Back to Journals » Risk Management and Healthcare Policy » Volume 14
Epidemiological Characteristics and Core Containment Measures of Imported COVID-19 Cases from Abroad in Early Phase in Guangdong, China
Authors Chen H, Shi L, Zhang Y, Wang X, Sun G ![]()
Received 28 April 2021
Accepted for publication 16 September 2021
Published 21 September 2021 Volume 2021:14 Pages 3955—3963
DOI https://doi.org/10.2147/RMHP.S317910
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Haiqian Chen,1 Leiyu Shi,2 Yuyao Zhang,1 Xiaohan Wang,1 Gang Sun1
1Department of Health Management, School of Health Management, Southern Medical University, Guangzhou, Guangdong, 510515, People’s Republic of China; 2Department of Health Policy and Management, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD, 21205, USA
Correspondence: Gang Sun
Department of Health Management, School of Health Management, Southern Medical University, Guangzhou, Guangdong, 510515, People’s Republic of China
Tel +86 14103189758
Email [email protected]; [email protected]
Objective: This study aimed to analyze the distribution characteristics and influencing factors for the interval between entering mainland China and the diagnosis of imported COVID-19 cases in Guangdong province, in order to provide valuable experience for global pandemic in prevention and control.
Methods: We collected publicly reported data between March 1 and June 2, 2020. Univariate and multivariate regression analyses were performed to identify the significant associated factors with the interval between entering mainland China and diagnosis of imported COVID-19 cases.
Results: As of June 2, 2020, a total of 200 imported cases were reported in Guangdong province. The average interval time was 4.25 days with a median of 2 days, the interval time of 68% cases was between 1 and 3 days. The multivariate model results show that the three following factors were critical influencing factors: nationality was foreign nationality (P = 0.037), results of initial nucleic acid detection were negative (P = 0.000) and the interval between entering mainland China and the detection of positive results (T) exceeded two days (P = 0.008).
Conclusion: The results suggested that all travelers and returning resident should be taken strict sampling and testing, and isolation measures, improved the accuracy of the initial nucleic acid test results, and the detection efficiency and shortening the interval between entering mainland China and detection of positive results.
Keywords: COVID-19, imported cases, Guangdong province, containment measures
Introduction
The coronavirus disease 2019 (COVID-19) was first detected in late December 2019 in Wuhan, China. COVID-19 is different from the coronaviruses causing severe acute respiratory syndrome (SARS) and the Middle East respiratory syndrome (MERS) and it can be further spread rapidly through asymptomatically infected persons.1,2 The World Health Organization (WHO) has declared the COVID-19 outbreak as a pandemic on March 11, 2020,3 which posed a severe challenge to the global public health and the world economy. As of June 7, 2020, there have been confirmed more than 6.8 million cases and nearly 399,000 deaths reported worldwide.4
In the early stage of the COVID-19 outbreak, the Chinese government took unprecedented nonpharmaceutical public health measures to contain the spread of COVID-19, which stabilizing the epidemic in China. While the epidemic has continued to spread globally, the complexity and high volume of international air travel has allowed the virus to spread rapidly. Continued, unwitting virus importation through air travelers could lead to large-scale community transmission without adequate control measures.5 Moreover, during the peak of the European pandemic in March–April 2020, the prevalence of SARS-CoV-2 positivity among air passengers was as high as 3–6%.6 Therefore, the imported cases will pose a huge challenge for China, and the imported cases epidemic prevention and control were particularly important for China. Besides, between March 1 and June 2, 2020, a total of 2415 new confirmed cases were reported in China, and the imported cases were 1762, accounting for 72.96%.7 This indicated that it is especially important to prevent and control imported cases from abroad.
Early detection, early reporting, and early isolation can effectively prevent and control the spread of imported cases in China. Also, studies showed that strictly strengthening the transmission mechanism of COVID-19 and the protection against the COVID-19 among returnees can prevent the occurrence of secondary transmission from travelers.8,9 And the time interval between entry and confirmation is an important basis for measuring the early and late detection of imported cases. Guangdong province is a coastal province in southern China, and adjacent to Hong Kong and Macao, with developed foreign trade and close foreign exchanges. So Guangdong province has a greater risk than other provinces or cities of China in the epidemic of imported COVID-19 cases. Our study aimed to analyze the distribution characteristics and influencing factors for the interval between entering mainland China and the diagnosis of imported COVID-19 cases from March 1 to June 2, 2020, and provide valuable experience for global pandemic prevention and control.
Materials and Methods
Variable Identification and Data Collection
All the data in this study were obtained from the official data released by the Guangdong Provincial Health Commission (http://wsjkw.gd.gov.cn/). Data were collected from March 1 through June 2, 2020. Next, we collected data on the web-page of the Guangdong Provincial Health Commission. The following variables were collected: age, gender, nationality, health status at the time of entry, occupation, results of initial nucleic acid detection, the method of case screening (active inspection by customs and relevant departments, seek medical advice actively, and investigated as close contacts), the interval between entering mainland China and detection of positive results (T), time of entering mainland China, type of quarantine (designated quarantine point, quarantine in hospital, quarantine at home, and no quarantine), confirmation time.
The COVID-19 confirmed cases are defined according to the diagnostic criteria for the COVID-19 prevention and control protocol (trial version 7), which was published by the National Health Commission.10 Viral nucleic acid detection using real-time polymerase chain reaction (RT-PCR) assay, which has been developed and used for detection of SARS-CoV-2 rapidly.11 The PCR technology faces the challenge of “false negative” results, but in the balance of sensitivity and specificity, compared to some rapid detection methods, the best balance is still RT-PCR detection technology. From the past major outbreaks, whether it is Ebola virus in West Africa, influenza A or Middle East Respiratory syndrome, RT-PCR is still the country’s first test method. And confirmation time is the interval between entering mainland China and the final clinical diagnosis.
Statistical Analysis
The data of imported COVID-19 cases were sorted out by Excel 2013 and set up a database. Enumeration data were expressed by frequency and percentage, while the measurement data were expressed by mean±standard deviation. Mann–Whitney U-test and Kruskal–Wallis H-test were used, respectively, to compare whether the difference was statistically significant in the time interval between two groups and multiple groups. A binary logistic regression model was used for multivariate analysis, the standard of confirmation time was whether it was exceeded 4 days, which was based on the average interval time between entering mainland China and diagnosis was 4.25 days. Two hundred cases were divided into two groups: the late detection group (denoted as 1) and the reference group (denoted as 0). Influencing factors with statistical significance in univariate analysis were included as independent variables in the logistic regression model for analysis, and variable screening was performed by the Forward LR method. All statistical analyses were done using the user-coded, syntax-based interface of SPSS Version 20.0. A p-value of 0.05 or less was considered statistically significant.
Results
A total of 200 imported COVID-19 cases from abroad were confirmed in Guangdong province between March 1 to June 20, 2020. The first imported COVID-19 case was confirmed in Shenzhen city, Guangdong province on March 1, 2020.12 Figure 1 shows that there is a trend of new imported COVID-19 cases in Guangdong province. The imported COVID-19 cases were mainly concentrated between mid-late March and mid-early April. In May and June, the new imported COVID-19 cases were less than 2. Figure 2 shows that the interval between entering mainland China and diagnosis was skewed distribution, the average interval was 4.25 days, the median interval was 2 days, the maximum was 23 days and the minimum was 0 days. The interval focused on 1 day, 2 days, and 3 days with 17.5%, 37%, and 13.5%, respectively.
 |
Figure 1 The prevalence of new imported COVID-19 cases in Guangdong province. |
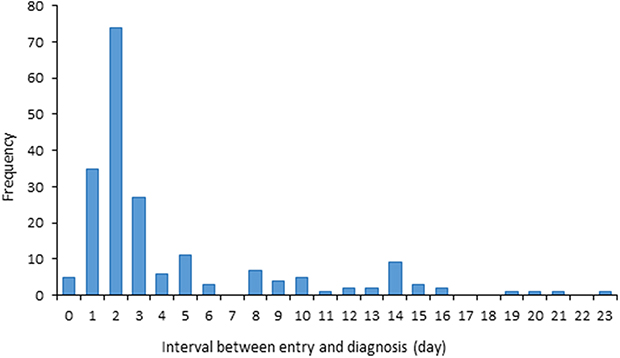 |
Figure 2 Frequency distribution of the interval between entering mainland China and diagnosis of imported COVID-19 cases in Guangdong province. |
Table 1 shows that among the 200 imported cases, 126 were male (63%) with a median age of 31.57 years (range: 2 to 70 years). Most of the imported cases were Chinese overseas students (38%) and businessmen or workers (35%). Chinese nationality accounted for 81% of imported cases, the source of infection from the United Kingdom, the United States, the Philippines, and France represented 61.5% of the imported cases from overseas. Most of the imported cases were present asymptomatic (79.5%) before they arrived in Guangdong. In total, 78% of the imported cases entered mainland China at Guangzhou Baiyun International Airport and 14% of the imported cases entered Shenzhen Bay Port. Among the 200 imported cases, most of them were reported in Guangzhou and Shenzhen, which accounted for 67% and 19.5%, respectively.
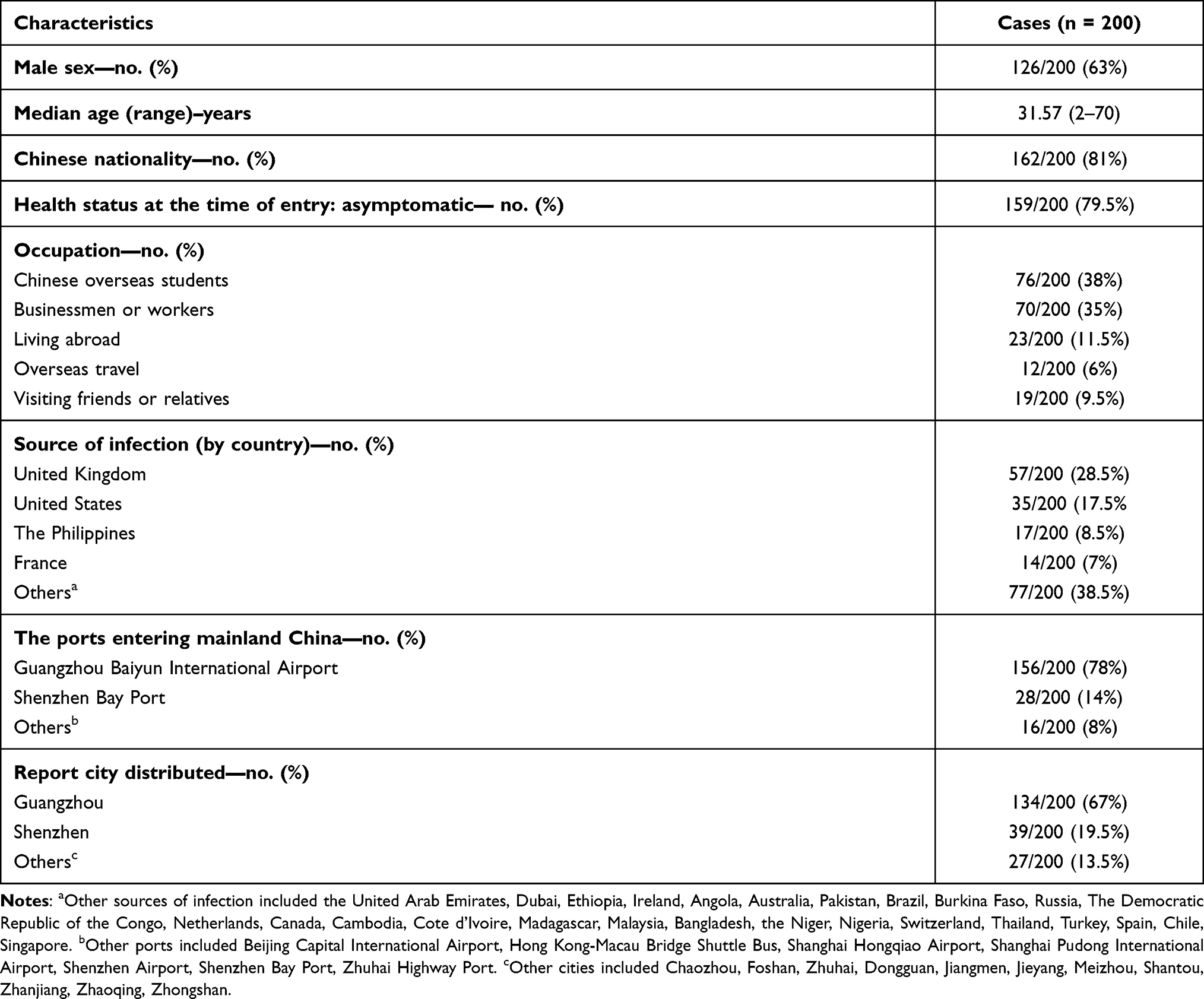 |
Table 1 Demographic Characteristics of the Imported COVID-19 Cases from Abroad in Guangdong Province, Confirmed Between March 1 and June 20, 2020 |
Table 2 shows the results of univariate analyses for factors associated with the interval between entering mainland China and the diagnosis of imported COVID-19 cases. The univariate analysis of confirmation time shows that the following factors were influenced the confirmation time: Nationality (P = 0.000), the type of quarantine (P = 0.000), health status at the time of entry (P = 0.000), results of initial nucleic acid detection (P = 0.000), the method of case screening (P = 0.035), the place of entering mainland China (P = 0.001) and the interval between entering mainland China and detection of positive results (T). However, the following factors were not relative to the confirmation time: gender (P = 0.515), age (P = 0.079) and personnel category (P = 0.153).
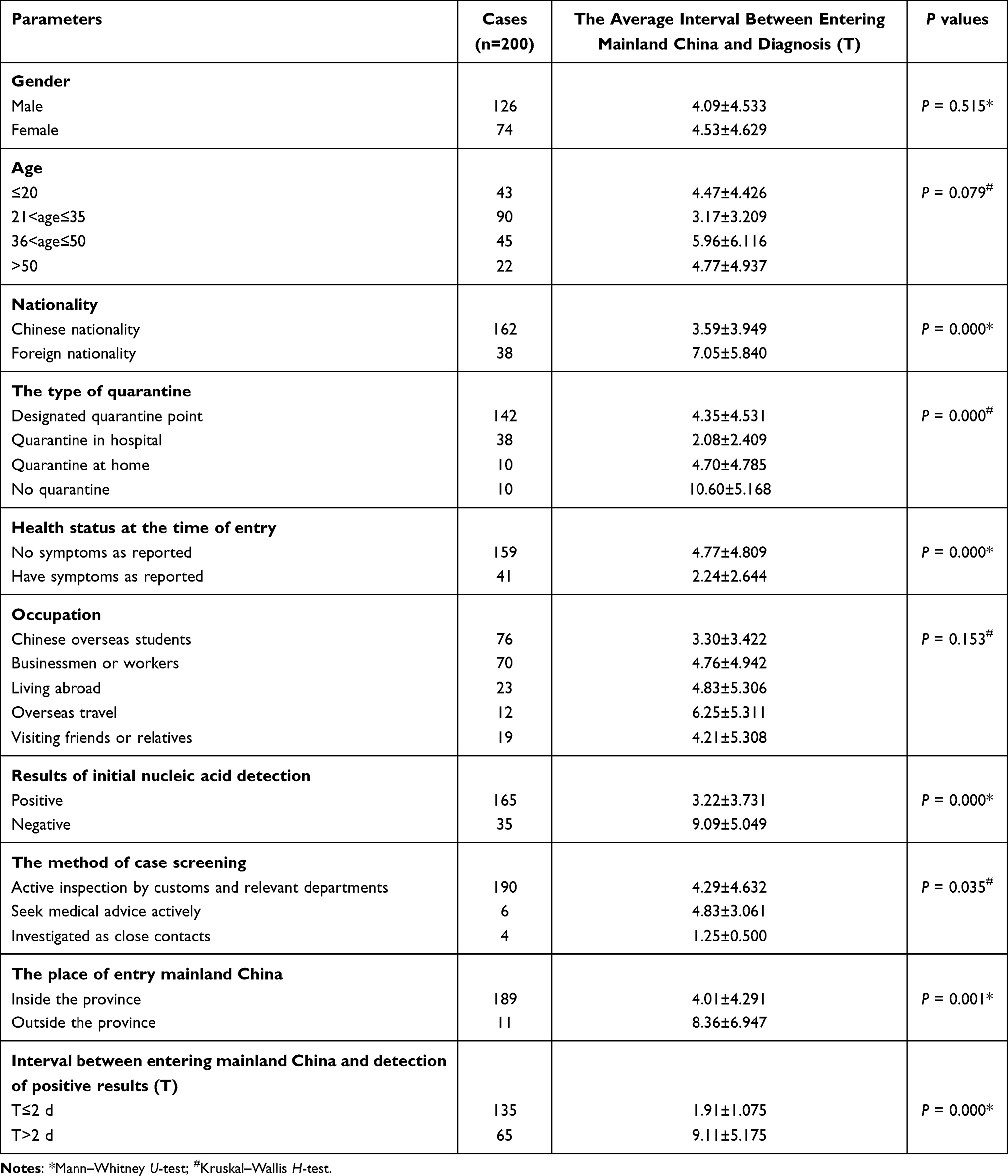 |
Table 2 Univariate Analyses for Factors Associated with Interval Between Entering Mainland China and Diagnosis of Imported COVID-19 Cases in Guangdong Province (Mean±SD) |
Table 3 shows the results of multivariate logistic regression analyses for factors associated with the interval between entering mainland China and the diagnosis of imported COVID-19 cases. The independent variables with statistically significant differences (nationality, the type of quarantine, health status at the time of entry, results of initial nucleic acid detection, the place of entry mainland China, and interval between entering mainland China and detection of positive results) in the univariate analysis of Table 2 were included in the multivariate logistic regression model for analysis. Multivariate logistic regression analysis shows that a logistic regression model excluded three following factors: the type of quarantine, the health status at the time of entry, and the place of entering mainland China. The independent variables that finally entered the equation were nationality, the interval between entry to mainland China and detection of positive results (T), and results of initial nucleic acid detection. Among them, the nationality was foreign (P = 0.037), the initial nucleic acid test result was negative (P = 0.000), the interval between entering mainland China and detection of positive results (T) > 2d (P = 0.008) were risk factors for late detection of imported COVID-19 cases.
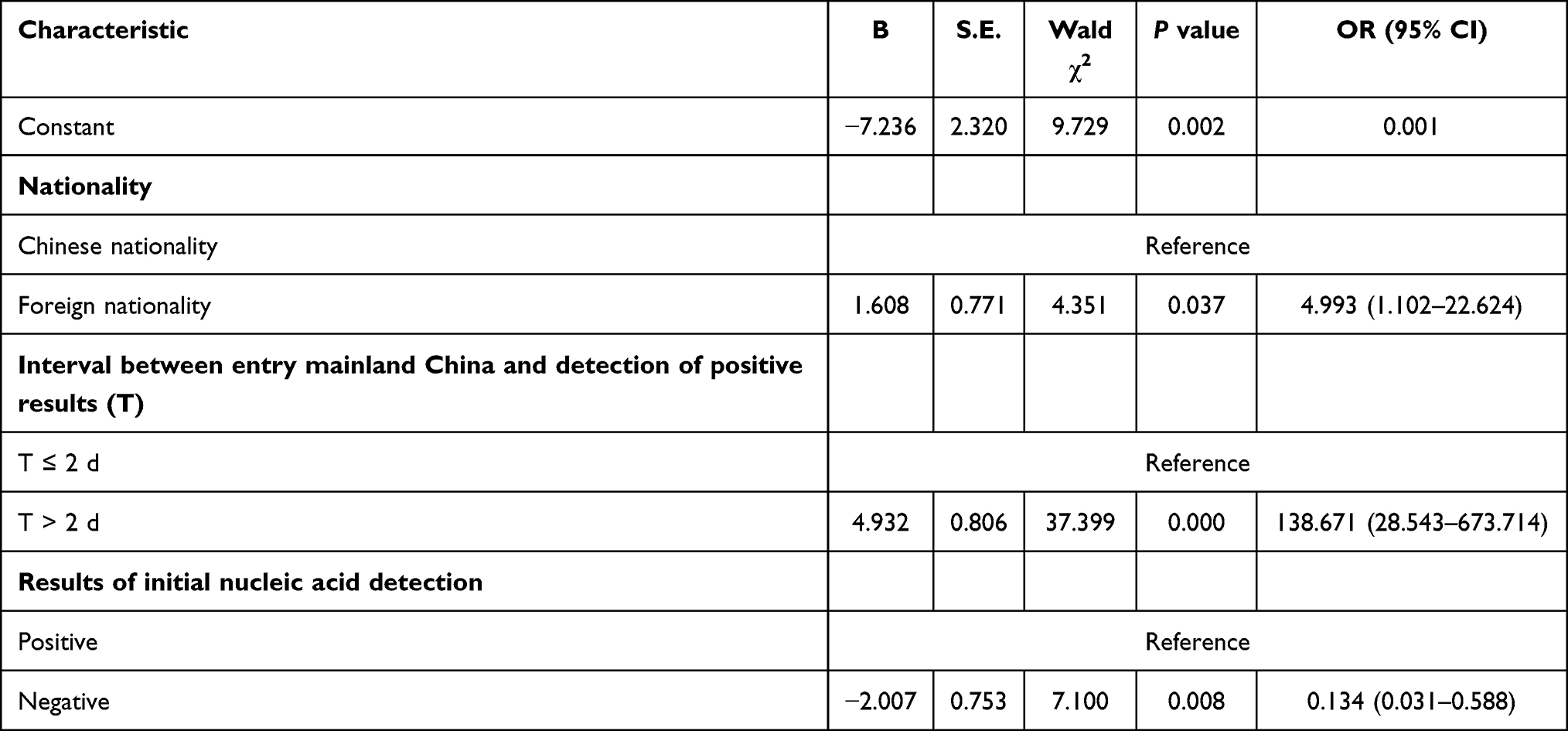 |
Table 3 Multivariate Logistic Regression Analyses for Factors Associated with Interval Between Entering Mainland China and Diagnosis of Imported COVID-19 Cases in Guangdong Province |
Discussion
In the past several months when China was fighting against the COVID-19 pandemic, China adopted the most thorough, rigorous, and comprehensive prevention and control measures, unprecedentedly enforced quarantine and isolation, and mobilized medical resources across China. It has ensured that all those in need have been tested, quarantined, hospitalized, or treated. With these measures in place, China has prevented a wider spread and further development of the virus.13 On March 18, 2020, China’s new local confirmed cases achieved first zero reporting, and China’s epidemic prevention and control efforts have also shifted from local cases transmission to imported cases transmission.14 Therefore, it is crucial to control the epidemic of imported COVID-19 cases, and early detection, early reporting, and early isolation can contain the transmission of the epidemic in mainland China. Moreover, the experiences of Singapore, South Korea, and Taiwan and Hong Kong, China in early imported cases from abroad have shown that timely inbound temperature and symptom screening, isolation, close contact tracing, under strict enforcement of these measures and aggressive border control measures are effective in preventing COVID-19 community transmission.5,15,16
The SARS-CoV-2 positive nucleic acid test is a crucial standard for the detection and confirmation of COVID-19 cases.10 Furthermore, a study showed that rapid and accurate testing of clinical samples dictates the effective response.17 Our study found that the interval between entering mainland China and detection of positive results (T) was an important influencing factor for the diagnosis of imported COVID-19 cases. The risk of late diagnosis in the T > 2 days group was significantly higher than that in the T ≤ 2 days group. The average interval time in the T > 2 days group was 9.11 days, which was much greater than 1.91 days in the T ≤ 2 days group. The interval between entering mainland China and detection of positive results (T) is close relative to the time of sample collection. Therefore, we should shorten the time of sample collection and improve the efficiency of testing, which can prevent the spread of the epidemic within China.
However, the COVID-19 has a longer incubation period and the median incubation period of COVID-19 was 3.0 days (range, 0 to 24.0 days), which lead to most COVID-19 patients had no obvious symptoms or mild symptoms in the early stage.18 Besides, the previous studies have shown that asymptomatic persons infected with the SARS-CoV-2 virus were infectious and might subsequently become symptomatic.19–21 Therefore, all travels or returning residents who entered Guangdong province through immigration checkpoints should be required real-time reverse transcription-polymerase chain reaction (rRT-PCR) test and subjected to a 14-day quarantine, similarly to what Singapore did. If these travelers and residents do not present with symptoms and are tested negative for SARS-COV-2 after 14 days of isolation, they will be released from isolation.1,22 Our study also found that the results of initial nucleic acid detection were an important influencing factor for the interval between entering mainland China and diagnosis of imported cases. The risk of late diagnosis in the negative initial nucleic acid tests was significantly higher than positive, and the average interval between initial negative nucleic acid tests was 9.09 days, which was much greater than 3.22 days of positive tests. Thus, it is necessary to take samples for nucleic acid testing and screening in time. However, the late confirmed cases were due to the initial negative nucleic acid test, and some inbound travelers have been negative many times during the entry nucleic acid test. This means that those who were negative for the initial nucleic acid test must be rechecked multiple times, and imaging results of clinical symptoms can be combined to speed up the diagnosis during the screening and diagnosis process. However, to prevent community transmission caused by imported cases from outside China, all inbound persons, whether positive or negative nucleic acid test results, are subjected to a 14-day quarantine observation and multiple nucleic acid tests that on the first, seventh and 14th days are performed during the observation period.23
Besides, nationality was a crucial factor for the interval between entering mainland China and diagnosis of imported cases. For the risk of late diagnosis of imported COVID-19 cases, foreign nationality is higher than Chinese nationality. The average interval time of foreign nationality between entering mainland China and diagnosis was 7.05 days, which is greater than 3.59 days of Chinese nationality. Thus, the local government required that all travelers and returning residents, whether Chinese or foreign nationality, should take strict sample collection, test nucleic acid, and quarantine for 14 days. Meanwhile, it is necessary to strictly prevent major entry-exit ports and strengthen the inspection of entry-exit personnel to control the spread of the imported cases. Implementing strict sampling inspection and isolation measures can speed up the imported COVID-19 cases confirmed.24 Moreover, Guangdong Province has been strictly enforcing the “five lines of defense” policy of port quarantine, medical observation and isolation points, community screening, fever clinics, and hospital treatment for all inbound personnel, with a closed-loop management of the whole process.23 Meanwhile, a study of imported cases from abroad in Shanghai showed that the closed-loop management model of the joint prevention and control mechanism at the port was effective in detecting and managing imported cases from abroad.25
There are limitations in the present study that epidemiological investigations have recall bias, especially the difficulty in judging the source of infection at the origin place, and clinical symptom indicators may be further improved. Nevertheless, our study analyzes the distribution characteristics and influencing factors for the interval between entering mainland China and the diagnosis of imported COVID-19 cases in Guangdong province, the findings could provide valuable experience for the global pandemic in preventing and controlling the imported COVID-19 cases.
Conclusion
The study found that the interval between entering mainland China and detection of positive results (T), the results of initial nucleic acid detection, and nationality were critical factors for the interval between entering mainland China and diagnosis of imported cases. So, the following policy measures were suggested to implement. First, strengthening the prevention and control of major entry-exit ports. All travelers and returning residents, whether Chinese or foreign nationality, should be taken strict sampling and testing, and isolation measures. All inbound personnel needs closed-loop management with nucleic acid testing and 14-day quarantine observation. During the quarantine observation period, nucleic acid tests will be carried out on the first, seventh, and 14th days. Second, improving the accuracy of the initial nucleic acid test results, which can avoid false-negative results lead to cannot confirm imported cases in time. The initial nucleic acid test must be retested several times and can be combined with clinical symptoms imaging findings during the screening and diagnosis process to speed up the diagnosis. Third, improving the detection efficiency and shortening the interval between entering mainland China and detection of positive results. So, Nucleic acid testing samples should be delivered early, frequently, and quickly.
Paper Context
The COVID-19 pandemic is continuing to spread worldwide. After the COVID-19 outbreak, China took unprecedented nonpharmaceutical public health measures to contain the spread of COVID-19. This study found that nationality was foreign nationality, results of initial nucleic acid detection were negative, and the interval between entering mainland China and detection of positive results (T) exceeded two days influenced the interval between entering mainland China and diagnosis of imported COVID-19 cases in Guangdong province.
Ethics and Consent
This study did not involve ethical issues.
Acknowledgments
The authors gratefully acknowledge the financial support provided by the National Social Science Fund of China (No. 16BGL184).
Funding
The National Social Science Fund of China (No. 16BGL184).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Zhang Z-B, Li L, Qin P-Z, et al. Countries of origin of imported COVID-19 cases into China and measures to prevent onward transmission. J Travel Med. 2020;27(8):8. doi:10.1093/jtm/taaa139
2. Li Z, Chen Q, Feng L, et al. Active case finding with case management: the key to tackling the COVID-19 pandemic. Lancet. 2020;396(10243):63–70.
3. World Health Organization. WHO Director-General’s opening remarks at the media briefing on COVID-19-11; March, 2020. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020.
4. COVID-19 Case Tracker. Follow global cases and trends. Updated daily. Available from: https://coronavirus.jhu.edu/?from=groupmessage.
5. Liu JY, Chen TJ, Hwang SJ. Analysis of imported cases of COVID-19 in Taiwan: a nationwide study. Int J Environ Res Public Health. 2020;17:9.
6. Zhang Z-B, Li L, Qin P-Z, et al. Countries of origin of imported COVID-19 cases into China and measures to prevent onward transmission. J Travel Med. 2020;27:8.
7. GotRo K All about Korea’s Response to COVID-19; 2020. Available from: http://www.mofa.go.kr/viewer/skin/doc.html?fn=20201021031300238.pdf&rs=/viewer/result/202103.
8. Chiew CJ, Li Z, Lee VJ. Reducing onward spread of COVID-19 from imported cases: quarantine and ‘stay at home’ measures for travellers and returning residents to Singapore. J Travel Med. 2020;27(3):taaa049.
9. Dickens BL, Koo JR, Lim JT, et al. Strategies at points of entry to reduce importation risk of COVID-19 cases and reopen travel. J Travel Med. 2020;27:8.
10. Wong JEL, Leo YS, Tan CC. COVID-19 in Singapore-current experience: critical global issues that require attention and action. JAMA. 2020;323(13):1243–1244.
11. Xiang F, Wang X, He X, et al. Antibody detection and dynamic characteristics in patients with coronavirus disease 2019. Clin Infect Dis. 2020;71(8):1930–1934.
12. Or Z, Gandre C, Durand Zaleski I, Steffen M. France’s response to the Covid-19 pandemic: between a rock and a hard place. Health Econ Policy Law. 2021;1–13. doi:10.1017/S1744133121000165
13. Carroll WD, Strenger V, Eber E, et al. European and United Kingdom COVID-19 pandemic experience: the same but different. Paediatr Respir Rev. 2020;35:50–56.
14. Coccia M. The relation between length of lockdown, numbers of infected people and deaths of Covid-19, and economic growth of countries: lessons learned to cope with future pandemics similar to Covid-19 and to constrain the deterioration of economic system. Sci Total Environ. 2021;775:145801.
15. Lee H, Kim Y, Kim E, Lee S. Risk assessment of importation and local transmission of COVID-19 in South Korea: statistical modeling approach. JMIR Public Health Surveill. 2021;7(6):e26784.
16. Gwee SXW, Chua PEY, Wang MX, Pang J. Impact of travel ban implementation on COVID-19 spread in Singapore, Taiwan, Hong Kong and South Korea during the early phase of the pandemic: a comparative study. BMC Infect Dis. 2021;21(1):799.
17. Sule WF, Oluwayelu DO. Real-time RT-PCR for COVID-19 diagnosis: challenges and prospects. Pan Afr Med J. 2020;35(Suppl 2):121.
18. Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720.
19. Cao S, Gan Y, Wang C, et al. Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China. Nat Commun. 2020;11(1):5917.
20. He D, Zhao S, Lin Q, et al. The relative transmissibility of asymptomatic COVID-19 infections among close contacts. Int J Infect Dis. 2020;94:145–147.
21. Gandhi M, Yokeo DS, Havlir DV. Asymptomatic Transmission, the Achilles’ heel of current strategies to control Covid-19. N Engl J Med. 2020;382(22):2158–2160.
22. Lee VJ, Chiew CJ, Khong WX. Interrupting transmission of COVID-19 lessons from containment efforts in Singapore. J Travel Med. 2020;27(3):taaa039.
23. Guangdong has strictly adhered to the “five lines of defense” to prevent imported COVID-19; 2020. Available from: http://gd.people.com.cn/n2/2020/0409/c123932-33936255.html.
24. Bedford J, Enria D, Giesecke J, et al. COVID-19: towards controlling of a pandemic. Lancet. 2020;395(10229):1015–1018.
25. Fang Q, Gong X, Xiao W, et al. Epidemiological characteristics and measures of prevention and control of imported COVID-19 cases in early phase in Shanghai. Chinese J Epidemiol. 2020;41(12):2034–2039.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.