Back to Journals » Advances in Medical Education and Practice » Volume 17
Enrollment Problems and Training Models for Training Postgraduate Students in Clinical Laboratory Diagnosis (Professional Degree) During the “Four Certificates in One” Era in China
Authors Yan Z ![]() , Fu Y, Cui Y, Kuang L, Shi H, Liu T, Liu X, Jiang Y
, Fu Y, Cui Y, Kuang L, Shi H, Liu T, Liu X, Jiang Y
Received 17 November 2025
Accepted for publication 19 February 2026
Published 25 February 2026 Volume 2026:17 582154
DOI https://doi.org/10.2147/AMEP.S582154
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Ziyi Yan,1,2 Yunhan Fu,1,3 Yali Cui,1,4,5 Linghan Kuang,1,6 Hua Shi,1 Ting Liu,1 Xingxin Liu,1 Yongmei Jiang1,2
1Department of Laboratory Medicine, West China Second University Hospital, Sichuan University, Chengdu, People’s Republic of China; 2Key Laboratory of Birth Defects and Related Diseases of Women and Children (Sichuan University), Ministry of Education, Chengdu, People’s Republic of China; 3West China School of Medicine, Sichuan University, Chengdu, People’s Republic of China; 4Department of Laboratory Medicine, Sichuan Provincial Children’s Hospital, Meishan, People’s Republic of China; 5Department of Laboratory Medicine, Meishan Women and Children’s Hospital, Meishan, People’s Republic of China; 6Department of Laboratory Medicine, Chengdu Hi-Tech Zone Hospital for Women and Children (Chengdu Hi-Tech Zone Hospital for Maternal and Child Healthcare), Chengdu, People’s Republic of China
Correspondence: Ziyi Yan, Department of Laboratory Medicine, West China Second University Hospital, Sichuan University, No. 20, Section 3, South Renmin Road, Chengdu, Sichuan, People’s Republic of China, Email [email protected] Yongmei Jiang, Department of Laboratory Medicine, West China Second University Hospital, Sichuan University, No. 20, Section 3, South Renmin Road, Chengdu, Sichuan, People’s Republic of China, Email [email protected]
Abstract: Postgraduate training in clinical laboratory diagnostics (professional degree) in China operates under a “four certificates in one” framework tightly coupled with standardized residency training. However, a structural recruitment–training mismatch has emerged: eligible applicants increasingly come from clinical medicine undergraduate programs with limited early exposure to laboratory medicine governance, quality systems, and post-analytical assurance, contributing to persistent under-enrollment and heterogeneous training experiences across schools. Using a strengths–weaknesses–opportunities–threats (SWOT) framework, this review synthesized objective enrollment signals and analyzed how policy constraints, competency gaps, and evolving service expectations jointly shape training feasibility. We also examined recent “laboratory physician training” pilot/experimental classes that front-load laboratory exposure and improve pathway continuity and translated these pilots into a rotation-wide competency framework with corresponding teaching activities and workplace-based assessment tools to support implementation across varied settings. Because these pilots are recent and outcome data remains limited, the implications are primarily policy- and design-based. Overall, this review contributes an actionable competency-alignment perspective for medical education and training reform, highlighting early exposure, structured reskilling/upskilling in quality management, interpretive reporting and clinical communication, and context-sensitive incorporation of digital/AI-enabled workflows where available.
Keywords: medical education, Chinese medical education, clinical laboratory, professional degree, laboratory physicians, SWOT, China
Since the 1980s, China’s laboratory medicine discipline has expanded rapidly alongside economic development and advances in clinical laboratory technology, and postgraduate education in clinical laboratory diagnostics was established by 1986.1 Subsequent higher-education reforms and the differentiation of professional versus academic degrees reshaped training pathways, while laboratory medicine and medical technology evolved with increasing separation from clinical medicine, creating gaps between university training structures and service needs.
In the current “four certificates in one” training environment, professional master’s programs in clinical laboratory diagnostics are expected to prepare laboratory physicians who can support clinical decision-making. However, their implementation is constrained by a recruitment–training misalignment: the eligible recruitment pool increasingly consists of clinical medicine undergraduates who often enter with limited systematic exposure to laboratory medicine competencies and workflows. This mismatch elevates the onboarding cost during rotations and contributes to persistent enrollment difficulty and heterogeneous training experiences across schools.
Existing discussions frequently describe policy evolution or rotation arrangements but less often connect enrollment dynamics to competency-oriented training design in an actionable way. There is a need for an integrative analysis that explains why recruitment challenges persist and translates that diagnosis into feasible alignment mechanisms for training reform.
Therefore, the objective of this review is to apply a strengths–weaknesses–opportunities–threats (SWOT) framework to (i) synthesize the key drivers of enrollment difficulties and training misalignment in China’s professional master’s programs in clinical laboratory diagnostics and (ii) derive practical implications for training reform, including pilot pathway design and competency-oriented implementation in rotation-based settings.
Master’s Degree Training in Clinical Laboratory Diagnostics in the Four Certificates in One Era
The 2012 Reform of Undergraduate Majors in Chinese Universities and Colleges, Including the Five-to-Four Reform in the Medical Laboratory System
In the “Undergraduate Program Catalog for Regular Higher Education Institutions”2 issued by the Ministry of Education in 1998, clinical medicine and medical technology were presented as belonging to the same first-level discipline in the medical discipline category (code 10), namely, the “clinical medicine and medical technology class” (code 1003). At this stage, the medical laboratory (100304) major, which was a second-level discipline under the first-level discipline, could be awarded a Bachelor of Medicine or Science degree according to the specific training program of each university. Students who successfully completed the five-year program received a Bachelor of Medicine, while students who completed the four-year program were awarded a Bachelor of Science.
By 2012, China’s economic and social development had progressed significantly. To adapt to the needs of national and regional economic and social development and to optimize the structure of the discipline, the Ministry of Education revised the previously issued regulations on program requirements. This revision led to the introduction of the “Undergraduate Program Catalog for Regular Higher Education Institutions (2012)” (the new catalog) and the “Comparison Table of Old and New Programs in the Undergraduate Program Catalog” (the comparison table).3 In the new catalog, clinical medicine and medical technology were no longer affiliated with the same first-level discipline; instead, there were independent categories, ie, clinical medicine (1002) and medical technology (1010). As stipulated in the comparison table, the medical laboratory (100304) discipline was changed to the medical laboratory technology (101001) discipline, and the academic disciplines were unified into a four-year science degree.
The 2015 Reform of Professional Master’s Programs in Clinical Medicine Prevented Medical Laboratory Technology Undergraduates from Pursuing Professional Degrees in Clinical Laboratory Diagnostics
In the reform of undergraduate specialties, medical laboratory technology studies were completely transformed from medical training (five years) to science training (four years), but a demand for clinical physicians persists in China. In accordance with the “Catalog of Degrees and Personnel Training Disciplines (2011)”4 issued by the Academic Degrees Committee of the State Council and the “Implementation Rules for the Independent Establishment of Secondary Disciplines for Doctoral and Master’s Degrees and Graduate School”5 issued by the Ministry of Education, the curricula of degree-conferring institutions include the first-level discipline of clinical medicine (1051) and a professional degree in clinical laboratory diagnostics was established to cultivate a team of laboratory physicians with combined clinical, research, and teaching capabilities.
In 2015, the Ministry of Education issued the “Guiding Training Program for Postgraduates with a Master’s Degree in Clinical Medicine” to strengthen the connection between training for master’s students in clinical medicine (specialized master’s-level training) and a standardized training system for resident physicians (regular training system).6 In the program, the enrollment subjects for the “master of clinical medicine” are specified as “current or past undergraduate students who meet the requirements for the Physician’s Qualifying Examination” and that “the training process should be standardized in accordance with the training content and standards of the resident medical program”. According to the “Regulations on Registration Qualifications for Physician Qualification Examination (2014 Edition)”7 which is still in use, only some specialties within an undergraduate degree program lasting five years or longer (such as five-year clinical medicine and five-year medical laboratory programs) can be used as educational backgrounds when prospective students apply to medical doctor programs. Currently, four-year medical laboratory technology undergraduate students trained by the faculty of the Department of Medical Laboratory/Medical Laboratory Institute at various universities are not eligible for clinical laboratory diagnostics (professional degree) programs and cannot receive further training as laboratory physicians.
Serial Reforms Completely Changed the Enrollment Process for Students in Clinical Laboratory Diagnostics Master’s Degree Programs and Gave Rise to the “Four Certificates in One” Era
Following a series of top-down reforms in undergraduate specialties and graduate training, the primary source of students for the professional master’s program in clinical laboratory diagnostics changed from undergraduates in medical laboratory science (trained by the faculty in this discipline) to undergraduates in clinical medicine, who typically lack familiarity with medical laboratory science. The training objectives are oriented mainly toward improving students’ ability to practice in the clinic. Clinical rotations are conducted in accordance with the “Standardized Resident Standardized Training Base Identification Criteria” and “Standardized Resident Standardized Training Content and Standards”.8 That is, the students complete a total of 33 months of rotation training, including 11 months of rotations in clinical departments and 22 months of rotations in the laboratory (Table 1). After students pass various assessments, those who graduate with a professional master’s degree in clinical laboratory diagnostics obtain a physician qualification certificate, standardized resident training certificate, postgraduate graduation certificate and master’s degree certificate; thus, the master’s degree training in clinical laboratory diagnostics has officially entered the “four certificates in one” era.
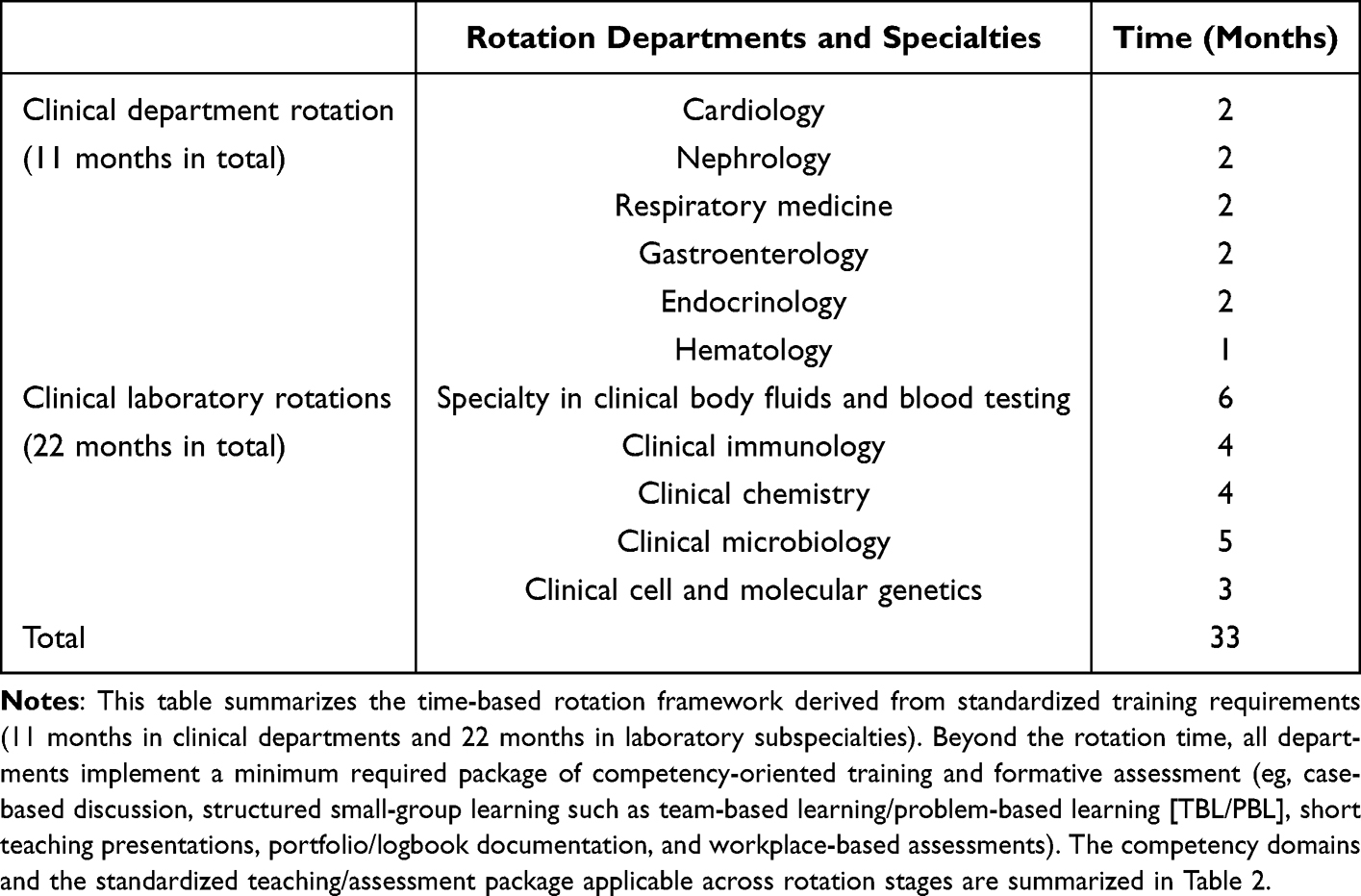 |
Table 1 Standardized Rotation Schedule for Laboratory Medicine Trainees Under the “Four Certificates in One” Training Pathway in China (33 Months in Total)8 |
Opportunities and Challenges Pertaining to the Development of Undergraduate Students in Clinical Medicine for a Master’s Degree in Clinical Laboratory Diagnostics from the SWOT Perspective
Before the “four certificates in one” era, a series of national reforms in undergraduate majors and professional master’s training were intended to recruit clinical medicine undergraduates—who possess stronger clinical fundamentals—and subsequently cultivate them into laboratory physicians through standardized postgraduate rotations. However, in implementation, the primary bottleneck has become recruitment itself, with many clinical laboratory diagnostics (professional degree) programs struggling to enroll qualified applicants.
As of 2025, 27 second-level disciplines are included under the first-level discipline of clinical medicine (professional degree), including clinical laboratory diagnostics (105120).9 In contrast, within traditional “popular” tracks (eg, internal medicine and surgery), universities often provide multiple third-level directions (for example, 17 third-level disciplines within internal medicine and surgery at Sichuan University).9 Faced with abundant alternatives, clinical medicine undergraduates frequently treat auxiliary departments, including laboratory medicine as a last choice, which translates into weak application volume and quality for 105120 programs. Publicly available admission statistics illustrate this pattern. In 2023, the reexamination cutoff for the clinical medicine professional master’s category (1051) at Capital Medical University was 330, and the clinical laboratory diagnostics program (105120) admitted two candidates with preliminary scores of 330 and 331.10 In 2024, the same program enrolled zero students via the primary admission route (including merit-based direct admission) and ultimately admitted two students via the transfer pool.11 At Shanghai Jiao Tong University in 2024, 105120 applicants were scarce across multiple affiliated hospitals, with several sites relying on transfers to fill seats.12 These objective signals indicate that the specialty’s recruitment challenge is structural rather than incidental.
To clarify why clinical medicine undergraduates hesitate to choose laboratory medicine—and how the “four certificates in one” framework reshapes training feasibility—this section applied the SWOT framework13 to analyze the internal strengths/weaknesses and external opportunities/threats for clinical medicine undergraduates entering clinical laboratory diagnostics (professional degree) training.
Internal Strengths Analysis (S)
Clinical Reasoning and Communication Can Compensate for Early Limitations in Laboratory Interpretation and Consultation
The core advantage of clinical medicine undergraduates in laboratory settings is their relatively strong clinical knowledge base and early exposure to clinical reasoning. Undergraduate training in clinical medicine typically covers core clinical disciplines (internal medicine, surgery, obstetrics and gynecology, pediatrics, and infectious diseases) and is accompanied by structured clerkships and/or internship experiences that emphasize bedside decision-making and patient-facing communication. This background helps trainees interpret laboratory results in the clinical context and communicate effectively with clinicians—capabilities that are particularly relevant as laboratory medicine increasingly extends beyond “data reporting” toward interpretive and consultative services.
In the standardized training stage, clinical laboratory diagnostics professional master’s trainees also rotate through clinical departments and may function as frontline “bedside physicians” for a defined period. This experience creates a concrete demand for high-quality reports and fosters a user-centered perspective: trainees learn to think like clinicians who rely on laboratory information for diagnosis and management rather than as operators who only validate analytic outputs.
Licensed Physicians are Institutionally Positioned to Issue Interpretive Diagnostic Reports
China’s regulatory framework emphasizes physician responsibility in diagnostic reporting. The Administrative Measures for Clinical Laboratories in Medical Institutions specify that diagnostic clinical examination reports should be issued by licensed physicians.14 In parallel, the Laboratory Physician Branch of the Chinese Medical Doctor Association has issued multiple expert consensuses describing diagnostic reporting models across subspecialties (eg, microbiology, genetics, urinalysis, anemia-related testing, and others).15–27 Graduates of clinical laboratory diagnostics professional master’s programs hold both physician qualifications and standardized residency training completion credentials, with an accredited scope of practice in “Medical Laboratory and Pathology”. This positioning supports the development of interpretive reporting and structured consultation as formal responsibilities of laboratory physicians rather than optional add-ons.
A Hybrid “Clinical + Laboratory” Profile is Relatively Scarce and Can Act as an Interdisciplinary Bridge
Most laboratory teams are still dominated by technologists, and many departments report persistent needs in terms of clinical consultation capacity, interpretive reporting, and clinically oriented research. Trainees who combine clinical reasoning, laboratory workflow understanding, and research literacy can become interdisciplinary “bridging” talent—especially in settings where laboratory services are expected to integrate quality governance, report standardization, and clinician-facing communication.
Analysis of Internal Weaknesses (W)
Insufficient Laboratory Medicine Theory and Workflow Governance in the Early Stage
A major weakness lies in the early-stage mismatch between the eligible recruitment pool (clinical medicine undergraduates) and laboratory medicine’s competency demands. In many undergraduate curricula, laboratory medicine exposure is limited to small components embedded in diagnostic teaching, with insufficient systematic training in quality management, pre/postanalytical governance, or structured report interpretation. As a result, trainees may experience high onboarding costs when they enter laboratory rotations and may require a longer period to form a stable professional identity in laboratory medicine.
Career Advancement May Be More Challenging on Physician Tracks Than on Technologist Tracks
Under existing promotion systems, physician-track title requirements are often more demanding than those for technologists, while physician positions may be fewer. This structural reality can weaken specialty attractiveness, particularly when students compare opportunity costs across clinical disciplines.
Post Availability May Lag Behind Training Objectives in Some Institutions
In some hospitals, laboratory output remains dominated by analytic data reports, and interpretive reporting/consultation services are not yet institutionalized. Consequently, newly trained laboratory physicians may initially be assigned to technologist-like roles. This does not negate the value of physician training, but it can dilute early career identity formation and reduce the perceived return on training investment.
External Opportunities Analysis (O)
Systemic-Level Reforms May Rebalance Specialty Choices and Push Laboratories Toward Higher-Value Services
With increasing healthcare reform, the attractiveness and competitive returns of traditionally popular clinical departments may change, and the selection of specialties may become more diversified. Under reforms such as the promotion of the Sanming healthcare reform experience nationwide,28–30 institutions are increasingly incentivized to realign income distribution with service workload and quality. For laboratory departments, this trend encourages transformation beyond assembly line numerical reporting toward higher-value services, including clinical communication, multidisciplinary consultation (MDT), and interpretive reporting. Such service upgrading creates a clearer value proposition and organizational space for laboratory physicians.
Pilot Establishment of Laboratory Testing Clinics Expands the Clinical Interface of Laboratory Medicine
The 2022 Administrative Measures for the Mutual Recognition of Inspection and Test Results encourage qualified institutions to establish examination and laboratory testing clinics staffed by physicians specializing in medical laboratory and pathology, enabling independent diagnostic reporting services.31 Early implementations in several tertiary hospitals suggest an expanding space for laboratory physicians to deliver post-analytical interpretation, triage suggestions, and joint clinics, thereby creating clearer role legitimacy and stronger employment pathways.
The “Silver Economy” Increases the Demand for Diagnostic Stratification and Longitudinal Management
With population aging and policy support for the “silver economy”, laboratory diagnosis is being increasingly embedded in early screening, chronic disease management, and precision stratification.32 This demand strengthens the rationale for training laboratory physicians capable of integrating test interpretation with clinical pathways, especially for complex, long-term conditions.
External Obstacles Analysis (T)
DRG/DIP-Style Payment Reform May Compress Margins and Intensify Efficiency Pressure
Payment reforms based on diagnosis-related grouping and bundled packages can constrain resources and alter test utilization patterns. Laboratories may face pressure to justify testing value, optimize test menus, and reduce waste. In the absence of strong quality management and clinical communication capacity, laboratories risk being positioned as cost centers rather than clinical partners.
Interdisciplinary Boundary Growth Creates Governance and Training Challenges
As point-of-care testing expands, questions arise regarding who performs testing, who ensures quality, and how results are governed across pre-/post-analytical stages. Uniform qualification/training requirements for POCT examiners and reviewers are not always specified in existing consensus documents.33 These boundary dynamics increase the need for laboratory physicians, who can lead in governance, standardization, and cross-department collaboration.
Synthesis of SWOT Findings and Implications for Training Design
Collectively, the SWOT analysis indicates that the central problem is not a lack of policy intention but a structural misalignment: clinical medicine undergraduates constitute the main eligible recruitment pool, yet they often enter training with limited laboratory theory and governance exposure, while employment environments vary in how fully laboratory physician roles are implemented. Therefore, the key educational task is to translate the above findings into a training pathway that (i) builds longitudinal competencies spanning quality management, consultation/communication, and informatics/workflow governance and (ii) uses feasible, workplace-based methods to document progress across heterogeneous training programs. The practical realization of this translation is discussed in Practical Exploration of the Experimental Class Model Used for Training Laboratory Physicians–4.
Practical Exploration of the Experimental Class Model Used for Training Laboratory Physicians
Clinical + Laboratory Medicine: Training Laboratory Physicians from the Undergraduate Stage
A key barrier identified in the SWOT analysis (Section 2) is the early stage mismatch between the current eligible recruitment pool (clinical medicine undergraduates) and the competency demands of laboratory medicine. Clinical medicine undergraduates often lack systematic exposure to laboratory medicine theory, workflow governance, and post-analytical quality assurance. As a result, the transition to laboratory rotations may be characterized by high onboarding costs and delayed professional identity formation. These gaps cannot be fully addressed by relying solely on postgraduate rotations if upstream exposure remains insufficient. Therefore, a training pathway that “front loads” laboratory medicine exposure—while maintaining the clinical reasoning strengths of medical undergraduates—has become an important direction for reform.
In this context, China has initiated pilot reforms to integrate clinical and laboratory medicine training earlier in the education continuum. In 2022, the Ministry of Education issued a policy notice supporting selected universities to accelerate the training of high-level laboratory medicine personnel, and multiple institutions subsequently introduced “laboratory physician training pilot/experimental classes” that connect an undergraduate clinical medicine track with a downstream professional master’s pathway in clinical laboratory diagnostics.34–37 These pilots are intended to narrow the upstream exposure gap and to strengthen continuity between undergraduate education and the “four certificates in one” postgraduate pathway by enabling trainees to enter laboratory medicine with clearer expectations and a more coherent competency trajectory.
Brief international and cross-disciplinary comparisons suggest that the direction of these pilots is consistent with mature competency-based training concepts. In Europe, the EFLM postgraduate syllabus for specialists in laboratory medicine explicitly includes longitudinal competencies beyond analytic techniques, such as laboratory organization/management, quality systems, and clinical consultation functions.38 The IFCC curriculum similarly frames laboratory medicine training as a blend of laboratory organization and management, evidence-based laboratory medicine, and clinical interpretation responsibilities.39 In related service-intensive medical disciplines (eg, pathology residency training), workplace-based assessment toolkits are widely used to document progression through real clinical work—commonly including portfolios/logbooks, direct observation tools (mini-CEX/OSCE-type assessments), and multisource feedback—to provide pragmatic templates for tracking competency development across heterogeneous training settings.40,41 These brief comparisons are not intended to advocate direct transplantation of foreign administrative structures; rather, they provide a training rationale for why China’s pilot programs emphasize competency mapping and assessment packaging in addition to rotation duration, particularly where trainees enter with heterogeneous foundations and where training quality may vary across schools.
In the pilot model, the training process is typically organized as an undergraduate stage (a clinical medicine track) followed by a postgraduate stage (a three-year professional master’s program in clinical laboratory diagnostics).34–36 The undergraduate stage is designed to introduce laboratory medicine earlier while preserving core clinical medicine learning, thereby narrowing the informational and cognitive gap between clinical medicine undergraduates and laboratory practice. Outstanding graduates who meet institutional standards may subsequently enter clinical laboratory diagnostics professional master’s programs through structured selection pathways (eg, recommendation/exemption mechanisms implemented by individual institutions) and ultimately pursue integrated outcomes aligned with the “four certificates in one” framework. Importantly, this approach does not seek to restore the pre-2012 five-year “clinical laboratory” undergraduate major. Instead, it aims to conform to the current policy environment for physician training while creating a coherent pipeline that develops laboratory physicians with both a clinical orientation and laboratory governance competence.
The intended outcome of the experimental class is to cultivate well-rounded laboratory physicians who are “proficient in the clinical laboratory” and who can participate in laboratory work as laboratory physicians in the future. This includes strengthening communication between laboratory examinations and clinical practice, participating in multidisciplinary consultation, providing decision-making advice regarding diagnosis and treatment, and conducting research oriented towards clinical problems with laboratory solutions.37 In this sense, the pilot class responds directly to the upstream recruitment and competency mismatch identified in Section 2: it aims to reduce onboarding costs, accelerate professional identity formation, and make post-analytical and governance-oriented competencies trainable and assessable across the education continuum.
Table 2 translates the pilot model into a rotation-wide competency framework with corresponding teaching activities and assessment tools. Importantly, because these pilots have been implemented only recently and the first cohort has not yet completed the full training cycle, the available evidence is primarily policy- and design-based rather than outcome-based. Therefore, the practical exploration in this section focuses on training alignment mechanisms, competency design, and foreseeable implementation challenges, while future evaluation priorities are proposed.
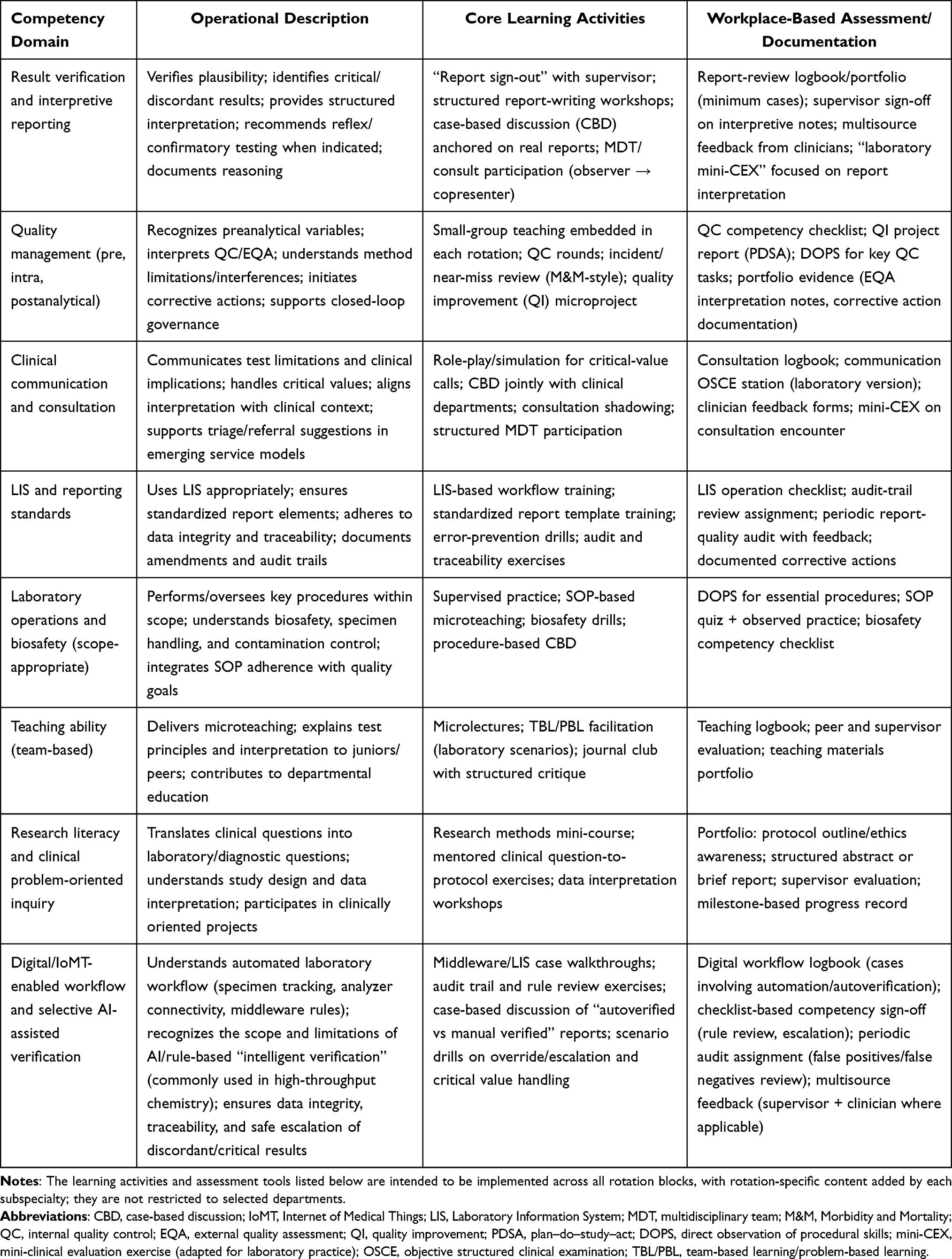 |
Table 2 Competency-Oriented Training Package Applicable Across Laboratory Rotations for Laboratory Physician Trainees |
Implementation Barriers and Key Alignment Issues in Training Practice
Although the experimental class model offers a policy-conforming route to rebuild the laboratory-physician pipeline, early implementation has faced predictable constraints. These constraints do not invalidate the mo rather, they indicate that training design must be coupled with governance and alignment mechanisms across curriculum, recruitment, program capacity, and career pathways.
First, curriculum capacity and faculty workload are binding constraints. Achieving integrated training in “clinical medicine + laboratory medicine” within a five-year undergraduate program requires restructuring the curriculum (contact hours, sequencing, and integration). This reform has increased the burden of teaching and supervision across departments and is highly dependent on adequate faculty pools and stable teaching organization. Without explicit workload recognition and cross-departmental coordination, implementation quality may become heterogeneous and difficult to sustain.
Second, expectation management and informed selection are essential. A recurring challenge is that students may enter the experimental class without a realistic understanding of laboratory medicine as a specialty and of the current role boundaries of laboratory departments. Misinterpretation of the pathway as a guaranteed “5+3 integrated” route can lead to disappointment, identity diffusion, or attrition when students later clarify the actual selection standards and career realities. Therefore, recruitment should be coupled with transparent information disclosure (role definition, competencies, realistic career pathways) and early exposure mechanisms. Institutional adjustments in selection strategies reported by pilot universities further suggest that optimizing recruitment entrance and timing is critical for reducing mismatch and improving retention.34–36
Third, alignment with SRT-based governance and institutional capacity must be considered. Professional master’s training is deeply embedded in hospital departments that simultaneously function as SRT specialties/professions.6,8 Base governance typically includes routine evaluation and an exit mechanism, and sustained recruitment performance is closely linked to the stability of the training platform. Under-enrollment may therefore become not only an educational problem but also a risk to training continuity at the base level. For this reason, experimental classes should be designed to stabilize the upstream recruitment pipeline while maintaining clear progression rules and quality thresholds.
Fourth, digital transformation and selective AI-enabled practices also imply new reskilling/upskilling needs. Notably, AI-related content is not explicitly specified as a mandatory requirement in current national training standards for laboratory physicians. Nevertheless, the degree of digitalization varies across training programs. In some hospitals, the laboratory has implemented automated specimen-processing lines and AI-assisted or rule-based “intelligent verification” workflows for laboratory reports, most commonly in high-throughput clinical chemistry testing. These location-specific practices do not constitute a uniform policy mandate, but they are increasingly relevant to day-to-day laboratory governance and post-analytical decision support. Therefore, it is pragmatic to incorporate reskilling/upskilling elements into the training design as a competency extension—focusing on digital workflow literacy, data integrity, audit trails, and the safe use/limitations of AI-assisted verification—while allowing flexibility according to local infrastructure and the scope of practice.
Finally, downstream career pathways must match the training objectives. If institutions lack mature laboratory physician roles (eg, interpretive reporting workflows, consultation services, or laboratory clinics), graduates may be deployed into technologist-like roles, weakening professional identity formation and reducing the perceived return on training. Therefore, the sustainability of experimental classes depends on parallel organizational development: defining laboratory physician responsibilities, establishing service scenarios in which interpretive competencies are used, and building career ladders and evaluation standards that recognize consultative and quality-governance contributions.
Reflection on and Prospects of Master’s Degree Training in Clinical Laboratory Diagnostics
Under the “four certificates in one” framework, the training of professional master’s students in clinical laboratory diagnostics is tightly coupled with standardized residency training (SRT). In China, SRT is implemented through accredited training programs at the hospital level and their specialty/professional programs at the department level. For laboratory medicine, the “training setting” is, in practice, the hospital laboratory department: the same personnel and infrastructure simultaneously undertake routine laboratory service delivery, SRT responsibilities, and the hospital-based component of postgraduate professional degree training. Under this governance structure, base qualifications are dynamic rather than permanent. Training programs are subject to routine evaluation and accountability mechanisms, and sustained recruitment performance is an essential element of program operations. When annual recruitment fails to meet regulatory expectations or when persistent under-enrollment prevents normal training organization, schools may receive warnings and be required to rectify the deficiencies; continued failure may lead to the suspension of recruitment eligibility or the withdrawal of program qualifications. Once the corresponding program qualification is restricted or withdrawn, the institution’s ability to provide an SRT-aligned professional master’s training pathway is directly undermined. Therefore, under-enrollment is not merely an admission issue—it can evolve into a systemic risk to training continuity.
A second structural contradiction lies in the mismatch between who is eligible to apply and who is most likely to identify with the specialty. The higher education reform in clinical laboratory medicine over the past decade aimed to attract clinical medicine graduates to transition to laboratory physicians through postgraduate training. However, many clinical medicine undergraduates enter the application stage with a limited understanding of laboratory medicine, unclear career images, and insufficient awareness of the professional role of laboratory physicians. Conversely, young people who develop an early professional identity and a sense of belonging to laboratory medicine often follow medical technology majors, but they may not follow the clinical laboratory diagnostics (professional degree) laboratory physician qualification pathway. This mismatch weakens both recruitment quality and long-term retention.
Given these constraints, future optimization should focus on interventions that are feasible within the existing policy framework and that directly target the recruitment–training–career alignment chain.
Strengthening Early Exposure and Informed Choice at the Undergraduate Stage
Interest and sustained motivation are strong drivers of professional development, yet high school graduates typically cannot make an informed choice of subspecialty. In clinical medicine undergraduate education, increasing the coverage of auxiliary departments (including laboratory medicine) during clerkships and advancing the timing of such exposure can help students convert early “perceptual impressions” into informed, rational career decisions. Earlier and broader exposure can reduce information asymmetry, improve specialty fit, and, importantly, stabilize the upstream recruitment pipeline that is necessary for maintaining base-level training continuity.
Policy-Sensitive Talent Cultivation in Top-Tier Medical Schools
To reduce excessive competition concentrated in a small set of traditionally popular specialties and to cultivate talent for auxiliary departments, top-tier medical schools can implement targeted adjustments in both undergraduate training and postgraduate admissions. The “laboratory physician training class” piloted in recent years illustrates a policy-conforming approach: by embedding laboratory medicine more explicitly within clinical medicine education and by providing a clearer training route to laboratory physician roles, such pilots can improve specialty visibility and reduce mismatch. At the current stage—given the short implementation history—these pilots should be framed as institutional mechanisms for recruitment stabilization and competency scaffolding, with transparent selection criteria and realistic career information to prevent expectation bias.
Bridging the Early-Stage Knowledge Gap at the Master’s Level
To address the consistently observed weakness of clinically trained entrants—insufficient laboratory medicine theory at entry—a structured laboratory medicine theory module should be incorporated into the professional master’s training pathway. This can be implemented in two complementary formats: (1) a credit-bearing graduate course incorporated into the university training plan and assessed through the graduate school and/or (2) rotation-embedded small-group teaching for each laboratory subspecialty, delivered and assessed by the specialty faculty within the SRT-aligned platform. The goal is to shorten the onboarding time and enable trainees to transition from routine operational tasks to quality-aware verification, interpretive reporting, and consultation competencies.
Matching Training Objectives with Real Service Scenarios and Career Ladders
Even with well-designed training, the sustainability of the laboratory physician pathway depends on whether hospitals provide mature service scenarios in which physician-track competencies are used and recognized. Laboratories should progressively establish standardized interpretive reporting workflows, consultation pathways, and, where policy and institutional conditions permit, service models such as laboratory testing clinics. In parallel, hospitals should clarify laboratory physician responsibilities and develop evaluation and promotion mechanisms that recognize contributions in consultation, quality governance, education, and clinically oriented research so that graduates can form a stable professional identity and perceive a meaningful return on training.
Strengthening the Medical Technology Graduate Pipeline and Employment Alignment
To promote the multidimensional development of laboratory medicine teams (medicine, technology, teaching, and research), it is also necessary to improve admission–training–employment alignment for medical technology graduate students. Since 2012, although the undergraduate five-year medical laboratory major has been adjusted into a four-year medical laboratory technology major, the development of graduate-level medical technology disciplines has been relatively slow, and clinical laboratory diagnostics (academic degree) has often remained a primary route for further education. Moreover, some employers and regional systems have not fully updated position eligibility catalogs in response to discipline reforms, leading to situations in which positions still rigidly require a “clinical laboratory diagnostics” background and thereby constrain employment opportunities for qualified medical technology master’s/doctoral graduates. Universities, as key actors in educational reform, should proactively communicate with recruiting units to improve the recognition of medical technology degrees and to promote appropriate recruitment of medical technology graduates. Regional health authorities should also update position eligibility directories in a timely manner to reflect discipline changes and to fully leverage available talent.
In addition, as laboratory digitalization advances unevenly across bases, competency frameworks should be periodically updated to include reskilling/upskilling components related to LIS/middleware governance, IoMT-enabled workflow literacy, and the safe use and limitations of AI-assisted verification, rather than treating such content as a uniform policy requirement at the current stage.
Overall, because current pilot laboratory physician classes have been implemented only for a short period and cohort outcome data are not yet available, near-term priorities should emphasize process transparency and prospective evaluation. Recommended evaluation elements include recruitment and retention indicators, competency milestone attainment (via portfolios/logbooks and workplace-based assessments), multisource feedback from clinicians, and medium-term graduate outcomes. Such evidence is essential for scaling effective elements of the training pathway and refining policy design.
Conclusion
In summary, with the rapid evolution of clinical diagnosis and treatment, laboratory services are expected to move beyond delivering numerical test results toward providing interpretation, diagnostic suggestions, and consultative support that can be integrated into clinical decision-making. In this context, graduates trained in the professional master’s pathway of clinical laboratory diagnostics are indispensable for modern medical laboratory teams. However, persistent under-enrollment and suboptimal specialty fit among applicants remain the principal bottlenecks, weakening the continuity and sustainability of laboratory physician training pathways.
This review highlights that the core challenge is a recruitment–training–career alignment problem rather than an isolated curriculum issue. Upstream, earlier and broader exposure to laboratory medicine within undergraduate clinical training is needed to reduce information asymmetry and support informed specialty choice. During postgraduate training, deliberate reskilling/upskilling should be strengthened to address common competency gaps among clinical medicine entrants—particularly in laboratory medicine fundamentals, quality management across the total testing process, interpretive reporting, and structured clinical communication/consultation—so that trainees can progress beyond routine operations to quality-aware verification and clinically meaningful decision support. Downstream, hospitals should ensure that physician-track competencies can be practiced and recognized through clearly defined service scenarios and role expectations, thereby improving professional identity formation and retention.
Future research should move from policy- and design-based discussion to outcome-based evaluation. Priority directions include multicenter prospective assessments of recruitment and retention, competency milestone attainment (using workplace-based assessments and longitudinal portfolios), quality indicators for interpretive reports and consultation services, and medium-term career outcomes. In addition, as laboratory digitalization expands unevenly across schools, further work is needed to evaluate how local AI-assisted verification and informatics-enabled workflows affect competency requirements, training delivery, and patient care value.
Author Contributions
All the authors made significant contributions to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Sichuan Science and Technology Program (No. 2024NSFSC1555).
Disclosure
The authors report there are no conflicts of interest in this work.
References
1. Wang C. Development and prospect of laboratory medicine in China in the past 70 years. Chin Jf Laborat Med. 2019;
2. Ministry of Education of the People’s Republic of China. (2012). Undergraduate program catalog for regular higher education institutions[1998]No. 8. Available from: http://www.moe.gov.cn/srcsite/A08/moe_1034/s3882/199807/t19980706_109699.html.
3. Ministry of Education of the People’s Republic of China. (2012). Circular on Issuing the “Undergraduate Program Catalog for Regular Higher Education Institutions (2012)” and the “Regulations on the Management of Undergraduate Program Establishment in Regular Higher Education Institutions” [Jiao Gao] [2012] No. 9. Available from: http://www.moe.gov.cn/srcsite/A08/moe_1034/s3882/201209/t20120918_143152.html.
4. Academic Degrees Committee of the State Council & Ministry of Education of the People’s Republic of China. Circular on Issuing the “ Catalog of degrees and personnel training disciplines (2011):document of the academic degree committee [2011] No. 11. 2011. Available from: http://www.moe.gov.cn/srcsite/A22/moe_833/201103/t20110308_116439.html.
5. General Office of the Ministry of Education of the People’s Republic of China. Circular on issuing the implementation rules for the independent establishment of secondary disciplines for doctoral and master’s degrees and graduate school[2010] 1. 2010. Available from: http://www.moe.gov.cn/srcsite/A22/s7065/201012/t20101224_113508.html.
6. Academic Degrees Committee of the State Council. Circular on Issuing the Guiding Training Schemes for Professional Master’s Degree Postgraduates in Clinical Medicine, Stomatology, and Chinese Medicine [2015] No 9. Available from: http://www.moe.gov.cn/srcsite/A22/moe_826/201506/t20150618_190613.html.
7. National Health and Family Planning Commission of the People’s Republic of China, Ministry of Education of the People’s Republic of China, & State Administration of Traditional Chinese Medicine of the People’s Republic of China. Notice on issuing the “Regulations on physician qualification examination registration eligibility (2014 edition)”. State Council Gazette. 2014;2014(20).
8. General Office of the National Health and Family Planning Commission of the People’s Republic of China. (2014). Notice on Issuing the “Standards for recognizing standardized residency training bases (Trial)” and the “Content and standards for standardized residency training (Trial)” [Document No. Guo Wei Ban Ke Jiao Fa (2014) No. 48]. Available from: http://www.nhc.gov.cn/cms-search/xxgk/getManuscriptXxgk.htm?id=946b17f463fa4e5dbcfb4f7c68834c41.
9. China Graduate Enrollment Information Network. (2025). Master’s program catalog. Available from: https://yz.chsi.com.cn/zsml/a/.
10. Capital Medical University Graduate School. (2023). Statistics on master’s program admissions by major. Available from: https://yjsh.ccmu.edu.cn/zsgz/lnqk/759a76cea4fc4a9d95fa12ed626fc108.htm.
11. Capital Medical University Graduate School. (2024). Statistics on master’s program admissions by major. Available from: https://yjsh.ccmu.edu.cn/zsgz/lnqk/7f188a88ac4b4f31af2f1531961d6cc3.htm.
12. Shanghai Jiao Tong University Graduate Admissions Website. (2024). Statistics of applicants and admitted students for master’s programs at Shanghai Jiao Tong University. Available from: https://yzb.sjtu.edu.cn/post/2565.
13. Xie Y, Gu W, Meng X, et al. Thoughts and exploration on cultivating excellent clinical medical talents in the cross-disciplinary context of medicine and engineering and the background of “New medicine”. Chin J Med Educ Res. 2024;09:1221–13. doi:10.3760/cma.j.cn116021-20240311-01852
14. Ministry of Health of the People’s Republic of China. Notice on issuing the “Administrative measures for clinical laboratories in medical institutions” [Document No. Wei Yi Fa (2006) No. 73]. 2006. Available from: http://www.nhc.gov.cn/yzygj/s3577/200804/d3281df051d44badbd45cf12fe95a28e.shtml.
15. Infectious Diseases Laboratory Medicine Expert Committee, Chinese Physician Association Laboratory Physician Branch. Expert consensus on diagnostic reporting models for clinical microbiology testing. Nat Med J China. 2016;96(12):937–939. doi:10.3760/cma.j.issn.0376-2491.2016.12.006
16. Molecular Diagnostics Expert Committee, Chinese Physician Association Laboratory Physician Branch. Expert consensus on diagnostic reporting models for clinical genetic testing. Nat Med J China. 2016;96(14):1087–1090. doi:10.3760/cma.j.issn.0376-2491.2016.14.005
17. Chinese Physician Association Laboratory Physician Branch. Expert consensus on diagnostic reporting models for routine urine tests. Nat Med J China. 2017;97(18):1369–1372. doi:10.3760/cma.j.issn.0376-2491.2017.18.003
18. Chinese Physician Association Laboratory Physician Branch. Committee of laboratory medicine for anemic diseases. Exp Consens Diagnost Report Model Anemic Dis. 2016;96(12):930–932. doi:10.3760/cma.j.issn.0376-2491.2016.12.004
19. Chinese Physician Association Laboratory Physician Branch. Committee of laboratory medicine for sexually transmitted diseases. expert consensus on diagnostic reporting models for sexually transmitted diseases. Nat Med J China. 2016;96(14):1075–1079. doi:10.3760/cma.j.issn.0376-2491.2016.14.002
20. Chinese Physician Association Laboratory Physician Branch. Committee of laboratory medicine for hematopoietic and lymphoid neoplasms. expert consensus on diagnostic reporting models for hematopoietic and lymphoid neoplasms. Nat Med J China. 2016;96(12):918–929. doi:10.3760/cma.j.issn.0376-2491.2016.12.003
21. Chinese Physician Association Laboratory Physician Branch. Committee of laboratory medicine for rapid diagnosis of infectious diseases. expert consensus on diagnostic reporting models for intestinal infectious diseases. Nat Med J China. 2016;96(14):1083–1086. doi:10.3760/cma.j.issn.0376-2491.2016.14.004
22. Chinese Physician Association Laboratory Physician Branch. Expert consensus on diagnostic reporting models for chromosomal karyotype testing. Nat Med J China. 2016;96(12):933–936. doi:10.3760/cma.j.issn.0376-2491.2016.12.005
23. Chinese Physician Association Laboratory Physician Branch. Committee of laboratory medicine for alzheimer’s disease. expert consensus on diagnostic reporting models for alzheimer’s disease. Nat Med J China. 2016;96(14):1080–1082. doi:10.3760/cma.j.issn.0376-2491.2016.14.003
24. Chinese Physician Association Laboratory Physician Branch. Expert consensus on diagnostic reporting models for catheter-related bloodstream infections. Nat Med J China. 2017;97(18):1376–1379. doi:10.3760/cma.j.issn.0376-2491.2017.18.005
25. Chinese Physician Association Laboratory Physician Branch, Autoimmune Diseases Expert Committee. Expert consensus on diagnostic reporting models for primary biliary cholangitis. Nat Med J China. 2017;97(18):1373–1375. doi:10.3760/cma.j.issn.0376-2491.2017.18.004
26. Chinese Physician Association Laboratory Physician Branch. Expert consensus on diagnostic reporting models for hepatitis B virus infection. Nat Med J China. 2017;97(18):1363–1368. doi:10.3760/cma.j.issn.0376-2491.2017.18.002
27. Chinese Physician Association Laboratory Physician Branch. Committee of laboratory medicine for thyroid diseases. Expert consensus on diagnostic reporting models for thyroid diseases. Nat Med J China. 2017;97(18):1380–1386. doi:10.3760/cma.j.issn.0376-2491.2017.18.006
28. Jifu Z, Yang Y, Lu J. Sanming healthcare reform: a forced reform—my experience with the sanming healthcare reform. Chin Hospital CEO. 2018;12(23):50–55. doi:10.21053/ceo.2018.00213
29. Leading Group for Deepening Healthcare System Reform of the State Council. Implementation Opinions on Further Promoting the Experience of Sanming City, Fujian Province and Deepening the Healthcare System Reform [Document No. Guo Yi Gai Fa].[2021] 2. 2021. Available from: https://www.gov.cn/zhengce/zhengceku/2021-10/15/content_5642920.htm.
30. National Healthcare Security Administration. (2024). Notice on further promoting the sanming healthcare reform experience and continuously driving innovation and development of healthcare insurance work [Document No. Yi Bao Han (2024) No. 25]. Available from: https://www.gov.cn/zhengce/zhengceku/202405/content_6953510.htm.
31. National Health Commission of the People’s Republic of China, National Administration of Traditional Chinese Medicine, National Healthcare Security Administration, et al. Notice on issuing the “Administrative measures for mutual recognition of inspection and test results among healthcare institutions” [Document No. Guo Wei Yi Fa (2022) No. 6]. 2022. Available from: https://www.gov.cn/zhengce/zhengceku/2022-02/19/content_5674575.htm.
32. General Office of the State Council of the People’s Republic of China. Opinions on developing the silver economy and enhancing the well-being of older persons [Document No. Guo Ban Fa (2024) No. 1]. Available from: https://www.gov.cn/zhengce/content/202401/content_6926087.htm.
33. Chinese Association of Medical Equipment. Laboratory medicine branch & chinese society of laboratory medicine, Chinese Medical Association. Chinese experts consensus on the reporting and release of POCT clinical results. Chin Jf Laborat Med. 2020;43(5):567–569. doi:10.3760/cma.j.cn114452-20190918-00542
34. School of Laboratory Medicine, Chongqing Medical University. Clinical medicine (Experimental class for the cultivation of laboratory physicians). 2022. Available from: https://jyx.cqmu.edu.cn/info/1100/2507.htm.
35. China Medical University Undergraduate Admissions Website. Illustrated guide to majors: clinical medicine (Experimental class for the cultivation of laboratory physicians). 2022. Available from: https://www.cmu.edu.cn/bkzs/info/4634/1632.htm.
36. Wenzhou Medical University Undergraduate Admissions Website. Clinical medicine (Experimental class for the cultivation of laboratory physicians). 2024. Available from: https://zhaosheng.wmu.edu.cn/info/1169/5083.htm.
37. School of Laboratory Medicine, Chongqing Medical University. Clinical medicine [i.e. Clinical medicine (Experimental class for the cultivation of laboratory physicians)]. 2024. Available from: https://jyx.cqmu.edu.cn/info/1099/3097.htm.
38. Jassam N, Lake J, Dabrowska M, Queralto J, Rizos D. The European federation of clinical chemistry and laboratory medicine syllabus for postgraduate education and training for specialists in laboratory medicine: version 5 – 2018. Clin Chem Lab Med. 2018;56(11):1846–1863. doi:10.1515/cclm-2018-0344
39. Greaves RF, Smith JM, Beastall G, et al. The IFCC curriculum – phase 1. EJIFCC. 29(1):55–93.
40. The Royal College of Pathologists. Curriculum for Specialty Training in Chemical Pathology. London: RCPath; 2021.
41. Accreditation Council for Graduate Medical Education (ACGME). Pathology milestones (Second revision). version 2 1. 2019.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.