Back to Journals » International Journal of Nanomedicine » Volume 21
Engineering Multi-Scale Transdermal Delivery Systems for Atopic Dermatitis: Emerging Insights from the Gut–Skin Axis
Authors Teng C, He M, Tang Y, Zhang Q, Song Z, Xu Y, Du H, An X, Yang Y ![]() , Feng L
, Feng L
Received 9 February 2026
Accepted for publication 7 July 2026
Published 15 July 2026 Volume 2026:21 602330
DOI https://doi.org/10.2147/IJN.S602330
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jie Huang
Chi Teng,1 Miao He,2 Yufang Tang,2 Qingya Zhang,1 Zimeng Song,1 Yaru Xu,1 Haoyang Du,1 Xiaohong An,3 Yanjun Yang,1 Liang Feng1
1School of Traditional Chinese Pharmacy, China Pharmaceutical University, Nanjing, 211198, People’s Republic of China; 2School of Pharmacy, Yunnan Provincial Key Laboratory of Entomological Biopharmaceutical R&D, Dali University, Dali, Yunnan, 671003, People’s Republic of China; 3Yunnan Characteristic Plant Extraction Laboratory Co., Ltd., Kunming, Yunnan, 650106, People’s Republic of China
Correspondence: Liang Feng, Email [email protected] Yanjun Yang, Email [email protected]
Abstract: Atopic dermatitis (AD) is a chronic, recurrent inflammatory skin disease, for which traditional treatments are constrained by limited efficacy, high relapse rates, and poor long-term safety. The gut–skin axis has emerged as a critical regulatory network linking intestinal homeostasis and skin health, and is increasingly recognized as a potential contributor to the onset and progression of AD. It plays a multifaceted regulatory role in maintaining immune homeostasis, reconstructing barrier functions, and mediating microbial metabolite signaling. Within this conceptual framework, this review summarizes recent advances in multi-scale transdermal delivery strategies for AD. It particularly emphasizes the unique value of multi-scale transdermal delivery strategies of active components in traditional Chinese medicine (TCM) in immune balance and barrier repair. Building on this, we highlight the integrated innovation of modern delivery technologies, emphasizing the unique advantages of multiscale transdermal systems in regulating the skin barrier, improving active components bioavailability, and modulating cross-compartment biological signaling. Importantly, while emerging studies suggest potential interactions between transdermal delivery systems and gut–skin axis-related pathways, experimentally validated evidence directly linking multi-scale transdermal systems with gut–skin axis regulation remains limited. Therefore, this review also critically discusses current knowledge gaps and highlights the need for further mechanistic and experimental validation. Unlike prior reviews centered on single mechanisms or delivery methods, this work provides a structured overview of active components, intestinal–cutaneous communication, and multi-scale delivery technologies, and proposes a conceptual framework for their potential integration. This perspective aims to support future experimental efforts toward establishing a mechanistically validated link between advanced transdermal systems and gut–skin axis regulation, facilitating the translation of TCM-derived bioactive compounds combined with advanced delivery platforms for AD treatment.
Keywords: atopic dermatitis, gut-skin axis, barrier repair, immune homeostasis, multiscale transdermal delivery
Introduction
AD is a chronic inflammatory skin disease driven by multiple factors including genetics, immunity, and environment. Its prevalence has been increasing globally year by year, particularly with an incidence rate of 15–20% among children, significantly impacting patients’ quality of life and imposing a substantial socioeconomic burden.1,2 The pathological mechanisms of AD are complex, encompassing impaired skin barrier function, Th2-biased immune dysregulation, and skin microbiome dysbiosis, among other factors (Figure 1).3,4 Although therapies such as glucocorticoids, calcineurin inhibitors, biologics, and emerging Janus kinase inhibitors can alleviate symptoms in the short term, long-term treatment is often accompanied by adverse effects, high costs, incomplete disease control, and poor patient compliance.5–7 Increasing evidence suggests that AD should not be regarded solely as a localized skin disorder but rather as a multifactorial disease involving coordinated dysfunction of epithelial barriers, immune networks, and microbial ecosystems.8,9 Therefore, developing safer and more precise therapeutic strategies capable of addressing these interconnected pathological processes remains a major challenge in AD management.
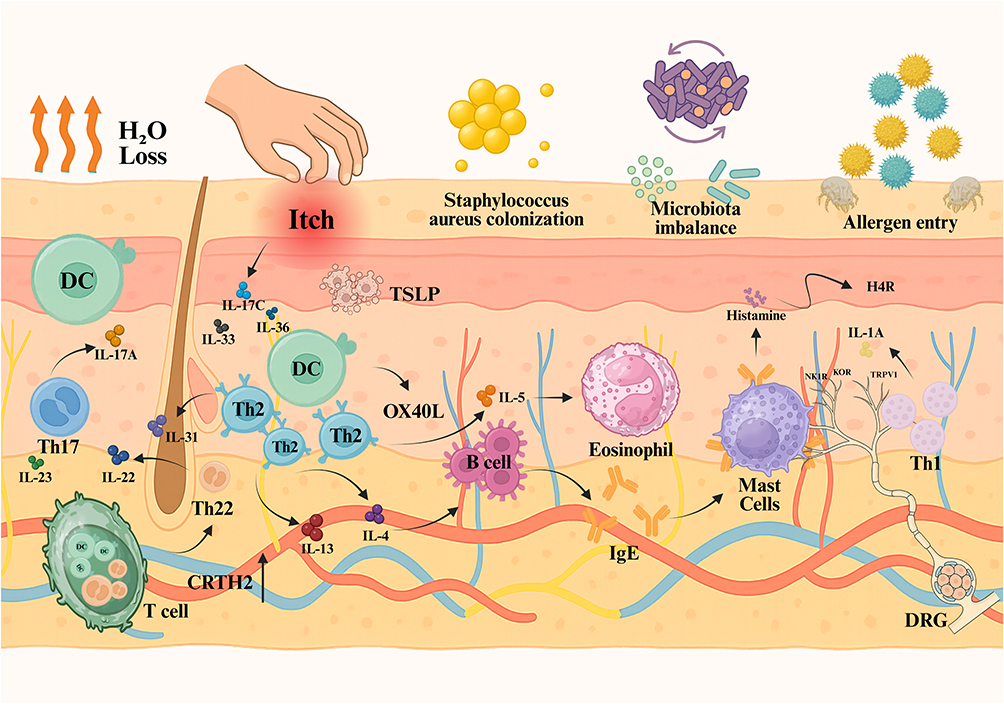 |
Figure 1 Schematic diagram of the pathological mechanism of AD. The damaged skin barrier activates keratinocytes, prompting them to produce TSLP, IL-23, and IL-33. Under these inflammatory stimuli, DC take up penetrating antigens and migrate to skin-draining lymph nodes, where they activate and induce T cells to differentiate into Th2 and Th22 subsets. Subsequently, Th2 lymphocytes promote the production of IgE by activated B cells. Factors released by inflammatory cells lead to edema, erythema, and pruritus. Abbreviations: TSLP, Thymic stromal lymphopoietin; OX40L, The tumor necrosis factor receptor OX40 ligand; IL-1α, Interleukin-1 alpha; IL-4, Interleukin-4; IL-5, Interleukin-5; IL-13, Interleukin-13; IL-17C, Interleukin-17C; IL-22, Interleukin-22; IL-23, Interleukin-23; IL-31, Interleukin-31; IL-33, Interleukin-33; IL-36, Interleukin-36; H4R, Histamine H4 Receptor; Th1, T helper 1 cell; DRG, Dorsal root ganglion; DC, Dendritic cell; IgE, Immunoglobulin E; CRTH2, Chemoattractant Receptor-homologous molecule expressed on Th2 cells; Th17, T helper 17 cell; Th22, T helper 22 cell; NK1R, Neurokinin-1 receptor; KOR, Kappa opioid receptor; TRPV1, Transient receptor potential vanilloid 1. Note: The black upward arrow in the figure indicates an upregulation of CRTH2 expression. |
Beyond cutaneous abnormalities, accumulating studies have revealed a close association between AD and disturbances in the gut microbiota–metabolite–immune network.10 Altered intestinal microbial composition, impaired intestinal barrier function, and reduced production of immunoregulatory metabolites, particularly short-chain fatty acids, can influence systemic immune responses and subsequently affect skin inflammation and barrier integrity.11 The concept of the gut–skin axis has therefore emerged as an important framework for understanding the bidirectional communication between intestinal homeostasis and cutaneous immunity. Importantly, variations in gut microbial composition among pediatric and adult AD patients may contribute to disease heterogeneity and therapeutic responsiveness, suggesting that local skin-targeted interventions alone may not fully address the complexity of AD pathogenesis. Consequently, integrating gut–skin axis-related regulatory concepts into therapeutic design has become an emerging direction for precision intervention in AD.
Given the aforementioned clinical and pathological challenges, transdermal drug delivery, as a strategy that directly targets the lesion, possesses inherent advantages—it can concentrate drugs within the epidermis and dermis while avoiding first-pass metabolism, thereby reducing systemic side effects and improving local therapeutic efficacy.12 However, the skin is a highly stratified and dynamic biological barrier with distinct molecular, nanoscale, and microscale structural characteristics.13 Moreover, barrier disruption, inflammatory microenvironment alterations, and microbial dysbiosis can further hinder drug penetration and compromise therapeutic outcomes.14 Consequently, conventional single-scale delivery approaches often struggle to simultaneously achieve efficient penetration, controlled release, barrier restoration, and immune modulation. To address these limitations, multiscale transdermal delivery systems have been developed by integrating molecular permeation enhancement, nanoscale carriers, microscale delivery devices, and intelligent responsive platforms,15,16 thereby enabling spatially and temporally controlled intervention within the skin microenvironment (Figure 2). Nevertheless, while most current studies focus primarily on improving local therapeutic efficacy, the potential interactions between these delivery systems and gut–skin axis-associated regulatory pathways remain insufficiently discussed.
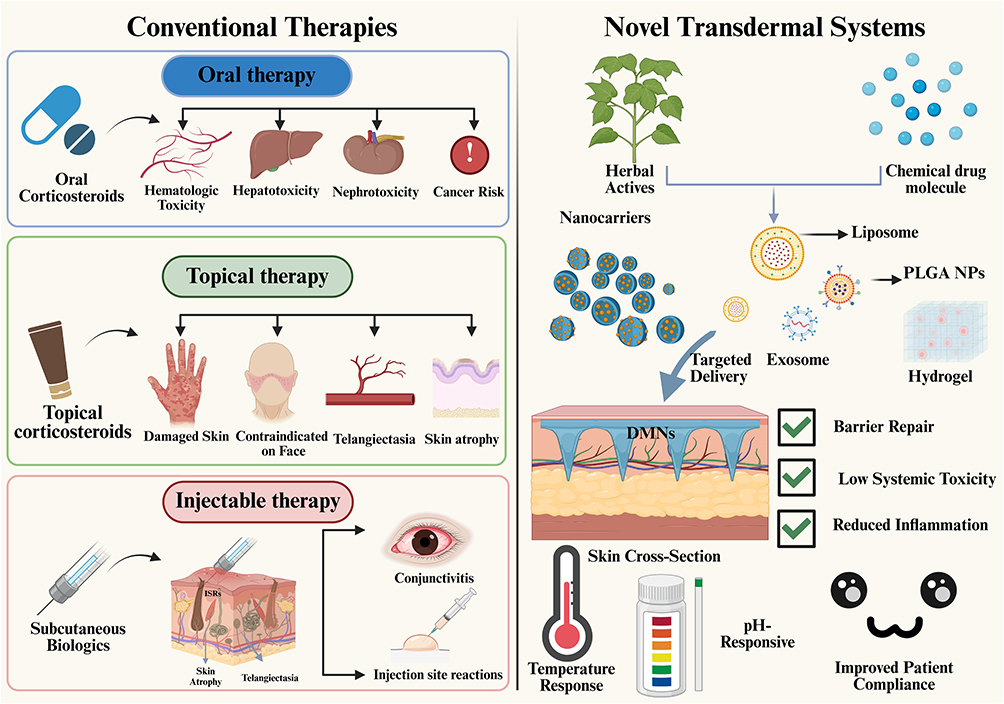 |
Figure 2 Comparison of traditional treatments for AD with multiscale transdermal delivery for improving AD. Abbreviation: PLGA NPs, poly(lactic-co-glycolic acid nanoparticles. |
In this context, transdermal drug delivery is primarily considered in this review as a local therapeutic strategy for AD, whereas gut–skin axis regulation is discussed as an emerging mechanistic perspective that may help explain broader therapeutic outcomes. TCM-derived active compounds are included not as a separate topic, but as representative examples of structurally diverse bioactive molecules that are particularly suitable for multiscale delivery engineering owing to their multi-target and multi-pathway regulatory properties. Based on this perspective, this review provides an overview of recent advances in multiscale transdermal delivery systems for AD, discusses their potential interactions with skin barrier repair, immune modulation, and gut–skin axis-associated pathways, and highlights current challenges in mechanistic validation and clinical translation. By linking AD pathophysiology, multiscale delivery engineering, and emerging gut–skin axis concepts, this review aims to provide a clearer framework for future interdisciplinary research and precision therapeutic development.
Gut–Skin Axis Mechanisms Relevant to Transdermal Therapy
AD is not merely the result of skin barrier impairment or isolated immune dysregulation.17 Instead, it represents a multiscale, cross-system pathological network in which the gut–skin axis plays a central role (Table 1). Within this framework, intestinal barrier disruption, microbial dysbiosis, and altered metabolite signaling can compromise epidermal integrity through systemic immune–metabolic pathways, aggravating local inflammation (Figure 3).18 Conversely, chronic skin inflammation and barrier dysfunction feedback to destabilize intestinal homeostasis, forming a bidirectional pathogenic loop.19 This cross-system interplay occurs across multiple biological scales: molecular (microbial metabolites, inflammatory mediators), cellular (immune cell activation, keratinocyte dysfunction), tissue and organ levels (intestinal mucosal integrity, epidermal barrier function). Understanding these multiscale interactions provides a theoretical foundation for designing transdermal delivery strategies that simultaneously address local skin pathology and systemic gut–skin modulation.
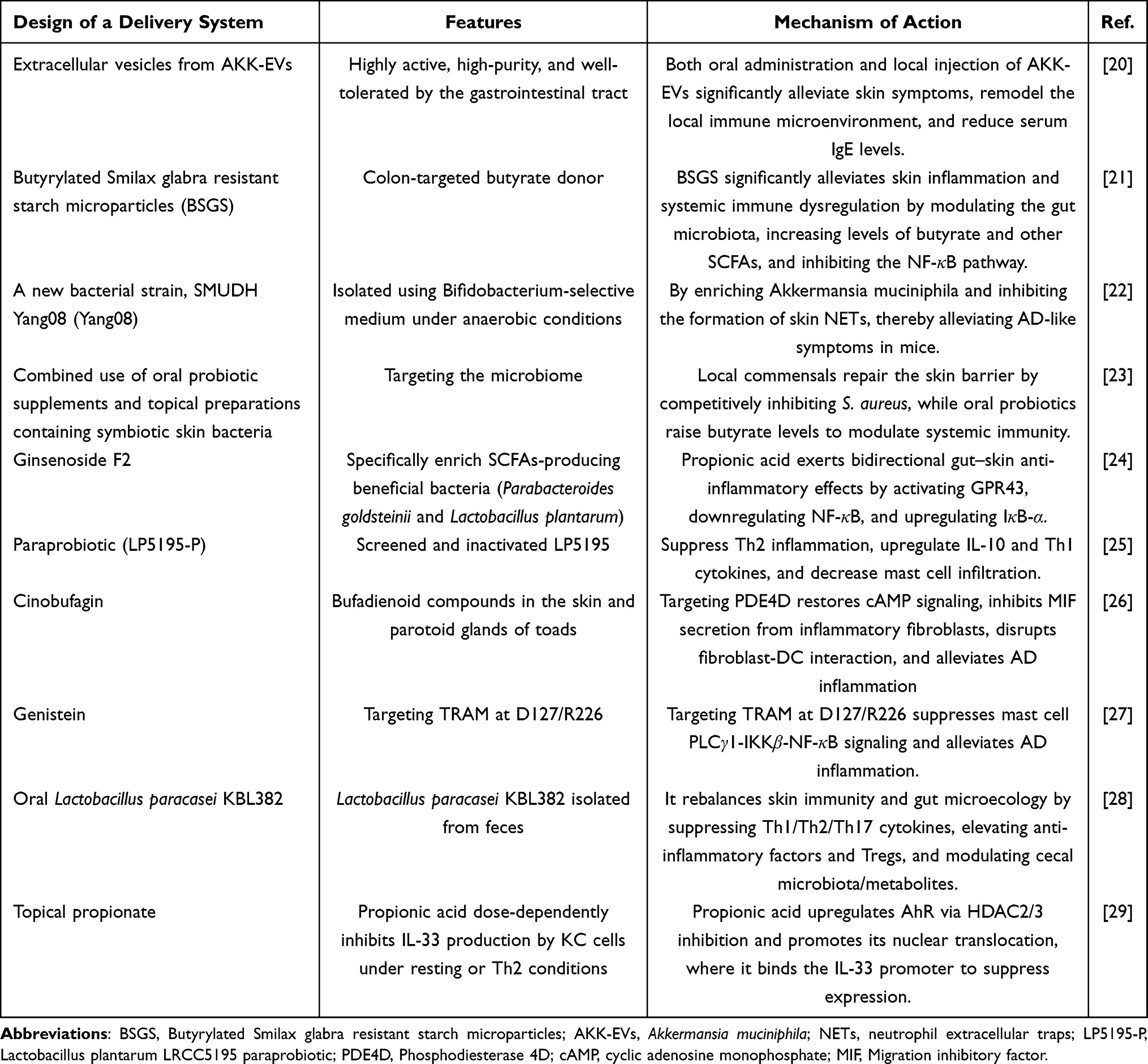 |
Table 1 Mechanisms Underlying the Improvement of AD via the Gut-Skin Axis |
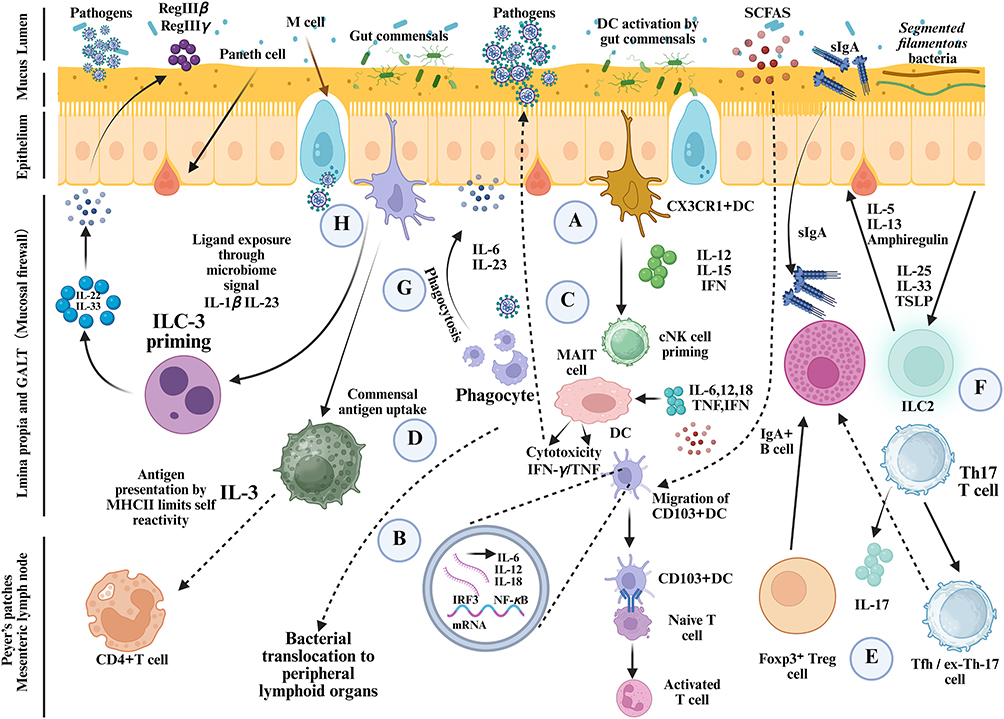 |
Figure 3 Gut–skin axis‑mediated immunopathogenesis of AD. Abbreviations: sIgA, Secretory IgA; MHCII, Major histocompatibility complex II; IRF3, Interferon regulatory factor 3; cNK, Conventional NK; CX3CR1, CX3C chemokine receptor 1; DC, Dendritic cell; Foxp3+, Forkhead box protein P3; Treg, Regulatory T cells; IgA+, Immunoglobulin-A; CD103, Integrin αE subunit; M cell, Membranous/microfold cell; GALT, Gut-associated lymphoid tissue. Notes: A–H represent microbiota-driven mucosal immune pathways: activation of CX3CR1⁺ dendritic cells by gut commensals (A), bacterial translocation to peripheral lymphoid organs and activation of IRF3/NF-κB-dependent cytokine responses (B), priming of MAIT cells and conventional natural killer cells by dendritic cell-derived cytokines (C), commensal antigen uptake and MHCII-dependent restriction of self-reactivity (D), regulation of Foxp3⁺ Treg cells, Th17/Tfh-like cells and IgA responses (E), ILC2-mediated epithelial repair and type 2 immune responses driven by IL-25, IL-33 and TSLP (F), phagocytosis-associated IL-6 and IL-23 production (G), and microbiome-dependent ILC3 priming that promotes IL-22-related RegIIIβ/RegIIIγ-mediated antimicrobial barrier defense (H). |
Bidirectional Interplay Between Intestinal Barrier Dysfunction and Skin Inflammation
The gut-skin axis refers to the bidirectional communication pathway between the gut and skin mediated by immune, metabolic, and neural signals.30 In AD, reduced expression of intestinal tight junction proteins (eg, Occludin, Claudin-1, ZO-1) increases gut permeability, allowing antigens and microbial products to enter circulation and induce skin inflammation.31 Systemically elevated Th2 cytokines such as IL-4 and IL-13 exacerbate both skin barrier dysfunction and intestinal permeability, establishing a negative feedback loop.32 Preclinical models, such as DSS-induced intestinal barrier disruption in AD mice, demonstrate heightened skin inflammation, reduced stratum corneum thickness, and increased immune cell infiltration, confirming the pivotal role of gut barrier integrity in skin homeostasis.33 A large body of evidence suggests that skin inflammatory processes are closely related to loss of gut homeostasis.34 Gut dysbiosis can lead to “leaky gut syndrome”, characterized by disruption of the intestinal epithelial lining, allowing bacteria and other endotoxins to enter the bloodstream and cause intestinal and systemic inflammation.35 Immune cells activated in the gut can migrate to the skin, leading to AD.36 Cutaneous immune responses are closely associated with the cytokine profile generated in the gut, which is reflected by elevated levels of serum inflammatory cytokines. Studies using prebiotics and probiotics have shown that alleviating intestinal inflammation results in corresponding improvements in AD symptoms.37 For example, oral administration of a probiotic mixture containing Lactobacillus and Bifidobacterium has been shown to reduce calprotectin levels (a marker of intestinal inflammation) and exert beneficial effects on the skin, manifested as decreased SCORing for AD (SCORAD) index and transepidermal water loss (TEWL).38 In a DNFB-induced mouse model of AD, oral administration of Dendrobium nobile polysaccharides or olive-derived antioxidant dietary fiber reduced serum levels of IL-1β, TNF-α, IL-4, IFN-γ, and IL-6 while increasing IL-10. This restoration of cytokine balance contributed to the improvement of AD symptoms.39
Effects of the Gut Microbiota–Metabolite–Immune Network on the Skin Barrier
Gut microbiota shape systemic and local immune responses via metabolites, forming a core regulatory node of the gut–skin axis. The gut microbiota regulates systemic immune responses through metabolites, serving as a core node in the gut-skin axis.40 AD patients often exhibit reduced microbial diversity and decreased probiotic abundance, resulting in impaired production of beneficial metabolites like short-chain fatty acids (SCFAs) (Figure 4).41 Supplementation with Bifidobacterium longum or SCFAs has been shown to activate the Aryl hydrocarbon receptor (AhR) receptor, modulate Tregs, suppress Th2 responses, and improve skin barrier function. Conversely, long-chain saturated fatty acids (LCSFA) induce an increase in inflammatory ILC3 cells in the gut, which migrate to the skin and trigger AD.19 Furthermore, gut-derived SCFAs, particularly butyrate, can enhance keratinocyte mitochondrial metabolism and strengthen skin barrier function through the “fatty acid oxidation (FAO)–lipid synthesis–keratinocyte differentiation” axis, providing strong evidence for nutritional interventions in AD and therapeutic strategies targeting the “gut–skin axis”.42 Clinical studies indicate that children with AD exhibit reduced gut microbiota diversity, decreased abundance of Bifidobacterium, and a significant increase in pro-inflammatory bacteria such as Clostridium difficile, which correlates with symptoms of dry skin and itching.18,31 Animal experiments further confirm that supplementation with probiotics or a diet rich in SCFAs can improve skin barrier function and reduce skin inflammation scores.22,43 These findings illustrate a multi-level regulatory circuit: gut microbes–metabolites–immune modulation–skin barrier effects, providing precise intervention targets for multi-scale transdermal delivery systems.
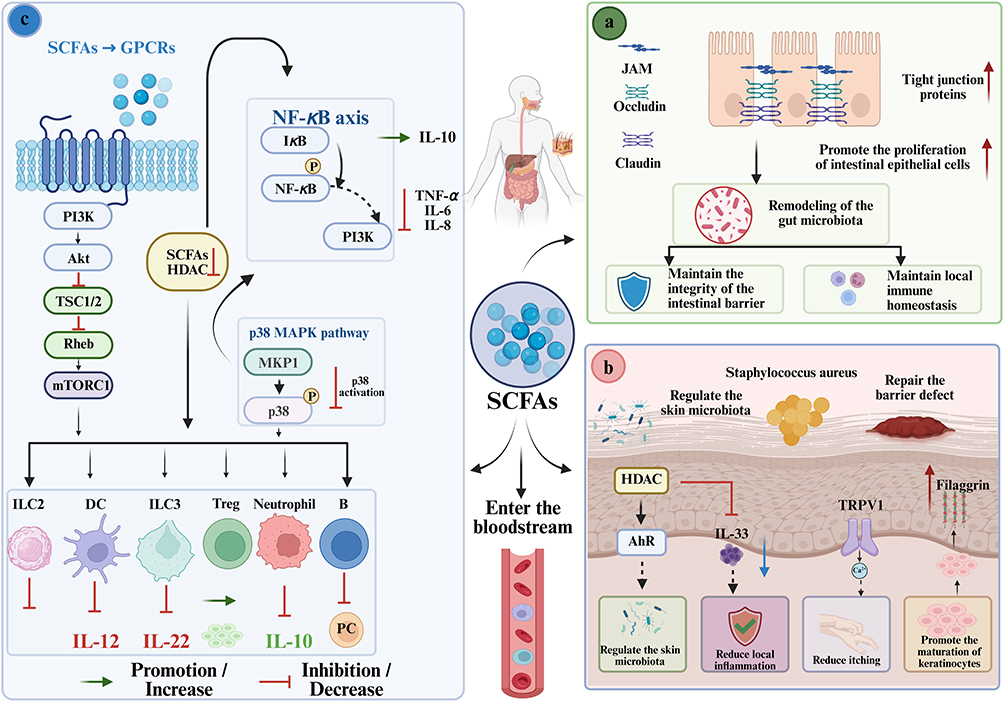 |
Figure 4 Dual regulatory effects of SCFAs on the gut and skin immune microenvironments in AD. (a) In the gut: SCFAs enhance tight junctions and epithelial proliferation, maintain barrier and microbial homeostasis, and enter the circulation to reach skin. (b) SCFAs regulate cutaneous microbiota, promote differentiation, suppress IL-33, and restore barrier via modulation of barrier proteins, alleviating pruritus. (c) In both: SCFAs modulate immune cell functions and signaling pathways via HDAC inhibition and GPCR activation. Abbreviations: GPR109A, G protein-coupled receptor 109A; PI3K, Phosphoinositide 3-kinase; Akt, Protein kinase B; TSC1/2, Tuberous sclerosis complex 1/2; Rheb, Ras homolog enriched in brain; mTORC1, Mechanistic target of rapamycin complex 1; HDAC, Histone deacetylase; NF-κB, Nuclear factor kappa-light-chain-enhancer of activated B cells; IκB, Inhibitor of κB; IL-10, Interleukin-10; TNF-α, Tumor necrosis factor-alpha; IL-6, Interleukin-6; IL-8, Interleukin-8; MAPK, Mitogen-activated protein kinase; MKP1, MAPK phosphatase 1; ILC2/3, Group 2/3 innate lymphoid cell 2/3; DC, Dendritic cell; B, B cell; PC, Plasma cell; IL-12, Interleukin-12; JAM, Junctional adhesion molecule; TRPV1, Transient receptor potential vanilloid 1. Notes: In (a), the red upward arrows indicate increased expression of tight junction proteins (including JAM, occludin, and claudin) and enhanced proliferation of intestinal epithelial cells. In (b), the red upward arrows indicate increased filaggrin expression, while the blue downward arrows indicate decreased IL-33 levels. |
The Gut-Skin Axis as a Core Component of Cross-System Regulation
The gut–skin axis functions as a central hub integrating microbial, immune, and epidermal responses, establishing a bidirectional communication network between the gut and skin.44 Experimental evidence demonstrates that dysbiosis of gut microbiota directly correlates with AD severity: for example, pediatric AD patients show a significant reduction in Bifidobacterium and Lactobacillus species, accompanied by increased Clostridium and Staphylococcus species, which correlates with elevated circulating IL-4 and IL-13 levels.45 These systemic cytokines exacerbate epidermal barrier dysfunction, highlighting the role of gut-derived immune modulation in local skin pathology.
Probiotic or prebiotic interventions provide clear experimental support for the gut–skin regulatory mechanism (Figure 5). Administration of Bifidobacterium longum in AD mouse models reduced serum IgE levels, restored stratum corneum thickness, and decreased dermal mast cell infiltration,46 demonstrating a cross-system effect on both intestinal microbiota and cutaneous inflammation. Similarly, oral supplementation with Lactobacillus rhamnosus GG (LGG) in infants at high risk of AD decreased the incidence and severity of eczema,47 indicating that modulation of gut microbiota can exert preventative and therapeutic effects on the skin through systemic immune pathways. Another study suggests that oral administration of Ruminococcus (a gut commensal bacterium more abundant in the intestines of healthy infants than in those with AD) to AD mice increases cecal butyrate levels, the number of Treg cells in mesenteric and skin-draining lymph nodes, and Foxp3 expression in the skin.48 These findings highlight the role of gut-derived SCFAs as a means of communication to support and promote skin health in patients with AD.
 |
Figure 5 Probiotic intervention alleviates AD by modulating the gut microbiota. Abbreviations: AD, Atopic dermatitis; Th1, T helper 1 cell; Th2, T helper 2 cell; Th17, T helper 17 cell; IDEC, Inflammatory dendritic epidermal cell; LC, Langerhans cell; IgE, Immunoglobulin E; TSLP, Thymic stromal lymphopoietin; CCL17, C-C motif chemokine ligand 17; CCL18, C-C Motif chemokine ligand 18C-C; CCL22, C-C motif chemokine ligand 22; IL-31, Interleukin-31; IL-13, Interleukin-13; IL-4, Interleukin-4; IL-33, Interleukin-33; IL-17, Interleukin-17; IL-22, Interleukin-22; IFN-γ, Interferon-gamma; TNF-α, Tumor necrosis factor-alpha; T-bet, T-box expressed in T cells; STAT1, Signal transducer and activator of transcription 1; STAT4, Signal transducer and activator of transcription 4; GPR43, G protein-coupled receptor 43; AhR, Aryl hydrocarbon receptor. Notes: In Figure 5, the blue downward arrows indicate that, following probiotic-mediated regulation of the gut microbiota, levels of Th2-related cytokines (including IL-31, IL-13, and IL-4) and TSLP decreased. |
Metabolite-mediated mechanisms further exemplify the core regulatory role of the gut–skin axis. SCFAs, such as butyrate and propionate, produced by commensal gut bacteria, can enhance regulatory Treg function and suppress Th2-mediated skin inflammation (Figure 6).49 A recent study demonstrated that butyrate supplementation in AD mice increased Foxp3⁺ Treg populations in skin-draining lymph nodes, reduced IL-4 and IL-5 levels, and promoted expression of epidermal barrier proteins filaggrin and loricrin,50 supporting both immune and barrier restoration functions.
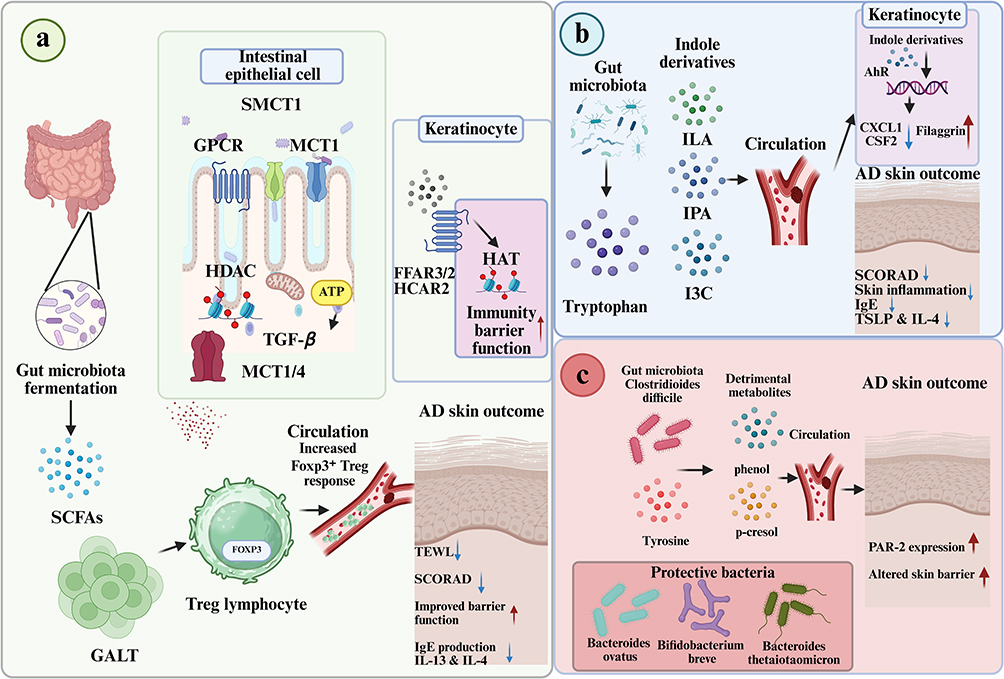 |
Figure 6 The gut microbiota exerts significant effects on immune regulation and skin barrier function in AD through the production of SCFAs and the catabolism of tryptophan and tyrosine. (a) SCFAs generated by microbial fermentation are absorbed by colonic epithelial cells and partially enter the bloodstream via the portal vein for systemic distribution. (b) Indole derivatives derived from microbial tryptophan metabolism alleviate AD symptoms by regulating keratinocyte gene expression. (c) Phenolic metabolites derived from Clostridioides difficile can induce skin barrier damage and promote the pathogenesis of AD, probiotic intervention reduces serum p‑cresol levels and restores skin barrier function. Abbreviations: SCFAs,Short-chain fatty acids; SMCT1, Sodium-coupled monocarboxylate transporter 1; MCT1/4, Monocarboxylate transporter 1/4; GPCR,G protein-coupled receptor; HDAC, Histone deacetylase; ATP, Adenosine triphosphate; TGF-β, Transforming growth factor-beta; FFAR3/2, Free fatty acid receptor 3/2; HCAR2, Hydroxycarboxylic acid receptor 2; HAT, Histone acetyltransferase; GALT, Gut-associated lymphoid tissue; FOXP3/Foxp3, Forkhead box P3; TEWL, Transepidermal water loss; SCORAD SCORing atopic dermatitis; ILA, Indole-3-lactic acid; IPA, Indole-3-propionic acid; I3C, Indole-3-carbinol; CXCL1, C-X-C motif chemokine ligand 1; CXCL1, C-X-C motif chemokine ligand 1; PAR-2,Protease-activated receptor 2. Notes: In (a) the red upward arrows indicate enhanced immune barrier function in keratinocytes and improved skin barrier function, while the blue downward arrows indicate reduced TEWL, lower SCORAD scores, decreased IgE production, and lower levels of IL-13 and IL-4. In (b) the red upward arrow in keratinocytes indicates increased filaggrin expression, while the blue downward arrow indicates decreased CXCL1 and CSF2 expression, a lower SCORAD score, reduced skin inflammation, decreased IgE levels, and lower TSLP and IL-4 levels. In (c), the red upward arrow indicates increased PAR-2 expression induced by harmful metabolites and worsened skin barrier damage. |
In keratinocytes, AhR is an important regulator in response to inflammatory stimuli. Human keratinocytes lacking AhR overexpress C-X-C motif chemokine ligand 1 (CXCL1) and granulocyte-macrophage colony-stimulating factor (CSF2) when exposed to the inflammatory mediator IL-1β.51 Furthermore, stimulation of human keratinocytes with the AhR agonist 6-formylindolo[3,2-b]carbazole (FICZ) leads to upregulation of filaggrin (FLG), and the importance of AhR activation in FLG transcription has been demonstrated in an in vitro AD model.52 Thus, the production of indole derivatives from tryptophan by microorganisms represents a pathway through which AhR activation and its modulation of inflammation and skin barrier function can influence skin health. Although the beneficial effects of AhR activation on keratinocytes open up possibilities for interventional therapies for AD, further studies are needed to understand the underlying mechanisms of the physiological consequences of AhR signaling in the immune system.
Collectively, these studies emphasize that the gut–skin axis serves as a core integrative regulator in AD pathogenesis. Interventions targeting the gut microbiota, its metabolites, or systemic immune mediators can restore barrier integrity, modulate inflammation, and improve clinical outcomes. Such insights provide a mechanistic rationale for designing multi-scale transdermal delivery systems that not only act locally on the skin but also synergize with systemic gut–skin interactions to achieve holistic disease modulation.
Design Implications for Transdermal Delivery Based on the Gut–Skin Axis
The multiscale and cross-system nature of the gut–skin axis in AD provides critical guidance for designing transdermal delivery systems. Transdermal platforms are no longer limited to local drug administration but can be engineered to modulate systemic immune responses via gut–skin interactions. For example, a recent study has for the first time revealed the potential of exosomes derived from the probiotic Limosilactobacillus fermentum SLAM216 (LF216EV) in alleviating symptoms of AD. LF216EV modulates the gut microbiota and metabolite profiles, promotes serotonin synthesis, and upregulates genes related to serotonin synthesis in both the skin and the gut, thereby improving the clinical symptoms of AD.53 Another recent study shows that loss of intestinal epithelial TLR4 causes gut dysbiosis, increasing trimethylamine N-oxide (TMAO) production via choline metabolism. Elevated TMAO correlates with AD risk and severity. Mechanistically, TMAO activates protein phosphatase 5 (PPP5) in CD4⁺ T cells, dephosphorylates peroxisome proliferator-activated receptor γ (PPARγ), and drives Th2 differentiation, exacerbating skin inflammation.54
Micron-scale strategies, such as dissolvable microneedles or porous microspheres, enable precise local deposition of active compounds, including TCM-derived active components, which have multi-target and multi-pathway regulatory properties. These platforms can be combined with stimuli-responsive materials that sense local pH, enzyme activity, or redox states to trigger on-demand release, synchronizing local barrier repair with modulation of gut-mediated immune pathways. According to a related study, a multifunctional bilayer microneedles (MNs) patch (CET@PB NPs) has been developed for the long-term effective treatment of AD. By integrating therapeutic nanoparticles and live bacteria, this MNs patch not only scavenges ROS and ameliorates the oxidative stress microenvironment in AD lesions but also enables sustained release of antihistamines in the skin, relieving itching and improving skin barrier function (Figure 7).55 Another recent study has designed dissolvable MNs containing hyaluronic acid (HA) and purslane polysaccharide (POP), and used the MNs to deliver purslane-derived nanovesicles (PDNV). These MNs can treat AD by modulating macrophage polarization and inhibiting the NF-κB and cCAG-STING signaling pathways.56
 |
Figure 7 A novel multifunctional double-layer MNs patch for treating AD. Prepared from a water-soluble matrix, the patch dissolves and releases rapidly. The needle tip layer is coated with CET@PB NPs, while the backing layer is coated with live Bs. Upon skin insertion, the MNs rapidly dissolve, releasing CET@PB NPs within the skin. Abbreviations: Bs, Bacillus subtilis; CET@PB NPs, Cetirizine hydrochloride-loaded Prussian blue nanoparticles; M1, Classically activated macrophages; M2, Replace activated macrophages; H1R, Histamine receptor. |
Nanoscale carriers, including liposomes, polymeric nanoparticles, and self-assembled structures, further facilitate gut–skin axis modulation by enhancing bioavailability of metabolites or immune-regulatory molecules. For example, SCFAs such as butyrate are important immunomodulatory metabolites produced by the gut microbiota. Encapsulation of butyrate in liposomes enables controlled release for transdermal delivery. Studies have shown that in AD-like mouse models, liposomal butyrate not only enhances drug accumulation in skin lesions but also effectively downregulates systemic Th2-type cytokines such as IL-4 and IL-13, thereby alleviating skin inflammation and reinforcing barrier integrity.57 Polymeric nanoparticles, in turn, can be loaded with active ingredients from TCM to indirectly modulate gut microbiota composition and metabolite profiles via lymphatic drainage, establishing bidirectional signaling between the skin and the gut. For instance, a study constructed self-assembled nanoparticles derived from Coptis chinensis decoction (CR-SAN). These nanoparticles enhance skin penetration and retention by disrupting the stratum corneum structure, altering lipid organization, and modifying the secondary structure of keratin.58 Subsequently, they transmit delivery signals through the lymphatic circulation to gut-associated lymphoid tissue, affecting the structure and SCFAs production of distal gut microbiota. Such nanocarrier-based transdermal intervention strategies provide a verifiable technological pathway for triggering systemic microbial–metabolic–immune regulation through topical administration.
Overall, the gut–skin axis provides a clear functional framework for the rational design of multi-scale transdermal delivery systems. Future efficient transdermal strategies should integrate multiple capabilities: they should not only promote skin barrier restoration and exert local anti-inflammatory effects, but also modulate immune functions in skin and gut-associated lymphoid tissues. At the same time, stimulus-responsive mechanisms should be employed to achieve precise drug release aligned with the dynamic microenvironment of AD lesions. This design concept, which combines localized precision delivery with systemic immune regulation, holds promise for advancing next-generation transdermal systems from mere symptom alleviation toward long-term disease management, thereby offering new directions for precision therapy and clinical translation in AD.
Multi-Scale Transdermal Delivery Systems for AD
Multi-scale transdermal delivery systems emphasize the synergistic interaction between different spatial and functional levels, including molecular-level pathological microenvironment responses, nanoscale targeted delivery, microscale physical penetration, and programmed drug administration at the device-platform level, thereby addressing the integrated needs for barrier repair, immune modulation, and microbiome intervention in the complex pathology of AD.
Design Principles for Gut–Skin Axis-Oriented Transdermal Delivery
AD exhibits pathological alterations across multiple biological scales, including disruption of epidermal barrier proteins, activation of Th2-dominant immune responses, microbial imbalance, and systemic immune abnormalities associated with the gut–skin axis.1 Therefore, effective therapeutic interventions need not only to restore local skin homeostasis but also to mitigate the spread of systemic inflammation arising from intestinal immune dysfunction. From this perspective, multiscale transdermal delivery systems are designed to integrate molecular, nanoscale, microscale, and device-platform level functions into a coordinated therapeutic framework.
At the molecular level, delivery systems are designed to respond to the pathological features of AD lesions, including elevated pH, excessive ROS, protease overactivity, and accumulation of inflammatory cytokines. These stimulus-responsive mechanisms enable precise spatiotemporal release and improve therapeutic selectivity. At the nanoscale, carriers such as liposomes, polymeric nanoparticles, and self-assembled nanostructures enhance skin penetration, cellular uptake, and local retention, thereby enabling targeted modulation of keratinocytes, dendritic cells, and macrophages (Figure 8). A research team prepared high-purity EVs derived from Akkermansia muciniphila (AKK-EVs) using differential centrifugation. AKK-EVs selectively accumulated in inflamed skin lesions via the gut–skin axis, significantly improving skin symptoms, reshaping the local immune microenvironment, and reducing serum IgE levels, thereby demonstrating the potential translational value of orally administered probiotic-derived exosome nano-systems for AD therapy.20 At the microscale, microneedles and porous microspheres can overcome the stratum corneum barrier and achieve controlled drug deposition within deeper skin layers. Recent studies have reported the design of butyrylated Smilax glabra resistant starch microparticles (BSGS) as a colon-targeted butyrate delivery system, which restores gut–skin axis homeostasis and offers a promising therapeutic strategy for AD.21 At the device-platform level, hydrogel matrices and wearable patches provide prolonged drug retention and sustained regulation of the local inflammatory microenvironment. For example, one research group loaded curcumin into a zinc-doped ferrocyanide-derived metal–organic framework (Cur/ZnMOF) and subsequently incorporated it into a gelatin–silk fibroin crosslinked network.59 The resulting hydrogel dressing exhibited remarkable self-healing capability, strong tissue adhesiveness, and excellent mechanical properties. This intelligent multifunctional hydrogel represents a promising alternative to conventional antibiotic-loaded wound dressings and may offer an effective strategy for the rapid treatment of AD.
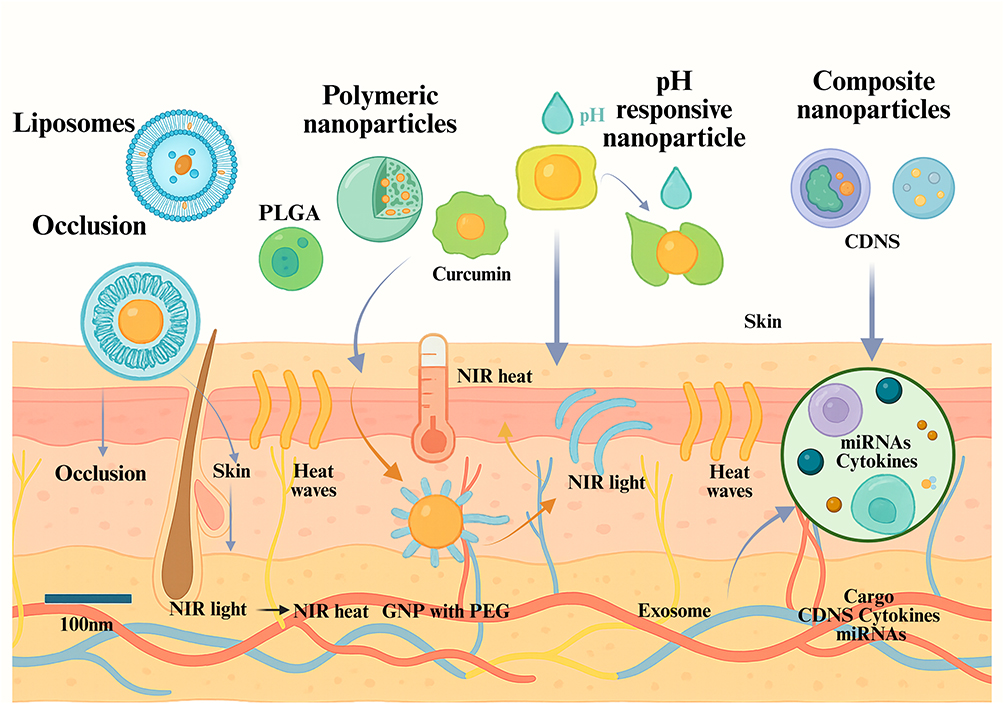 |
Figure 8 Construction and application of transdermal delivery systems at the nanoscale. Abbreviations: CDNS, Cyclodextrin nano-sponge; NIR, Near-infrared light; GNP with PEG, Gold nanoparticles with polyethylene glycol. |
Notably, the rationale for multiscale design lies not only in improving local drug delivery. Growing evidence indicates that the restoration of epidermal integrity can indirectly modulate gut–skin axis signaling. Human β-defensin-3 (hBD-3) can alleviate IL-4- and IL-13-mediated damage to the tight junction barrier by activating autophagy in keratinocytes (involving the AhR signaling pathway), thereby alleviating AD-like inflammation.60 These findings provide important directions for the development of therapeutic agents for AD. Thus, multiscale delivery systems can be regarded as an integrated platform that simultaneously addresses local skin pathology and systemic immune dysregulation.
Molecular-Level Regulation of the AD Microenvironment
At the molecular scale, transdermal delivery systems primarily employ small-molecule carriers that directly interact with the skin barrier and local microenvironment to enhance drug penetration, target immune cells, and respond to inflammation-specific stimuli. Molecular-scale strategies not only provide foundational support for nano- and micro-scale delivery platforms but also enable early, precise intervention along the skin barrier–immune axis.
Penetration Enhancers and Barrier Modulation Pathways
The stratum corneum serves as the primary barrier to transdermal drug delivery, where its densely organized lipid matrix and keratin network severely restrict the penetration of both small-molecule and macromolecular therapeutics.61 Molecular-scale penetration enhancers improve transdermal transport by reversibly altering lipid organization within the stratum corneum, increasing membrane fluidity, or enhancing skin hydration.62 Among conventional chemical enhancers, phospholipids and cholesterol derivatives can intercalate into the intercellular lipid bilayers of the stratum corneum, disrupting their highly ordered arrangement and thereby facilitating the diffusion of both hydrophilic and lipophilic compounds.63 Short-chain alcohols, such as ethanol and propylene glycol, primarily enhance drug permeation by increasing stratum corneum hydration and improving the partitioning of active ingredients into epidermal tissues.64
In recent years, cell-penetrating peptides (CPPs) have emerged as an important molecular strategy for enhancing the transdermal delivery of macromolecules in AD. For example, TAT peptide-modified anti-inflammatory agents have demonstrated improved dermal penetration and enhanced local anti-inflammatory efficacy in experimental dermatitis models compared with their unmodified counterparts.65 Notably, many bioactive compounds derived from TCM, including baicalin, berberine (BER), puerarin, and glycyrrhizic acid, exhibit limited transdermal permeability owing to their relatively large molecular size and/or complex polar structures.66 Molecular-level penetration-enhancement strategies therefore provide a critical technological basis for the topical application of these natural products, enabling the effective utilization of their anti-inflammatory, antioxidant, and immunomodulatory properties.
From the perspective of the gut–skin axis, enhanced local drug penetration not only increases therapeutic concentrations at lesion sites but may also contribute to the suppression of epithelial-derived cytokines such as interleukin (IL)-33, thymic stromal lymphopoietin (TSLP), and IL-25.54 These cytokines can enter systemic circulation, promote Th2-skewed immune responses, and amplify allergic inflammation in the intestinal mucosa. Although direct evidence remains limited, improved local inhibition of TSLP, IL-33, and IL-25 may potentially reduce systemic Th2 inflammatory signaling associated with gut–skin axis dysregulation, thereby contributing to the restoration of immune homeostasis across both tissues.
Stimuli-Responsive Molecular Systems
Conventional topical formulations usually release drugs at a fixed rate and cannot adapt to the dynamically changing inflammatory microenvironment of AD lesions. To address this, researchers have developed stimuli-responsive molecular systems capable of sensing specific pathological signals and releasing drugs on demand. The pH characteristics of AD lesions are well documented: healthy skin surfaces are weakly acidic (pH 4.5–5.5), whereas AD-affected areas often have elevated pH levels around 6.0–6.5 or higher.67 This alkalization can activate serine proteases (kallikreins KLK5 and KLK7), disrupt the optimal acidic environment of stratum corneum lipid-processing enzymes (β-glucocerebrosidase), impair barrier function, and promote Staphylococcus aureus colonization.
pH-responsive delivery systems exploit these differences to achieve lesion-selective drug release. For instance, anti-inflammatory agents can be conjugated to pH-sensitive polymers such as poly (diethylaminoethyl methacrylate) or Eudragit® L100-55, remaining stable under healthy skin pH but rapidly releasing the drug in the slightly alkaline environment of AD lesions via ester hydrolysis or polymer swelling.68 Another key strategy is ROS-responsive systems. Excess ROS in AD lesions can damage keratinocyte DNA and membrane lipids, promote the production of pro-inflammatory cytokines (IL-4, IL-13, IL-31) and form an oxidative stress-inflammation vicious cycle.69 ROS-responsive carriers typically incorporate chemical groups such as thioketal (TK) or selenocystamine that break under ROS attack, releasing the payload. Studies have shown that curcumin-loaded ROS-responsive nanocarriers not only enhance antioxidant activity but also significantly inhibit the NF-κB signaling pathway and downstream inflammatory cytokines.70 Many bioactive compounds from TCM, such as curcumin, epigallocatechin-3-gallate (EGCG), baicalin, and resveratrol, inherently possess ROS-scavenging properties.71 Integrating these natural antioxidants into responsive delivery systems allows synchronized spatiotemporal control of anti-inflammatory and antioxidant effects, yielding synergistic therapeutic outcomes.
Notably, oxidative stress and systemic immune activation are considered important bridges between gut microbiota dysbiosis and skin inflammation. AD patients often exhibit reduced gut microbial diversity and diminished short-chain fatty acid production, leading to increased intestinal barrier permeability (leaky gut), which allows bacterial endotoxins and pro-inflammatory mediators to enter circulation and further exacerbate skin oxidative stress.31 ROS-responsive delivery systems that remove excess ROS locally in the skin may interrupt this peripheral inflammation amplification loop, indirectly stabilizing gut–skin axis signaling.
Nanoscale Delivery Systems Linking Local AD Therapy with Gut–Skin Axis Regulation
In AD, nanoscale transdermal delivery systems not only enhance drug penetration efficiency but, more importantly, can influence disease progression by precisely modulating the local pathological microenvironment. Accumulating evidence indicates that AD is not merely a localized inflammatory skin disorder but is closely associated with systemic immune imbalance and aberrant activation of the gut–skin axis.72 Therefore, the value of nano-delivery systems should not be limited to increasing drug concentrations at lesion sites; instead, greater emphasis should be placed on their integrated roles in regulating Th2-type inflammation, restoring skin barrier integrity, suppressing oxidative stress, and reducing the systemic spillover of inflammatory mediators.
Compared with conventional topical formulations, nanocarriers possess tunable particle size, surface charge, and interfacial properties, enabling precise drug distribution in the epidermis, dermis, and even immune cell-enriched regions. Through sustained release of anti-inflammatory and barrier-repairing active ingredients, nanoscale systems can reduce the levels of key inflammatory mediators such as IL-4, IL-13, TSLP, and IL-33, thereby alleviating local immune activation and neuroinflammatory responses.73 Notably, these cytokines are not only involved in the progression of skin lesions but are also considered to be closely associated with intestinal mucosal immune activation and systemic Th2-biased inflammation. Therefore, effective intervention of nanoscale delivery systems on local pathological processes may indirectly reduce the systemic spread of aberrant inflammatory signals, thereby influencing the gut–skin axis-related immune network.
Based on the above understanding, various platforms developed in recent years, including liposomes, nanoemulsions, polymeric nanoparticles, self-assembled nanostructures, and exosome-like nanocarriers, have gradually evolved from simple drug delivery vehicles into therapeutic systems that integrate barrier repair, immune modulation, and disease microenvironment remodeling. Particularly in the field of delivering active ingredients from TCM, these nanoplatforms have not only improved the stability and bioavailability of natural products such as curcumin, baicalin, and BER but also provided an important foundation for constructing novel therapeutic strategies that combine local treatment with gut–skin axis regulation.
Lipid-Based Nanocarriers for Barrier Restoration and Gut–Skin Axis Modulation
Lipid-based nanocarriers are among the most clinically advanced nanoplatforms for transdermal drug delivery. Their advantages extend beyond enhancing transdermal drug transport, as they can also mimic the natural lipid environment of the skin, thereby providing dual functions of drug delivery and barrier repair. Liposomes possess a phospholipid bilayer structure similar to that of cellular membranes, enabling the simultaneous encapsulation of both hydrophilic and hydrophobic drugs. This characteristic not only improves drug stability and skin retention but also facilitates targeted delivery to the epidermal and dermal layers.74
In AD treatment, liposomes can significantly enhance the local accumulation of anti-inflammatory drugs at lesion sites. Notably, a representative study demonstrated that a cream containing mallow flower extract was significantly effective in a randomized controlled trial involving children with mild-to-moderate AD. The mallow extract group showed marked improvements in skin thickening score, redness score, and total SCORAD score compared with the placebo group.75 Similarly, curcumin-loaded liposomes enhanced local anti-inflammatory effects by promoting uptake in keratinocytes and immune cells, while inhibiting NF-κB activation and downstream pro-inflammatory cytokine expression.76 For poorly soluble or unstable herbal active compounds such as baicalin, BER, and tanshinone IIA, liposomes also improved transdermal delivery efficiency and local bioavailability.77 Nanoemulsions, on the other hand, rely on their extremely large interfacial area and excellent skin-spreading properties to enhance drug penetration. A study has reported a polymeric nanoparticle hydrogel formulation loaded with BER hydrochloride and caffeic acid (CA) for the topical treatment of AD. The BER‑CA co‑loaded polymeric nanoparticle hydrogel formulation significantly reduced the SCORAD index, epidermal thickening, acanthosis, and other histopathological features, and suppressed the inflammatory response by downregulating the pro‑inflammatory cytokines IL‑4 and TNF‑α.78 Certain nanoemulsion systems can further incorporate barrier lipids such as ceramides, cholesterol, or fatty acids, simultaneously deliver drugs and replenish the lipid structure of the damaged stratum corneum, thereby enabling concurrent therapeutic intervention and barrier restoration.79
From the perspective of the gut–skin axis, the significance of lipid-based nanocarriers extends beyond simply increasing local drug concentrations. Growing evidence suggests that skin barrier dysfunction is one of the major drivers of persistent systemic Th2 inflammation. By restoring the lipid architecture of the stratum corneum, reducing transepidermal water loss, and suppressing the release of epithelial-derived alarmins such as TSLP, IL-33, and IL-25, lipid nanocarriers can attenuate the propagation of local inflammation into the systemic immune network.80 Furthermore, restoration of barrier integrity may alleviate oxidative stress and suppress STAT6-mediated Th2 inflammatory amplification through activation of the AhR/ARNT signaling pathway, upregulation of tight junction proteins such as CLDN4 and OCLN, and promotion of NRF2 nuclear translocation.81 Collectively, these effects contribute to reducing aberrant gut–skin axis signaling and facilitate the restoration of systemic immune homeostasis. Therefore, liposomes and nanoemulsions are no longer regarded merely as transdermal delivery vehicles, they are increasingly emerging as multifunctional nanotherapeutic platforms that integrate skin barrier repair, immune modulation, and gut–skin axis homeostasis restoration.
Polymeric Nanocarriers: A New Platform Bridging Local Therapy and Gut–Skin Axis Immunomodulation
Polymer nanoparticles offer unique advantages for local AD therapy due to their highly tunable structures and excellent biocompatibility. By selecting different polymer backbones, molecular weights, and surface modifications, drug release kinetics, targeting specificity, and penetration depth can be precisely controlled. PLGA nanoparticles, chitosan (CS) nanoparticles, and stimuli-responsive smart polymers have been widely applied for the transdermal delivery of herbal active components.82 In AD treatment, polymeric nanocarriers not only enhance drug retention in the epidermis and dermis but also inhibit the secretion of Th2-related cytokines (IL-4, IL-13, IL-31) through sustained release, thereby alleviating local inflammation.83 This local intervention not only improves the skin microenvironment but also indirectly mitigates gut mucosal immune dysregulation by reducing the systemic dissemination of inflammatory mediators, thereby modulating gut–skin axis signaling. For example, curcumin-loaded PLGA nanoparticles significantly increased epidermal penetration and reduced ear thickness and mast cell infiltration in an AD mouse model.84 CS nanoparticles form a drug reservoir on the skin surface, enabling prolonged retention and release for over 48 h while exhibiting inherent antibacterial activity.85 Smart polymeric nanocarriers, such as ROS-responsive PLGA particles containing thioether linkages, specifically release drugs in high-ROS inflammatory microenvironments while remaining largely inert in healthy skin, achieving precise temporal and spatial control.86
Through these designs, polymer nanoparticles can efficiently deliver anti-inflammatory and immunomodulatory agents locally while minimizing stimulation of systemic Th2 responses, thereby stabilizing bidirectional gut–skin axis signaling. This multilayered regulation not only enhances local therapeutic efficacy in AD but also provides a feasible strategy for modulating the gut–skin axis via nanotechnology, laying the foundation for future multiscale delivery platforms integrated with microbiome-based interventions.
Self-Assembled Nanostructure-Based Strategy for Gut–Skin Axis Synergistic Regulation
Self-assembled nanostructures represent a delivery paradigm in which ordered nanoscale systems spontaneously form through weak intermolecular interactions such as hydrogen bonding, π–π stacking, and electrostatic forces, offering unique advantages for the transdermal translation of natural products.87 Compared to conventional “carrier–drug separate” nanocarriers, self-assembled systems emphasize the intrinsic structural properties of bioactive molecules to drive assembly, creating a “drug-as-structural-unit” delivery mode that provides a novel material basis for understanding the synergistic effects of multi-component herbal medicines. For example, baicalin can self-assemble into stable spherical nanoparticles via intermolecular hydrogen bonding and π–π stacking without the need for exogenous carrier materials. This “carrier-free nano-system” avoids potential immunogenicity associated with polymeric or lipid materials while preserving and locally concentrating baicalin’s anti-inflammatory, antibacterial, and antioxidant activities.88
Mechanistically, a key advantage of self-assembled nanostructures lies in their “multi-molecule coordinated organization with multi-target synchronized release”.89 Multi-component herbal systems, such as polysaccharide–saponin and flavonoid–alkaloid combinations, can form stable supramolecular aggregates at the nanoscale via noncovalent interactions, enabling the co-delivery of different pharmacologically active compounds in both space and time to simultaneously target inflammation, oxidative stress, and barrier repair.90 Compared with single-agent delivery systems, this approach is more aligned with the complex pathological network characteristic of chronic inflammatory skin diseases. More importantly, self-assembled nanostructures offer a potential material link for gut–skin axis regulation. On one hand, certain natural products such as polysaccharides and flavonoids have been shown to modulate gut microbiota composition or promote SCFAs production.91 On the other hand, following local transdermal delivery, these compounds can reduce peripheral dissemination of systemic immune activation signals by lowering Th2 cytokines such as IL-4 and IL-13, thereby indirectly mitigating abnormal gut mucosal immune stimulation.
Therefore, self-assembled nanostructures not only serve as a technology to enhance transdermal delivery efficiency of natural products but also potentially establish a bridging platform connecting “local skin microenvironment modulation” with “systemic gut–skin axis homeostasis restoration”, providing a new nanotechnological framework and translational pathway for multi-component herbal therapy in AD.
Exosome-Based Nano-Therapy Strategy for Gut–Skin Axis Synergistic Regulation
Plant-derived exosome-like nanoparticles (P-EVs) exhibit unique advantages in transdermal therapy for dermatology.92 Compared with traditional nanocarriers, these exosomes combine natural biocompatibility, low immunogenicity, and intrinsic pharmacological activity, enabling both drug delivery and intercellular signaling regulation.93 Studies have confirmed that extracellular vesicle-like nanoparticles (PELNs) derived from purslane exert potent anti-inflammatory effects on skin-related cells, effectively alleviating oxidative stress in the skin, inhibiting pathological skin crusting, and restoring the Th1/Th2 immune balance.94
Exosomes are naturally involved in intercellular communication and immune regulation, and the bioactive RNAs, proteins, and lipids they carry can be taken up by recipient cells, directly influencing the local immune microenvironment.95 Notably, such signals may further act on distal mucosal immune tissues, including gut-associated lymphoid tissue, via the lymphatic or circulatory pathways, thereby participating in the regulation of the gut–skin axis. Therefore, exosomes not only enable precise intervention in local skin inflammation but may also indirectly modulate systemic immune–microbial homeostasis through endogenous signaling pathways, achieving multidimensional synergistic regulation of AD lesions and the gut–skin axis.
Furthermore, combining exosomes with nanoengineering technologies such as loading anti-inflammatory drugs, microneedle delivery, or smart responsive systems, which can further enhance their targeting and controlled-release performance. For example, loading levofloxacin into Staphylococcus epidermidis-derived exosomes (SE-EVs) and delivering them through hyaluronic acid microneedles enables selective clearance of Staphylococcus aureus (S. aureus) and local immune modulation, thereby indirectly improving intestinal mucosal inflammation.96 Such strategies fully demonstrate the potential of exosome-based nano-therapy in bridging “local skin microenvironment regulation” and “gut–skin axis homeostasis remodeling”, offering a novel multiscale intervention approach for the precision treatment of AD.
Applications of Microbiome-Targeting Nano-Delivery Strategies in AD
The typical feature of the skin microbiome in AD patients is the overcolonization of S. aureus and a reduction in the diversity of commensal bacteria. S. aureus colonization is detected in over 90% of AD lesions and exacerbates barrier disruption and inflammation amplification by producing superantigens, toxins, and virulence factors that activate Th2-skewed immune responses.97,98 In this context, microbiome-targeted therapies are evolving from proof-of-concept studies toward systematic strategy optimization and engineering, forming a spectrum that spans from non-specific interventions to precision-targeted approaches.
Non-targeted strategies, including probiotics (live bacterial preparations), prebiotics (substrates that selectively promote the growth of beneficial bacteria), and postbiotics (metabolites of probiotics), have been extensively explored. However, conventional topical application of probiotics faces limitations such as low viability of live bacteria, uncertain colonization efficiency, and potential infection risks.96 A review published in 2026 systematically evaluated the prospects and challenges of live microbial-containing biotherapeutic products for AD treatment, pointing out that successful topical biotherapy requires overcoming the limitations of the pharmaceutical-centered paradigm and the inertial constraints of traditional academic understanding.99 Targeted strategies have advanced rapidly. For instance, bacteriophages and their lysins can selectively lyse S. aureus with minimal impact on commensal bacteria, quorum-sensing inhibitors block the expression of virulence factors without killing bacteria.100 Synthetic biology enables the construction of engineered live biotherapeutic products that sense skin signals and responsively produce therapeutic molecules.101 Autologous microbiome transplantation has also shown potential.102 These multi-level, multi-precision intervention modalities provide a rich toolbox for integration with nano-delivery systems.
In nanoparticle fusion strategies, researchers have integrated probiotics, prebiotics, and their metabolites into carriers such as lipid nanoparticles, polymeric nanoparticles, and self-assembled hydrogels to achieve precise delivery and microbiome modulation. For example, skin commensal bacterial extracellular vesicles (SE-EVs) loaded with levofloxacin and incorporated into hyaluronic acid microneedles can be selectively taken up by S. aureus, providing synergistic antibacterial and anti-inflammatory effects, alleviating skin inflammation, and promoting barrier repair.96 Although Cutibacterium acnes is commonly associated with acne, it can suppress Th2-skewed AD pathology by inducing a Th1-type immune response. Researchers developed C. acnes nanoparticle formulations, and with sponge-hydrogel microneedles enhancing transdermal delivery, they significantly reduced epidermal thickness, serum IgE, and IL-4 levels, accelerated skin repair, and alleviated Th2 polarization.103 Postbiotics, which are bioactive metabolites produced by probiotic fermentation, possess both antibacterial and antioxidant functions. However, their direct application is limited by cytotoxicity and low transdermal efficiency. One study constructed hyalurosome hybrid nanoparticles (80–200 nm) based on hyaluronic acid to deliver postbiotics. Hybrid nanoparticles loaded with Lactobacillus rhamnosus postbiotics completely cleared S. aureus within 48 h, while those loaded with Weissella cibaria postbiotics maintained strong antioxidant activity.104 Importantly, nanoparticle encapsulation significantly reduced cytotoxicity, improving human dermal fibroblast viability from 60% (free postbiotics) to over 90%.104 This approach provides a nanotechnology-based solution for local delivery bottlenecks of microbiome-derived bioactives, enabling dual modulation of local microbiota and oxidative stress.
In addition, natural polysaccharides from TCM, cell-penetrating peptide (CPP)-modified macromolecular antibacterial or immune-modulating agents, and smart carriers such as pH- or ROS-responsive nano-systems can all be integrated with microbiome-targeted interventions to achieve lesion-specific, spatiotemporally controlled delivery while minimizing impact on healthy skin microbiota. Research integrating 3D-printed microneedle arrays with microbiome-modulating agents has also begun, enabling programmable release of active components across different skin layers by controlling microneedle geometry, providing a novel engineering approach for personalized microbiome interventions. Collectively, microbiome-targeted transdermal therapy for AD is evolving from “single-component delivery” toward a multidimensional integration of “carrier–active agent–microbiome modulation,” with the incorporation of nanocarrier engineering significantly expanding the scope of local AD therapy and providing a potential platform for gut–skin axis intervention (Table 2).
 |
Table 2 Applications and Characteristics of Nanoscale Delivery Systems Regulated by the Gut-Skin Axis |
The Regulatory Effects of Micron-Scale Transdermal Delivery Systems on the Skin Barrier and the Gut-Skin Axis
The Role of Dissolving Microneedles (MNs) Array Delivery in Precision Intervention and Gut–Skin Axis Regulation in AD
Dissolving microneedle arrays penetrate the stratum corneum barrier under painless or low-pain conditions through micron-scale needles, creating controlled transient delivery channels at the epidermal–dermal junction, thereby enabling efficient localized release of therapeutic molecules (Table 3). Unlike nanoscale delivery systems that rely on diffusion or endocytosis, microneedles directly bypass the stratum corneum barrier via a “structural barrier remodeling” approach, allowing rapid accumulation of macromolecular drugs such as peptides, proteins, and nucleic acids within the local inflammatory microenvironment. In AD therapy, dissolving microneedles can precisely deliver glucocorticoids (eg, triamcinolone, dexamethasone) or immunomodulatory molecules to inflamed dermal regions, thereby more effectively suppressing the local expression of Th2-associated cytokines such as IL-4, IL-13, and IL-31.109,110
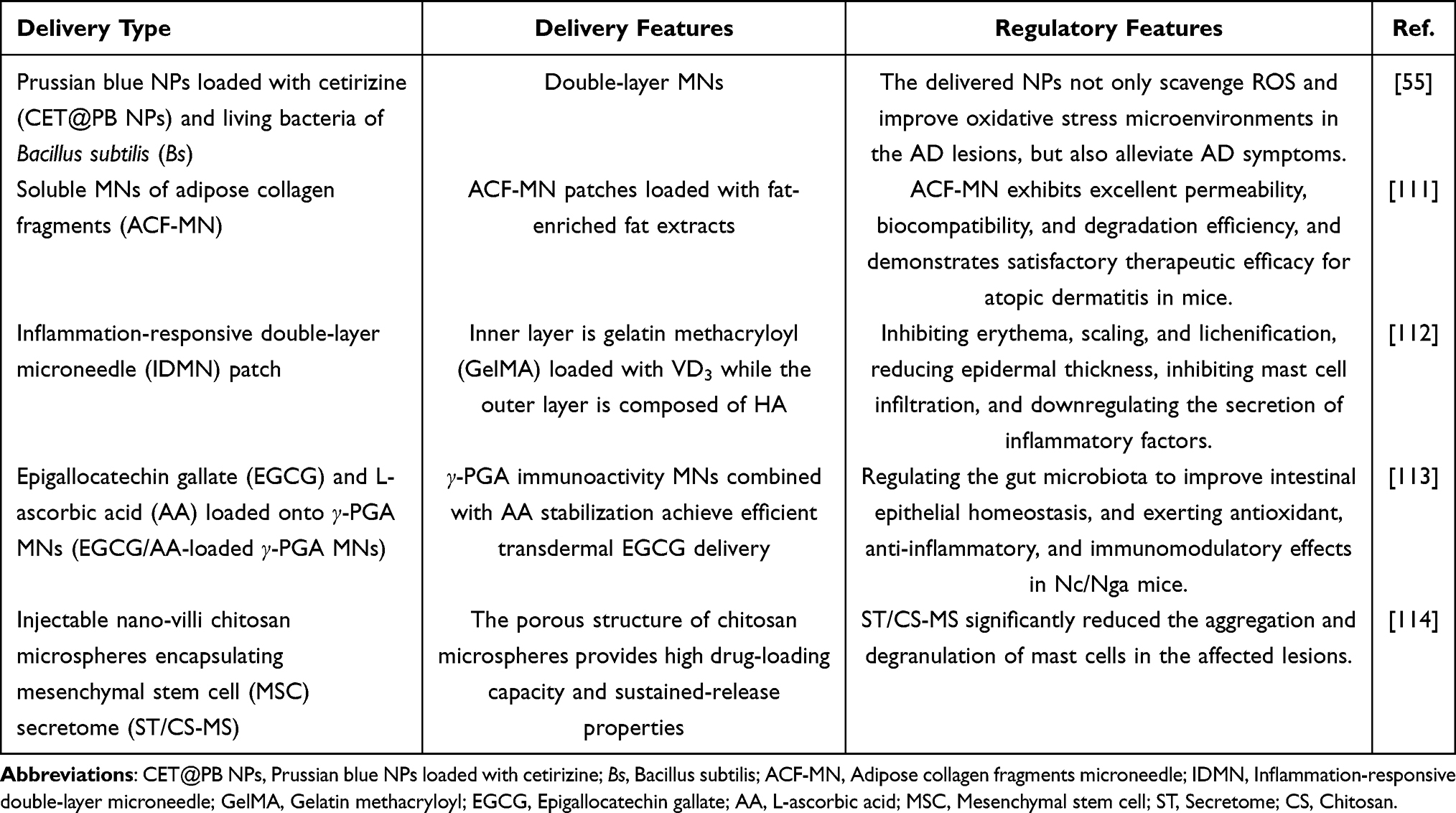 |
Table 3 Regulatory Effects of Micron-Scale Transdermal Delivery Systems on the Skin Barrier and the Gut-Skin Axis |
From the perspective of gut–skin axis regulation, the core value of dissolving microneedles lies not only in local inflammation control but also in their modulatory effect on “skin-derived systemic immune signal input”. The persistently elevated Th2-type inflammatory cytokines and epithelial-derived alarmins in AD lesions can amplify peripheral immune responses through the circulatory route and further affect intestinal mucosal immune homeostasis.115 By reducing the sustained release intensity of these signals, MNs-mediated efficient local delivery helps attenuate the aberrant driving force from the skin toward the systemic immune network, thereby indirectly alleviating the inflammatory amplification loop of the gut–skin axis.116
In recent years, the material systems of dissolving microneedles have gradually expanded to incorporate natural bioactive components. For instance, polysaccharides derived from C. okamuranus exhibit considerable promise in AD treatment, attenuating epidermal hyperplasia and inflammation via induction of tolerogenic dendritic cells that subsequently activate regulatory T cells and suppress Th2‑associated cytokines, including TSLP, IL‑5, and IL‑33.117 Polysaccharides also benefit intestinal regulation. Being macromolecules, they resist gastric metabolism and are efficiently utilized in the gut. They act as carbon/energy sources for selective gut microbes, shaping microbial composition. Furthermore, they modulate intestinal immunity, alter microbiota, and boost SCFAs production to relieve AD.118 To address the chronic, recurrent nature of AD and the need for long-term maintenance therapy, multi-layered or graded-structure dissolving microneedles (eg, PLGA–HA composite systems) enable a time-programmed release strategy featuring “rapid onset–sustained maintenance”.119 In the initial phase, rapid release reduces local inflammatory burden; in the later phase, sustained release from the reservoir structure maintains immune homeostasis, thereby reducing inflammatory recurrence and systemic immune fluctuations, and further stabilizing the immune signaling crosstalk network between the skin and the gut.
Overall, dissolving microneedle arrays are not only an efficient transdermal delivery tool but also an important engineering platform that bridges “local barrier repair” and “systemic immune homeostasis remodeling (gut–skin axis)”, providing a novel technological pathway for stratified therapy and long-term management of AD.
Application of Porous Microsphere Delivery Systems
Porous microspheres (particle size 5–300 μm), due to their dimensions being far larger than the pore size of the stratum corneum, are unable to penetrate an intact skin barrier. Paradoxically, this “limitation” confers a unique advantage for localized epidermal drug delivery.120 After drug loading within their porous network, microspheres primarily remain on the skin surface and in the superficial layers beneath the stratum corneum, with minimal dermal deposition. This enables maintenance of an effective local drug concentration while significantly reducing the risk of systemic absorption. This property is particularly important for AD therapy, as patients often exhibit impaired skin barrier function, and increased systemic absorption may lead to unnecessary adverse effects. The high drug-loading capacity and sustained-release characteristics of porous microspheres make them ideal carriers for poorly water-soluble natural bioactive compounds such as naringenin and asiaticoside. For example, a naringenin microsponge gel achieved approximately threefold higher skin deposition compared with conventional gels, without causing skin irritation.121 From the perspective of gut–skin axis synergy, porous microspheres concentrate active compounds within the epidermis, effectively suppressing local inflammatory mediators such as TNF-α and IL-6, thereby reducing leakage of inflammatory signals into systemic circulation. Meanwhile, carrier materials such as PLGA and CS derivatives can be engineered to possess prebiotic-like activity, and their degradation fragments may indirectly modulate the gut microbiota via lymphatic absorption.122 Accordingly, porous microspheres provide a “high epidermal local concentration–low systemic exposure” safety strategy, offering a feasible technological approach for long-term topical AD therapy and gut–skin axis–oriented disease management.
Overall, micron‑scale transdermal delivery systems (including dissolving microneedles and porous microspheres) exhibit clear differentiation and complementarity with nanoscale delivery systems (Figure 9): while nanocarriers excel in deep tissue penetration and target recognition, micron‑scale systems offer advantages in interfacial retention, programmed release, and regulation of cross‑system immune signaling. Together, they construct a multi‑level delivery framework that spans from “local barrier intervention” to “systemic immune remodeling”, thereby providing engineering‑based technical support for stratified therapy of AD and long‑term disease management aligned with the gut–skin axis.
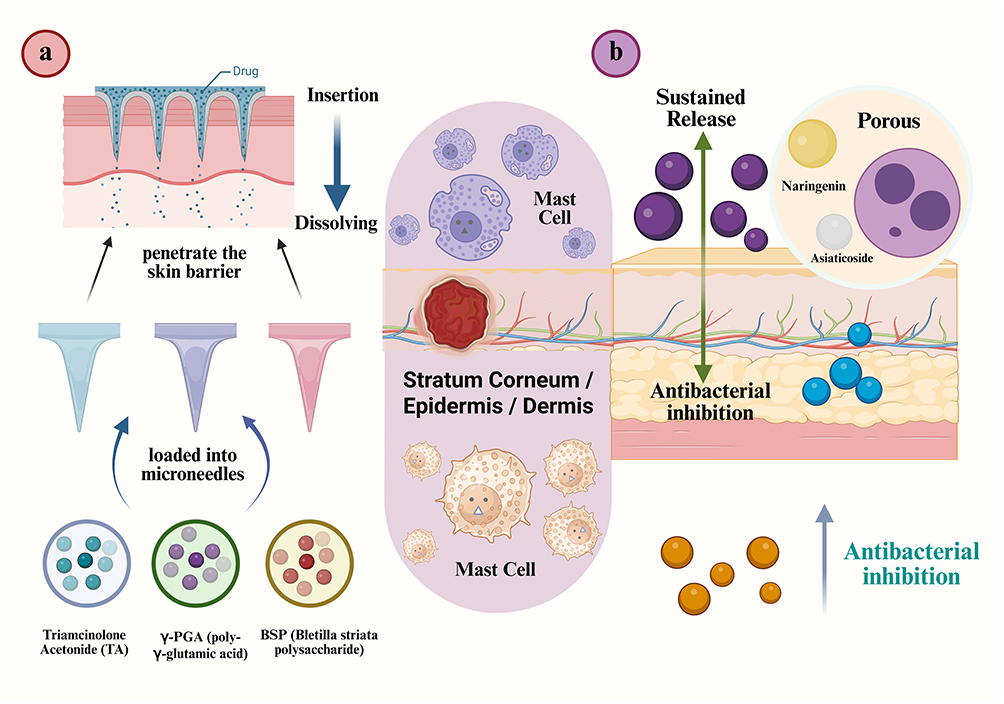 |
Figure 9 Delivery mechanisms for drug release: MNs and porous microspheres. (a) Dissolving MNs loaded with triamcinolone acetonide (TA), γ‑PGA, and Bletilla striata polysaccharide penetrate the skin barrier and dissolve within the stratum corneum, epidermis, and dermis to release drugs, targeting local inflammatory regions and mast cells to alleviate inflammation. (b) Porous delivery systems loaded with naringenin, asiaticoside, and other active components achieve sustained drug release within the skin, enhancing local antimicrobial effects and prolonging therapeutic efficacy. Abbreviations: TA, Triamcinolone acetonide; BSP, Bletilla striata polysaccharide; γ-PGA, poly-γ-glutamic acid. |
A Platform for Remodeling the Skin Microenvironment and Regulating the Gut-Skin Axis Based on Hydrogel Interfaces
A Composite Hydrogel-Based System for Local Immune Modulation and Intervention via the Gut-Skin Axis
As a typical soft matter interfacial material, composite hydrogels have gradually expanded their role in AD from a “local drug carrier” to a “skin microenvironment modulation platform”. By constructing an interfacial layer with high water content and low mechanical irritation, these materials create a stable physical buffering zone on the surface of lesional skin, thereby reducing the sustained activation effect of external stimuli on the compromised barrier (Figure 10).
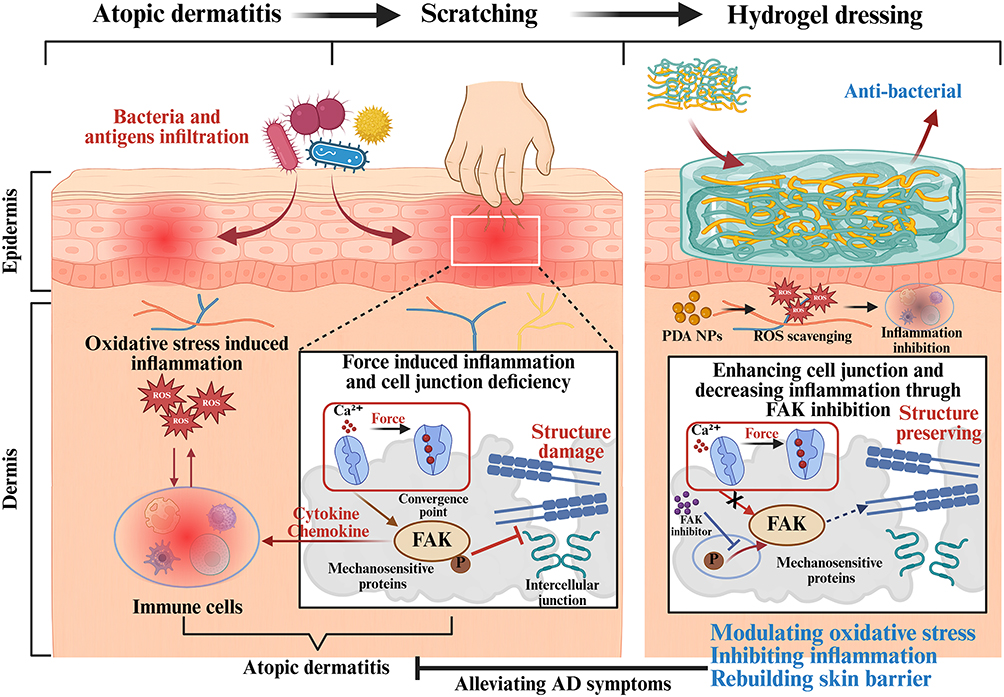 |
Figure 10 Application of hydrogel transdermal delivery systems for improving AD. Abbreviations: FAK, Focal adhesion kinase; PDA, Polydopamine nanoparticles. |
Under AD pathological conditions, disruption of the stratum corneum structure together with exposure of nerve endings leads to a marked increase in local sensitivity and persistently amplifies the inflammatory cycle.2 Through their flexible three-dimensional network, composite hydrogels can effectively reduce local friction and irritation, providing a “low-stress recovery window” for the compromised barrier, thereby indirectly promoting spontaneous repair of the epidermal structure.123 Unlike conventional transdermal delivery systems that emphasize “drug entry into the skin”, composite hydrogels highlight their role as a “signal-buffering layer”. The hydrated interface they form on the skin surface attenuates the diffusion gradient of local inflammatory mediators, flattening the local peaks of IL-4, IL-13, and other inflammatory mediators, thereby reducing their sustained output intensity into the circulatory system. Furthermore, certain bioactive polysaccharide- or natural polymer-based hydrogels, upon contact with the skin surface microbiota, can alter the local nutritional and hydration status, thereby affecting the ecological structural stability of the resident skin flora.124 This alteration does not directly kill or inhibit bacteria but indirectly promotes the restoration of commensal bacteria predominance through a “microenvironment rebalancing” approach.
From the perspective of the gut–skin axis, the sustained release of inflammatory signals from AD lesions is considered a major source driving systemic immune imbalance.9 By reducing the amplitude of local inflammatory fluctuations and the intensity of signal output, composite hydrogels can alleviate the sustained activation burden on the peripheral immune system, thereby attenuating the immune coupling amplification effect between the skin and the gut at its source. This regulatory mechanism does not rely on systemic intervention but achieves indirect modulation of cross-organ inflammatory propagation through “local signal buffering”.
Overall, composite hydrogels are not merely a class of topical drug delivery vehicles but also serve as important interfacial materials that connect the skin physical barrier, local immune homeostasis, and the systemic inflammatory network, offering a novel materials-based pathway for long-term AD management and gut–skin axis homeostasis reconstruction.
Self-Assembled Hydrogel-Driven Skin Interface Remodeling and Coordinated Regulation of the Gut-Skin Axis
Self-assembled hydrogels are three-dimensional supramolecular network systems spontaneously organized from natural small molecules, polysaccharides, or peptides through noncovalent interactions such as hydrogen bonding, π–π stacking, and hydrophobic interactions (Figure 11).125 Unlike conventional composite hydrogels, which rely on a structural framework consisting of a polymeric matrix loaded with active agents, the essence of self-assembled hydrogels lies in the fact that the bioactive molecules themselves serve as the structural building blocks, thereby establishing an integrated material paradigm in which structure and function are inherently unified. In such systems, therapeutic molecules not only exert pharmacological effects but also directly determine the spatial architecture and stability of the hydrogel network, endowing the material with a highly integrated capacity for interfacial regulation. This “drug-as-architecture” characteristic enables self-assembled hydrogels to form a highly biomimetic and flexible network interface on the skin surface, providing continuous structural support and microenvironmental stabilization for the damaged stratum corneum.
 |
Figure 11 Assembly mechanisms and applications of hydrogels formed by the interaction and co-assembly of small molecules designed to improve AD. Abbreviations: GA, glycyrrhetic acid; CU, cryptotanshinone-peptide conjugate. |
Under the pathological conditions of AD, skin barrier disruption is often accompanied by disturbances in the local microenvironment, including impaired hydration, surface charge imbalance, and fluctuations in the skin microbiota.3 Owing to their dynamically reconfigurable supramolecular networks, self-assembled hydrogels can adaptively respond to local environmental changes without the need for strong external stimuli, thereby gently remodeling the physicochemical state of the skin surface.126 This interfacial adaptability represents a key advantage that distinguishes them from conventional delivery systems.
More importantly, multicomponent self-assembled systems can integrate natural molecules with distinct pharmacological properties into a unified functional architecture through intermolecular cooperative interactions, enabling multidimensional biological regulation within a single material platform. For example, polyphenol–alkaloid and polysaccharide–flavonoid systems can co-assemble into stable nano-/microscale network structures, enhancing local bioadaptability while maintaining material stability.127,128 This mode of structural integration reduces reliance on exogenous carriers and minimizes the biological uncertainty associated with material heterogeneity.
From the perspective of gut–skin axis regulation, the primary significance of self-assembled hydrogels lies not in improving drug delivery efficiency, but in their ability to systematically “reduce noise” within the inflammatory signaling environment of the skin. By stabilizing the local microenvironment and minimizing stimulus-induced overactivation of immune cells, these systems can reduce the sustained release of epithelial-derived signals, including Th2-associated inflammatory mediators, thereby attenuating their long-term driving effects on systemic immunity. This signal-source regulation strategy provides a novel materials-based approach for mitigating inflammatory coupling between the skin and the gut.
Furthermore, some naturally derived self-assembled systems may release small bioactive fragments with metabolic regulatory potential during degradation or dynamic network remodeling. Following local absorption or systemic transport, these components may contribute to the indirect regulation of immune homeostasis.129 Although the mechanisms underlying such distal effects remain to be fully elucidated, they offer important insights into the cross-scale interactions among local biomaterials, systemic immunity, and the intestinal microenvironment. Overall, guided by the design principle that molecular structure itself serves as the functional unit, self-assembled hydrogels integrate local skin interface reconstruction with systemic inflammatory signal regulation, providing a promising therapeutic framework for AD that combines material adaptability with the potential for cross-organ immune modulation.
Multiscale Delivery Systems and Synergistic Regulation of the Gut–Skin Axis
AD is increasingly recognized as a systemic disorder characterized not only by localized skin inflammation but also by dysregulated immune–metabolic communication along the gut–skin axis.10 In this context, multiscale drug delivery systems, spanning molecular, nano-, micro-, and macroscopic hydrogel platforms, provide a hierarchical and coordinated strategy to simultaneously regulate cutaneous lesions and distant intestinal immune homeostasis. The fundamental advantage of these systems lies in their ability to integrate spatially targeted delivery with temporally controlled release, thereby bridging local skin microenvironment modulation and systemic immunological rebalancing.
From a mechanistic perspective, different delivery scales correspond to distinct regulatory layers of the gut–skin axis. Nanoscale systems (liposomes, polymeric nanoparticles, self-assembled nanostructures, and exosome-like vesicles) primarily function at the cellular and subcellular levels, modulating keratinocyte signaling, antigen presentation, and Th2 immune polarization. These nano-systems can effectively suppress key cytokines such as IL-4, IL-13, and IL-31, thereby reducing systemic inflammatory spillover that contributes to intestinal immune activation. Microscale systems, including dissolving microneedles and porous microspheres, act as intermediate modulators by enhancing epidermal penetration efficiency and providing depot-like drug reservoirs within the stratum corneum and superficial dermis. These platforms ensure sustained suppression of local inflammatory signaling, thereby limiting chronic immune crosstalk between skin and gut.
At the macroscopic level, hydrogel-based systems serve as an interface for prolonged local intervention and barrier reconstruction. Composite and self-assembled hydrogels not only maintain a hydrated microenvironment conducive to epidermal repair but also function as long-term cytokine regulation reservoirs. By continuously suppressing Th2-skewed inflammatory mediators and restoring filaggrin-mediated barrier integrity, hydrogels reduce the systemic dissemination of inflammatory signals that may perturb gut microbiota composition and intestinal mucosal immunity. Importantly, the synergistic effect of multiscale systems arises from their hierarchical integration rather than isolated function. For instance, nanoscale carriers embedded within hydrogel matrices or delivered via microneedles can achieve sequential release profiles, where rapid anti-inflammatory action is followed by sustained immunomodulation.130 Simultaneously, polysaccharide-based carriers and degradation products from these systems may act as prebiotic-like modulators, influencing gut microbial composition and SCFAs production after systemic distribution.131 This establishes a bidirectional feedback loop in which skin-targeted therapy indirectly reshapes intestinal microbial ecology, while gut-derived metabolites further reinforce cutaneous immune homeostasis.
Overall, multiscale delivery systems provide a unified framework for translating local dermatological intervention into systemic immunoregulatory outcomes. By coordinating spatially distinct yet functionally interconnected delivery modalities, they offer a rational strategy for breaking the chronic inflammatory amplification loop characteristic of AD and achieving long-term stabilization of the gut–skin axis.
Multiscale Transdermal Delivery and Skin–Gut Axis Regulation Driven by Cutting-Edge Engineering Technologies
With the continuous advancement of multiscale transdermal delivery systems, engineering strategies are propelling the field into a new era of precision, intelligence, and personalization.132 These breakthroughs not only enhance transdermal efficiency and local targeting of drugs but also address key challenges such as dynamic monitoring, responsive regulation, and multimodal therapy in the complex pathological environment of skin diseases. In recent years, permeation-enhancing techniques mediated by physical energy, intelligent wearable systems, as well as programmable delivery platforms have emerged as research frontiers, showing unique application prospects in the delivery of active ingredients from TCM.
Energy-Driven Modulation of the Skin Barrier and Gut–Skin Axis-Responsive Transdermal Delivery
Energy-driven transdermal delivery technologies utilize external physical fields to temporarily disrupt or bypass the stratum corneum barrier, thereby significantly enhancing drug penetration.133 Unlike conventional formulation-based strategies, these methods enable on-demand, spatially and temporally controlled transdermal enhancement, making them particularly suitable for macromolecular drugs or nanocarrier systems, which have limited passive diffusion capabilities. In the treatment of AD, where the skin barrier is compromised and exhibits marked heterogeneity, energy-assisted delivery can increase local drug concentration while reducing systemic exposure, helping to modulate local immune responses and maintain skin microbiome balance, thereby indirectly optimizing gut–skin axis signaling.
Iontophoretic Delivery for Inflammatory Signal Regulation Along the Gut–Skin Axis
Iontophoresis (IP) enhances transdermal delivery by applying a low-intensity (typically 0.1–0.5 mA/cm2) continuous or pulsed direct current, utilizing the synergistic effects of electrorepulsion and electroosmosis to drive charged therapeutic molecules or colloidal carriers across the skin barrier.134 Within the context of the gut–skin axis, iontophoresis can enable nanocarriers loaded with anti-inflammatory or microbiome-modulating agents to precisely target AD inflammatory lesions, suppress local levels of IL-4, IL-13, and TSLP, and simultaneously reduce the aberrant stimulation of intestinal mucosal immunity by these mediators, thereby modulating systemic Th2-biased inflammation.
In engineered transdermal systems, iontophoresis can be combined with nanocarriers such as liposomes and polymeric nanoparticles.135 Positively charged carriers migrate directionally toward deeper skin layers under anodic iontophoresis, whereas negatively charged carriers can be guided toward targeted delivery under cathodic conditions. This “electric field–carrier” synergistic strategy significantly enhances the localized accumulation of drugs within AD inflammatory lesions while reducing nonspecific distribution.
More importantly, drug flux can be precisely programmed by modulating current density, application duration, and electrode polarity, enabling a dual-phase delivery profile consisting of rapid loading (achieving therapeutic levels within minutes) followed by sustained release (continuous infusion under low current). From an engineering perspective, iontophoresis can be integrated into flexible wearable patches that dynamically adjust output parameters according to disease flare and remission states in AD, thereby providing a programmable driving force for personalized transdermal therapy.
Electroporation-Mediated Reversible Barrier Remodeling and Macromolecular Delivery Across the Gut–Skin Axis
Electroporation employs short, high-voltage electric pulses (typically 50–1500 V, with pulse durations in the microsecond to millisecond range) to transiently create hydrophilic aqueous pores within the lipid bilayers of the stratum corneum, thereby significantly enhancing skin permeability.136 Unlike iontophoresis, which relies on continuous ion migration, electroporation primarily achieves reversible barrier disruption through electrically induced structural perturbations. The resulting microchannels can range from tens to hundreds of nanometers in diameter, allowing rapid penetration of peptides, proteins, nucleic acids, and nanocarriers into the epidermis and even the dermis. When electrical pulse parameters (voltage, number of pulses, pulse width) are appropriately controlled, these channels spontaneously close within minutes to tens of minutes without causing permanent tissue damage.
Recent engineering advances have integrated miniaturized electroporation modules into wearable transdermal devices, using flexible electrode arrays to achieve localized, controllable permeability enhancement in target lesion areas while substantially reducing patient discomfort and skin irritation.137 In AD, electroporation can create an on-demand “drug-entry window”, facilitating the local delivery of gene-editing therapeutics, siRNA, and microbiome-derived nanocarriers (AKK-EVs).60 By enhancing the penetration and bioavailability of these advanced therapeutics within skin lesions, electroporation may enable simultaneous modulation of the cutaneous inflammatory microenvironment and gut–skin axis-associated immune signaling, thereby providing a promising strategy for integrated local and systemic regulation.
Ultrasound-, Thermal-, and Laser-Assisted Enhancement of Skin Permeability and Microenvironment Reprogramming
Beyond electric field-based methods, various physical energy modalities have been developed to enhance skin permeability, each relying on distinct biophysical mechanisms. Ultrasound-mediated delivery (also known as sonophoresis) primarily utilizes low-frequency ultrasound (20–100 kHz) to induce cavitation: microbubbles form and collapse on the stratum corneum surface, generating shock waves and microjets that transiently disrupt the ordered lipid arrangement, thereby facilitating transdermal absorption of both small and large molecules.138 High-frequency ultrasounds (>1 MHz) mainly leverage thermal and mechanical effects to increase membrane fluidity.139
Thermal-assisted strategies, such as radiofrequency heating or thermal pulses, locally raise the temperature to 40–45 °C, transforming stratum corneum lipids from a gel to a liquid-crystalline state, reducing viscosity, increasing diffusion coefficients, and enhancing the mobility of nanocarriers.140 Laser systems, particularly fractional ablative lasers like Er:YAG or CO2 lasers, create microchannel arrays (diameters 50–200 μm, adjustable density) in a highly controlled spatial pattern on the skin surface, enabling localized and repeatable drug deposition while preserving surrounding healthy tissue as a rapid repair “reservoir”.141
Notably, these energy-driven approaches are not mutually exclusive and can be synergistically integrated with micro- or nanoscale delivery systems to form a “device–carrier–energy” composite framework. For example, ultrasound combined with microbubbles can enhance transcellular transport of nanoparticles, while laser-pretreated skin combined with iontophoresis can further reduce the required energy intensity.142,143 Interestingly, when integrated with micro- or nanoscale delivery systems, these energy-assisted approaches can precisely regulate drug distribution within inflammatory skin lesions, enabling multidimensional modulation of local Th2-driven inflammation, oxidative stress, and skin microbiota composition. Such effects may further influence gut–skin axis signaling by reducing peripheral inflammatory amplification and restoring immune–microbial homeostasis.
Intelligent Wearable Patches and Microneedle Systems for Closed-Loop Regulation of the Skin–Immune–Gut Axis
The integration of electronic skin and flexible sensor technologies has introduced a new paradigm for intelligent and precise transdermal delivery systems. These systems incorporate flexible sensors into hydrogels, polymer films, or wearable patches to enable real-time monitoring of multidimensional parameters such as local skin pH, temperature, moisture, and mechanical stress. More recently, a study has proposed a paper-based, battery-powered, ion-electroosmosis-driven microneedle patch (PBIMNP) for self-administration and personalized treatment of skin diseases (Figure 12).144 The collected signals can be converted into quantifiable data via electrochemical, optical, or resistive changes, and interfaced with drug delivery modules to achieve a closed-loop “sensing–feedback–response” regulation.145 In practical applications, researchers have developed a flexible e-patch based on HA that serves simultaneously as a moisturizing agent, drug carrier, and sensor support platform.146 Aloe polysaccharides loaded within the patch not only exhibit anti-inflammatory and barrier-repairing properties but also interact with local skin moisture signals to form a feedback mechanism. When excessive dryness is detected, the sensor triggers the control module to adjust the drug release rate, thereby providing enhanced moisturizing and reparative effects.
 |
Figure 12 A paper-based, battery-powered, ion-electroosmosis-driven microneedle patch (PBIMNP) for self-administration and personalized treatment of skin diseases. Notes: The pink (α1), purple (α2), and blue (α3) lines represent the three branches of the gelatin triple helix structure. |
The above studies demonstrate the potential for integrating active ingredients from TCM with flexible electronics technology. This emerging strategy offers a personalized and intelligent intervention approach for chronic skin diseases such as AD, eczema, and psoriasis, and also opens new avenues for the precise delivery of TCM active components.
The integration of smart dressings with soluble MNs technology provides a novel strategy for precise and controllable transdermal drug delivery. According to reports, a research team has designed a microneedle system based on sodium alginate (SA), the carbohydrate-recognizing molecule Con A, and the antimicrobial agent Reuterin (Figure 13).147 This system enables the targeted delivery of the antimicrobial agent and the controlled release of NO, and combines multiple functions such as biofilm penetration, antimicrobial activity, anti-inflammatory effects, and tissue regeneration. Although this platform has not yet been directly applied to the treatment of AD, its design philosophy and functional characteristics offer potential technical insights for multi-target interventions in the AD microenvironment. These systems typically combine MNs arrays with sensors, electronic feedback modules, or responsive hydrogels to form an integrated “delivery–monitoring–regulation” platform. The MNs penetrate the stratum corneum to create microchannels, allowing drugs to act directly on the AD, thereby significantly enhancing delivery efficiency while minimizing systemic side effects.148 The inclusion of sensors enables real-time monitoring of local physiological parameters, such as inflammatory factor levels, pH, skin hydration, providing intelligent feedback for dynamic regulation of drug release. For example, a dissolvable microneedle patch loaded with the TCM-derived active compound tanshinone IIA has been shown in AD models to achieve localized delivery of anti-inflammatory agents while simultaneously providing dynamic feedback on the inflammatory status of lesions.149 This integrated approach enables coordinated regulation of skin barrier integrity, local immune responses, and microbial homeostasis. By synchronously adjusting local drug concentrations and microenvironmental conditions, such intelligent delivery systems may also contribute to stabilizing gut–skin axis function and mitigating the systemic inflammatory signals associated with AD progression.
 |
Figure 13 Design of a Novel multifunctional metal nanowire patch loaded with RE@SA-Con A/SNO NPs. Abbreviations: SA, Sodium alginate; Con A, Concanavalin A; NO, Nitric oxide; RE, Reuterin; RE@SA Con A/SNO NPs, Reuterin@Sodium alginate Concanavalin A/Nitric oxide nanoparticles. Note: The red downward arrow indicates a decrease in the levels of the pro-inflammatory factors of IL-6 and TNF-α, as well as a decrease in the number or proportion of M1 cells. |
3D-Printed and Programmable Delivery Platforms for Precision Gut–Skin Axis Modulation
With advances in micro- and nanofabrication technologies, 3D-printed microneedle arrays have emerged as an important tool for precise transdermal delivery.150 By controlling the geometric features of the microneedles, such as needle length, density, arrangement, and tip angle—drug delivery can be targeted to specific skin layers, meeting tailored therapeutic requirements. For instance, using TCM active components, researchers have employed alginate-gelatin composite materials as MNs substrates, loading catecholamines to construct a 3D-printed MNs array that exhibits distinct layer-specific release profiles (Figure 14).151 In the epidermis, catecholamines is rapidly released to exert antimicrobial effects and inhibit bacterial colonization on the skin surface, while in the dermis, the MNs dissolve slowly, enabling sustained drug release. This approach reduces recurrent inflammation and improves the local immune microenvironment. Such structurally tunable MNs arrays not only enhance the transdermal efficiency of active components but also improve local bioavailability, offering precise therapeutic strategies for chronic inflammatory skin diseases.
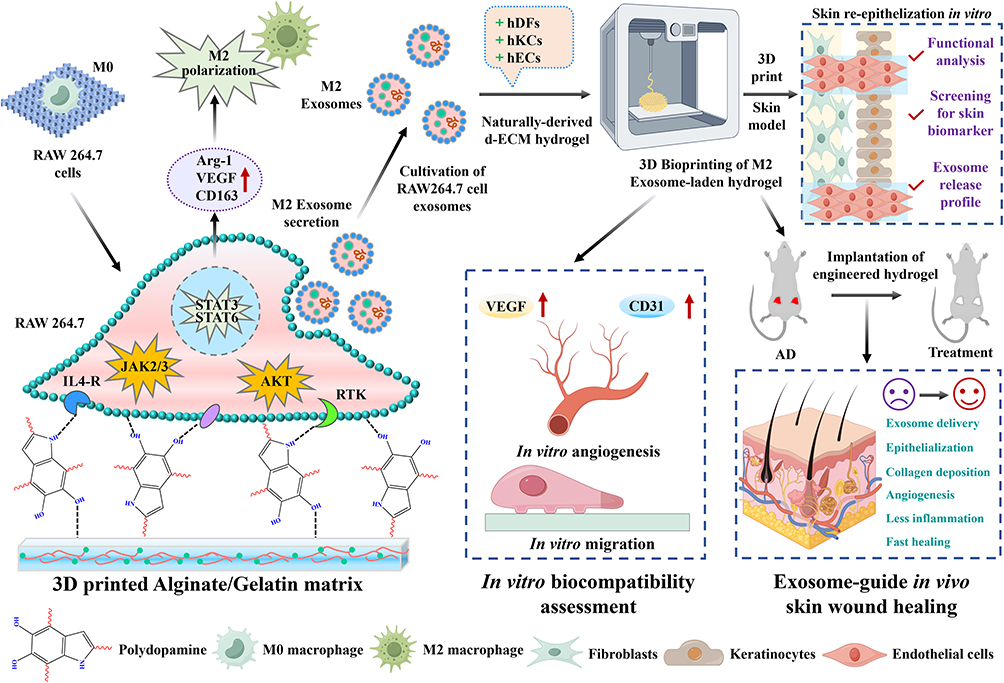 |
Figure 14 A bioink design to enhance M2 macrophage polarization and Exo, as well as 3D bioprinting of skin cells to improve AD. This is primarily achieved by developing a catecholamine-based bioink (Alg/Gel/PDA NSPs) that promotes macrophage adhesion, proliferation, and polarization. Abbreviations: Exo, Exosome; Alg/Gel/PDA NSPs, Alginate/gelatin/polydopamine nanospheres; Arg-1, Arginase 1; IL4-R, Interleukin-4 receptor tyrosine kinases; hDFs, Human dermal fibroblasts; hKCs, Keratinocytes; hECs, Human endothelial cells; d-ECM, Decellularized extracellular matrix; M0, Unpolarized macrophages. Notes: The red upward arrow indicates elevated levels of VEGF, CD31, CD163, and Arg-1. |
Programmable microneedle systems based on multi-material printing or layered assembly can achieve sequential release of multiple drugs, tailored to the complex course of disease.152 Studies have shown that by designing layered microneedles, anti-inflammatory drugs such as matrine can be positioned in the upper layer for rapid early-stage suppression of inflammation, while pro-repair factors like EGF are embedded in the deeper layer to sustain later-stage tissue repair and angiogenesis.153 This strategy fully leverages the spatial advantage of multilayer structures, enabling drugs to be delivered according to disease progression, thereby significantly improving healing outcomes in chronic wounds or AD. Furthermore, by precisely designing the microneedle architecture, anti-inflammatory drugs can act rapidly on the epidermis to suppress Th2 inflammation, while pro-repair factors are slowly released in the dermis to improve barrier function and the local immune microenvironment. Combining this with responsive hydrogels or nanocarriers allows further modulation of release kinetics, enabling precise intervention targeting the skin microbiota and the gut–skin axis.154
Overall, 3D-printed microneedles and programmable multilayer systems provide high-efficiency, targeted, and temporally controlled drug delivery. They are particularly well-suited for the application of TCM active components in complex skin disease courses, offering a new engineering solution for intelligent transdermal therapy.
Bridging Gut–Skin Axis Biology and Transdermal Delivery Engineering
Although substantial progress has been achieved in transdermal drug delivery for AD, the integration of gut–skin axis biology with multi-scale delivery engineering remains at an early stage. Current studies primarily focus on improving local drug penetration, retention, and anti-inflammatory efficacy, whereas the systemic regulatory consequences of transdermal interventions on gut microbiota, intestinal immunity, and gut-derived metabolites remain insufficiently understood. Future research should therefore move beyond conventional evaluations of skin lesion improvement and establish mechanistic frameworks that simultaneously assess cutaneous responses, intestinal barrier integrity, microbial composition, metabolite profiles, and systemic immune signaling. Such multidimensional analyses will be essential for determining whether local transdermal interventions can genuinely influence gut–skin axis homeostasis rather than merely alleviate skin symptoms.
A second priority is the development of gut–skin axis-oriented delivery systems. Most currently reported carriers are designed to overcome the skin barrier or achieve local controlled release, while relatively few are engineered to regulate both local and systemic disease drivers. Emerging evidence suggests that microbial metabolites, including short-chain fatty acids, tryptophan-derived metabolites, and bile acid derivatives, participate in immune communication between the intestine and skin. Future delivery platforms may therefore incorporate prebiotics, postbiotics, microbial metabolites, or natural compounds capable of modulating gut microbiota, enabling transdermal systems to function not only as local drug depots but also as regulators of systemic immune–microbial networks. In particular, natural-product-based self-assembled nanostructures and plant-derived extracellular vesicles represent promising candidates because they combine intrinsic bioactivity with delivery functionality and may provide a direct mechanistic bridge between local skin treatment and gut–skin axis regulation.
From an engineering perspective, future advances are expected to arise from the convergence of responsive materials, wearable devices, and programmable delivery technologies. The pathological microenvironment of AD is highly dynamic, characterized by fluctuations in pH, reactive oxygen species, protease activity, microbial colonization, and inflammatory mediator production. Accordingly, next-generation systems should evolve from passive carriers toward intelligent platforms capable of sensing disease-associated signals and adapting drug release in real time. Integration of microneedles, smart patches, biosensors, electroporation modules, and wireless monitoring systems may enable closed-loop therapeutic strategies that continuously synchronize drug administration with disease activity, thereby improving therapeutic precision and reducing overtreatment.
Finally, clinical translation remains the most critical challenge. Most current studies are confined to in vitro experiments or animal models, and direct evidence supporting gut–skin axis modulation through transdermal delivery in AD patients remains scarce. Future clinical investigations should incorporate biomarkers related to intestinal microbiota, circulating cytokines, microbial metabolites, and immune-cell dynamics in addition to conventional dermatological endpoints. Establishing standardized evaluation criteria and mechanistic clinical evidence will be crucial for validating the therapeutic relevance of gut–skin axis-targeted transdermal interventions.
Overall, the future development of transdermal therapy for AD should move beyond merely improving skin barrier penetration and instead focus on how to leverage the skin as an entry point to systematically remodel the gut–skin axis. This shift will elevate transdermal delivery from a tool for local symptom control to a cross-organ, multiscale platform for precise immune modulation, offering new technological avenues for long-term management and personalized treatment of AD.
Abbreviations
AD, Atopic dermatitis; TCM, Traditional Chinese medicine; Th2, T helper 2/type 2 helper T-cell response; ZO-1, Zonula occludens-1; IL-4, Interleukin-4; IL-13, Interleukin-13; DSS, Dextran sulfate sodium; SCORAD, SCORing atopic dermatitis index; TEWL, Transepidermal water loss; DNFB, 2,4-dinitrofluorobenzene; IL-1β, Interleukin-1 beta; TNF-α, Tumor necrosis factor-alpha; IFN-γ, Interferon-gamma; IL-6, Interleukin-6; IL-10, Interleukin-10; SCFAs, Short-chain fatty acids; AhR, Aryl hydrocarbon receptor; Treg/Tregs, Regulatory T cell(s); LCSFA, Long-chain saturated fatty acid(s); ILC3, Group 3 innate lymphoid cells; FAO, Fatty acid oxidation; IgE, Immunoglobulin E; LGG, Lactobacillus rhamnosus GG; Foxp3, Forkhead box P3; IL-5, Interleukin-5; CXCL1, C-X-C motif chemokine ligand 1; CSF2, Colony-stimulating factor 2/granulocyte-macrophage colony-stimulating factor; FICZ, 6-formylindolo[3,2-b]carbazole; FLG, Filaggrin; LF216EV, Limosilactobacillus fermentum SLAM216-derived extracellular vesicles/exosomes; TLR4, Toll-like receptor 4; TMAO, Trimethylamine N-oxide; PPP5, Protein phosphatase 5; CD4⁺, Cluster of differentiation 4-positive T cells; PPARγ, Peroxisome proliferator-activated receptor gamma; pH, Potential of hydrogen; MNs, Microneedles; CET@PB NPs, Cetirizine@Prussian blue nanoparticles; NPs, Nanoparticles; ROS, Reactive oxygen species; HA, Hyaluronic acid; POP, Purslane polysaccharide; PDNV, Purslane-derived nanovesicles; NF-κB, Nuclear factor kappa B; cCAG-STING, as written in manuscript, likely cGAS-STING pathway; CR-SAN, Coptis chinensis decoction-derived self-assembled nanoparticles; EVs, Extracellular vesicles; AKK-EVs, Akkermansia muciniphila-derived extracellular vesicles; BSGS, Butyrylated Smilax glabra resistant starch microparticles; Cur/ZnMOF, Curcumin-loaded zinc-doped ferrocyanide-derived metal-organic framework; ARNT, Aryl hydrocarbon receptor nuclear translocator; hBD-3, Human β-defensin-3; STAT6, Signal transducer and activator of transcription 6; CPP/CPPs, Cell-penetrating peptide(s); TAT, Trans-activator of transcription peptide; BER, Berberine; IL, Interleukin; IL-33, Interleukin-33; TSLP, Thymic stromal lymphopoietin; IL-25, Interleukin-25; KLK5, Kallikrein 5; KLK7, Kallikrein 7; DNA, Deoxyribonucleic acid; IL-31, Interleukin-31; TK, Thioketal; EGCG, Epigallocatechin-3-gallate; CA, Caffeic acid; BER-CA, Berberine-caffeic acid co-loaded formulation; PLGA, Poly(lactic-co-glycolic acid); CS, Chitosan; P-EVs, Plant-derived exosome-like nanoparticles/plant-derived extracellular vesicles; PELNs, Plant-derived extracellular vesicle-like nanoparticles; Th1, T helper 1/type 1 helper T-cell response; RNAs, Ribonucleic acids; SE-EVs, Staphylococcus epidermidis-derived extracellular vesicles/exosomes; S. aureus, Staphylococcus aureus; C. acnes, Cutibacterium acnes; 3D, Three-dimensional; C. okamuranus, Cladosiphon okamuranus; PLGA-HA, PLGA-hyaluronic acid composite system; IP, Iontophoresis; siRNA, Small interfering RNA; Er:YAG, Erbium-doped yttrium aluminum garnet laser; CO2, Carbon dioxide; e-patch, Electronic patch; EGF, Epidermal growth factor; PBIMNP, Paper-based, battery-powered, ion-electroosmosis-driven microneedle patch; SA, Sodium alginate.
Data Sharing Statement
No data was used for the research described in the article.
Consent for Publication
All authors have reviewed and consented to the submission of this manuscript. This manuscript has not been published in other publications.
Acknowledgments
Chi Teng and Miao He are contributed equally to this work. This research was sponsored by Yunnan Characteristic Plant Extraction Laboratory Projects [Project number: YKKF2024019]; Yunnan Fundamental Research Project [Project number: 202401AT070072]; Fundamental Research Funds for the Central Universities [Project number: 2632024TD05].
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas: took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Leung DY, Bieber T. Atopic dermatitis. Lancet. 2003;361(9352):151–35. doi:10.1016/S0140-6736(03)12193-9
2. Schuler CF, Billi AC, Maverakis E, et al. Novel insights into atopic dermatitis. J Allergy Clin Immunol. 2023;151(5):1145–1154. doi:10.1016/j.jaci.2022.10.023
3. Meledathu S, Naidu MP, Brunner PM. Update on atopic dermatitis. J Allergy Clin Immunol. 2025;155(4):1124–1132. doi:10.1016/j.jaci.2025.01.013
4. Fyhrquist N, Yang Y, Karisola P, et al. Endotypes of atopic dermatitis. J Allergy Clin Immunol. 2025;156(1):24–40.e4. doi:10.1016/j.jaci.2025.02.029
5. Zhang J, Li G, Guo Q, et al. Allergens in atopic dermatitis. Rev Allergy Immunol. 2025;68(1):11. doi:10.1007/s12016-025-09024-7
6. Park CO, Kim SM, Lee KH, Bieber T. Biomarkers for phenotype-endotype relationship in atopic dermatitis: a critical review. EBioMedicine. 2024;103:105121. doi:10.1016/j.ebiom.2024.105121
7. Li H, Zhang Z, Zhang H, et al. Update on the pathogenesis and therapy of atopic dermatitis. Clin Rev Allergy Immunol. 2021;61(3):324–338. doi:10.1007/s12016-021-08880-3
8. Sugita K. Adipose tissue remodeling via TSLP-mediated IL-4/IL-13 signaling: implications for atopic dermatitis and skin barrier. J Allergy Clin Immunol. 2024;154(2):282–284. doi:10.1016/j.jaci.2024.06.002
9. Liu S, Chen Q, Gu Y, Lei H, Li B, Qin Q. Microorganisms, microbial metabolites and precision nutrition: targeting the gut-skin axis for immune microenvironment remodeling in atopic dermatitis. Clin Rev Allergy Immunol. 2025;68(1):102. doi:10.1007/s12016-025-09112-8
10. Chen M, Wang R, Wang T. Gut microbiota and skin pathologies: mechanism of the gut-skin axis in atopic dermatitis and psoriasis. Int Immunopharmacol. 2024;141:112658. doi:10.1016/j.intimp.2024.112658
11. Xie M, Kong L, Hou L, Chen Y, Hou J. Atopic dermatitis: multi-omics insights into microbiota-driven modulation of the gut-skin axis. Microb Pathog. 2026;216:108504. doi:10.1016/j.micpath.2026.108504
12. Li S, Wu J, Peng X, Feng XQ. Unlocking the potential of transdermal drug delivery. Int J Smart Nano Mater. 2024;15(3):432–468. doi:10.1080/19475411.2024.2366210
13. Lehman H. Skin manifestations of primary immune deficiency. Clin Rev Allergy Immunol. 2014;46(2):112–119. doi:10.1007/s12016-013-8377-8
14. Fang Z, Li L, Zhang H, et al. Gut microbiota, probiotics, and their interactions in prevention and treatment of atopic dermatitis: a review. Front Immunol. 2021;12:720393. doi:10.3389/fimmu.2021.720393
15. Guo Z, Zhang Y, Zhao M, et al. Intelligent transdermal nanoparticles as synergizing advanced delivery systems for precision therapeutics. Mater Today Bio. 2025;34:102220. doi:10.1016/j.mtbio.2025.102220
16. Li J, Xia Q, Ma S, et al. Progressive microneedles for targeting and intelligent drug delivery. Asian J Pharm Sci. 2025;20(3):101051. doi:10.1016/j.ajps.2025.101051
17. Faye O, Flohr C, Kabashima K, et al. Atopic dermatitis across the globe: differences in prevalence and access to treatments. Br J Dermatol. 2023;188(6):e42. doi:10.1093/bjd/ljad145
18. Mahmud MR, Akter S, Tamanna SK, et al. Impact of gut microbiome on skin health: gut-skin axis observed through the lenses of therapeutics and skin diseases. Gut Microbes. 2022;14(1):2096995. doi:10.1080/19490976.2022.2096995
19. Fang Z, Pan T, Li L, et al. Bifidobacterium longum mediated tryptophan metabolism to improve atopic dermatitis via the gut-skin axis. Gut Microbes. 2022;14(1):2044723. doi:10.1080/19490976.2022.2044723
20. Wang N, Wu L, Su Y, Zhang C, Chen X, Yuan H. Butyrylated Smilax glabra starch relieves atopic dermatitis through gut-skin axis modulation via colon-targeted delivery. Acta Pharm Sin B. 2025;15(12):6587–6606. doi:10.1016/j.apsb.2025.10.012
21. Wang J, Zhang Y, Yuan S, et al. Gut probiotic Akkermansia muciniphila-derived extracellular vesicles deliver miR-21-5p to alleviate atopic dermatitis by targeting TLR4 signaling. Nano Res. 2026;19(3):94908421. doi:10.26599/NR.2026.94908421
22. Shi Y, He S, Li C, et al. Bifidobacterium breve Yang08 alleviates atopic dermatitis by enriching Akkermansia muciniphila and inhibiting neutrophil extracellular traps formation in mice. Adv Sci. 2026;13(20):e18588. doi:10.1002/advs.202518588
23. Isaev EZ, Babaeva RR, Shalova MA, et al. Dual microbiome restoration as a novel therapeutic strategy for moderate-to-severe atopic dermatitis. J Biochem Technol. 2025;16(2):57–65. doi:10.51847/t4R5ZQ2Sns
24. Li D, Luo ZB, Zhu J, et al. Ginsenoside F2-mediated intestinal microbiota and its metabolite propionic acid positively impact the gut-skin axis in atopic dermatitis mice. J Agric Food Chem. 2024;72(1):339–350. doi:10.1021/acs.jafc.3c06015
25. Ahyoung L, Jihye B, Minju S, et al. Atopic dermatitis-alleviating effects of lactiplantibacillus plantarum LRCC5195 paraprobiotics through microbiome modulation and safety assessment via genomic characterization and in vitro analysis. Sci Rep. 2025;15:30545. doi:10.1038/s41598-025-16102-5
26. Li S, Xu D, Zhang C, et al. Cinobufagin directly targets PDE4D to disrupt fibroblast-dendritic cell crosstalk in atopic dermatitis. Adv Sci. 2025;12(48):e01670. doi:10.1002/advs.202501670
27. Du H, Wang N, Wang C, et al. Genistein alleviates skin inflammation in atopic dermatitis by inhibiting mast cell degranulation through toll-like receptor. Phytomedicine. 2026;157:158308. doi:10.1016/j.phymed.2026.158308
28. Kim WK, Jang YJ, Han DH, et al. Lactobacillus paracasei KBL382 administration attenuates atopic dermatitis by modulating immune response and gut microbiota. Gut Microbes. 2020;12(1):1–14. doi:10.1080/19490976.2020.1819156
29. Qiu Z, Zhu Z, Liu X, et al. A dysregulated sebum–microbial metabolite–IL-33 axis initiates skin inflammation in atopic dermatitis. J Exp Med. 2022;219(10):e20212397. doi:10.1084/jem.20212397
30. Zhao Y, Yu C, Zhang J, Yao Q, Zhu X, Zhou X. The gut‑skin axis: emerging insights in understanding and treating skin diseases through gut microbiome modulation. Int J Mol Med. 2025;56(6):210. doi:10.3892/ijmm.2025.5651
31. Zheng SQ, Li P, Huang ZM, et al. Research progress on probiotic regulation of immune and metabolic functions via the gut-skin axis for the alleviation of atopic dermatitis. Food Sci. 2025;46(23):347–358. doi:10.7506/spkx1002-6630-20250515-096
32. Gangane P, Sharma V, Selokar M, et al. A review of anti-inflammatory phytoconstituents used in herbal cosmeceuticals for the treatment of atopic dermatitis. Curr Drug Deliv. 2024;21(3):312–325. doi:10.2174/1567201820666230512110344
33. Dokoshi T, Chen Y, Cavagnero KJ, et al. Dermal injury drives a skin to gut axis that disrupts the intestinal microbiome and intestinal immune homeostasis in mice. Nat Commun. 2024;15(1):3009. doi:10.1038/s41467-024-47072-3
34. Rigoni R, Fontana E, Dobbs K, et al. Cutaneous barrier leakage and gut inflammation drive skin disease in Omenn syndrome. J Allergy Clin Immunol. 2020;146(5):1165–1179.e11. doi:10.1016/j.jaci.2020.04.005
35. Ghosh SS, Wang J, Yannie PJ, Ghosh S. Intestinal barrier dysfunction, LPS translocation, and disease development. J Endocr Soc. 2020;4(2):bvz039. doi:10.1210/jendso/bvz039
36. Majamaa H, Isolauri E. Evaluation of the gut mucosal barrier: evidence for increased antigen transfer in children with atopic eczema. J Allergy Clin Immunol. 1996;97(4):985–990. doi:10.1016/s0091-6749(96)80074-1
37. Merana GR, Dwyer LR, Dhariwala MO, et al. Intestinal inflammation alters the antigen-specific immune response to a skin commensal. Cell Rep. 2022;39(9):110891. doi:10.1016/j.celrep.2022.110891
38. Yoon W, Park SH, Lee JS, et al. Probiotic mixture reduces gut inflammation and microbial dysbiosis in children with atopic dermatitis. Australas J Dermatol. 2021;62(3):e386–e392. doi:10.1111/ajd.13644
39. Liang Y, Liu G, Xie L, et al. Dendrobium candidum polysaccharide reduce atopic dermatitis symptoms and modulate gut microbiota in DNFB-induced AD-like mice. Front Physiol. 2022;13:976421. doi:10.3389/fphys.2022.976421
40. Yu L, Peng S, Chen X, et al. Intestinal dysbiosis exacerbates skin inflammation via microbial metabolite-driven Th2 cell differentiation. Immunity. 2026;59(6):1545–1560.e6. doi:10.1016/j.immuni.2026.03.019
41. Song HK, Mun SH, Han DW, et al. Probiotics ameliorate atopic dermatitis by modulating the dysbiosis of the gut microbiota in dogs. BMC Microbiol. 2025;25:228. doi:10.1186/s12866-025-03924-6
42. Trompette A, Pernot J, Perdijk O, et al. Gut-derived short-chain fatty acids modulate skin barrier integrity by promoting keratinocyte metabolism and differentiation. Mucosal Immunol. 2022;15(5):908–926. doi:10.1038/s41385-022-00524-9
43. Park H, Arellano K, Lee Y, et al. Pilot study on the forehead skin microbiome and short chain fatty acids depending on the SC functional index in Korean Cohorts. Microorganisms. 2021;9(11):2216. doi:10.3390/microorganisms9112216
44. Jimenez-Sanchez M, Celiberto LS, Yang H, Sham HP, Vallance BA. The gut-skin axis: a bi-directional, microbiota-driven relationship with therapeutic potential. Gut Microbes. 2025;17(1):2473524. doi:10.1080/19490976.2025.2473524
45. Zhao M, Shen C, Ma L. Treatment efficacy of probiotics on atopic dermatitis, zooming in on infants: a systematic review and meta-analysis. Int J Dermatol. 2018;57(6):635–641. doi:10.1111/ijd.13873
46. Fang ZF, Li LZ, Liu XY, et al. Strain-specific ameliorating effect of Bifidobacterium longum on atopic dermatis in mice. Funct Foods. 2019;60:103426. doi:10.1016/j.jff.2019.103426
47. Boggio Marzet C, Burgos F, Del Compare M, Gerold I, Tabacco O, Vinderola G. Approach to probiotics in pediatrics: the role of Lactobacillus rhamnosus GG. Arch Argent Pediatr. 2022;120(1):e1–e7. doi:10.5546/aap.2022.eng.e1
48. Ahn JR, Lee SH, Kim B, et al. Ruminococcus gnavus ameliorates atopic dermatitis by enhancing treg cell and metabolites in BALB/c mice. Pediatr Allergy Immunol. 2022;33(1):e13678. doi:10.1111/pai.13678
49. Rios-Carlos M, Cervantes-García D, Córdova-Dávalos LE, Bermúdez-Humarán LG, Salinas E. Unraveling the gut-skin axis in atopic dermatitis: exploiting insights for therapeutic strategies. Gut Microbes. 2024;16(1):2430420. doi:10.1080/19490976.2024.2430420
50. Zhang K, Kim SM, Kwon HK, et al. Peripherally induced RORγt+ skin-resident regulatory T cells mediate the efficacy of allergen-specific immunotherapy. Sci Transl Med. 2025;17(800):eado1375. doi:10.1126/scitranslmed.ado1375
51. Di Meglio P, Duarte JH, Ahlfors H, et al. Activation of the aryl hydrocarbon receptor dampens the severity of inflammatory skin conditions. Immunity. 2014;40(6):989–1001. doi:10.1016/j.immuni.2014.04.019
52. Tsuji G, Hashimoto-Hachiya A, Kiyomatsu-Oda M, et al. Aryl hydrocarbon receptor activation restores filaggrin expression via OVOL1 in atopic dermatitis. Cell Death Dis. 2017;8(7):e2931. doi:10.1038/cddis.2017.322
53. Choi H, Kwak MJ, Choi Y, et al. Extracellular vesicles of Limosilactobacillus fermentum SLAM216 ameliorate skin symptoms of atopic dermatitis by regulating gut microbiome on serotonin metabolism. Gut Microbes. 2025;17(1):2474256. doi:10.1080/19490976.2025.2474256
54. Yu L, Peng S, Chen X, et al. Intestinal dysbiosis exacerbates skin inflammation via microbial metabolite-driven Th2 cell differentiation. Immunity. 2026;S1074-7613(26):00130. doi:10.1016/j.immuni.2026.03.019
55. Zhang W, Lei J, Jiang P, et al. Double-layered microneedle patch integrated with multifunctional nanoparticles and live bacteria for long-term treatment of atopic dermatitis. Small. 2025;21(3):e2409121. doi:10.1002/smll.202409121
56. Long M, Li J, Zhu Y, et al. Microneedle-facilitated Portulaca oleracea L.-derived nanovesicles ameliorate atopic dermatitis by modulating macrophage M1/M2 polarization and inhibiting NF-κB and STING signaling pathways. Acta Pharm Sin B. 2025;15(11):5966–5987. doi:10.1016/j.apsb.2025.08.021
57. Liu T, Chen G, Zhao C, et al. Hyaluronic acid-butyrate conjugates for barrier restoration in atopic dermatitis: CD44-mediated retention and inflammation-responsive release. Carbohydr Polym. 2026;375:124786. doi:10.1016/j.carbpol.2025.124786
58. Song R, Zhu Y, Xue K, et al. A “controlled assembly” strategy for constructing Coptidis Rhizoma self-assembled nanoparticles to ameliorate inflammatory damage in Atopic dermatitis. Bioact Mater. 2025;56:234–247. doi:10.1016/j.bioactmat.2025.10.010
59. Su S, Wang Y, Xiang Y, et al. A smart hydrogel dressing balances reactive oxygen species levels for effective treatment of bacteria-infected atopic dermatitis. Adv Healthc Mater. 2025;14(20):e2501142. doi:10.1002/adhm.202501142
60. Peng G, Tsukamoto S, Ikutama R, et al. Human β-defensin-3 attenuates atopic dermatitis-like inflammation through autophagy activation and the aryl hydrocarbon receptor signaling pathway. J Clin Invest. 2022;132(17):e156501. doi:10.1172/JCI156501
61. Xu F, Qiu Z, Zhang M, et al. Transdermal drug delivery systems: a comprehensive review of mechanisms, technologies, and clinical applications. Pharm Res. 2025;42(12):2429–2442. doi:10.1007/s11095-025-03962-9
62. Yan Z, Zhang S, Wu G, et al. Advances in nanotechnology-based topical delivery systems for skincare applications. Pharmaceutics. 2026;18(1):63. doi:10.3390/pharmaceutics18010063
63. Seo SG, Kwon TG, Ha JW, Oh J, Kim MJ, In S. Recovery effects of various skin lipid components and their structural derivatives on skin barrier damage. Int J Cosmet Sci. 2026;48(1):110–120. doi:10.1111/ics.70023
64. Ruan J, Liu C, Wang J, Zhong T, Quan P, Fang L. Efficacy and safety of permeation enhancers: a kinetic evaluation approach and molecular mechanism study in the skin. Int J Pharm. 2022;626:122155. doi:10.1016/j.ijpharm.2022.122155
65. Wu Q, Liu S, Li Z, et al. FGF-21 fusion proteins ameliorate atopic dermatitis by inhibiting the TLR/TSLP signaling pathway: anti-inflammatory and skin barrier repair effects. Int Immunopharmacol. 2025;159:114920. doi:10.1016/j.intimp.2025.114920
66. Liu T, Chen L, Zhao X, et al. An AI-assisted designed supramolecularly engineered nanoplatform reverses pigmentation by triggering an ineffective compensatory melanin production program. Bioact Mater. 2026;60:243–260. doi:10.1016/j.bioactmat.2026.01.027
67. Hülpüsch C, Tremmel K, Hammel G, et al. Skin pH-dependent Staphylococcus aureus abundance as predictor for increasing atopic dermatitis severity. Allergy. 2020;75(11):2888–2898. doi:10.1111/all.14461
68. Slavkova M, Lazov C, Spassova I, et al. Formulation of budesonide-loaded polymeric nanoparticles into hydrogels for local therapy of atopic dermatitis. Gels. 2024;10(1):79. doi:10.3390/gels10010079
69. Raimondo A, Serio B, Lembo S. Oxidative stress in atopic dermatitis and possible biomarkers: present and future. Indian J Dermatol. 2023;68(6):657–660. doi:10.4103/ijd.ijd_878_22
70. Wen HT, Du YN, Wang WQ, et al. CD44/TRPV1 dual-targeted nanocarrier enables drug retention and multidimensional therapy for inflammatory skin diseases. Innov Mater. 2026;540:177278. doi:10.1016/j.cej.2026.177278
71. Chandimali N, Hong SM, Bae J, et al. Harnessing antioxidant properties of plant-derived bioactive compounds to alleviate atopic dermatitis symptoms: a review. Curr Pharm Des. 2026;32(13):1013–1026. doi:10.2174/0113816128368673250611114044
72. Yang L, Xia JN. Beyond the skin: exploring the gut-skin axis and metabolic pathways in atopic dermatitis pathogenesis. Int J Gen Med. 2025;18:6123–6136. doi:10.2147/IJGM.S550152
73. Ha YJ, Tak KH, Lee JL, et al. Polynucleotides enhance skin barrier function and reduce inflammation in a 2,4-dinitrochlorobenzene-induced mouse model of atopic dermatitis. Skin Res Technol. 2025;31(6):e70189. doi:10.1111/srt.70189
74. Pareek A, Kumari L, McMahon LR, Chuturgoon A, Pareek A. Cannabinoids for dermatological applications: mechanistic insights, clinical evidence, and emerging nanotechnology-enabled delivery strategies. Pharmaceutics. 2026;18(4):469. doi:10.3390/pharmaceutics18040469
75. Meysami M, Hashempur MH, Kamalinejad M, Emtiazy M. Efficacy of short term topical Malva Sylvestris L. cream in pediatric patients with atopic dermatitis: a randomized double-blind placebo-controlled clinical trial. Endocr Metab Immune Disord Drug Targets. 2021;21(9):1673–1678. doi:10.2174/1871530320666201023125411
76. Sharma T, Singh J, Sharma V, et al. Curcumin-loaded nanocarriers for dermatological applications: current advances and biomedical implications. EXCLI J. 2026;25:654–689. doi:10.17179/excli2026-9317
77. Li M, Xu Y, Yu Y, et al. Transdermal delivery of natural products against atopic dermatitis. Chin J Nat Med. 2024;22(12):1076–1088. doi:10.1016/S1875-5364(24)60681-3
78. Kaushal P, Awasthi R. Berberine hydrochloride-caffeic acid loaded polymeric nanoparticle based hydrogel formulation for topical management of skin inflammation and atopic dermatitis: in vivo studies. J Drug Deliv Sci Tec. 2026;123:108516. doi:10.1016/j.jddst.2026.108516
79. Zhou Y, Wu L, Zhang Y, et al. Topical delivery of ceramide by oil-in-water nanoemulsion to retain epidermal moisture content in dermatitis. Biomolecules. 2025;15(5):608. doi:10.3390/biom15050608
80. Almeida C, Roque R, Vieira J, et al. Lipid extract from Black Soldier Fly larvae: a high value excipient for solid lipid nanoparticles tailored to tackle atopic dermatitis. Int J Pharm. 2024;667(Pt B):124929. doi:10.1016/j.ijpharm.2024.124929
81. Wang X, Mao D, Jia J, Zhang J. Benvitimod inhibits IL-4- and IL-13-induced tight junction impairment by activating AHR/ARNT pathway and inhibiting STAT6 phosphorylation in human keratinocytes. J Invest Dermatol. 2024;144(3):509–519.e7. doi:10.1016/j.jid.2023.07.027
82. Lu W, Cao J, Lv Y, Li M, Tang Y, Feng Y. Progress and prospects of transdermal treatment of allergic skin diseases with natural drugs based on nanotechnology. AAPS Pharm Sci Tech. 2025;27(1):21. doi:10.1208/s12249-025-03244-y
83. Kim Y, Park K, Kim MS. Recent advances in polymer-based drug delivery systems for atopic dermatitis: enhancing therapeutic efficacy and outcomes. Mater Today Bio. 2025;35:102517. doi:10.1016/j.mtbio.2025.102517
84. Sivamaruthi BS, Suganthy N, Chaiyasut C, Khongtan S, Fukngoen P, Kesika P. Curcumin for the management of skin diseases: a review of the results of preclinical and clinical trials and nanoformulations. Curr Pharm Des. 2026. doi:10.2174/0113816128452868260112115950
85. Lee JS, Oh E, Oh H, et al. Tacrolimus-loaded chitosan-based nanoparticles as an efficient topical therapeutic for the effective treatment of atopic dermatitis symptoms. Int J Biol Macromol. 2024;273(Pt 1):133005. doi:10.1016/j.ijbiomac.2024.133005
86. Zhang Y, Tang X, Ma Y, et al. Microneedle-delivered ROS-adaptive asiatic acid nanoparticles promote scarless repair via remodeling the pathological microenvironment. J Nanobiotechnology. 2026;24(1):171. doi:10.1186/s12951-025-03946-2
87. Park G, Na W, Lim JW, et al. Self-assembled nanostructures presenting repetitive arrays of subunit antigens for enhanced immune response. ACS Nano. 2024;18(6):4847–4861. doi:10.1021/acsnano.3c09672
88. Chen W, Raza F, Li K, et al. Traditional Chinese medicine-based self-assembled nanomaterials for cancer therapy. J Control Release. 2026;393:114826. doi:10.1016/j.jconrel.2026.114826
89. Lee WH, Kim W. Self-assembled hyaluronic acid nanoparticles for the topical treatment of inflammatory skin diseases: beyond drug carriers. J Control Release. 2024;366:114–127. doi:10.1016/j.jconrel.2023.12.026
90. Li D, Han Y, Zhou J, et al. Flavonoids in atopic dermatitis: mechanisms, delivery innovations, and translational strategies. Front Pharmacol. 2025;16:1631977. doi:10.3389/fphar.2025.1631977
91. Zhang D, Wei Y, Zhu X, et al. Study on the intervention mechanism of Ganodermalucidum polysaccharides in mice with atopic dermatitis. Food Res Int. 2025;221(Pt 1):117212. doi:10.1016/j.foodres.2025.117212
92. Burshtein J, Wei J, Majewska L, Schlesinger T. Plant-derived extracellular vesicles in dermatology: a review of emerging therapeutic applications. J Clin Aesthet Dermatol. 2026;19(2):15–21.
93. Shen H, Lu Q, Huang Y, et al. Plant-derived extracellular-vesicle-like particles: immune regulation and disease therapy. Research. 2026;9:1264. doi:10.34133/research.1264
94. Zhao B, Jiang X, Li W, et al. ROS-scavenging microneedles loaded with Portulaca oleracea L.-derived exosomes for atopic dermatitis therapy. Nano Res. 2025;18(12):94908151. doi:10.26599/NR.2025.94908151
95. Liu W, Yin X, Zhang Z, et al. Plant-derived exosome-like nanoparticles: mechanisms of cross-kingdom regulation and perspectives as natural drug carriers for disease treatment. Int J Nanomed. 2026;21:581774. doi:10.2147/IJN.S581774
96. van Hout NE, Nevot G, Jansen PAM, et al. From prebiotics to engineered microbes: microbe-inspired treatments for atopic dermatitis. Br J Dermatol. 2026;194(3):420. doi:10.1093/bjd/ljaf451
97. Gao JL, Hata TR. Microbiome as a potential target for treatment and prevention of atopic dermatitis. Immunol Allergy Clin North Am. 2025;45(4):501–513. doi:10.1016/j.iac.2025.06.003
98. Das M, Alasharee M, Woods B, et al. S. aureus exposure during cutaneous antigen sensitization causes basophil- and interleukin-4-dependent exaggerated food anaphylaxis. Immunity. 2025;58(11):2769–2784.e6. doi:10.1016/j.immuni.2025.09.001
99. Osei-Karikari K, Jones K, Erickson A, Myles IA. Emerging microbiome-based therapies for atopic dermatitis: clinical insights and future development. Expert Opin Emerg Drugs. 2026;1–12. doi:10.1080/14728214.2026.2667256
100. Jin R, Wang M, Ke J, Gao X, Zhang L. Correlation between Staphylococcus aureus colonization and disease severity in atopic dermatitis: a systematic review and meta-analysis of randomized controlled trials. Front Immunol. 2026;17:1820411. doi:10.3389/fimmu.2026.1820411
101. Hendricks AJ, Mills BW, Shi VY. Skin bacterial transplant in atopic dermatitis: knowns, unknowns and emerging trends. J Dermatol Sci. 2019;95(2):56–61. doi:10.1016/j.jdermsci.2019.07.001
102. Zhou H, Zhang S, Liu X, Feng A, Chen S, Liu W. Microneedle delivery platform integrated with Staphylococcus epidermidis-derived extracellular vesicles-based nanoantibiotics for efficient bacterial infection atopic dermatitis treatment. Acta Pharm Sin B. 2025;15(4):2197–2216. doi:10.1016/j.apsb.2025.02.038
103. Jin Y, Zhang C, Jia M, Chen M. Enhanced dermal delivery of nanoparticulate formulation of Cutibacterium acnes using sponge spicules for atopic dermatitis treatment. Int J Nanomed. 2025;20:3235–3249. doi:10.2147/IJN.S509798
104. Morakabi SF, Shahraky MK, Ahmadian G, Asl RM. Postbiotic_loaded hyalurosome: investigating their potential as antimicrobial and antioxidant agents. J Cosmet Dermatol. 2026;25(4):e70777. doi:10.1111/jocd.70777
105. Mun D, Ryu S, Choi H, Kwak MJ, Oh S, Kim Y. Bovine colostrum-derived extracellular vesicles modulate gut microbiota and alleviate atopic dermatitis via the gut-skin axis. Drug Deliv Transl Res. 2026;16(1):367–380. doi:10.1007/s13346-025-01875-z
106. Li M, Mao B, Ren B, et al. Limosilactobacillus reuteri CCFM1040 extracellular vesicles alleviate atopic dermatitis through signal transducer and activator of transcription STAT3-dependent modulation of epithelial cytokine. Int J Biol Macromol. 2025;334(Pt 2):148671. doi:10.1016/j.ijbiomac.2025.148671
107. Su D, Li M, Xie Y, et al. Gut commensal bacteria Parabacteroides goldsteinii-derived outer membrane vesicles suppress skin inflammation in psoriasis. J Control Release. 2025;377:127–145. doi:10.1016/j.jconrel.2024.11.014
108. Badale A, Zdrîncă M, Maghiar L, Magyar I, Zaha DC. Multi-kingdom synergy of Perilla frutescens-derived effector vesicles and postbiotics: a triple-action strategy for atopic dermatitis. Life. 2026;16(5):769. doi:10.3390/life16050769
109. Ben David N, Richtman Y, Gross A, et al. Design and evaluation of dissolvable microneedles for treating atopic dermatitis. Pharmaceutics. 2023;15(4):1109. doi:10.3390/pharmaceutics15041109
110. Jang M, Kang BM, Yang H, Ohn J, Kwon O, Jung H. High-dose steroid dissolving microneedle for relieving atopic dermatitis. Adv Healthc Mater. 2021;10(7):e2001691. doi:10.1002/adhm.202001691
111. Guan J, Chen K, Lu F, He Y. Dissolving microneedle patch loaded with adipokines-enriched adipose extract relieves atopic dermatitis in mouse via modulating immune disorders, microbiota imbalance, and skin barrier defects. J Tissue Eng. 2025;16:20417314241312511. doi:10.1177/20417314241312511
112. Song L, Chi J, Li Z, et al. An inflammation-responsive double-layer microneedle patch for recurrent atopic dermatitis therapy. Int J Pharm. 2023;643:123215. doi:10.1016/j.ijpharm.2023.123215
113. Chiu YH, Wu YW, Hung JI, Chen MC. Epigallocatechin gallate/L-ascorbic acid-loaded poly-γ-glutamate microneedles with antioxidant, anti-inflammatory, and immunomodulatory effects for the treatment of atopic dermatitis. Acta Biomater. 2021;130:223–233. doi:10.1016/j.actbio.2021.05.032
114. Oh SJ, Nguyen TT, Seo Y, et al. Sustained release of stem cell secretome from nano-villi chitosan microspheres for effective treatment of atopic dermatitis. Int J Biol Macromol. 2024;277(Pt 4):134344. doi:10.1016/j.ijbiomac.2024.134344
115. Deng WY, Chen DM, Wei YF, et al. Washed microbiota transplantation relieves atopic dermatitis via gut–skin microbiome rebalancing. BMC Microbiol. 2026;26:149. doi:10.1186/s12866-026-04717-1
116. Cao X, He R, Xu D, Zhao Y. Interdisciplinarity traditional Chinese medicine microneedles in skin disease treatment: recent advances and challenges. Bioact Mater. 2025;55:568–601. doi:10.1016/j.bioactmat.2025.09.040
117. Wang WJ, Shao LJ, Jiang X, et al. Therapy and mechanism of natural polysaccharides for atopic dermatitis treatment. Food Sci Hum Wellness. 2025;14(5):9250101. doi:10.26599/FSHW.2024.9250101
118. Xie LN, Yang KY, Liang YH, et al. Tremella fuciformis polysaccharides alleviate induced atopic dermatitis in mice by regulating immune response and gut microbiota. Front Pharmacol. 2022;13:944801. doi:10.3389/fphar.2022.944801
119. Chen YL, Chang CC, Lin YC, Chen MC. Double-layered PLGA/HA microneedle systems as a long-acting formulation of polyphenols for effective and long-term management of atopic dermatitis. Biomater Sci. 2023;11(14):4995–5011. doi:10.1039/d3bm00182b
120. Srinatha N, Battu S, Vishwanath BA. Microsponges: a promising frontier for prolonged release-current perspectives and patents. Beni-Suef Univ J Basic Appl Sci. 2024;13:60. doi:10.1186/s43088-024-00519-4
121. Wang Y, Wang ZQ, Liu Y, Li WX, Zhang XR. Preparation of a quercetin-loaded porous microsphere gel for the treatment of atopic dermatitis in BALB/c mice. New J Chem. 2026;50:4744–4756. doi:10.1039/D5NJ04337A
122. Fan Y, Keerthisinghe TP, Nian M, et al. Comparative secretome metabolic dysregulation by six engineered dietary nanoparticles (EDNs) on the simulated gut microbiota. J Hazard Mater. 2024;465:133003. doi:10.1016/j.jhazmat.2023.133003
123. Jia Y, Hu J, An K, et al. Hydrogel dressing integrating FAK inhibition and ROS scavenging for mechano-chemical treatment of atopic dermatitis. Nat Commun. 2023;14(1):2478. doi:10.1038/s41467-023-38209-x
124. Zhu WJ, Guo Y, Mao YX, Zhao JH, Ling GX, Zhang P. Engineered dual-polysaccharide hydrogel loaded with ROS-scavenging nanozymes for atopic dermatitis therapy. Chem Eng J. 2026;534:175306. doi:10.1016/j.cej.2026.175306
125. Wang S, Wang R. Supramolecular self-assembly of natural herb extracts: from molecular interactions to functional biomaterials. Innovation Materials. 2026;4(2):100206. doi:10.59717/j.xinn-mater.2026.100206
126. Shi W, Zhang D, Han L, et al. Supramolecular chitin-based hydrogels with self-adapting and fast-degradation properties for enhancing wound healing. Carbohydr Polym. 2024;323:121374. doi:10.1016/j.carbpol.2023.121374
127. Zhu H, Liu M, Wang Z, et al. Self-assembly of plant-derived bioactive nanostructures in traditional Chinese medicine. iScience. 2026;29(2):114667. doi:10.1016/j.isci.2026.114667
128. Wu Y, Liu X, Su H, et al. Colloidal self-assembly of astilbin with smilax glabra polysaccharides enables carrier-free delivery and improved anti-inflammatory performance. Colloids Surf B Biointerfaces. 2026;259:115286. doi:10.1016/j.colsurfb.2025.115286
129. Han X, Bai B, Zhou Q, et al. Dietary supplementation with polysaccharides from Ziziphus Jujuba cv. Pozao intervenes in immune response via regulating peripheral immunity and intestinal barrier function in cyclophosphamide-induced mice. Food Funct. 2020;11(7):5992–6006. doi:10.1039/d0fo00008f
130. Dartora VFC, Passos JS, Osorio B, et al. Chitosan hydrogels with MK2 inhibitor peptide-loaded nanoparticles to treat atopic dermatitis. J Control Release. 2023;362:591–605. doi:10.1016/j.jconrel.2023.08.061
131. Yang Y, Zhou Y, Wang L, Ai C, Fu Y, Song S. Photoelectrocatalytic degradation of hyaluronic acid and regulation effects of its degradation products on gut microbiota in vitro. Int J Biol Macromol. 2024;283(Pt 2):137813. doi:10.1016/j.ijbiomac.2024.137813
132. Kougkolos G, Laudebat L, Dinculescu S, et al. Skin electroporation for transdermal drug delivery: electrical measurements, numerical model and molecule delivery. J Control Release. 2024;367:235–247. doi:10.1016/j.jconrel.2024.01.036
133. Abbasi M, Heath B. Iontophoresis and electroporation-assisted microneedles: advancements and therapeutic potentials in transdermal drug delivery. Drug Deliv Transl Res. 2025;15(6):1962–1984. doi:10.1007/s13346-024-01722-7
134. Piscazzi F, D’Oria F, Ramirez MA, Ardigò M. Iontophoresis-based topical drug delivery for dermatologic conditions: a systematic review. Pharmaceuticals. 2026;19(5):765. doi:10.3390/ph19050765
135. Bakhrushina EO, Shumkova MM, Avdonina YV, et al. Transdermal drug delivery systems: methods for enhancing skin permeability and their evaluation. Pharmaceutics. 2025;17(7):936. doi:10.3390/pharmaceutics17070936
136. Liu S, Deng T, Cheng H, Lu J, Wu J. Advances in transdermal drug delivery systems and clinical applications in inflammatory skin diseases. Pharmaceutics. 2025;17(6):746. doi:10.3390/pharmaceutics17060746
137. Kushwaha R, Palei NN. Transdermal drug delivery systems: different generations and dermatokinetic assessment of drug concentration in skin. Pharmaceut Med. 2024;38(6):407–427. doi:10.1007/s40290-024-00537-8
138. Gaikwad SS, Zanje AL, Somwanshi JD. Advancements in transdermal drug delivery: a comprehensive review of physical penetration enhancement techniques. Int J Pharm. 2024;652:123856. doi:10.1016/j.ijpharm.2024.123856
139. Marathe D, Bhuvanashree VS, Mehta CH, A T, Nayak UY. Low-frequency sonophoresis: a promising strategy for enhanced transdermal delivery. Adv Pharmacol Pharm Sci. 2024;2024:1247450. doi:10.1155/2024/1247450
140. Vita ED, Presti DL, Massaroni C, et al. A review on radiofrequency, laser, and microwave ablations and their thermal monitoring through fiber Bragg gratings. iScience. 2023;26(17):108260. doi:10.1016/j.isci.2023.108260
141. Zhao Y, Voyer J, Li Y, Kang X, Chen X. Laser microporation facilitates topical drug delivery: a comprehensive review about preclinical development and clinical application. Expert Opin Drug Deliv. 2023;20(1):31–54. doi:10.1080/17425247.2023.2152002
142. Tao W, Lai Y, Zhou X, Yang G, Wu P, Yuan L. A narrative review: ultrasound-assisted drug delivery: improving treatments via multiple mechanisms. Ultrasonics. 2025;151:107611. doi:10.1016/j.ultras.2025.107611
143. Fang JY, Hwang TL, Huang YB, Tsai YH. Transdermal iontophoresis of sodium nonivamide acetate. V. Combined effect of physical enhancement methods. Int J Pharm. 2002;235(1–2):95–105. doi:10.1016/s0378-5173(01)00972-3
144. Gao J, Chen F, Wang C, et al. Paper battery powered iontophoresis microneedles patch for hypertrophic scar treatment. Microsyst Nanoeng. 2025;11(1):46. doi:10.1038/s41378-024-00823-0
145. Wang G, Moriyama N, Tottori S, Nishizawa M. Recent advances in iontophoresis-assisted microneedle devices for transdermal biosensing and drug delivery. Mater Today Bio. 2025;31:101504. doi:10.1016/j.mtbio.2025.101504
146. Chen S, Liao T, Zhao S, et al. High strength “breathable” glycosilicone/Aloe vera polysaccharide-based gel dressing for efficient wound repair. Int J Biol Macromol. 2024;281(Pt 4):136293. doi:10.1016/j.ijbiomac.2024.136293
147. Jin Y, Liu S, Wang X, Wang C, Ruan Q, Li W. Multifunctional microneedle patches loaded with engineered nitric oxide-releasing nanocarriers for targeted and synergistic chronic wound therapy. Adv Mater. 2025;37(5):e2413108. doi:10.1002/adma.202413108
148. Han Y, Qin X, Lin W, et al. Microneedle-based approaches for skin disease treatment. Nano-Micro Lett. 2025;17(1):132. doi:10.1007/s40820-025-01662-y
149. Zhang T, Gao Z, Wang Y. Tanshinone in acne therapeutics: integrating molecular mechanisms, drug development, and multimodal treatment strategies. Fitoterapia. 2025;186:106822. doi:10.1016/j.fitote.2025.106822
150. Jacob S, Nair AB, Patel V, Shah J. 3D printing technologies: recent development and emerging applications in various drug delivery systems. AAPS Pharm Sci Tech. 2020;21(6):220. doi:10.1208/s12249-020-01771-4
151. Tan Y, Sun H, Lan Y, et al. Study on 3D printed MXene-berberine-integrated scaffold for photo-activated antibacterial activity and bone regeneration. J Mater Chem B. 2024;12(8):2158–2179. doi:10.1039/d3tb02306k
152. Zhang Y, Wang S, Yang Y, et al. Scarless wound healing programmed by core-shell microneedles. Nat Commun. 2023;14(1):3431. doi:10.1038/s41467-023-39129-6
153. Ma N, Fang J, He L, et al. Fabrication of bio-based nanomicrospheres with a 3D porous structure for efficient matrine adsorption using cellulose-functionalized dendritic mesoporous organosilica nanoparticles. Int J Biol Macromol. 2025;309(Pt 2):142924. doi:10.1016/j.ijbiomac.2025.142924
154. He X, Zhao W, Xu H, et al. Smart core-shell microneedles for psoriasis therapy: in situ self-assembly of calcium ion-coordinated dexamethasone hydrogel. J Control Release. 2025;379:786–796. doi:10.1016/j.jconrel.2025.01.037
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.