Back to Journals » Journal of Inflammation Research » Volume 18
Eosinophilic Granulomatosis with Polyangiitis Presenting as Acute Abdomen: A Rare Case Report
Authors Liao Y, Xiong J, Huang W
Received 8 August 2025
Accepted for publication 27 November 2025
Published 28 December 2025 Volume 2025:18 Pages 18193—18204
DOI https://doi.org/10.2147/JIR.S559438
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Wenjian Li
Yan Liao, Jiao Xiong, Wenlong Huang
Department of Emergency Medicine, General Hospital of the Western Theater Command, Chengdu, Sichuan, 610083, People’s Republic of China
Correspondence: Wenlong Huang, Department of Emergency Medicine, General Hospital of the Western Theater Command, No. 270, Rongdu Avenue, Jinniu District, Chengdu, Sichuan, 610083, People’s Republic of China, Email [email protected]
Background: ANCA-associated vasculitis (AAV) is a group of autoimmune diseases characterized by necrotizing inflammation and fibrinoid necrosis of small- and medium-sized blood vessels. Renal involvement is common in AAV; however, renal hemorrhage is extremely rare, particularly in cases of eosinophilic granulomatosis with polyangiitis (EGPA). Spontaneous renal hemorrhage often presents as acute abdomen.
Case Presentation: We report a 51-year-old male with a prior diagnosis of EGPA who presented to the emergency department with acute left-sided abdominal pain and signs of hypovolemic shock. Imaging revealed a massive left perirenal hematoma without active contrast extravasation, suggestive of renal rupture. Initial management focused on hemostasis and stabilization, but recurrent contralateral renal hemorrhage occurred during hospitalization. Further immunological, histopathological, and bone marrow evaluations confirmed EGPA complicated by renal involvement. The patient was treated with corticosteroids, cyclophosphamide, and rituximab, but recurrent hemorrhage indicated rapid disease progression or insufficient therapeutic response. Due to financial constraints, the patient was discharged prematurely, precluding long-term follow-up.
Discussion: This case highlights the complexity of diagnosing and managing AAV-associated renal hemorrhage, particularly in EGPA patients. While the renal vascular changes observed, such as inflammation and potential necrosis, may be linked to the underlying vasculitis in EGPA, causality should be interpreted with caution, as other factors like coagulopathy, concurrent infections, or iatrogenic effects could contribute. Current literature suggests that ANCA-associated mechanisms, including NETs formation, play a role in vascular damage, but direct causation in rare complications like renal hemorrhage remains uncertain and requires further investigation. While EGPA treatment primarily involves immunosuppressive therapy targeting vasculitis and eosinophilia, spontaneous renal hemorrhage requires an integrated approach, including conservative management, interventional embolization, or surgical exploration in life-threatening cases. Reports of AAV-associated renal hemorrhage are rare, and large-scale studies are lacking, necessitating further research to optimize treatment strategies.
Keywords: vasculitis, anti-neutrophil cytoplasmic antibody-associated vasculitis, renal hemorrhage
Introduction
Acute abdomen is a common critical condition encountered in emergency medicine, with non-traumatic causes accounting for approximately 5–10% of all emergency department (ED) visits based on recent multicenter studies and registries.1 For instance, a 2023 analysis of over 1 million ED presentations in the US reported non-traumatic acute abdominal pain in 6.8% of cases, while a 2024 European cohort study documented rates up to 9.2% in high-volume centers.1 These updated figures reflect variations by region, patient demographics, and healthcare access, but consistently highlight its prevalence in emergency settings. Renal hemorrhage can present as a distinct acute abdominal syndrome and is classified based on its etiology into traumatic and spontaneous renal hemorrhage. Spontaneous renal hemorrhage (SPH), also known as spontaneous renal hematoma, subcapsular renal hemorrhage, non-traumatic perirenal hematoma, or Wunderlich syndrome (WS),2 refers to an acute onset of non-traumatic subcapsular and perirenal hematomas. Its typical clinical manifestations include the triad of acute lower back pain, abdominal pain, and hypovolemic shock.3 Common underlying causes of SPH include rupture of renal angiomyolipomas, renal tumor rupture, hemorrhage from multiple renal cysts, rupture of renal vascular lesions, or coagulation disorders leading to spontaneous renal bleeding.
Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is clinically classified into granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), and eosinophilic granulomatosis with polyangiitis (EGPA).4 Lesions in EGPA are comprised of necrotizing vasculitis associated with ANCA and eosinophil-associated tissue damage. A recent study demonstrated the importance of neutrophils in the development of vasculitis associated with ANCA.5 Another study visualized the behavior of eosinophils in EGPA.6 The diagnostic criteria for EGPA, according to the 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification, include a scoring system where a total score of ≥6 points strongly supports the diagnosis. Key items include: maximum eosinophil count ≥1 × 109/L (+5 points), obstructive airway disease (+3 points), nasal polyps (+3 points), cytoplasmic ANCA or anti-PR3 positivity (−3 points), extravascular eosinophilic-predominant inflammation (+2 points), mononeuritis multiplex or motor deficit not due to radiculopathy (+1 point), and hematuria (−1 point).7 AAV is a rare autoimmune disease, with reported prevalence rates ranging from 23 to 421 cases per million population in various studies,8 and has become a significant focus of international and domestic research in recent years. Its clinical features are diverse and can include constitutional symptoms such as fever, fatigue, weight loss, malaise, night sweats, arthralgias, and myalgias; pulmonary involvement with cough, hemoptysis, dyspnea, and infiltrates; renal manifestations including hematuria, proteinuria, and rapidly progressive glomerulonephritis; ear, nose, and throat symptoms such as sinusitis, otitis media, and nasal crusting; skin lesions like palpable purpura; neurological symptoms including peripheral neuropathy and mononeuritis multiplex; and laboratory abnormalities such as anemia, thrombocytosis, elevated erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP).9 The exact etiology of AAV remains unclear, although it is believed to involve a combination of genetic predisposition and environmental triggers, including infections, silica exposure, and certain drugs.10 ANCA is an autoantibody found in the serum of patients with vasculitis and serves as a specific marker for its diagnosis. AAV is characterized by necrotizing inflammation of small blood vessels with immune complex deposition, often leading to systemic involvement. Due to the kidney’s rich vascularity, AAV frequently manifests as segmental necrotizing glomerulonephritis in the early stages. Advanced disease or severe cases can present with crescentic glomerulonephritis, fibrinoid necrosis of small renal arterioles, or leukocytoclastic vasculitis in the renal medulla, resulting in diverse clinical manifestations.
This report describes the diagnosis and management of a case of vasculitis presenting with acute abdominal syndrome. By reviewing the literature, we discuss the complications, pathogenesis, clinical manifestations, and emergency management strategies for ANCA-associated vasculitis, with the aim of enhancing clinicians’ understanding of acute abdomen and ANCA-associated vasculitis complicated by renal hemorrhage. This study was approved by the Ethics Committee of General Hospital of the Western Theater Command (approval number: 2021ky105-1).
Case Presentation
A 51-year-old male patient presented to the emergency department on September 5, 2024, with a chief complaint of severe left-sided abdominal pain accompanied by profuse sweating lasting for one hour. The symptoms began one hour prior while the patient was using a massage device to gently tap on his lower back. He experienced sudden, severe pain in the left upper abdomen, which worsened with movement and deep breathing. The pain was accompanied by left-sided lower back discomfort, nausea, and profuse sweating. The patient denied any chest pain, diarrhea, vomiting, hemoptysis, or hematuria. After a brief period of rest, the symptoms partially alleviated. The patient had no history of trauma, poisoning, or hereditary diseases, and was brought to the emergency department by family members for further evaluation.
Physical Examination: The patient was alert and coherent but displayed signs of distress, with profuse sweating and a painful facial expression. Vital signs revealed a heart rate of 115–126 beats per minute, oxygen saturation of 98%, blood pressure ranging from 106–112/67–75 mmHg, and a body temperature of 38.9°C. Physical examination showed tenderness and rebound tenderness in the left upper and middle abdominal quadrants, along with localized muscle guarding. There was no tenderness in the right or lower abdominal regions. Percussion tenderness was noted in the left flank. Multiple dark purple, non-blanching rashes were observed on both upper and lower extremities. Two days prior to presentation, the patient had self-administered traditional Chinese medicine and Tibetan medicine, after which lower extremity purpura appeared, leading to a suspicion of allergic purpura (Henoch-Schönlein purpura, HSP); he was already receiving oral anti-allergic medication prescribed by an external hospital. Additionally, both ankles showed swelling and tenderness without evidence of skin ulceration (Figure 1).
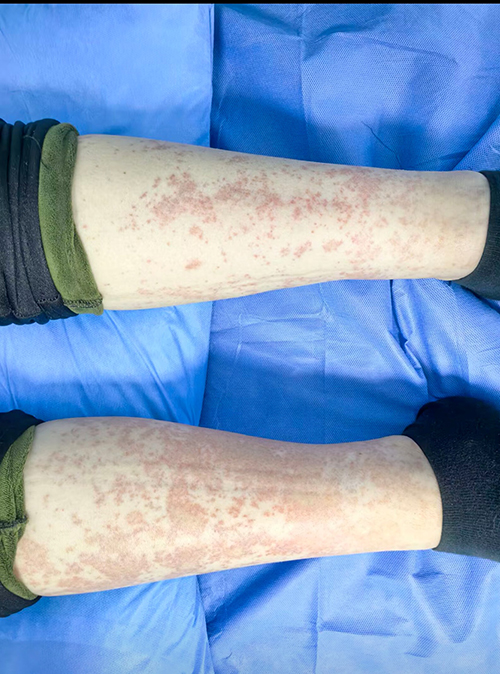 |
Figure 1 Purpuric Rash and Swelling of the Lower Extremities in a Patient with Eosinophilic Granulomatosis with Polyangiitis (EGPA). Multiple dark purple, non-blanching rashes are observed on the patient’s lower extremities, consistent with purpura, a characteristic manifestation of vasculitis. Additionally, swelling and tenderness are noted at both ankles, without evidence of skin ulceration. These findings support the clinical suspicion of systemic involvement in EGPA, which can include cutaneous manifestations such as purpura and eosinophilic infiltration in small vessels. |
Past Medical History: The patient was diagnosed with EGPA in the nephrology department of our hospital approximately one month prior, based on blood test results (including positive c-ANCA and anti-PR3 antibodies), skin biopsy findings consistent with vasculitis and eosinophilic infiltration, and clinical features such as asthma history, eosinophilia, and multi-organ involvement; abdominal ultrasound and CT at that time showed no abnormal renal changes, though urinalysis indicated occult blood (+-), proteinuria (+-), negative leukocytes, and urinary microalbumin/creatinine ratio of 70.13 mg/mmol. Renal and pulmonary biopsies were recommended but refused by the patient, who opted for treatment and observation instead. During the induction remission phase, the patient received methylprednisolone (glucocorticoid, GC) combined with cyclophosphamide (CTX) therapy. However, due to persistent and significant joint pain that did not respond to symptomatic treatment, the regimen was switched to rituximab (RTX) combined with glucocorticoid therapy. The patient reported no significant discomfort during this treatment. At the time of presentation, the patient was undergoing maintenance therapy with methylprednisolone (GC) and methotrexate (MTX). One month prior, during nephrology admission, abdominal CT showed left adrenal thickening with nodular protrusions, but no obvious parenchymal renal lesions (renal CTA was not performed), and no baseline vascular changes were documented.
Emergency management: The patient was placed under continuous electrocardiographic monitoring and administered 500 mL of lactated Ringer’s solution via intravenous infusion. Comprehensive emergency investigations were performed, including complete blood count (CBC), biochemical panel, coagulation profile, infectious panel, blood typing, and crossmatching. Additional imaging studies were conducted, including bedside ultrasound, chest and abdominal computed tomography (CT), and electrocardiogram (ECG). Preparations were made for potential surgical intervention.
Inspection result: The ECG showed sinus tachycardia. Bedside ultrasound revealed no abnormalities in the size or morphology of both kidneys, but a hypoechoic area measuring 12.7×6.7 cm with irregular borders and no detectable blood flow was observed around the left kidney, consistent with a hematoma. No significant intraperitoneal fluid was found. Chest CT indicated scattered ground-glass opacities in the middle lobe of the right lung and the dorsal segment of the left lower lobe. Abdominal CT revealed irregular morphology and heterogeneous density of the left kidney, suggestive of renal rupture with the formation of a perirenal hematoma (Figure 2). Laboratory tests upon admission showed elevated white blood cell count (16.63 × 109/L) and absolute neutrophil count (14.34 × 109/L), with an absolute eosinophil count of 1.3 × 109/L, a hemoglobin level of 101 g/L and platelet count of 407 × 109/L. Inflammatory markers were elevated, with high-sensitivity C-reactive protein (hs-CRP) at 96.4 mg/L and plasma D-dimer at 4.74 mg/L. Renal function tests showed elevated urea (12.01 mmol/L) and creatinine (168 μmol/L), with a reduced estimated creatinine clearance of 60.6 mL/min. Protein studies revealed low total protein (51.9 g/L) and albumin (28.7 g/L). Urinalysis was positive for occult blood and proteinuria.
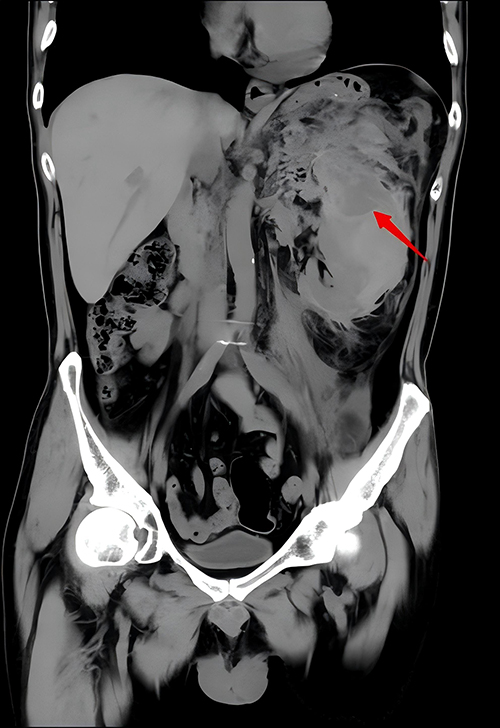 |
Figure 2 CT Image of Left Kidney Rupture with Perirenal Hematoma. A heterogeneous density shadow is observed surrounding the left kidney, accompanied by thickening and swelling of the renal fascia. The perirenal fat space is blurred, with multiple linear and flake-like mixed density areas present. The red arrow indicates the large perirenal hematoma formed due to the rupture and bleeding of the left kidney. |
Emergency treatment: The patient was placed on strict bed rest and nil per os (NPO). Tramadol (100 mg) was administered intramuscularly for pain relief, and intravenous aminocaproic acid (2 g) was given to control bleeding. Urological consultation was sought, and to prevent further hemorrhage and clinical deterioration, emergency digital subtraction angiography (DSA) was recommended with possible embolization if necessary. However, the patient was unable to tolerate the supine position and interventional procedure, and the family declined to proceed further. The procedure was terminated, and the patient was managed conservatively. Continued monitoring was advised, and if the patient experienced worsening hemorrhage, a decline in hemoglobin levels, or clinical deterioration, interventional or surgical procedures were planned under sedation and analgesia. The patient was subsequently admitted to the intensive care unit (ICU) for further treatment and investigation of the underlying cause.
Initial emergency diagnosis: The preliminary diagnosis upon emergency evaluation was as follows: left renal hemorrhage, hypovolemic shock (compensatory phase), ANCA-associated vasculitis, and pulmonary infection.
Inpatient management: Following ICU admission, the patient’s vital signs were continuously monitored, and absolute bed rest was enforced. Treatment included intravenous cefoperazone-sulbactam (2 g, three times daily) for infection control, intravenous aminocaproic acid (1 g, twice daily) for hemostasis, and intermittent tramadol for pain relief. Further diagnostic evaluations were conducted to clarify the underlying etiology.
Follow-Up diagnostic findings: Urinary microalbumin levels were significantly elevated at 98.30 mg/L. Urinary microalbumin-to-creatinine ratios were also elevated, with 11.06 mg/L (UACR-I) and 76.79 mg/L (UACR-II). Immunological testing revealed positive cytoplasmic anti-neutrophil cytoplasmic antibodies (c-ANCA) with a titer of 1:32 and strongly positive anti-proteinase 3 (PR3) antibodies (+++). Additional findings included elevated immunoglobulin E (IgE) at 1350.00 IU/mL, complement C3 at 1.53 g/L, and procalcitonin at 0.214 ng/mL. Serum protein electrophoresis showed decreased albumin (45.48%), increased α1-globulin (9.71%) and α2-globulin (15.91%), reduced β1-globulin (5.05%), and a reduced albumin-to-globulin ratio (0.81). Rheumatoid factor was elevated at 181.6 IU/mL. Plasma D-dimer was markedly elevated at 6.38 mg/L. Flow cytometry revealed negative T-lymphocyte subset abnormalities. Serum free light chain analysis showed elevated κ-free light chains (54.1 mg/L) and λ-free light chains (64.9 mg/L).
Pathological review: Bone marrow aspiration revealed nucleated cell volumes ranging from 41% to 60%, indicative of active bone marrow proliferation, with no other significant abnormalities noted. Cytological analysis of bone marrow showed hyperactive proliferation of nucleated cells, with granulocyte lineage accounting for 76% and erythroid lineage accounting for 15.5%, yielding a granulocyte-to-erythroid ratio of 4.9. Eosinophils constituted 21% of cells, with generally normal morphology. Erythroid lineage displayed active proliferation, predominantly at the mid-to-late erythroblast stage, with no significant abnormalities in cell morphology (Figure 3A). Skin biopsy review showed epidermal detachment, irregular squamous epithelial hyperplasia with excessive keratinization, and dense infiltration of lymphocytes and occasional eosinophils around small dermal vessels and appendages (Figure 3B).
 |
Figure 3 Histopathological Findings from Skin and Bone Marrow Biopsies. (A) Skin biopsy shows loss of the stratum lucidum, irregular hyperplasia of squamous epithelium, and hyperkeratosis. In the dermis, small blood vessels and adnexal structures are infiltrated by lymphocytes and scattered eosinophils, indicating cutaneous involvement of vasculitis. (B) Bone marrow biopsy reveals significantly increased nucleated cell proliferation with active granulopoiesis and a markedly elevated proportion of eosinophils, consistent with eosinophilic hyperplasia often observed in eosinophilic granulomatosis with polyangiitis (EGPA). |
Final diagnosis: The patient was diagnosed with the following conditions: left renal hemorrhage, EGPA, ANCA-associated nephritis, Henoch-Schönlein purpura, mild anemia, and pulmonary infection.
Specialized treatment plan: After nephrology consultation, a specialized treatment plan was initiated. The patient received methylprednisolone (40 mg intravenous infusion once daily), along with vitamin D supplementation, gastric acid suppression, and neurotrophic support. Meropenem (1 g intravenous infusion every 12 hours) was administered for infection control, and trimethoprim-sulfamethoxazole was prescribed for Pneumocystis jirovecii pneumonia prophylaxis. Blood bacterial culture and next-generation sequencing (NGS) of blood samples were recommended to further investigate the underlying cause. On September 9, the patient developed persistent fever with temperatures fluctuating between 38.0–39.3°C. NGS results detected cytomegalovirus (CMV) infection, and ganciclovir (0.25 g intravenous infusion once daily) was added for antiviral therapy. From September 12 to September 14, the patient’s temperature normalized. Repeat blood tests showed a WBC count of 15.92 × 109/L, platelet count of 434 × 109/L, neutrophil percentage of 91.6%, and high-sensitivity C-reactive protein (hs-CRP) reduced to 20.44 mg/L. Antibiotics were adjusted to moxifloxacin (0.4 g intravenous infusion once daily) and piperacillin-tazobactam (2.25 g intravenous infusion every 12 hours). Methylprednisolone was continued at 20 mg intravenous infusion three times daily, while ganciclovir (0.25 g once daily) and oral trimethoprim-sulfamethoxazole (0.48 g once daily) were maintained. A repeat abdominal ultrasound revealed partial absorption of the left perirenal hematoma (Figure 4A). The current treatment regimen was continued with periodic follow-up of laboratory and imaging indicators. Serial laboratory results for key parameters (Hb, WBC, and Cr) demonstrated progressive changes during hospitalization, reflecting anemia worsening with bleeding episodes, leukocytosis consistent with inflammation/infection, and fluctuating renal function indicative of ongoing vasculitis/nephritis (Table 1).
 |
Table 1 Serial Laboratory Results for Hb, WBC, and Cr Trends |
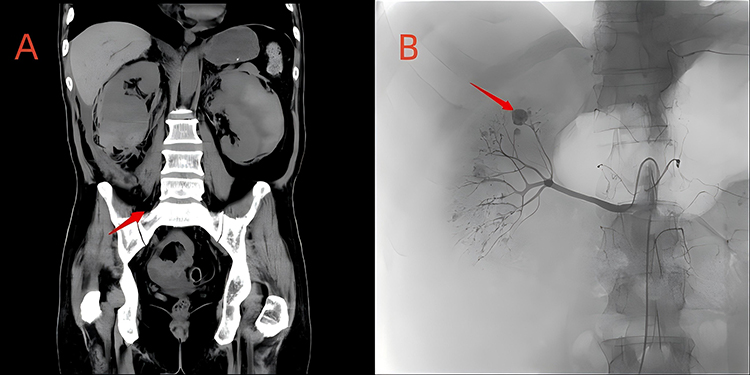 |
Figure 4 CT and Intraoperative Findings of Renal Hemorrhage and Arterial Aneurysms. (A) Coronal CT image showing a heterogeneous density shadow (indicated by the red arrow) around the right kidney consistent with recent bleeding and hematoma formation. The surrounding hematoma around the right kidney is fresh, while hemorrhage near the left kidney shows absorption signs. (B) Intraoperative angiography revealing scattered small arterial aneurysms. The red arrow specifically indicates a small arterial aneurysm in a branch of the renal artery. The image also shows that the active bleeding site was successfully controlled with coil embolization. |
On September 18, the patient experienced sudden, severe pain in the right flank. Repeat abdominal ultrasound suggested possible right renal hemorrhage, and the patient exhibited signs of shock. Emergency transfusions of packed red blood cells and cryoprecipitate were administered. DSA was performed, revealing scattered small arterial aneurysms in both renal arteries. Although arterial aneurysms are extremely rare in EGPA, in this case, they may be attributable to the underlying necrotizing vasculitis causing vessel wall weakening and aneurysmal dilatation, potentially exacerbated by ongoing inflammation or incomplete disease control, as no alternative causes such as connective tissue disorders or infections were identified in the workup. No active contrast extravasation was observed in the left renal region. Active bleeding from a branch of the right renal artery was identified and treated with coil embolization (Figure 4B).
Eight hours post-procedure, the patient’s heart rate stabilized at 120 beats per minute, with normal blood pressure and oxygen saturation. Follow-up laboratory tests showed a hemoglobin level of 57 g/L, WBC count of 29.98 × 109/L, platelet count of 479 × 109/L, and neutrophil percentage of 92.6%. Additional transfusions of packed red blood cells were administered. The patient’s condition was stabilized, and the previous treatment regimen was continued with close monitoring.
On September 20, due to financial constraints, the patient’s family opted to discontinue treatment, and the patient was discharged from the hospital. Treatment algorithm flowchart see Figure 5.
 |
Figure 5 Treatment Algorithm Flowchart. |
Discussion
Background and Purpose
Rupture and hemorrhage of solid organs is a common critical condition encountered in the emergency department. In the absence of a history of trauma, such conditions are often overlooked. Spontaneous renal hemorrhage, commonly presenting as acute abdomen, is usually caused by ruptured angiomyolipomas, renal tumors, cysts, or aneurysms resulting from vascular malformations. These conditions are often detected during routine physical examinations or emergency imaging at the time of symptom onset. However, renal hemorrhage associated with ANCA-associated vasculitis is rare and poses unique diagnostic challenges. The kidney structure may appear normal in the absence of bleeding, and even during active hemorrhage, imaging studies may fail to identify specific lesions.
In this case, the patient presented with acute abdomen and was diagnosed with a massive perirenal hematoma. The initial focus in emergency management was to stabilize the patient’s condition and control the bleeding. However, identifying the underlying cause was critical to prevent further complications. Additional findings, including purpura on the patient’s lower extremities and acute-onset hypoalbuminemia, raised suspicion of a systemic disease rather than an isolated organ pathology. This prompted further investigations, including immunological assays, skin biopsy, and bone marrow aspiration, which ultimately confirmed the diagnosis.
This case highlights the importance of considering systemic diseases as potential causes of acute and critical conditions in the emergency setting. Emergency physicians must go beyond symptomatic management and actively seek underlying etiologies to optimize treatment and prevent disease progression.
Pathogenesis of Renal Hemorrhage Induced by AAV
ANCA-AAV is a group of autoimmune diseases characterized by necrotizing inflammation and fibrinoid necrosis of small- and medium-sized blood vessels. AAV can affect multiple organs and tissues throughout the body, with the kidneys and lungs being the most commonly involved. Other potential targets include the gastrointestinal tract, brain, eyes, ears, and skin. Renal involvement is a frequent manifestation of AAV, with kidney damage occurring in approximately 90% of microscopic polyangiitis (MPA) cases, 80% of granulomatosis with polyangiitis (GPA) cases, and 45% of eosinophilic granulomatosis with polyangiitis (EGPA) cases.11 Renal damage is often characterized by crescentic glomerulonephritis or sclerosing glomerulonephritis.12 The disease frequently involves renal microvasculature, causing inflammation, necrosis, and granulomatous infiltration of the glomeruli and small renal arteries. Clinically, this manifests as hematuria, edema, rapid elevation of serum creatinine, hypertension, proteinuria, and rapidly progressive glomerulonephritis (RPGN).13
In this case, the patient had a prior diagnosis of AAV, specifically the EGPA subtype, which is relatively rare. The primary pathological features of EGPA include eosinophilic infiltration, granuloma formation, and necrotizing vasculitis involving small- and medium-sized vessels. Despite ongoing maintenance therapy, the patient experienced renal hemorrhage after mild external force—using a massage device on the lower back—which likely caused minor trauma to the diseased renal tissue. The kidney, already extensively affected by vasculitis, with rich blood supply and fragile tissue integrity, rapidly developed significant hemorrhage. This led to acute symptoms, including flank pain, abdominal pain, peritoneal irritation, tachycardia, profuse sweating, and eventually hypovolemic shock.
Treatment
Management of Renal Hemorrhage
The causes of renal hemorrhage include iatrogenic injury, spontaneous renal rupture, and trauma-induced renal laceration. Spontaneous renal rupture may be caused by benign or malignant tumors, inflammation, calculi, cysts, vascular diseases, or coagulation disorders. Tumors that grow rapidly and increase in size can compress renal tissue, causing localized ischemia and rendering the tissue more fragile. Infections such as bacterial or tuberculosis-related infections can also lead to degenerative necrosis and rupture of renal tissue. Additionally, minor trauma or physical activities such as coughing, constipation, or running can cause vascular rupture in cases of vascular abnormalities. Renal hemorrhage often results in perirenal, subcapsular, or retroperitoneal hematomas, which are typically confirmed in the emergency setting using ultrasound, abdominal CT, or contrast-enhanced CT imaging.
The management of renal hemorrhage includes conservative medical therapy, surgical intervention, and interventional embolization. Not all cases of renal hemorrhage require emergency surgical treatment. For patients suspected of having ongoing bleeding with progressive hemoglobin decline, digital subtraction angiography (DSA) and interventional embolization should be performed promptly. In cases where bleeding cannot be controlled, surgical exploration may be necessary. For patients with stable hemoglobin levels and no evidence of ongoing hemorrhage, conservative treatment with strict bed rest and close monitoring is appropriate. If the cause of the hemorrhage is unclear, nephrectomy should be approached with caution.
For active bleeding, interventional embolization has become the preferred treatment due to its minimally invasive nature, high accuracy, and low complication rate. The choice of embolization technique depends on the etiology of the bleeding. For small-caliber bleeding vessels, gelatin sponge particles can be used for embolization, while larger vessels may require microcoils. In complex cases involving rich vascularity, such as pseudoaneurysms, microcoils alone or in combination with gelatin sponge particles are often utilized for embolization.14
In this case, the patient was diagnosed with renal hemorrhage in the emergency department and was closely monitored. As the patient did not initially exhibit active hematuria or hemodynamic instability, he was treated conservatively with hemostatic agents. However, during the observation period, the patient showed signs of active bleeding, prompting an urgent interventional procedure for embolization.
Treatment of AAV-Associated Renal Hemorrhage
Organ hemorrhage resulting from ANCA-AAV is a life-threatening manifestation of the disease. Hemorrhage can occur in various organs, including the lungs, gastrointestinal tract, brain, skin, muscles, and soft tissues. Among these, alveolar hemorrhage is the most common hemorrhagic complication, with an incidence of 25%–60%. Gastrointestinal hemorrhage occurs in 22–30% of cases, while cerebral hemorrhage is relatively rare, occurring in approximately 4% of cases, primarily in patients with anti-MPO-ANCA positivity.15 Renal hemorrhage secondary to AAV is exceptionally rare, with only a few reported cases.16,17 Due to the scarcity of such cases, there is limited clinical experience in its treatment, which mainly focuses on addressing the underlying cause combined with supportive care.
The clinical management of AAV with organ involvement or life-threatening manifestations follows established treatment protocols. These typically consist of two components: initial immunosuppressive therapy (induction therapy) aimed at achieving disease remission, and maintenance immunosuppressive therapy designed to prevent disease relapse.18
For EGPA with renal hemorrhage as in this case, treatment targeted both vasculitis and eosinophilia to control disease activity and prevent further bleeding. Systemic corticosteroids (GC) served as the cornerstone, with induction therapy using high-dose methylprednisolone combined with cyclophosphamide (CTX) for severe manifestations, consistent with guidelines for patients with poor prognostic factors (FFS ≥ 1).19 Due to refractory joint pain, the regimen was switched to rituximab (RTX), which depletes B cells and has shown efficacy in ANCA-positive EGPA with renal involvement.20 Anti-IL-5 therapies like mepolizumab were not used here but could be considered in future relapses to target eosinophilia and reduce glucocorticoid dependence, as supported by clinical trials demonstrating remission and steroid-sparing effects.21 Upon admission for hemorrhage, the patient met criteria for severe active disease and received corticosteroid pulse therapy with CTX, leading to temporary stabilization before recurrent bleeding prompted embolization and supportive care.
Analysis of Recurrent Hemorrhage During Treatment
The patient was undergoing maintenance therapy at the time of the initial renal hemorrhage, which was triggered by minor external force applied to the kidney. This raises the possibility that the disease was not fully controlled, though limited case data precludes definitive conclusions regarding suboptimal regimen or relapse. After the initial hemorrhage, the patient was admitted and reinitiated on induction therapy, leading to gradual absorption of the hematoma in the affected kidney and temporary stabilization of the disease. However, subsequent hemorrhage occurred in the contralateral kidney, which may have been due to rapid disease progression or insufficient efficacy of the treatment. Additionally, the possibility of the chosen treatment regimen being unsuitable for this patient, requiring adjustment of drug types and dosages, cannot be excluded. Unfortunately, as the patient was discharged prematurely due to financial constraints, the long-term treatment efficacy could not be evaluated, nor was it possible to modify the therapeutic approach to clarify whether the recurrent bleeding was related to the choice of medication.
Currently, reports and research on ANCA-AAV complicated by renal hemorrhage are scarce, and EGPA-induced renal hemorrhage is even more uncommon.16,22 A single case has been reported in China, but without detailed documentation. Although there are reports of other hemorrhagic complications of AAV, such as cerebral, pulmonary, and gastrointestinal bleeding, large-scale studies are lacking.
This case provides valuable insight into the clinical recognition of vasculitis-associated renal hemorrhage. It emphasizes the importance of adopting a systemic approach to diagnosing and managing such cases in emergency settings. Emergency physicians should avoid oversimplifying the condition and instead focus on deeper exploration of the underlying systemic disease. This can help ensure that treatment is not merely symptomatic but also addresses the root cause, effectively preventing further deterioration and recurrence. To prevent such recurrences and monitor disease progression in similar cases, a standardized follow-up protocol is recommended based on established vasculitis guidelines. This could include: (1) Clinical assessments every 1–3 months post-discharge to evaluate symptoms, vital signs, and organ function; (2) Laboratory monitoring every 1–3 months, including complete blood count (with eosinophil count), renal function tests (creatinine, eGFR, urinalysis for hematuria/proteinuria), inflammatory markers (ESR, CRP), and ANCA titers to detect early relapse; (3) Imaging follow-up with abdominal ultrasound or CT every 3–6 months initially, or sooner if symptoms recur, to assess hematoma resolution, renal morphology, and vascular integrity; (4) Adjustment of immunosuppressive therapy based on disease activity scores (eg, BVAS) and consultation with rheumatology/nephrology specialists; and (5) Patient education on avoiding trauma and recognizing warning signs of bleeding or relapse.19,23 Such a protocol aims to optimize long-term outcomes, reduce relapse risk, and facilitate early intervention in AAV patients with renal involvement.
Conclusion
This case report describes a rare presentation of EGPA manifesting as acute abdomen due to spontaneous renal hemorrhage, highlighting the diagnostic and therapeutic challenges in emergency settings. Despite initial conservative management and subsequent immunosuppressive therapy, the patient experienced recurrent bilateral renal bleeding, underscoring the potential for rapid disease progression in AAV even under maintenance treatment. Key insights include the importance of recognizing systemic vasculitis as an underlying cause of non-traumatic renal hemorrhage, the value of prompt immunological and pathological investigations, and the efficacy of interventional embolization for controlling active bleeding when conservative measures fail. Clinicians should adopt a comprehensive, multidisciplinary approach to address both hemorrhagic complications and the root autoimmune pathology, potentially preventing further organ damage and improving outcomes. However, a major limitation of this report is the absence of long-term follow-up data due to the patient’s early discharge for financial reasons, which precludes assessment of treatment durability, disease remission, or potential relapses. Further studies and case series are needed to better understand the pathogenesis, optimal management strategies, and prognosis of EGPA-associated renal hemorrhage.
Data Sharing Statement
The experimental data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
Institutional approval for the publication of this case report was obtained from the Ethics Committee of General Hospital of the Western Theater Command. (approval number: 2021ky105-1). All methods were carried out in accordance with Declaration of Helsinki.
Consent for Publication
The author obtained permission from the patient to publish this case report. The patient explicitly agreed to the anonymized reporting of their case details, in accordance with the Declaration of Helsinki and the Ethics Committee of General Hospital of the Western Theater Command ethical guidelines.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not fund by anything.
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Wu RR, Adjei-Poku MN, Kelz RR, et al. Trends in visits, imaging, and diagnosis for emergency department abdominal pain presentations in the United States, 2007-2019. Acad Emerg Med. 2025;32(1):20–31. doi:10.1111/acem.15017
2. Shah JN, Gandhi D, Prasad SR, et al. Wunderlich syndrome: comprehensive review of diagnosis and management [published correction appears in radiographics. 202343(7):e239007]. Radiographics. 2023;43(6):e220172. doi:10.1148/rg.220172
3. Elbaset MA, Zahran MH, El-Baz R, Badawy M, Osman Y. Spontaneous renal hemorrhage: critical analysis of different lines of management in non-traumatic patients: a single tertiary center experience. Int Urol Nephrol. 2020;52(3):423–429. doi:10.1007/s11255-019-02333-9
4. Nakazawa D, Masuda S, Tomaru U, Ishizu A. Pathogenesis and therapeutic interventions for ANCA-associated vasculitis [published correction appears in Nat Rev Rheumatol. 201915(2):123]. Nat Rev Rheumatol. 2019;15(2):91–101. doi:10.1038/s41584-018-0145-y
5. Koike H, Takahashi M, Ohyama K, Fukami Y, Aoki M, Katsuno M. Early ultrastructural lesions of anti-neutrophil cytoplasmic antibody- versus complement-associated vasculitis. Neuropathology. 2022;42(5):420–429. doi:10.1111/neup.12821
6. Koike H, Takahashi M, Ohyama K, Fukami Y, Aoki M, Katsuno M. In vivo visualization of eosinophil secretion in eosinophilic granulomatosis with polyangiitis: an ultrastructural study. Allergol Int. 2022;71(3):373–382. doi:10.1016/j.alit.2022.02.009
7. DCVAS Study Group, Grayson PC, Ponte C, Suppiah R, et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for eosinophilic granulomatosis with polyangiitis. Ann Rheum Dis. 2022;81(3):309–314. doi:10.1136/annrheumdis-2021-221795
8. Berti A, Cornec D, Crowson CS, Specks U, Matteson EL. The epidemiology of antineutrophil cytoplasmic autoantibody–associated vasculitis in Olmsted County, Minnesota: a twenty-year US population–based study. Arthritis Rheumatol. 2017;69(12):2338–2350. doi:10.1002/art.40207
9. Almaani S, Fussner LA, Brodsky S, Meara AS, Jayne D. ANCA-associated vasculitis: an update. J Clin Med. 2021;10(7):1446. doi:10.3390/jcm10071446
10. Geetha D, Jefferson JA. ANCA-Associated Vasculitis: core Curriculum 2020. Am J Kidney Dis. 2020;75(1):124–137. doi:10.1053/j.ajkd.2019.04.031
11. Ross C, Makhzoum JP, Pagnoux C. Updates in ANCA-associated vasculitis. Eur J Rheumatol. 2022;9(3):153–166. doi:10.5152/eujrheum.2022.20248
12. Göçeroğlu A, Berden AE, Fiocco M, et al. ANCA-associated glomerulonephritis: risk factors for renal relapse. PLoS One. 2016;11(12):e0165402. doi:10.1371/journal.pone.0165402
13. Shiratori-Aso S, Nakazawa D. The involvement of NETs in ANCA-associated vasculitis. Front Immunol. 2023;14:1261151. doi:10.3389/fimmu.2023.1261151
14. Heras MH, Hernández RS, Fernández-Reyes MJ, Díez AI. Manejo de la hemorragia perioperatoria en el paciente renal [Management of perioperative bleeding in the renal patient]. Nefrologia. 2008;28(6):593–596.
15. Bando M, Homma S, Harigai M. MPO-ANCA positive interstitial pneumonia: current knowledge and future perspectives. Sarcoidosis Vasc Diffuse Lung Dis. 2022;38(4):e2021045. doi:10.36141/svdld.v38i4.11808
16. Yu R, Zhang L, Long T, et al. Case report: spontaneous renal hemorrhage in anti-neutrophil cytoplasmic antibody-associated vasculitis. Front Immunol. 2025;16:1544263. doi:10.3389/fimmu.2025.1544263
17. Tong J, Zhou ZY, Liu X, Wang DX, Deng W. Antineutrophil cytoplasmic antibody-associated vasculitis with alveolar hemorrhage and ruptured renal aneurysm: a case report and literature review. Medicine. 2022;101(1):e28543. doi:10.1097/MD.0000000000028543
18. Floege J, Jayne DRW, Sanders JF, et al. Executive summary of the KDIGO 2024 clinical practice guideline for the management of ANCA-associated vasculitis [published correction appears in Kidney Int. 2024 106(1):163-164]. Kidney Int. 2024;105(3):447–449. doi:10.1016/j.kint.2023.10.009
19. Chung SA, Langford CA, Maz M, et al. 2021 American College of Rheumatology/vasculitis foundation guideline for the management of antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Care Res. 2021;73(8):1088–1105. doi:10.1002/acr.24634
20. Aguirre-Valencia D, Posso-Osorio I, Bravo JC, Bonilla-Abadía F, Tobón GJ, Cañas CA. Sequential rituximab and omalizumab for the treatment of eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome). Clin Rheumatol. 2017;36(9):2159–2162. doi:10.1007/s10067-017-3780-9
21. Wechsler ME, Akuthota P, Jayne D, et al. Mepolizumab or Placebo for Eosinophilic Granulomatosis with Polyangiitis. N Engl J Med. 2017;376(20):1921–1932. doi:10.1056/NEJMoa1702079
22. Kawaguchi R, Usagawa H, Miyawaki Y, Oiwa H. A case of eosinophilic granulomatosis with polyangiitis associated with diffuse alveolar haemorrhage: a case report and case-based review. Mod Rheumatol Case Rep. 2024;8(2):398–403. doi:10.1093/mrcr/rxae019
23. Hellmich B, Sanchez-Alamo B, Schirmer JH, et al. EULAR recommendations for the management of ANCA-associated vasculitis: 2022 update. Ann Rheum Dis. 2024;83(1):30–47. doi:10.1136/ard-2022-223764
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.