Back to Journals » International Journal of General Medicine » Volume 18
Epidemiological and Pathogenic Characteristics of Benign and Malignant Thyroid Nodules Undergoing Ultrasonography for Health Checkup Population
Authors Yao Z ![]() , Zhou W, Shen Z, Li Q
, Zhou W, Shen Z, Li Q
Received 21 January 2025
Accepted for publication 20 May 2025
Published 28 May 2025 Volume 2025:18 Pages 2769—2779
DOI https://doi.org/10.2147/IJGM.S517851
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Satish Nair
Zhifeng Yao, Weihong Zhou, Zhixiang Shen, Qingxia Li
Department of Health Management Center, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China
Correspondence: Qingxia Li, Department of Health Management Center, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, No. 321, Zhongshan Road, Gulou District, Nanjing, Jiangsu, 210008, People’s Republic of China, Tel +8615996301027, Email [email protected]
Purpose: To analyze the epidemiological and pathogenic characteristics of benign and malignant thyroid nodules undergoing ultrasonography for health checkup population and evaluate the value of ultrasonography in early detection of thyroid cancer.
Methods: The thyroid nodules ultrasonic characteristics of 70430 examinees in different ages and genders were retrospectively analyzed according to the Chinese Thyroid Imaging Reporting and Data System (C-TIRADS). The high-risk thyroid nodules pathological results were compared with ultrasonic C-TIRADS to analyze the value of ultrasonography in early detection of thyroid cancer.
Results: The total thyroid nodules prevalence was 47.64%. Females had a significantly higher prevalence of thyroid nodules than males (52.10% vs 43.48%; P < 0.01), and thyroid nodules prevalence was gradually increased with age (P for trend < 0.01). Thyroid nodules were mainly multiple, unilateral lobe, maximum diameter < 1cm and solid nodules. The distribution of thyroid nodules in different genders was different in number, location, maximum diameter, echo characteristics and C-TIRADS (P < 0.01). The distribution of C-TIRADS in different ages was statistically different (P < 0.01). The thyroid nodules prevalence of C-TIRADS 2, 3, 4A, 4B, 4C, and 5 were 12.88%, 32.04%, 2.33%, 0.36%, 0.02% and 0.009%, respectively (P < 0.01). A total of 436 examinees were definitely diagnosed, of which 323 were benign and 113 were malignant, and the difference in the prevalence of malignancies among different C-TIRADS was statistically significant (P < 0.01). Well-differentiated papillary thyroid cancer accounted for 86.73% and most were early stage cancer and micro-carcinoma. The sensitivity, specificity and accuracy of ultrasonic C-TIRADS diagnosis of thyroid cancer were 84.07%, 97.41%, and 97.39%, respectively.
Conclusion: Age and gender are closely related to thyroid nodules prevalence. Ultrasonography based on C-TIRADS has certain value in detecting thyroid nodules and screening early thyroid cancer.
Keywords: thyroid nodules, ultrasonography, epidemiology, C-TIRADS, screening
Introduction
The thyroid gland, consisting of two connected lobes, is one of the largest endocrine glands in the human body, weighing 20–30 g in adults. As the most common thyroid disease, thyroid nodules are lesions characterized by local abnormal hyperplasia of thyroid cells. The incidence rates of thyroid nodules have risen to very high levels in the past few decades, and approximately 19%–68% of the population has thyroid nodules worldwide, most of which are benign, and malignant nodules account for about 7–15%.1–4 In addition to malignant potential of some thyroid nodules, they often may cause other clinical symptoms, such as thyroid dysfunction, compressive symptoms, hoarseness, dysphagia, shortness of breath, and pain.5 However, most thyroid nodules are asymptomatic or have no specific symptoms, and thyroid hormone secretion is usually normal.
Currently, the clinical techniques including ultrasonography, computed tomography (CT) and nuclear imaging, are mainly used to distinguish benign and malignant thyroid nodules. As the most accurate and sensitive imaging method for thyroid nodules detection, ultrasonography is the first choice and widely used for thyroid disease screening due to its advantages of non-invasive, painless, radiation-free, high resolution, repeatable, dynamic observation and simple operation. The growing global incidence of thyroid nodules and thyroid cancer is primarily due to the increasing application of ultrasonography in thyroid examination. Ultrasound-guided fine-needle aspiration biopsy (FNAB) is known as the “gold standard” for the diagnosis of thyroid nodules, and the nature of thyroid nodules can be further diagnosed through pathology.6–9
To standardize the diagnosis and treatment of thyroid nodules, various thyroid imaging reporting and data system (TIRADS) have been promulgated worldwide, such as American College of Radiology (ACR) TIRADS,10 Korean (K) TIRADS11 and European (EU) TIRADS.12 In 2020, under the support of the Superficial Organ and Vascular Ultrasound Group of the Society of Ultrasound in Medicine of the Chinese Medical Association, as well as the Chinese Artificial Intelligence Alliance for Thyroid and Breast Ultrasound, the Chinese TIRADS (C-TIRADS) was developed in line with China’s national conditions and medical status. Meanwhile, compared to other TIRADS, C-TIRADS is easier and more suitable for Chinese population and has been widely used in China.13 The recent study has indicated C-TIRADS has a high diagnostic efficacy for thyroid nodules, with sensitivity and negative predictive value over 90% and 95%, separately.14
Despite some studies have been conducted on thyroid nodules in certain areas of China, China is a large eastern country of multiple races and diverse environments where various risk factors are likely to exist and the incidence of thyroid nodules and thyroid cancer varies in different regions. Due to the variations in the distributions of age, race and gender composition, and the relatively smaller sample size in previous studies, the reported thyroid nodules prevalence was not consistent, ranging from 10% to 50%, which makes it difficult for drawing a conclusive conclusion.15–20 Due to some diagnosis methods, such as CT and nuclear imaging, are not suitable for screening large sample population, ultrasonic C-TIRADS has been widely used to differentiate benign and malignant thyroid tumors.21 In the present study, we aimed to conduct a retrospective study incorporating thyroid ultrasonic results of over 70 thousand health checkup population and use ultrasonic C-TIRADS standard to screen thyroid nodules over one-year period in Nanjing, China, to clarify the epidemiological and pathogenic characteristics of benign and malignant thyroid nodules in this health checkup population in order to provide a reference that can guide the prevention or treatment of thyroid nodules and diagnose thyroid cancer as early as possible.
Materials and Methods
Study Subjects
This retrospective cross-sectional study enrolled healthy participants who undergone health checkup at the Health Management Center of Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University from January to December 2023. Eligible health checkup participants were individuals ≥18 years of age who underwent thyroid ultrasound scans and volunteered to be followed up for one year. The clinical data and ultrasonic report of participants were complete and standardized. Thyroid nodules have been classified by C-TIRADS. Participants were excluded if their data were derived from repeat examinations, they were pregnant or lactating females, they had any history of thyroid disease and had undergone thyroid surgery or pharmacological treatment, or they had been diagnosed with cancer or any other serious disease, or those who refused to follow-up and lost their follow-up.
This study was approved by the Ethics Committee of Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University (NO. 2022–046-01) and was conducted in accordance with the Helsinki Declaration (revised 2013). The need for individual informed consent was waived by the committee due to the retrospective character of the study.
Apparatus and Methods
Thyroid Ultrasonography
All of the participants with a supine position fully exposed the neck and professional and skilled sonographers performed thyroid ultrasonography via 7.5MHz linear transducer (Resona8T, Mindray, China and EPIQ5, Philips, Holland). The cervical thyroid region was scanned continuously in transverse and longitudinal sections. Thyroid nodule characteristics were recorded, including nodule size (length, width and depth), shape (aspect ratio ≥1 or aspect ratio <1), structure (cystic, cystic-solid or solid), location, echo (no echo, high echo, equal echo, low echo or shallow echo), edge (regular, irregular or extraglandular invasion) and calcification. The risk assessment of benign and malignant thyroid nodules was carried out through C-TIRADS criteria as Category 1 (normal thyroid without any apparent nodules), Category 2 (definite benign lesions including spongiform nodules and cystic nodules, nodular goiter and simple calcifications), Category 3 (potentially benign nodules not exhibiting any malignant signs and the risk of malignancy is <2%), Category 4 (suspected malignancies, subclassified into categories 4A, 4B, or 4C based on whether they exhibited 1, 2, or 3–4 malignant signs, and the possibility of malignancy is 2%–10%, 10%–50% or 50%–90%), Category 5 (thyroid nodules exhibiting 5 malignant signs) or Category 6(malignancies confirmed by biopsy and pathology).13 The five potential sonographic signs of assessing malignant thyroid nodules included solid structure, low or shallow echo, irregular margins or extraglandular invasion, vertical orientation (aspect ratio ≥1), microcalcifications. If there is cervical lymph node metastasis or infiltration of surrounding tissues in the Categorie4, they are classified into Categorie5.
Follow-Up and Risk Stratification of Thyroid Cancer
Follow-up was conducted by telephone follow-up and outpatient consultation, starting from the health checkup day, followed up for one year. A total of 15 cases refused to be followed up and the rate of refusing to follow-up was 0.02%. A total of 87 cases were lost to follow-up and the loss rate was 0.12%.
Clinical staging of thyroid cancer was based on TNM staging criteria of thyroid cancer and differentiated thyroid cancer of American Joint Committee on Cancer (AJCC) in the 7th edition (2010). According to the C-TIRADS classification and the different risk of thyroid cancer, thyroid nodules Category1–3 were regarded as the low-risk group of thyroid cancer, and Category 4–5 as the high-risk group of thyroid cancer.
Statistical Analysis
Excel 2007 was used to input the data of thyroid ultrasonography, and SPSS version 19.0 (IBM Corporation, Somers, NY, USA) was used for statistical analysis of all data. Categorical variables were expressed as frequencies (n) and percentage (%), and the chi-square (χ2) test was used to compare differences between categorical variables of the two cohorts. Continuous variables conforming to normal distribution were presented as mean ± standard deviation ( ), and independent-sample t-test was used to compare differences between continuous variables of the two cohorts. The trend comparison of the incidence of thyroid nodules between male and female in different age groups was conducted by χ 2 trend test. The change trend of C-TIRADS in thyroid nodules prevalence among different age groups was performed by Gamma test. A P-value of < 0.05 was considered statistically significant.
), and independent-sample t-test was used to compare differences between continuous variables of the two cohorts. The trend comparison of the incidence of thyroid nodules between male and female in different age groups was conducted by χ 2 trend test. The change trend of C-TIRADS in thyroid nodules prevalence among different age groups was performed by Gamma test. A P-value of < 0.05 was considered statistically significant.
Results
The Basic Features of General Participants
In total, this study incorporated 70430 healthy adults (average age of 44.89 ± 4.76) years, including 36402 males (51.69%) and 34028 females (48.31%). The age ranged from 20 to 89 years old with an average age of (45.28 ± 4.17) years for males and (43.63 ± 3.41) years for females.
The Prevalence of Thyroid Nodules in the Health Checkup Population
Of the included 70430 subjects, 33554 subjects were found to have thyroid nodules, with the prevalence of 47.64%. The prevalence of thyroid nodules in female (52.10%, n = 17728) was significantly higher than that in male (43.48%, n = 15826) (χ2 for trend = 9362.239, P for trend < 0.01). According to the stratified analysis of different age groups, there was a significant difference in the thyroid nodules prevalence among male and female groups, with a chi-square trend test indicating that the prevalence of thyroid nodules rose with age (χ2 for trend = 5826.514, 4655.173, respectively, P for trend < 0.01), further details are provided in Table 1.
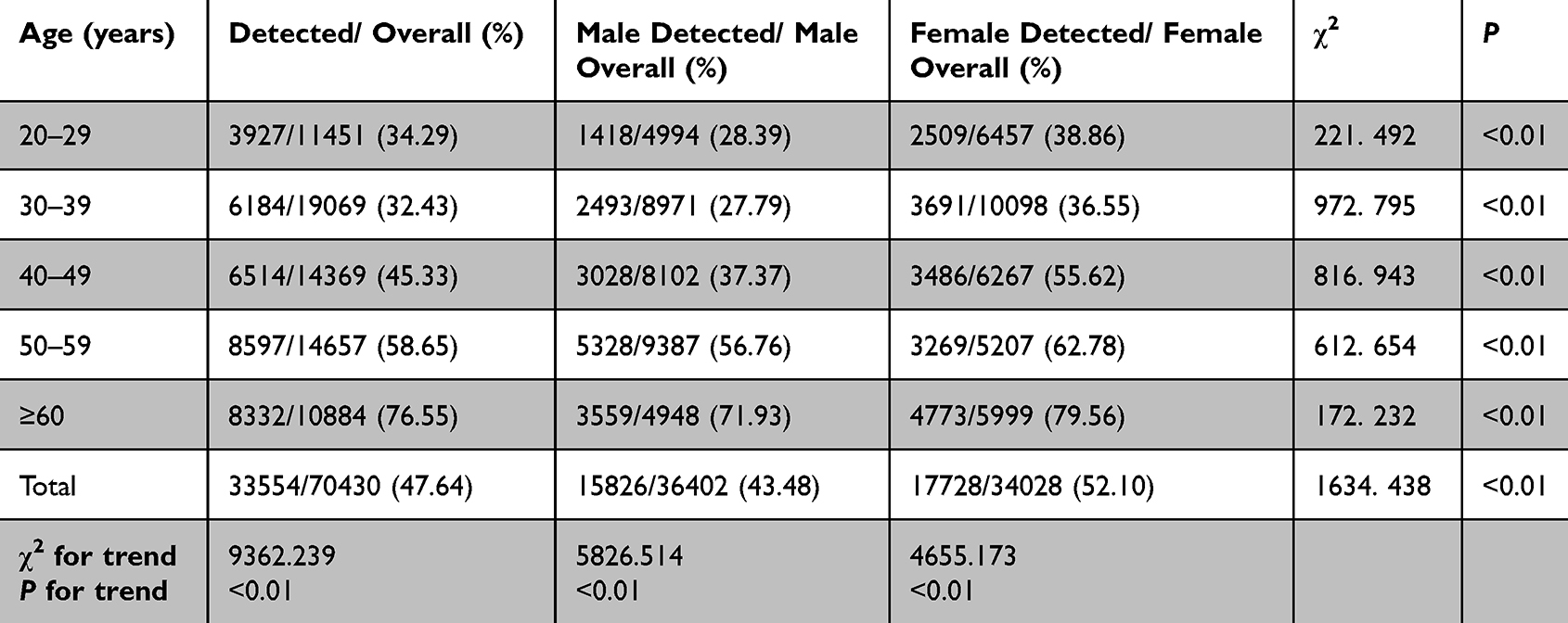 |
Table 1 Comparison of Detection Rate of Thyroid Nodules in Different Genders and Age Groups (n, %) |
The Ultrasound Features of Thyroid Nodules of Different Genders in the Health Checkup Population
Among those subjects with thyroid nodules, single thyroid nodule accounted for 34.87% (n =11699), while multiple thyroid nodules accounted for 65.13% (n = 21855), with the prevalence of 16.6% and 31.0%, respectively. A total of 20722 cases (61.76%) located in unilateral lobes, 12534 cases (37.35%) located in bilateral lobes and 298 cases (0.89%) located in thyroid isthmus. Maximum diameter of nodules was less than 1cm in 26088 cases (77.75%), 1–2cm in 5229 cases (15.58%) and ≥ 2cm in 2237 cases (6.67%). There were 19134 cases of solid nodules (57.02%), 11363 cases of cystic nodules (33.86%) and 3057 cases of mixed cystic-solid nodules (9.11%). There were significant differences in the number, location, maximum diameter and echo of thyroid nodules between different genders (P < 0.01), further details are provided in Table 2.
 |
Table 2 Distribution of Thyroid Nodule Characteristics in Different Genders (n, %) |
C-TIRADS of Thyroid Nodules in Different Gender and Age Groups in the Health Checkup Population
As is showed in Table 3, the proportions of Category 2, Category 3 and ≥ Category 4 in all thyroid nodules were 27.04% (9072/33554), 67.25% (22565/33554) and 5.71% (1917/33554), respectively. The distributions of thyroid nodules detected in different gender and age groups were different in C-TIRADS classification. With the increase of age, the higher the C-TIRADS classification of thyroid nodules was, and the differences were statistically significant (P < 0.01).
 |
Table 3 Distribution of C-TIRADS of Thyroid Nodules in Different Genders and Age Groups (n, %) |
The Prevalence of Thyroid Nodules with Different C-TIRADS
The thyroid nodules with C-TIRADS ≥ Category 4 are high-risk nodules of thyroid cancer, so this study classified these nodules into Category 4A, 4B, 4C and 5 in detail. Among the 70430 health checkup individuals, the prevalence rate of Category 2, 3, 4A, 4B, 4C and 5 was 12.88% (9072/70430), 32.04% (22565/70430), 2.33% (1642/70430), 0.36% (253/70430), 0.02% (16/70430) and 0.009% (6/70430), and there was a significant difference in the thyroid nodules prevalence of different Categories (χ2 = 42000.00, P<0.01). According to C-TIRADS Category, 68513 cases were low-risk thyroid nodules and 1917 cases were high-risk thyroid nodules among 70430 healthy people.
In descending order, the prevalence rate of thyroid nodules was C-TIRADS Category 3, Category 2, Category 4A, Category 4B, Category 4C and Category 5. When the same subject has multiple thyroid nodules, the nodule with the highest C-TIRADS classification was included in the analysis.
Malignant Thyroid Nodules in Health Checkup Population
After one year’s follow-up, the detection rates of malignant thyroid nodules in male and female healthy people were 0.15% (53/36402) and 0.18% (60/34028), respectively, with no statistical significance (χ 2 = 0.008, P > 0.05).
The Follow-Up Results of High-Risk Thyroid Nodules and Pathological Features of Malignant Thyroid Nodules in the Health Checkup Population
Excluding the nodules that could not be diagnosed qualitatively by pathological results, 436 cases of C-TIRADS 4–5 were followed up and confirmed by FNAB or surgery. Among them, there were 323 cases of benign nodules and 113 cases of malignant nodules. Typical ultrasonic images of benign and malignant thyroid nodules are shown in Figure 1. The benign thyroid nodules included 166 cases of thyroid adenoma, 128 cases of nodular goiter, 8 cases of thyroiditis and 21 case of scar formation after cystadenoma absorption. During the one-year follow-up, 113 cases of malignant nodules underwent surgery and were diagnosed by postoperative histopathological examination, of which 93 cases were micro-carcinoma, accounting for 82.30%. The malignant thyroid nodules included 98 cases of papillary carcinoma, 8 cases of medullary carcinoma and 7 cases of follicular carcinoma. In the clinical stages of malignant thyroid nodules, there were 78 cases, 21 cases, 9 cases and 4 cases in stage I,II, III and IVa, respectively. Papillary carcinoma accounted for the highest proportion in all the malignant thyroid nodules, reaching 86.73%, including 48 males and 50 females.
 |
Figure 1 Typical ultrasonic features of benign and malignant thyroid nodules. (a) thyroid adenoma (b) nodular goiter (c) subacute thyroiditis (d) Hashimoto’s thyroiditis (e and f) papillary thyroid carcinoma (g) follicular thyroid carcinoma (h and i) medullary thyroid carcinoma. |
There were 18 cases in Category 3, 19 cases in Category 4A, 57 cases in Category 4B,13 cases in Category 4C, and 6 cases in Category 5 in all the 113 cases of malignant nodules. According to C-TIRADS Category, 18 cases were in low-risk group and 95 cases were in high-risk group. In the pathological results of 436 cases, the malignant prevalence rates of C-TIRADS 4–5 were 8.64%(19/220) for Category 4A, 29.38% (57/194) for Category 4B, 81.25% (13/16) for Category 4C and 100.00% (6/6) for Category 5, respectively, showing a rising trend, and the difference was statistically significant from Category 4A to Category 5(χ 2 = 56.42, P < 0.01).
The Value of Ultrasound C-TIRADS Grading in the Diagnosis of Thyroid Cancer
By comparing the final results of C-TIRADS screening and follow-up confirmed by FNAB or surgery, it was found that the sensitivity and specificity of C-TIRADS grading system in the diagnosis of thyroid cancer were 97.34% and 97.43%, respectively. The positive predictive value was 5.74%, the negative predictive value was 99.99% and the accuracy was 97.43%, further details are shown in Table 4.
 |
Table 4 Effect of Ultrasound C-TIRADS Category on Screening Thyroid Cancer the Health Checkup Population |
Discussion
With changing lifestyle factors, popularization of health checkup and widespread application of thyroid ultrasonography, thyroid nodules detection rates are rising in China and throughout the globe. Data were analyzed for 70430 examinees who underwent health checkup in a Grade A hospital, revealing a thyroid nodules detection rate of 47.64%, which was higher than that in Germany (33%)22 and Kora (34.2%).23 The variations in the thyroid nodules prevalence also existed in different regions of the same country. During the past decades, several studies have tried to investigate the thyroid nodules prevalence in China, and a systematic review and meta-analysis suggested the overall thyroid nodules prevalence in China was about 22.7%.24 The present study suggested the thyroid nodules prevalence in Nanjing was higher than that in Liaoning (10.17%– 12.64%)25 and Guangdong (31.65%),26 but lower than that in Beijing (58.69%).27 The difference of lifestyle and dietary habit maybe induce the difference of thyroid nodules prevalence between our study and those performed in the other regions of China. Additionally, the thyroid nodules prevalence in our study was similar to the result reported in Nanjing 10 years ago, with the prevalence of 46.6%.28
This study first compared the detection of thyroid nodules in different gender and age groups in the health checkup population. The current results showed that the detection rates of thyroid nodules in male and female health checkup population were 43.48% and 52.10%, respectively, which was in accordance with the past investigation showing that females were more likely to develop thyroid nodules than males.23,24,29,30 The gender differences in thyroid nodules may be due to physiology, pregnancy, and estrogen exposure of female.31 Estrogen accelerates the proliferation of thyroid stem cells and progenitor cells through classical genomic and non-genomic pathways and contributes to the generation of thyroid nodules.32,33 Moreover, a higher detection rate of thyroid nodules was observed among females in every age group, also similar to the results of other studies.34,35
The detection rates of thyroid nodules in different age groups were shown in Table 1, among which the highest detection rate was ≥60 years old (76.55%), followed by 50–59 years old (58.65%) and the lowest was 30–39 years old (32.43%). With the increase of age, the thyroid nodules prevalence gradually increased, especially among people over 50 years old, the prevalence rate of thyroid nodules was above 50%, indicating that the growth of age is another cause of high thyroid nodules prevalence. It is generally accepted that reactive oxygen and free radicals precipitate with age, contributing to the accumulation of pernicious changes in thyroid cells and fibrosis in thyroid tissue.36 Furthermore, hyperplasia of fibrous connective tissue, inflammatory infiltration in the interstitium of thyroid tissue and vacuolation of the vesicle cells cytoplasm ultimately lead to the formation of thyroid nodules.37 Meanwhile, the thyroid function decreases with age, its ability to regulate iodine decreases, and the thyroid gland undergoes degenerative changes.38 When the participants were stratified based on age, higher age was associated with an elevated detection of thyroid nodules. It has been found in our study that thyroid nodules increased with age, and the detection rate of thyroid nodules was as high as 76.55% in population at the age over 60 years. In other words, ultrasound examination of the thyroid in heath checkups should be given prominence, especially in elder female population.
This study also found that most thyroid nodules were small nodules (77.75%). Small thyroid nodules are often missed by examination with palpation due to the lack of obvious symptoms. However, the early malignant thyroid nodules also lack typical clinical manifestations, which need to be carefully differentiated, especially by high-resolution ultrasound. It has been reported that the prevalence rate of thyroid malignant nodules is 1.60%–12.00%,39 but a total of 436 cases in this study were confirmed by pathology and 113 cases were malignant, with a prevalence rate of 0.16%(113/70430), which was significantly lower than the literature statistics. The main reason is that this study is aimed at the investigation of epidemiology and disease characteristics with a large sample size. Most benign thyroid nodules often do not need FNAB or surgery, and only C-TIRADS 4–5 and a few C-TIRADS3 nodules with malignant possibility have undergone FNAB or surgery during follow-up, so the sample size of pathological results is small. In this paper, papillary thyroid carcinoma accounted for 86.73%, which was consistent with the conclusion that papillary thyroid carcinoma is the most common and accounts for 50.00%–90.00% of thyroid carcinoma.40 Although papillary thyroid carcinoma has a high incidence rate, it has the high degree of differentiation, the low degree of malignancy and the best prognosis.
Thyroid cancer is a common endocrine malignant tumor, and its incidence is still on the rise, second only to breast cancer. However, due to different geographical factors and social environment, the incidence of thyroid cancer varies among different regions. Understanding the incidence and characteristics of thyroid cancer in Nanjing can provide theoretical support for prevention and therapy of thyroid cancer. Advanced thyroid cancer often has obvious symptoms, while early thyroid cancer is characterized by small thyroid nodules, which often have no obvious symptoms and are not easy to be found. C-TIRADS graded the malignant possibility of thyroid nodules by evaluating their tiny calcification, low or extremely low echo, aspect ratio, irregular edge and suspicious lymph nodes. Therefore, this study applied C-TIRADS grading standard as the key technology for early screening of thyroid cancer, and evaluated its value in early screening of thyroid cancer. Among 68513 cases in the low-risk group and 1917 cases in the high-risk group, 18 cases and 95 cases were finally diagnosed as thyroid cancer after thyroidectomy. The detection rate of thyroid nodules in female checkup population was higher than that in male. However, the detection rate of thyroid cancer was not obviously affected by gender, and there was no significant difference between male and female health checkup population.
Thyroid cancers diagnosed in this study have the following characteristics. First, most of them were well-differentiated papillary thyroid carcinoma, and only 15 cases were non-papillary thyroid carcinoma. Second, most thyroid cancers were micro-carcinoma, accounting for 82.30% (93/113). Third, the clinical stages were mostly early, and papillary thyroid carcinoma in stage I–II accounted for 87.61% (99/113), and the risk of recurrence was low. Fourth, no significant difference in the thyroid cancer prevalence was observed between male and female health checkup population, which was inconsistent with the traditional data that the incidence rate of thyroid cancer in females was 2–3 times higher than that in males. It may be related to the short follow-up time and the small number of cases.
At last, the health checkup population was divided into low-risk group and high-risk group with reference to ultrasound C-TIRADS classification. The detection rate of thyroid cancer in low-risk group was 0.03% and that in high-risk group was 4.96%. The sensitivity and specificity of C-TIRADS grading system in the diagnosis of thyroid cancer were 84.07% and 97.41%, respectively, and the accuracy was 97.39%. This study reflects the preliminary results of ultrasonic diagnosis technology in thyroid nodules early screening, and brings the screened high-risk population into the health management system. The precise health management of high-risk group health examinees is very necessary for providing more opportunities for early diagnosis and treatment of thyroid cancer.
This study has several limitations. First, this study is a cross-sectional retrospective study, and there may be bias in evaluating C-TIRADS positive features and its exact causal relationship needs to be further demonstrated by a future prospective studies. Furthermore, this study is a single-center study, which inevitably has the problem of a small number of samples, and the sample selection of healthy people is still limited, especially the thyroid nodules larger than 1cm are few. Therefore, it is very important to conduct a wider epidemiological investigation through a well-designed prospective cohort to find out the risk factors of thyroid nodules more accurately. Third, the follow-up time of this study is only one year, which is relatively short for the majority of thyroid cancers with relatively good prognosis. Considering that some patients with thyroid cancer may be included in the low-risk group without follow-up or FNAB, the detection rate of thyroid cancer in the low-risk group is low, with only 18 thyroid cancer patients, which leads to the high sensitivity of C-TIRADS in diagnosing thyroid cancer. During the follow-up period, the proportion of surgical cases in the high-risk group is only 4.96%, which is not enough to truly evaluate the value of thyroid ultrasound diagnosis, and further follow-up is needed. Fourth, C-TIRADS is to evaluate the risk of nodules only by the number of malignant ultrasound features, without adding the weight factor of each malignant sign, which will lead to the difference of malignant risk rate of the same type of nodules, especially for thyroid nodules C-TIRADS Category 4A, 4B and 4C. Last, the personal experience of sonographer is different, so the understanding of C-TIRADS will be different among different sonographers.
Conclusion
To sum up, with the popularization of health checkup and the application of high-resolution ultrasonic probe and color Doppler technology, the detection rate of thyroid nodules in healthy people has increased significantly. The incidence of thyroid nodules in the regional health checkup population is high, with the overall detection rate close to 50% and increases gradually with age, which is significantly higher in female than in male. Despite the fact that thyroid nodules are usually benign lesions, a certain percentage can transform into malignant nodules, and therefore identification of high-risk factors is extremely important in order to reduce occurrence of thyroid cancer. Ultrasonography has become an important means to screen thyroid nodules and follow-up the changes of thyroid nodules, greatly improving the differentiation accuracy of benign and malignant thyroid nodules. Ultrasound C-TIRADS grading has certain value in detecting thyroid nodules and differentiating benign from malignant thyroid nodules in healthy population. It is an effective noninvasive screening approach and appropriate for screening thyroid cancer in large-scale population as early as possible.
Ethical Statement
The authors are accountable for all aspects of this work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All procedures involving human participants were performed in accordance with the Declaration of Helsinki (revised 2013). The ethics committee of Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University approved this retrospective study, and waived the requirement for informed consent. Health checkup population information, such as name, age, sex, occupation, address, ID card and related diseases, were provided by Department of Health Management Center, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
All authors declare that they have no conflicts of interest in this work.
References
1. Hyun MK, Kim JH, Kwon JW. Incidence of thyroid cancer and medical cost among patients with newly diagnosed thyroid nodules in Korea: a retrospective cohort study using nationwide data. J Cancer Res Ther. 2019;15:676–680. doi:10.4103/0973-1482.204895
2. Wang J, Yu F, Shang Y, et al. Thyroid cancer: incidence and mortality trends in China, 2005-2015. Endocrine. 2020;68:163–173. doi:10.1007/s12020-020-02207-6
3. Pizzato M, Li M, Vignat J, et al. The epidemiological landscape of thyroid cancer worldwide: GLOBOCAN estimates the incidence and mortality rates of thyroid cancer in 2020. Lancet Diabetes Endocrinol. 2022;10:264–272. doi:10.1016/S2213-8587(22)00035-3
4. Miranda-Filho A, Lortet-Tieulent J, Bray F, et al. Thyroid cancer incidence trends by histology in 25 countries: a population-based study. Lancet Diabetes Endocrinol. 2021;9:225–234. doi:10.1016/S2213-8587(21)00027-9
5. Popoveniuc G, Jonklaas J. Thyroid nodules. Med Clin N Am. 2012;96:329–349. doi:10.1016/j.mcna.2012.02.002
6. Holt EH. Current evaluation of thyroid nodules. Med Clin North Am. 2021;105:1017–1031. doi:10.1016/j.mcna.2021.06.006
7. Alexander EK, Doherty GM, Barletta JA. Management of thyroid nodules. Lancet Diabetes Endocrinol. 2022;10:540–548. doi:10.1016/S2213-8587(22)00139-5
8. Kobaly K, Kim CS, Mandel SJ. Contemporary management of thyroid nodules. Annu Rev Med. 2022;73:517–528. doi:10.1146/annurev-med-042220-015032
9. Alexander EK, Cibas ES. Diagnosis of thyroid nodules. Lancet Diabetes Endocrinol. 2022;10:533–539. doi:10.1016/S2213-8587(22)00101-2
10. Tessler FN, Middleton WD, Grant EG, et al. ACR thyroid imaging reporting and data system (TI-RADS): white paper of the ACR TI-RADS committee. J Am Coll Radiol. 2017;14:587–595. doi:10.1016/j.jacr.2017.01.046
11. Shin JH, Baek JH, Chung J et al; Korean society of thyroid radiology (KSThR) and the Korean society of radiology, et al. Ultrasonography diagnosis and imaging-based management of thyroid nodules: revised Korean society of thyroid radiology consensus statement and recommendations. Korean J Radiol. 2016;17:370–395. doi:10.3348/kjr.2016.17.3.370
12. Russ G, Bonnema SJ, Erdogan MF, et al. European thyroid association guidelines for ultrasound malignancy risk stratification of thyroid nodules in adults: the EU-TIRADS. Eur Thyroid J. 2017;6:225–237. doi:10.1159/000478927
13. Zhou J, Yin L, Wei X, et al. 2020 Chinese guidelines for ultrasound malignancy risk stratification of thyroid nodules: the C-TIRADS. Endocrine. 2020;70:256–279. doi:10.1007/s12020-020-02441-y
14. Jin Z, Pei S, Shen H, et al. Comparative study of C-TIRADS, ACR-TIRADS, and EU-TIRADS for diagnosis and management of thyroid nodules. Acad Radiol. 2023;30:2181–2191. doi:10.1016/j.acra.2023.04.013
15. Song B, Zuo Z, Tan J, et al. Association of thyroid nodules with adiposity: a community-based cross-sectional study in China. BMC Endocr Disord. 2018;18:3. doi:10.1186/s12902-018-0232-8
16. Jiang H, Tian Y, Yan W, et al. The prevalence of thyroid nodules and an analysis of related lifestyle factors in Beijing communities. Int J Environ Res Public Health. 2016;13:442. doi:10.3390/ijerph13040442
17. Chen Z, Xu W, Huang Y, et al. Associations of noniodized salt and thyroid nodule among the Chinese population: a large cross-sectional study. Am J Clin Nutr. 2013;98:684–692. doi:10.3945/ajcn.112.054353
18. Fan L, Tan L, Chen Y, et al. Investigation on the factors that influence the prevalence of thyroid nodules in adults in Tianjin, China. J Trace Elem Med Biol. 2018;50:537–542. doi:10.1016/j.jtemb.2018.03.004
19. Song J, Zou SR, Guo CY, et al. Prevalence of thyroid nodules and its relationship with iodine status in shanghai: a population-based study. Biomed Environ Sci. 2016;29:398–407. doi:10.3967/bes2016.052
20. Li Y, Jin C, Li J, et al. Prevalence of thyroid nodules in China: a health examination cohort-based study. Front Endocrinol. 2021;12:676144. doi:10.3389/fendo.2021.676144
21. Qu C, Li HJ, Gao Q, et al. Alteration trend and overlap analysis of positive features in different-sized benign and malignant thyroid nodules: based on Chinese thyroid imaging reporting and data system. Int J Gen Med. 2024;17:1887–1895. doi:10.2147/IJGM.S461076
22. Guth S, Theune U, Aberle J, et al. Very high prevalence of thyroid nodules detected by high frequency (13 MHz) ultrasound examination. Eur J Clin Invest. 2009;39:699–706. doi:10.1111/j.1365-2362.2009.02162.x
23. Moon JH, Hyun MK, Lee JY, et al. Prevalence of thyroid nodules and their associated clinical parameters: a large-scale, multicenter-based health checkup study. Korean J Intern Med. 2018;33:753–762. doi:10.3904/kjim.2015.273
24. Zhao W, Han C, Shi X, et al. Prevalence of goiter and thyroid nodules before and after implementation of the universal salt iodization program in mainland China from 1985 to 2014: a systematic review and meta-analysis. PLoS One. 2014;9:e109549. doi:10.1371/journal.pone.0109549
25. Yu X, Fan C, Shan Z, et al. A five-year follow-up study of goiter and thyroid nodules in three regions with different iodine intakes in China. J Endocrinol Invest. 2008;31:243–250. doi:10.1007/BF03345597
26. Liang Q, Yu S, Chen S, et al. Association of changes in metabolic syndrome status with the incidence of thyroid nodules: a prospective study in Chinese adults. Front Endocrinol. 2020;11:582. doi:10.3389/fendo.2020.00582
27. Yang HX, Zhong Y, Lv WH, et al. Association of adiposity with thyroid nodules: a cross-sectional study of a healthy population in Beijing, China. BMC Endocr Disord. 2019;19:102. doi:10.1186/s12902-019-0430-z
28. Guo H, Sun M, He W, et al. The prevalence of thyroid nodules and its relationship with metabolic parameters in a Chinese community-based population aged over 40 years. Endocrine. 2014;45:230–235. doi:10.1007/s12020-013-9968-0
29. Knudsen N, Laurberg P, Perrild H, et al. Risk factors for goiter and thyroid nodules. Thyroid. 2002;12:879–888. doi:10.1089/105072502761016502
30. Chen Y, Zhu C, Chen Y, et al. The association of thyroid nodules with metabolic status: a cross-sectional SPECT-China study. Int J Endocrinol. 2018;2018:6853617. doi:10.1155/2018/6853617
31. Dauksiene D, Petkeviciene J, Klumbiene J, et al. Factors associated with the prevalence of thyroid nodules and goiter in middle-aged euthyroid subjects. Int J Endocrinol. 2019;2019:9131406. doi:10.1155/2019/9131406
32. Derwahl M, Nicula D. Estrogen and its role in thyroid cancer. Endocr Relat Cancer. 2014;21:T273–283. doi:10.1530/ERC-14-0053
33. Manole D, Schildknecht B, Gosnell B, et al. Estrogen promotes growth of human thyroid tumor cells by different molecular mechanisms. J Clin Endocrinol Metab. 2001;86:1072–1077. doi:10.1210/jcem.86.3.7283
34. Liu Y, Lin Z, Sheng C, et al. The prevalence of thyroid nodules in northwest China and its correlation with metabolic parameters and uric acid. Oncotarget. 2017;8:41555–41562. doi:10.18632/oncotarget.14720
35. Wang K, Yang Y, Wu Y, et al. The association of menstrual and reproductive factors with thyroid nodules in Chinese women older than 40 years of age. Endocrine. 2015;48:603–614. doi:10.1007/s12020-014-0342-7
36. Su Y, Zhang Y, Zhao M, et al. Association between thyroid nodules and volume and metabolic syndrome in an iodine-adequate area: a large community-based population study. Metab Syndr Relat Disord. 2019;17:217–222. doi:10.1089/met.2018.0094
37. Zaki SM, Mohamed EA, Abdel FS, et al. Age-associated functional morphology of thyroid and its impact on the expression of vimentin, cytokeratins and VEGF. The role of nigella in refinement. Folia Histochem Cytobiol. 2018;56:159–171. doi:10.5603/FHC.a2018.0015
38. Sharen G, Zhang B, Zhao R, et al. Retrospective epidemiological study of thyroid nodules by ultrasound in asymptomatic subjects. Chin Med J. 2014;127:1661–1665. doi:10.3760/cma.j.issn.0366-6999.20132469
39. Grant EG, Tessler FN, Hoang JK, et al. Thyroid ultrasound reporting lexicon: white paper of the ACR thyroid imaging, reporting and data system (TIRADS) committee. J Am Coil Radiol. 2015;12:1272–1279. doi:10.1016/j.jacr.2015.07.011
40. Siraj AK, Hussain AR, AI-Rasheed M, et al. Demethylation of TMSl gene sensitizes thyroid cancer cells to TRAIL-induced apoptosis. J Clin Endocrinol Metab. 2011;96:E215–224. doi:10.1210/jc.2010-0790
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.