Back to Journals » Drug Design, Development and Therapy » Volume 19
Enhanced Nutritional Support May Ameliorate Rivaroxaban-Related Rapid Renal Function Decline: New Insights from a Real-World Study
Authors Meng C, Li L, Han Y, Zhang X, Lin Y, Liu H ![]() , Jiang S, Yan T, Zhang L, Chang B, Zhou X, Jia J
, Jiang S, Yan T, Zhang L, Chang B, Zhou X, Jia J
Received 29 August 2025
Accepted for publication 27 November 2025
Published 3 December 2025 Volume 2025:19 Pages 10691—10701
DOI https://doi.org/10.2147/DDDT.S564100
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Cheng Meng,1,* Linjie Li,2,* Ying Han,2,* Xinxin Zhang,1 Yujia Lin,1 Hangkuan Liu,2 Shichen Jiang,2 Tiekun Yan,1 Lirong Zhang,3 Baocheng Chang,4 Xin Zhou,2 Junya Jia1
1Department of Nephrology, Kidney Disease Medical Center, General Hospital, Tianjin Medical University, National Key Clinical Specialty, Tianjin Key Medical Discipline, Tianjin, People’s Republic of China; 2Department of Cardiology, Tianjin Medical University General Hospital, Tianjin, 300052, People’s Republic of China; 3Department of Biochemistry and Molecular Biology, School of Basic Medical Sciences, Tianjin Medical University, Tianjin, People’s Republic of China; 4NHC Key Laboratory of Hormones and Development, Tianjin Key Laboratory of Metabolic Diseases, Chu Hsien-I Memorial Hospital & Tianjin Institute of Endocrinology, Tianjin Medical University, Tianjin, 300134, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Junya Jia, Email [email protected] Xin Zhou, Email [email protected]
Aim: Aim to compare the effects of rivaroxaban and warfarin on rapid renal function decline.
Methods: 8842 patients from the Tianjin Health and Medical Data Platform, with a 2.3 years median follow-up (interquartile range,1.5– 3.4), were assigned to either the warfarin group (n = 3913) or rivaroxaban group (n = 4929). Logistic models, inverse probability of treatment weighting(IPTW), and propensity score-matched (PSM) analyses were employed to compare the risk of rapid renal function decline associated with rivaroxaban versus warfarin. The multivariable fractional polynomial interaction(MFPI) was used to investigate interactions between continuous variables and the adverse outcome. Restricted cubic splines(RCS) were applied to assess the relationship between the prognostic nutritional index (PNI) score and the adverse outcome.
Results: Rivaroxaban was associated with an increased risk of rapid renal function decline compared with warfarin in both the univariate (odds ratio [OR], 1.24; 95% confidence interval [CI], 1.14– 1.36; P < 0.001) and multivariate (OR, 1.17; 95% CI, 1.07– 1.29; P = 0.001) logistic models. Similar trends were observed in the IPTW (OR, 1.16; 95% CI, 1.09– 1.33; P < 0.001), PSM model (OR, 1.21; 95% CI, 1.09– 1.33; P < 0.001), and all subgroup analyses. In the MFPI analysis, the adverse outcome was significantly alleviated with an increasing PNI score (threshold at PNI score of 50, P = 0.039). A linear negative relationship (P for nonlinearity = 0.221) between the PNI score and rapid renal function decline was observed in patients receiving rivaroxaban.
Conclusion: Rivaroxaban was associated with a higher risk of rapid renal function decline than warfarin. Enhanced nutritional support may help mitigate this adverse outcome.
Keywords: rivaroxaban, warfarin, rapid renal function decline, nutritional support
Introduction
Over the past decade, the rise of direct oral anticoagulants (DOACs) has reshaped the anticoagulant therapy landscape. Their safety has been shown to be non-inferior in various settings and, for some indications, superior to warfarin in both safety and efficacy. Between 2011 and 2020, the use of DOACs in patients with atrial fibrillation rose significantly from 4.7% to 47.9%, while warfarin use declined from 52.4% to 17.7%.1 Major guidelines recommend DOAC therapy over warfarin because of its higher safety profile and greater convenience, particularly by reducing the need for routine monitoring and dietary restrictions.2–9 Nevertheless, increasing reports of DOAC-related renal function decline have raised growing concerns.
Studies focusing on apixaban10 and dabigatran11 are being increasingly performed, and most of them are case reports. However, the role of rivaroxaban in renal function decline has received little attention. Rivaroxaban is a direct factor Xa inhibitor that has been studied in the treating various thromboembolic and atherosclerotic conditions.12 Presently, it is mainly used for the treatment of nonvalvular atrial fibrillation and deep vein thrombosis, and its use in vascular diseases is increasing.13
Because DOAC-related renal function decline is an underestimated event, prescribers may not realize the potential renal impairment related to DOACs, especially rivaroxaban. Delayed recognition of DOAC-related renal function decline could lead to irreversible renal damage if the drug is not promptly discontinued or switched to another therapy. A meta-analysis suggested that only 40% of patients experienced kidney function recovery after discontinuation of anticoagulant therapy, while most patients did not.14 Furthermore, recent studies have shown that DOAC-related renal function decline may be related to continuous lysis of red blood cells, leading to the intratubular obstruction and accumulation of heme molecules and catalytic iron, thereby generating harmful hydroxyl radicals.14 How to reduce the incidence of renal function decline and optimize the therapeutic effect of rivaroxaban has become an urgent issue. We performed the present study to guide more effectively the clinical application of rivaroxaban and improve patients’ quality of life.
Methods
Study Design and Population
Tianjin, located in northern China, has a population of 13.9 million. This study utilized data from the Tianjin Health and Medical Data Platform (THMDP), which includes comprehensive healthcare records from 42 (100%) of 42 tertiary general hospitals, 261 (97.8%) of 267 community healthcare centers, and 36 (66.7%) of 54 secondary hospitals across Tianjin. The THMDP database contains inpatient, outpatient, and mortality records from these facilities. Key data elements included are as follows: essential demographic information (eg, age, sex, marital status); diagnoses, categorized under the International Classification of Diseases, Tenth Revision (ICD-10), using the National Clinical Edition 2 ICD Dictionary; prescription details; clinical laboratory results; procedural codes; and outcomes such as mortality rates, discharge statuses, and hospital stay durations. Each patient is assigned a unique identifier, enabling the correlation of multiple visits by the same patient (details are available in our previously published research15). To protect patient privacy, all personal information is encrypted. Use of the THMDP was approved by the Tianjin Health Commission, and the analysis scheme was approved by the Ethics Committee of Tianjin Medical University General Hospital (No. IRB2022-YX-235-01). This study complies with the Declaration of Helsinki.
We established a cohort based on the THMDP database, aiming to enroll 68,809 new oral anticoagulant users (including warfarin, dabigatran, rivaroxaban, apixaban, and endoxaban) between January 2015 and June 2020. After excluding 42,239 patients with missing creatinine data, 16,329 patients with a creatinine test interval of < 1 year, 2 patients aged < 18 years, 824 patients using other oral anticoagulants (dabigatran, apixaban, or endoxaban), and 582 patients with end-stage renal disease, 8842 patients were enrolled in this study. The selection process is illustrated in Figure 1.
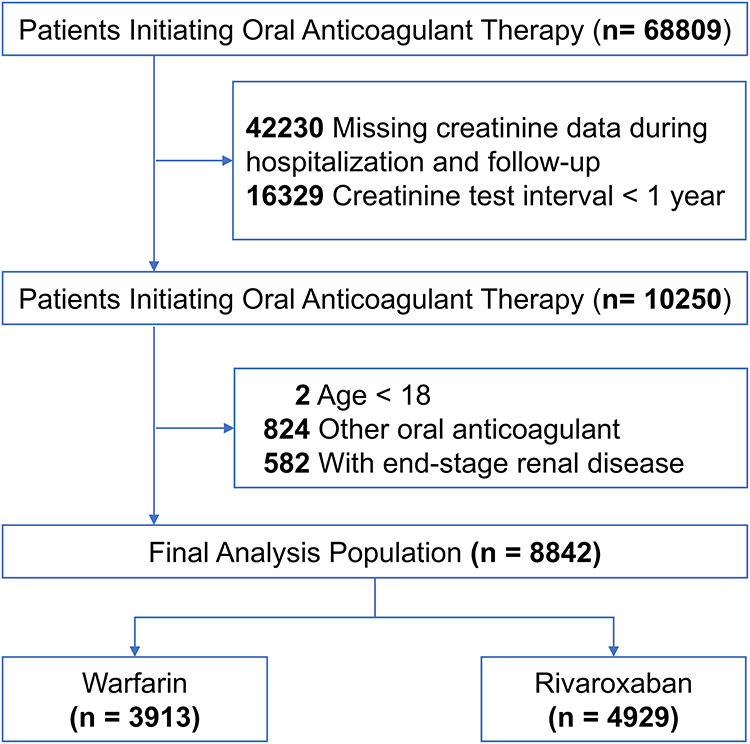 |
Figure 1 Inclusion and exclusion flowchart. |
Definition of Outcomes
The eGFR was calculated according to the 2012 clinical practice guidelines, Kidney Disease: Improving Global Outcomes (KDIGO), and the Chronic Kidney Disease Epidemiology Collaboration formula.16,17 The eGFR slope was calculated for each patient using the difference between the last and first eGFR measurements divided by the time interval (in years) between these two measurements. Rapid renal function decline was defined as an annual eGFR decrease of > 3 mL/min/1.73 m2.18
Study Variables
Covariates were as follows: patient demographics [age, sex, current drinking, daily smoking, and local resident], treatment indication [atrial fibrillation (AF), venous thromboembolism (VTE), and others], past medical history, clinical characteristics [estimated glomerular filtration rate (eGFR), lymphocyte count.
(PCS/uL), serum albumin and prognostic nutritional index (PNI) score], and previous medication use [antiplatelet agents, statins, angiotensin-converting enzyme inhibitor (ACEI)/angiotensin II receptor blocker (ARB), β-blocker, and antidiabetic drug]. The study used ICD-10 codes to identify prior disease history from the day of study entry or earlier. Definitions of the study variables and outcomes are provided in Table S1 and Table S2.
Statistical Analyses
For normally distributed data, variables are reported as mean ± standard deviation. For non-parametric data, variables are reported as the median of the quartile range. Categorical variables are expressed as percentages. Using Fisher exact test to compare the differences between the binomial data, and the Mann–Whitney U-test and unpaired t test were used to compare the continuous variables with skewed distribution and normal distribution, respectively.
First, we presented the distribution of the annual decline in the eGFR using a histogram (Figure S1). To explore the relationship between the type of anticoagulant (rivaroxaban vs warfarin) and the decline in the eGFR, we used warfarin as the reference in the following four models: a univariable logistic model, a multivariable adjusted logistic model, IPTW, and PSM analysis with maximum 1-to-1 matching. The OR and CI were calculated. The multivariable logistic model was applied to adjust for as many clinically relevant confounding variables as possible, providing a more accurate estimate of the independent effect of rivaroxaban. In addition, to further reduce selection bias and strengthen the robustness of the findings, we employed IPTW and PSM methods. These approaches allowed us to balance baseline covariates between treatment groups by assigning weights based on propensity scores (IPTW) or by matching patients with similar characteristics (PSM), thus mimicking the conditions of a randomized controlled trial as closely as possible. PSM was performed using the “calipmath” command in STATA with a greedy matching algorithm and no replacement. A caliper width of 0.2 of the standard deviation of the logarithm of the propensity score was used for all matching. To assess the adequacy of matching, absolute standardized differences in baseline covariates were calculated pre- and post-matching, with covariates having less a < 10% difference after matching considered adequately matched.
We performed interaction tests and subgroup analyses on the entire cohort. For continuous variables, we applied the MFPI to explore potential interactions between continuous variables and the type of anticoagulant (rivaroxaban vs warfarin) in relation to rapid renal function decline.
Considering the impact of different PNI scores on the effect of anticoagulants on eGFR decline, we further evaluated the effect of PNI scores on rapid renal function decline in the rivaroxaban population, to identify potential risk thresholds. Restricted cubic splines in the multivariable adjusted logistic model were used to assess the association between PNI scores and the risk of eGFR decline. The “xblc” command in STATA was used to estimate the OR for the association between PNI scores and the risk of eGFR decline.
The missing rates are presented in Table S3. Statistical analysis was performed using STATA (version 16.0). Defined as significant as a P-value of < 0.05 in two-tailed tests.
Results
Characteristics of Patients
Totally, 8842 patients were evaluated (Figure 1). Of these, 3913 (44.3%) patients used warfarin and 4929 (55.7%) used rivaroxaban. The median follow-up was 2.3 years (1.5–3.4). The baseline characteristics are presented in Table 1. The median age was 67 years, and about half were men. Compared with the warfarin group, the rivaroxaban group was slightly older (mean age 69 years) and had a higher prevalence of comorbidities such as hypertension (71.3% vs 66.5%), diabetes (16.6% vs 10.8%), ischemic stroke (14.5% vs 10.0%), and cancer (8.4% vs 5.1%), whereas the warfarin group had a higher rate of heart failure (48.7% vs 32.1%). The baseline eGFR was similar between the two groups (84.4 ± 19.1 vs 83.9 ± 19.6 mL/min/1.73 m2; P = 0.24). The average annual decrease in the eGFR across the entire population was 2.09 mL/min/1.73 m2 (1.75 and 2.36 mL/min/1.73 m2 in the warfarin and rivaroxaban groups, respectively; P = 0.001).
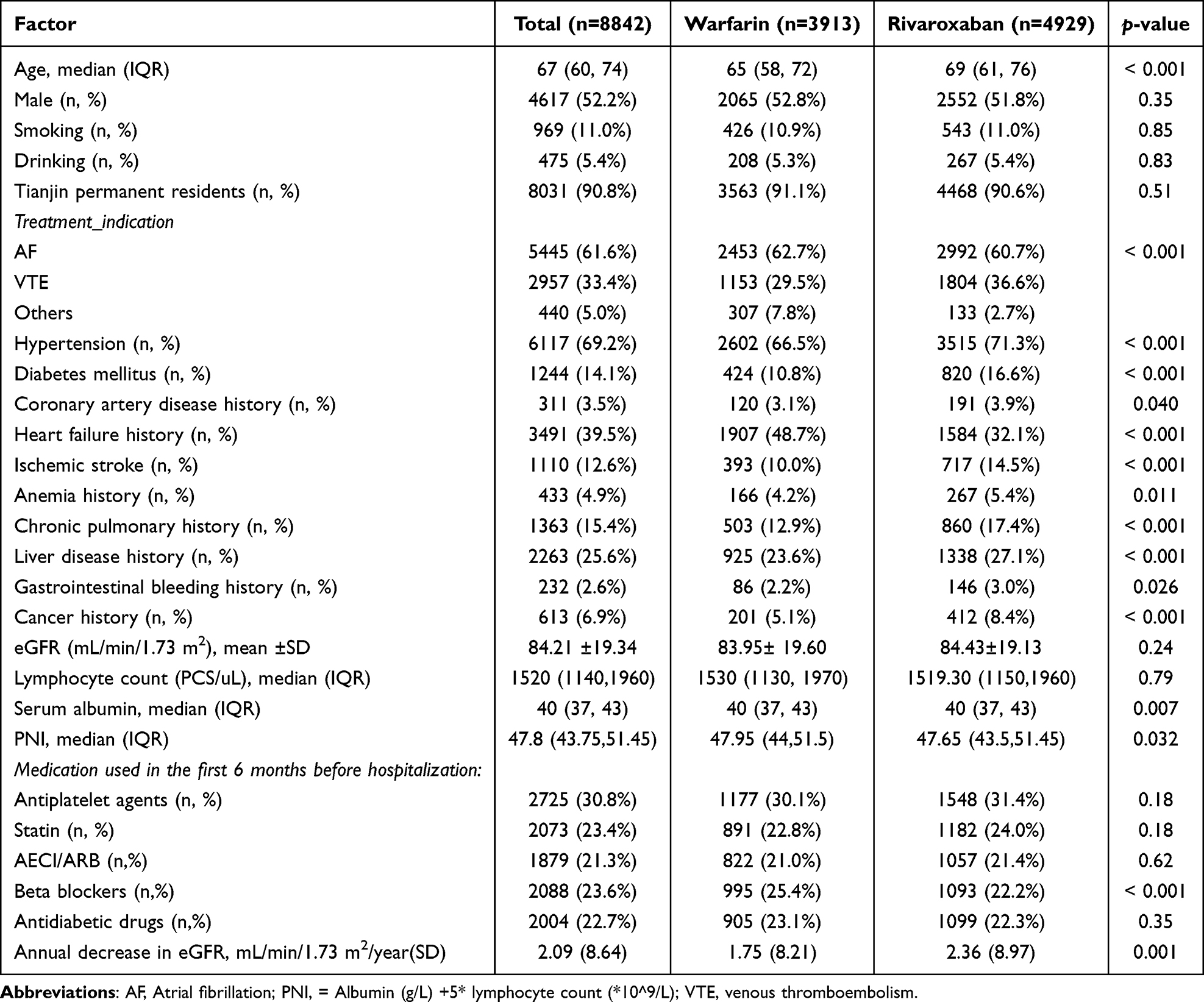 |
Table 1 Patient Characteristics |
Effects of Rivaroxaban and Warfarin on Risk of Rapid Renal Function Decline in Different Models
Rapid renal function decline was analyzed as a binary variable. In the entire cohort, rapid renal function decline occurred in 3249 (36.7%) patients, including 1921 (39.0%) in the rivaroxaban group and 1328 (33.9%) in the warfarin group. As shown in Figure 2, rivaroxaban was associated with a higher risk of rapid renal function decline than was warfarin in the univariate logistic model (OR, 1.24; 95% CI, 1.14–1.36; P < 0.001). This association was statistically significant after multivariate analysis (OR, 1.17; 95% CI, 1.07–1.29; P = 0.001). Similarly, the inverse probability of treatment weighting model (OR, 1.16; 95% CI, 1.09–1.24; P < 0.001) and the PSM model (OR, 1.21; 95% CI, 1.09–1.33; P < 0.001) demonstrated the same trend. The covariate balance after propensity score matching is presented in Table S4, and all covariates showed absolute standardized differences of less than 10%, indicating adequate matching between the two groups.
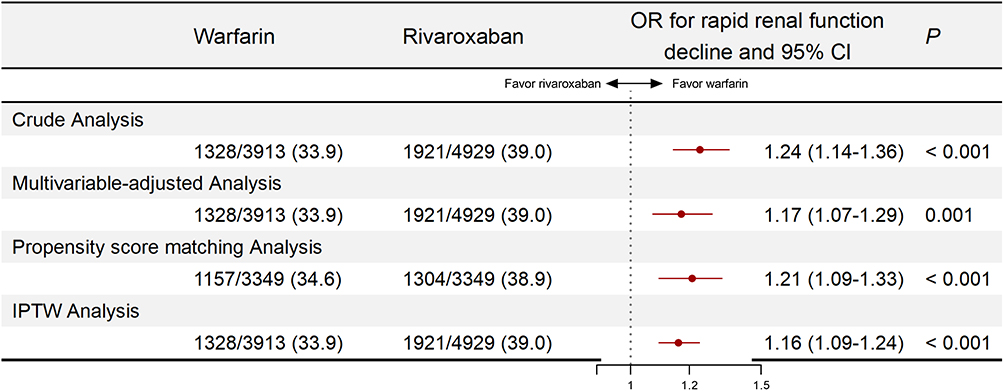 |
Figure 2 Comparison of rivaroxaban and warfarin in the risk of rapid renal function decline in different models. |
Subgroup Analyses
Our results showed a consistent increase in the risk of rapid renal function decline in patients using rivaroxaban compared with those using warfarin across all subgroups (Figure 3). All interaction P values exceeded 0.05, suggesting no significant heterogeneity across subgroups.
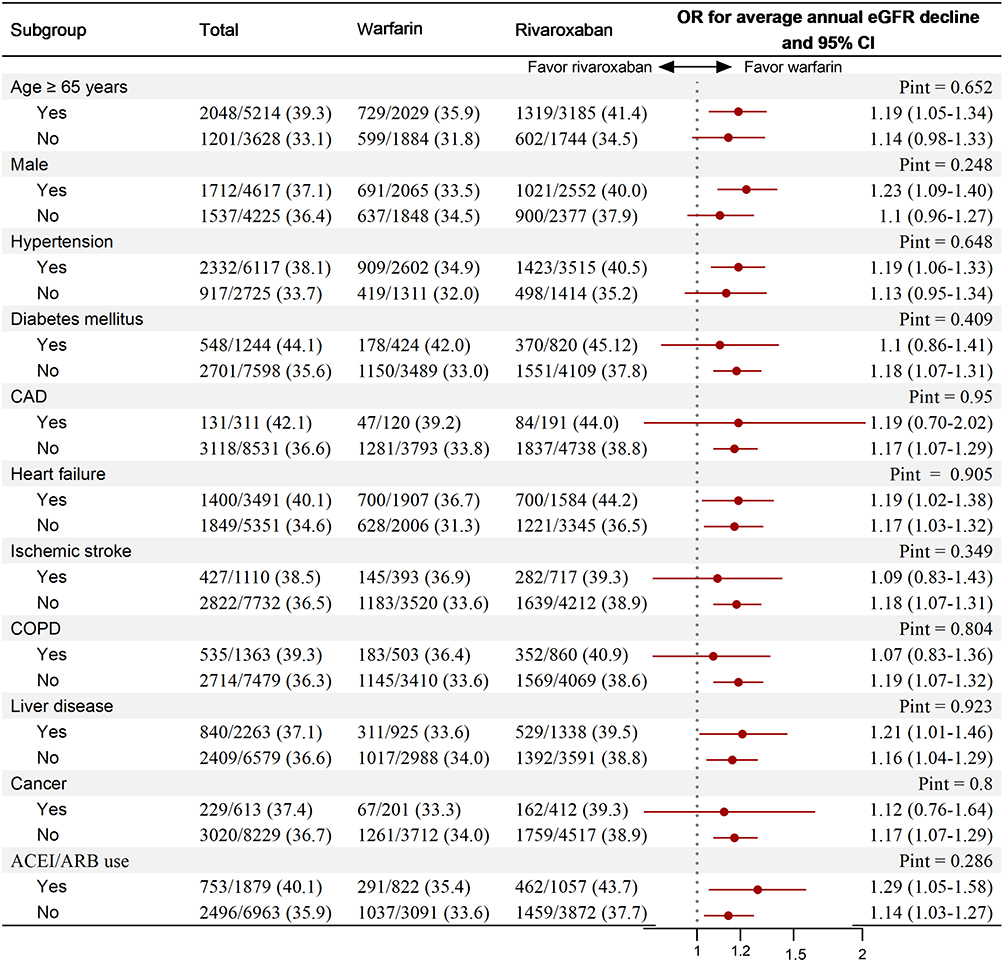 |
Figure 3 Rivaroxaban versus warfarin on the risk of rapid renal decline in different subgroups. Abbreviations: CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease. |
Effect of Continuous Variables on Rivaroxaban-Related Rapid Renal Function Decline
In the multivariable fractional polynomial interaction analysis (Figure 4), we compared the relative risk differences between rivaroxaban and warfarin across varying levels of low-density lipoprotein cholesterol, systolic blood pressure, baseline eGFR, and PNI. The results showed that neither low-density lipoprotein cholesterol concentration nor baseline eGFR significantly influenced the association between rivaroxaban use and rapid renal function decline (P = 0.744 and P = 0.727, respectively). Although not statistically significant (P = 0.529), we observed that a decrease in systolic blood pressure attenuated the risk of rivaroxaban-related rapid renal function decline, particularly below 120 mmHg. Notably, an increase in the PNI score also attenuated the risk, with a threshold observed at a PNI score of 50 and a significant interaction (P = 0.039). According to subgroup analyses stratified by PNI, rivaroxaban use was associated with a higher risk of renal function decline compared with warfarin when the PNI was below 50 (OR, 1.25; 95% CI, 1.12–1.40; P < 0.001), whereas no significant difference was observed between the two groups when the PNI exceeded 50 (OR, 1.04; 95% CI, 0.88–1.22; P = 0.661).
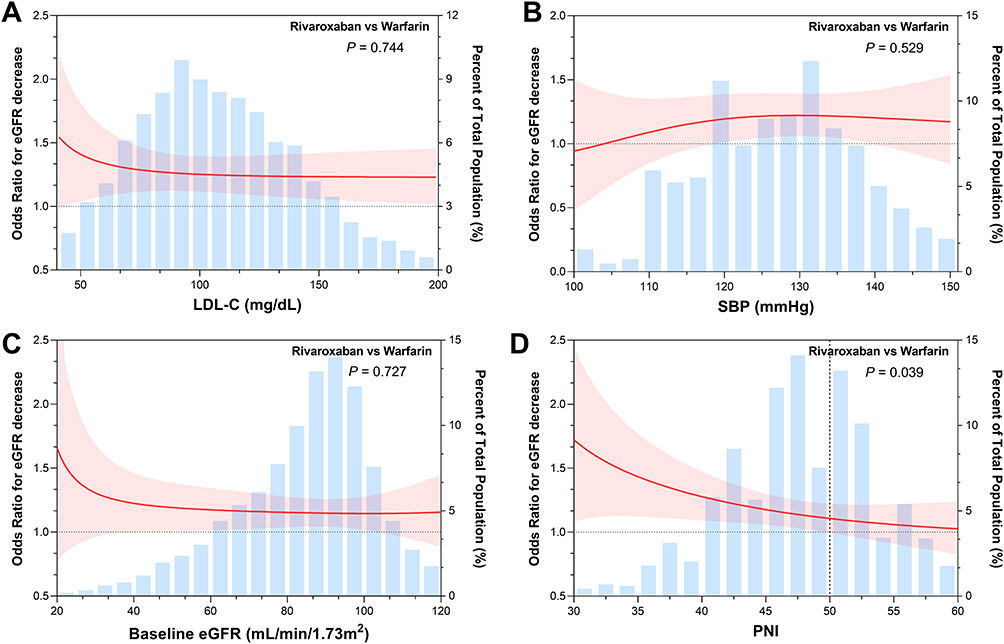 |
Figure 4 Effect of LDL-C (A), SBP (B), baseline eGFR (C) and PNI (D) on rivaroxaban-related rapid renal function decline. Abbreviations: LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure. |
Associations Between PNI Score and Rivaroxaban-Related Rapid Renal Function Decline
Finally, restricted cubic spline curves were used to assess the association between PNI scores and rapid renal function decline among patients using rivaroxaban (Figure 5). A linear negative relationship was observed (P for nonlinearity = 0.221) between PNI scores and the risk of rapid renal function decline. As the PNI increased, the risk of renal function decline gradually decreased among patients receiving rivaroxaban. A PNI score of 50 was identified as the threshold associated with an increased risk of rapid renal function decline.
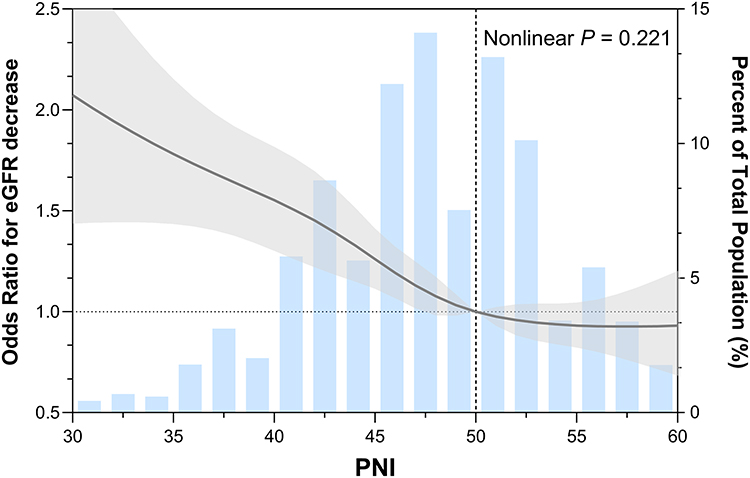 |
Figure 5 The restricted cubic splines in the multivariable adjusted logistic model assessed the relationship between PNI and the risk of rapid renal function decline. |
Discussion
In our multicenter cohort, rivaroxaban was associated with a higher risk of rapid renal function decline than was warfarin across different model analyses. Further analyses revealed a noteworthy linear negative correlation between the PNI score and this adverse outcome, suggesting that improved nutritional support could help reduce the incidence of rapid renal function decline, enhance the prognosis, and optimize the therapeutic effect of rivaroxaban.
As DOAC usage continues to rise,19 concerns are growing about the risk of renal function decline associated with their use. From 2020 to date, 65 cases of anticoagulation-related renal function decline have been reported in the FDA Adverse Event Reporting System public dashboard: 49% of these cases involved warfarin, 14% dabigatran, 11% rivaroxaban, and 8% edoxaban. However, the current incidence of this condition in patients using DOACs remains unclear.20 With the growing use of DOACs in patients with end-stage renal disease, failure to recognize their increased risk of chronic kidney disease (CKD) could result in worse outcomes. In this study, we found that rivaroxaban had a significantly more harmful effect on rapid renal function decline, as compared to warfarin, supported by multiple models and subgroup analyses. Given the widespread global use of rivaroxaban and the limited reports of rapid renal decline, our findings should prompt clinicians to monitor patients carefully and consider reducing or discontinuing the drug when appropriate. Another retrospective meta-analysis of 24 cases reported that kidney recovery occurred in only 40% of patients after discontinuation of anticoagulation therapy, with the majority of patients failing to regain renal function.14 This underscores the urgent need to explore the mechanisms underlying rivaroxaban-related renal function decline and to identify potential treatment targets.
The mechanism underlying rivaroxaban-related rapid renal function decline is still unknown, but nephron damage appears to have an obstructive etiology. This includes the formation of red blood cell casts that cause obstruction and further damage to the nephron. Additionally, the ongoing lysis of red blood cells leads to the accumulation of heme-containing molecules and catalytic iron, which generate harmful hydroxyl radicals.14 From the perspective of common risk factors, major contributors to renal function decline include advanced age, diabetes, hypertension, and heart failure,21,22 which may also important in the onset of rapid renal function decline.
Because anticoagulant therapy is often lifelong, preserving renal function has become a critical issue in the management of patients with anticoagulant treatment.23 Recently, a study revealed that in patients suffered from CKD, lower dietary protein intake (< 92 g/day) rather than higher intake (> 163 g/day) was associated with renal function decline.24 This highlights the importance of enhanced nutritional support for these patients.
In a recent study, the PNI score was associated with the prevalence of CKD, whereas hypoalbuminemia was not. The PNI is a lymphocyte- and albumin-based index designed to reflect robustly an individual’s immune and nutritional status. Emerging evidence suggests that the PNI score could predict the prognosis of cancer,25–28 cardiovascular disease,29,30 and renal injury.31 Furthermore, a low PNI score is related to death in patients with CKD.32,33 Other studies have shown that the PNI score is an independent predictor of all-cause mortality in patients with diabetic kidney disease, possibly because this score serves as a more comprehensive marker than the albumin concentration or lymphocyte count alone. The PNI score integrates immune, nutritional, and chronic inflammatory factors,30 which are important drivers of disease. In fact, patients with atrial fibrillation and renal injury are usually in a highly inflammatory state, which could significantly deteriorate their nutritional status. Therefore, PNI, which represents nutritional status and chronic inflammation, may be applicable to the clinical management of these patients.30 In this study, we also found that lower PNI scores promote rapid renal function decline. When the PNI score is > 50, it significantly slows the rate of renal function decline, underscoring the importance of enhanced nutritional support, such as maintaining proper BMI and hemoglobin levels.30 Besides, high quality protein and foods rich in antioxidants, and appropriate supplementary keto acid analogues also benefits of nutritional support. This finding has potential implications for the clinical application of rivaroxaban, suggesting that enhanced nutritional support could optimize its therapeutic effect and improve the disease prognosis. Additionally, although not statistically significant, we observed that, as the systolic blood pressure decreased, the risk of rapid renal function decline associated with rivaroxaban was attenuated, particularly below 120 mmHg. This finding highlights the potential importance of intensive antihypertensive therapy in the anticoagulant patients. In view of the low plasma albumin level and hypertension in most patients in this study, our conclusions provide feasible options to some extent, such as strengthening nutritional support and maintaining good blood pressure.
The major advantage of this research is its use of electronic medical record data, which reflect real-world clinical practice and provide sufficient power to examine the relationship between anticoagulants and the adverse outcomes. However, the study had three main limitations. Firstly, because this was an observational study, residual confounding due to unmeasured or unknown factors cannot be fully excluded despite the use of multiple adjustment methods. We were unable to establish a causal relationship between anticoagulants and the risk of rapid renal function decline. Additionally, we excluded patients without creatinine records during follow-up, which may have introduced potential bias. Besides, as the data is from an electronic medical record system, there is a lack of detailed records of nutritional descriptions, making it difficult to conduct a more detailed analysis of the patient’s nutritional imbalance.
Conclusion
In a word, this multicenter study provides valuable insight into the harmful effects of rivaroxaban on rapid renal function decline and highlights the importance of maintaining a proper nutritional status, which may also enhance the effectiveness of rivaroxaban treatment. Nevertheless, these findings require further validation in prospective studies, with longer follow-up periods.
Data Sharing Statement
The datasets supporting the conclusions of this article are included within the article and its additional files. All authors agree to share the primary research data used in support of the key conclusions.
All experiments were performed in accordance with relevant guidelines and regulations. The institutional and licensing committee approved all experiments, including any relevant details.
Ethics Approval and Consent to Participate
THMDP has been approved for use by Tianjin Health Commission, and the analysis scheme has been approved by the Ethics Committee of Tianjin Medical University General Hospital (No. IRB2022-YX-235-01).
Acknowledgments
The authors are grateful to the research team of the Department of Nephrology and the Department of Cardiology at the Tianjin Medical University General Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Tianjin Health Research Project (Grant No.TJWJ2025QN014) and Tianjin Education Commission Research Project (2024KJ165).
Disclosure
There is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
References
1. Navar AM, Kolkailah AA, Overton R, et al. Trends in oral anticoagulant use among 436 864 patients with atrial fibrillation in community practice, 2011 to 2020. J Am Heart Assoc. 2022;11(22):e026723. doi:10.1161/JAHA.122.026723
2. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981–992. doi:10.1056/NEJMoa1107039
3. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361(12):1139–1151. doi:10.1056/NEJMoa0905561
4. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883–891. doi:10.1056/NEJMoa1009638
5. Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369(22):2093–2104. doi:10.1056/NEJMoa1310907
6. Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955–962. doi:10.1016/S0140-6736(13)62343-0
7. Chatterjee S, Sardar P, Biondi-Zoccai G, Kumbhani DJ. New oral anticoagulants and the risk of intracranial hemorrhage: traditional and Bayesian meta-analysis and mixed treatment comparison of randomized trials of new oral anticoagulants in atrial fibrillation. JAMA Neurol. 2013;70(12):1486–1490. doi:10.1001/jamaneurol.2013.4021
8. Salazar CA, Del Aguila D, Cordova EG. Direct thrombin inhibitors versus vitamin K antagonists for preventing cerebral or systemic embolism in people with non-valvular atrial fibrillation. Cochrane Database Syst Rev. 2014;2014(3):Cd009893. doi:10.1002/14651858.CD009893.pub2
9. Bruins Slot KM, Berge E. Factor Xa inhibitors versus vitamin K antagonists for preventing cerebral or systemic embolism in patients with atrial fibrillation. Cochrane Database Syst Rev. 2018;3(3):Cd008980. doi:10.1002/14651858.CD008980.pub3
10. Brodsky SV, Mhaskar NS, Thiruveedi S, et al. Acute kidney injury aggravated by treatment initiation with apixaban: Another twist of anticoagulant-related nephropathy. Kidney Res Clin Pract. 2017;36(4):387–392. doi:10.23876/j.krcp.2017.36.4.387
11. Böhm M, Ezekowitz MD, Connolly SJ, et al. Changes in renal function in patients with atrial fibrillation: an analysis from the RE-LY trial. J Am Coll Cardiol. 2015;65(23):2481–2493. doi:10.1016/j.jacc.2015.03.577
12. Mueck W, Stampfuss J, Kubitza D, Becka M. Clinical pharmacokinetic and pharmacodynamic profile of rivaroxaban. Clin Pharmacokinet. 2014;53(1):1–16. doi:10.1007/s40262-013-0100-7
13. Ajmal M, Friedman J, Sipra Q, Lassar T. Rivaroxaban: expanded role in cardiovascular disease management-a literature review. Cardiovasc Ther. 2021;2021:8886210. doi:10.1155/2021/8886210
14. Chen S, Liao D, Yang M, Wang S. Anticoagulant-related nephropathy induced by direct-acting oral anticoagulants: clinical characteristics, treatments and outcomes. Thromb Res. 2023;222:20–23. doi:10.1016/j.thromres.2022.12.002
15. Liu Y, Li L, Li J, et al. Development and validation of a predictive model for intracranial haemorrhage in patients on direct oral anticoagulants. Clin Appl Thromb Hemost. 2024;30:10760296241271338. doi:10.1177/10760296241271338
16. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
17. Stevens PE, Levin A. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013;158(11):825–830. doi:10.7326/0003-4819-158-11-201306040-00007
18. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. Chapter 2: definition, identification, and prediction of CKD progression. Kidney Int Suppl. 2013;3(1):63–72. doi:10.1038/kisup.2012.65
19. Shaw JR, Castellucci LA, Siegal D, Carrier M. DOAC-associated bleeding, hemostatic strategies, and thrombin generation assays - a review of the literature. J Thromb Haemost. 2023;21(3):433–452. doi:10.1016/j.jtha.2022.11.029
20. Brodsky SV, Nadasdy T, Rovin BH, et al. Warfarin-related nephropathy occurs in patients with and without chronic kidney disease and is associated with an increased mortality rate. Kidney Int. 2011;80(2):181–189. doi:10.1038/ki.2011.44
21. Lim AK, Campbell DA. Haematuria and acute kidney injury in elderly patients admitted to hospital with supratherapeutic warfarin anticoagulation. Int Urol Nephrol. 2013;45(2):561–570. doi:10.1007/s11255-012-0364-0
22. Brodsky SV, Collins M, Park E, et al. Warfarin therapy that results in an international normalization ratio above the therapeutic range is associated with accelerated progression of chronic kidney disease. Nephron Clin Pract. 2010;115(2):c142–146. doi:10.1159/000312877
23. Lee SR, Choi EK, Park SH, et al. Renal outcomes of rivaroxaban compared with warfarin in Asian patients with nonvalvular atrial fibrillation: a nationwide population-based cohort study. Front Cardiovasc Med. 2023;10:1040834. doi:10.3389/fcvm.2023.1040834
24. Zhang J, Chen Y, Zou L, Gong R. Prognostic nutritional index as a risk factor for diabetic kidney disease and mortality in patients with type 2 diabetes mellitus. Acta Diabetol. 2023;60(2):235–245. doi:10.1007/s00592-022-01985-x
25. Wang D, Hu X, Xiao L, et al. Prognostic nutritional index and systemic immune-inflammation index predict the prognosis of patients with HCC. J Gastrointest Surg. 2021;25(2):421–427. doi:10.1007/s11605-019-04492-7
26. Onodera T, Goseki N, Kosaki G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi. 1984;85(9):1001–1005.
27. Mirili C, Yılmaz A, Demirkan S, Bilici M, Basol Tekin S. Clinical significance of prognostic nutritional index (PNI) in malignant melanoma. Int J Clin Oncol. 2019;24(10):1301–1310. doi:10.1007/s10147-019-01461-7
28. Yamamoto T, Kawada K, Obama K. Inflammation-related biomarkers for the prediction of prognosis in colorectal cancer patients. Int J Mol Sci. 2021;22(15):8002.
29. Zencirkiran Agus H, Kahraman S. Prognostic nutritional index predicts one-year outcome in heart failure with preserved ejection fraction. Acta Cardiol. 2020;75(5):450–455. doi:10.1080/00015385.2019.1661139
30. Hu Y, Cao Q, Wang H, et al. Prognostic nutritional index predicts acute kidney injury and mortality of patients in the coronary care unit. Exp Ther Med. 2021;21(2):123. doi:10.3892/etm.2020.9555
31. Dong X, Wang B, Chen S, et al. Association between prognostic nutritional index and contrast-associated acute kidney injury in patients complicated with chronic kidney disease and coronary artery disease. J Interv Cardiol. 2021;2021:2274430. doi:10.1155/2021/2274430
32. Zhang H, Tao Y, Wang Z, Lu J. Evaluation of nutritional status and prognostic impact assessed by the prognostic nutritional index in children with chronic kidney disease. Medicine. 2019;98(34):e16713. doi:10.1097/MD.0000000000016713
33. Barutcu Atas D, Tugcu M, Asicioglu E, et al. Prognostic nutritional index is a predictor of mortality in elderly patients with chronic kidney disease. Int Urol Nephrol. 2022;54(5):1155–1162. doi:10.1007/s11255-021-03002-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.