Back to Journals » Medical Devices: Evidence and Research » Volume 18
Energy Output Variability Among Phacoemulsification Tips Using Calorimetry
Authors Cardenas IA ![]() , Ricks RG
, Ricks RG ![]() , Jensen JL
, Jensen JL ![]() , Nelson TK
, Nelson TK ![]() , Barlow Jnr WR
, Barlow Jnr WR ![]() , Olson RJ
, Olson RJ ![]() , Pettey JH
, Pettey JH ![]()
Received 7 May 2025
Accepted for publication 24 September 2025
Published 3 October 2025 Volume 2025:18 Pages 485—493
DOI https://doi.org/10.2147/MDER.S538849
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ivan A Cardenas,1,2 Reiker G Ricks,1,2 Jenna L Jensen,1,2 Tanner K Nelson,1,2 William R Barlow Jnr,1 Randall J Olson,1 Jeff H Pettey1
1Department of Ophthalmology and Visual Sciences, John a Moran Eye Center, University of Utah, Salt Lake City, UT, USA; 2University of Utah School of Medicine, Salt Lake City, UT, USA
Correspondence: Jeff H Pettey, John a Moran Eye Center, University of Utah, 65 Mario Capecchi Drive, Salt Lake City, UT, 84132, USA, Tel +18015812352, Fax +18015813357, Email [email protected]
Purpose: To determine if using different phacoemulsification (phaco) tips will impact thermal energy output utilizing calorimetry.
Methods: The Alcon Centurion was used with the Infiniti OZil handpiece and balanced, hybrid, or MST Dewey A1 mini tip. Settings were 100% power, continuous torsional or longitudinal ultrasound, 0mmHg vacuum limit, and flow rate 12mL/min. Outflow tubing was removed from the handpiece and inflow tubing was manually occluded. The handpiece tip was placed into the calorimeter filled with 50mL of degassed deionized water and ultrasound was initiated for 1 minute. Temperature rise and cumulative dissipated energy (CDE) were recorded; ten trials were performed for each group.
Results: Statistically significant differences in energy output, measured in Joules, were found between all three tips in both ultrasound modes. Balanced tips showed the highest output, Dewey tips had the lowest. Hybrid tips had significantly increased output in longitudinal mode, whereas Dewey tips had significantly decreased output in longitudinal mode. No significant differences were seen in CDE between tips in either ultrasound mode, but significant increases were seen in longitudinal mode within each tip.
Conclusion: This study demonstrated differences in thermal energy production of three different phaco handpiece tips. This provides insight into how thermal injuries occur and what might cause these differences. Our methodology provides a novel way for accurate energy measurement at the tip, though it differs when compared to external energy production measurements. Surgeons should take into consideration the significant variability in thermal energy created by handpiece tips.
Plain Language Summary: Modern cataract surgery employs phacoemulsification, a technique that breaks apart a cataract using ultrasonic energy. A rare but possible complication of this technology is thermal (heat) injury. Several factors contribute to energy generation during cataract fragmentation, such as friction at the incision site and impedance of flow rate. This study examines the thermal energy produced at the handpiece tip, where ultrasonic movement occurs. The energy delivered to the eye from the handpiece consists of mechanical energy in the form of kinetic and acoustic energy, leading to cavitation, mechanical disruption of the lens, and heat. It remains unclear how the design of phacoemulsification tips influences the energy transfer from piezoelectric crystals to the mechanical energy delivered to the eye. We used calorimetry to measure the thermal energy output, measured in Joules, between three different tips in longitudinal (forward and backward) and torsional (side to side) ultrasound modes, using the same settings, handpiece, and machine. The handpiece tip was submerged in the calorimetry chamber with water and operated for 60 seconds; a temperature probe measured the temperature change. The temperature changes were converted to energy and compared, and the energy measurement generated by the machine was recorded. We found significant differences in energy output between the three tips in both ultrasound modes, the Dewey tip demonstrated the lowest energy output and the balanced tip had the highest, in torsional and longitudinal mode. We found the measured energy differed significantly from the machine-generated measurement. These findings highlight the variability in energy output and expand on the potential contributing factors to energy generation and thermal injury in cataract surgery.
Keywords: cataract surgery, output, thermal injury, ultrasound mode, variability
Introduction
Cataract surgery has greatly improved in efficiency and overall safety since it began in 1967. In a field marked by a relentless focus on advancement and innovation, phacoemulsification (phaco) fits well within this context. To study the effects of phaco and ensure its optimization, it is essential to thoroughly understand its individual components, providing patients with the best and safest outcomes while equipping surgeons with the most efficient tools. Desired advances in the field aim to reduce complications such as endophthalmitis, posterior capsular rupture, and corneal incision contracture (CIC) injury.1,2
CIC is the result of thermal damage at the wound site during cataract surgery. Research has shown an overall low rate of thermal wound injury;3,4 however, when it does occur, it can result in endothelial cell damage, fistula formation, and high magnitude post-operative astigmatism. Manufacturer recommendations advise clearing of viscoelastic material, adequate flow rate, and ensuring an appropriate working space.5 The primary factor contributing to this complication is the energy generated at the phaco handpiece tip. The key elements that may cause increased energy generation leading to thermal injury include ultrasonic energy, friction between the tip and sleeve, cavitation, heat produced by the piezoelectric crystals, viscoelasticity, and occlusion events.6 These elements are influenced by the amount of ultrasonic power used, type of ultrasound (US), fluid flow rate, and physical materials such as fluid type, the phaco handpiece, sleeve, and tip. When studying these individual components, attention must turn to the variables directly impacting heat generation, in this case, to the tip of the handpiece and the method of US energy delivery.
A wide variety of handpiece tips are available, differing in the shape of the tip, the angle of the bevel, and, in some cases, the material used to make the tip. The material for tip manufacturing is primarily composed of titanium alloy,7,8 which has a low thermal conductivity ranging from 6 to 20 watts per meter kelvin (W/mK) depending on the alloy grade. This indicates an improvement in the ability to prevent energy transfer when compared to other metals such as copper or aluminum,9 which have thermal conductivities of 401 W/mK and 237 W/mK, respectively. The tip itself relies on US motion to generate energy. Most machines employ a longitudinal, or forward-and-backward motion, while other machines utilize a torsional, or a horizontal side-to-side motion. The differences between these two modes have been evaluated, with the horizontal torsional mode demonstrating overall superiority in efficiency and safety. However, the energy output differences between the two modes remain unclear.10,11
Historically, the phaco machine itself reported a measure of this ultrasound energy. The commonly cited measurement for this machine is cumulative dissipated energy (CDE); however, this metric is specific to one manufacturer, and some machines lack an energy measurement entirely.12–14 Currently, there are significant differences in energy output between machines, handpieces, or among tips in various cases. There is variability in the findings; for example, recent studies have indicated a significant difference in efficiency between a typical steel tip and a hybrid polymer tip.15,16 It remains unknown whether differences in these tips might affect energy output during procedures.
Prior studies of energy output have employed temperature probes, infrared/thermal cameras, and blackbody film, and have been conducted in laboratory, porcine, and human eyes.6,17–20 To measure the variability in output through a standardized method applicable across machines and materials, calorimetry has been used as an objective means of quantifying ultrasonic energy.21–25 This novel approach has been applied to phaco, highlighting differences in CDE relative to measured energy, and facilitates accurate and replicable assessments of temperature changes among the three tips. The goal of the present study is to identify the differences in energy output among three distinct phaco tips as measured by calorimetry, thus further clarifying which tips may have an increased potential for US-induced tissue damage or direct thermal injury.
Methods
This study did not involve human subjects or animals, so Institutional Review Board approval was not required.
Phacoemulsification
All trials were conducted on the Alcon Centurion machine, utilizing the Infiniti OZil handpiece (Alcon Inc., Fort Worth, Texas, US). The settings included 100% continuous power, 0 mmHg vacuum limit, and a minimum aspiration rate of 12 mL/min; these settings were employed in both torsional and longitudinal US modes. The inflow tubing of the handpiece was manually occluded with a hemostat, and the outflow tubing was removed to prevent fluid replacement during the trials. This manual occlusion eliminated the minimum required aspiration of 12 mL/min.
Calorimetry
A double-walled aluminum calorimeter was used for all trials (Figure 1). The inner chamber was filled with 50 mL of degassed, deionized water, which was replaced and weighed for each trial. The phaco handpiece was inserted through a central hole in the lid of the calorimeter. Additionally, the lid featured two holes to accommodate the temperature probe and stirring rod.
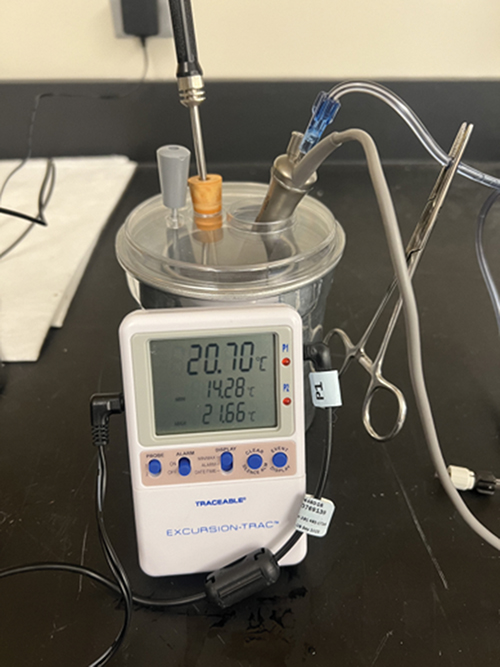 |
Figure 1 Experimental setup showing calorimeter, temperature probe, handpiece with hemostat, and stirring rod. |
Tips
Three tips were compared (Figure 2). Tip 1, the metal Dewey tip (MicroSurgical Technology [MST], Redmond, Washington, US), featured a 0.9mm opening, a 12-degree bend, and a 30-degree bevel. Tip 2, the metal balanced tip (Alcon), had a 0.9mm opening and a 30-degree bevel, but no bend. Tip 3, the hybrid polymer-coated tip (Alcon), featured a 0.9mm semicircular bend and a 30-degree bevel. Each tip was equipped with the manufacturer’s recommended sleeve and included an aspiration bypass system (ABS) hole; however, since there was no flow, this did not impact the measurements.
 |
Figure 2 Image showing the three tips utilized in the experiment. Images are labeled as follows: Dewey tip (1), hybrid tip (2), balanced tip (3). |
Trials
The trials were conducted with the tip of the handpiece fully submerged in the measured and replaced water, with the stirring rod and temperature probe positioned around the tip. Ultrasound was activated by pressing the foot pedal to position 3 for 60 seconds, timed by an observer. After each trial, the handpiece was cooled in a separate container of water. Investigators recorded temperature changes in degrees Celsius and machine-measured CDE for each trial. The handpiece tip was tightened every five trials to ensure consistency throughout the evaluations and reduce the likelihood of the tip loosening due to extensive use. A total of ten trials were performed in each ultrasound mode for each handpiece.
Statistical Analysis
Microsoft Excel (version 16.60) was used for data tracking, compilation, and statistical analysis. Results were analyzed by first converting the change in temperature to energy, as measured in Joules, by utilizing the equation q = mcΔT where c is the specific heat of water (4.184), m is the mass of water as measured for each individual trial, and ΔT is the temperature change in degrees Celsius. The energy changes, as well as the CDE changes, from the three tips were compared within and between each US mode with a one-way ANOVA and Student’s T-test. A P < 0.05 indicated statistical significance.
Results
Table 1 presents raw data illustrating overall changes in temperature, energy, and CDE for each tip. In torsional US mode, there was a statistically significant difference in energy output between the Dewey tip and hybrid tip (P < 0.05), the Dewey tip and balanced tip (P < 0.001), and between the hybrid and balanced tip (P < 0.001) (Figure 3A). In longitudinal US mode, a statistically significant difference in energy output was also observed between the dewey tip and the hybrid tip (P < 0.001), between the Dewey tip and balanced tip (P < 0.001), and between the hybrid tip and balanced tip (P < 0.001) (Figure 3B). When examining differences between US modes for the tips, the output of the MST Dewey tip was statistically significantly lower in longitudinal mode compared to torsional mode (P < 0.05) (Figure 4A). A statistically significant increase in output for the hybrid tip was noted in longitudinal mode compared to torsional mode (P < 0.01) (Figure 4B). No statistically significant difference in output of the balanced tip between US modes was observed (P = 0.2). In terms of machine-reported CDE, there was a statistically significant increase in CDE in longitudinal US mode compared to torsional mode across all tips (P < 0.001) (Figure 5A and B). There was no statistically significant difference in CDE between tips within the individual US modes.
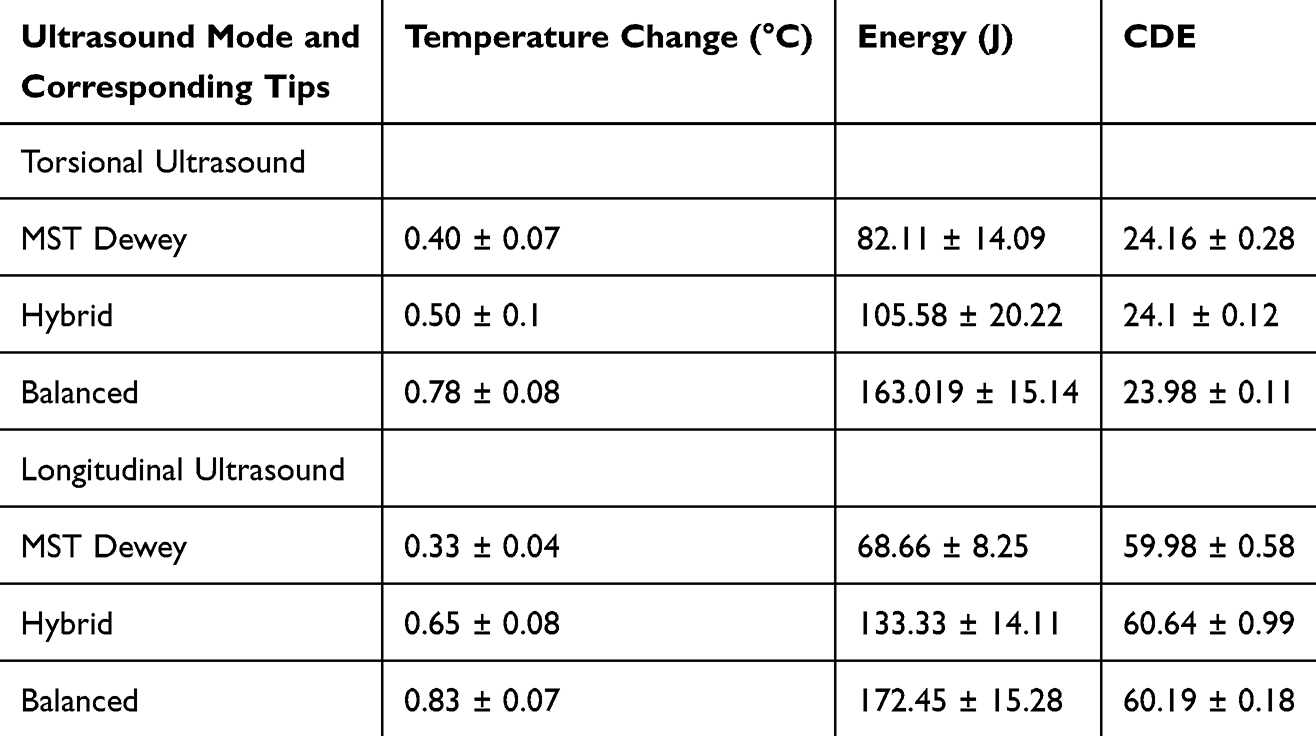 |
Table 1 Raw Data of the Three Tips Grouped within Torsional or Longitudinal Ultrasound Mode, Showing the Mean Change and Standard Deviations of Temperature in Celsius, Energy in Joules, and Cumulative Dissipated Energy (CDE) |
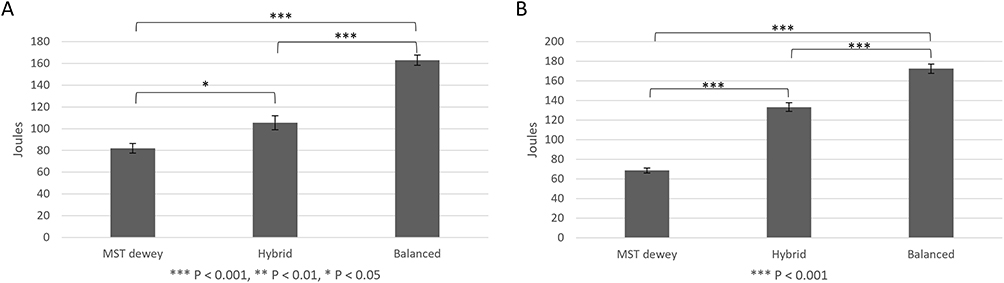 |
Figure 3 Figures demonstrating the amount of energy output in Joules between the three tips in torsional ultrasound mode (A) and longitudinal ultrasound mode (B). |
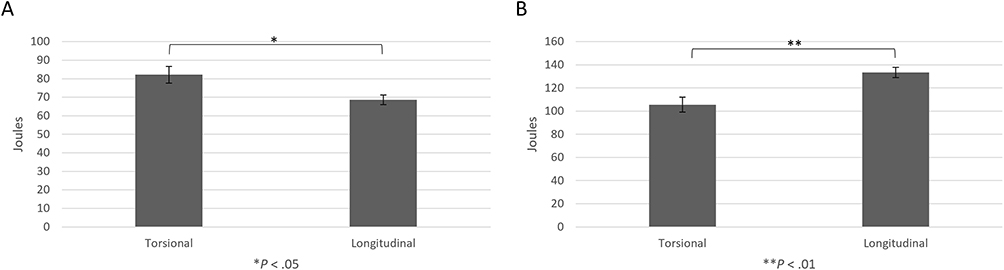 |
Figure 4 Figures demonstrating amount of energy output in Joules between torsional and longitudinal ultrasound mode for the Dewey tip (A) and hybrid tip (B). |
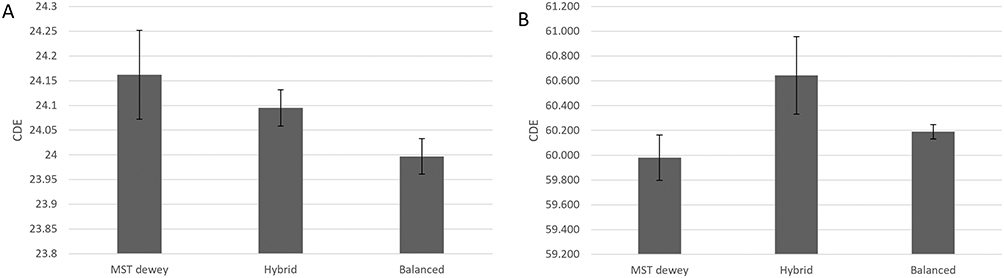 |
Figure 5 Figures demonstrating amount of CDE measured between the three tips in torsional ultrasound mode (A) and longitudinal ultrasound mode (B). |
Discussion
This study highlights the variability in energy output among various handpiece tips through the use of calorimetry, a novel method. This investigation builds on existing research, both in our laboratory and by other researchers,6,17,18,20,25–28 that focuses on measuring temperature changes during phaco, ultimately aiming to enhance safety. While it is assumed that the main thermal injury that occurs in CIC is at the wound site, there are components along both the proximal and distal end of the tip that contribute to energy production which can be harmful in the eye. The results presented here add a new layer of understanding to energy output during phaco, showing subtle differences that may arise when using different phaco tips. In this case, we observed significant differences among all three tips, with the Dewey tip demonstrating the lowest energy output and the balanced tip showing the highest energy output in both US modes (Figure 3A and B).
The decreased overall energy output of the Dewey tip may be due to its 12-degree bend, which is not observed in the balanced or hybrid tips. The bevel angle, opening, and ultrasound frequency were identical for all three tips, leaving the difference in stroke length, or amplitude, as the possible distinguishing factor. A previous study assessed these differences using high-speed videography, which revealed an increased amplitude in the balanced tip compared to a straight tip in the torsional ultrasound mode.21 These differences identified by Noguchi et al were thought to result from the balanced tip having a larger fixed base attached to the handpiece than the base of the straight tip, a semicircular distal tip design believed to block energy return to the tip shaft, and an increased pliability of the distal tip, given its overall configuration. This is likely true in our study, as the increased amplitude of the balanced tip is expected to generate more energy, whereas the slight angle of the Dewey tip, without any arc, may create a smaller amplitude that results in less energy generation (Figure 2). The base of the Dewey tip appears to have its mass concentrated more at the base, rather than spread further out like the balanced tip, suggesting that having the mass of the base closer to itself could decrease its overall energy output.
The hybrid tip is designed similarly to the balanced tip, but features a polymer coating that surrounds the metal. It showed a significantly different energy output compared to the other two tips, with this output falling within a range between those of the other tips (Figure 3A and B). This finding may emphasize the influence of material composition rather than the physical design of the tip. Theoretically, the polymer coating could lead to a reduction in energy transmission, as plastics and rubbers possess exceptionally low thermal conductivity compared to metals. If the hybrid tip had been entirely composed of polymer, the result could have been much lower; however, such a design would be impractical for phaco because it would not be able to transmit enough ultrasonic energy to disintegrate cataracts. Additionally, the variable weight distribution due to the polymer in the hybrid tip, compared to the balanced tip, may affect motion and energy transfer within the system.
Within the two different US modalities, energy output differences between these tips persisted: the Dewey tip exhibited the lowest energy output, while the balanced tip showed the highest. However, this was contradicted by the measured CDE in the same trials (Figure 5A and B). CDE did not differ significantly among the tips but did vary when comparing the two US modes, specifically being higher in the longitudinal setting. The manufacturer defines the CDE calculation as: (Longitudinal time x Average longitudinal power) + (Torsional time x 0.4 x Average torsional amplitude), where 0.4 represents the approximate reduction of heat dissipated at the incision compared to conventional phaco, and this calculation accounts for the total US energy with the foot pedal at position 3.29 Given this equation, several factors may contribute to the observed discrepancies. The CDE calculation employs a correction factor of 0.4 specifically for the torsional calculations to account for the perceived benefits of torsional US. This means longitudinal calculations will always show higher values, irrespective of extrinsic variables such as tip choice. Additionally, it differentiates longitudinal calculations from torsional calculations by comparing longitudinal power to torsional amplitude. Theoretically, this should show differences between the tips in torsional mode based on the expected difference in amplitude related to tip design; however, the CDE is essentially equal for all three. This discrepancy can also be explained by the results of a previous study.23 In brief, the longitudinal tip movement generates increased friction and heat along both the distal and proximal ends, while the oscillating motion of the torsional US concentrates most of the energy at the distal end. Our methods include measuring energy along the entire tip length, demonstrating overall energy changes within the system; meanwhile, CDE appears to specifically assess changes at the wound, disregarding variations seen at the distal end including thermal energy and mechanical damage to anterior and posterior chamber structures, given the large distal end stroke length.
Taken together, these mechanisms may help explain several significant differences. There was an increase in the energy output of the Dewey tip in torsional mode compared to the energy output in longitudinal mode (Figure 4A), while the hybrid tip showed increased energy output in longitudinal mode compared to its torsional mode output (Figure 4B). It is likely that these differences are equally influenced by the tip design itself, rather than being determined solely by the directionality of the ultrasound modality. For instance, torsional mode appears to concentrate its energy at the tip, which could negate the energy produced along the shaft seen in longitudinal mode due to its jackhammer mechanism. In the case of the Dewey tip, its torsional mode trials demonstrated increased energy production. This suggests that the primary factor contributing to this finding is the tip itself, possibly due to its 12-degree bend. In contrast, the hybrid tip, with its relatively static design aside from the polymer coating, might be expected to depend more on the ultrasound mode, with the less energy-efficient longitudinal motion leading to greater energy output. By measuring the thermal energy across the entire system, rather than just at the wound site, and by recognizing the multiple contributing variables, we can attain a more nuanced and complete assessment of all the components affecting energy generation.
Regardless of the mechanisms involved in energy generation, the absolute energy delivered to the eye varies significantly among the different tips, while the cumulative dissipated energy (CDE) remains consistent across them. In one instance, an inverse trend was demonstrated, where the Dewey tip displayed a higher calorimetry reading for torsional ultrasound (Figure 4A), yet the CDE measurements were greater for its longitudinal trials (Figure 5A and B). This emphasizes the need for a more comprehensive understanding of each component involved in energy generation during phacoemulsification. Surgeons should recognize that a CDE measurement does not serve as an absolute indicator of energy delivery to the eye and surrounding tissues, potentially creating a false sense of security, as CDE does not fully correlate with the energy delivered to the system.
The study was conducted in a laboratory setting, and we recommend that future research focus on the in vivo evaluation of tip variability. For example, the heat generated by occluding inflow and outflow, along with the subsequent measurement of wound damage, has been assessed in post-mortem porcine eyes.30,31 At this time, it is also feasible to compare surgical outcomes and the rate of thermal injury by tip in phaco to gain a better overall understanding of thermal injury. While this study’s methodology of calorimetry and occlusion might not be feasible in both in vivo models and humans, differences in heat generation among tips can be measured by using non-invasive temperature probes in living models.18 The scenario evaluated in this study was designed to be static, with a protocol established to best measure energy output directly from the tip while controlling external variables. Although a time of 60 seconds for occluded phaco may not be realistic, it allows for adequate measurement of energy change. A sample size of 50 mL is not physiologic but permits proper submersion of the calorimeter and temperature probe, which is considered in the calorimetry equation. The use of calorimetry necessitates a closed system; therefore, mass cannot be exchanged, requiring the occlusion of the tubing, which simulates intra-operative occlusion, albeit for much longer periods. In a physiologic setting, other significant variables also affect energy transmission, including the use of balanced salt solution, continuous fluid replacement, ophthalmic viscosurgical devices, variability in parameters, and procedure duration. There is also incision compression at the proximal end of the tip that was not simulated in this experimental setup. In an in vivo model, it may be challenging to identify which of these variables affect energy transmission. Therefore, it is crucial to understand these components ex vivo to more accurately explain the changes observed in a living model in either an animal or human eye.
Conclusion
This study demonstrated differences in the energy production of three distinct handpiece tips during phaco. Our findings offer additional insight into how thermal injuries may occur in cataract surgery and which aspects of phaco contribute to variations in thermal energy production. The methods utilized in this study provide a way to accurately measure energy at the handpiece tip. However, these measurements differ when compared to external energy production measurements, highlighting the need for further studies on precise energy measurement. While the individual parameters used in phaco vary, surgeons should consider the significant variability in energy produced by handpiece tips.
Abbreviations
ABS, aspiration bypass system; ANOVA, analysis of variance; AUC, area under the curve; CDE, cumulative dissipated energy; LS, least squares; MST, MicroSurgical Technology; NE, not estimable; phaco, phacoemulsification; US, ultrasound; W/mK, watts per meter kelvin.
Acknowledgment
Susan Schulman assisted with editing and manuscript preparation.
Funding
This study was supported in part by a grant from Research to Prevent Blindness, Inc., New York, New York, USA. The sponsor had no involvement in any of the stages from study design to submission of the paper for publication.
Disclosure
Dr. Olson is on the Board of Directors of Perceive Bio and the Scientific Advisory Board of Perfect Lens. Dr. Pettey reports a Consulting agreement for Lensar, outside the submitted work and consulting from Alcon, during the conduct of the study. The other authors report no conflicts of interest in this work.
References
1. Stein JD. Serious adverse events after cataract surgery. Curr Opin Ophthalmol. 2012;23(3):219–225. doi:10.1097/ICU.0b013e3283524068
2. Sippel KC, Pineda R Jr. Phacoemulsification and thermal wound injury. Semin Ophthalmol. 2002;17(3–4):102–109. doi:10.1076/soph.17.3.102.14776
3. Bradley MJ, Olson RJ. A survey about phacoemulsification incision thermal contraction incidence and causal relationships. Am J Ophthalmol. 2006;141(1):222–224. doi:10.1016/j.ajo.2005.08.018
4. Sorensen T, Chan CC, Bradley M, Braga-Mele R, Olson RJ. Ultrasound-induced corneal incision contracture survey in the United States and Canada. J Cataract Refract Surg. 2012;38(2):227–233. doi:10.1016/j.jcrs.2011.08.039
5. Centurion® Vision System Operator’s Manual 8065752943. Irvine, CA, USA: Alcon Research, Ltd; 2014:24.
6. Zacharias J. Laboratory assessment of thermal characteristics of three phacoemulsification tip designs operated using torsional ultrasound. Clin Ophthalmol. 2016;10:1095–1101. doi:10.2147/OPTH.S105065
7. Cecchini P, D’Aloisio R, Antonuccio M, et al. Chemical and physical analysis of phaco handpiece tip surfaces before and after cataract surgery. J Cataract Refract Surg. 2017;43(8):1107–1114. doi:10.1016/j.jcrs.2017.05.027
8. AZO Materials. Titanium alloys - physical properties. AZONetwork; 2002. Available from: https://www.azom.com/article.aspx?ArticleID=1341.
9. Engineering ToolBox. ThermalConductivity of metals and alloys: data table & reference guide; 2005. Available from: https://www.engineeringtoolbox.com/thermal-conductivity-metals-d_858.html.
10. Rekas M, Montés-Micó R, Krix-Jachym K, Kluś A, Stankiewicz A, Ferrer-Blasco T. Comparison of torsional and longitudinal modes using phacoemulsification parameters. J Cataract Refract Surg. 2009;35(10):1719–1724. doi:10.1016/j.jcrs.2009.04.047
11. Ungricht EL, Culp C, Qu P, et al. Effect of longitudinal and torsional ultrasound on corneal endothelial cells: experimental study in rabbit eyes. J Cataract Refract Surg. 2022;48(3):349–354. doi:10.1097/j.jcrs.0000000000000737
12. Chen M, Anderson E, Hill G, Chen JJ, Patrianakos T. Comparison of cumulative dissipated energy between the infiniti and centurion phacoemulsification systems. Clin Ophthalmol. 2015;9:1367–1372. doi:10.2147/OPTH.S88225
13. Bui AD, Sun Z, Wang Y, et al. Factors impacting cumulative dissipated energy levels and postoperative visual acuity outcome in cataract surgery. BMC Ophthalmol. 2021;21(1):439. doi:10.1186/s12886-021-02205-w
14. Helvacioglu F, Yeter C, Sencan S, Tunc Z, Uyar OM. Comparison of two different ultrasound methods of phacoemulsification. Am J Ophthalmol. 2014;158(2):221–226.e1. doi:10.1016/j.ajo.2014.04.015
15. Shumway C, Ellis N, Heczko J, Jiang B, Werner L, Mamalis N. Evaluation of the capsular safety of a new hybrid phacoemulsification tip in a cadaver eye model. J Cataract Refract Surg. 2019;45(11):1660–1664. doi:10.1016/j.jcrs.2019.06.016
16. Cardenas IA, Ungricht EL, Zaugg B, Olson RJ, Pettey JH. Efficiency of a polymer-coated phacoemulsification tip in cataract surgery. J Cataract Refract Surg. 2023;49(10):1056–1060. doi:10.1097/j.jcrs.0000000000001198
17. Suzuki H, Oki K, Igarashi T, Shiwa T, Takahashi H. Temperature in the anterior chamber during phacoemulsification. J Cataract Refract Surg. 2014;40(5):805–810. doi:10.1016/j.jcrs.2013.08.063
18. Nair S, Nair RU. Wound and surface temperatures in vivo in torsional and longitudinal modalities of ultrasound in coaxial microincisional cataract surgery. Clin Ophthalmol. 2017;11:249–255. doi:10.2147/OPTH.S123222
19. Olson MD, Miller KM. In-air thermal imaging comparison of legacy advantec, millennium, and sovereign whiteStar phacoemulsification systems. J Cataract Refract Surg. 2005;31(8):1640–1647. doi:10.1016/j.jcrs.2005.01.016
20. Jun B, Berdahl JP, Kim T. Thermal study of longitudinal and torsional ultrasound phacoemulsification: tracking the temperature of the corneal surface, incision, and handpiece. J Cataract Refract Surg. 2010;36(5):832–837. doi:10.1016/j.jcrs.2009.11.015
21. Noguchi S, Nakakura S, Tokuoka N, Tabuchi H, Maeda N, Nishida K. Difference in torsional phacoemulsification oscillation between a balanced tip and a mini tip using an ultra-high-speed video camera. J Cataract Refract Surg. 2016;42(10):1511–1517. doi:10.1016/j.jcrs.2016.06.038
22. Morgado G, Miqueleti S, Costa-Felix R. Ultrasound power measurement with a water-based calorimeter. Paper presented at: XXVI Brazilian Congress on Biomedical Engineering. Armação de Buzios, Rio de Janeiro, Brazil;2018.
23. Ricks RG, Cardenas IA, Jensen JL, Nelson TK, Olson RJ, Pettey JH. Discrepancies in CDE and measured phaco tip energy: comparison of energy produced in longitudinal and torsional ultrasound using calorimetry. Med Devices. 2024;17:339–348. doi:10.2147/MDER.S484843
24. Morgado G, Miqueleti S, Costa-Felix R. Measurement of ultrasound power using a calorimeter. J Phys. 2017;26–29.
25. Nelson TK, Ricks RG, Cardenas IA, et al. Comparison of ultrasound energy delivered to the anterior segment across different phacoemulsification surgical platforms. Med Devices. 2024;17:1–7. doi:10.2147/MDER.S429206
26. Ngo WK, Lim LW, Tan CS, Heng WJ. Heat profiling of phacoemulsification tip using a thermal scanning camera. Int Ophthalmol. 2013;33(6):645–649. doi:10.1007/s10792-013-9752-4
27. Henriksen BS, Gardiner G, Garff K, et al. Thermal evaluation of two phacoemulsification systems. Can J Ophthalmol. 2016;51(1):14–18. doi:10.1016/j.jcjo.2015.10.013
28. Schmutz JS, Olson RJ. Thermal comparison of infiniti ozil and signature ellips phacoemulsification systems. Am J Ophthalmol. 2010;149(5):762–767.e1. doi:10.1016/j.ajo.2009.12.006
29. Cumulative dissipated energy (CDE). In: Centurion® Vision System Operator’s Manual 8065752943. Irvine, CA, USA: Alcon Research, Ltd.; 2014. 90.
30. Bende T, Walker R, Jean B. Thermal collateral damage in porcine corneas after photoablation with free electron laser. J Refract Surg. 1995;11(2):129–136. doi:10.3928/1081-597X-19950301-14
31. Sato T, Yasuhara T, Fukumoto M, et al. Investigation of scleral thermal injuries caused by ultrasonic pars plana phacoemulsification and aspiration using pig eyes. Int Ophthalmol. 2019;39(9):2015–2021. doi:10.1007/s10792-018-1036-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.