Back to Journals » OncoTargets and Therapy » Volume 8
Enzalutamide for patients with metastatic castration-resistant prostate cancer
Authors Ramadan W, Kabbara W ![]() , Al Basiouni Al Masri H
, Al Basiouni Al Masri H
Received 7 January 2015
Accepted for publication 29 January 2015
Published 17 April 2015 Volume 2015:8 Pages 871—876
DOI https://doi.org/10.2147/OTT.S80488
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Daniele Santini
Wijdan H Ramadan,1 Wissam K Kabbara,1 Hiba S Al Basiouni Al Masri2
1Department of Pharmacy Practice, School of Pharmacy, Lebanese American University, Byblos, Lebanon; 2School of Pharmacy, Beirut Arab University, Beirut, Lebanon
Objective: To review and evaluate current literature on the US Food and Drug Administration (FDA)-approved drug enzalutamide (XTANDI®) in metastatic castration-resistant prostate cancer.
Data sources: Literature search was done through PubMed using the terms enzalutamide, MDV3100, abiraterone, and castration-resistant prostate cancer. Data from FDA product labels were also used.
Study selection and data extraction: Recent and relevant studies were included in the review. Collected clinical trials were screened and evaluated.
Data synthesis: Enzalutamide is an androgen receptor (AR) inhibitor with high selectivity and affinity to the AR. It was approved by the FDA to treat metastatic castration-resistant prostate cancer in patients previously treated with docetaxel, after a Phase III trial (AFFIRM) that showed a 4.8-month survival benefit in this population. Recently, the FDA expanded the approval of enzalutamide as first-line therapy for metastatic castration-resistant prostate cancer (mCRPC) who did not receive chemotherapy. Moreover, enzalutamide is shown to be associated with an acceptable safety profile.
Conclusion: Enzalutamide has been shown to be both safe and effective in improving overall survival in metastatic castration-resistant prostate cancer postchemotherapy with docetaxel and as a first line treatment before initiation of chemotherapy. However, additional studies and head-to-head trials are needed.
Keywords: enzalutamide, castration-resistant prostate cancer
Introduction
Prostate cancer is the second leading cause of male cancer-related death in the United States.1,2 In fact, the American Cancer Society’s estimates for prostate cancer in the USA for 2015 are about 220,800 new cases of prostate cancer and about 27,540 deaths from prostate cancer.2 During the early phase, prostate cancer is an androgen- or testosterone-dependent disease. Therefore, therapy aims at decreasing serum testosterone levels to castrate levels (≤0.5 ng/mL).1 This is called androgen deprivation therapy (ADT). However, sensitivity to ADT varies and ranges from few weeks to several years (median time: 18–30 months) before it becomes castration-resistant prostate cancer (CRPC).1 CRPC is a state wherein reactivation of the disease occurs despite reducing testosterone levels below castrate levels. This state is also known as the hormone-refractory or androgen-independent phase.3,4 One possible mechanism behind this form of resistance is ligand-independent activation of the androgen receptor (AR), caused by the oncogenes ERBB2 or HRAS. Another mechanism includes AR overexpression with a functional ligand-binding domain (LBD) that was shown to be both necessary and sufficient to switch to the hormone-refractory stage. In addition, DNA mutations to the AR gene affect the LBD, causing altered response of the AR to hormones other than testosterone, such as estrogen or hydrocortisone, as well as responding to AR antagonists such as bicalutamide.5
During this period, in which CRPC occurs in the absence of symptoms of metastases or minimal metastases, the current approved therapy includes sipuleucel-T immunotherapy.1 When the CRPC starts to spread and metastasize, docetaxel, a chemotherapeutic agent, is initiated in combination with prednisone.1 Second-line options are available in case of resistance to docetaxel or intolerability of side effects. The main options include cabazitaxel, which is an alternative chemotherapeutic agent used also in combination with prednisone; and abiraterone, which is an inhibitor of cytochrome P450 (CYP) 17, an enzyme required for the biosynthesis of testosterone.1 In addition, a new antiandrogen, enzalutamide, known as MDV3100 and marketed under the name of XTANDI® by Astellas Pharma Incorporation and Medivation Incorporation and manufactured by Catalent Pharma Solutions, was approved by the US Food and Drug Administration (FDA) on August 31, 2012 for the treatment of patients with metastatic castration-resistant prostate cancer (mCRPC) who have previously received docetaxel.6 On September 10, 2014, the FDA expanded the approval of enzalutamide as first-line therapy for mCRPC patients who did not receive chemotherapy.6 Therefore, this review was conducted in order to describe, enhance the understanding of, and evaluate both the efficacy and safety of the FDA-approved drug, enzalutamide.
Methods for selection of literature
Recent and relevant studies were included in the review. Collected clinical trials were screened and evaluated. PubMed (2005–2015) was searched for primary literature and review articles using the terms enzalutamide, MDV3100, abiraterone, and CRPC. The search was limited to human studies in the English language and included both safety and efficacy outcomes. All of the retrieved clinically relevant articles were used as references for this review manuscript. As for the clinical trials, only Phase II and Phase III randomized studies were selected. Data from FDA product labels were also used.
Mechanism of action
Enzalutamide is a second-generation competitive inhibitor of AR. It impairs the AR signaling pathway on three levels – through inhibition of androgen binding, nuclear translocation, and DNA binding – and thus induces apoptosis. Though it has a two to three fold lower affinity for the AR than dihydrotestosterone, it has an eight fold higher affinity for the receptor than the first-generation antiandrogen bicalutamide. Moreover, unlike bicalutamide, enzalutamide retains its pure antagonism in prostate cells overexpressing AR.7–9 Therefore, these unique properties in the pharmacology of enzalutamide make it an attractive option in mCRPC.
Pharmacokinetics
Important pharmacokinetic information of enzalutamide is shown in Table 1.7
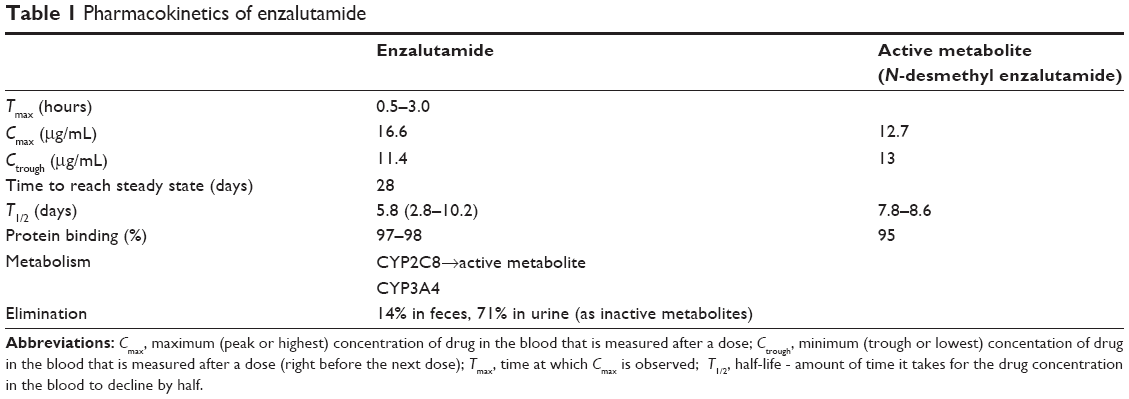 | Table 1 Pharmacokinetics of enzalutamide |
Renal impairment
In a study on 59 healthy males and 926 patients with mCRPC, 512 had normal renal function (creatinine clearance (CrCl): ≥90 mL/minute), 332 had mild renal impairment (CrCl: 60 mL/minute to <90 mL/minute), 88 had moderate renal impairment (CrCl: 30 mL/minute to <60 mL/minute), and 1 had severe renal impairment (CrCl: <30 mL/minute); the renal clearance of enzalutamide in patients with preexisting mild and moderate renal impairment (CrCl: 30 mL/minute to <90 mL/minute) was not different from that in patients with normal kidney function. However, because only one patient had preexisting severe renal failure, assessment of renal elimination cannot be done in this population and thus enzalutamide use is not recommended in this category.7
Hepatic impairment
The pharmacokinetics of enzalutamide and its active metabolite did not differ in mild (Child-Pugh A) to moderate (Child-Pugh B) liver diseases from normal liver function. Information for severe (Child-Pugh C) hepatic impairment is not available, thus enzalutamide use is not recommended in this category.7
Dosage and administration
Enzalutamide comes as 40 mg capsules. The daily dose is four capsules (160 mg) orally once daily with or without food and does not require coadministration of prednisone. If a patient develops toxicity or a side effect of grade 3 or higher, the drug should be stopped for 1 week or until symptoms improve (grade 2 or lower). The decision of whether to reinitiate enzalutamide at the original dose or at a decreased dose should be based on clinical judgment. In addition, given the strong interaction between enzalutamide and strong CYP2C8 inhibitors, the dose of enzalutamide should be reduced to 80 mg once daily when such coadministration cannot be avoided.7
Dosing in renal impairment
For CrCl ≥30 mL/minute, no dose adjustment is needed. For CrCl <30 mL/minute, use was not assessed.7
Dosing in hepatic impairment
For Child-Pugh classes A and B, no dose adjustment is needed. For Child-Pugh class C, use was not assessed.7
Clinical trials
The AFFIRM study (Safety and Efficacy Study of MDV3100 in Patients With Castration-Resistant Prostate Cancer Who Have Been Previously Treated With Docetaxel-Based Chemotherapy) was a Phase III randomized, double-blind, placebo-controlled, multicenter trial assessing the efficacy and safety of enzalutamide in patients with mCRPC who had previously received docetaxel. A total of 1,199 male patients were included in the study and 800 were randomized to receive 160 mg enzalutamide orally once daily and 399 received placebo. The primary end point was overall survival. During the study period, patients continued with their ADT and they were able to continue or start glucocorticoids. Patients were included in the study if they had a confirmed diagnosis of prostate cancer, castrate levels of testosterone <50 ng/dL, previous docetaxel use, and had disease progression. On the other hand, patients who had a history of, or were at increased risk of, seizure were excluded from the study.10 Table 2 indicates the overall survival of patients treated with enzalutamide versus placebo.7,10 In fact, enzalutamide provided a median 4.8-month improvement in overall survival, with a 37% reduction in risk of death. These positive results caused the Independent Data and Safety Monitoring Committee to recommend stopping the study and unblinding it and shifting those on placebo to the study drug if they were eligible. Furthermore, 54% of patients had more than a 50% decrease in their baseline prostate-specific antigen levels in the enzalutamide group versus only 2% in the placebo group (P-value <0.001). It also showed superiority in improving quality of life, with a quality-of-life response rate of 43% with enzalutamide versus 18% with placebo (P-value <0.001). Five patients (0.6%) in the enzalutamide group experienced seizures as opposed to none in the placebo group. In addition, adverse events of grade 3 or higher were lower in patients receiving enzalutamide than in those receiving placebo.10 This finding suggests that part of the adverse effects in the placebo group were actually symptoms of disease progression.11
 | Table 2 Overall survival of patients treated with enzalutamide versus placebo |
The Prevail Study is a double-blind, Phase III study where 1,717 patients were randomly assigned to receive either enzalutamide (at a dose of 160 mg) or placebo once daily. The primary end points were radiographic progression-free survival and overall survival. Secondary end points included the time until the initiation of cytotoxic chemotherapy, the time until the first skeletal-related event, the best overall soft-tissue response, the time until prostate-specific antigen progression and a decline in the prostate-specific antigen level of 50% or more from baseline. The study showed a benefit of the active treatment. The rate of radiographic progression-free survival at 12 months was 65% among patients treated with enzalutamide, as compared with 14% among patients receiving placebo (81% risk reduction; hazard ratio in the enzalutamide group, 0.19; 95% CI, 0.15 to 0.23; P<0.001). A total of 626 patients (72%) in the enzalutamide group, as compared with 532 patients (63%) in the placebo group, were alive at the data-cutoff date (29% reduction in the risk of death; hazard ratio, 0.71; 95% CI, 0.60 to 0.84; P<0.001). The benefit of enzalutamide was shown with respect to all secondary end points, including the time until the initiation of cytotoxic chemotherapy (hazard ratio, 0.35), the time until the first skeletal-related event (hazard ratio, 0.72), a complete or partial soft-tissue response (59% versus 5%), the time until prostate-specific antigen progression (hazard ratio, 0.17), and a rate of decline of at least 50% in prostate-specific antigen (78% versus 3%) (P<0.001 for all comparisons). Enzalutamide significantly decreased the risk of radiographic progression and death and delayed the initiation of chemotherapy in men with metastatic prostate cancer. 12 A similar trial for abiraterone has also shown positive results in the interim analysis. The COU-AA-302 trial was a randomized, controlled Phase III trial assessing the efficacy of abiraterone in patients with mCRPC who are naïve to chemotherapy. Considering that the end points of overall survival and radiographic progression-free survival favored abiraterone versus placebo, the study was unblinded and eligible patients were switched from placebo to abiraterone.13 Furthermore, one trial, the TERRAIN trial, is currently in the pipeline. It is a multinational, Phase II trial comparing enzalutamide with bicalutamide in men with early mCRPC. The study achieved its primary endpoint demonstrating a statistically significant increase in progression-free survival (PFS) for enzalutamide compared to bicalutamide (hazard ratio, 0.44; 95% CI, 0.34–0.57; P<0.0001). Median PFS was 15.7 months in the enzalutamide group compared to 5.8 months in the bicalutamide group. Grade 3 or higher adverse events were reported in 5.5% of enzalutamide-treated patients versus 2.1% of bicalutamide-treated patients. The results of this study showed that enzalutamide provides a longer duration of disease control in the studied patient population as compared to bicalutamide, but with a higher incidence of adverse effects.14
Contraindications/precautions/adverse events/drug interactions
Contraindications
Enzalutamide is contraindicated in pregnancy. However, this is not the patient population targeted with this therapy.7
Precaution
In the AFFIRM study, five patients out of 800 receiving enzalutamide (0.6%) experienced seizures and none in the placebo group. These patients had predisposing factors such as brain metastasis or brain atrophy or concomitant medications, such as haloperidol or lidocaine, which would decrease seizure threshold. In those experiencing seizures, the medication was discontinued and the seizures were self-resolved.10 In fact, enzalutamide-induced seizure is dose dependent and was seen at a starting dose of 360 mg/day and higher in the Phase I/II trials.8 One hypothesis on the mechanism by which enzalutamide decreases seizure threshold is by inhibiting the gamma aminobutyric acid-gated chloride channel.10 Because of the risk of seizure associated with enzalutamide use, caution should be taken in patients who have a history of seizure; patients with predisposing factors for seizure such as brain metastasis, stroke, and alcoholism; or patients using concomitant medications that may lower the seizure threshold. In addition, patients should be advised of the risk of engaging in any activity during which sudden loss of consciousness could cause serious harm to themselves or others.7
Adverse events
The most important adverse drug reactions that require monitoring are seizure, hot flashes, fatigue, diarrhea, and headache.7 The frequencies and severities are summarized in Table 3.7
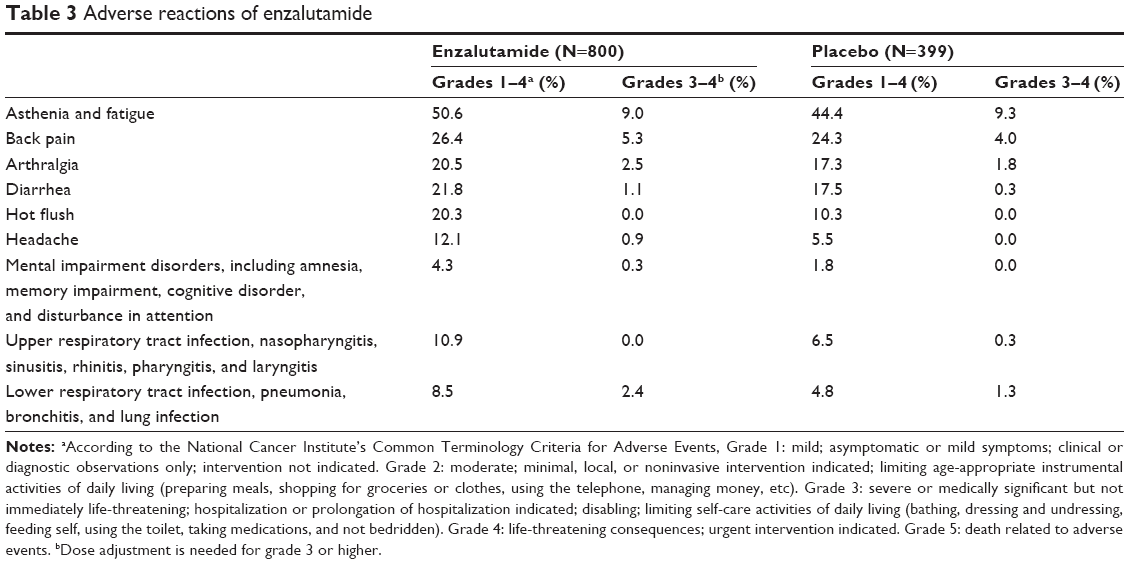 | Table 3 Adverse reactions of enzalutamide |
Drug interactions
Being metabolized by CYP2C8 and CYP3A4, coadministration of enzalutamide with strong inhibitors or inducers of these enzymes should be avoided. In addition, enzalutamide itself is a strong CYP3A4 inducer and a moderate CYP2C9 and CYP2C19 inducer; thus, combination with drugs metabolized by these enzymes should be also avoided, especially with substrates with narrow therapeutic index. Important drug interactions with XTANDI® are depicted in Table 4.7
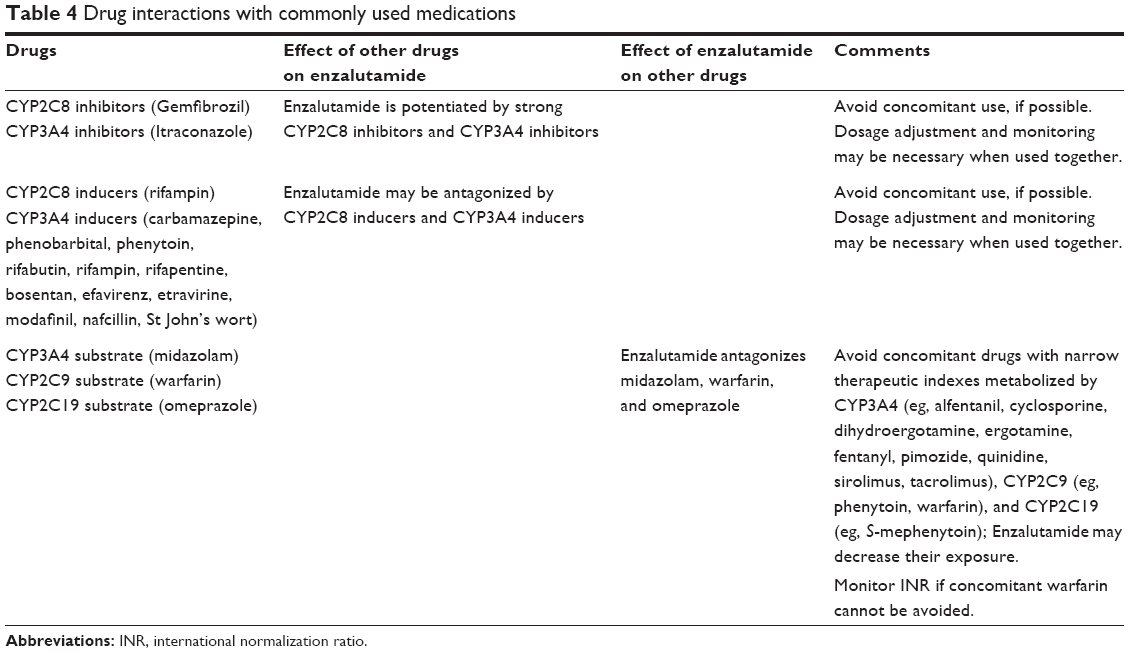 | Table 4 Drug interactions with commonly used medications |
Cost
Enzalutamide is more expensive than abiraterone; the expected wholesale acquisition cost is US$7,450 for a 30-day supply, whereas a month’s supply of abiraterone costs only $5,000.15,16 Thus, cost-effectiveness trials are further needed.
Formulary considerations
As mentioned previously, the AFFIRM trial has shown an additional survival benefit of 4.8 months with enzalutamide versus placebo. On the other hand, abiraterone increased overall survival by 4.6 months (hazard ratio, 0.74; P<0.0001) in a Phase III trial assessing its efficacy in patients with mCRPC who previously used docetaxel versus placebo.17 In addition, unlike enzalutamide, abiraterone is given with prednisone to reduce its mineralocorticoid side effect profile. This, however, leads to steroid-related side effects, such as hypokalemia (abiraterone 4.4% vs placebo 0.8%), hypertension (abiraterone 1.3% versus placebo 0.3%), and fluid retention.17 Another interesting point is that one hypothesis for resistance to abiraterone was activation of mutant AR by the glucocorticoids. This can be inhibited with enzalutamide; hence, further trials are needed to assess combining it with abiraterone therapy.18 Furthermore, both are oral medications, but enzalutamide is independent of food, whereas abiraterone has to be taken 2 hours before food or 1 hour after.7 Enzalutamide also has the ability to cross the blood–brain barrier, which although increasing the risk of seizure, makes it a suitable option when epidural or meningeal metastasis is present.11 The positive results of enzalutamide in the AFFIRM study support the notion that CRPC is not really androgen independent. In other words, tumor growth still depends on the AR signaling axis even after the tumor becomes castration resistant. The peculiar mode of action of enzalutamide on the three different levels (from ligand binding to signal transduction to DNA binding), its high affinity for the AR, its ability to retain its antagonism in cases of overexpression of AR, the significant increase in overall survival, the decrease in risk of death, and the improvement in quality of life have given enzalutamide a promising place in the therapy of prostate cancer.19,20
Moreover, the PREVAIL study showed that in men with minimally symptomatic or asymptomatic metastatic prostate cancer who had not received chemotherapy, enzalutamide significantly delayed radiographic disease progression or death, the need for cytotoxic chemotherapy, and the deterioration in quality of life and significantly improved overall survival.12
Conclusion
Currently, administration of enzalutamide (XTANDI®) is approved by the FDA in patients with metastatic castration-resistant prostate cancer (mCRPC) with previous use of docetaxel. It is so far the fourth drug approved for this indication after abiraterone, cabazitaxel, and sipuleucel-T.21,22 In September 2014, the FDA expanded the approval of enzalutamide as a first-line therapy for mCRPC. The new indication is for use in men with mCRPC who have not received chemotherapy. It follows a priority review of the supplemental new drug application that was based on results of the Phase III PREVAIL trial in men with mCRPC and no previous chemotherapy.6,12 Further trials comparing enzalutamide to abiraterone or cabazitaxel are needed.
Disclosure
The authors report no conflicts of interest in this work.
References
Oudard S. Progress in emerging therapies for advanced prostate cancer. Cancer Treat Rev. 2012;39:275–289. | ||
American Cancer Society: Cancer Facts and Figures 2015. Atlanta, Ga: American Cancer Society, 2015. http://www.cancer.gov/cancertopics/types/commoncancers. Accessed March 15, 2015. | ||
Scher HJ, Sawyers CL. Biology of progressive castration resistant prostate cancer: directed therapies targeting the androgen–receptor signaling axis. J Clin Oncol. 2005;23:8253–8261. | ||
Attard G, Richards J, de Bono JS. New strategies in metastatic prostate cancer: targeting the androgen receptor signaling pathway. Clin Cancer Res. 2011;17:1649–1657. | ||
Chen CD, Welsbie DS, Tran C, et al. Molecular determinants of resistance to antiandrogen therapy. Nat Med. 2004;10:33–39. | ||
US Food and Drug Administration. FDA Approves New Treatment for a Type of Late Stage Prostate Cancer; 2014. Available from: http://www.medscape.com/viewarticle/831548. Accessed January 5, 2015. | ||
Xtandi. FDA Label for Enzalutamide – August 2012; 2012. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/203415lbl.pdf. Accessed November 10, 2014. | ||
Scher HI, Beer TM, Higano CS, et al; Prostate Cancer Foundation/Department of Defense Prostate Cancer Clinical Trials Consortium. Antitumor activity of MDV3100 in castration-resistant prostate cancer: a phase 1–2 study. Lancet. 2010;375:1437–1446. | ||
Tran C, Ouk S, Clegg NJ, et al. Development of a second generation antiandrogen for the treatment of advanced prostate cancer. Science. 2009;324:787–790. | ||
Scher HI, Fizazi K, Saad F, et al. Increased survival with enzalutamide in prostate cancer after chemotherapy (the AFFIRM trial). N Eng J Med. 2012;367(13):1187–1197. | ||
Vogelzang NJ. Enzalutamide – a major advance in the treatment of metastatic prostate cancer. N Eng J Med. 2012;367(13):1256–1257. | ||
Beer TM, Armstrong AJ, Rathkopf DE, et al. Enzalutamide in Metastatic Prostate Cancer before Chemotherapy (the PREVAIL trial). N Engl J Med. 2014;371:424–433. | ||
Ryan CJ, Smith MR, De Bono JS, et al. Interim analysis (IA) results of COU-AA-302, a randomized, phase III study of abiraterone acetate (AA) in chemotherapy-naive patients (pts) with metastatic castration-resistant prostate cancer (mCRPC). J Clin Oncol. 2012;30(suppl):abstrLBA4518. | ||
Clinical trials. A Study of MDV3100 Versus Bicalutamide in Castrate Men with Metastatic Prostate Cancer (TERRAIN); 2014. Available from: http://clinicaltrials.gov/ct2/show/NCT01288911?term=MDV3100&rank=13. Accessed March 15, 2015. | ||
Pollack A. New Drug for Prostate Cancer Gets FDA Nod. New York: The New York Times; 2012. | ||
Maverick NY. Abiraterone now Approved as Zytiga by the FDA for Castrate Resistant Prostate Cancer: Pharma Strategy Blog; 2011. Available from: http://pharmastrategyblog.com/2011/04/abiraterone-now-approved-as-zytiga-by-the-fda-in-castrate-resistant-prostate-cancer.html/. Accessed November 10, 2014. | ||
Fizazi K, Scher HI, Molina A, et al. Final overall survival (OS) analysis of COU-AA-301, a phase 3 study of abiraterone acetate plus prednisone in patients with metastatic castration-resistant prostate cancer (mCRPC) pretreated with docetaxel. Eur J Cancer. 2011;47:S483–S484. [abstract 7000]. | ||
Richards J, Lim AC, Hay CW, et al. Interactions of abiraterone, eplerenone and prednisolone with wild type and mutant androgen receptor: a rationale for increasing abiraterone exposure or combining with MDV3100. Cancer Res. 2012;72:2176–2182. | ||
Holzbeierlein J, Lal P, Latulippe E, et al. Gene expression analysis of human prostate carcinoma during hormonal therapy identifies androgen responsive genes and mechanism of therapy resistance. Am J Pathol. 2004;164:217–227. | ||
Donkena KV, Yuan H, Young CY. Recent advances in understanding hormonal therapy resistant prostate cancer. Curr Cancer Drug Targets. 2010;10:402–410. | ||
Choudhury AD, Kantoff PW. New agents in metastatic prostate cancer. J Natl Compr Canc Netw. 2012;10:1403–1409. | ||
American Association for Cancer Research. Enzalutamide shows efficacy in advanced prostate cancer. Cancer Discovery. 2012;2:OF5. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.