Back to Journals » Cancer Management and Research » Volume 14
Epidemiological and Histopathological Characteristics of Renal Cell Carcinoma in Somalia
Authors Mohamed AH ![]() , Abdullahi IM
, Abdullahi IM ![]() , Eraslan A, Mohamud HA, Gur M
, Eraslan A, Mohamud HA, Gur M
Received 9 February 2022
Accepted for publication 22 May 2022
Published 30 May 2022 Volume 2022:14 Pages 1837—1844
DOI https://doi.org/10.2147/CMAR.S361765
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bilikere Dwarakanath
Abdikarim Hussein Mohamed,1 Ismail Mohamud Abdullahi,2 Aşır Eraslan,1 Hussein Ali Mohamud,1 Metin Gur1
1Urology Department, Mogadishu Somalia Turkish Training and Research Hospital, Mogadishu, Somalia; 2Pathology Department, Mogadishu Somalia Turkish Training and Research Hospital, Mogadishu, Somalia
Correspondence: Abdikarim Hussein Mohamed, Mogadishu Somalia Turkish Training and Research Hospital, Mogadishu, Somalia, Tel +252615167182, Email [email protected]
Background: There is a scarcity of studies regarding renal cell carcinoma (RCC) reported from Sub-Saharan Africa.
Objective: The present study is the first report evaluating the prevalence and clinical and histopathological features of RCC at a tertiary hospital in Somalia.
Methods: This retrospective study included 84 patients with histologically confirmed RCC over 5-years. The investigated parameters were sociodemographic features, radiological and histopathological characteristics, mortality, and overall 5-year survival rate.
Results: The prevalence of RCC in our study was 0.7%. The mean age of the patients was 53.74± 5.5 years, 67.9% were male, and 32.1% were female, with a 2:1 male-to-female ratio. The mean tumor size was 6.38± 2.4 cm. Clear cell RCC was the most common histological type in 67.8%, followed by papillary RCC (15.6%), unclassified RCC (9.5%), and chromophobe RCC was the least common in 7.1% of the cases. About one-third of the case had locally advanced RCC with positive nodal involvement, 26.2% of the patients had metastatic disease, and a further 6% progressed to metastatic cancer despite surgical resection. Eight percent of our cases returned with local recurrence. The mortality rate was 37.2%. More than eighty percent of females had a low-stage and a low-grade RCC, while males held higher stages and higher grades RCC in 37% and 63%, respectively (p< 0.001). Smokers were male-only, while obesity was common in female patients (p=0.02).
Conclusion: The study findings showed a satisfactory outcome, 71.4% of our patients presented with localized RCC, the five-year survival rate of the patients was 62.8%, and the mortality rate was substantially higher for patients with a higher stage, a higher grade tumor, and metastatic disease at the time of diagnosis.
Keywords: renal cell carcinoma, Sub-Saharan Africa, mortality, five-year survival rate
Introduction
Renal cell carcinoma (RCC) is a molecularly and histopathologically group of heterogeneous tumors. The most common subtypes of RCC are Clear cell RCC (65–70%), papillary RCC (15–20%), and chromophobe RCC (5–7%), respectively.1
The prevalence of renal cell carcinomas (RCCs) represents 3% of all visceral neoplasms and is the seventh most common cancer with an increasing prevalence.2 RCC accounts for 90% of tumors originating from the kidneys. It is common in the sixth and seventh decade of life with a median age of 64 years and primarily is a disease of the elderly, with a twofold male predominance.3,4
Smoking, male gender, age, hypertension, and obesity are several risk factors related to RCC.5,6 A first-degree relative is also associated with an increased risk of having RCC.7
The severity and prognosis of RCC correlate with the tumor stage, histopathological grade, presence of sarcomatoid and rhabdoid features, and fat and vascular invasion.8
Despite the advancements in diagnosis and management of RCC in the last two decades, RCC still is the most lethal urological cancer resulting in a mortality rate of about 40%.2 In recent years, RCC incidence increasing worldwide and per nation, despite the majority of the renal tumors being identified accidentally through medical imaging (abdominal ultrasound and computed tomography).9 In cases of metastatic tumors, the mortality of RCC is high, with a low survival rate of about 0–13%.10
Cancer is one of the leading causes of mortality worldwide. Before the age of 70, cancer is the first or second cause of death in 91/172 countries and the third or fourth cause of death in twenty-two countries.11 Africa has the lowest RCC incidence and mortality rate, with a cumulative risk below 0.2% for both gender groups. Egypt (2.4), Libya (2.3), Mali (1.8), and Tunisia (1.7) had the highest mortality rates, with a cumulative mortality risk between 0.17% and 0.27%.12
The present study is the first report from Somalia evaluating the prevalence and clinical and histopathological features of RCC at a tertiary hospital (the sole tertiary and referral hospital and the only cancer center) in Somalia.
Method
This retrospective study included all patients who have received the diagnostic code of RCC in agreement with the International Classification of Diseases (ICD-10) system and underwent contrast-enhanced computed tomography of the abdomen and nephrectomy over 5-years using the electronic hospital information system (HIS). The study included 84 patients with histologically confirmed renal cell carcinoma. Patients with the Bosniak classification system indicating benign renal cyst, those with inflammatory and metastatic mass with known other primary origins, and patients with incomplete data were excluded from the study.
Investigated parameters of the patients included age of the patients, gender group, site of the tumor (right, left, and bilateral), location of the mass (upper pole, middle pole, lower pole, and more than one pole of the kidney), clinical tumor stage, lymph node involvement, distant metastasis, and type of operation (laparoscopic, open vs radical, partial nephrectomy). Axial (with 1 mm cross-section), coronal and sagittal planes of CT abdominopelvic with and without contrast were used to determine renal mass size and localization. Histopathological results such as type of renal cell carcinoma, grade of the tumor in accordance to the World Health Organization/International Society of Urologic Pathology
(WHO/ISUP) grading systems were evaluated too.
WHO/ISUP grading system 2016, fourth edition, is the current internationally recommended system for typing renal tumors and was used to report the histopathological findings. T stage was classified into pTX: primary tumor cannot be assessed, pT0: No evidence of primary tumor, pT1a: ≤ 4 cm, limited to the kidney, pT1b: > 4 cm and ≤ 7 cm, limited to the kidney, pT2a: > 7 cm and ≤ 10 cm, limited to the kidney, pT2b: > 10 cm, limited to the kidney, pT3a: invades renal vein/branches, perirenal fat, renal sinus fat or pelvicalyceal system, pT3b: extends into vena cava below the diaphragm, pT3c: extends into vena cava above the diaphragm or invades vena cava wall, pT4: invades beyond Gerota fascia, including a direct extension to the adrenal gland.
WHO/ISUP grading system: Grade 1: Nucleoli are absent or inconspicuous and basophilic at 40x. Grade 2: Nucleoli are not prominent at 10x but visible and eosinophilic at 40x. Grade 3: Nucleoli conspicuous and eosinophilic at 10x. Grade 4: Extreme nuclear pleomorphism, multinucleated cells, and rhabdoid or sarcomatoid differentiation.
The ethical research board committee of Mogadishu Somalia Turkish Training and Research Hospital (REF. MSTH-9006) approved the research. In addition, all study participants and a parent of participants under 18 years of age previously consented to use their medical and surgical data in this study. This study was carried out in accordance to the Helsinki Declaration contents.
Statistical analyses were used in the Statistical Package for Social Sciences (SPSS-IBM) for Windows version 23. The data were analyzed using univariate descriptive statistics. The frequencies and percentages, as well as the mean ± (SD), were presented. Cross-tabulations were used to determine the association between the variables.
Results
A total of 84 patients with histopathologically proven RCC over 5-years were included in this study. The prevalence of RCC in our study was 0.7%. The mean age of the patients in our study was 53.74±5.5 years, 48.8% of the cases were elder (≥60 years), and 38.21% were between 40–59 years, while 13% of the patients were younger than 40 years. The gender distribution of RCC was 67.9% male and 32.1% female, showing more than twofold male predominance. The mean tumor size was 6.38±2.4 cm. The right kidney harbored most of the masses in 57%, 40.5% in the left, while 2.4% were bilateral involvement (Table 1). Open radical nephrectomy was the predominant operation performed in 54.7% of the cases, 32% underwent laparoscopic radical nephrectomy, and the remaining 13% underwent open partial nephrectomy. As shown in Table 2, Clear cell RCC was the most common histological type in about 67.8%, followed by papillary RCC (15.6%), unclassified RCC (9.5%), and Chromophobe RCC was the least common in 7.1% of the cases. Half of the patients held tumor stage 2, followed by T1 in 21.4%, 15.5% in T4, and 13.1% in T3. WHO/ISUP grading system revealed that half of the patients had high-grade tumors (G4 in 28.7% and G3 in 20.2%), while the remaining 50% had low-grade tumors (G2 in 44% and G1 in 7.1%). Three cases had rhabdoid features, two male and one female patient. About one-third of the case had locally advanced RCC with positive nodal involvement, while 26.2% of the cases revealed distant metastasis such as lungs. Regarding the comorbidities, 28.6% had diabetes, 25% were obese, 19% of the patients had hypertension, and 15.4% were smokers. One patient with a left upper pole 7cm mass who had undergone laparoscopic radical nephrectomy developed a pancreatic tail injury, which transformed into necrotizing pancreatitis. Unfortunately, after consecutive interventions patient died due to massive uncontrollable bleeding. Five-years follow-up, 67 patients were reached through telephone obtained from the hospital information system, and 42 patients were alive (62.8%). Seven cases returned with local recurrence, 5 in the renal fossa, and 2 in the abdominal wall. Five cases developed distant metastasis. The mortality rate in our study was 37.2%. 56% (14/25) of the cases died within 2 years, primarily in patients with a higher stage, a higher grade, and distant metastasis at the time of diagnosis; 11 patients died within 5-years postoperatively.
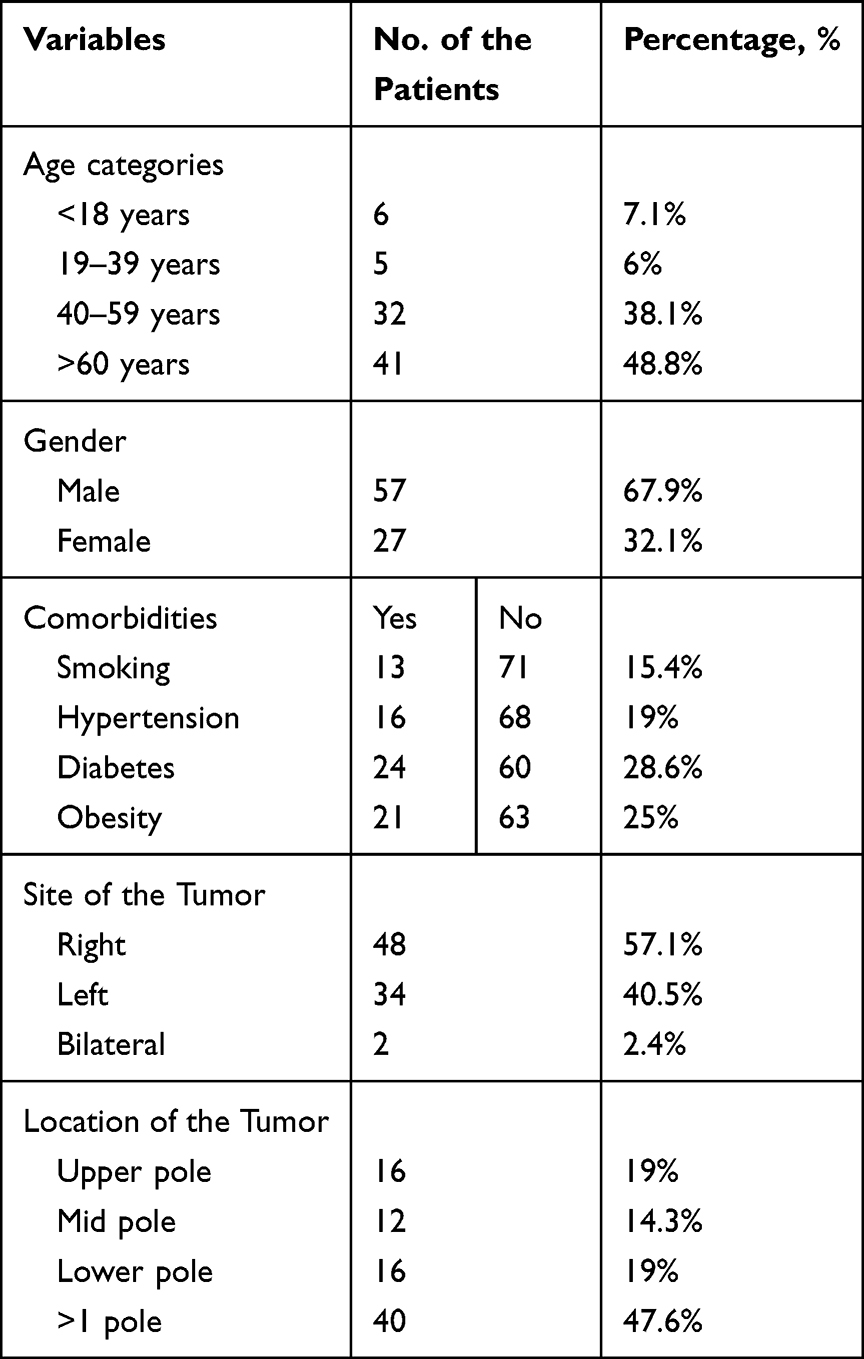 |
Table 1 Sociodemographic Characteristics of the Patients |
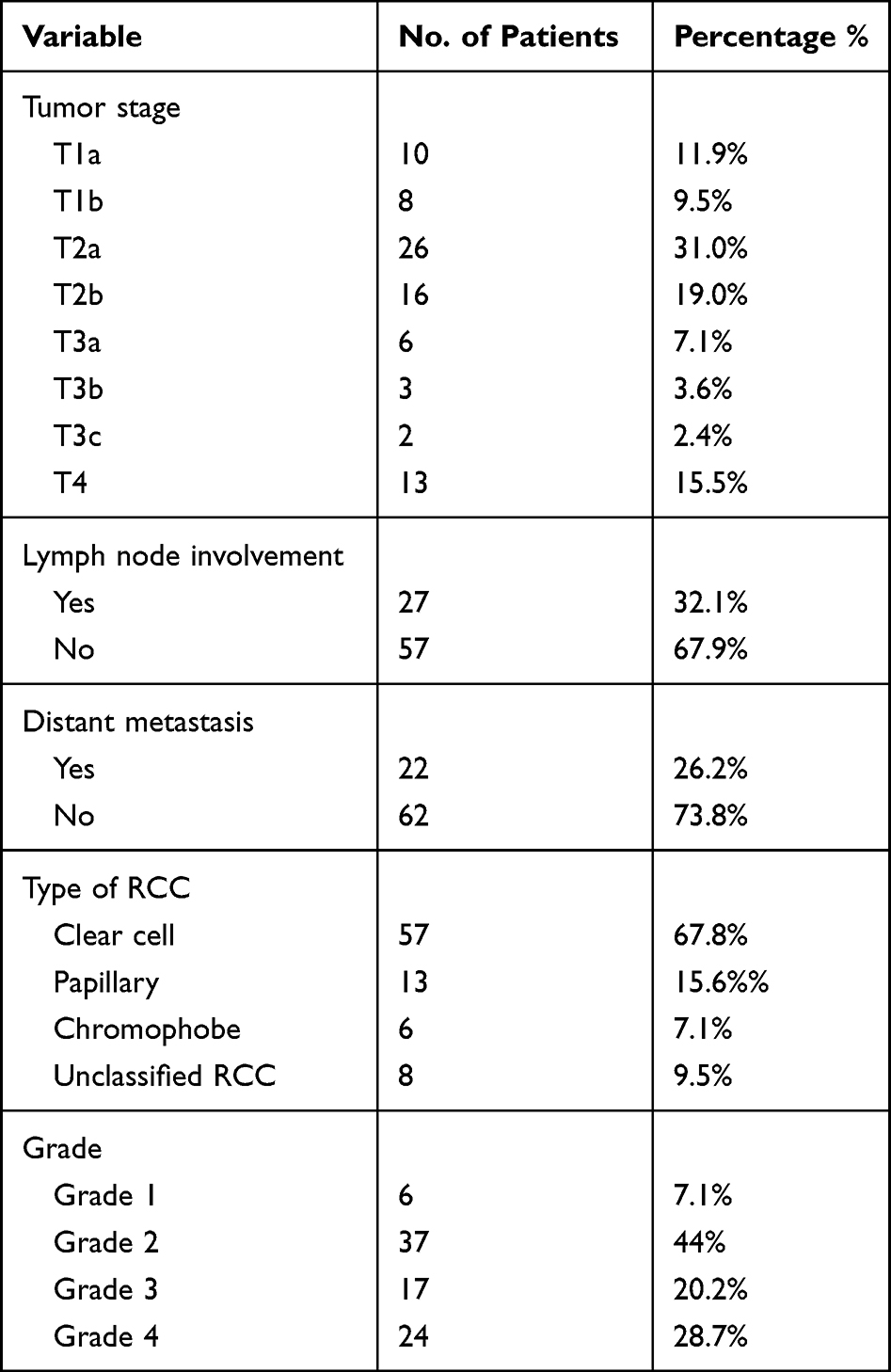 |
Table 2 Radiological and Histopathological Features of the Cases |
Assessment of gender variation of tumor stage, grade, and comorbidities revealed a statistically significant difference between the pattern of stage and grade of RCC and gender group (Table 3). More than eighty percent of females had a low-stage and a low-grade RCC, while males held higher stages and higher grades RCC in 37% and 63%, respectively (p<0.001). Smokers were male-only, while obesity was common in female patients (p=0.02).
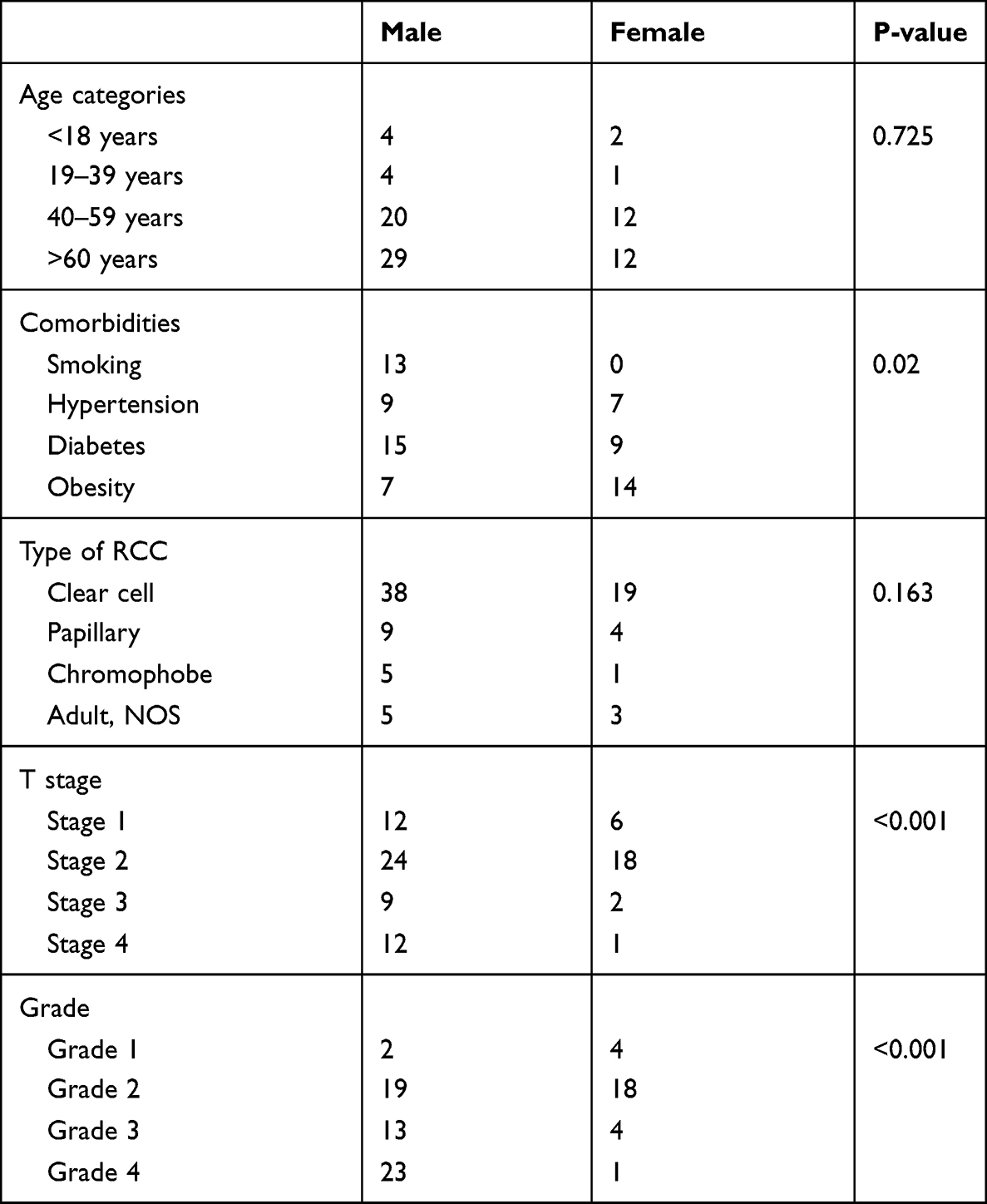 |
Table 3 Gender Variation of Tumor Type, Stage, Grade, and Associated Comorbidities |
Our review showed that 54.5% (6/11) and 73.9% (54/73) of patients younger than 40-years and elderly patients had localized RCC. Clinically symptomatic cases were predominantly patients younger than 40-years compared to older patients, 78% versus 55%, respectively.
Discussion
There is a scarcity of studies in the body of the literature regarding renal cell carcinoma reported from Sub-Saharan Africa (SSA) including Somalia. There were eleven published studies from Nigeria, Senegal, Benin, and Togo that contained 482 patients with RCC.13 There have been no previous studies reported from Somalia regarding the prevalence, clinical and histopathological features of renal cell carcinoma. This study is aimed to evaluate the epidemiological and histopathological characteristics of renal cell carcinoma at a tertiary hospital in Somalia.
RCC incidence rates differ significantly around the world. North America has the highest estimated incidence globally (12/100 000), with 1.8% and 0.9% cumulative risks for males and females. Western Europe (9.8) has the highest incidence rates for both sexes in Europe, while Africa has the lowest incidence and mortality rate, below 0.2% cumulative risks for both sexes.14 RCC in the pediatric population is rare and accounts for 2% to 6% of malignant renal tumors.15 The prevalence of RCC in our study was 0.7%, and 6 cases were pediatric age group.
The peak incidence of renal cell carcinoma appears between the sixth and seventh decade of age, with a median age of 64 years, and primarily is a disease of the elderly. The mean age of the patients in our study was 53.74±5.5 years. In discrepancy to sub-Saharan African countries, the mean age of the patients was 47.4 years, demonstrating early age incidence of the disease.13
There is a male predominance of renal masses with a 3:2 ratio of male to female, as stated in the European association of urology guidelines on renal cell carcinoma.16 In contrast to the pooled analysis of data from sub-Saharan African countries, except for two studies (Benin 1.6:1, Nigeria 13:5 male-to-female ratio), there was a female predominance of RCC in 57.2% of the cases compared to males in 42.8%.17,18 The current study noticed a 2:1 male-to-female ratio of renal mass, showing more than twofold male predominance.
In our study, most of the masses were in the right kidney, which aligns with a study reported by Muhammed A et al, who conducted a 10 years retrospective study in Nigeria and observed right-side predominance in 68.6%.19
More than 90% of RCC histological subtypes are clear cell, papillary, and chromophobe. Clear cell RCC represents 75% of RCC cases and is the most common and aggressive type, while papillary RCC accounts for 10%; and has a better survival rate than the clear cell. Chromophobe RCC accounts for 5% and carries the best prognosis rate and the lowest metastatic rate in only 7% of cases.12 Our cohort revealed that clear cell RCC was the most common histological type, followed by papillary RCC. Regarding the comorbidities, 28.6% had diabetes, 25% were obese, 19% of the patients had hypertension, and 15.4% were smokers. To date, smoking, obesity, and hypertension are the consistent risk factors for RCC.14
About 20–30% overall recurrence rate after nephrectomy was reported depending on the clinical stage and grade, while the 5-year risk of recurrence in several retrospective studies has shown 60% in high-risk patients and 7–10% in low-risk patients. About 8.3% of our cases returned with local recurrence.20 Most of the patients do not return with follow-up with medical imaging due to the inability to access the health facility, shortage of tertiary centers, far distance from health services, and the low socioeconomic state of our people. In a retrospective study of 74 RCC patients from Senegal over a nine-year, B. Fall et al reported a 12% tumor recurrence and 47.3% cancer-specific mortality rate, which is compatible with the present study.21
The 5-year survival rate for stage I is 93%, stage II/III is 72.5%, and stage IV only for 12%. A multi-institutional large retrospective study of 5670 patients over 36 years who underwent radical or partial nephrectomy from seven Latin American countries and Spain reported by Zequi et al found the 5-year survival for RCC to be 86.1%.22 The five-year survival rate of our study was 62.8%, which is lower than the survival rate mentioned above. About 26.2% of the cases were diagnosed with metastatic disease, and a further 6% progressed to metastatic cancer despite surgical resection.
Most of the data reported from SSA have shown locally advanced to metastatic disease presentation. Only SALAKO from Nigeria and Tengue from Togo reported that 60.8% and 47.1% of the cases had localized RCC.18,23 Seventy-one percent of our patients presented with localized RCC. Fifty percent of the patients in this study held tumor stage 2, followed by T1 in 21.4%, 15.5% in T4, and 13.1% in T3, which is in contrast to most of the studies reported from SSA. Tijani from Nigeria reported that most of his cases bore T3 in 39 (60.9%) and T4 in 21 (32.8%) of patients.24 58% had T4, and 21% had T3 in a retrospective study reported by MBAERI TU and associates.25
Our cohort revealed that 54.5% of patients younger than 40-years had localized RCC, with clinically symptomatic cases predominantly patients younger than 40-year. A 10-year retrospective Indian study, which included 198 patients (n=36, 18% <40 years and n=162, 82% older patients) reported that 63.8% of younger patients were diagnosed with RCC stages 1 and 2.26 Another 10-year review study of 445 (n=104, 23% patients 40 years or younger) presented that younger patients had more aggressive diseases such as positive lymph node and metastasis at the time of diagnosis.27 The present study showed that the rate of young patients was 13%. The previously reported rate ranges between 3% and 7% in patients <40-years. However, an increasing incidence rate in this age group was observed in the last decades compared to older patients.28
The mean tumor size in our research was 6.38±2.4 cm. Four SSA publications reported an average tumor size of 15.1 cm.29 Most RCC cases in developed countries are discovered incidentally on imaging based on ultrasound and computed tomography of the abdomen. The survival rate is highly dependent on the stage at diagnosis, with metastatic disease having the least survival rate of about 12% at five years.12 Due to less access to the health services and facilities, the absence of the awareness of the population, deficiency of well-equipped hospitals, rural distribution, and poverty status of the patients living in low-income countries lead to present with late and advanced disease.
Strengths and Limitations
1) this is a single-center-based study, although it is the sole tertiary and referral hospital and the only cancer center. 2) The study misses several factors such as lifestyle habits and occupational exposures. 3) No molecular biology and adjuvant chemotherapy available in Somalia. The present study is the first report regarding the prevalence, clinical and histopathological features of RCC in Somalia. We believe that the results of this study provide a significant contribution to global RCC incidence and mortality.
Conclusion
The study findings showed a satisfactory outcome, 71.4% of our patients presented with localized RCC, the five-year survival rate of the patients was 62.8%, and the mortality rate was substantially higher for patients with a higher stage, a higher grade tumor, and metastatic disease at the time of diagnosis. The prevalence of RCC in our study was 0.7%, and 6 cases were pediatric age group. Less access to the health services and facilities, the absence of the awareness of the population, limited availability of endourological equipment, inadequate expertise and imaging modalities, a far distance from health services, and the low socioeconomic status lead to most of the patients living in low-income countries presenting with advanced diseases.
Abbreviations
ISUP, International Society of Urologic Pathology; ICD, International Classification of Diseases; HIS, hospital information system; RCC, renal cell carcinoma; SSA, Sub-Saharan Africa; WHO, World Health Organization.
Data Sharing Statement
Data included in the manuscript.
Institutional Review Board Statement
The ethical research board committee of Mogadishu Somalia Turkish Training and Research Hospital (REF. MSTH-9006) approved the research. This study was carried out in accordance to the Helsinki Declaration contents.
Informed Consent Statement
All study participants and a parent of participants under 18 years of age previously consented to use their medical and surgical data in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that this study has not received any funding resources.
Disclosure
The authors report no conflicts of interest associated with this publication.
References
1. Inamura K. Renal cell tumors: understanding their molecular pathological epidemiology and the 2016 WHO classification. Int J Mol Sci. 2017;18(10):15–20. doi:10.3390/ijms18102195
2. Muglia VF, Prando A. Renal cell carcinoma: histological classification and correlation with imaging findings. Radiol Bras. 2015;48(3):166–174. doi:10.1590/0100-3984.2013.1927
3. Mahasin SZ, Aloudah N, Al-Surimi K, Alkhateeb S. Epidemiology profile of renal cell carcinoma: a 10-year patients’ experience at King Abdulaziz Medical City, National Guard Health Affairs, Saudi Arabia. Urol Ann. 2018;10(1):59–64. doi:10.4103/UA.UA_102_17
4. Thorstenson A, Bergman M, Scherman-Plogell AH, et al. Tumour characteristics and surgical treatment of renal cell carcinoma in Sweden 2005–2010: a population-based study from the National Swedish Kidney Cancer Register. Scand J Urol. 2014;48(3):231–238. doi:10.3109/21681805.2013.864698
5. Hötker AM, Karlo CA, Di Paolo PL, et al. Renal cell carcinoma: associations between tumor imaging features and epidemiological risk factors. Eur J Radiol. 2020;129:109096. doi:10.1016/j.ejrad.2020.109096
6. Tahbaz R, Schmid M, Merseburger AS. Prevention of kidney cancer incidence and recurrence: lifestyle, medication and nutrition. Curr Opin Urol. 2018;28(1):62–79. doi:10.1097/MOU.0000000000000454
7. Taneja SS. Re: large prospective investigation of meat intake, related mutagens, and risk of renal cell carcinoma. J Urol. 2012;187(6):2022–2023. doi:10.1016/j.juro.2012.02.2546
8. Andreiana BC, Stepan AE, Mărgăritescu C, et al. Histopathological prognostic factors in clear cell renal cell carcinoma. Curr Heal Sci J. 2018;44(3):201–205.
9. Rossi SH, Prezzi D, Kelly-Morland C, Goh V. Imaging for the diagnosis and response assessment of renal tumours. World J Urol. 2018;36(12):1927–1942. doi:10.1007/s00345-018-2342-3
10. Ferlay J, Colombet M, Soerjomataram I, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries and 25 major cancers in 2018. Eur J Cancer. 2018;103:356–387. doi:10.1016/j.ejca.2018.07.005
11. Tahtabasi M, Mohamud Abdullahi I, Kalayci M, Gedi Ibrahim I, Er S. Cancer incidence and distribution at a Tertiary Care Hospital in Somalia from 2017 to 2020: an initial report of 1306 cases. Cancer Manag Res. 2020;12:8599–8611. doi:10.2147/CMAR.S277202
12. Padala SA, Barsouk A, Thandra KC, et al. Epidemiology of renal cell carcinoma. World J Oncol. 2020;11(3):79–87. doi:10.14740/wjon1279
13. Cassell A, Jalloh M, Yunusa B, et al. Management of renal cell carcinoma — current practice in Sub-Saharan Africa. J Kidney Cancer VHL. 2019;6(4):1–9. doi:10.15586/jkcvhl.2019.122
14. Capitanio U, Bensalah K, Bex A, et al. Epidemiology of renal cell carcinoma [figure presented]. Eur Urol. 2019;75(1):74–84. doi:10.1016/j.eururo.2018.08.036
15. van der Beek JN, Hol JA, Coulomb-l’Hermine A, et al. Characteristics and outcome of pediatric renal cell carcinoma patients registered in the International Society of Pediatric Oncology (SIOP) 93-01, 2001 and UK-IMPORT database: a report of the SIOP-Renal Tumor Study Group. Int J Cancer. 2021;148(11):2724–2735. doi:10.1002/ijc.33476
16. Ljungberg B, Bensalah K, Canfield S, et al. EAU guidelines on renal cell carcinoma: 2014 update. Eur Urol. 2015;67(5):913–924. doi:10.1016/j.eururo.2015.01.005
17. Avakoudjo D, Hounnasso PP, Traore MT, et al. Experience with managing solid kidney tumours in Cotonou, Benin Republic. J West African Coll Surg. 2014;4;4:100–111.
18. Salako AA, Badmus TA, Badmos KB, David RA, Laoye A, Akinbola IA. Renal cell carcinoma in a semi-urban population of south-western Nigeria. East Afr Med J. 2017;94(1):37–43.
19. Muhammed A, Tijjani L, Yusuf M, Abdullahi S, Ahmad B, Almustapha L. Pathologic characteristics and management of renal cell carcinoma in Zaria, Nigeria. Sub-Saharan African J Med. 2015;2(1):1. doi:10.4103/2384-5147.151559
20. Mayrhofer K, Niedersüß-Beke D. Evidence-based follow-up in renal cell carcinoma. Mag Eur Med Oncol. 2020;13(1):78–83.
21. Fall B, Diao B, Sow Y, et al. Le cancer du rein de l’adulte au Sénégal: aspects épidémiologiques et cliniques actuels et évolution du profil sur les deux dernières décennies. [Adult renal cancer in Senegal: Current epidemiological, clinical features,profile’s evolution over the two past decades]. Prog En Urol. 2011;21(8):521–526. French. doi:10.1016/j.purol.2011.02.013
22. Zequi SDC, Mourão TC, De Oliveira MM, et al. Predictors of survival outcomes in non-metastatic renal cell carcinoma in Latin America and Spain: a multicentric analysis. Kidney Cancer. 2019;3(4):253–261. doi:10.3233/KCA-190068
23. De RS, Sylvanus CHU. Le cancer du rein de l’adulte au Togo: frequence, diagnostic, traitement et evolution renal carcinoma of adult in Togo: frequency, diagnosis, therapeutic and evolutionary aspects. Revue Africaine d’Urologie Et d’Andrologie. 2015;1:177–182.
24. Tijani KH, Anunobi CC, Ezenwa EV, et al. Adult renal cell carcinoma in Lagos: experience and challenges at the Lagos University Teaching Hospital. African J Urol. 2012;18(1):20–23. doi:10.1016/j.afju.2012.04.005
25. Mbaeri TU, Orakwe JC, Nwofor AM, Oranusi CK, Ulebe AO. Malignant renal tumours in adults in Nnamdi Azikiwe University Teaching Hospital, Nnewi, Nigeria. Niger J Med. 2012;21(3):300–303.
26. Pal DK, Maurya AK, Jana D. Comparative study of renal cell carcinoma in patients less than 40 years of age and older age patients: a retrospective single-center study. Indian J Cancer. 2018;55(3):297. doi:10.4103/ijc.IJC_636_17
27. Douglas B, Davaro F, May A, Siddiqui S, Hamilton Z. Clinical characteristics of renal cell carcinoma in patients under the age of 40. Urol Oncol. 2021;39(7):438–e23. doi:10.1016/j.urolonc.2021.04.008
28. Sierra PS, Cordeiro MD, Albuquerque EV, et al. Oncologic outcomes in young adults with kidney cancer treated during the targeted therapy era. Clin Genitourin Cancer. 2020;18(2):e134–e144. doi:10.1016/j.clgc.2019.09.012
29. Coulibaly M, Sissoko I, Berthé A, et al. Management of kidney cancers in urology department of the Gabriel Toure University Hospital/Bamako. Surg Sci. 2018;9(6):183–188. doi:10.4236/ss.2018.9621
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.