")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Environmental Contamination of SARS-CoV-2 Delta VOC by COVID-19 Patients Staying in the Hospital for More Than Two Weeks
Authors Ge J, Zhang C, Peng Z , Chu M, Chen W, Li Z, Liu S, Yang Y, Chu M
Received 6 April 2023
Accepted for publication 4 October 2023
Published 17 October 2023 Volume 2023:16 Pages 2163—2170
DOI https://doi.org/10.2147/RMHP.S413639
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Jingwu Ge,1,* Chuanmeng Zhang,2,* Zhihang Peng,3 Minjuan Chu,4 Wensen Chen,1 Zhanjie Li,1 Shuangyuan Liu,1 Yongfeng Yang,5 Ming Chu6
1Department of Infection Management, The First Affiliated Hospital of Nanjing Medical University, Nanjing, 210009, People’s Republic of China; 2The Center for Translational Medicine, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou, 225300, People’s Republic of China; 3Department of Epidemiology and Biostatistics, School of Public Health, Nanjing Medical University, Nanjing, Jiangsu, 211166, People’s Republic of China; 4Department of Critical Care Medicine, The First Affiliated Hospital of Nanjing Medical University, Nanjing, 210009, People’s Republic of China; 5Center of Infectious Diseases, Affiliated Nanjing Hospital of Nanjing University of Chinese Medicine (The No. 2 Hospital of Nanjing), Nanjing, 211113, People’s Republic of China; 6Department of Infection Management, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou, 225300, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ming Chu, Department of Infection Management, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou, 225300, People’s Republic of China, Email [email protected]
Background: Patients infected with SARS-CoV-2 Delta VOC have a longer course of disease. We detected the air, surfaces, and patient’s personal items in the wards of the second hospital of Nanjing during the outbreak of the COVID-19 Delta Variant to identify the environmental contamination, which provides a theoretical basis for the prevention and control of COVID-19 variation beads in the future.
Methods: In the cross-sectional study, we collected and analyzed clinical features, demographic and epidemiological data, laboratory and swab test results, and surface and air samples of 144 COVID-19 cases.
Results: The time from symptom onset to surface sampling was 25 days (IQR, 21 to 33 days). Positive throat swabs were detected in 52(36.1%) patients, of which only 8(5.6%) patients had N or ORF1a/b genes Ct value < 35 on the surface sampling day. Among the 692 environmental surface and air specimens collected from 144 COVID-19 cases, 3 specimens (3/692, 0.4%) related to 5 cases (3.5%, 5/144) were detected positive on RT-PCR. Overall, bedside tables (2/144, 1.4%) were most likely to be contaminated, followed by toilet seats (1/81, 1.2%).
Conclusion: The environmental contamination by SARS-CoV-2 Delta VOC-infected cases with disease duration of more than two weeks is limited.
Keywords: COVID-19, delta VOC, environmental contamination, SARS-CoV-2
Introduction
Severe acute respiratory syndrome type 2 coronavirus (SARS-CoV-2) has caused a serious global pandemic and brought major public health problems.1,2 Multi-national government has taken a variety of measures to fight against COVID-19, such as converting large public utility spaces into makeshift healthcare centers, increase in-hospital COVID-19 beds and ICU capacities and so on.3 The virus has undergone several mutations that will promote the evolution of the virus, which may affect the transmission and pathogenicity of the virus, as well as immune escape and resistance to therapeutic drugs.1
Since the Delta variant strain of SARS-CoV-2 was first detected in India in October 2020, it had been identified as the variant of concern (VOC) by the World Health Organization (WHO) and affected more than 80 countries.4 Since Delta VOC is more virulent, the patients infected have about twice the risk of hospital admission compared with those infected with Alpha VOC.5 The Delta VOC also shows a prolonged viral shedding, compared with the wild-type.6
SARS-CoV-2 is transmitted via respiratory droplets,7 close contact,8 and touching the contaminated object surface.9 Studies have shown that SARS-CoV-2 is widely distributed in the air and on object surfaces in the hospital.10,11 Positive specimens in the environment may appear on almost all the frequently touched surfaces in the isolation ward,12 included mobile phones,13 shelves in the toilet,13 bedside handrails,14 bedside tables, pillows, bed sheets, air exhaust outlets,15 and even the shoes.16 However, one study has indicated that the SARS-CoV-2 contamination on environmental surfaces in the hospital is limited, although it may persist for a longer time on surfaces under controlled laboratory conditions.17 Another study also indicates that the rate of environmental contamination by COVID-19 patient with prolonged viral carriage is low.18
Patients infected with Delta VOC have a longer course of disease. To the best of our knowledge, few studies have focused on the environmental contamination associated with Delta VOC-infected patients with the duration of more than two weeks. On 30 July, one official of Nanjing Center for Disease Control and Prevention reported the results of virus gene sequencing in 52 related cases in the outbreak of the COVID-19.19 The virus genome sequences were highly homologous, which indicates the same transmission chain. The early cases (Lukou international airport cleaners) have been confirmed to share the same RNA sequence as the Delta VOC, which was consistent with the genetic sequence of one imported patient on Flight CA910 from Russia on 10 July 2021.
Therefore, we detected the contamination of air, surfaces, and patient’s personal items in the isolation wards among patients with Delta VOC infection with duration of more than two weeks in Nanjing. In addition, the study of environmental contamination of SARS-CoV-2 Delta VOC is of great significance to guide the prevention of COVID-19 infected by other mutants in the future, because there is no difference in there pollution to the environment.20 Moreover, hospital risk control needs to have a better understanding of different modes of transmission.
Methods
Study Design and Setting
This study was conducted in four non-negative pressure general wards randomly selected from The Second Hospital of Nanjing. Biological, environmental samples from COVID-19 patients with duration of more than two weeks were collected (Figure 1). On August 21, 23, 27 and 30, 2021, the environmental samples were collected from four wards (Ward A, B, C, and D), where 144 COVID-19 cases were hospitalized in the 81 rooms, including 22 single-bed rooms, 55 two-bed rooms, and 4 three-bed rooms. General environmental sampling was performed in Ward A, B and C, including the patients’ rooms and public areas, while enhanced environmental sampling was conducted in Ward D, with additional sampling of air, personal items, masks (inside and outside) apart from the general sampling.
 |
Figure 1 Flowchart of selecting study cases. |
Demographic and Epidemiological Data
The patients’ epidemiological data were collected, including basic demographic information (such as age, gender, marital status, place of residence, education background), date of symptom onset, severity of disease, first symptoms (such as fever, dry cough, expectoration, fatigue, myalgia, diarrhea), and date of environmental sample collection.
Sample Collection
The corridors and nurse station of the ward were cleaned and disinfected twice daily by nurses. The floor of the corridors and nurse station was disinfected with 1000 mg/liter chlorine solution and cleaned with the mop. The other surfaces were wiped with chlorine-containing disinfectant wipes. The inside and outside of the garbage bin and the contents inside the bin were disinfected with 2000 mg/liter chlorine solution before garbage collection. The surfaces and floors in the patient’s rooms, including the toilet bowls, were also disinfected. The air of wards (including the corridors, patient’s rooms, and nurse station) was disinfected with UV lamps twice a day for 1 hour each time.
Throat swabs were collected from the patients in the morning. The environmental samples were collected from bedside tables, bedrails, garbage bins (both bedside and toilet), and toilet seats before the first cleaning of the day. In ward D, samples from patient’s personal items, including masks (both inside and outside) and mobile phones, were collected. Samples from public area were collected from garbage bins, mobile treatment carts, armrests and electrocardiographs in the corridor, mobile phones of physicians and nurses, keyboards, mice, telephones, and desktop in the nurse station. For larger surfaces such as the bedside table, samples were collected from a minimum area of 100 cm2, and for smaller surfaces, such as mobile phones, samples should be collected in an area as large as possible. All samples were collected using sterile swabs (Yocon, Beijing, China) and kept in virus preservation solution (Yocon, Beijing, China).
We sampled the air in Ward D (8 rooms) where stayed 15 cases with positive throat swab on August 22 before disinfection using the Aerosol Particle Liquid Concentrator (model WA-400II, Beijing Dingblue Technology Co., Ltd.) at 400 L/min for 20 minutes. Each air sample was collected and stored in 3 mL of the virus sampling liquid as previously mentioned.21,22
Viral RNA Detection by Reverse Transcription-Polymerase Chain Reaction (RT-PCR)
The samples were stored in virus medium. Viral RNA was extracted within 2 hours of collection using the Nucleic Acid Isolation Kit (Jiangsu Bioperfectus Technologies Co., Ltd, China) according to the manufacturer’s instructions. RT-PCR was conducted with primers and probes targeting at the N, ORF1a/b genes and a positive reference gene by using the RNA Detection Kit for SARS-CoV-2 (Jiangsu Bioperfectus Technologies Co., Ltd, China).6 The reaction system and amplification conditions followed the manufacturer’s specification (Bioperfectus Technologies Co., Ltd). The detection limit of cycle threshold (Ct) was set to be 40 (500 copies/mL). Samples were considered positive when N or ORF1a/b genes were detected with Ct values ≤40. All tests were performed under strict biosafety conditions following the standard operating procedures.
Statistical Analyses
All participants were divided into the positive and negative groups based on the environmental surface sampling results. Categorical variables were expressed as numbers and percentages. Continuous variables were presented as medians and interquartile ranges (IQRs). SPSS software version 26.0 (IBM Co. LTD, Chicago, IL, USA) was used for all statistical analyses.
Ethics Statement
Our study protocol was approved by the Ethics Committee of The Second Hospital of Nanjing (2021-ls-ky030). In addition, we confirm that this study was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from the patients before the questionnaire survey. Personal information was not involved in this study.
Results
Baseline Characteristics
Table 1 shows the characteristics of 144 COVID-19 cases. Among these patients, 69 (47.9%) were male; 22 (15.3%) were under the age of 18 years, 100 (69.4%) were aged 18–59 years, and 22 (15.3%) were aged 60 years and greater; 80 (55.6%) lived in the city, while 64(44.4%) lived in the countryside; 100(69.4%) cases had a high school or lower educational background; 52(36.1%) received 2 doses of vaccination, 34(23.6%) received 1 dose, and 58 (40.3%) were unvaccinated. In terms of clinical severity, 30 (20.8%) were mild, 114 (79.2%) were moderate, and all were cured and discharged. The common symptoms at onset were cough (including dry cough) (81, 56.3%), fever (57, 39.6%), throat discomfort (24, 16.7%), fatigue (19, 13.2%), hyposmia (4, 2.8%), and CT lung abnormalities 114(79.2%). The lowest PCR Ct value on gene N was 22 (IQR, 18 to 25.8), and lowest PCR Ct value on gene ORF1a/b was 23.5 (IQR, 19 to 28).
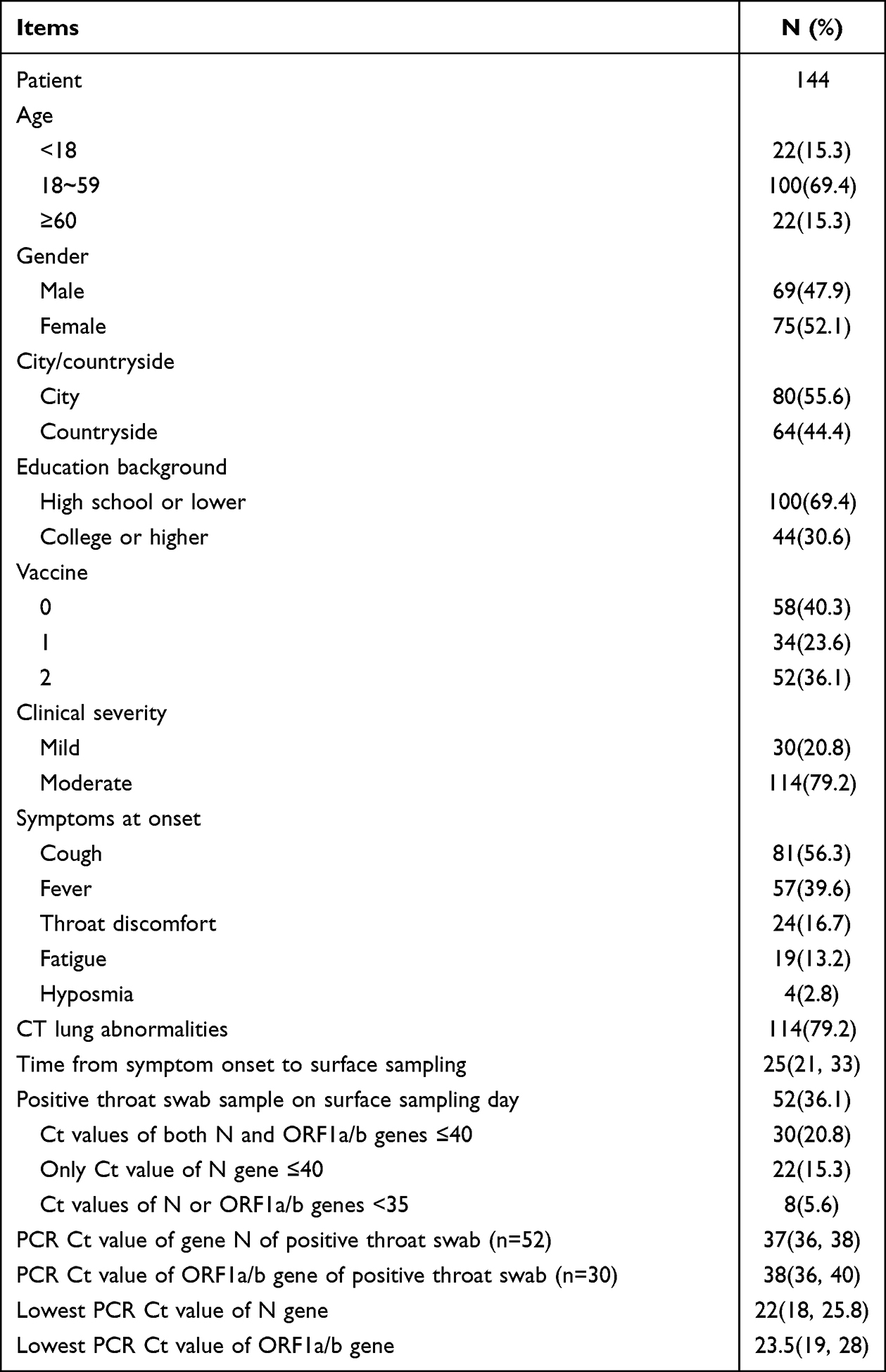 |
Table 1 Baseline Characteristics of 144 COVID-19 Cases |
The time from symptom onset to surface sampling was 25 days (IQR, 21 to 33 days). Positive throat swabs were detected in 52(36.1%) patients, of which 30 (20.8%) had both N and ORF1a/b genes Ct value ≤40, and 22(15.3%) had only N genes Ct value ≤40. PCR Ct value on gene N was 37 (IQR, 36 to 38), and PCR Ct value on gene ORF1a/b was 38 (IQR, 36 to 40). Only 8(5.6%) patients had N or ORF1a/b genes Ct value <35.
Environmental Samples
A total of 692 environmental surfaces and air specimens were collected among 144 COVID-19 cases, and 3 specimens (3/692, 0.4%) related to 5 cases (3.5%, 5/144) were detected positive on RT-PCR (Table 2). Overall, bedside tables (2/144, 1.4%) were most likely to be contaminated, followed by toilet seats (1/81, 1.2%). By contrast, specimens from the garbage bins (at bedside and in the toilet), masks (both inside and outside), the patients’ mobile phones, public areas (including the corridor and nurse stations) were all tested negative on RT-PCR. All air samples (from bedside and toilet) were negative in patients’ rooms (Table 3).
 |
Table 2 Information of 3 Positive Environmental Specimens Related to 5 COVID-19 Cases |
 |
Table 3 Distribution of Environmental Specimens of 144 COVID-19 Cases |
Discussion
In the present study, we assessed the environmental contamination of SARS-CoV-2 among 692 environmental surfaces, personal items, and air specimens related to 144 Delta VOC-infected cases with duration of more than two weeks in a hospital. Our study evidenced that the SARS-CoV-2 Delta VOC contamination on object surfaces or in the air might be limited, though a small number of positive samples were found from bedside tables and toilets. All personal item and air specimens were negative.
Delta VOC was the culprit of the infection among all these patients. Our study showed that the median lowest Ct value of throat swabs was 22 (gene N), indicating a high viral load. Previous studies suggested that the viral load of Delta VOC was about 1000 times higher than the wild-type strain, with a prolonged shedding time.6 Another study showed that compared with the wild-type, the Delta VOC was associated with a longer duration of Ct value ≤30 (median duration 18 days for Delta VOC, and 13 days for wild-type).8
Our study showed that in the hospital, the contamination of SARS-CoV-2 Delta VOC from COVID-19 patients with duration of more than two weeks was limited, which may be explained by the following factors. First, in the later stages of COVID-19, the patients release fewer viruses through the respiratory tract. Previous studies showed that the virus was readily isolated during the first week of symptom onset, and no isolates were obtained from the samples on day 8 despite a persistent high viral load.23 The evidence suggests that the viral load of SARS-CoV-2 from upper respiratory tract samples peaks around the time of symptom onset or a few days after and would not be detectable within about two weeks24 One study showed that patients with Ct value (gene E) above 33–34 were not contagious.25 Our data demonstrated that the positive rate of pharyngeal swabs on the environmental sampling day was 36.1% (52/144), the median Ct value was 37 (IQR, 36 to 38) and the time from symptom onset to surface sampling was 25 days (IQR, 21 to 33 days). Second, the floor, surfaces, and the air were disinfected twice a day, which possibly played an important role. Third, the sampling was performed in early morning. In the wards, there was no treatment or care and patients were all asleep at night, which may reduce the possibility of environmental contamination.
Our study found that the Delta VOC was detected positive on bedside tables and toilet seats, which is consistent with some previous reports.21,26,27 A previous study showed a longer duration of virus in fecal samples than in the respiratory samples.28 That means that SARS-CoV-2 could be released through the stool despite the negative result of the throat swab. We also found that samples from the garbage bins (at bedside and in the toilet) and the air were all negative. According to one study22 the air samples from non-negative pressure general wards of four hospitals were detected positive (3 of 44, 6.8%). Surprisingly, another study discovered that all the air samples from negative-pressure wards were negative.18 Our study found that the air samples were negative, which was likely due to the prolonged course and the regular disinfection. While there was debate about the presence of SARS-CoV-2 in the air, some experts believe there was consistent, strong evidence that SARS-CoV-2 spreads by airborne transmission.29 Samples from masks (inside and outside) were detected negative. One study showed a 41.9% positivity rate of SARS-CoV-2 from the mask samples collected within 36 hours of their confirmed diagnosis.30 However, our mask sampling is more than two weeks after diagnosis.
This study has some limitations. First, we only tested viral nucleic acid and did not perform viral culture to demonstrate the viability. Second, only the general wards hospitalized with mild or moderate COVID-19 cases were detected. Third, we did not test the environmental samples at the early stage of admission. Despite these limitations, we believe that our findings can be applied in clinical practice to prevent and control the spread of SARS-CoV-2.
Conclusion
Our study revealed that the environmental contamination of SARS-CoV-2 Delta VOC-infected cases with duration of more than two weeks may be limited, which may be similar to that of the current Omicron. Hopefully, our findings can provide guidance on infection control for both COVID-19 patients and healthcare workers.
Acknowledgments
We thank KEY Translation Studio (Nanjing, China) for the critical revision of the English language and grammar in this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Taizhou Clinical Medical School of Nanjing Medical University (Taizhou People’s Hospital) (TZKY20220305) and Taizhou People’s Hospital Medical Innovation Team Foundation (CXTDA201901).
Disclosure
All the authors declared no conflicts of interest.
References
1. Shehata AA, Parvin R, Nagy A, et al. An overview of ongoing challenges in SARS-CoV-2 global control. Ger J Microbiol. 2021;1(2):1–18. doi:10.51585/gjm.2021.2.0006
2. Shehata AA, Attia YA, Rahman MT, et al. Diversity of coronaviruses with particular attention to the interspecies transmission of SARS-CoV-2. Animals. 2022;12(3):378. doi:10.3390/ani12030378
3. Umakanthan S, Bukelo MM, Gajula SS. The Commonwealth Caribbean COVID-19: regions resilient pathway during pandemic. Front Public Health. 2022;10:844333. doi:10.3389/fpubh.2022.844333
4. Liang Q, Sun C, Liu H, et al. Vaccination remains the first choice to control the spread of delta and other variants of severe acute respiratory coronavirus virus 2 (SARS-CoV-2). Infect Control Hosp Epidemiol. 2022;43(11):1749–1750. doi:10.1017/ice.2021.364
5. Sheikh A, Mcmenamin J, Taylor B, Robertson C. SARS-CoV-2 Delta VOC in Scotland: demographics, risk of hospital admission, and vaccine effectiveness. Lancet. 2021;397(10293):2461–2462. doi:10.1016/S0140-6736(21)01358-1
6. Wang Y, Chen R, Hu F, et al. Transmission, viral kinetics and clinical characteristics of the emergent SARS-CoV-2 Delta VOC in Guangzhou, China. EClinicalMedicine. 2021;40:101129. doi:10.1016/j.eclinm.2021.101129
7. Umakanthan S, Sahu P, Ranade AV, et al. Origin, transmission. diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad Med J. 2020;96(1142):753–758. doi:10.1136/postgradmedj-2020-138234
8. Chu DK, Akl EA, Duda S, Solo K, Yaacoub S, Schunemann HJ. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. 2020;395(10242):1973–1987. doi:10.1016/S0140-6736(20)31142-9
9. Karia R, Gupta I, Khandait H, Yadav A, Yadav A. COVID-19 and its modes of transmission. SN Compr Clin Med. 2020;2:1798–1801.
10. Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and surface distribution of severe acute respiratory syndrome Coronavirus 2 in Hospital Wards, Wuhan, China, 2020. Emerg Infect Dis. 2020;26(7):1583–1591. doi:10.3201/eid2607.200885
11. Geng Y, Wang Y. Stability and transmissibility of SARS-CoV-2 in the environment. J Med Virol. 2023;95(1):e28103. doi:10.1002/jmv.28103
12. Nagle S, Tandjaoui-Lambiotte Y, Boubaya M, et al. Environmental SARS-CoV-2 contamination in hospital rooms of patients with acute COVID-19. J Hosp Infect. 2022;126:116–122. doi:10.1016/j.jhin.2022.05.003
13. Wee LE, Arora S, Ko KK-K. Environmental contamination and evaluation of healthcare-associated SARS-CoV-2 transmission risk in temporary isolation wards during the COVID-19 pandemic. Am J Infect Control. 2023;51(4):413–419. doi:10.1016/j.ajic.2022.09.004
14. Huang Y, Ding Z, Chen Q, et al. Environmental virus detection associated with asymptomatic SARS-CoV-2-infected individuals with positive anal swabs. Sci Total Environ. 2021;753:142289. doi:10.1016/j.scitotenv.2020.142289
15. Wei L, Huang W, Lu X, et al. Contamination of SARS-CoV-2 in patient surroundings and on personal protective equipment in a non-ICU isolation ward for COVID-19 patients with prolonged PCR positive status. Antimicrob Resist Infect Control. 2020;9(1):167. doi:10.1186/s13756-020-00839-x
16. Ong S, Tan YK, Chia PY, et al. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA. 2020;323(16):1610–1612. doi:10.1001/jama.2020.3227
17. D’Accolti M, Soffritti I, Passaro A, et al. SARS-CoV-2 RNA contamination on surfaces of a COVID-19 ward in a hospital of Northern Italy: what risk of transmission? Eur Rev Med Pharmacol Sci. 2020;24(17):9202–9207. doi:10.26355/eurrev_202009_22872
18. Wei L, Lin J, Duan X, et al. Asymptomatic COVID-19 patients can contaminate their surroundings: an environment sampling study. Msphere. 2020;5(3). doi:10.1128/mSphere.00442-20
19. Liu Y, Yang B, Liu L, Jilili M, Yang A. Occupational characteristics in the outbreak of the covid-19 delta variant in Nanjing, China: rethinking the occupational health and safety vulnerability of essential workers. Int J Environ Res Public Health. 2021;18(20):10734.
20. Glinert I, Ben-Shmuel A, Szwartcwort-Cohen M, et al. Revisiting SARS-CoV-2 environmental contamination by patients with COVID-19: the Omicron variant does not differ from previous strains. Int J Infect Dis. 2022;118:211–213. doi:10.1016/j.ijid.2022.03.001
21. Chu M, Chu M, Mao Y, et al. Environmental sampling of the severe acute respiratory syndrome coronavirus 2 Delta variant in the inpatient wards of a hospital in Nanjing. Ann Transl Med. 2021;9(23):1712. doi:10.21037/atm-21-5147
22. Zhou L, Yao M, Zhang X, et al. Breath-, air- and surface-borne SARS-CoV-2 in hospitals. J Aerosol Sci. 2021;152:105693. doi:10.1016/j.jaerosci.2020.105693
23. Wolfel R, Corman VM, Guggemos W, et al. Virological assessment of hospitalized patients with COVID-2019. Nature. 2020;581(7809):465–469. doi:10.1038/s41586-020-2196-x
24. Walsh KA, Jordan K, Clyne B, et al. SARS-CoV-2 detection, viral load and infectivity over the course of an infection. J Infect. 2020;81(3):357–371. doi:10.1016/j.jinf.2020.06.067
25. La Scola B, Le Bideau M, Andreani J, et al. Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards. Eur J Clin Microbiol Infect Dis. 2020;39(6):1059–1061. doi:10.1007/s10096-020-03913-9
26. Liu J, Liu J, He Z, et al. Duration of SARS-CoV-2 positive in quarantine room environments: a perspective analysis. Int J Infect Dis. 2021;105:68–74. doi:10.1016/j.ijid.2021.02.025
27. Luo L, Liu D, Zhang H, et al. Air and surface contamination in non-health care settings among 641 environmental specimens of 39 COVID-19 cases. PLoS Negl Trop Dis. 2020;14(10):e8570. doi:10.1371/journal.pntd.0008570
28. Wu Y, Guo C, Tang L, et al. Prolonged presence of SARS-CoV-2 viral RNA in faecal samples. Lancet Gastroenterol Hepatol. 2020;5(5):434–435. doi:10.1016/S2468-1253(20)30083-2
29. Greenhalgh T, Jimenez JL, Prather KA, Tufekci Z, Fisman D, Schooley R. Ten scientific reasons in support of airborne transmission of SARS-CoV-2. Lancet. 2021;397(10285):1603–1605. doi:10.1016/S0140-6736(21)00869-2
30. Sriraman K, Shaikh A, Parikh S, et al. Non-invasive adapted N-95 mask sampling captures variation in viral particles expelled by COVID-19 patients: implications in understanding SARS-CoV2 transmission. PLoS One. 2021;16(4):e249525. doi:10.1371/journal.pone.0249525
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.