Back to Journals » Journal of Inflammation Research » Volume 18
Endoscopic Retroperitoneal Debridement Combined with Posterior Percutaneous Pedicle Screw Fixation for Lumbar Infectious Spondylodiscitis: A Retrospective Study and Preliminary Results
Authors Yang Y ![]() , Ruan W, Li J, Dang R, An H, Zhao W, Xu L, Tan H
, Ruan W, Li J, Dang R, An H, Zhao W, Xu L, Tan H
Received 28 October 2025
Accepted for publication 15 December 2025
Published 31 December 2025 Volume 2025:18 Pages 18331—18342
DOI https://doi.org/10.2147/JIR.S574973
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ujjwol Risal
Yongrui Yang, Wenkai Ruan, Jianlong Li, Rongpan Dang, Huigang An, Wentao Zhao, Liang Xu, Hongdong Tan
Department of Orthopedics, Shandong Public Health Clinical Center, Shandong University, Jinan, Shandong, 250013, People’s Republic of China
Correspondence: Hongdong Tan, Email [email protected]
Background: Lumbar infectious spondylodiscitis is a severe spinal condition traditionally managed with antibiotics, though some patients require surgical intervention. The heterogeneity in infection sites, causative pathogens, and clinical presentations leads to significant variability in surgical approaches, and optimal surgical strategies remain controversial. This study aims to evaluate the feasibility, safety, and preliminary efficacy of endoscopic retroperitoneal debridement combined with posterior percutaneous pedicle screw fixation for the treatment of lumbar infectious spondylodiscitis.
Methods: This retrospective study analyzed patients diagnosed with lumbar infectious spondylodiscitis and treated with endoscopic retroperitoneal debridement at our institution from June 2023 to June 2024. Baseline patient characteristics, operative time, intraoperative blood loss, postoperative lesion clearance, changes in inflammatory markers (eg, C-reactive protein[CRP] and erythrocyte sedimentation rate[ESR]), complication rates, Visual analog scale (VAS) scores for back pain, Oswestry Disability Index (ODI) scores, kyphotic angle changes at the infected level, and radiological follow-up outcomes were recorded.
Results: Of the 30 patients, 28 (28/30, 93.33%) showed improvement in clinical symptoms. During follow-up, all patients demonstrated significant improvements in VAS scores and ODI scores compared to preoperative values (p< 0.05). At the final follow-up, all patients exhibited a kyphotic angle change of less than 8°, and no spinal instability was observed. Computed tomography (CT) at the 12-month follow-up demonstrated intervertebral bone fusion in 27 cases (27/29, 93.10%). Postoperative inflammatory markers showed improved compared with preoperative levels (p< 0.001). No infection recurrence or serious surgery-related complications were observed during the postoperative follow-up period.
Conclusion: Endoscopic retroperitoneal debridement combined with posterior percutaneous pedicle screw fixation appears to be a safe and effective minimally invasive approach for treating lumbar infectious spondylodiscitis. However, long-term efficacy requires further validation through prospective studies with larger sample sizes and extended follow-up periods.
Keywords: endoscopic retroperitoneal debridement, lumbar infectious spondylodiscitis, endoscopic technology, minimally invasive surgery
Introduction
Lumbar infectious spondylodiscitis, encompassing conditions such as discitis, vertebral osteomyelitis, and spinal abscesses, pose significant challenges in clinical management due to their potential for severe morbidity and functional impairment. The primary hurdles in treating these infections include difficulties in identifying causative pathogens, inadequate infection control, and the risk of complications such as neurological deficits or spinal instability.1,2 Conservative treatment remains the preferred approach for managing lumbar infectious spondylodiscitis, typically involving prolonged antibiotic therapy and bracing. However, surgical intervention becomes essential when patients exhibit worsening infection, compromised neurological function, or spinal instability.3,4 The primary goals of surgical treatment are eradicate infection, protect neurologic function and maintain structural alignment.5 The choice of surgical approach is critical and depends on the extent of the lesion, anatomical considerations, and the need to minimize complications. Traditional posterior approaches may be limited by incomplete access to the anterior vertebral column and paraspinal tissues, potentially compromising thorough debridement. Conversely, anterior open surgery, while effective for debridement, is associated with significant drawbacks, including extensive tissue trauma, prolonged recovery, and increased risk of complications.6 Therefore, endoscopic retroperitoneal debridement has emerged as a promising alternative. This technique aims to achieve comprehensive lesion clearance and reduce perioperative complications, offering a balance between efficacy and minimized surgical morbidity. In 1991, Obenchain7 first reported the use of laparoscopic techniques for lumbar spine surgery, primarily for discectomy. In 1996, Regan et al8 expanded the application of laparoscopy to the field of lumbar infectious spondylodiscitis, performing abscess drainage and interbody fusion via a transperitoneal approach. As a department specializing in spinal infections, we have successfully performed a large number of endoscopic retroperitoneal debridements and have introduced innovative surgical techniques, including incision design and standardized lesion clearance procedures. This study aims to systematically describe the technique and evaluate the clinical efficacy of endoscopic retroperitoneal debridement combined with posterior percutaneous pedicle screw fixation for treating lumbar infectious spondylodiscitis, with the goal of providing evidence to address the therapeutic challenges associated with this condition.
Materials and Methods
This study was approved by the ethics committee of Shandong Public Health Clinical Center, Shandong University (approval number K2025137). Written informed consent was obtained from all patients.
Patient Population
Patients in this study were selected according to the following inclusion and exclusion criteria. Inclusion criteria: (1) Diagnosis of lumbar infectious spondylodiscitis confirmed by computed tomography (CT)-guided biopsy; (2) Single-segment lumbar infectious spondylodiscitis with or without psoas abscess; (3) Early-stage infection with poor response to conservative treatment; (4) Magnetic resonance imaging (MRI) showing high signal intensity in the intervertebral disc on T2-weighted images and/or varying degrees of destruction in the adjacent vertebral endplates; (5) Elevated C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR); (6) Primary lumbar infectious spondylodiscitis.
Exclusion criteria: (1) Incomplete clinical data or missing follow-up records; (2) Contraindications to surgery or refusal of surgical treatment; (3) Asymptomatic patients; (4) Complete paralysis of both lower limbs; (5) Spinal deformity or instability.
Preoperative CT-guided lesion biopsy confirmed the causative pathogens in all patients. Additionally, the following data were recorded: level and species of infection, antibiotic use, CRP and ESR levels at admission and discharge, preoperative and postoperative Visual Analog Scale (VAS) scores for back pain, Oswestry Disability Index (ODI) scores, kyphotic angle changes at the infected level, operative time, intraoperative blood loss, postoperative drainage volume, timing of drain removal, postoperative hospital stay, modified MacNab Criteria (MNC), and postoperative complications. Detailed information is presented in Tables 1 and 2.
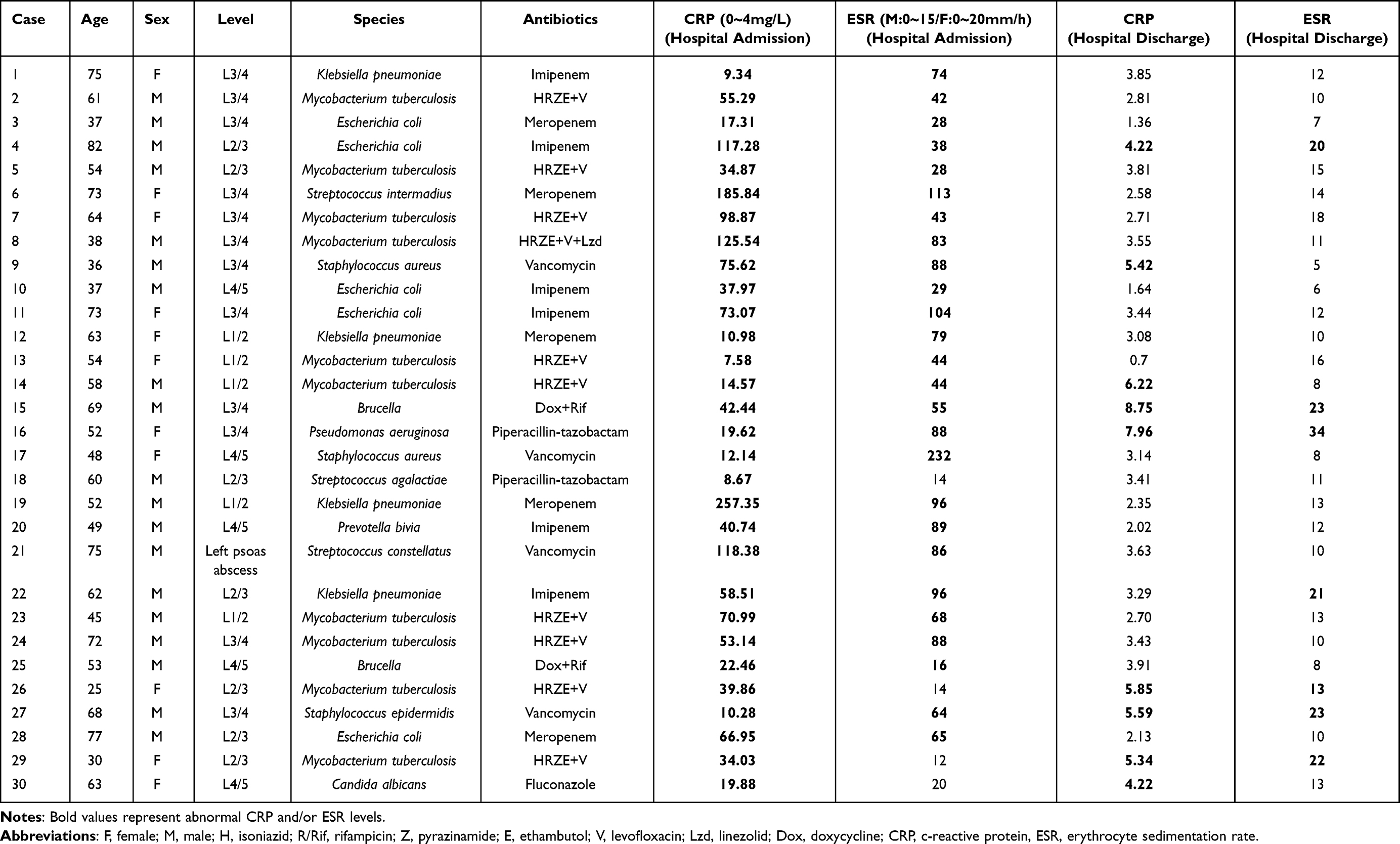 |
Table 1 Clinical and Treatment Characteristics |
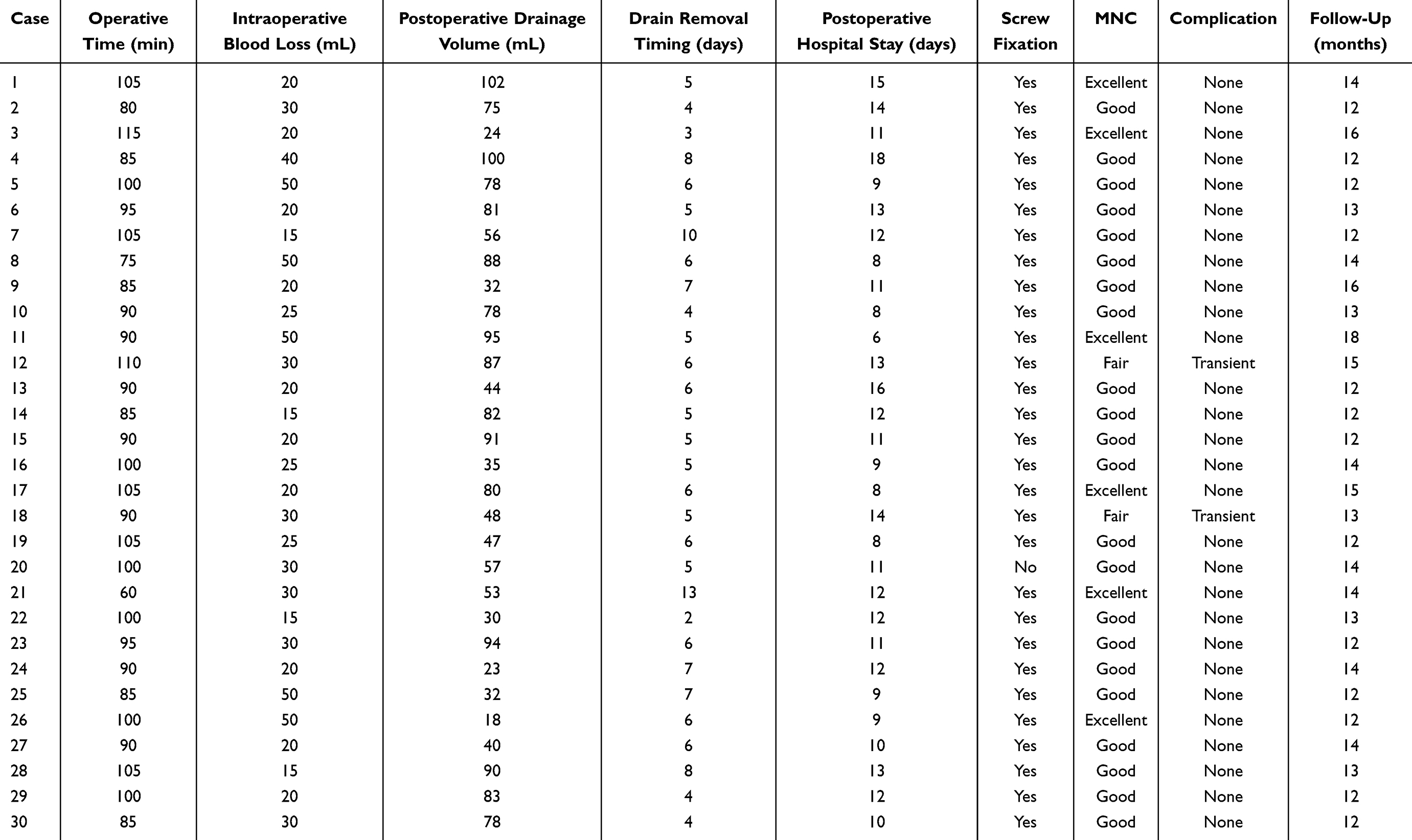 |
Table 2 Surgical Characteristics |
Surgical Technique
Positioning
Under general anesthesia, the patient is placed in a standard lateral decubitus position with the abscess and lesion oriented upward, and the lower limbs were flexed to relax the psoas muscle. The vertebral endplates should appear as a single line on both anteroposterior (AP) and lateral views, with the bilateral pedicle shadows equidistant from the spinous process on the AP view and completely overlapping on the lateral view.
Incision
Preoperative fluoroscopic imaging is used to determine the location of the responsible segment, and the skin is marked to indicate the intervertebral gap of the affected segment and the positions of each channel. The marked points are as follows:
- Midpoint of the lesion gap.
- Intersection located 1.5 cm posterior to the posterior margin of the vertebral body and the lesion gap.
- Intersection located 1.5 cm anterior to the anterior border of the vertebral body and the lesion gap.
- Anterior superior angle of the vertebral body above the lesion gap (D1) or anterior inferior angle of the vertebral body below the lesion gap (D2) (endoscopic channel).
- 2 cm anterior to the anterior border of the vertebral body at the intersection with the lesion gap, either 4 cm cranially (E2) or 4 cm caudally (E1) (Figure 1).
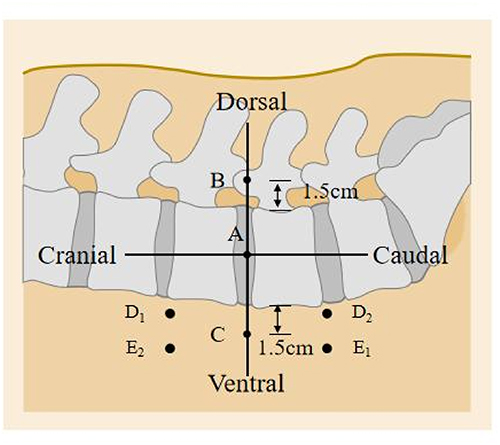 |
Figure 1 Surgical Incision Design Diagram. (A) Midpoint of the lesion gap. (B) The intersection point 1.5 cm posterior to the posterior margin of the vertebral body and the lesion gap. (C) The intersection point 1.5 cm anterior to the anterior border of the vertebral body and the lesion gap. (D) The anterior superior angle of the vertebral body above the lesion gap (D1) or the anterior inferior angle of the vertebral body below the lesion gap (D2) (endoscopic channel). (E) 2 cm anterior to the anterior border of the vertebral body at the intersection with the lesion gap, either 4 cm cranially (E2) or 4 cm caudally (E1). |
Surgical Procedure
The surgical steps are as follows: a. An incision is made at point B, and a custom balloon is used to create a cavity (500–600 mL). b. Trocars are inserted at points C, D1, and E1 (or C, D2, and E2). c. The psoas muscle is dissected and exposed up to its anterior edge. d. At the lesion intervertebral gap, the psoas muscle is retracted posteriorly to the posterior edge of the vertebral body. e. The intervertebral gap and the margins of the adjacent vertebral bodies are exposed transversely. f. The lesion is removed using a curette or osteotome. g. The area is irrigated, bone grafting is performed for fusion, a drainage tube is placed, and the incision is sutured (Figure 2). All patients underwent posterior lumbar percutaneous pedicle screw fixation postoperatively (except for those solely with psoas abscess).
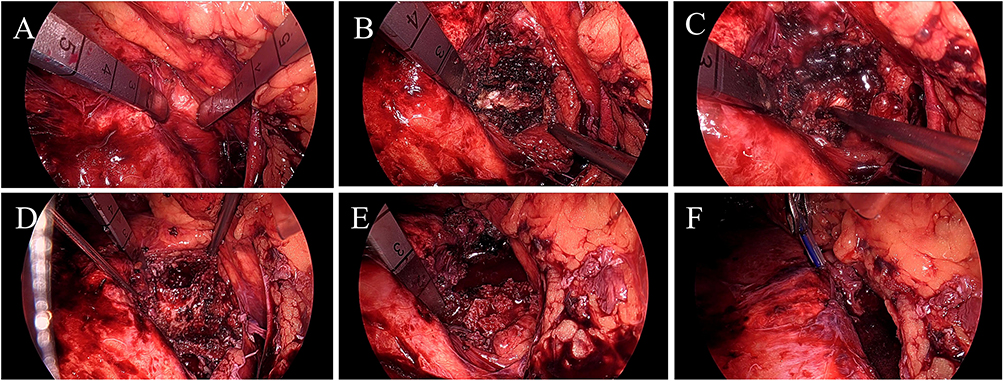 |
Figure 2 (A) Dissect and expose up to the anterior margin of the psoas. (B) Expose the intervertebral space (lesion). (C) Clear the lesion using a curette or osteotome. (D) Expose the affected vertebral body. (E) Implant allogeneic bone for fusion. (F) Irrigate with physiological saline and place a drainage tube. |
Outcome Assessment
Operative time, intraoperative blood loss, postoperative drainage volume, postoperative timing of drain removal, postoperative hospital stay, preoperative and postoperative CRP/ESR follow-up results, postoperative complications, VAS scores, ODI scores, and the MNC were used to assess the clinical effectiveness. The MNC categorizes outcomes as follows: “Excellent” (patient is symptom-free and able to resume daily activities and work), “Good” (slight residual symptoms, minor activity limitation, no impact on daily life or work), “Fair” (partial symptom relief, significant activity limitation, daily life and work affected), or “Poor” (postoperative symptoms unchanged or worse compared with preoperative status).
Statistical Analysis
All the statistical analyses were conducted using SPSS version 23.0. Descriptive data are presented as the means and Standard Deviations (SDs). Student’s t tests were used to compare continuous variables when the data were continuous, normally distributed, and homoscedastic. Chi-square tests and Fisher’s exact tests were applied to assess differences in categorical variables. A p-value < 0.05 was considered statistically significant.
Results
This study included 30 patients with lumbar infectious spondylodiscitis who underwent endoscopic retroperitoneal debridement between June 2023 and June 2024. Of these, 29 patients with significant vertebral destruction underwent interbody bone grafting followed by posterior percutaneous pedicle screw fixation, whereas the remaining patient, who had an isolated psoas abscess with minimal vertebral involvement underwent endoscopic retroperitoneal psoas abscess debridement alone.
Among the 30 patients, 19 were male (19/30, 63.33%) and 11 were female (11/30, 36.67%), with a mean age of 56.83±14.80 years. The infection levels ranged from L1/2 to L4/5, with 5 cases at L1/2, 7 cases at L2/3, 12 cases at L3/4, and 5 cases at L4/5. Additionally, one patient had a left psoas abscess. All patients were diagnosed with primary lumbar infectious spondylodiscitis. Species including Mycobacterium tuberculosis in 10 cases (10/30, 33.33%), Escherichia coli in 5 cases (5/30, 16.67%), Klebsiella pneumoniae in 4 cases (4/30, 13.33%), Staphylococcus aureus and Brucella species each in 2 cases (2/30, 6.67%), Streptococcus intermedius, Pseudomonas aeruginosa, Streptococcus agalactiae, Prevotella bivia, Streptococcus constellatus, Staphylococcus epidermidis, and Candida albicans each in 1 case (1/30, 3.33%) (Table 1).
Additionally, the mean operative time was 93.67±11.18 min (range, 60–115 min), mean intraoperative blood loss was 27.83±11.45 mL (range,15–50 mL), mean postoperative drainage volume was 64.03±25.98 mL (range,18–102 mL), mean time to drain removal was 5.83±2.03 days (range,2–13 days), and mean postoperative hospital stay was 11.23±2.60 days (range, 6–18 days). All patients were followed for a minimum of 12 months, with a mean follow-up of 13.3±1.51 months (range, 12–18 months). During postoperative follow-up, two patients experienced transient sensory abnormalities in the affected lumbar segment, which resolved spontaneously within 1–2 weeks. No recurrence of infection or serious surgery-related complications was observed in any patient during the follow-up period (Table 2).
This study also found that postoperative CRP and ESR levels were significantly reduced compared to preoperative values (p < 0.001). In addition to surgical intervention, these improvements likely reflect the standardized anti-infective treatment administered to the patients. Furthermore, VAS and ODI scores demonstrated significant improvements in lumbar pain and function, which remained stable throughout the follow-up period (p < 0.05). No signs of spinal instability were observed in any cases during follow-up, and the mean kyphotic angle increased by 1.39° (Table 3).
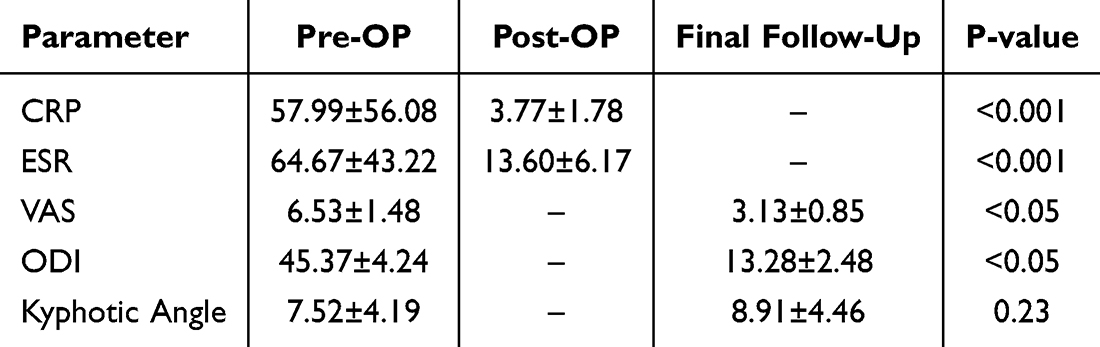 |
Table 3 Pre- and Post-Operative Clinical Outcomes |
Discussion
In recent years, the incidence of common pathogens associated with lumbar infectious spondylodiscitis, such as Methicillin-Resistant Staphylococcus aureus (MRSA) and Mycobacterium tuberculosis (MT), has been increasing in endemic regions.9 For patients with identified pathogens and no neurological or structural damage, antibiotics combined with bed rest remain the preferred conservative treatment. However, with the rise of antibiotic-resistant bacteria and delays in diagnosis, the failure rate of conservative treatment has been increasing, necessitating surgical intervention for patients who fail conservative management. Currently, there is significant controversy regarding surgical approaches for lumbar infectious spondylodiscitis. We propose and validate the efficacy and safety of endoscopic retroperitoneal debridement combined with posterior percutaneous pedicle screw fixation for the treatment of lumbar infectious spondylodiscitis.
Recently, surgery for lumbar infectious spondylodiscitis has become increasingly common. Ideal treatment combines the universal goals of any spine surgery, which are decompression of the neural elements and stabilization, with source control and eradication of the infection.6 Recent advancements in anterior, oblique, and lateral surgical approaches have provided improved operative fields for anterior debridement and reconstruction.10,11 The anterior approach not only enables precise correction of lumbar lordosis but also optimizes sagittal alignment, offering unique advantages for cases of lower lumbar pyogenic spondylitis.12
However, conventional lateral or anterior approaches are often constrained by limited exposure and restricted working corridors due to the use of tubular retractors, which may hinder adequate debridement in lumbar infections.13,14 In contrast, the retroperitoneoscopic technique used in our study utilizes CO2-induced pneumoperitoneum together with flexible endoscopic instruments to create a spacious and well-illuminated operative field, allowing more comprehensive lesion clearance without requiring a wide surgical exposure. Moreover, compared with traditional lateral or anterior approaches, the retroperitoneoscopic method is distinctly less invasive, requiring only a 1.5-cm incision. Unlike procedures that involve muscle splitting or transection,6,15 this technique relies on pneumoperitoneum and gentle blunt separation of the psoas muscle, thereby minimizing tissue trauma and facilitating faster postoperative recovery.
From a clinical perspective, significant symptom improvement was observed based on VAS scores and ODI scores in our study. Similarly, Choi et al16 demonstrated that percutaneous endoscopic debridement and drainage (PEDD) provided immediate pain relief and reduced disability in treating spinal infections, particularly in elderly patients with comorbid conditions. Tang et al17 reported that endoscopic debridement significantly reduced operative time and intraoperative blood loss, facilitating faster recovery and shorter hospital stays. In this study, the mean operative time was 93.67 ± 11.18 minutes, intraoperative blood loss was 27.83 ± 11.45 mL, and the average postoperative hospital stay was 11.23 ± 2.60 days, all of which were significantly lower than those associated with traditional open surgery.
Endoscopic retroperitoneal debridement provides direct access for comprehensive lesion clearance and reliable catheter drainage. Specifically, paraspinal, epidural, and psoas abscesses can be successfully treated without opening the epidural space because abscesses and infected areas are almost always interconnected.18 Traditionally, for patients with isolated psoas abscess, CT-guided percutaneous drainage has limited applicability due to frequent catheter occlusion caused by viscous pus. Studies suggest that irrigation during drainage can improve outcomes,19,20 but issues such as exudation and inadequate drainage persist. Endoscopic debridement addresses these challenges by thoroughly clearing infectious abscesses and achieving wide anterior decompression. This technique also prepares an optimal environment for allograft placement to facilitate fusion, while enabling intraoperative local antibiotic administration and continuous postoperative drainage (Figure 3). Similarly, endoscopic debridement addresses these challenges by thoroughly clearing lesions, allowing local antibiotic application intraoperatively and continuous postoperative drainage. Katara et al21 first described retroperitoneoscopic drainage of a psoas abscess in a pediatric patient, and three case series22–24 confirmed the safety and efficacy of this approach in patients with psoas abscess secondary to spondylodiscitis. Froiio25 reported successful infection control in a patient with a psoas abscess caused by Streptococcus sp. using retroperitoneoscopic drainage. Consistent with their findings, in all cases involving abscesses treated with the endoscopic retroperitoneal technique in the present study, the abscesses were effectively cleared and brought under satisfactory control.
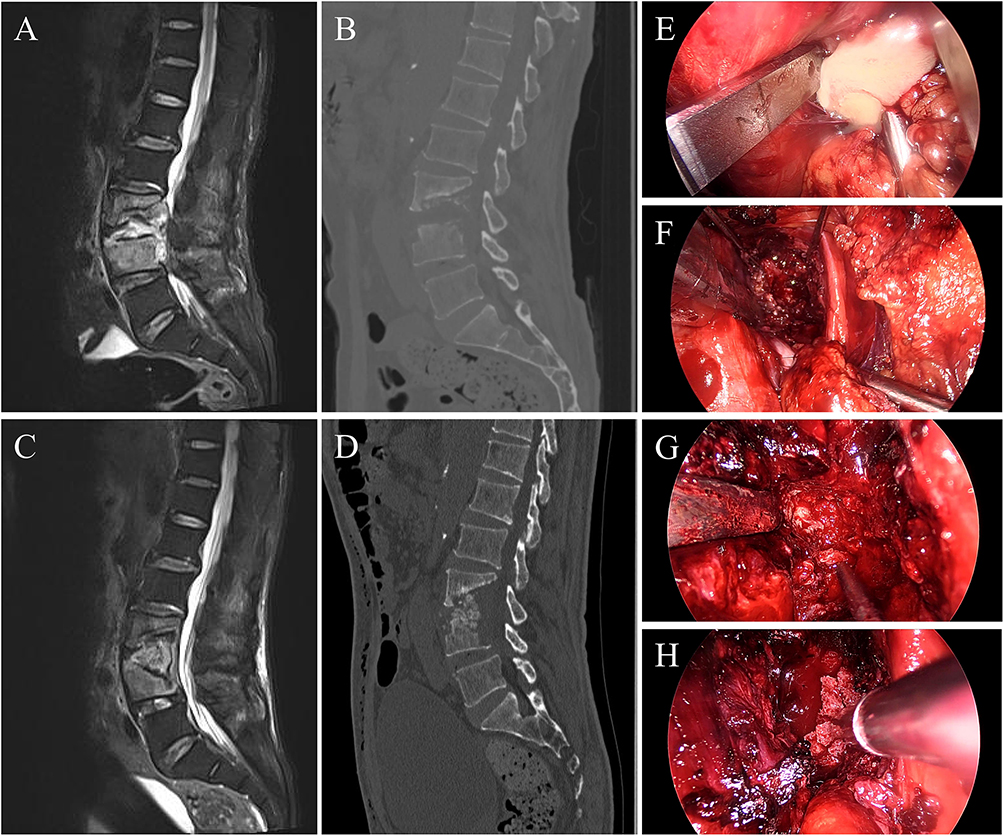 |
Figure 3 Case 24 - Lumbar Tuberculosis (A) Preoperative MRI demonstrates a lesion at the L3/4 level with an associated abscess causing spinal cord compression. (B) Preoperative CT reveals severe destruction of the L3/4 vertebral bodies accompanied by a posterior wall defect. (C) Postoperative MRI shows complete resolution of the abscess and decompression of the spinal cord. (D) Six-month postoperative CT indicates partial fusion of the affected vertebrae without evidence of vertebral collapse. (E) Intraoperative exposure of the psoas muscle with abscess clearance. (F) Exposure and debridement of the intervertebral space to remove pathological tissue. (G) Exposure of the posterior vertebral wall for spinal canal decompression. (H) Implantation of allogeneic bone graft to facilitate vertebral fusion. |
For cases involving both intervertebral disc and vertebral body infection, endoscopic retroperitoneal debridement not only enables thorough lesion clearance but also provides sufficient space for the placement of interbody graft placement to facilitate spinal fusion (Figures 4 and 5). In the present study, 29 of the 30 patients who exhibited severe vertebral bone destruction underwent anterior allogeneic bone grafting with posterior percutaneous fixation. Follow-up results demonstrated that the majority of these patients (27/29, 93.10%) achieved solid bony fusion. The two patients who did not achieve fusion were likely due to insufficient follow-up duration rather than failure of the fusion process. One patient, who presented with a psoas abscess with only mild vertebral destruction, underwent lesion clearance alone, followed by posterior percutaneous pedicle screw fixation once the infection was controlled, without anterior interbody grafting. These findings suggest that endoscopic retroperitoneal debridement combined with allogeneic bone grafting, together with posterior percutaneous fixation, effectively promotes stable bony fusion.
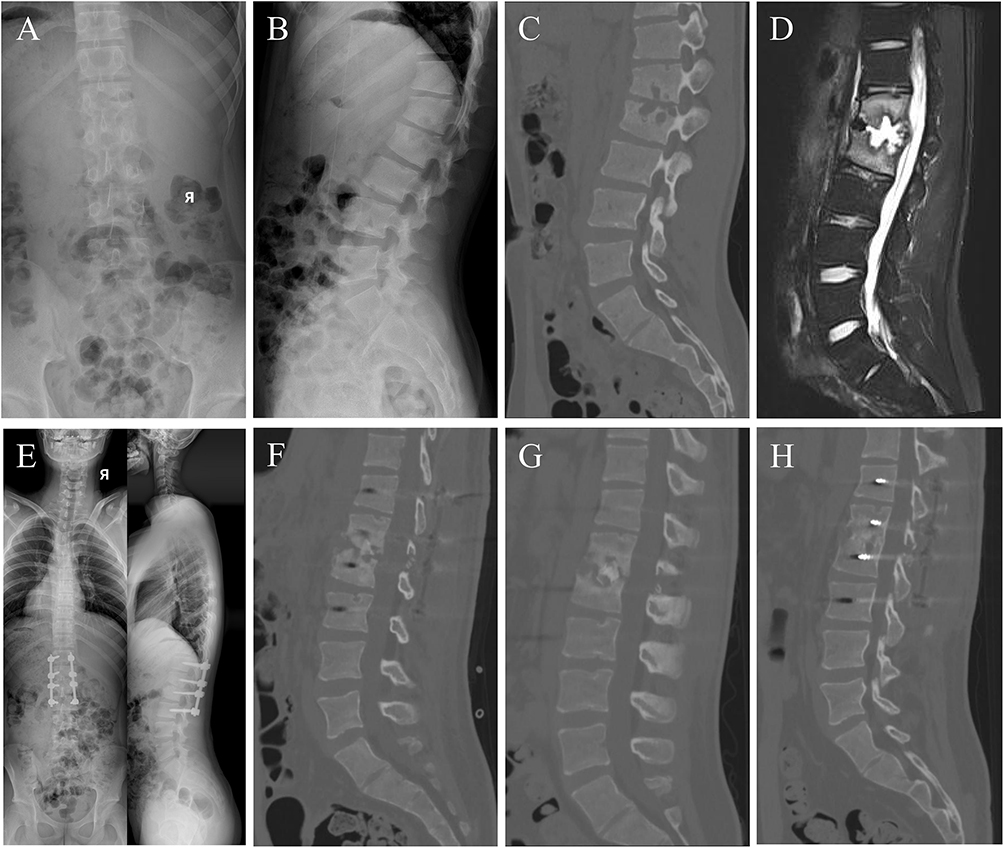 |
Figure 4 Case 12 -Lumbar infectious spondylodiscitis (Klebsiella pneumoniae) (A and B) Preoperative X-ray revealed narrowing of the L1/2 intervertebral space. (C) Preoperative CT demonstrated bone destruction at L1/2. (D) Preoperative MRI (T2 fat-suppressed) indicated abscess formation at L1/2. (E) X-ray at 1 month postoperatively. (F) CT at 1 month postoperatively showed initial fusion at L1/2. (G) CT at 3 months postoperatively revealed substantial fusion at L1/2. (H) CT at 10 months postoperatively confirmed complete fusion at L1/2. |
 |
Figure 5 Case 18 -Lumbar infectious spondylodiscitis (Streptococcus agalactiae) (A) Preoperative X-ray revealed narrowing of the L2/3 intervertebral space. (B) Preoperative CT revealed bone destruction and narrowing of the intervertebral space at L2/3. (C) Preoperative MRI (T2 fat-suppressed) indicated abscess formation at L2/3. (D) X-ray at 1 month postoperatively. (E) CT at 3 months postoperatively showed substantial fusion at L2/3. (F) CT at 13 months postoperatively confirmed complete fusion at L2/3. |
Comparison of pre- and postoperative radiographic imaging revealed an average change in local kyphotic angle of only 1.39 degrees at final follow-up. The lack of significant postoperative sagittal alignment changes in our cohort may be partially explained by the study’s inclusion criteria, as all included patients were without spinal deformity and instability. In addition, several biological and biomechanical factors may also have contributed to rapid structural recovery: first, the intervertebral disc annulus, spinal ligaments, and the junction of the cartilaginous endplate are rich in mesenchymal cells, where repeated mechanical stimulation or local inflammation may trigger rapid osteogenesis.26,27 Second, narrowing of the intervertebral space allows rapid contact between the cranial vertebral endplate and the caudal endplate of the middle spine, forming a supportive structure posterior to the intervertebral joint. Third, in infectious spondylodiscitis, the posterior ligamentous complex typically remains intact, acting as a tension band to inhibit kyphotic deformity progression. Postoperative timely fixation and a full course of effective anti-infective therapy, combined with improved sagittal alignment, likely further accelerated bone tissue healing.
Common complications of anterior lumbar surgery include vertebral collapse, postoperative ileus, vascular injury, nerve injury, ureteral injury, and the need for blood transfusion.28,29 Mehren et al30 reported a vascular/nerve complication rate of 0.37% (3/812) for anterior lumbar surgery. In this study, no significant intraoperative complications were observed, with only two patients experiencing transient postoperative sensory abnormalities, which resolved by the end of follow-up. This low morbidity rates may be attributed to three main factors. First, as a minimally invasive procedure, it involves a short operative duration, substantially reducing the time patients spend under anesthesia. Second, minimal intraoperative trauma results in reduced blood loss, thereby maintaining stable hemodynamics in patients. Third, rapid postoperative recovery enables early ambulation, minimizing complications associated with prolonged bed rest.
This study has several limitations, including a small sample size and the absence of a control group. All enrolled cases involved single-level lumbar infectious spondylodiscitis, and the efficacy of endoscopic retroperitoneal debridement for multi-level lumbar infectious spondylodiscitis remains unclear. We believe that multicenter, long-term follow-up randomized controlled trials are necessary to address these limitations. Nevertheless, this study demonstrates that endoscopic retroperitoneal debridement is a feasible option for treating lumbar infectious diseases.
Conclusion
Endoscopic retroperitoneal debridement combined with posterior percutaneous pedicle screw fixation is an effective and reliable approach for treating lumbar infectious spondylodiscitis. This method efficiently clears the lesion, significantly improves patient symptoms, and is associated with low postoperative complication and infection recurrence.
Abbreviations
CRP, C-Reactive Protein; ESR, Erythrocyte Sedimentation Rate; VAS, Visual Analog Scale; ODI, Oswestry Disability Index; MNC, MacNab Criteria; AP, AnteroPosterior; MRSA, Methicillin-Resistant Staphylococcus Aureus; MT, Mycobacterium Tuberculosis; PEDD, Percutaneous Endoscopic Debridement and Drainage.
Data Sharing Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The portions of this study involving human participants, human materials or human data were conducted in accordance with the Declaration of Helsinki and were approved by the Ethics committee of Shandong Public Health Clinical Center, Shandong University (approval number K2025137). All patients provided written informed consent, explicitly informed that the study aims to investigate the application and efficacy of endoscopic retroperitoneal debridement combined with posterior percutaneous pedicle screw fixation. Written informed consent was obtained from the patient for publication of this research and any accompanying images.
Author Contributions
Yongrui Yang and Wenkai Ruan - Conceptualization, Writing original draft. Jianlong Li and Rongpan Dang - Data curation, Writing - original draft. Huigang An and Wentao Zhao - Methodology, Writing - original draft. Liang Xu and Hongdong Tan - Formal analysis, Validation, Writing – revise & editing. All authors took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no financial support was received for the research and/or publication of this article.
Disclosure
The authors declare that they have no competing interests.
References
1. Berbari EF, Kanj SS, Kowalski TJ, et al. 2015 Infectious Diseases Society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in adults. Clin Infect Dis. 2015;61(6):e26–e46. doi:10.1093/cid/civ482
2. Babic M, Simpfendorfer CS. Infections of the Spine. Infect Dis Clin N Am. 2017;31(2):279–297. doi:10.1016/j.idc.2017.01.003
3. Pola E, Taccari F, Autore G, et al. Multidisciplinary management of pyogenic spondylodiscitis: epidemiological and clinical features, prognostic factors and long-term outcomes in 207 patients. Eur Spine J. 2018;27(Suppl 2):229–236. doi:10.1007/s00586-018-5598-9
4. Rutges JPHJ, Kempen DH, van Dijk M, Oner FC. Outcome of conservative and surgical treatment of pyogenic spondylodiscitis: a systematic literature review. Eur Spine J. 2016;25(4):983–999. doi:10.1007/s00586-015-4318-y
5. Lin CY, Chang CC, Chen YJ, et al. New strategy for minimally invasive endoscopic surgery to treat infectious spondylodiscitis in the thoracolumbar spine. Pain Physician. 2019;22(3):281–293. PMID: 31151336.
6. Campbell DH, Dowling TJ, Hah R, et al. Surgical strategies for spinal infections: a narrative review. N Am Spine Soc J. 2023;16:100293. doi:10.1016/j.xnsj.2023.100293
7. Obenchain TG. Laparoscopic lumbar discectomy: case report. J Laparoendosc Surg. 1991;1(3):145–149. doi:10.1089/lps.1991.1.145
8. Regan JJ, McAfee PC, Guyer RD, et al. Laparoscopic fusion of the lumbar spine in a multicenter series of the first 34 consecutive patients. Surg Laparosc Endosc. 1996;6(6):459–468. PMID: 8948039. doi:10.1097/00019509-199612000-00009
9. Leowattana W, Leowattana P, Leowattana T. Tuberculosis of the spine. World J Orthop. 2023;14(5):275–293. doi:10.5312/wjo.v14.i5.275
10. Wang B, Chen C, Hua W, et al. Minimally invasive surgery oblique lumbar interbody debridement and fusion for the treatment of lumbar spondylodiscitis. Orthop Surg. 2020;12(4):1120–1130. doi:10.1111/os.12711
11. Tong YJ, Liu JH, Fan SW, et al. One-stage debridement via oblique lateral interbody fusion corridor combined with posterior pedicle screw fixation in treating spontaneous lumbar infectious spondylodiscitis: a case series. Orthop Surg. 2019;11(6):1109–1119. doi:10.1111/os.12562
12. Choi SH, Koo JW, Hur JM, et al. A new surgical strategy for infective spondylodiscitis: comparison between the combined antero-posterior and posterior-only approaches. Spine. 2020;45(19):E1239–E1248. doi:10.1097/BRS.0000000000003544
13. Hah R, Kang HP. Lateral and oblique lumbar interbody fusion-current concepts and a review of recent literature. Curr Rev Musculoskelet Med. 2019;12(3):305–310. doi:10.1007/s12178-019-09562-6
14. Shi J, Wu H, Li F, et al. Meta-analysis of the efficacy and safety of OLIF and TLIF in the treatment of degenerative lumbar spondylolisthesis. J Orthop Surg Res. 2024;19(1):242. doi:10.1186/s13018-024-04703-1
15. Sun D, Liang W, Hai Y, Yin P, Han B, Yang J. OLIF versus ALIF: which is the better surgical approach for degenerative lumbar disease? A systematic review. Eur Spine J. 2023;32(2):689–699. doi:10.1007/s00586-022-07516-0
16. Choi EJ, Kim SY, Kim HG, et al. Percutaneous endoscopic debridement and drainage with four different approach methods for the treatment of spinal infection. Pain Physician. 2017;20(6):E933–E940. PMID: 28934797.
17. Tang Y, Ye J, Hu X, et al. Retroperitoneoscopic debridement and internal fixation for the treatment of lumbar tuberculosis. Medicine. 2021;100(37):e27198. doi:10.1097/MD.0000000000027198
18. Yu CH. Full-endoscopic debridement and drainage treating spine infection and psoas muscle abscess. J Spine Surg. 2020;6(2):415–423. doi:10.21037/jss.2020.01.04
19. Matsumoto T, Yamagami T, Morishita H, et al. CT-guided percutaneous drainage within intervertebral space for pyogenic spondylodiscitis with psoas abscess. Acta Radiol. 2011;53(1):76–80. doi:10.1258/ar.2011.110418
20. Ran B, Chen X, Zhong Q, et al. CT-guided minimally invasive treatment for an extensive spinal epidural abscess: a case report and literature review. Eur Spine J. 2017;27(Suppl 3):380–385. doi:10.1007/s00586-017-5307-0
21. Katara AN, Shah RS, Bhandarkar DS, et al. Retroperitoneoscopic drainage of a psoas abscess. J Pediatr Surg. 2004;39(9):e4–5. doi:10.1016/j.jpedsurg.2004.05.033
22. Büyükbebeci O, Seçkiner I, Karslı B, et al. Retroperitoneoscopic drainage of complicated psoas abscesses in patients with tuberculous lumbar spondylitis. Eur Spine J. 2011;21(3):470–473. doi:10.1007/s00586-011-2049-2
23. Zhang X, Zhang Z, Zhang Y, et al. Minimally invasive retroperitoneoscopic surgery for psoas abscess with thoracolumbar tuberculosis. Surg Endosc. 2014;29(8):2451–2455. doi:10.1007/s00464-014-3913-z
24. Joob B, Wiwanitkit V. Retroperitoneoscopic drainage of bilateral psoas abscesses. Asian J Endosc Surg. 2014;7(4):345. doi:10.1111/ases.12117
25. Froiio C, Bernardi DT, Asti E, et al. Retroperitoneoscopic drainage of cryptogenic psoas abscess. BMJ Case Rep. 2020;13(7):e235579. doi:10.1136/bcr-2020-235579
26. Berthelot JM, Le Goff B, Maugars Y. Pathogenesis of hyperostosis: a key role for mesenchymatous cells? Joint Bone Spine. 2013;80(6):592–596. doi:10.1016/j.jbspin.2013.03.013
27. Hsu LC, Tseng TM, Yang SC, et al. Bilateral portal percutaneous endoscopic debridement and lavage for lumbar pyogenic spondylitis. Orthopedics. 2015;38(10):e856–63. doi:10.3928/01477447-20151002-50
28. He L, Xie P, Shu T, et al. Clinical and radiographic results of a minimally invasive lateral transpsoas approach for treatment of septic spondylodiscitis of the thoracolumbar and lumbar spine. World Neurosurg. 2018;116:e48–e56. doi:10.1016/j.wneu.2018.03.193
29. Tschugg A, Hartmann S, Lener S, et al. Minimally invasive spine surgery in lumbar spondylodiscitis: a retrospective single-center analysis of 67 cases. Eur Spine J. 2017;26(12):3141–3146. doi:10.1007/s00586-017-5180-x
30. Mehren C, Mayer HM, Zandanell C, et al. The oblique anterolateral approach to the lumbar spine provides access to the lumbar spine with few early complications. Clin Orthop Relat R. 2016;474(9):2020–2027. doi:10.1007/s11999-016-4883-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.