Back to Journals » Research and Reports in Urology » Volume 15
Endoscopic Management of Upper and Lower Ureteric Stones Using Pneumatic Lithotripter: A Retrospective Medical Records Review
Authors Mustafa M, Al Zabadi H ![]() , Mansour S, Nabulsi A
, Mansour S, Nabulsi A
Received 18 October 2022
Accepted for publication 23 December 2022
Published 11 February 2023 Volume 2023:15 Pages 77—83
DOI https://doi.org/10.2147/RRU.S392881
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Mahmoud Mustafa,1,2 Hamzeh Al Zabadi,3 Shaden Mansour,1 Aya Nabulsi1
1Department of Urology, An-Najah National University Hospital, An-Najah National University, Nablus, Palestine; 2Medicine Department, Faculty of Medicine and Health Sciences, An-Najah National University, Nablus, Palestine; 3Public Health Department, Faculty of Medicine and Health Sciences, An-Najah National University, Nablus, Palestine
Correspondence: Mahmoud Mustafa, Department of Urology, An-Najah National University Hospital, An-Najah National University, Nablus, Palestine, Email [email protected] Hamzeh Al Zabadi, Public Health Department, Faculty of Medicine and Health Sciences, An-Najah National University, Nablus, Palestine, Email [email protected]
Background: In this study we aimed to assess and compare the rate of sem-irigid ureterorenoscope in the treatment of upper and lower ureter stones through pneumatic lithotripsy (PL).
Materials and Methods: Ninety-two patients with a mean age±SD of 45± 15years who had had a surgical procedure performed by the same experienced surgeon between January 2013 and July 2015 were included in the study. The mean±SD stone size was 8.8± 2.6 mm. Forty-two of the patients (45.7%) had upper ureter stones and 50 (54.3%) had lower ureter stones in order to increase the success rate and avoid stone migration. The medical files of the patients were reviewed regarding age, sex, stone size, stone location, success rate, complications, and presence of hydronephrosis. Success was operationally defined as the complete fragmentation of stone to very small parts that could pass or complete extraction of the stone.
Results: Eighty-four of the patients were stone free (91%). The success rates for patients with upper or lower ureteric stones were 93% and 90%, respectively (P=0.63). There were no complications during the operation. However, 4 patients (4.4%) had postoperative complications in terms of urinary tract infection or urosepsis. Those were accurately managed by the suitable medical treatment.
Conclusion: Semi-rigid ureterorenoscopy by using PL was a safe and practical treatment option for managing the upper and lower ureter stones. Performing the tips and tricks of ureterorenoscopy by an experienced surgeon seems to enhance the success rate, especially in upper ureter stones.
Keywords: pneumatic lithotripsy, Palestine, ureterorenoscopy, ureter stone, ureter
Introduction
Ureterorenoscopy (URS) can be used singly or with various lithotripters: electrohydraulic, pneumatic, ultrasonic or laser lithotripters. Currently, pneumatic lithotripters (PL) are more frequently used. The working principle of PL is based on the conduction of air pressure on the metal bar at certain frequencies. A pneumatic lithotripter can be best performed using a rigid instrument. It is very durable and it can be used many times. The main disadvantage is that the broken fragments should be extracted one by one using stone forceps. It can also push the fragments back into the renal collecting system. The pneumatic lithotripter is more effective than URS for hard stones like cystine or calcium oxalate monohydrates.1 Laser lithotripters (LL) are expensive and need continuous maintenance, but higher successful fragment rates are achieved with LL. The zone of thermal injury associated with laser energy ranges from 0.5 to 1 mm.2 This photo thermal may cause ureteral injury and may damage guide wire or the basket. The greatest advantages of laser energy are high success and low risk of stone migration, especially in upper ureter stone management.3 In a recent comparative study between LL and PL, Kizlay et al reported that both energies are safe in children and adults, with similar clinically insignificant complication rates.3 However, in the short term, LL provides better stone-free rates in both children and adults, especially in upper ureteral stones.3 While the rationale for the use of URS in the lower ureter stone is well known and documented, URS has comparable effects or is even superior to extracorporeal shock wave lithotripsy (ESWL) in the managements of upper ureter stones. All operations were done by a single experienced surgeon utilizing many tips and tricks to improve the expected low success rate of endoscopic management of upper ureter stone when using PL. We aimed to evaluate and compare the success rate of semi-rigid ureterorenoscope in the management of upper and lower ureter stones using pneumatic lithotripsy (PL).
Materials and Methods
Ninety-two patients with a mean±SD age of 45±15 years, of whom 73.9% were male and 26.1% were female, who underwent endoscopic management of ureter stones by a single experienced surgeon between January 2013 and July 2015 were included. Table 1 shows the demographic characteristics of the study groups.
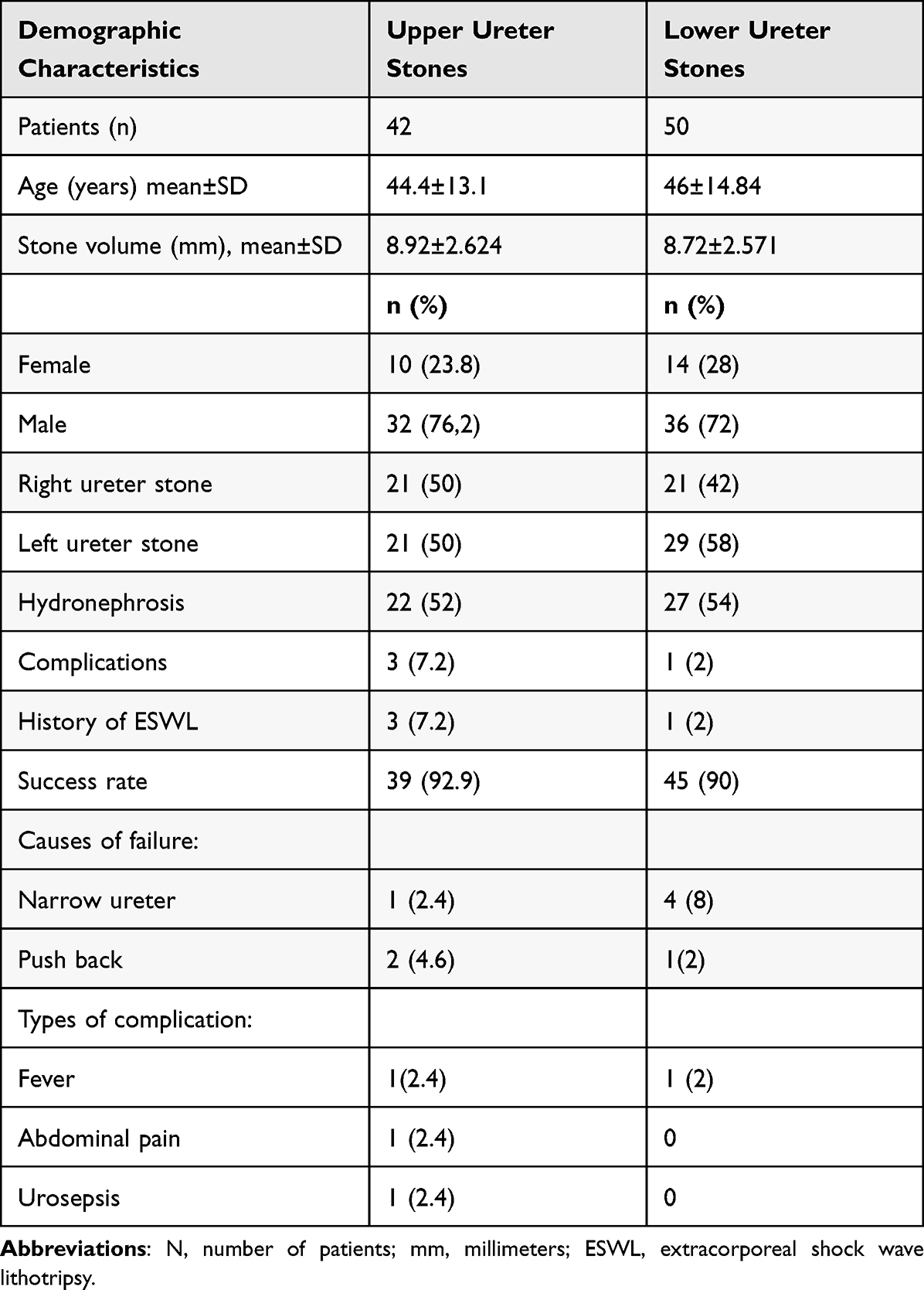 |
Table 1 Demographic Characteristics of the Study Groups |
The mean stone size was 8.8±2.6 mm. Forty-two patients (45.7%) had upper ureter stones, and 50 patients (45.3%) had lower ureter stones. All patients were operated as a day case procedure.
All patients had a preoperative evaluation in terms of full biochemistry and radiologic evaluation: ultrasound and kidney ureter bladder (KUB) and/or noncontrast-enhanced computer tomography (CT). All URS was performed with 8/9.8 Fr semi-rigid ureterorenoscope by the same surgeon as a day case procedure. Many tips and tricks were used to improve the success rate of URS, especially for the upper ureter stones. Pneumatic lithotripters (Vibrolith Lithotripsy System-ELMED, Turkey) were used in all operations (probe 3.6mm). All patients with fever, abnormal septic parameters and/or positive urine culture were given appropriate medical therapy and, after normalization of the parameters, were included. The medical records were retrospectively reviewed in terms of: age, sex, stone size, stone location, success rate and complications. The success rate was defined as a complete extraction of the stone as a unit or its fragments or fragmentation of the stone to small pieces that can pass smoothly. All patients were monitored as outpatients at 2 weeks and real abdominal ultrasound and KUB were done for all patients. The average operative time was 20 minutes (range: 15–25 minutes. Double J-stent (DJS) was placed for the patient who had a huge load of fragments, had push backed the stone or had failed trial of the URS.
Statistical Analysis
The SPSS ver. 10.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. A p-value of greater than 0.05 was accepted as insignificant. Comparison between the parameters of subgroups was calculated by use of Student’s t-test. Pearson correlation test was used to determine the factors which influence the success rate.
Results
Stone free was achieved in 84 patients (91%). The success rates for upper and lower ureteric stones were 93% and 90%, respectively (p=0.63). There were no serious preoperative complications. Postoperative complications were found in 4 patients (4.4%). Complications were fever in two patients (2.2%), abdominal pain in one patient (1.1%), and urosepsis in one patient (1.1%), and all of these complications were managed with appropriate medical therapy. All complications occurred in patients with upper ureter stones except one patient who had lower ureter stones. Management failed in 8 patients (8.7%): five of them (5.4%) due to narrow ureter (4 patients had lower ureter stones) and three patients (3.3%) due to push back of the stone to the kidney (1 patient had lower ureter stones). There was no significant correlation between success rates and age, stone volume, stone location, age, presence of hydronephrosis, sex and success rates.
Discussion
URS is defined as an endoscopic visualisation of the renal pelvis and ureter for diagnostic and/or therapeutic objectives. Various therapeutic alternatives such as extracorporeal shock wave lithotripsy (ESWL), flexible URS, antegrade URS, retrograde URS, and laparoscopic ureterolithotomy are available. URS is the backbone in the management of lower third ureteric stones, with an approximate success rate of more than 90%.4,5 ESWL has a low success rate in the management of lower third ureteric stones, but good results in the management of upper stones.6 In the large impacted upper ureteral calculi with size more than 1 cm, URS is superior to ESWL.7
In our study, we investigated the efficacy of semi-rigid ureterorenoscope in the management of upper and lower ureter stones using PL. To improve the success rate of URS for upper ureter stones, many trips and tricks were used. Our overall success rate was 91%, which is comparable to international published data.1,8 Many studies in the literature reported that the fragmentation rates of holmium laser-assisted ureteroscopy are significantly better in the upper ureter and the need for auxiliary procedures is significantly less when compared with pneumatic lithotripsy.3 The main disadvantage of PL is stone migration. Most stone migration usually occurred in proximal ureteric stones and the rate of migration was reported to be about 30%. Therefore, many different methods are used for prevention of stone migration during ureteroscopic lithotripsy, like Stone Cone™, PercSys and lidocaine jelly instillation.9,10 Although lidocaine instillation was found to have no significant effect on reduction of stone migration, Stone Cone™ and PercSys do reduce migration to 4.5% and 8.7%, respectively.9 Also, XenX was found to be a safe and effective device for the treatment of upper ureteric tract stones and it may reduce the risk for the need of auxiliary procedures and for the insertion of a DJS.10 Nevertheless, push back of the stones remains the most challenging cause of failure. In our study, to minimize fragment migration a lot of tips and trick were applied. URS was placed over 4 Fr ureter catheter instead of guide wire, thus pushing the stone by irrigation flow is minimized. Slowly moving inside the ureter and sometime closing irrigation completely thus avoids the pushing force of irrigation. Using a thick probe of 3.6 Fr for stone fragmentation may reduce the pushing force of the water; reducing the frequency of the shock waves may also help in minimizing the risk of stone migration. If the stone is about to escape to the renal pelvis or has started moving up, then we catch the stone in the basket and fragment the stone by 2 Fr probe through the same working channel. It is helpful to consult an anaesthesiologist to control patients’ respiratory movement during stone fragmentations, especially in the upper third stone and renal stones. This will increase the efficacy of the pneumatic fragmentation and decrease the risk of ureter perforation and avoid bleeding from the ureter wall, thus helping to reduce the overall operating time. Some authors reported that using warm saline irrigation in endoscopic surgeries results in better surgical outcomes, including a lower ureteral spasm rate, greater ureteral muscle relaxation and better access to the upper ureteral zone, and a lower rate of complications, such as ureteroscope impaction, ureteral dislodge and stone retropulsion.11 During our daily practice, although we use these tips and tricks, sometimes we found ourselves in need of using laser energy instead of PL, especially when the stone is hard and resistant to PL.
We have no ureteral perforation; however, 2% to 4% of ureter wall perforation was reported either with laser or pneumatic energy.3 In our study, we had three stone migrations (3.2%) and 2 of them had an upper ureter stone and both of them had hydronephrosis and the stone volume was less than 1 cm thus increasing the risk of migration. In both cases the stone was pushed back not through fragmentation but before we started fragmentation. Therefore, we do recommend decreasing the force of irrigation flow by the above mentioned tricks to avoid stone migration. The cost-effectiveness of anti-retropulsion devices used during ureteroscopic lithotripsy is an important consideration; however, using the tips and tricks may result in reduction of stone migration to the same level without any financial cost to the patient.12 Ursiny et al concluded that it is cost-effective to use an anti-retropulsion device at a retropulsion rate of greater than 6.3%.12 The authors estimated costs of secondary procedures needed to treat retropulsed stones as $5290 for shock wave lithotripsy and $6390 for ureteroscopy. Average device cost was $278. Thus, the average additional cost of ureteroscopic lithotripsy with versus without an anti-migration device would be $384 versus $952.12
Eight patients had failed procedures; 5 of them had a lower ureter stone and the cause was narrow ureter with small size of the stone. A lot of tips and tricks were used to overcome the narrow ureter. If the passage is obstructed at the level of ureter orifice, we rotate the semi-rigid ureteroscope 180 degrees, enabling the peak of the scope to pass through ureter orifice more easily. If we are still unable to pass the orifice, then we stent the ureter and repeat the procedure in approximately 2–3 weeks. During our daily practice, we do expect narrow ureter in any patient with small size stone (less than 5 mm) without spontaneous passage for a week or more. In such cases, DJS will be placed for 2–3 weeks then removal of DJS and stone extraction are performed at the same time. Some authors do extensive balloon dilatation to pass a tight ureter but risk of trauma and long-term ureter stricture formation should be considered.13
We recommend not forcing ureteroscope to pass the ureter because perforation or avulsion of the ureter as well as severe postoperative pain may occur. In such cases we believe that using low-caliber URS (6/7.5Fr) may help in passing the narrow ureter. In literature the incidence of anatomic abnormalities, a narrow ureteric lumen, tortuous ureteric path was found to be 8% in a tertiary referral unit and this should be considered and indeed discussed with patients when obtaining pre-operative consent, especially for purely elective, non-urgent, cases.13 In such cases the operation can be converted to flexible URS; however, sometimes it is not easy to access the virgin ureter with flexible URS. Moreover, the cost of flexible URS is much higher when compared to semi-rigid URS and this tool can easily malfunction. The cost of flexible URS has been reported to be $1116 for each patient with the use of additional equipment.14 Semi-rigid URS means wider working channels and better images obtained using high irrigation. Flexible URS can be difficult to manipulate and insert into the ureter orifice with smaller optic diameters and working channels and longer operation times.15 However recently, following the introduction of disposable flexible URS and highly effective laser machine for stone fragmentation, flexible URS started to replace semi-rigid URS in definite cases of upper ureter stone, although the primary indication of flexible URS is moderate size kidney pelvis or lower pole stone. In developing countries, financial considerations and the cost-effectiveness of procedures do limit the available equipment; thus, mastering semi-rigid URS in the management of ureter stone is of great value. When placing the stent, if we find difficulty with bucking at the ureter orifice, bring the cystoscope closer to the ureter orifice and push slowly under vision. If the stent is not moving, check the wire placement in the collecting system because the excess wire in the renal end can equally hamper progress; by pulling back the wire slightly under fluoroscopy monitoring, the stent can then be advanced. It is important to not leave the distal end too short because migration into the ureter may occur. We usually perform URS and place the stent without fluoroscopy. In one of the recent systematic reviews and meta-analysese in the literature where fluoroless and conventional URS were compared, the authors concluded that fluoroless URS is equally safe and effective, with zero radiation exposure.16 However, it needs to be cautiously conducted in selected patients and fluoroscopy equipment should always be available intraoperatively.16 In our study we placed the guide wire using a ureteroscope and inserted the stent slowly by keeping the guide wire straight by applying minimal tension; then, we advanced the pusher to continue advancing the stent until it approximately reached the prostatic urethral or ureter orifice; then, we inserted the ureteroscopy beside the pusher and continued pushing the pusher and the stent under vision of ureterorenoscope until the end of the stent was seen near to ureter orifice; then, we pulled out the guide wire and the pusher, respectively.
All preoperative parameters (Table 2) for patients with upper or lower ureter stones were homogenous and success rates were similar for both groups. These findings do confirm the benefit of the tips and tricks in improving success in the endoscopic management of upper ureter stones.17 In the literature, success rates in the management of upper ureter stones using PL are 86% and 97%, respectively, when using laser energy.3
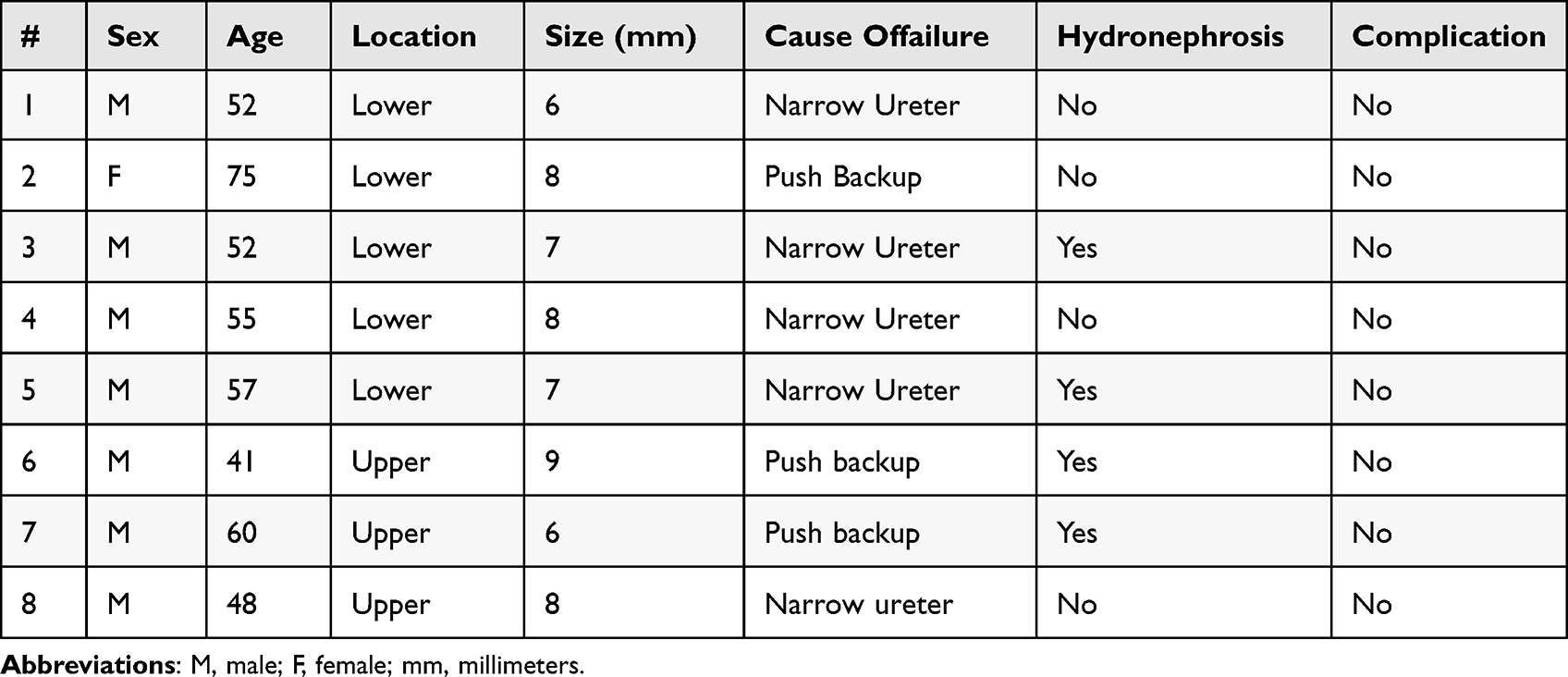 |
Table 2 Characteristics of Patients with Failed Ureterorenoscopy |
In our study group there were no intraoperative complications. In the literature, the complication rate following stone fragmentation with URS appears to be less than 5%; the most frequently seen major complications were ureteral perforation and avulsion and development of ureteral stenosis in the long term3 Some serious but rare complications were reported after URS with LL but not with PL, like subcapsular renal hematoma (0.36%) and retroperitoneal hemorrhage.18–20 In patients with known and uncorrected bleeding, diathesis small caliber of URS with LL is safer and more effective for treating upper urinary tract calculi.
We believe that hand experience may be one of the most common reasons behind the low rates of intraoperative complications. In our study, postoperative complications occurred only in 4 patients (4.4%); all of these complications were managed with appropriate medical therapy. Only one patient had urosepsis (1.1%), who needed admission for IV medical therapy. Infection is one of the most common postoperative complications (2–4%); this may be due to nature of the operation and the use of multi-instruments like camera, guide wire and endoscopies. Multivariate analysis was done and there was no relationship between the results of surgery and location; side, age and size of ureteric stones were not significant (p-value=0.63, 0.63, 0.45, 0.08, respectively). We postulate that primary stone size, side, age and location have no effect on the result of surgery.
It should be noted that this paper was uploaded to the DSpace software of An-Najah National University repository as a thesis on 26th May 2016.21
Conclusions
Pneumatic ureteroscopy in the management of ureter stones is a safe and feasible treatment option for upper and lower stones. The tips and tricks in ureterorenoscopy do improve the success rate of URS, especially for upper ureter stones. Patients with longstanding small ureter stones and lower ureter stones may have narrow ureters, and ureter stent placing is thus the best option for such cases. Location of the stone seems not to have an important impact on the success rate of the endoscopic management. Further studies with a larger number of patients should be conducted to confirm our findings.
Ethical Approval
Data was extracted from medical records. The study was approved by An-Najah National University institutional review board (IRB) ethics committee. All procedures performed in the study involving human participants were in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The administrative approval was obtained from the hospital administration.
Consent to Publication
None of the participants was from a vulnerable population. In Table 2, all cases or next of kin provided written voluntary informed consent for the data presented regarding the characteristics of participants with failed ureterorenoscopy.
Acknowledgments
The authors would like to thank An-Najah National University Hospital and University for the permission to conduct this study.
Disclosure
The authors declare that they have no conflicts of interest in this work. The abstract of this paper was presented at the 26th Turkish International Urology Meeting 2017, as an abstract presentation with interim findings. The poster’s abstract was published in ‘Poster Abstracts’ in 26th Turkish international Urology Meeting 2017, for viewing on-site only [https://staff.najah.edu/en/publications/8543/]. Furthermore, this paper was uploaded to the DSpace software of An-Najah National University repository as a thesis on 26th May 2016 [https://hdl.handle.net/20.500.11888/15120].
References
1. Yuksel OH, Akan S, Urkmez A, Uruc F, Verit A. Efficacy and safety of semirigid ureteroscopy combined with holmium: YAG laser in the treatment of upper urinary tract calculi: is it a good alternative treatment option of flexible ureteroscopy for developing countries? J Pak Med Assoc. 2015;65(11):1193–1196.
2. Kronenberg P, Traxer O. Update on lasers in urology 2014: current assessment on holmium: yttrium-aluminum-garnet (Ho: YAG)laser lithotripter settings and laser. World J Urol. 2015;33:463–469. doi:10.1007/s00345-014-1395-1
3. Kızılay F, Kalemci S, Turna B, Şimşir A, Nazlı O. Laser versus pneumatic lithotripsy for management of pediatric ureteral stones: a prospective-comparative analysis with adults.J. Pediatr Urol. 2020;16:35. doi:10.1016/j.jpurol.2019.11.006
4. Zhang J, Shi Q, Wang GZ, Wang F, Jiang N. Cost-effectiveness analysis of ureteroscopic laser lithotripsy and shock wave lithotripsy in the management of ureteral calculi in eastern China. Urol Int. 2011;86:470–475. doi:10.1159/000324479
5. Drake T, Grivas N, Dabestani S, Knoll T, Lam T. What are the Benefits and Harms of Ureteroscopy Compared with Shock-wave Lithotripsy in the Treatment of Upper Ureteral Stones? A Systematic Review. Eur Urol. 2017;72:772–786. doi:10.1016/j.eururo.2017.04.016
6. Yang C, Li S, Cui Y. Comparison of YAG Laser Lithotripsy and Extracorporeal Shock Wave Lithotripsy in Treatment of Ureteral Calculi: a Meta-Analysis. Urol Int. 2017;98:373–381. doi:10.1159/000452610
7. Wu CF, Shee JJ, Lin WY, Lin CL, Chen CS. Comparison between extracorporeal shock wave lithotripsy and semirigid ureterorenoscope with holmium: yAGlaser lithotripsy for treating large proximal ureteral stones. J Urol. 2004;172:1899. doi:10.1097/01.ju.0000142848.43880.b3
8. Kijvikai K, Haleblian GE. Shock wave lithotripsy or ureteroscopy for the management of proximal ureteral calculi: an old discussion revisited. J Urol. 2007;178:1157–1163. doi:10.1016/j.juro.2007.05.132
9. Sen H, Bayrak O, Erturhan S, et al. Comparing of different methods for prevention stone migration during ureteroscopic lithotripsy. Urol Int. 2014;92:334–338. doi:10.1159/000351002
10. Sanguedolce F, Montanari E, Alvarez-Maestro M, Macchione N, Hruby S. Use of XenX™, the latest ureteric occlusion device with guide wire utility: results from a prospective. multicentric comparative study. World J Urol. 2016;34:1583–1589. doi:10.1007/s00345-016-1806-6
11. Mohammadzadeh Rezaei MA, Akhavan Rezayat A, Tavakoli M, Jarahi L. Evaluation the result of warm normal saline irrigation in ureteral endoscopic surgeries. Urol J. 2018;3:83–86. doi:10.22037/uj.v15i4.4682
12. Ursiny M, Eisner BH. Cost-effectiveness of anti-retropulsion devices for ureteroscopic lithotripsy. J Urol. 2013;189:1762–1766. doi:10.1016/j.juro.2012.11.085
13. Cetti RJ, Biers S, Keoghane SR. The difficult ureter: what is the incidence of pre-stenting? Of pre-stenting? Ann R Coll Surg Engl. 2011;93:31–33. doi:10.1308/003588411X12851639106990
14. Gurbuz C, Atış G, Arikan O, et al. The cost analysis of flexible ureteroscopic lithotripsy in 302 cases. Urolithiasis. 2014;42(2):155–158. doi:10.1007/s00240-013-0628-x
15. Miernik A, Schoenthaler M, Wilhelm K, Wetterauer U, Zyczkowski M, Paradysz A. Combined semirigid and flexible ureterorenoscopy via a large ureteral access sheath for kidney stones >2 cm: a bicentric prospective assessment. World J Urol. 2014;32(3):697–702. doi:10.1007/s00345-013-1126-z
16. Peng L, Wang W, Gao X, Di X, Luo D. Fluoroless versus conventional ureteroscopy for urinary stones: a systematic review. Minerva Urol Nephrol. 2021:1:73. doi: 10.23736/s2724-6051.20.04042-4
17. Garg S, Mandal AK, Singh SK, et al. Ureteroscopic laser lithotripsy versus ballistic lithotripsy for treatment of ureteric stones: a prospective comparative study. Urol Int. 2009;82:341–345. doi:10.1159/000209369
18. Tao W, Cai CJ, Sun CY, Xue BX, Shan YX. Subcapsular renal hematoma after ureteroscopy with holmium: yttrium-aluminum-garnetlaser lithotripsy. Lasers Med Sci. 2015;30:1527–1532. doi:10.1007/s10103-015-1760-3
19. Chiu PK, Chan CK, Ma WK, To KC, Cheung FK, Yiu MK. Subcapsular hematoma after ureteroscopy and laser lithotripsy. J Endourol. 2013;27:1115–1119. doi:10.1089/end.2013.0128
20. Chouhan JD, Zhao HH, Magee B, McNeil BK. Retroperitoneal hemorrhage after ureteroscopy without laser lithotripsy: an extreme example of an underreported event?Can. J Urol. 2016;23:8324–8328.
21. DSpace software of an-najah national university repository; 2016. Available from: https://hdl.handle.net/20.500.11888/15120.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.