Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Enhancing Respiratory Support in COPD Patients with Nasal High Flow Using an Asymmetrical Cannula Interface: A Randomized Cross-Over Study
Authors Nilius G, Domanski U, Khalaf M, Schroeder M, Tatkov S
Received 17 October 2025
Accepted for publication 1 March 2026
Published 10 March 2026 Volume 2026:21 528199
DOI https://doi.org/10.2147/COPD.S528199
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Georg Nilius,1,2 Ulrike Domanski,1 Mohamed Khalaf,2,3 Maik Schroeder,1 Stanislav Tatkov4
1Klinikum Dortmund gGmbH, Pneumology, Dortmund, Germany; 2Universitaet Witten/Herdecke, Witten, Germany; 3Kliniken Essen-Mitte gGmbH, Pneumology, Essen, Germany; 4Fisher & Paykel Healthcare, Auckland, New Zealand
Correspondence: Maik Schroeder, Klinikum Dortmund gGmbH, Pneumology, Dortmund, 44145, Germany, Email [email protected]
Purpose: Nasal high flow (NHF) is increasingly used in COPD patients with chronic respiratory failure. An asymmetrical cannula interface (AI) may enhance these benefits by combining increased airway pressure with reduced rebreathing from anatomical dead space. The aim of this study was to compare the effects of NHF using an AI versus a conventional symmetrical interface (SI) on tidal volume (Vt), respiratory rate (RR), minute ventilation (MV), gas exchange, and neuro-respiratory drive (NRD).
Methods: Following a 15-minute baseline period, COPD patients recovering from acute exacerbation underwent two randomized 45-minute sessions of NHF therapy using either the AI or SI. All sessions were conducted during daytime in a semi-recumbent position. Ventilation was recorded using calibrated respiratory inductance plethysmography, and transcutaneous CO2 (TcCO2) and oxygen saturation (SpO2) were continuously monitored. In addition, intercostal surface electromyography (sEMG) of the parasternal muscles was performed to assess NRD.
Results: In a group of 18 patients NHF significantly reduced RR and TcCO2, regardless of the interface used. AI significantly reduced MV compared with both baseline and SI (p = 0.048), while SpO2 increased. sEMG activity increased compared with baseline without a corresponding rise in tidal volume; however, no difference was observed between the two interfaces.
Conclusion: NHF reduced RR by increasing both expiratory and inspiratory times without altering the duty cycle. The lower MV during NHF with AI, accompanied by higher SpO2, may indicate improved gas exchange efficiency. The use of AI could enhance the respiratory support effects of NHF in patients with advanced COPD.
Keywords: nasal high flow, COPD, minute ventilation, gas exchange, work of breathing
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous lung disease characterized by progressive, irreversible or only partially reversible obstruction of the peripheral airways.1 It is associated with expiratory flow limitation and increased airway resistance, leading to progressive lung hyperinflation, increased end-expiratory lung volume, and reduced inspiratory capacity. Impaired respiratory mechanics further contribute to reduced lung elastance and elastic recoil. As the disease progresses, pulmonary emphysema develops, accompanied by damage to the pulmonary vascular bed and increased dead space ventilation. Collectively, these changes increase the work of breathing.2
With disease progression, patients with COPD may develop chronic respiratory failure of the hypoxemic or combined hypoxemic-hypercapnic type, which is associated with poor prognosis.3 Chronic hypoxemia typically requires long-term oxygen therapy. Severe hypercapnia with acidosis is managed with non-invasive ventilation (NIV), which increases ventilation via larger tidal volume (VT). In the home setting, NIV therapy after exacerbation improves gas exchange and decreases exacerbations and hospital admissions, improving QoL and survival.4 However, its benefits depend on higher ventilator pressures and patient adherence.5–7
There is a growing body of evidence supporting respiratory support with nasal high flow (NHF) in COPD with chronic respiratory failure.8 Introduced in the early 2000s for acute hypoxemic respiratory failure, NHF provides efficient oxygenation by limiting entrainment of room air and maintaining a high inspired oxygen fraction.9 NHF also reduces rebreathing from anatomical dead space, and, despite generating only modest positive end-expiratory pressure (PEEP), modifies the breathing pattern by prolonging expiration, reducing respiratory rate (RR), and may increase VT without inspiratory pressure support. These effects improve gas exchange and reduce the work of breathing.10 NHF is now established as first-line therapy for acute hypoxemic respiratory failure of various etiologies and is recommended by the European Respiratory Society over NIV and conventional oxygen therapy.11
NHF reduces dyspnea and respiratory rate compared with conventional oxygen therapy, and may reduce short-term mortality in acute respiratory failure compared with NIV.12,13 A meta-analysis reported that NHF reduces arterial carbon dioxide by ~3 mmHg in stable COPD, lowers exacerbation rates, and improves quality of life, without affecting mortality or hospitalization rates.8 In 2022, Nagata et al demonstrated that combining long-term oxygen therapy with home NHF prolonged the time to next exacerbation and reduced symptom burden.14 Another study showed that nocturnal NHF attenuated the rise in transcutaneous carbon dioxide (TcCO2) during sleep in hypercapnic COPD, although without improving sleep quality.15 In randomized trials and meta analyses comparing NHF use with NIV in acute COPD exacerbations, NHF generally showed similar mortality and intubation rates and was better tolerated with fewer complications, but evidence on treatment failure was mixed, with some studies suggesting higher failure rates and others showing comparable efficacy.16–19 A recent review highlighted survival and long-term benefits of NHF as either an alternative or adjunct to NIV in hypercapnic respiratory failure.20
Different flow rates and cannula sizes influence the physiological effects of NHF. Larger prongs increase nares occlusion, generating higher airway pressures, particularly during expiration, which may contribute to a reduction in breathing frequency. In contrast, smaller prongs, through increased leak, enhance the clearance of expired gas from the upper airways and an increase in NHF rate augments these effects.21 An asymmetrical cannula interface (AI), with one larger and one smaller prong, may amplify these benefits at the same NHF rate by combining improved airway pressure with reduced dead space rebreathing.22,23 This design could be particularly advantageous in COPD, where hyperinflation and rapid breathing limit expiration and reduce time available for dead space clearance.
The aim of this study was to compare the effects of NHF delivered via a novel AI versus a conventional symmetrical cannula interface (SI) on ventilation, gas exchange, and neuro-respiratory drive (NRD) in COPD patients with chronic respiratory failure.
Methods
This was a monocentric, randomized, controlled cross-over study in patients hospitalized with an acute exacerbation of COPD. It was approved by the Ethics Committee of the University of Witten/Herdecke (No. 125/2022) and conducted in accordance with ICH-GCP guidelines and the declaration of Helsinki. The study was prospectively registered at ClinicalTrials.gov (No. NCT05676502). All participants were informed both orally and in writing about the study and the planned measurements, and written informed consent was obtained. Patients with advanced COPD (stages 3 and 4 according to the GOLD classification) who were hospitalized at the Department of Pulmonology, Kliniken Essen-Mitte (KEM) between January 2023 and January 2024 with acute exacerbation were included. Exclusion criteria were age <18, other severe acute physical disease, that did not allow the subject to participate in a clinical trial, language, cognitive, or other barriers that made study participation impossible, pregnancy or nursing.
After a 15-minute baseline measurement with individualized oxygen administration, each session consisted of a 45-minute period of NHF therapy using one of two cannula interfaces: either AI or the standard SI typically used in clinical practice. All sessions were conducted on the same day during daytime, with a washout and lunch break of approximately 2h between the measurements, and in a semi-recumbent position under the supervision of trained study personnel and investigators (see study flow chart in Figure 1).
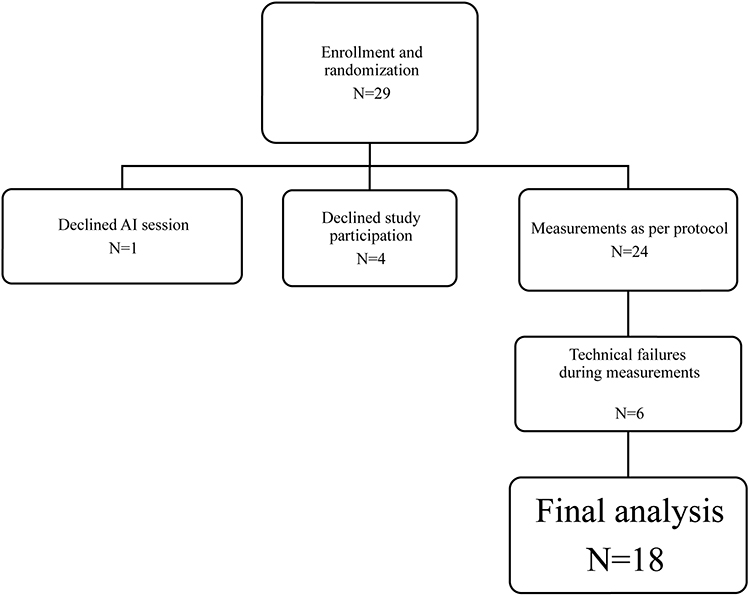 |
Figure 1 Study Flow Chart. |
The AIRVO2 device was used with NHF 30 L/min, the standard SI was the Optiflow+ and the AI was the Optiflow+ DUET (Fisher & Paykel Healthcare, Auckland, New Zealand). The supplemental oxygen flow rate was individually titrated for each patient and remained unchanged throughout the study protocol. Breathing was recorded using calibrated respiratory inductance plethysmography (Respitrace QDC, Viasys Services, Lakeland, FL, USA). TcCO2 and SpO2 were monitored with the SenTec V-Sign system (SenTec, Switzerland), and data were acquired with a 16-bit ADC converter PowerLab 16/30, and analyzed using LabChart v.8 (ADInstruments, New Zealand). Additionally, the following routine clinical data were collected: demographics, underlying and secondary diseases, lung function parameters, and blood gas analyses.
Electromyographic (EMG) recording of the parasternal muscles was performed to assess neural respiratory drive from accessory expiratory muscle activity, as previously described in detail.24,25 Signal calibration was performed prior to the study, after which participants were asked to perform two maximal inspiratory maneuvers to obtain the highest recorded parameter. Continuous monitoring of parasternal muscle activity during tidal breathing was recorded as “sEMG.”. After visual inspection and removal of artifacts (eg, periods of coughing), the maximal root mean square EMG was evaluated breath by breath. Finally, respiratory muscle EMG signals were normalized to the EMG obtained during the maximal inspiratory maneuvers, which represents neural respiratory drive (NRD). The product of this value and RR was calculated as the NRD index (NRDI).
Endpoints
The primary endpoint was the difference in the decrease in minute ventilation (MV) over 45 min under NHF with SI compared to AI. The secondary endpoints were the comparison of other respiratory parameters such as VT, RR, duty cycle, transcutaneous CO2 (TcCO2) and SpO2 values and the NRD parameters.
Statistics
This investigation was designed as a pilot study to generate new hypotheses and to describe the effects of NHF with AI and SI. Given the limited data on that subject, no sample size calculation was feasible. A total of 20 datasets was considered sufficient to detect differences between the cannula interfaces and baseline values for the primary outcome. Descriptive statistics were calculated for all data, including means and standard deviations. For the primary aim, comparative statistics were performed using the Wilcoxon test.
Results
Twenty-nine patients with COPD GOLD III–IV were initially enrolled. Four declined participations before any measurements began, and one withdrew during the study. Thus, 24 patients underwent the full study protocol. Due to technical issues, reliable and complete data evaluation was not possible for six of these patients. Ultimately, data from 18 patients were analyzed. Six were female; six had no known history of exacerbations; six experienced at least one exacerbation 2–6 months prior, and four within the preceding 1–2 years. Baseline data are presented in Table 1, the results in Table 2 with individual values in Figure 2.
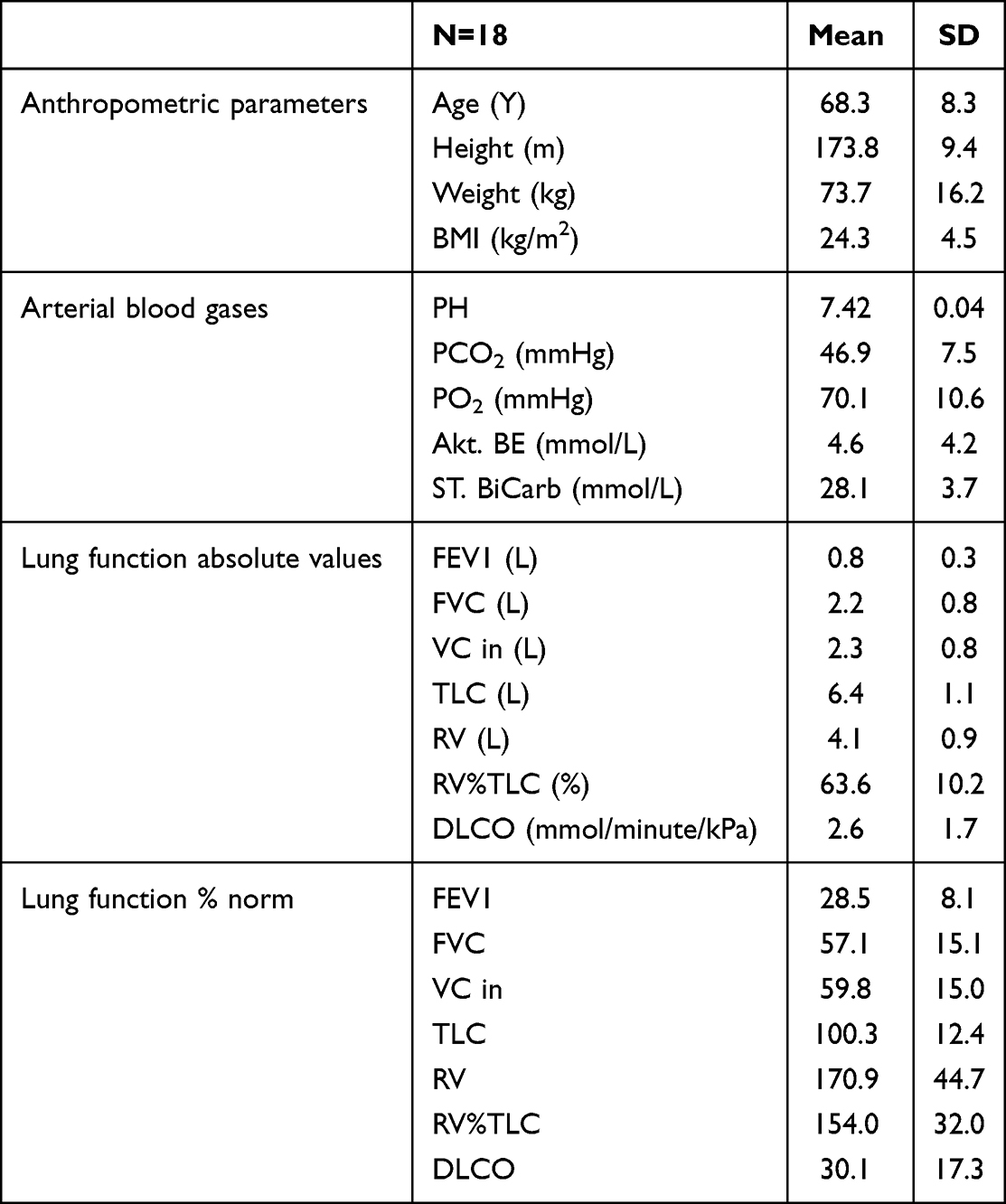 |
Table 1 Patients Baseline Data |
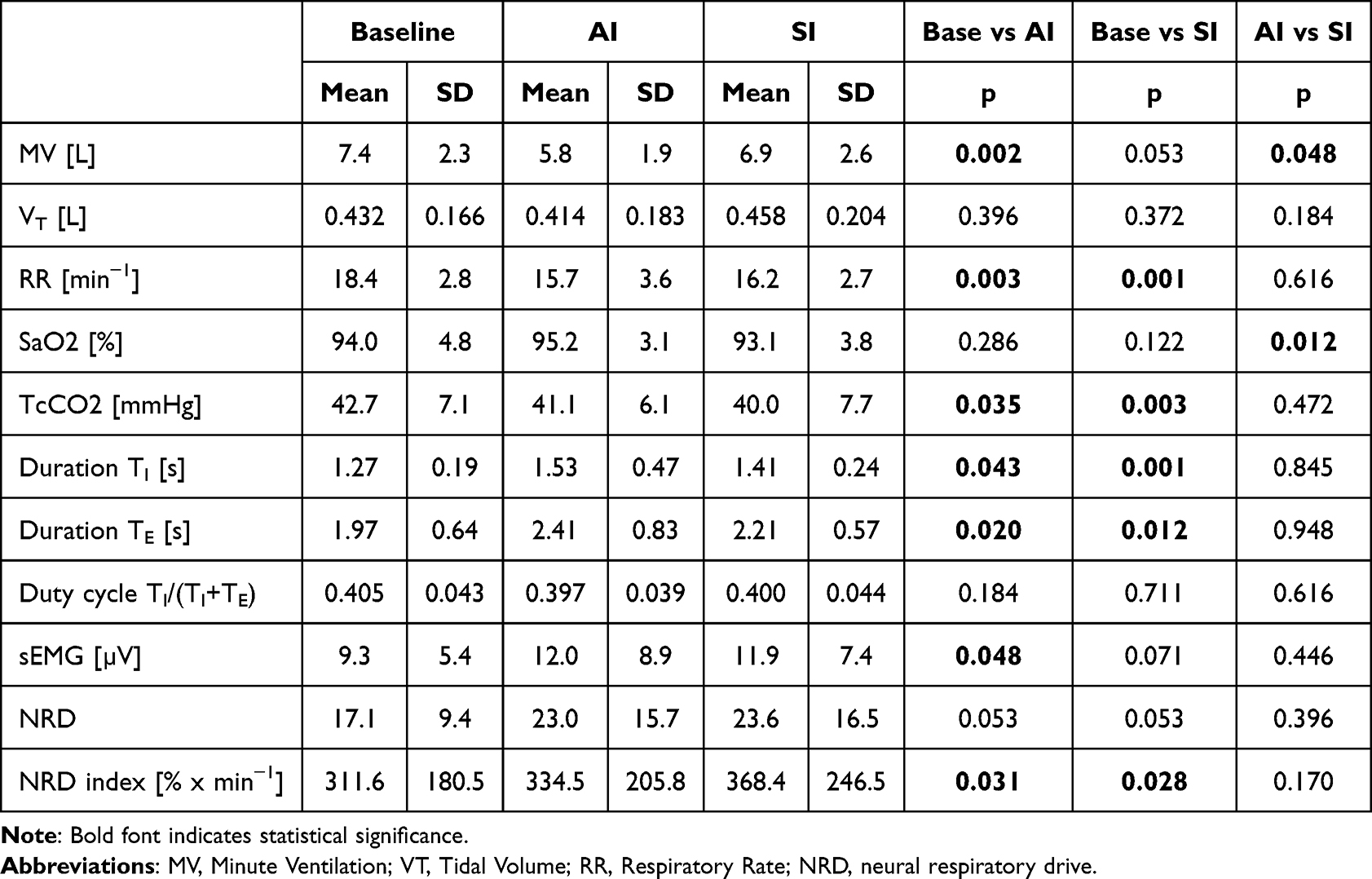 |
Table 2 Results: Baseline vs Interfaces |
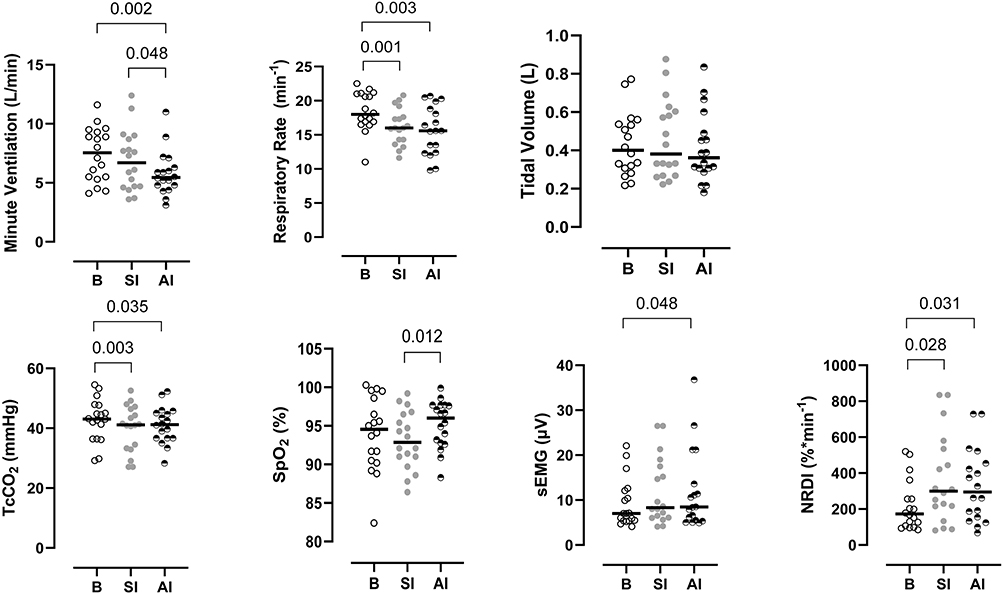 |
Figure 2 Scatter Plots of respiratory parameters and electromyography. |
Ventilation
Mean MV was 5.8 (SD 1.9) L/min during NHF with AI and 6.9 (SD 2.6) L/min with SI (p = 0.048). Compared with baseline, mean MV was lower by 1.6 L/min with AI (p = 0.002) and by 0.5 L/min with SI (p = 0.053).
No differences in VT were observed, either compared with baseline or between the two interfaces. Compared with baseline, mean RR was reduced by 2.8 min−1 with AI (p = 0.003) and by 2.2 min−1 with SI (p = 0.001) without a change in the duty cycle, but there was no statistically significant difference in RR between the two interfaces. Mean SpO2 was higher with AI (95.2 ± 3.1% vs 93.1 ± 3.8%; p = 0.012). TcCO2 decreased significantly during NHF with both interfaces.
Neural Respiratory Drive
Mean NRD was 23.0 (SD 15.7%) during NHF with AI and 23.6 (SD 16.5%) with SI, with no statistically significant difference between interfaces. Evaluation of the NRD index revealed significant differences compared with baseline only. There was no correlation between VT and sEMG (Pearson r=−0.112, p=0.389) and between VT and sEMG during maximal inspiratory maneuver (Pearson r=−0.137, p=0.325).
Discussion
The present study in patients with severe COPD during acute exacerbation requiring hospitalization demonstrated that NHF with AI significantly reduced MV compared with both baseline and SI, which is commonly used in clinical practice. Short-term NHF resulted in statistically significant reductions in RR, MV, and TcCO2, regardless of the interface. SpO2 was significantly higher during NHF with AI at the same fraction of inspired oxygen, and together with the lower MV, this may indicate improved gas exchange.
In summary, NHF reduced RR by increasing both inspiratory and expiratory times without altering the duty cycle. Contrary to our expectations, there was an increase in sEMG without a corresponding increase in VT. EMG measurements, as an indicator of NRD and thus central respiratory drive, did not show statistically significant differences between interfaces, and VT did not correlate with parasternal muscle activity on a per-breath basis. However, in contrast to MV, the NRD index was significantly higher during NHF compared with baseline. The discrepancy between this parameter and MV may suggest that NRD in severe COPD patients does not change over a short observation period, or that the neural breathing pattern controlled by the brainstem’s central pattern generator shifts towards increased activity of the accessory respiratory muscles.
The reported results are largely consistent with the current literature, although data on AI remain scarce given this relatively new therapeutic approach. Benchtop experiments with simulated breathing have demonstrated that AI is associated with accelerated clearance of expired gas from the upper airway during NHF, achieved by the creation of a differential pressure between the nasal cavities and the resulting unidirectional flow via the choanae. However, the magnitude of these effects was dependent on the breathing pattern. Increased airway pressure during NHF with AI, resulting from the decreased combined leak around the prongs, could also be beneficial for COPD patients, who commonly present with expiratory flow limitation.23,26
Slobod et al conducted a physiological crossover study with a design comparable to the current work. However, their study population consisted of patients with acute hypoxemic respiratory failure who were receiving intensive medical care, and hypercapnia or respiratory acidosis was an exclusion criterion. Consistent with our data, the authors reported that AI was associated with a significant reduction in MV, as well as a decrease in the work of breathing determined by esophageal manometry. Nevertheless, no significant differences were observed in gas exchange parameters or respiratory mechanics.27
In a recently published study, Pisani et al demonstrated a further reduction in TcCO2 in a subgroup of patients with severe hypercapnia during NHF with AI, but they did not observe statistically significant differences in ventilation parameters.22 Although the methodology was similar, their study population differed: patients were older, had considerably better lung function parameters, particularly FEV1, yet exhibited worse RR, VT, and TcCO2 values compared with the current cohort. It is reasonable to assume that it is easier to demonstrate benefits of NHF with AI in patients with more advanced disease who have higher dead space ventilation. Furthermore, the pause between the end of expiration and the start of inspiration is very short due to prolonged expiration caused by flow limitation. Both factors make clearance of the upper airways during NHF particularly difficult. Measurements from lung models suggest a stronger dead-space clearance effect when using AI, especially in advanced COPD, which could explain the differences between Pisani’s study and our results.22
Another physiological randomized controlled crossover study with AI was conducted in an intensive care setting. Twenty patients with hypoxemic respiratory failure in the post-extubation phase were enrolled. All patients received oxygen therapy via Venturi mask as baseline, followed by randomized NHF via AI or SI during the first 120 minutes after extubation. A reduction in MV and an increase in therapy comfort were reported in favor of AI, but no differences were found between the two interfaces regarding gas exchange or diaphragm thickening fraction.28 With respect to using diaphragm thickening fraction measured by ultrasound as a surrogate for inspiratory work of breathing, caution is warranted in the post-ventilation setting, since invasive ventilation can substantially affect diaphragm function and thickening fraction, even when the duration of ventilation is less than 36 hours.29
Numerous studies have described the physiological effects of NHF therapy in COPD patients, with largely consistent results. NHF has been shown to decrease RR, increase VT, reduce MV, and prolong expiratory time.30 In contrast to the present investigation, a physiological study in severe stable hypercapnic COPD patients using a similar experimental setup found that, apart from a significant reduction in MV, NHF did not reduce TcCO2 during the short-term daytime measurements, suggesting a different physiological response when hypercapnia has been present for a considerable period of time.15
A recent review found favourable physiological responses that support the use of NHF in acute state of COPD exacerbation, either as a viable alternative to NIV, during NIV breaks or post-extubation. The authors emphasized that NHF did not demonstrate increased failures rates, exhibited superior tolerance, and could serve as an alternative for patients intolerant to NIV.31
Patients with severe acute respiratory failure can tolerate NHF rates of up to 60 L/min; however, for longer-term support in chronic respiratory failure, clinical experience suggests that lower flow rates are better tolerated and may improve compliance.32 The enhanced respiratory support with AI at lower NHF settings in stable COPD patients may have clinically relevant effects, providing a potential rationale for future studies in this population.
Strengths and Limitations
The following aspects may limit the applicability of our work and should therefore be acknowledged. This was a pilot study with a limited number of severely ill patients and a short observation period, so no general recommendations regarding the choice of interface for NHF in this patient group can be derived. All patients were assessed during daytime and while awake. Since the effects of NHF therapy may differ during sleep in COPD patients, future studies are needed to investigate whether and how the effect of NHF with AI persist over longer periods and during sleep.33 The increased combined cross-sectional area of nasal prongs in AI reduces gas velocity, which may lower noise, but it also increases expiratory resistance due to the decreased leak area around the prongs. As a result, daytime and nighttime tolerance of NHF with AI may vary. Furthermore, mouth opening was not assessed during our measurements. It has been demonstrated that mouth opening can influence the pressures generated by NHF in the airways. Air leakage through an open mouth may reduce the generated pressure but could also decrease rebreathing.34 Methodological limitations also apply to electromyography of the intercostal muscles, as signal contamination from adjacent non-respiratory thoracic muscles cannot be excluded. Inter-individual variability in COPD patients may be greater than in healthy individuals, although still within an acceptable range.35,36 Finally, inspiratory muscle signal strength can vary with body position.37 However, this factor is unlikely to have influenced our results, since all patients were examined in a comparable semi-recumbent position. This study did not address the mechanisms underlying the observed reduction in MV during NHF with AI. The improvement could be attributed to both dead-space reduction and increased airway pressure, while the absence of an anticipated decrease in NRD during NHF highlights the need for further mechanistic research on non-invasive respiratory support. Comfort during NHF was not assessed systematically due to complex instrumentation; however, patients tolerated NHF well with both interfaces.
Conclusion
To maximize the benefits of respiratory support with NHF, it is essential to select both the optimal flow settings and the most appropriate cannula interface for each patient. The use of AI may enhance the physiological effects of NHF in patients with advanced COPD at a flow rate of 30 L/min, which was well tolerated in this cohort. However, it remains unclear whether and to what extent AI use influences other clinically relevant outcomes, such as exacerbation rates or the long-term management of chronic hypercapnia.
Data Sharing Statement
Individual deidentified participant data are not publicly available. The data underlying the results presented in this article may be made available upon reasonable request to the authors. Data will be available after publication for 5 years. Requests should be directed to the corresponding author.
Funding
This study received funding from Fisher & Paykel Healthcare, NZ. This has gone into department funds.
Disclosure
GN received financial support for this trial from Fisher & Paykel Healthcare, this has gone into department funds. ST is employee of Fisher & Paykel Healthcare; and reports US Patent No. 10569043 “Asymmetrical nasal delivery elements and fittings for nasal interfaces”. MK, UD, and MS declare no conflict of interest.
References
1. Agustí A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Eur Respir J. 2023;61(4):2300239. PMID: 36858443; PMCID: PMC10066569. doi:10.1183/13993003.00239-2023
2. Anzueto A, Miravitlles M. Pathophysiology of dyspnea in COPD. Postgrad Med. 2017;129(3):366–9. PMID: 28277858. doi:10.1080/00325481.2017.1301190
3. Calverley PM. Respiratory failure in chronic obstructive pulmonary disease. Eur Respir J Suppl. 2003;47:26s–30s. PMID: 14621114. doi:10.1183/09031936.03.00030103
4. Murphy PB, Rehal S, Arbane G, et al. Effect of home noninvasive ventilation with oxygen therapy vs oxygen therapy alone on hospital readmission or death after an acute COPD exacerbation: a randomized clinical trial. JAMA. 2017;317(21):2177–2186. doi:10.1001/jama.2017.4451
5. van der Leest S, Duiverman ML. High-intensity non-invasive ventilation in stable hypercapnic COPD: evidence of efficacy and practical advice. Respirology. 2019;24(4):318–328. doi:10.1111/resp.13450
6. Raveling T, Vonk J, Struik FM, et al. Chronic non-invasive ventilation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2021;8(8):CD002878. doi:10.1002/14651858.CD002878.pub3
7. Raveling T, Vonk JM, Hill NS, et al. Home noninvasive ventilation in severe COPD: in whom does it work and how? ERJ Open Res. 2024;10(1):00600–2023. doi:10.1183/23120541.00600-2023
8. Bonnevie T, Elkins M, Paumier C, et al. Nasal high flow for stable patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. COPD. 2019;16(5–6):368–377. doi:10.1080/15412555.2019.1672637
9. Nishimura M. High-flow nasal cannula oxygen therapy devices. Respir Care. 2019;64(6):735–742. PMID: 31110041. doi:10.4187/respcare.06718
10. Nishimura M. High-flow nasal cannula oxygen therapy in adults: physiological benefits, indication, clinical benefits, and adverse effects. Respir Care. 2016;61(4):529–541. PMID: 27016353. doi:10.4187/respcare.04577
11. Oczkowski S, Ergan B, Bos L, et al. ERS clinical practice guidelines: high-flow nasal cannula in acute respiratory failure. Eur Respir J. 2022;59(4):2101574. doi:10.1183/13993003.01574-2021
12. Bell N, Hutchinson CL, Green TC, et al. Randomised control trial of humidified high flow nasal cannulae versus standard oxygen in the emergency department. Emerg Med Australas. 2015;27(6):537–541. doi:10.1111/1742-6723.12490
13. Frat JP, Thille AW, Mercat A, et al; FLORALI Study Group; REVA Network. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med. 2015;372(23):2185–2196. doi:10.1056/NEJMoa1503326
14. Nagata K, Horie T, Chohnabayashi N, et al. Home high-flow nasal cannula oxygen therapy for stable hypercapnic COPD: a randomized clinical trial. Am J Respir Crit Care Med. 2022;206(11):1326–1335. doi:10.1164/rccm.202201-0199OC
15. Nilius G, Schroeder M, Domanski U, et al. Nocturnal respiratory support with nasal high flow in hypercapnic COPD: a randomised, crossover trial. ERJ Open Res. 2025;11(3):01063–2024. doi:10.1183/23120541.01063-2024
16. Yang H, Huang D, Luo J, et al. The use of high-flow nasal cannula in patients with chronic obstructive pulmonary disease under exacerbation and stable phases: a systematic review and meta-analysis. Heart Lung. 2023;60:116–126. doi:10.1016/j.hrtlng.2023.02.016
17. Pantazopoulos I, Boutlas S, Mavrovounis G, et al. Nasal high flow or noninvasive ventilation? Navigating hypercapnic COPD exacerbation treatment: a randomized noninferiority clinical trial. Respir Med. 2024;232:107762. doi:10.1016/j.rmed.2024.107762
18. Tan D, Wang B, Cao P, et al. High flow nasal cannula oxygen therapy versus non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease with acute-moderate hypercapnic respiratory failure: a randomized controlled non-inferiority trial. Crit Care. 2024;28(1):250. doi:10.1186/s13054-024-05040-9
19. Du Y, Zhang H, Ma Z, et al. High-flow nasal oxygen versus noninvasive ventilation in acute exacerbation of chronic obstructive pulmonary disease patients: a meta-analysis of randomized controlled trials. Can Respir J. 2023;2023:7707010. doi:10.1155/2023/7707010
20. Pintaudi G, Cutuli SL, Rosà T, et al. High-flow nasal oxygen in patients with acute hypercapnic respiratory failure: a narrative review of the physiological rationale and clinical evidence. J Clin Med. 2024;13(21):6350. doi:10.3390/jcm13216350
21. Bräunlich J, Mauersberger F, Wirtz H. Effectiveness of nasal highflow in hypercapnic COPD patients is flow and leakage dependent. BMC Pulm Med. 2018;18(1):14. doi:10.1186/s12890-018-0576-x
22. Pisani L, Vega ML, Ageno E, et al. Effects of asymmetric nasal high-flow cannula on carbon dioxide in hypercapnic patients: a randomised crossover physiological pilot study. Pulmonology. 2025;31(1):2411813. doi:10.1080/25310429.2024.2411813
23. Tatkov S, Rees M, Gulley A, et al. Asymmetrical nasal high flow ventilation improves clearance of CO2 from the anatomical dead space and increases positive airway pressure. J Appl Physiol. 2023;134(2):365–377. doi:10.1152/japplphysiol.00692.2022
24. Reilly CC, Jolley CJ, Elston C, et al. Measurement of parasternal intercostal electromyogram during an infective exacerbation in patients with cystic fibrosis. Eur Respir J. 2012;40(4):977–981. doi:10.1183/09031936.00163111
25. Wu W, Guan L, Li X, et al. Correlation and compatibility between surface respiratory electromyography and transesophageal diaphragmatic electromyography measurements during treadmill exercise in stable patients with COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:3273–3280. doi:10.2147/COPD.S148980
26. Vieira F, Rodrigues A, Schreiber A, et al. Comparing physiological effects of standard vs asymmetrical high-flow nasal cannula: a bench study. In: Canadian Critical Care Forum. Toronto, Canada; 2022.
27. Slobod D, Spinelli E, Crotti S, et al. Effects of an asymmetrical high flow nasal cannula interface in hypoxemic patients. Crit Care. 2023;27(1):145. doi:10.1186/s13054-023-04441-6
28. Boscolo A, Pettenuzzo T, Zarantonello F, et al. Asymmetrical high-flow nasal cannula performs similarly to standard interface in patients with acute hypoxemic post-extubation respiratory failure: a pilot study. BMC Pulm Med. 2024;24(1):21. doi:10.1186/s12890-023-02820-x
29. Goligher EC, Fan E, Herridge MS, et al. Evolution of diaphragm thickness during mechanical ventilation. Impact of inspiratory effort. Am J Respir Crit Care Med. 2015;192(9):1080–1088. doi:10.1164/rccm.201503-0620OC
30. Pinkham MI, Domanski U, Franke KJ, et al. Effect of respiratory rate and size of cannula on pressure and dead-space clearance during nasal high flow in patients with COPD and acute respiratory failure. J Appl Physiol. 2022;132(2):553–563. doi:10.1152/japplphysiol.00769.2021
31. Colaianni-Alfonso N, Herrera F, Flores D, et al. Physiological effects and clinical evidence of high-flow nasal cannula during acute exacerbation in COPD patients: a narrative review. J Intensive Med. 2024;5(2):127–133. doi:10.1016/j.jointm.2024.10.005
32. Smallwood N, Pascoe A, Buchan C, et al. A mixed-methods pilot study of domiciliary nasal high-flow therapy for breathlessness in people with chronic obstructive pulmonary disease who do not qualify for domiciliary long-term oxygen therapy. Ther Adv Respir Dis. 2025;19:17534666251314722. doi:10.1177/17534666251314722
33. Mündel T, Feng S, Tatkov S, et al. Mechanisms of nasal high flow on ventilation during wakefulness and sleep. J Appl Physiol. 2013;114(8):1058–1065. PMID: 23412897; PMCID: PMC3633436. doi:10.1152/japplphysiol.01308.2012
34. Vieira F, Bezerra FS, Coudroy R, et al. High flow nasal cannula compared to continuous positive airway pressure: a bench and physiological study. J Appl Physiol. 2022;132:1580–1590. doi:10.1152/japplphysiol.00416.2021
35. Luo YM, Moxham J, Polkey MI. Diaphragm electromyography using an oesophageal catheter: current concepts. Clin Sci. 2008;115(8):233–244. doi:10.1042/CS20070348
36. Murphy PB, Kumar A, Reilly C, et al. Neural respiratory drive as a physiological biomarker to monitor change during acute exacerbations of COPD. Thorax. 2011;66(7):602–608. doi:10.1136/thx.2010.151332
37. Wanke T, Lahrmann H, Formanek D, et al. Effect of posture on inspiratory muscle electromyogram response to hypercapnia. Eur J Appl Physiol Occup Physiol. 1992;64(3):266–271. PMID: 1563372. doi:10.1007/BF00626290
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.