Back to Journals » Risk Management and Healthcare Policy » Volume 19
Enhancing Medical Record Quality in Psychiatric Care Through PDCA Cycle Management
Authors Pan L
Received 12 February 2026
Accepted for publication 24 May 2026
Published 8 June 2026 Volume 2026:19 603196
DOI https://doi.org/10.2147/RMHP.S603196
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Keon-Hyung Lee
Li Pan
Medical Affairs Department, Wuhan Rongjunyoufu Hospital (Wuhan Third Psychiatric Hospital), Wuhan, 430023, People’s Republic of China
Correspondence: Li Pan, Medical Affairs Department, Wuhan Rongjunyoufu Hospital (Wuhan Third Psychiatric Hospital), No. 187, Development Avenue, Tangjia Deng Street, Jianghan District, Wuhan, 430023, People’s Republic of China, Tel +86-15387139729, Email [email protected]
Objective: To evaluate the effect of Plan-Do-Check-Act (PDCA) cycle management on psychiatric medical record quality.
Methods: This pre-post intervention study implemented PDCA from February 2023. A time-series analysis compared monthly Class A record rates (≥ 90% on a standardized checklist) across 12 months post-implementation (Feb 2023–Jan 2024). Using stratified random sampling by department, 150 records per group were selected: pre-intervention control (before 2023), observation group 1 (Feb 2023–Jan 2024, comprehensive review), and observation group 2 (Jan–Dec 2025, spot-check review). Fourteen ward physicians rated satisfaction pre- and post-intervention. Possible confounders (department, time) were addressed via stratified sampling and time-series segmentation. Statistical analyses included ANOVA with effect sizes (η2) for group comparisons and paired t-test with Cohen’s d for satisfaction scores.
Results: After implementation of the PDCA cycle, the monthly Class A record rate remained above 90% (range: 94.49– 98.48%). Statistically significant between‑month differences were observed at several time points (eg, April and September 2023, both p< 0.01). One‑way ANOVA indicated a statistically significant difference among the three groups (F=57.59, p< 0.01, η2=0.205). Quality scores were higher in both observation groups compared with the control group (observation group 1: 95.01± 2.44 vs control: 92.26± 3.58; observation group 2: 95.29± 1.79 vs control: 92.26± 3.58; both p< 0.01), whereas no significant difference was found between the two observation groups (p> 0.05). Physician satisfaction scores also showed a statistically significant increase (97.29± 2.09 vs 85.14± 4.35; t = − 12.02, p< 0.01, Cohen’s d = − 3.213). In the present study, the Class A rate was maintained above 90% and physician satisfaction was higher after PDCA implementation.
Conclusion: In this single‑center pre‑post study, implementation of the PDCA cycle was associated with improvements in medical record quality and physician satisfaction. Further research is needed to confirm these findings in other settings.
Keywords: medical quality, medical record quality, PDCA cycle management, quality control, quality management
Introduction
Medical record quality is a direct indicator of a healthcare institution’s management capacity and technical standards. It is critical for patient safety, legal documentation, hospital operations, medical insurance reimbursement, and medical education and research.1 Consequently, improving the quality of inpatient medical records is of both theoretical and practical importance.
The Plan–Do–Check–Act (PDCA) cycle is a widely recognized management model used across industries to support iterative quality improvement through four sequential phases: planning, execution, evaluation, and corrective action.2,3 For instance, in the context of medical record quality, if a hospital identifies that “course records are not completed within three days after discharge” as a common problem (Plan), it may implement targeted reminders and training for physicians (Do), then audit the next month’s records to measure the error rate (Check), and finally require corrective revisions before the next cycle (Act). Through repeated cycles, such a specific defect can be progressively reduced. However, most existing evidence on PDCA’s effectiveness in medical record management comes from general hospitals or specific clinical departments (eg, emergency, surgery, oncology).3–5 Psychiatric hospitals face unique documentation challenges, including subjective symptom description, legal issues related to patient autonomy and involuntary admission, and higher risks of missing or delayed entries due to heavy clinical workloads.6 To date, empirical data specifically evaluating PDCA cycle management for psychiatric medical records remain scarce. Moreover, previous studies often failed to distinguish PDCA from routine quality control (QC) – the latter typically involves periodic checks without a structured, closed-loop feedback mechanism – leading to overestimation of intervention effects.
In routine hospital practice, quality control of medical records is often limited to post-hoc sampling inspections by a medical records department, with inconsistent feedback and corrective actions. By contrast, PDCA cycle management integrates four iterative stages: identifying problems (Plan), implementing targeted training and workflow adjustments (Do), systematic review with quantifiable metrics (Check), and feeding results back to frontline clinicians for correction before the next cycle (Act). This closed-loop, continuous improvement mechanism is hypothesized to yield sustained gains in documentation quality.
Thus, the present study addresses the following research gap, whether PDCA cycle management can effectively improve medical record quality in a psychiatric hospital setting, where documentation standards are uniquely challenging. To test this, we designed a pre-post intervention study with three specific objectives: (1) to examine monthly changes in the Class A record rate (defined as ≥90% on a standardized checklist) over one year of PDCA implementation; (2) to compare medical record quality scores among three independent groups (pre-PDCA control, early post-PDCA comprehensive review, and later post-PDCA spot-check review); and (3) to assess physician satisfaction with medical record quality before and after PDCA implementation.
By situating our study within the broader international literature on continuous quality improvement (CQI)7,8 and addressing the specific documentation challenges of psychiatric care, we aim to provide empirical evidence that can inform quality management practices in mental health settings worldwide.
Data and Methods
PDCA Cycle Model for Medical Record Quality Control in the Study Hospital
- Plan: According to the Basic Norms for Writing Medical Records (Hubei Province Medical Institution Medical Record Writing Standards, 2025 Edition), a Class A medical record was defined as achieving a total score ≥90% on a standardized quality control checklist. The quantifiable target was to maintain the monthly Class A rate above 90% and to ensure complete and accurate uploading of the medical record front page.9 Submission of records within two days post-discharge was required to protect patients’ rights to access and copy their records.
- Do: A three-level quality control working group was established: departmental quality control, hospital-level quality control (comprehensive review by the medical records department’s dedicated quality control specialist, ie, the author), and hospital-level sampling quality control (monthly inspections by department directors). Training was provided to all physicians, particularly newly appointed physicians, covering psychiatric symptom documentation, legal knowledge, and completion of the medical record front page.
- Check: The quality control specialist conducted a complete census of all medical records submitted to the medical records department from February 1, 2023 to January 31, 2024. Each record was scored using a standardized checklist based on the Basic Norms for Writing Medical Records. The monthly proportion of records with point deductions and the monthly Class A rate were calculated. For the three-group comparative study, stratified random sampling by department was used to select 150 records per group (control, observation group 1, observation group 2). The hospital-level sampling inspections by department directors were not used in the quantitative analysis reported here.
- Act: Results of quality control reviews (including specific error types and point deductions) were communicated to each department monthly. Physicians were required to make timely revisions. Common issues were analyzed and corrective actions implemented before the next PDCA cycle.
Study Method
This was a pre‑post intervention study with three analytical components.
Component 1 (Time‑series Analysis)
All medical records filed from February 2023 to January 2024 were included. No inclusion or exclusion criteria were applied because this was not a human subject experiment; all records archived during this period were reviewed.
Component 2 (Three‑group Comparative Study)
Medical records were categorized into three temporal groups:
Control group: records completed before 2023 (pre‑PDCA).
Observation group 1: records filed from February 2023 to January 2024 that underwent comprehensive review by the quality control specialist under PDCA cycle management.
Observation group 2: records filed from January to December 2025 that were managed with PDCA but underwent spot‑check review (stratified sampling) by the same quality control specialist.
Sample size rationale: Based on national quality monitoring standards for medical records, a sample of 150 records per group is considered adequate to represent the overall quality level of the respective time period. This sample size also ensures sufficient statistical power for ANOVA and t-tests (assuming a moderate effect size, α = 0.05, power = 0.80).
Sampling method: The total number of medical records filed during the study period was 7456 for the 12 months from February 2023 to January 2024 (as shown in Table 1). From the control group (pre-PDCA, before 2023) to group 2 (January-December 2025), similar annual volumes were approximately 7500.
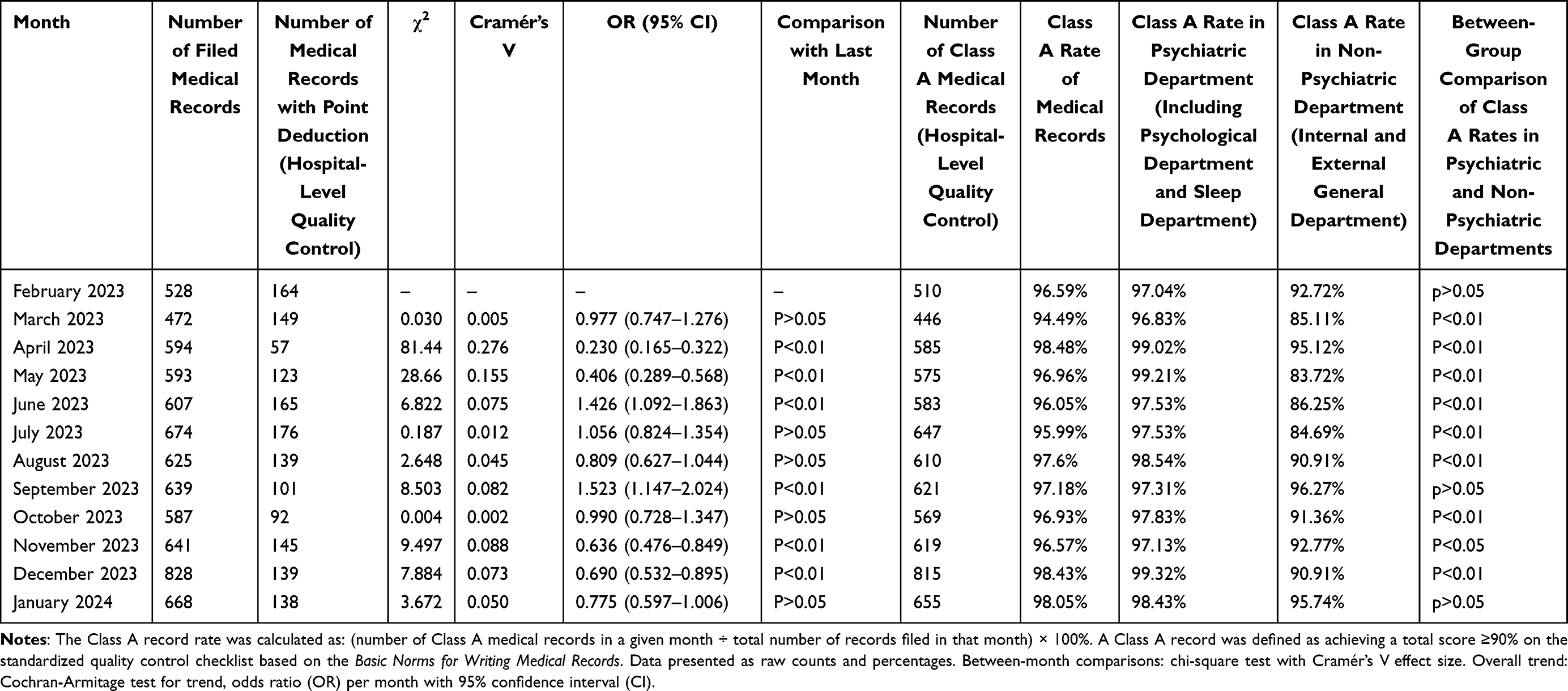 |
Table 1 Changes in the Class A Rate of Inpatient Medical Records After Implementation of PDCA Cycle Management |
Using stratified random sampling by department, 150 records were selected for each of the three groups. The stratification and sample allocation were as follows:
For the control group and observation group 1 (both during periods when the hospital had 10 psychiatric wards [including psychology, sleep medicine, and integrated traditional Chinese and Western medicine psychiatry], two general medical wards [internal medicine and surgery], and one rehabilitation ward):
10 psychiatric wards × 10 records each = 100
Internal medicine ward: 20 records
Surgery ward: 20 records
Rehabilitation ward: 10 records
Total = 150 records
For observation group 2 (January–December 2025, during which the rehabilitation ward was replaced by a newly established child and adolescent psychiatry ward):
10 psychiatric wards (including the new child and adolescent psychiatry ward) × 10 records each = 100
Internal medicine ward: 20 records
Surgery ward: 20 records
Child and adolescent psychiatry ward: 10 records
Total = 150 records
Within each department, records were randomly selected from all eligible inpatient records during the respective time period using a random number generator. This stratified approach ensured that the sample reflected the departmental distribution of the hospital’s patient population.
Sample size rationale (updated): A sample of 150 records per group represents approximately 2% of the annual total of about 7500 records. This sampling fraction is higher than routine quality control standards (eg, 1% for inpatient medication order reviews and 0.1% for outpatient prescriptions in typical Chinese hospital audits). Therefore, it provides a reasonable basis for statistical inference. Power analysis (assuming a moderate effect size, α=0.05, power=0.80) also supported a target sample size of at least 120 per group, making 150 adequate.
Component 3 (Physician Satisfaction Survey)
Fourteen quality control physicians (one from each inpatient ward) rated their satisfaction with medical record quality. Each physician provided two ratings: one for records completed before 2023 (control) and one for records completed after PDCA implementation (February 2023 onwards).
Measurement instrument: A single‑item numeric rating scale (0–100) was used, asking “How satisfied are you with the overall quality of medical records in your ward?” All ratings were signed and confirmed by the physicians. No formal scale validation was performed, as no validated satisfaction scale for medical record quality was available in the literature.
Potential common method bias: Because the same physicians provided both pre‑ and post‑implementation ratings using the same single‑item measure, common method variance cannot be excluded. However, the direction of change (post‑implementation scores were higher) and the magnitude of the difference are unlikely to be explained solely by such bias, especially given that the physicians were aware that their ratings would be used for quality improvement rather than individual performance evaluation. Nevertheless, this limitation is addressed in the Discussion.
Statistical Analysis Method
All statistical analyses were performed using SPSS software (version 26.0) and JASP software. The Class A record rate was calculated as: (number of Class A medical records in a given month ÷ total number of records filed in that month) × 100%. A Class A record was defined as achieving a total score ≥90% on the standardized quality control checklist based on the Basic Norms for Writing Medical Records.9
Assumption Testing for Parametric Tests
Before using parametric tests (ANOVA, t-test), we assessed the normality of the distribution of medical record quality scores within each group using the Shapiro–Wilk test (p > 0.05 indicating normality). Homogeneity of variances was tested using Levene’s test. If assumptions were violated, non‑parametric alternatives (Kruskal–Wallis test for ANOVA, Mann–Whitney U-test for t-test) would be reported; however, the assumptions were met for the present data.
Comparison Among Three Groups (Control, Observation Group 1, Observation Group 2)
Medical record quality scores (continuous data, expressed as mean±standard deviation) were compared using one‑way ANOVA, followed by post‑hoc pairwise comparisons with Bonferroni correction. Effect size (η2) was reported.
Comparison Between Two Time Points for Physician Satisfaction
Paired t-test was used to compare satisfaction scores before and after PDCA implementation, with Cohen’s d as the effect size.
Time‑series Analysis of Monthly Class A Rates
Monthly Class A rates were compared using chi‑square tests for independence between consecutive months. A p value < 0.05 was considered statistically significant for all analyses.
Ethical Considerations
This study involved retrospective review of medical records and anonymous physician satisfaction ratings. No patient identifying information was extracted. The study has been reviewed and approved by Ethics Committee of Wuhan Rongjunyoufu Hospital (No. 2025-012-01).
Results
Comparison of Medical Record Quality
Following implementation of PDCA cycle management, the monthly Class A rate consistently remained above 90% (range: 94.49–98.48%). Table 1 presents the monthly data.
Following implementation of PDCA cycle management, medical record quality demonstrated significant improvement in April and September 2023 (p < 0.01), with a period of fluctuation or plateau observed between these two time points. A further significant improvement was observed in December 2023 (p < 0.01), and medical record quality remained stable at a high level in January 2024 compared with December 2023 (p > 0.05).
Psychiatric department records consistently achieved higher Class A rates (range: 96.83–99.32%) compared with non‑psychiatric departments (range: 83.72–96.27%). Between‑group comparisons (psychiatric vs non‑psychiatric) are shown in Table 1. Most months showed statistically significant differences (p < 0.01 or p < 0.05), with the psychiatric department outperforming others. However, by December 2023 and January 2024, the non‑psychiatric departments also achieved Class A rates above 90% (90.91% and 95.74%, respectively), and the difference between department types was no longer significant in September 2023 (p > 0.05) and January 2024 (p > 0.05).
Comparison of Writing Norms for Medical Records
Using stratified random sampling by department, 150 records were selected from each group: control (pre-PDCA), observation group 1 (Feb 2023–Jan 2024, comprehensive review), and observation group 2 (Jan–Dec 2025, spot-check review). Table 2 presents the mean scores, standard deviations, and 95% confidence intervals for each group.
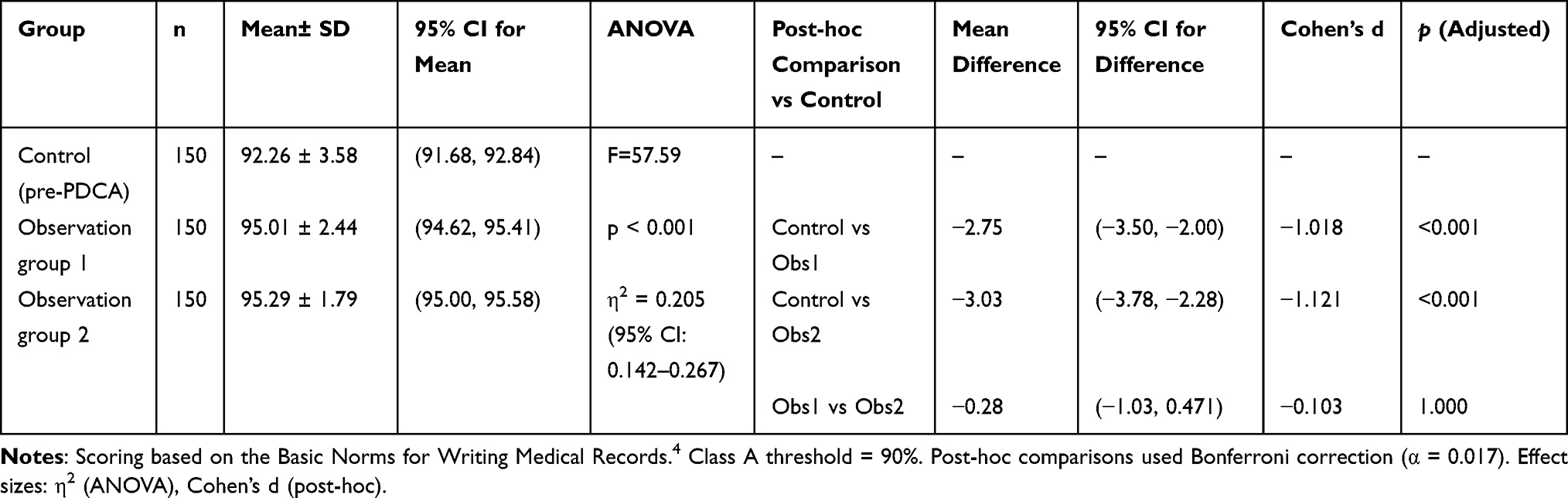 |
Table 2 Comparison of Medical Record Quality Scores Among Three Groups |
A statistically significant difference was found among the three groups (F = 57.59, p < 0.01, η2 = 0.205, 95% CI for η2: 0.142–0.267). Post-hoc pairwise comparisons using Bonferroni correction showed that both observation groups had significantly higher quality scores than the control group, with large effect sizes. No significant difference was found between observation group 1 and observation group 2, indicating sustained improvement over time. Detailed post-hoc results are provided in Table 2.
Figure 1 displays the mean quality scores with standard deviation error bars for the three groups. The plot visually confirms the higher scores and reduced variability in both observation groups compared with the control group.
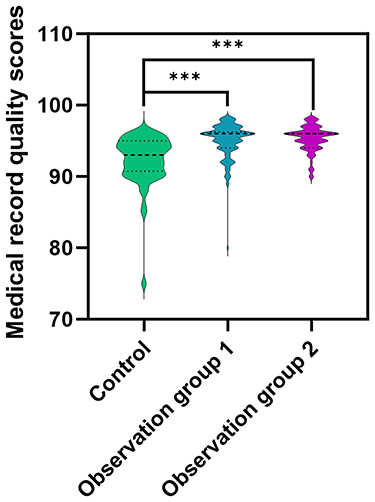 |
Figure 1 Comparison of medical record quality scores among three groups. ***P<0.05 vs control. |
Doctors’ Satisfaction with Medical Record Quality
Satisfaction with medical record quality was assessed by 14 quality control physicians from each inpatient ward for medical records completed before 2023 (control group) and for medical records managed using the PDCA cycle after February 2023 (observation group). As presented in Table 3, satisfaction among quality control physicians was higher after the implementation of PDCA cycle management.
 |
Table 3 Comparison of Satisfaction with Medical Record Quality Among Ward-Based Quality Control Physicians Before and After PDCA Cycle Management |
Discussion
This study evaluated the effect of PDCA cycle management on medical record quality in a psychiatric hospital. The key findings are: (1) after PDCA implementation, the monthly Class A record rate consistently exceeded 90%, with significant improvements at multiple time points; (2) PDCA significantly increased objective quality scores and physician satisfaction; and (3) the improvement was sustained over time, with no significant difference between comprehensive review (observation group 1) and spot‑check review (observation group 2).
Comparison with Existing Literature
The observed trends in our study are broadly consistent with previous reports that found positive associations between PDCA implementation and quality metrics.4,5 For example, Chen et al4 reported that PDCA cycle management improved the timeliness of electronic medical record documentation among resident physicians. Similarly, Zhang et al5 found that PDSA (a variant of PDCA) enhanced the accuracy of primary diagnosis documentation on medical record front pages. However, most prior evidence comes from general hospitals or specific clinical departments (eg, emergency, surgery, oncology). To our knowledge, this is one of the first studies to apply PDCA specifically to psychiatric medical records-a setting with unique documentation challenges, including subjective symptom description, legal issues related to involuntary admission, and high clinical workload.5
Compared with routine quality control, our PDCA intervention achieved a large effect size (η2 = 0.205), meaning that the variance in medical record quality scores was explained by the intervention. This is considerably higher than effect sizes reported in some non‑PDCA quality improvement studies in medical records,10 suggesting that the closed‑loop, iterative nature of PDCA may be more effective than one‑time audits.
The very large effect size for physician satisfaction indicates that frontline clinicians perceived substantial improvements in record quality. This is clinically meaningful because physician buy‑in is critical for sustained quality improvement.11 The magnitude of this effect likely reflects that PDCA not only improved objective metrics but also reduced documentation burden and error‑related rework, thereby enhancing user experience.
Mechanisms Linking PDCA to Improved Documentation Behaviour
The observed improvements can be attributed to several interconnected mechanisms.
Unlike routine QC, which often ends with error identification, PDCA’s “Act” phase required physicians to correct errors within 3 days and to avoid repeated point deductions. This created a clear accountability loop. The significant reduction in point‑deduction rates (eg, from 164 in February 2023 to 57 in April 2023) suggests that feedback alone was insufficient; the requirement for timely correction drove behavior change.
The cyclical nature of PDCA (monthly cycles) provided repeated opportunities for learning and reinforcement. Errors that persisted in one cycle were targeted in the next, leading to progressive reduction of common problems (eg, missing signatures, delayed course records). This aligns with behavioral learning theory, where spaced repetition and corrective feedback strengthen desired behaviors.7
The “Do” phase included structured training on psychiatric symptom documentation and legal requirements. By standardizing expectations, PDCA reduced variability among physicians. The finding that non‑psychiatric departments (which initially had lower Class A rates, eg, 83.72% in May 2023) eventually achieved rates above 90% by December 2023 supports the role of training and standardization.
Initially, physicians may have changed behavior simply because they knew they were being monitored (Hawthorne effect). However, the sustained improvement from observation group 1 (comprehensive review) to observation group 2 (spot‑check review, 1.5 years later) with no significant decay (p = 0.47) suggests that genuine learning and habit formation occurred, rather than a temporary response to observation.
Limitations
Several limitations should be acknowledged.
The study was conducted at one psychiatric hospital in China. Findings may not be generalizable to other settings (eg, general hospitals, outpatient psychiatry, or different healthcare systems). Replication in multiple centers is needed.
Grouping records by calendar time may introduce bias from unmeasured temporal factors (eg, changes in hospital policy, seasonal patient acuity, physician turnover). Although stratified random sampling by department mitigated some confounding, we cannot rule out time‑related confounders. The lack of a concurrent control group (eg, a ward not receiving PDCA) limits causal inference.
The quality control specialist (author) who performed the complete census and scored the records was not blinded to the time period. This introduces potential bias, although the use of a standardized checklist (based on national guidelines) reduces but does not eliminate subjectivity. Future studies should use blinded independent assessors.
Satisfaction was assessed using a non‑validated single‑item scale completed by the same physicians before and after the intervention. This introduces potential common method bias, as the physicians’ post‑intervention ratings might be influenced by their recollection of pre‑intervention ratings or by a desire to show improvement. Although the large effect size and the fact that ratings were signed and used only for quality improvement (not performance evaluation) mitigate this concern to some extent, the lack of a validated multidimensional instrument and the absence of blinding remain important limitations. Future studies should consider using validated scales and collecting independent ratings from multiple sources (eg, external auditors).
The chi‑square tests for monthly comparisons involved 11 pairwise tests. Although we reported p < 0.01 as significant, we did not apply a Bonferroni correction for these exploratory analyses. The pattern of significant improvements at multiple time points, however, is unlikely to be due entirely to chance.
The study hospital had a dedicated quality control specialist (the author) who performed comprehensive reviews. Hospitals without such resources may achieve different results. The effectiveness of PDCA may depend on staffing, training, and institutional support.
While stratified random sampling by department ensured proportional representation, the total sample of 150 records per group (2% of annual volume) may still miss rare but critical documentation errors. However, this sampling fraction exceeds routine quality control benchmarks in Chinese hospitals, and the consistency of findings across three independent groups supports the robustness of the results.
Implications for Healthcare Quality Management
Despite these limitations, our findings have several practical implications.
PDCA cycle management is feasible and effective for improving medical record quality, even in settings with complex documentation requirements (eg, subjective symptom descriptions, legal documentation for involuntary patients). The sustained improvement with spot‑check review suggests that after initial intensive cycles, a lighter monitoring touch may suffice. The mechanisms identified (closed‑loop feedback, behavioral reinforcement, standardization) are not unique to psychiatric records. PDCA could be applied to other documentation challenges (eg, electronic health record completeness, discharge summary timeliness) across various departments.
The finding that observation group 2 (spot‑check review) achieved equivalent quality to comprehensive review (observation group 1) suggests that once baseline quality is established, intermittent sampling may be cost‑effective. Hospitals with limited quality control personnel could consider a phased approach: initial comprehensive PDCA cycles followed by reduced monitoring. Medical record quality is a key indicator in hospital accreditation (eg, in China, JCI, ISO). Our results support the inclusion of PDCA‑based continuous quality improvement as a standard requirement for medical record management.
Conclusion
In this single‑center pre‑post study, implementation of the PDCA cycle was observed in parallel with improvements in medical record quality and physician satisfaction scores. For example, through iterative PDCA cycles, the common problem of delayed medical records was substantially reduced. These preliminary findings from a single center suggest that further research on PDCA as a quality improvement tool for psychiatric medical records is warranted.
Abbreviations
PDCA, Plan-do-check-act; CQI, Continuous Quality Improvement; DRG, Diagnosis Related Groups.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Wuhan Rongjunyoufu Hospital (No. 2025-012-01). This study was conducted in accordance with the declaration of Helsinki. Due to the retrospective nature of the study, the requirement of patient consent for inclusion was waived by Ethics Committee of Wuhan Rongjunyoufu Hospital. No patient identifying information was extracted.
Acknowledgments
The author would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
No external funding received to conduct this study.
Disclosure
The author declares no competing interests in this work.
References
1. Albano GD, Bertozzi G, Maglietta F, et al. Medical records quality as prevention tool for Healthcare-Associated Infections (HAIs) related litigation: a case series. Curr Pharm Biotechnol. 2019;20(8):653–10. doi:10.2174/1389201020666190408102221
2. Gu S, Zhang A, Huo G, et al. Application of PDCA cycle management for postgraduate medical students during the COVID-19 pandemic. BMC Med Educ. 2021;21(1):308. doi:10.1186/s12909-021-02740-6
3. Zeng X, Huang X, Wang P, et al. The application of the PDCA cycle in the nutritional management of patients with nasopharyngeal carcinoma. Support Care Cancer. 2023;31(5):251. doi:10.1007/s00520-023-07724-4
4. Chen J, Li Z, Ma W, et al. Enhancing the timeliness of EMR documentation in resident doctors: the role of PDCA cycle management. BMC Med Educ. 2024;24(1):1367. doi:10.1186/s12909-024-06134-2
5. Zhang LP, Liu HH, Chen WP. Application effectiveness of PDSA cycle management in filling out the primary diagnosis on hospitalized patient case summaries. Chin Med Record. 2025;26(3):5–7.
6. Williams F, Boren SA. The role of the electronic medical record (EMR) in care delivery development in developing countries: a systematic review. Inform Prim Care. 2008;16(2):139–145. doi:10.14236/jhi.v16i2.685
7. Moyce S, Claudio D, Velazquez M. Using the PDCA cycle to uncover sources of mental health disparities for Hispanics. Int J Ment Health Nurs. 2023;32(2):556–566. doi:10.1111/inm.13100
8. Bonsel JM, Itiola AJ, Huberts AS, et al. The use of patient-reported outcome measures to improve patient-related outcomes - a systematic review. Health Qual Life Outcomes. 2024;22(1):101. doi:10.1186/s12955-024-02312-4
9. He Y, Li D, Yang Q, et al. Hubei Province Medical Institution Medical Record Writing Standards (2025 Edition).
10. Yuan B, Song S, Tang X, et al. Application of multidimensional quality management tools in the management of medical adverse events. Risk Manag Healthc Policy. 2024;17:91–99. doi:10.2147/RMHP.S436083
11. Qin QH. Practical application of the PDCA method to improve the quality of inpatient medical record front pages. Chin Med Record. 2025;26(11):17–19.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.