Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Enhancing Collaboration and Patient-Centered Care Through Moderated Multidisciplinary Consultations
Authors Hulbaek M ![]() , Edal BT, Thude BR
, Edal BT, Thude BR
Received 21 April 2025
Accepted for publication 23 July 2025
Published 30 August 2025 Volume 2025:18 Pages 5393—5403
DOI https://doi.org/10.2147/JMDH.S530549
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Mette Hulbaek,1,2 Betina Torpegaard Edal,3 Bettina Ravnborg Thude4
1Department of Gynecology and Obstetrics, University Hospital of Southern Denmark, Sønderborg, Denmark; 2IRS- Institute for Regional Health Research, University of Southern Denmark, Odense, Denmark; 3Department of Cardiology, University Hospital of Southern Denmark, Aabenraa, Denmark; 4Internal Medicine Research Unit, University Hospital of Southern Denmark, Aabenraa, Denmark
Correspondence: Mette Hulbaek, Email [email protected]
Background: In the last decade, multimorbidity has risen in Western countries. Treating patients with multiple symptoms and health conditions is complex and competencies from different specialties are needed. The World Health Organization emphasizes a multidisciplinary approach to address these complex conditions. Patients with pelvic floor disorders suffer from multiple symptoms, yet today their care is often fragmented across specialties and clinicians focus on symptoms within their own diagnostic frameworks, potentially limiting holistic care. Thus, this study aimed to explore if and how a multidisciplinary organizational set-up for complex patients with pelvic floor disorders can support interprofessional collaboration and approach a complex patient in a patient-centered way.
Methods: The study was a qualitative interview study among healthcare professionals in a pelvic floor clinic using a hermeneutic approach in the setting of multidisciplinary team consultations for referred patients with pelvic floor disorders and with multiple and complex pelvic floor conditions.
Results: Thematic analysis identified two themes and six subthemes. Theme 1; Coordinated consultation included the subthemes: Providing a framework, Involving team members, and Establishing overview. Theme 2; Patient-centered care set-up included the subthemes: Aligning expectations, Involving the patient, and Ensuring the patient feels comfortable and cared for.
Conclusion: To ensure patient involvement and patient-centeredness, a framework for the decision-making process is required involving management and an overview of the dialogue, timelines, and communication models for involving the patient as well as healthcare professionals. Using a moderator during consultations increased focus on interprofessional collaboration and may be the key for multidisciplinary consultations in the future helping “put the patient in the center of care”.
Keywords: interprofessional collaboration, multidisciplinary consultations, pelvic floor disorders, pelvic organ prolapse, fecal incontinence
Introduction
Multimorbidity has risen during the last decades in Western countries.1 In many European countries, including Denmark, a demographic shift characterized by an increasing proportion of elderly individuals is expected and since age and multimorbidity are associated, an increase in multimorbidity and comorbidity is also expected.2,3
Multimorbidity is defined as the coexistence of two or more diseases or conditions.4 Treating a patient with multiple symptoms from various health conditions is complex, and future health systems should focus on the complex needs of these patients.4 However, patients with multimorbidity and multiple symptoms often experience that each condition is treated separately in a healthcare system where treatment and care is organized in fragmented parts and where guidelines only describe and treat single conditions.5 Health care systems need to deliver coordinated, patient- centered care.4 Patient-centered care is an evolving concept with numerous conceptual frameworks, and its successful implementation remains somewhat unexplored.6 However, there is consensus about its most important elements – patient empowerment, patient individuality, and a biopsychosocial approach.7
The growing multimorbidity and complex conditions in healthcare demand a multidisciplinary approach.8 Multidisciplinary healthcare is defined as integrating the work of multidisciplinary healthcare workers in the multidisciplinary team in managing people with multiple conditions, including integrated care plans.9 With all specialties present at the same time and in the same room, every perspective on the problem is considered, and all relevant knowledge is brought to the table.
Complex chronic conditions are best managed through a multidisciplinary team approach which was proven effective across various medical fields eg oncology, diabetes and in primary health care.10
Patients with pelvic floor disorders (PFDs) suffer from multiple symptoms originating from various health conditions in the pelvic floor,11 including faecal incontinence (FI), bowel- and urinary symptoms, and sexual health problems. Women constitute the majority of patients with PFDs,12 and present symptoms such as pelvic and vaginal pain, urogenital prolapse and altered body image.13 Consequently, population ageing will likely lead to a higher prevalence of PFD symptoms.12 A study from 2008 reported that the weighted prevalence of older women (60–79 years) experiencing PFDs was 36.5% and 49.7% (80 years and over) compared with women aged 20–39 years (9.7%).12 PFD treatment and care tend to be disjointed and uncoordinated across healthcare providers, with health care professionals from various professions and specialities involved to explore symptoms from distinct diagnostic perspectives with specific standardizations and eg specified questionnaires.14–17
An interview study of Danish women’s perception of the various symptoms of a PFD indicated that symptoms were tangled together and significance for them depended on how they affected everyday life, so specifying symptoms for single measures for specific questionnaires or specialities was unlikely to reflect their true perception of the condition.18 Thus, beyond a multidisciplinary approach, treating these patients requires patient-centeredness and involvement to explore symptoms and make decisions.19 In this way, interdisciplinary collaboration between professions and specialized healthcare professionals in the team becomes essential.
Beyond involving the patient with PFDs in decision-making, a multidisciplinary team (MDT) must ensure meeting the patient with a patient-centered and all-encompassing approach to explore all the multiple symptoms and understand their coherence.20 A shared decision-making (SDM) process could ensure patient involvement21 and enhance patient- centered care.22 SDM is a conceptual construction where healthcare professionals and patients are partners, and essential elements of patient-centered healthcare such as patient values and preferences, options, patient participation, patient education, information of benefits, risks, pros and cons and deliberation and negotiation is a part of the decision-making process.22,23
Establishing multidisciplinary teams is common in healthcare but yet the multidisciplinary setup is often not described nor explored.19,20 Further, research exploring the setup from an organizational perspective is also uncommon in clinical research. However, we need to understand how this works and how to make space for interprofessional collaboration and patient involvement in such healthcare teams and consultations.
This study aimed to explore if and how the organizational setup of multidisciplinary consultations may support interprofessional collaboration and the opportunity to approach the patient in a patient-centered manner.
Materials and Methods
The study was a qualitative interview study in a pelvic floor clinic (PFC) using a hermeneutic approach in the setting of multidisciplinary team (MDT) consultations for referred patients with PFDs having more than two symptoms belonging to more than two different specialities (urology, proctology, gynecology or sexology).
The Setting for the Study
The PFC was established in 2019 at a small regional hospital in Denmark. The MDT conducted multidisciplinary consultations once a week, alongside a nurse-driven clinic. The PFC has an annual capacity for 250 multidisciplinary consultations, primarily female patients with urinary incontinence and bowel disorders. During the consultations, the patients, in collaboration with the healthcare professionals, should identify what is most important to them, including their preferences regarding the course of care, examinations, and treatments. This means that the patients determine the focus of the group discussion. Besides the decision making, the team gathers relevant information from the patients.
Ten appointed healthcare professionals from different professions and specialties constitute the five-member team (MDT) performing the joint consultation – one gynecologist, one urologist, one proctologist, one specialist nurse and one specialist physiotherapist. A moderator is appointed for each consultation. The moderator is either the specialist nurse or the physiotherapist but never one of the consultants. The setup also involves an initial telephone call to the upcoming patients by the PFC secretary after referral but prior to consultation. The patient pathway in the PFC is shown in Figure 1.
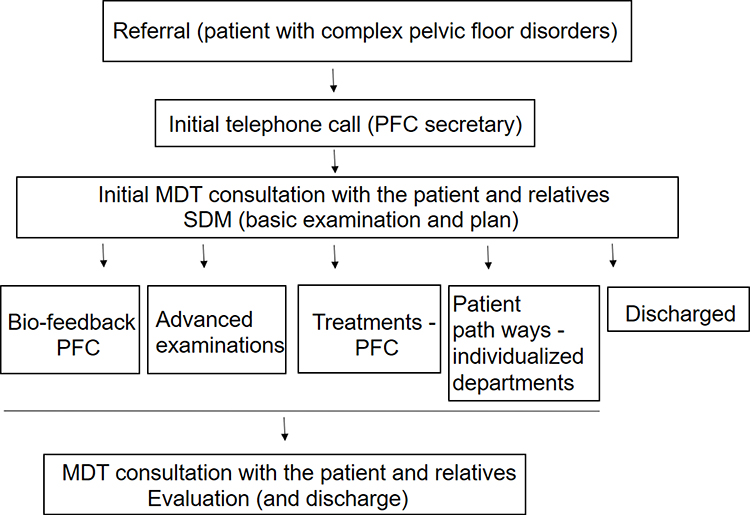 |
Figure 1 Patient pathway PFC. |
The PFC collaborates well with the X-ray department, a co-opted radiologist, and other relevant partners within the hospital. Patients requiring advanced examinations, eg, dynamic MR scans are examined and discussed collaboratively with radiology regularly at MDT conferences.
Informants
Eligible informants were all appointed healthcare professionals (consultants, nurses and physiotherapists) engaged in MDT consultations for more than 50% of consultations within the year prior to the interviews. Nine of ten healthcare professionals were eligible and invited to participate. All invited healthcare professionals consented to participate, but one was unable to participate because of workload.
Data Collection and Analysis
A nurse from the author group (BTE) collected the data. She was chosen as she was not working or connected to the department and was not familiar with the PFC, MDT consultations or the patient group beforehand. Semi-structured individual interviews were conducted face-to-face or by phone in a secluded office. Interviews were audio-recorded, and recordings were anonymous to others from the PFC, the MDT including the PFC member from the author group (MH). The importance of this confidentiality was to ensure free speech for all interviewees.
The semi-structured interview guide for the study focused on the three research questions: How do you experience…
- the cooperation between different healthcare professionals in the MDT consultation?
- the role of the moderator function?
- the involvement of the patient in decision-making?
BTE from the author group transcribed the recordings and analyzed data using Braun and Clarke’s thematic analysis.24 BTE performed a naive listening to the audio recordings, which were preceded by a verbatim transcription. BTE read transcriptions several times to search the data set for repeated patterns. Line by line, interesting or important text sequences (meaning units of phrases, sentences and sections) were coded using a semantic approach, understanding the data on explicit levels and then seeking and understanding the potential latent levels or implicit meanings.
Ethics
According to Danish law, approval from the National Committee on Health Research Ethics was not required, as no biomedical intervention was performed. The study was conducted in accordance with the Helsinki Declaration (World Medical Association’s meeting of October 2013).
Participants were informed that anonymity may be challenging due to the small number of healthcare professionals in the PFC, but this was countered during transcription and analysis by content pseudonymization if supervision was required during the process. Written informed consent including publication of anonymized responses/direct quotes was obtained from all participants.
Participants had the right to withdraw their consent or statements from their interview.
Data was managed according to GDPR Danish Law and stored at a logged regional server (SharePoint). Data permission was obtained from the regional authority (Journal number: 19/46,391).
Results
Eight interviews were performed in November 2023. Seven female and one male participated (ages 37–60 years). The mean number of years working with patients with PFDs was 15 years (5–33 years of medical experience). Five informants potentially had the role of moderator, and three were team members who would never have the moderator role since they were consultants. Four interviews were performed by phone and four were conducted face to face in the PFC. Interviews had a duration of 16 to 48 minutes.
Thematic Analysis
The following sections present the findings of two identified themes; Theme 1 Coordinated consultation and Theme 2 Patient- centered care set-up. Findings are supported by selected quotes. Interviewees are identified as with or without the moderator role.
Theme 1 Coordinated Consultation
This theme encapsulates the subthemes Providing a framework, Involving team members, and Establishing overview.
Providing a Framework
Informants describe how the moderator provides the framework for the consultation by ensuring the agreed organizational agenda and structure of the consultation and the dialogue.
So, I am the one that organises it. Where we are, timelines and how long it takes, presenting participants. The format and structure of the consultation is established by the moderator. (Informant B - with the moderator function)
Before introducing a moderator, consultations had always been delayed. The moderator helps provide structure to the consultation by managing time. The role of the moderator is described by both healthcare professionals with and without a moderating role as the one who on behalf of the patient and the team keeps track of time and is responsible for managing time during the consultation. After a consultation, each consultant must leave for their office to document decisions and care in the electronic patient journal. The Informants describe how the moderator is responsible for ensuring everybody is present and ready for the next consultation.
We felt it right from the start … we were totally behind (schedule) … and then, if I remember correctly, it was their (quality department’s) idea to bring in a moderator. And since then, it’s worked much better. There were other things, but the moderator made a big difference. (Healthcare professional H - without the moderator function)
Since factors such as essential examinations during consultations, eg anoscopy or gynecological examinations, also influence time schedules, the moderator specifically structures the consultation, playing a significant role in effectively managing time.
And so it’s our job to be on time and make sure things flow smoothly, and make sure that we cover everything—so there’s time to ask questions and complete examinations. (Informant D - with the moderator function)
The moderator follows the patient from the waiting room, presenting team members around the table, initiating the conversation, reviewing the plan at the end of the consultation, and concluding the session. In this manner, she provides the framework for the consultation from the beginning to the end.
I think, when it comes to the setup of the facility, it makes really good sense for the moderator to be the one who both fetches the patient and says goodbye to the patient at the end. (Informant G - without the moderator function)
The informants agree that the moderating role has positively impacted the consultations by framing the consultation, structuring the dialogue and keeping track of time.
Involving Team Members
Data also indicates that the moderator is responsible for involving all team members in the consultation and inviting relevant competencies into the dialogue.
Some informants note that not only focusing on one’s own expertise but also adding and following up on colleagues’ recommendations is challenging but accepted by other team members. The moderator helps guide the conversation and assigns space and time for each team member.
(...) in any case, it has helped to have a moderator who is responsible for managing things and ensuring that everyone gets equal speaking time. So, it becomes a conversation that everyone is involved in. (Informant D - with the moderator function)
Additionally, the moderator seems to strive to maintain focus on what needs to be discussed during the consultation.
And she must be able to guide the patient in accordance with the worst (problem), just like triaging her problems according to which doctor is most important to talk to and hear from first. (Informant E - with the moderator function)
Another challenge occurs when team members must communicate and reconcile treatment options during a consultation. Data show that all team members expect the moderator to have comprehensive knowledge of all the specialities involved in a consultation. The moderator also reassures everyone they have speaking time. This encourages interdisciplinary collaboration and ensures the involvement of all different team members, promoting a better, more patient-centered consultation.
(…) our moderator also keeps an eye on the other colleagues. (…) but I think the moderator more or less manages everything; I pay attention to my recommendations, and the moderator manages all recommendations from all colleagues … (Informant F - without the moderator function)
Establishing Overview
The moderator is across team members described as the one team member with the general overview of the consultation. There was a common expectation that the moderator maintains this overview during the whole consultation.
(…) but when I am the moderator, I withdraw to the background a little and try to maintain an overall view of the discussion. (Informant A - with the moderator function)
Data describe how the moderator moderates the dialogue process. The moderator can step back and act passive and inconspicuous but can also be more of a mediator between the patient and different team members.
What I believe the moderator does is to keep the bigger picture in mind, so she has the opportunity, firstly to be the bridge between the healthcare professionals and the patient, but also to maintain a helicopter perspective of the problem. (Informant G - without the moderator function)
One team member described that nurses have an advantage in the moderator role as they not only have a broad knowledge of PFDs but possess many of the competencies required, such as overview, the patient’s project manager, interdisciplinary skills, patient guidance and empathetic abilities alongside the clinical competencies within the speciality.
But I think it suits a nurse well to have this overall perspective. (…) the private sector recognizes a project leader as a job role, and it is a form of project management that the discussion needs to make sure everything works. (Informant A - with the moderator function)
The theme Coordinated consultation highlights that the moderator provides the framework for the consultation, including managing the time during the consultation and adherence to the timeframe. Additionally, the moderator coordinates the consultation by involving team members according to expertise and the patients’ problems. She ensures that the patient and all healthcare professional from the team get a say during the consultation.
Theme 2 Patient-Centered Care Set up
Theme 2 encompasses the subthemes Aligning expectations, Involving the patient, and Ensuring the patient feels comfortable and cared for.
The theme describes how the moderator places the patient at the center of care through all stages of the consultation – beginning, during and at the end of consultation.
Aligning Expectations
The moderator aligns expectations with the patient before and during the consultation. The informants describe how the moderator is expected to understand what is discussed and agreed upon and then clarify this for the patient.
Yes, (as the moderator) I make sure the patient understands all the way through (the discussion) and that there are no misunderstandings, and I check that the patient has understood things the way different (healthcare professionals) intended. (Informant C - with the moderator function)
The quote shows that the moderator understands what the team members are communicating and recaps this information for the patient during the consultation to ensure the patient understands the discussed information and the suggested options.
Another moderator describes how she aligns expectations with the patient before the consultation by using the walk from the waiting room to the consultation to explain the purpose of the consultation, inform the patient about the setup and ensure that clear agreements made during the consultation consider the patient’s preferences.
And you need to make choices; if the patient has three problems, you need to prioritize with the patient and say: I understand and do you agree that this is the biggest issue, and this is what we should focus on this time. (Informant E - with the moderator function)
At the end of the consultation, the moderator verbally clarifies and summarizes the agreements and writes a resume of important information and decisions from the consultation. In this way, the moderator helps conclude the consultation by ensuring that the patient understands, accepts and commits to the treatment plan and that expectations between all parties are aligned.
And then finally, when we start to make a plan about what should happen next, it’s the moderator who ensures that what we propose and discussed matches the patient’s expectations and possibilities. (Informant G - without the moderator function)
Involving the Patient
The moderator initiates the consultation by inviting the patient to speak. Thus, the patient can determine the focus of the upcoming dialogue. Further, data clearly show that the moderator actively collaborates with the patient to ensure involvement and SDM.
It is actually the moderator’s task to ensure that we cover all areas and that the patient has a voice and is involved in the discussion in order for us to describe it as SDM. (Informant A - with the moderator function)
The above indicates that the moderator is responsible for applying the method of SDM, ensuring that the patient is involved in the decision-making. One healthcare professional described how the decision-making process was handled and was considered difficult before implementing a moderator role in the consultations.
We felt right from the start (before having a moderator) that we were completely behind (…) which meant that every day was ruined from the start, and you get stressed and think: this is not working well. Yeah, something needed to happen. (…) Okay, we cannot offer shared decision-making if we keep working this way. (Informant H - without the moderator function)
Ensuring the Patient Feels Comfortable and Cared for
The moderator ensures that the patient feels comfortable throughout the consultation. It is described as an asset to the process as the patient and moderator had the opportunity to relate to one another from the beginning, and the moderator’s ability to build a relationship with the patient had a positive effect during the consultation.
As moderators, we are those who have the initial contact and often develop a relationship. The patient often relies on this relationship when things get uncertain or uncomfortable Patients tend to look to the moderator as this is the person who made the initial connection and serves as the reference point. (Informant A - with the moderator function)
Data describe how, by escorting the patient from the waiting room, the moderator establishes a trusting relationship with the patient, which is utilized throughout the consultation. The moderator does not always know the patient prior to the consultation. However, if the moderator has familiarity with the patient, the role may be decided beforehand.
Considering the above, it seems that collaboration with the patient appeared to work best when the patient trusted the moderator. Additionally, having a designated moderator for the patient to turn to positively impact the relationship. Healthcare professional, with and without moderating functions, described how the moderator reassured and sustained the relationship eg, by maintaining eye contact with the patient, and ensuring that the patient felt comfortable and cared for during the consultation.
Of course, that supportive or care-giving role that’s inherent in nursing is still there. It’s still the nurse [moderator] who makes sure the patient is informed along the way, that the patient has someone holding their hand if needed, and also ensures that the patient is on board with everything happening. And then, when we start planning what comes next, it’s the nurse [moderator] again who makes sure that what we suggest aligns with the patient’s expectations and their capabilities. (Informant G - without the moderator function)
The theme Patient-Centered Care highlights how the moderator ensures the patient is placed at the centre of the consultation with shared decision-making. The strong relationship between the moderator and the patient appears to be a valuable asset. This is achieved by maintaining eye contact, aligning expectations with the patient before, during, and after the consultation, ensuring the patient is involved in decisions, and guiding the patient to prioritize the most important matters during the dialogue.
Discussion
We set out to explore the organizational setup within a PFC and how the setup supported interdisciplinary collaboration and patient-centered consultations. In light of this, we discuss the findings.
A Coordinated Consultation
The healthcare professionals describe the moderating role as a function that contributes to the structure and framework of the consultation. According to the American psychologist and organizational theorist Karl Weick, maintaining a certain structure is a way to create a framework that is recognizable so that staff know when and how to contribute and understand how their role and competencies are valuable in the situation.25 In this case, the structural model enables focus on the patient’s needs and most important issues. In agreement, Kurtz and Silverman argue that establishing a certain structure in the conversation between physicians and their patients helps the physician gain an overview of the conversation.26 The Calgary- Cambridge model focuses on the consultation process from initiating the session, gathering information, providing structure to the consultation, building a relationship, giving information by explaining and planning, and closing the session.26 Generally, this model resembles core elements of SDM.23,27
The moderator’s professional background, experience and relationship with colleagues appears relevant in creating a structure that matches everyone’s needs in a collaborative setting. The moderator adjusts according to the patient’s needs and preferences and the team members’ input. The moderator ensures that the patient is heard and that decisions about relevant themes on the agenda are made. Several informants mention the importance of maintaining a strict timeframe and finishing on time. The moderator is responsible for keeping track on time and finishing on time. In this case, the moderating function carries out a task the others otherwise would need to pay attention to separately and maybe uncoordinated. The presence of the moderator ensures that each team member can focus on the patient and their professional contribution. The moderator makes according to Weick a complex determination25 meaning that she tries to make sense of how the patient and her colleagues understand the situation and moderate the consultation based on this sense-making. This approach seems to work at the PFC. However, it requires all team members, including the physicians within the team, to accept management by a moderator. This may be challenging in some settings as physicians have the right to make decisions, and the power balance between nurses and physicians is historically unbalanced.28
However, all healthcare professionals described the moderator as a resource in the consultation. One of the healthcare professionals with a moderator function compared her function to that of a project manager, suggesting that moderating is perceived as an extensive and important function in itself that is essential for delivering coordinated patient -centered care. It is described how the moderator identifies and prioritizes which profession can meet the patient’s needs and preferences during the consultation, brings relevant professional competencies into play by utilizing their expertise during the conversation and in planning the patient’s care. Thus, the moderator must know how the other professionals can contribute and understand what is at stake for the patient. Therefore, the moderating role requires someone with a broad knowledge of the others’ professional expertise and personal competencies and preferences. According to sociologist Davina Allen, it is well known that nurses are the organizational glue that holds the healthcare system together.29 Nurses create working knowledge by gathering the entire patient’s fragmented information from the medical record and compiling it so relevant information can be passed to all professional groups. Thus, the nurse is expected to have an overview of the entire patient pathway and their needs.30 Allen’s research shows that nurses not only organize their own tasks but also essentially keep track of the tasks of other professional groups. They are described as able to connect network actors and include other professional groups.29,30 This is comparable with the MDT consultation in the PFC where the moderator keeps track of and includes other professional groups in the consultations. The nurse’s communicative skills are according to an American study by Azar et al the reason why the coordinating nurse is seen as an interdisciplinary coordinator, improving communication between interdisciplinary areas and integrating better collaboration between professional groups.31 Coordinating between professional groups and the patient, the nurse can influence the collaboration in the interdisciplinary team and the team’s relationship with the patient in a positive direction and contribute to improved patient satisfaction.31 Allen saw that the articulation work, among other things, involved the nurse ensuring that an activity took place at the right time and in the right order.29 The articulation work also involved the nurse mediating between the various parties involved in the process, including professional groups and the patient. Allen believes that there is virtually nothing in the healthcare system that does not pass through the hands of a nurse, which gives nurses a privileged position to build networks and act as mediators.29,30
A team with several professions can have a common purpose and at the same time work differently.32 Interprofessional collaboration aims to exceed the boundaries of the professions and thus work in a new way so that new understandings and knowledge can arise.32 Interprofessional collaboration helps to coordinate and ensure a smooth transition and a joint effort for the patient. The interprofessional collaboration includes consideration of the role and responsibilities of each profession to ensure the entirety of the patient’s treatment.32 We argue that findings, in this case, suggest that the consultations led by a moderator essentially have become interprofessional, so that the goal and the treatment options are now a common concern, and in this way, new knowledge and perspectives have occurred.
Patient Involvement
Patients with PFDs present with multiple symptoms and complex and intertwining conditions with various examinations and treatment options. This involves numerous professions and professionals from departments or clinics with expertise within PFDs. Patients understanding of the vast amount of information about the options and active involvement in their health care may give rise to added confusion and uncertainty and furthermore, patients with multi-illnesses demand a greater need for involvement in decisions about treatment and care, as the complexity of the illnesses affects everyday life.33 To involve patients from the PFC in decision-making in multidisciplinary consultations, we set out to discuss implementation of patient-centered care in this setup. Patient-centered care adapts to the patients’ needs and sees the patient as an individual rather than each patient fitting into health care and different “boxes” eg specialties or professions as described by Damarel and colleagues.5
Patient-centered care requires a framework where consultations are tailored to “understand each patient as a unique human being”.34 Consultations must be tailored to support the patient’s understanding of the different options, treatments pros and cons, tailored to engage and involve each patient in the decision-making process, essential elements for the process of SDM.22,23
Implementing patient-centered care and involving patients in decision-making is becoming more popular in Denmark but needs further work for implementation to be successful.35 Our findings suggest that prioritising a moderator seem to have extensive significance for ensuring patient-centered care in consultations and involving complex patients in decision-making. The moderator maintains relational care for patients by creating a safe space where patients can be involved in the decision-making. The moderator supports and clarifies information to patients to ensure that their preferences are considered. These elements are important in SDM. Elwyn and colleagues advocate that SDM can be implemented through the framework of a talking model; the team-talk (sharing decisions), the option talk (objective presentation of options), and the decision talk (deliberation and negotiation).27,36 Talks we find adhere to the framework and setup of the moderated consultation.
A Danish field study in a setting of cancer patients showed that nurses are a resource in the implementation of SDM.37 Observations showed how the nurse had a very unique relationship with the patient that the physician did not appear to have. The nurse allowed the patient to share thoughts and feelings about a given problem. She often unreflectively felt these competencies as part of nursing’s core tasks.37
Nurses’ abilities to promote patient involvement and SDM support increased use of nurse moderators in multidisciplinary consultations to provide better opportunities for patient-centered care and involvement.
Strengths and Weaknesses
Although this study only explores one clinic with multidisciplinary consultations, we think this study sheds light on interesting angles that can motivate further discussion and new research in the area. Clinical health research exploring intercollaboration in organizations with an organizational theoretical perspective is relatively new. Research of a unit and its setup in organizational research is defined as a case study.38 A case study is “an intensive study of a single unit with an aim to generalize across a larger set of units”,39 which is valuable for health science research to evaluate new programs and develop new interventions.40 This study has an increased reliability as it has applied a methodological analysis supported with extensive quotations. The detailed description of our setting strengthens transferability.
The choice of interviewer reflects strengths and weaknesses. As an outsider, the interviewer did not know anything about the specialty beforehand and this should have strengthened data collection with an open mindset and unbiased preconceptions. Further, interviewees could trust that the data collector was not judgmental and that their interviews could be anonymous and not conflict with subsequent collaboration with the other team members. However, as a novice in the field, the data collector may not have had the competencies to ask for more resounding information or avoided intimidating questions regarding cooperation, so as to not provoke answers that anybody would regret. This could have hidden some underlying conflicts and challenges within the team members and have distorted the full picture. Furthermore, interviews tend to show opinions and feelings that dominate the specific stage and current organizational setup, like snapshots. In addition, previous experiences and feelings through implementation phases could have faded and created recall-bias.
Conclusions
We set out to explore if and how the organizational setup of multidisciplinary consultations may support interprofessional collaboration and the opportunity to approach the patient in a patient-centered manner.
To ensure patient involvement and patient-centeredness, an organizational setup in a multidisciplinary team and a framework for the decision-making process was essential. A moderator was the guarantee for enforcing this framework and keeping an overview for all team members and the patient. The moderator identifies and prioritizes which profession can meet the patient’s needs and preferences to succeed in making sense of the complexity in a multidisciplinary consultation. Further, the moderator helped support the multidisciplinary team to engage in interprofessional collaboration and focus on a common goal. The moderator assembled the fragments from each specialty considering coherence with the patients’ preferences. This increased focus on interprofessional collaboration could be the key for multidisciplinary consultations in the future and help ‘put the patient in the center of care’.
Abbreviations
FI, fecal incontinence; MDT, Multidiciplinary team; PFC, pelvic floor clinic; PFD, pelvic floor disorders; SDM, Shared decision making.
Acknowledgments
We would like to thank all healthcare professionals for participating and for important contribution to this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Uijen AA, van de Lisdonk EH. Multimorbidity in primary care: prevalence and trend over the last 20 years. Eur J Gen Pract. 2008;14(sup1):28–32. doi:10.1080/13814780802436093
2. Kingston A, Robinson L, Booth H, Knapp M, Jagger C, Project M. Projections of multi-morbidity in the older population in England to 2035: estimates from the population ageing and care simulation (PACSim) model. Age Ageing. 2018;47(3):374–380. doi:10.1093/ageing/afx201
3. Møller SP, Laursen B, Johannesen CK, Schramm S. Multisygdom i Danmark. Statens Inst Folkesundhed, SDU. 2019;2019:1.
4. Albreht T, Dyakova M, Schellevis FG, Van den Broucke S. Many diseases, one model of care? J Comorbidity. 2016;6(1):12–20. doi:10.15256/joc.2016.6.73
5. Damarell RA, Morgan DD, Tieman JJ. General practitioner strategies for managing patients with multimorbidity: a systematic review and thematic synthesis of qualitative research. BMC Fam Pract. 2020;21:1–23. doi:10.1186/s12875-020-01197-8
6. Santana MJ, Manalili K, Jolley RJ, Zelinsky S, Quan H, Lu M. How to practice person-centred care: a conceptual framework. Health Expect. 2018;21(2):429–440. doi:10.1111/hex.12640
7. Grover S, Fitzpatrick A, Azim FT, et al. Defining and implementing patient-centered care: an umbrella review. Patient Educ Counsel. 2022;105(7):1679–1688. doi:10.1016/j.pec.2021.11.004
8. Mickan S, Hoffman SJ, Nasmith L, WHOSGoI E, Practice C. Collaborative practice in a global health context: common themes from developed and developing countries. J Interprofessional Care. 2010;24(5):492–502. doi:10.3109/13561821003676325
9. Mercer S, Furler J, Moffat K, Fischbacher-Smith D, Sanci L. Multimorbidity: technical series on safer primary care. World Health Org. 2016;2016:1.
10. Benagiano G, Brosens I. The multidisciplinary approach. Best Pract Res Clin Obstetrics Gynaecol. 2014;28(8):1114–1122. doi:10.1016/j.bpobgyn.2014.08.006
11. Abrams P, Cardozo L, Wagg A, Wein A. Incontinence.
12. Nygaard I, Barber MD, Burgio KL, et al. Prevalence of symptomatic pelvic floor disorders in US women. JAMA. 2008;300(11):1311–1316. doi:10.1001/jama.300.11.1311
13. Lowder JL, Ghetti C, Nikolajski C, Oliphant SS, Zyczynski HM. Body image perceptions in women with pelvic organ prolapse: a qualitative study. Am J Obstetrics Gynecol. 2011;204(5):
14. Rogers RG, Espuna Pons ME. The Pelvic Organ Prolapse Incontinence Sexual Questionnaire, IUGA-revised (PISQ-IR). Int Urogynecol J. 2013;24(7):1063–1064. doi:10.1007/s00192-012-1952-3
15. Price N, Jackson SR, Avery K, Brookes ST, Abrams P. Development and psychometric evaluation of the ICIQ Vaginal Symptoms Questionnaire: the ICIQ-VS. BJOG. 2006;113(6):700–712. doi:10.1111/j.1471-0528.2006.00938.x
16. Cotterill N, Norton C, Avery KN, Abrams P, Donovan JL. A patient-centered approach to developing a comprehensive symptom and quality of life assessment of anal incontinence. Dis Colon Rectum. 2008;51(1):82–87. doi:10.1007/s10350-007-9069-3
17. Due U, Brostrom S, Lose G. Validation of the Pelvic Floor Distress Inventory-20 and the Pelvic Floor Impact Questionnaire-7 in Danish women with pelvic organ prolapse. Acta Obstetricia et Gynecolog Scand. 2013;92(9):1041–1048. doi:10.1111/aogs.12189
18. Hulbaek M, Knutz E, Ebbesen NT, Primdahl J, Nielsen JB, Birkelund R. Pelvic organ prolapse and treatment decisions– developing an online preference-sensitive tool to support shared decisions. BMC Med Info Decision Making. 2020;20(1):265. doi:10.1186/s12911-020-01264-1
19. Hainsworth A, Ferrari L, Malde S, Berry L. Building a Multidisciplinary Pelvic Floor Clinic: why Bother? Seminars Colon Rectal Surg. 2023;34(1):100933. doi:10.1016/j.scrs.2022.100933
20. Ferrari L, Gala T, Igualada-Martinez P, Brown HW, Weinstein M, Hainsworth A. Multidisciplinary team (MDT) approach to pelvic floor disorders. Continence. 2023;7:100716. doi:10.1016/j.cont.2023.100716
21. Stacey D, Legare F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4:Cd001431. doi:10.1002/14651858.CD001431.pub5
22. Bomhof-Roordink H, Gärtner FR, Stiggelbout AM, Pieterse AH. Key components of shared decision making models: a systematic review. BMJ Open. 2019;9(12):e031763. doi:10.1136/bmjopen-2019-031763
23. Makoul G, Clayman ML. An integrative model of shared decision making in medical encounters. Patient Edu Counsel. 2006;60(3):301–312. doi:10.1016/j.pec.2005.06.010
24. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
25. Weick KE, Sutcliffe KM, Obstfeld D. Organizing and the process of sensemaking. Org Sci. 2005;16(4):409–421. doi:10.1287/orsc.1050.0133
26. Kurtz SM, Silverman JD. The Calgary—Cambridge Referenced Observation Guides: an aid to defining the curriculum and organizing the teaching in communication training programmes. Med Educ. 1996;30(2):83–89. doi:10.1111/j.1365-2923.1996.tb00724.x
27. Elwyn G, Durand MA, Song J, et al. A three-talk model for shared decision making: multistage consultation process. BM. 2017;359:j4891. doi:10.1136/bmj.j4891
28. Tang C, Chan S, Zhou W, Liaw SY. Collaboration between hospital physicians and nurses: an integrated literature review. Int Nurs Rev. 2013;60(3):291–302. doi:10.1111/inr.12034
29. Allen D. Translational mobilisation theory: a new paradigm for understanding the organisational elements of nursing work. Int J Nurs Stud. 2018;79:36–42. doi:10.1016/j.ijnurstu.2017.10.010
30. Allen D. Re-conceptualising holism in the contemporary nursing mandate: from individual to organisational relationships. Soc Sci Med. 2014;119:131–138. doi:10.1016/j.socscimed.2014.08.036
31. Azar JM, Johnson CS, Frame AM, Perkins SM, Cottingham AH, Litzelman DK. Evaluation of interprofessional relational coordination and patients’ perception of care in outpatient oncology teams. J Interprofessional Care. 2017;31(2):273–276. doi:10.1080/13561820.2016.1248815
32. Højholdt A. Tværprofessionelt samarbejde - i teori og praksis. Vol. 3.
33. Ørtenblad L, Meillier L, Jønsson AR. Multi-morbidity: a patient perspective on navigating the health care system and everyday life. Chronic Illness. 2018;14(4):271–282. doi:10.1177/1742395317731607
34. Balint E. The possibilities of patient-centered medicine. J Royal College Gen Practitioners. 1969;17(82):269.
35. Dahl Steffensen K, Mølri Knudsen B, Finderup J, Willemann Würgler M, Olling K. Implementation of patient-centred care in Denmark - The way forward with shared decision making. Zeitschrift Evidenz Fortbildung Qualitat Gesundheitswesen. 2022;171:36–41. doi:10.1016/j.zefq.2022.04.005
36. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Internal Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
37. Olesen CV, Jensen KM, Olling K. Sygeplejersken som en ressource for implementering af fælles beslutningstagning (The nurse as a resource for implementation of Shared Decision Making). Fag og Forskning. 2020;3:58–63.
38. Aberdeen T, Yin RK. Case study research: design and methods. Canad J Action Res. 2013;14(1):69–71. doi:10.33524/cjar.v14i1.73
39. Gerring J. What is a case study and what is it good for? Am Political Sci Rev. 2004;98(2):341–354. doi:10.1017/S0003055404001182
40. Baxter P, Jack S. Qualitative case study methodology: study design and implementation for novice researchers. Qual Rep. 2008;13(4):544–559.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.