Back to Journals » Advances in Medical Education and Practice » Volume 16
Enhancing Maternal ACLS Training: Evaluating the Effectiveness of a Modified Peyton’s Four-Step Teaching Approach
Authors Zhang X, Sun Z ![]() , Lan Q, Xu M
, Lan Q, Xu M ![]() , Guo X, Wei B
, Guo X, Wei B
Received 23 May 2025
Accepted for publication 6 September 2025
Published 10 October 2025 Volume 2025:16 Pages 1837—1845
DOI https://doi.org/10.2147/AMEP.S542286
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Xiaoqing Zhang,* Zhuonan Sun,* Qiong Lan, Mao Xu, Xiangyang Guo, Bin Wei
Department of Anesthesiology, Peking University Third Hospital, Beijing, 100191, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Wei, Email [email protected]
Purpose: Maternal Advanced Cardiovascular Life Support (ACLS) training is crucial for effective maternal cardiopulmonary resuscitation education. Traditional lecture-based approach for maternal cardiopulmonary resuscitation falls short in providing opportunities for adequate practice and active participating. Peyton’s four-step teaching method shows advantages in the acquisition of procedural skills. Its effectiveness is constrained in group settings due to the 1:1 teacher-student ratio requirement. This study aims to evaluate the effectiveness of a modified Peyton’s four-step teaching method in maternal ACLS training, with the objective of optimizing clinical training strategies.
Methods: Sixty physicians participating in ACLS training at our hospital from October 2023 to December 2024 were enrolled and randomly divided into an experimental group (n = 30) and a control group (n = 30). The experimental group received the modified Peyton’s four-step teaching method, while the control group underwent traditional lecture-based training. Teaching effectiveness was compared through knowledge assessments, skill evaluations, and feedback questionnaires.
Results: No significant difference was observed in knowledge scores between the two groups (experimental group: 94.6 ± 4.1 vs control group: 94.3 ± 3.9, P > 0.05). However, the experimental group demonstrated significantly higher accuracy in skill operations, including uterine displacement maneuvers, peripartum cesarean section decision-making, defibrillation, and resuscitation drug administration (P < 0.05). Teamwork performance and adherence to maternal cardiac arrest (CA) protocols were also superior in the experimental group (P < 0.05). Questionnaire results indicated higher satisfaction (4.5 ± 0.7 vs 4.1 ± 0.5, P < 0.05) and greater learning engagement (4.5± 0.6 vs 4.0± 0.6, P < 0.05) in the experimental group.
Conclusion: The modified Peyton’s four-step teaching method significantly enhances physicians’ mastery of maternal ACLS skills, improves teamwork capabilities, and elevates both teaching quality and learner satisfaction.
Keywords: Peyton’s four-step teaching method, cardiac arrest, maternal, advanced cardiovascular life support, physician
Cardiac arrest (CA), defined as the abrupt cessation of effective cardiac pumping function, represents a critical medical emergency necessitating immediate intervention.1 Maternal CA, a particularly high-risk event in obstetrics, emergency medicine, and critical care, presents distinct challenges due to its multifaceted etiologies (eg, obstetric hemorrhage, preeclampsia, amniotic fluid embolism, and anesthesia-related complications), the need for timely interventions, and dual maternal-fetal resuscitation demands.2 The increasing prevalence of advanced maternal age and pregnancy-related complications further complicates the management of maternal CA. However, the infrequency of these high-stakes scenarios and the limited training opportunities available to junior physicians impede the development of essential crisis management competencies. Traditional lecture-based training for maternal CA often lacks adequately incorporate content tailored to the specific physiological needs of this population, such as techniques for alleviating inferior vena cava compression through leftward uterine displacement and considerations for cesarean delivery during the perimortem period. This oversight leads to a significant gap between training and clinical practice.3 Consequently, the implementation of simulation-based education and standardized training protocols is crucial to bridging the gap between knowledge and practical application.4 The Peyton’s four-step teaching method, initially introduced by Walker and Peyton,5 is widely employed in medical skills education and shows significant advantages in acquisition of procedural skills.5,6 It is a stepwise teaching approach and consists of the following four steps: (i) step 1 refers to the demonstration of the whole procedure in real time (“demonstration”); (ii) in step 2 the teacher repeats the demonstration but this time all procedural sub-steps are described (“deconstruction”); (iii) during step 3 the student talks the teacher through the procedure. The teacher performs the procedure under the guidance of the student (“comprehension”) and (iv) in step 4 the students carry out the procedure on their own initiative (“performance”).
The traditional Peyton’s four-step method is characterized by its personalized approach, typically involving a teacher-student ratio of 1:1.5 However, achieving this ratio is challenging in medical skills training courses and clinical instructions, where typically in group learning format involving 4 to 8 participants. This discrepancy has led to the development of multiple modified versions of Peyton’s four-step teaching method, which incorporates a guidance-performance step between students within groups.7 Notably, the modified Peyton’s four-step teaching method has gained widespread endorsement as a recommended instructional strategy for advanced life support courses by the European Society of Cardiology and the European Resuscitation Council. Notably, this modified approach has received widespread endorsement as a recommended instructional strategy for advanced life support courses by both the European Society of Cardiology and the European Resuscitation Council.8
However, there was no study on the modified Peyton’s four step teaching method in maternal Advanced Cardiovascular Life Support (ACLS) training. In this study, we modified the Peyton’s approach in step 1 and 3 in order to facilitate its application within a group learning context. In the first step, a standard video demonstration was used. In the third step, rather than having the instructor perform under the guidance of the student, trainees were organized into pairs, with one member guide while the other perform. In light of the emphasis on teamwork within ACLS, we deliberately structured groups to comprise six individuals, which is the minimum number required for an ACLS team. This configuration was designed to facilitate mutual assistant learning and team member relationship between trainees during step 3. Consequently, during team collaboration training session, participants were anticipated to develop a heightened sense of teamwork, ultimately enhancing their performance outcomes. This study aims to evaluate the effectiveness of the modified Peyton’s four-step teaching method in maternal ACLS training, aiming to optimize clinical training strategies.
Materials and Methods
This study adhered to the guidelines outlined in the Helsinki Declaration (2013) and was approved by the ethics committee of Peking University Third Hospital (Grant number M2025170). All participants signed informed consents of investigation prior to their inclusion in the study.
Participants
Our hospital organizes ACLS training sessions annually. Registered physicians are required to participate in ACLS training every two years and may apply for the training at their convenient time. Physicians applied for ACLS training at our hospital from October 2023 to December 2024 were recruited. The exclusion criteria included physical conditions unsuitable for high-intensity motion (chest compression, uterine displacement), such as pregnancy or forearm fractures. Baseline data, including age, gender, specialty, professional experience, were collected. In our hospital, resident physicians are mandated to advance to the position of attending physicians within six years of clinical internship. Therefore, in this study, the professional experience quantified using the following variables: professional title, prior ACLS training experience, and CA management experience.
Study Design
This study was conducted in accordance with the Declaration of Helsinki. Every 6 physicians were randomly assigned to form a team and each team was randomly allocated to either the experimental or the control group, using a random number table. The experimental group was instructed using the modified Peyton’s method, while the control group received traditional didactic training. All instructional sessions were facilitated by a single instructor (B.W) certified by the American Heart Association (AHA).
Implementation
The training was implemented in a simulated scenario center, comprising 8-hour sessions focusing on maternal CA protocols. These sessions were standardized according to the AHA maternal CA rescue guidelines.9
There are six sessions, including: high-quality basic life support, electrical defibrillation, advanced airway, medicine administration, decision-making for peripartum cesarean section, and effective teamwork. Each session allocated one hour, with the left two hours reserved for systematic assessment.9 The instruction steps in the control and experiment group in every session were showed as follows:
Instruction Steps in the Control Group
Traditional teaching methods were adopted. Prior to the training sessions, the instructor familiarized himself with the rescue process of Maternal CA. The instructional procedures are outlined as follows:
First step. Video instruction. Instructors presented a standard ACLS teaching video and incorporate interactive questions and answers.
Second step. Deconstruction. The instructor conducted a deconstruction and step-by-step demonstration. The operational process adhered to the established protocol, detailing specific requirements and precautions. Trainees were encouraged to express their opinions, guided to pose questions, analyze problems, and develop solutions. Targeted examples, elaborations, expansions, and summaries were subsequently provided.
Third step. Independent practice. The trainees were allowed to practice on manikins concurrently while receiving demonstration and also after the demonstration of each step. The instructor monitored the practice after demonstration and addressed any questions.
Fourth step. Skill assessment. Standard evaluations were conducted following the training sessions. Trainees were required to take a paper-based exam on the knowledge framework and perform the ACLS procedures. Instructors assessing their performance, providing commentary on the operational process, and addressing any questions.
Instruction Steps in the Experimental Group
The experimental group was instructed using the modified Peyton teaching method. Prior to the training sessions, the instructor acquainted himself with the knowledge framework and implementation plan of the modified Peyton four-step teaching method. The video instruction, demonstration and the assessment section (the first, second and fourth steps) were consistent with those in the experimental group. The teaching process was structured as follows:
First step: The same with the first step of the control group.
Second step: The same with the second step of the control group.
Third step: Peer-guided practice in pairs. A structured training protocol involving three rounds of guided demonstration between trainees was implemented in the 6-participants team. During each round, trainees were divided into 3 pairs, with one member of each pair verbally articulating the operational steps while the other demonstrated them. The remaining 4 participants observed the process, provided feedback on deviations from the standard procedure, documented any existing issues, and rotated roles to ensure comprehensive training. During each session, every trainee assumed the role of either a guide or a demonstrator once, and served as an observer twice. Instructors played a crucial role in facilitating problem identification during training and ensured active participation from all trainees.
Fourth step: The same with the fourth step of the control group.
Evaluation of Instruction Effectiveness
Following the instructional session and group learning activities, the physicians proceeded to the testing room for evaluation. The assessment of instructional effectiveness was conducted by the teaching assistant (Z. S.), who was blinded to the group assignments.
Knowledge Assessment by Examination
After the training, both groups of physicians underwent tests on their knowledge of ACLS instruction using AHA standardized ACLS examination. The examination comprised 50 standard multiple-choice questions, with a maximum score of 100 points, and was administered in a paper-based format.
Clinical Skill Assessment
ACLS Megacode testing scenario was applied with a high-fidelity simulation manikin. ACLS megacode examinations are standard ACLS tests stimulated scenarios endorsed by the American Heart Association. For this study, we create a maternal CA scenario derived on the cardiac arrest scenario of the Megacode testing scenarios. The scoring criteria of the clinical evaluation were derived from the standard Megacode scenario testing checklist, with modifications to address maternal CA (Table 1). The 8 dimensions of the variable “Teamwork” (explained in Table 2) were assessed using a 5-point Likert scale.7 The scale ranges with strongly agree, agree, not sure, disagree, strongly disagree, scored as 5,4,3,2 and 1, separately. For variables other than Teamwork, physicians conduct all the accuracy was compared between the 2 groups using Chi-square test. The evaluation criteria include:
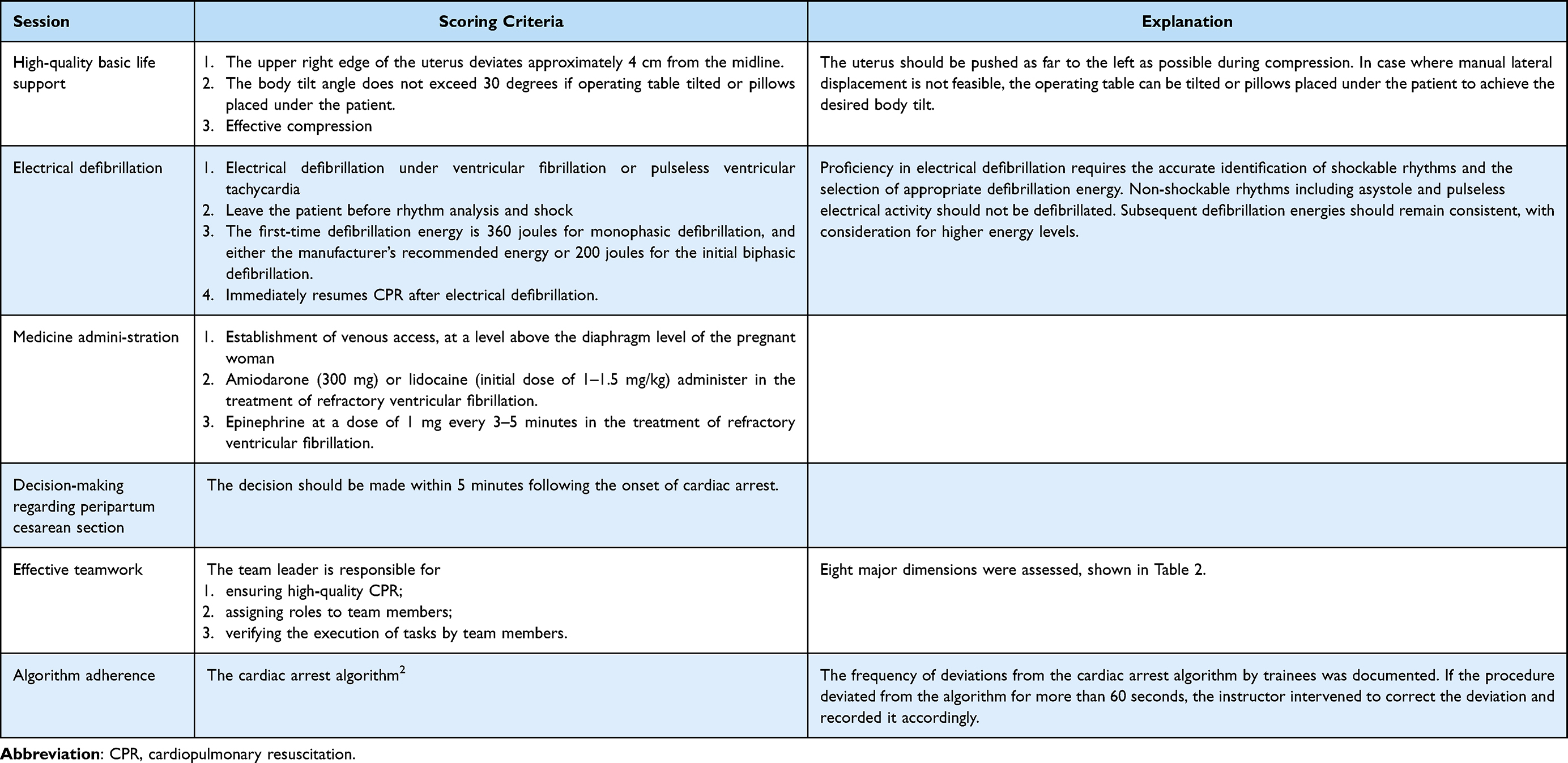 |
Table 1 The Clinical Skill Evaluation Criteria |
 |
Table 2 Dimensions of Teamwork Assessment |
Questionnaire Survey
Following the evaluation of instruction effectiveness, all physicians participated in a questionnaire survey. Two questions were asked: (1) To what extent, do you agree with the following statement: I am satisfied with the instruction; (2) To what extent, do you agree with the following statement: the teaching method can stimulate my interest in learning maternal ACLS. 5-scale Likert scale was used for evaluation.
Statistical Analysis
All data were analyzed using SPSS 25.0 software. For measurement data conforming to a normal distribution, the mean ± standard deviation ( ) was used for description, and the independent sample t-test was employed for comparison. For measurement data not conforming to a normal distribution, the median along with the interquartile range (25th percentile, 75th percentile) [Median (P25, P75)] was utilized for descriptive purposes. The Mann–Whitney U-test was applied to assess differences between groups. Categorical data were described using frequencies and percentages [n(%)], with group differences evaluated using the chi-square test or Fisher’s exact test. A P-value of less than 0.05 was considered indicative of statistical significance.
) was used for description, and the independent sample t-test was employed for comparison. For measurement data not conforming to a normal distribution, the median along with the interquartile range (25th percentile, 75th percentile) [Median (P25, P75)] was utilized for descriptive purposes. The Mann–Whitney U-test was applied to assess differences between groups. Categorical data were described using frequencies and percentages [n(%)], with group differences evaluated using the chi-square test or Fisher’s exact test. A P-value of less than 0.05 was considered indicative of statistical significance.
Results
Baseline Characteristics
Sixty physicians were enrolled in this study, 30 physicians in each group. No statistical significances were identified between the two groups of physicians regarding age, gender, secondary specialties, professional titles, or prior experience in defibrillation and ACLS training, indicating a comparable baseline characteristic between the two groups. Detailed results are presented in Table 3.
 |
Table 3 Comparison of Baseline Characteristics of Physicians in the Two Groups [n (%)] |
Knowledge Test Scores
Statistical analysis revealed no significant difference (P = 0.798) in knowledge test scores between the experimental group (94.6 ± 4.1) and the control group (94.3 ± 3.9).
Clinical Skill Operation Test Scores
In the skill operation test, the experimental group achieved a 96.7% accuracy rate in establishing venous access above the diaphragm level, compared to 93.3% in the control group. This difference was not statistically significant (P > 0.05). However, the experimental group significantly outperformed the control group in the correct application of the uterine lateral displacement technique with accuracy rates of 93.3% versus 70.0%, and in decision-making for cesarean sections during the peri-mortem period, with accuracy rates of 100.0% versus 70.0% (both P < 0.05). Furthermore, the experimental group demonstrated a significantly higher total score in team collaboration compared to the control group (38.5 ± 1.2 vs 31.8 ± 2.1, P < 0.05). Additionally, the experimental group exhibited superior performance in defibrillation operations, with accuracy rates of 86.7% vs 63.3%, and in the rational administration of resuscitation drugs, with accuracy rates of 96.7% vs 73.3% (both P < 0.05). Furthermore, the experimental group showed fewer deviations from the standard CA procedure than the control group [0.0 (0.0, 0.0) vs 0.0 (0.0, 1.0), P < 0.05]. Detailed results are presented in Table 4.
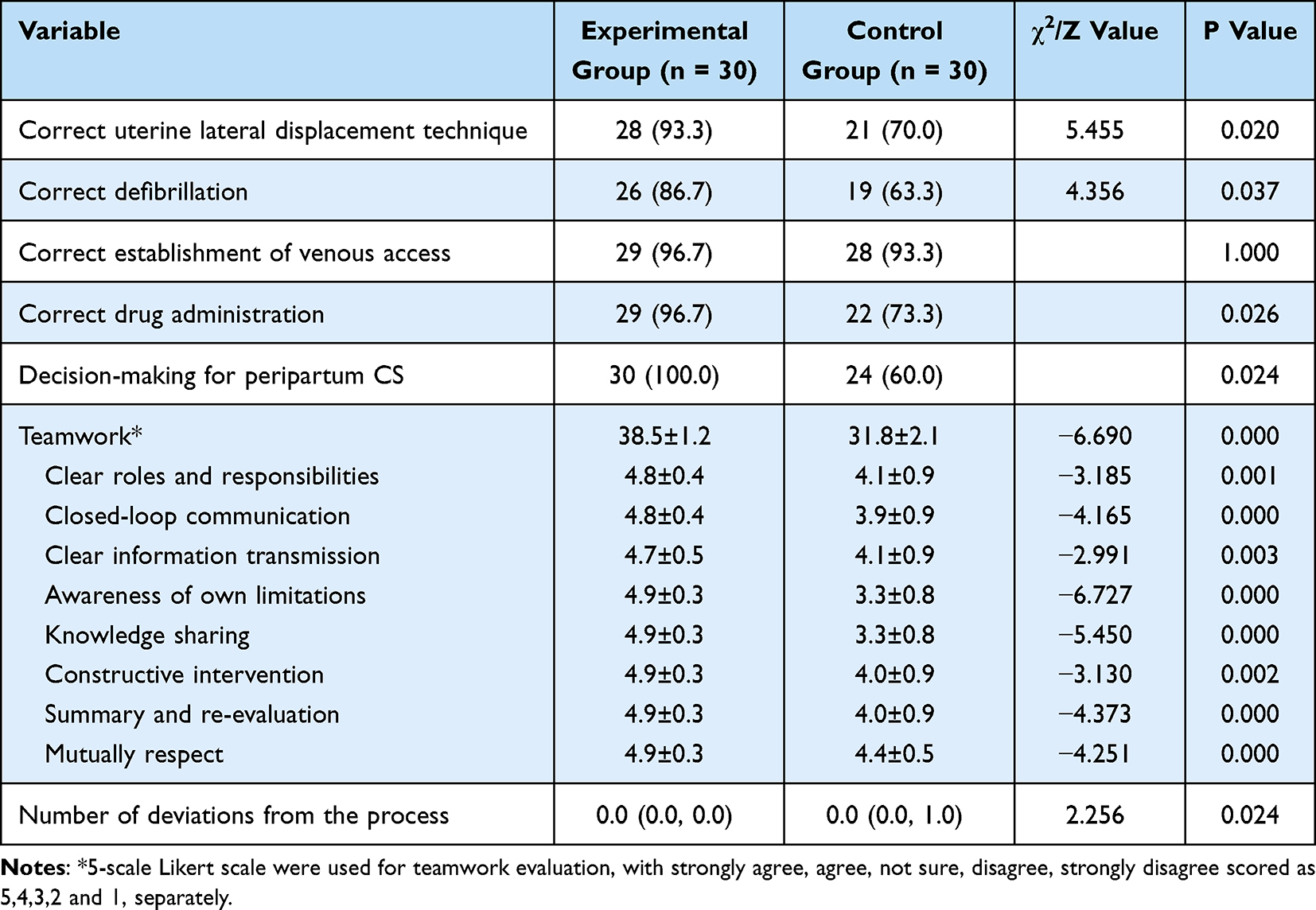 |
Table 4 Comparison of Skill Assessment Scores Between the Two Groups [n (%)] |
Questionnaires
A total of 60 questionnaires were distributed in this study with a valid response rate of 100.0%. The level of interest in learning among physicians in the experimental group was significantly higher than that in the control group, with all differences reaching statistical significance (P < 0.05). Detailed results are presented in Table 5.
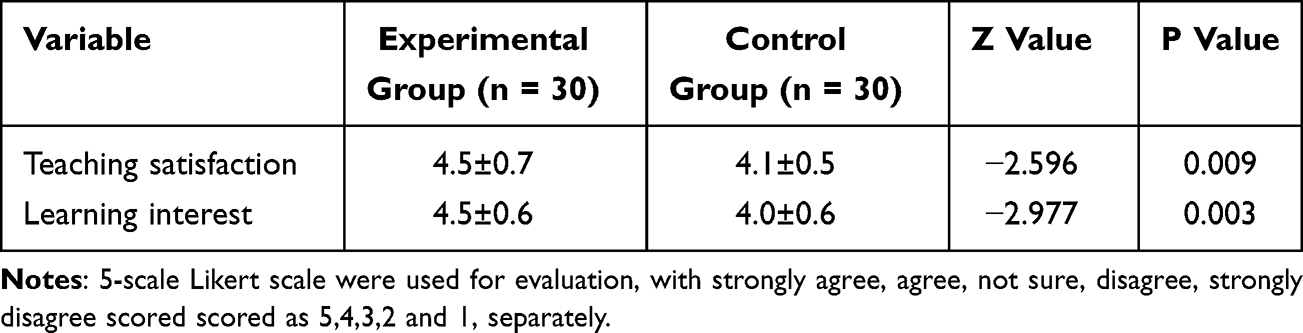 |
Table 5 Comparison of Questionnaire Survey Results Between the Two Groups |
Discussion
This study demonstrated that the modified Peyton four-step teaching method significantly enhanced skill operation levels, team collaboration efficiency, and process compliance in maternal ACLS training, compared to the traditional lecture method. Additionally, this approach garnered higher evaluations of teaching satisfaction. These findings offer innovative solutions to address critical challenges in current emergency training for this demographic. The superiority of this method can be attributed to two key dimensions: its adaptability to the unique characteristics of the obstetric specialty and the self-reflection of clinical skills deficiencies comparing to the traditional teaching methodologies.
Specialized training in ACLS tailored for pregnant and postpartum women can enhance trainees’ understanding of the critical and complex aspects specific to this demographic, such as the left uterine displacement technique. The AHA guidelines highlighted that in the ACLS training when maternal ACLS training is only conducted as one scenario session, participants were unable to accurately integrate the left uterine displacement technique with chest compressions during simulation exercises focused on ACLS for pregnant and postpartum women.9 This emphasized the specialized training for maternal ACLS.
In our point of view, the primary advantage of the modified Peyton’s four-step teaching method is the facilitation of peer assistance and mutual learning. During the third step of each session, groups of six participants were divided into three pairs, with one physician demonstrating a procedure under the guidance of the other, while the remaining four participants observed and provided feedback. Three rounds were conducted during the third step, ensuring that each physician assumed the roles of guider/demonstrator once and observer twice. According to Van Diggle’s peer teaching theory10,11 and Ericsson’s deliberate practice theory,12,13 when observing peers’ operations and identify differences and deficiencies, trainees may spontaneously activate their self-error monitoring and self-correction mechanism. Therefore, this structure facilitates self-reflection on personal skill deficiencies during identifying others’ oversights or errors. Furthermore, this format fosters motivation and interest through healthy competition between pairs within the group and enhances memorization. Consequently, the self-reflection of clinical skills deficiencies is a notable strength of the modified Peyton’s method compared to the traditional approach.
Additionally, the modified Peyton’s method also facilitated teamwork, as evidenced by the experimental group achieving higher scores across all 8 teamwork dimensions. Before the final teamwork session, physicians had already acquainted themselves through peer learning during earlier sessions. The role rotation during former trainings fostered role transitions and information-sharing. These improvements are vital in maternal cardiac arrest management, where effective coordination among obstetrics, anesthesia, and emergency teams is essential within a multidisciplinary teamwork under high-pressure conditions.14
Notably, knowledge scores were comparable between the 2 groups, highlighting the effectiveness of both methods in conveying knowledge.
Limitations and Future Directions
This single-center design and small sample size of this study limited its generalizability. To assess long-term skill retention, longitudinal studies are needed, and multicenter trials could validate applicability across diverse settings. Additionally, integrating bedside teaching may further bridge the gap between simulation and clinical practice.
Conclusion
The modified Peyton’s four-step teaching method, which incorporates the core mechanisms of peer assistant and mutual learning, is anticipated to address the issue of skill retention prevalent in traditional training approaches. This method offers a novel pathway for the development of emergency obstetric expertise. This study aims to establish an evidence-based foundation for the implementation of this teaching method within the realm of critical care for pregnant and postpartum women, thereby facilitating the transition of ACLS training from a model of “standardization” to one of “precision and contextualization”.
Data Sharing Statement
The data are available from the corresponding author on reasonable request.
Consent for Publication
Informed consent was obtained from all participants prior to their inclusion in the study. Participants also signed consents of publication the data of the study.
Funding
Medical Education Research Project of Peking University Health Science Center (2021YB38) and Key Clinical Projects of Peking University Third Hospital (No. BYSYZD2022032).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Andersen LW, Holmberg MJ, Berg KM, et al. In-hospital cardiac arrest: a review. JAMA. 2019;321(12):1200–1210. doi:10.1001/jama.2019.1696
2. Panchal AR, Bartos JA, Cabañas JG, et al. Part 3: adult basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142(16_suppl_2):S366–s468. doi:10.1161/cir.0000000000000916
3. Varghese S, Abraham L. Comparison of Peyton’s four-step approach with the conventional bedside technique in teaching clinical examination skills to medical students. Cureus. 2024;16(2):e54397. doi:10.7759/cureus.54397
4. Breckwoldt J, Cheng A, Lauridsen KG, et al. Stepwise approach to skills teaching in resuscitation: a systematic review. Resusc Plus. 2023;16:100457. doi:10.1016/j.resplu.2023.100457
5. Peyton MWR. Teaching in the Theatre. Manticore Publishers Europe; 1998.
6. Giacomino K, Caliesch R, Sattelmayer KM. The effectiveness of the Peyton’s 4-step teaching approach on skill acquisition of procedures in health professions education: a systematic review and meta-analysis with integrated meta-regression. PeerJ. 2020;8:e10129. doi:10.7717/peerj.10129
7. Xiaomin L, Wanhua X, Dan F, et al. Application of modified Peyton′s four-step approach in basic skills operation training for pediatric residents. Chin J Med Edu. 2023;43(12):942–946.
8. Lott C, Truhlář A, Alfonzo A, et al. European Resuscitation Council Guidelines 2021: cardiac arrest in special circumstances. Resuscitation. 2021;161:152–219. doi:10.1016/j.resuscitation.2021.02.011
9. Greif R, Bray JE, Djärv T, et al. 2024 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: summary from the basic life support; advanced life support; pediatric life support; neonatal life support; education, implementation, and teams; and first aid task forces. Circulation. 2024;150(24):e580–e687. doi:10.1161/cir.0000000000001288
10. Burgess A, van Diggele C, Roberts C, et al. Facilitating small group learning in the health professions. BMC Med Educ. 2020;20(Suppl 2):457. doi:10.1186/s12909-020-02282-3
11. Burgess A, van Diggele C, Roberts C, et al. Planning peer assisted learning (PAL) activities in clinical schools. BMC Med Educ. 2020;20(Suppl 2):453. doi:10.1186/s12909-020-02289-w
12. Podraza LC, Starnes LS, Starnes JR, et al. A novel pediatric clinical skills curriculum to prepare medical students for pediatrics clerkship. Med Sci Educ. 2025;35(1):343–350. doi:10.1007/s40670-024-02191-w
13. Rajaratnam V, Rahman NA, Dong C. Integrating instructional design principles into surgical skills training models: an innovative approach. Ann R Coll Surg Engl. 2021;103(10):718–724. doi:10.1308/rcsann.2020.7132
14. Wang M, Yang L, Zhang S, et al. The impact of a multidisciplinary experiential training model on knowledge, attitude and practice of healthcare workers in maternity health management: a preliminary study. J Multidiscip Healthc. 2024;17:3029–3039. doi:10.2147/jmdh.S465695
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.