An overview of the mechanisms of hpv-induced cervical cancer: the role of kinase targets in pathogenesis and drug resistance. Cancers. 2026;18(2).
3. Li S, He X, Li S, Su Y, Wang X, Li C. The prevalence of HPV in Chongqing, China from 2017 to 2022: a retrospective cohort study. Sci Rep. 2024;14(1):23973.
4. Chen J, Zhang Z, Pan W, et al. Estimated Human Papillomavirus Vaccine Coverage Among Females 9-45 Years of Age - China, 2017-2022. China CDC Wkly. 2024;6(19):413–417. doi:10.46234/ccdcw2024.080
5. Ma J, Yang M, Huang G. Human papillomavirus prevalence and genotype distribution among women with cervical cytological Abnormalities in Urumqi, Xinjiang, China. Diagn Cytopathol. 2025;53(7):315–324. doi:10.1002/dc.25467
6. Shi Y, Dong XY, Yimingjiang M, et al. The association between human papillomavirus infection, vaginal microecology, and cervical intraepithelial neoplasia in women from Xinjiang, China. J Obstet Gynaecol Res. 2024;50(6):982–990. doi:10.1111/jog.15932
7. Yin J, Cheng S, Liu D, et al. Head-to-head comparison of 7 high-sensitive human papillomavirus nucleic acid detection technologies with the SPF10 LiPA-25 system. J Natl Cancer Cent. 2022;2(3):148–154.
8. Humans IWGotEoCRt. Biological agents. IARC Monogr Eval Carcinog Risks Hum. 2012;100(Pt B):1–441.
9. Hohn AK, Brambs CE, Hiller GGR, May D, Schmoeckel E, Horn LC. who classification of female genital tumors. geburtshilfe frauenheilkd. 2021;81(10):1145–1153. doi:10.1055/a-1545-4279
10. Chen D, Shao W, Zhou Y, Pan Y. Investigation and analysis of human papillomavirus type 81 52 detection in 12,713 women. Maternal Child Health Care of China. 2024;39(12):2245–2248.
11. Zhang Z. A Study on the HPV Infection Status of Women in Guangzhou Area and Its Correlation with Cervical Lesions. Guangzhou Medical University; 2022.
12. Li P. A Retrospective Analysis of HPV Infection Status Among Women in Qiannan Bouyei and Miao Autonomous Prefecture and Its Correlation with Cervical Lesions. Jilin University; 2023.
13. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
14. Yao X, Liu M, Ren J, Gou T. Epidemiological characteristics of 30,929 cases of human papillomavirus infection in Chengdu. J Mol. Diagn. Ther. 2025;17(9):1796–1799.
15. Xu P, Liu Y, Wang M. The current situation and genotype analysis of human papillomavirus infections in 1587 female individuals in Xianyang City. Maternal Child Health Care of China. 2025;40(8):1376–1379.
16. Yang X, Li Y, Tang Y, et al. Cervical HPV infection in Guangzhou, China: an epidemiological study of 198,111 women from 2015 to 2021. Emerg Microbes Infect. 2023;12(1):e2176009. doi:10.1080/22221751.2023.2176009
17. de Sanjose S, Diaz M, Castellsague X, et al. Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: a meta-analysis. Lancet Infect Dis. 2007;7(7):453–459. doi:10.1016/S1473-3099(07)70158-5
18. Li S, Li M, Cong Q. Chinese expert consensus on clinical application of human papilloma virus vaccine. Chin. J. Front. Med. Sci. 2021;13(2):1–12.
19. Li X, Sun Y, Lun X, Liang Y, Jin R, Liu J. Trends and patterns of human papillomavirus infection among 33.7 million women in mainland China from 2015 to 2025: a nationwide observational study. J Infect. 2026;92(5):106732. doi:10.1016/j.jinf.2026.106732
20. Han S, Lin M, Liu M, et al. Prevalence, trends, and geographic distribution of human papillomavirus infection in Chinese women: a summative analysis of 2,728,321 cases. BMC Med. 2025;23(1):158. doi:10.1186/s12916-025-03975-6
21. Fontham ETH, Wolf AMD, Church TR, et al. Cervical cancer screening for individuals at average risk: 2020 guideline update from the American Cancer Society. CA Cancer J Clin. 2020;70(5):321–346. doi:10.3322/caac.21628
22. Bruni L, Diaz M, Castellsague X, Ferrer E, Bosch FX, de Sanjose S. Cervical human papillomavirus prevalence in 5 continents: meta-analysis of 1 million women with normal cytological findings. J Infect Dis. 2010;202(12):1789–1799. doi:10.1086/657321
23. Lv X, Lu J, Chen H, Zhou Z, Zheng M. Study on the Status of Cervical Human Papillomavirus Infection among 337 Kazak and 1000 Han Women in Kui-tun Area. Heilongjiang Med. J. 2022;46(15):1873–1876.
24. Zeng Y, He W, Meng C. Analysis of HPV infection genotype subtypes among different ethnic groups of women in urumqi area. Int J Lab Med. 2020;41(10):1769–1772.
25. Shi Y, Dong X, Yimingjiang M, Ma W, Ma Z. Analysis on HPV genotyping and quantitative detection results among 11 654 women in Urumqi city. Lab Med Clinic. 2024;21(12):1697–1703.
26. Dai S, Xu Q, Qin Q. Research progress of human papillomavirus infection and cervical intraepithelial neoplasia in gynecological cervical exami-nation. Chin. J. Fam. Plann. 2023;31(5):1232–1236.
27. Commission NH, Education M, MoC A, et al. Action plan for accelerating the elimination of cervical cancer(2023-2030). Chin. J. Viral Dis. 2023;13(4):243–244.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.