Back to Journals » Journal of Asthma and Allergy » Volume 16
Endobronchial Ultrasound is Useful in the Assessment of Bronchial Wall Changes Related to Bronchial Thermoplasty
Authors Soja J ![]() , Górka K, Gross-Sondej I, Jakieła B
, Górka K, Gross-Sondej I, Jakieła B ![]() , Mikrut S, Okoń K, Ćmiel A, Sadowski P
, Mikrut S, Okoń K, Ćmiel A, Sadowski P ![]() , Szczeklik W
, Szczeklik W ![]() , Andrychiewicz A, Stachura T, Bochenek G, Bazan-Socha S, Sładek K
, Andrychiewicz A, Stachura T, Bochenek G, Bazan-Socha S, Sładek K
Received 10 January 2023
Accepted for publication 7 April 2023
Published 1 June 2023 Volume 2023:16 Pages 585—595
DOI https://doi.org/10.2147/JAA.S404254
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Jerzy Soja,1,2 Karolina Górka,1,2 Iwona Gross-Sondej,1,2 Bogdan Jakieła,2 Sławomir Mikrut,3 Krzysztof Okoń,4 Adam Ćmiel,5 Piotr Sadowski,4 Wojciech Szczeklik,6 Anna Andrychiewicz,7 Tomasz Stachura,1,2 Grażyna Bochenek,1,2 Stanisława Bazan-Socha,2 Krzysztof Sładek1,2
1Department of Pulmonology and Allergology, University Hospital, Kraków, Poland; 2 2nd Department of Internal Medicine, Jagiellonian University Medical College, Kraków, Poland; 3Faculty of Mining, Surveying and Environmental Engineering, AGH University of Science and Technology, Kraków, Poland; 4Department of Pathology, Jagiellonian University Medical College, Kraków, Poland; 5Department of Applied Mathematics, AGH University of Science and Technology, Kraków, Poland; 6Centre for Intensive Care and Perioperative Medicine, Jagiellonian University Medical College, Kraków, Poland; 7Department of Endoscopy, University Hospital, Kraków, Poland
Correspondence: Jerzy Soja, Department of Internal Medicine, Faculty of Medicine, Jagiellonian University Medical College, Jakubowskiego 2, Krakow, 30-688, Poland, Email [email protected]
Background: Bronchial thermoplasty (BT) is an interventional endoscopic treatment for severe asthma leading to the clinical improvement, but morphologic changes of bronchial wall related to the procedure and predictors of a favorable response to BT remain uncertain. The aim of the study was to validate an endobronchial ultrasound (EBUS) in assessing the effectiveness of BT treatment.
Methods: Patients with severe asthma who met the clinical criteria for BT were included. In all patients clinical data, ACT and AQLQ questionnaires, laboratory tests, pulmonary function tests and bronchoscopy with radial probe EBUS and bronchial biopsies were collected. BT was performed in patients with the thickest bronchial wall L2 layer representing ASM. These patients were evaluated before and after 12 months of follow-up. The relationship between baseline parameters and clinical response was explored.
Results: Forty patients with severe asthma were enrolled to the study. All 11 patients qualified to BT successfully completed the 3 sessions of bronchoscopy. BT improved asthma control (P=0.006), quality of life (P=0.028) and decreased exacerbation rate (P=0.005). Eight of the 11 patients (72.7%) showed a clinically meaningful improvement. BT also led to a significant decrease in the thicknesses of bronchial wall layers in EBUS (L1 decreased from 0.183 to 0.173 mm, P=0.003; L2 from 0.207 to 0.185 mm, P = 0.003; and L3– 5 from 0.969 to 0.886 mm, P=0.003). Median ASM mass decreased by 61.8% (P=0.002). However, there was no association between baseline patient characteristics and the magnitude of clinical improvement after BT.
Conclusion: BT was associated with a significant decrease in the thickness of the bronchial wall layers measured by EBUS including L2 layer representing ASM and ASM mass reduction in bronchial biopsy. EBUS can assess bronchial structural changes related to BT; however, it did not predict the favorable clinical response to therapy.
Keywords: airway remodeling, airway smooth muscle, bronchial thermoplasty, bronchial wall layers, endobronchial ultrasound
Introduction
Asthma is a heterogeneous chronic inflammatory disease of the airways characterized by airway hyperreactivity and variable degree of bronchial obstruction. Up to 10% of all asthma patients have a severe or uncontrolled disease associated with an increased mortality rate, a higher number of hospitalizations and increased healthcare costs.1–3 In recent years, due to the identification of various phenotypes of severe asthma, it has been possible to implement innovative therapies, such as monoclonal antibodies targeting specific inflammatory pathways, which have shown considerable therapeutic efficacy.4,5
Bronchial thermoplasty (BT) is an endoscopic non-pharmacological treatment for severe asthma that reduces airway smooth muscle (ASM) mass by thermal ablation.6–8 Increased ASM mass is associated with airway hyperresponsiveness and has been regarded as a characteristic feature of severe asthma.9–11 Several randomized trials have proven that BT is a safe and effective method for reducing asthma exacerbations and improving asthma control and quality of life.12–14 However, the mechanism of action of BT is not fully understood. Previous studies have shown that BT reduces ASM layer, but also affects the function of airway nerves, epithelial cells, glands, inflammatory cells, and even components of the extracellular matrix.15–17 In addition to histopathological examination of bronchial biopsies, imaging methods, such as computed tomography (CT)18,19 or optical coherence tomography,20–22 have been implemented to assess asthma remodeling after BT. Still, these methods are rarely used or validated in relatively small study groups.
Several studies demonstrated that EBUS enables a reliable assessment of bronchial wall layers.23–25 As previously reported, a considerable consistency between the bronchial wall thickness measured by EBUS and high-resolution CT was documented.23,26 Soja et al23 also showed that the thickness of the bronchial wall and its layers were significantly greater in asthmatic patients compared to control subjects. According to a thorough review of the available literature, EBUS has not been used so far to evaluate the effectiveness of BT treatment. Therefore, the present study aimed to assess EBUS efficacy in identifying patients with increased smooth muscle thickness in whom we evaluated the clinical asthma course and airway structural changes in 1-year follow-up.
Methods
Patients and the Study Protocol
This prospective follow-up study included 40 patients with severe asthma, who were enrolled at the university hospital. All asthma patients met the qualifying criteria for BT.27 The diagnosis of asthma was consistent with the criteria of the Global Initiative for Asthma report. None of the patients were treated with biological therapies.
Before BT, all subjects underwent assessment of laboratory tests including blood eosinophilia and serum immunoglobulin E (IgE), spirometry (FEV1 and FVC) before and after administration of a short-acting β2-agonist to assess bronchial reversibility (Jaeger Master Screen, Höchberg, Germany), Asthma Control Test (ACT) and Asthma Quality of Life Questionnaire (AQLQ) and number of exacerbations and hospitalizations for asthma. In all patients, bronchoscopy with radial probe EBUS and bronchial biopsies were performed. The severity of the disease and the control of symptoms were evaluated using the Asthma Control Test (ACT) and Asthma Quality of Life Questionnaire (AQLQ).
Clinical response to BT treatment was assessed using ACT and AQLQ questionnaires. An improvement of ≥3 points on ACT or ≥0.5 points on AQLQ scores was considered as clinically relevant. Association between baseline patient characteristics (clinical parameters, bronchial layer thickness in EBUS, and histology) and the magnitude of clinical improvement after BT was assessed.
To select the best candidates for the BT procedure (ie, with the most advanced structural changes of the airway), we performed a bronchoscopy with EBUS and bronchial biopsy sampling. Based on EBUS measurements, we identified patients with the thickest L2 layer who were selected and qualified for bronchial thermoplasty. These patients were evaluated prior to BT and after 12 months of follow-up. The study protocol followed the Declaration of Helsinki and its amendments and was approved by the Ethics Committee of the Jagiellonian University Medical College on June 25, 2015 (KBET 122.6120.167.2015). All study participants gave written informed consent.
Bronchoscopy and Endobronchial Ultrasonography (EBUS)
Bronchoscopy was performed according to the ATS guidelines28 under local anesthesia (2% lidocaine) and conscious sedation (0.05–0.1 mg intravenous fentanyl and 2.5–5.0 mg intravenous midazolam) using the BF-190 fiberscope (Olympus, Tokyo, Japan). EBUS was performed using 20MHz ultrasound radial probes with flexible catheters having a balloon at the tip (Olympus, Tokyo, Japan) that cooperates with the EU-ME1 processor (Olympus, Tokyo, Japan). The probe was introduced through the working channel of the fiberscope into the segmental bronchi of the right lower lobe: superior (RB6), anterior basal (RB8), lateral basal (RB9), and posterior basal (RB10). EBUS allows differentiation of five layers of the bronchial wall. The inner layers of the bronchial wall, layer 1 (L1, representing the epithelium and part of submucosa) and layer 2 (L2, representing smooth muscles and part of submucosa), were analyzed separately. In contrast, the outer layers, 3, 4, and 5 (L3–5, representing cartilage), were measured together (Figure 1a). Layers L1, L2, and L3–5 represent the entire thickness of the bronchial wall. The ultrasound probe was placed into the same parts of the investigated segmental bronchi. To optimize the measurement of bronchial layer thickness, EBUS images were analyzed using the Feature Extraction Software (FES) developed at the University of Science and Technology in Kraków.
 |
Figure 1 Decreased thickness of airway wall layers after BT as measured by endobronchial ultrasonography (EBUS). Notes: (a) Representative EBUS image of the bronchus RB10 and the schematic outline of bronchial wall layers with major structural components highlighted. (b) The thickness of L1, L2 and L3–5 layers in asthma patients before BT and 12 months after the procedure. Data shown as medians and quartiles (n = 11; 2-sided exact Wilcoxon matched-pairs signed rank test). |
The images selected from the video recorded during bronchoscopy were saved as bitmaps and were imported to the FES software for further analysis. From the digital film sequences recorded during bronchoscopy, five frames were selected from each segmental bronchi in which the multilayered structure of the bronchial wall was clearly visible. The FES software was designed to process images, including converting data from the raster to vector format using the subpixel precision method. The borders of the individual layers were pointed manually by a researcher, blinded to the patient record and the sample status. The distance between the two points was then measured and converted into millimeters using FES software. From five measurements from each layer, the mean was calculated and used in the statistical analysis. For a better interpretation of the results, the vector data are superimposed on a raster layer. The width of the layers is measured to three decimal places (to the micrometer).
Bronchial Thermoplasty
BT was performed using the AlairTM Bronchial Thermoplasty System (Boston Scientific, Natick, MA, USA) under general anesthesia (propofol) with the laryngeal mask airway. A single-use catheter with a basket carrying four expandable electrodes was inserted into the bronchial tree. Using radiofrequency waves, thermal energy was supplied to the 3–10 mm diameter bronchi to induce ablations of short 5 millimeter sections. BT was applied in three sessions separated by three-week intervals. In the first session, the right lower lobe was treated, then the left lower lobe, and in the last session, both upper lobes. Patients received 50 mg of prednisone for 3 days before BT, on the day of the procedure, and 1 day after BT. BT was carried out in accordance with applicable guidelines.27
Bronchial Biopsy Histology
Bronchial biopsies were obtained from the segmental airway carinas of the right lower lobe for histological studies. During bronchoscopy 6 biopsies were taken using forceps FB-231D. Bronchial biopsy specimens were collected before and 12 months after BT procedure. The tissue was fixed in 10% buffered formalin, routinely processed, and embedded in paraffin. The 3 µm sections were stained with hematoxylin-eosin and immunohistochemically using antibodies detecting: dendritic cells (CD1a; clone NCL-L-CD1a-235; Leica Biosystems, Wetzlar, Germany), T-cells (CD3; 103R-95; Merck, Darmstadt, Germany), CD4+ T-cells (CD4; MS-1528-S; Thermo Fisher Scientific, Waltham, MA, USA), CD8+ T-cells (CD8; M7103; Dako Denmark A/S, Glostrup, Denmark), B-cells (CD20; M0755; Dako), NK-cells (CD56; 156R-96; Merck), eosinophils (eosinophil cationic protein [ECP]; PA5-79927; Invitrogen, Waltham, MA, USA), neutrophils (neutrophil elastase [NE]; M0752; Dako), mast cells (tryptase; NCL-MCTRYP; Leica Biosystems), epithelial goblet cells (MUC5AC; sc-33667; Santa Cruz Biotechnology, Dallas, TX, USA), and alpha-smooth muscle actin (α-SMA; M0851; Dako). The analysis of the specimens was performed by two experienced pathologists blinded to the clinical data. The expression of CD1a, CD3, CD4, CD8, CD20, CD56, tryptase, ECP, and NE was evaluated at 400x magnification consecutively in five fields of view, and in the case of smaller sections, in all available fields. The results were expressed as the ratio of the number of positive cells to the number of visual fields examined. The number of goblet cells was expressed as the percentage of epithelial cells positive for MUC5AC. The Olympus SC 180 camera (Olympus, Tokyo, Japan) and the Olympus cellSens Standard 2.3 software were used to evaluate the expression α-SMA. Smooth muscle surface area measurements were made at 40x magnification and were expressed as the ratio of α-SMA positive area to the area of the entire section. The thickness of the reticular basement membrane (RBM) was measured as previously described.23
Statistical Analysis
Data were analyzed using Statistica 13.1 software package (TIBCO Software, Palo Alto, CA, USA) and GraphPad Prism 9.4.0 (GraphPad Software, San Diego, CA, USA). Summary statistics were expressed as medians (25th and 75th percentiles). Due to the small sample size, exact Wilcoxon matched-pairs signed rank test was used to compare data before and after BT. For significant differences, the Hodges-Lehmann estimator of median of differences with 95% CI was also calculated to estimate shift parameter. The correlations between variables were calculated using the Spearman rank order correlation. The level of significance was set at P<0.05.
Results
Forty patients with severe asthma were enrolled to the study. Eleven patients with the thickest bronchial wall L2 layer representing ASM in EBUS were qualified for BT treatment. The study group consisted of 4 women and 7 men, the median age was 50 (range: 44–55) years, body mass index 25.1 (range: 21.9–28.2) kg/m2. The median duration of asthma was 16 (5–30) years.
All these patients successfully completed the 3 sessions of BT. A mean of 41.9 ± 8.05 radiofrequency activations was delivered to the right lower lobe, 43.5 ± 10.63 to the left lower lobe and 68.1 ± 12.33 to both upper lobes. BT was generally well tolerated. There were no cases of pneumothorax nor airway haemorrhage. Side-effects include asthma exacerbation (3%), chest pain (6%), atelectasis (6%) and dyspnoe (18%).
During bronchoscopy 6 biopsies from the segmental airway carinas of the right lower lobe (B8-B9, B9-B10, B6) were taken from one patient using biopsy forceps FB-231D. Bronchial biopsy specimens were collected before and 12 months after BT procedure.
Improvement in Asthma Control After Bronchial Thermoplasty
As shown in Table 1, BT significantly improved asthma control, as evidenced by an increase in the ACT score from a median of 15 points before BT to 18 at 12-month follow-up (P=0.006). Similarly, the quality of life related to asthma measured by the AQLQ improved from median 4.2 points before BT to 5.6 after BT (P=0.028). Eight of the 11 patients (72.2%) showed a clinically meaningful improvement of ACT and AQLQ questionnaires. Moreover, the median number of asthma exacerbations decreased from 6 in the year preceding BT to 1 after the treatment (P=0.005). The same trend applied to the exacerbations that required hospitalization with a median of 1 (1–5) per year before BT and none during follow-up (P=0.018). Similarly, the quality of life related to asthma measured by the AQLQ improved from median 4.2 points before BT to 5.6 after BT (P=0.028). We also noticed a marginal improvement in FEV1/FVC after BT from a median of 61% to 66% (P = 0.041); however, other measures of lung function did not change considerably (see details in Table 1).
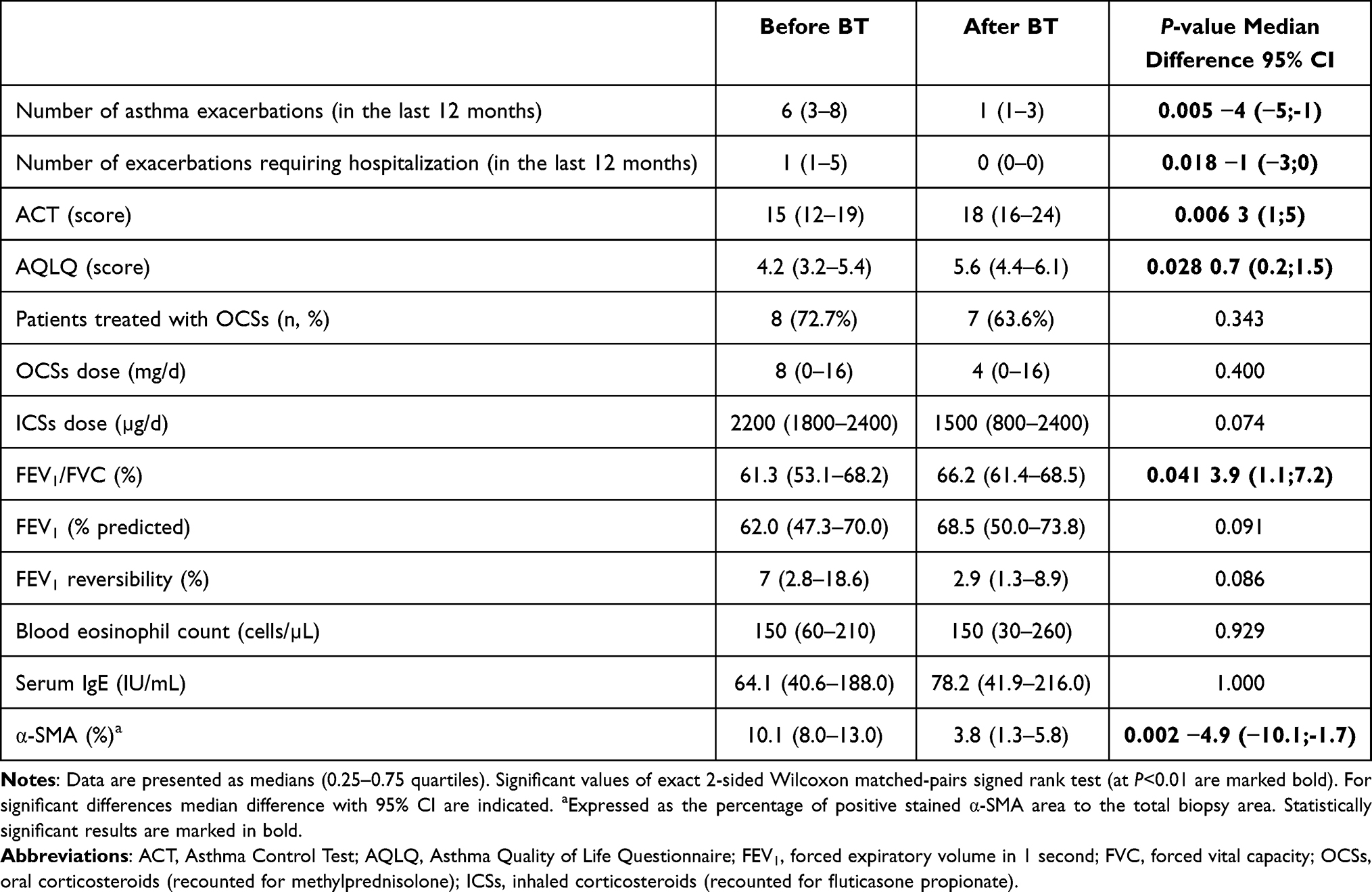 |
Table 1 Clinical Characteristics of Patients Before and After BT |
Decrease in the Thickness of Bronchial Wall Layers After Bronchial Thermoplasty
Treatment with BT led to a significant decrease in the thickness of bronchial walls and their layers as measured by EBUS (Figure 1b). Median thickness of L1 decreased from 0.183 (0.180–0.190) mm before BT to 0.173 (0.169–0.175) mm after BT (P=0.003). Similarly, L2 decreased from 0.207 (0.201–0.213) mm to 0.185 (0182–0.194) mm (P=0.003), while L3–5 from 0.969 (0.951–1.019) mm to 0.886 (0.853–0.890) mm (P=0.003). The thickness of combined L1 + L2 + L3–5 decreased from 1.363 (1.343–1.399) mm before BT to 1.240 (1.221–1.262) mm after BT (P=0.003).
Surprisingly, the decrease in the bronchial wall thicknesses and their layers did not correlate with the ACT or AQLQ score improvements (Table 2). It was also unrelated to the decrease in the exacerbation rate or the spirometry changes. Similarly, improvement in asthma control and asthma-related quality of life did not correlate with baseline thicknesses of the bronchial walls and their layers (data not shown).
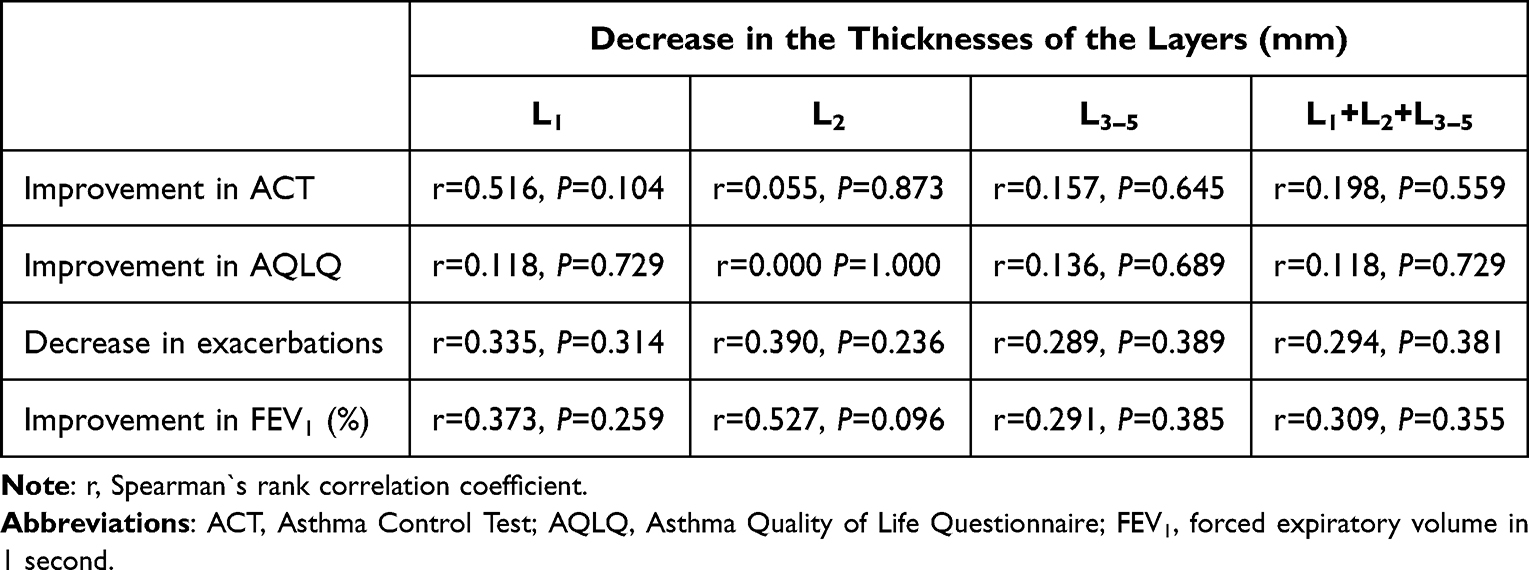 |
Table 2 Correlation Between the Decrease in Thickness of Bronchial Layers and Other Parameters |
Reduced Airway Smooth Muscle Mass After Bronchial Thermoplasty
Next, we analyzed BT-related changes in ASM mass and inflammatory cell composition in bronchial biopsy histology. In line with the EBUS data, BT resulted in a significant decrease in ASM mass (Figure 2a and b, Table 3), from the median of 10.1% at baseline to 3.8% at 12-month follow-up (P=0.002). On the contrary, there were no changes in the RBM thickness (median 6.7 vs 6.6 µm, P=0.206) (Figure 2c) or the abundance of MUC5AC-expressing epithelial cells (median 21.2 vs 20.7%) (Table 3). We also did not show any differences in the expression of immune cell markers before and after BT (Table 3).
 |
Table 3 Histological Analysis of Bronchial Biopsies Before and After BT |
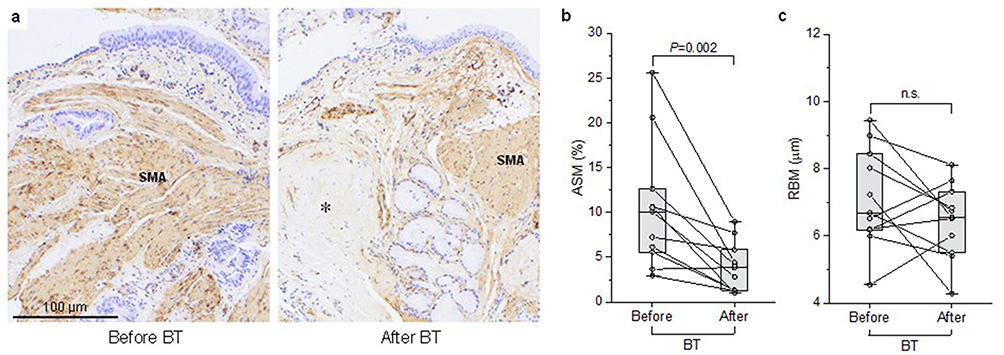 |
Figure 2 Bronchial wall histology changes related to BT. Notes: (a) Representative histological images of bronchial biopsy samples showing reduction in airway smooth muscle (ASM) after BT at 12 months follow-up. α-SMA staining, hematoxylin-eosin counterstain; 100x magnification. Asterisk indicates fibrous connective tissue. (b) Reduction in the ASM (expressed as the percentage of cross-section surface area) before and after BT. (c) No change in the thickness of reticular basement membrane (RBM) after BT. Data shown as medians and quartiles (n = 11; 2-sided exact Wilcoxon matched-pairs signed rank test). |
The reduction in ASM related to BT also did not correlate with ACT or AQLQ improvement (r = 0.161 P = 0.636 and r = 0.209 P = 0.537, respectively). Similarly, reported clinical improvement was not associated with baseline ASM mass, RBM thickness, or the number of immune cells in bronchial biopsy (data not shown).
Discussion
To our knowledge, this is the first study worldwide which evaluates the effect of BT treatment using radial probe EBUS. Our study shows that BT led to a significant decrease in the thicknesses of bronchial wall layers in EBUS including L2 layer representing ASM. The median ASM mass in histological examination of bronchial biopsies decreased by 61.8%. There was no association between clinical parameters, bronchial layer thickness in EBUS, and histology and the clinical improvement after BT. Our results suggest that EBUS can assess bronchial structural changes related to BT; however, it did not predict the favorable clinical response to therapy.
BT is recognized as a therapeutic option in patients with severe refractory asthma. However, broad inclusion criteria that do not include evaluation of the bronchial remodeling make it challenging to qualify patients for this procedure, especially when availability of this therapeutic option is limited. Therefore, in the present study, we sought to determine whether the assessment of bronchial wall layers by EBUS could identify asthma patients with increased smooth muscle thickness who may potentially benefit more from the BT procedure. Next, we evaluated the effectiveness of BT in this cohort by analyzing clinical data, lung function, and various measures of airway remodeling before the procedure and at 1-year follow-up.
Structural changes in the bronchial wall can be assessed directly by histopathological examination of biopsy samples and indirectly by various imaging methods, such as chest CT,29,30 OCT,31,32 or EBUS.23–26 Of these, only EBUS and OCT are sensitive enough to differentiate and measure five layers of the bronchial wall, including the L2 layer, which contains smooth muscle. Previously, EBUS has been used successfully in assessing airway remodeling in asthmatic patients by many researchers.23–26 However, only a few studies simultaneously evaluated the ASM layer in imaging methods and bronchial biopsies. For example, the experimental research conducted on horses by Bullone et al33 proved that EBUS enables a precise assessment of smooth muscle. Our study used EBUS as the principal imaging technique to identify severe asthma patients with more advanced bronchial remodeling. To achieve this, we enrolled 40 patients with severe asthma who met the clinical criteria for BT. In these patients, we performed EBUS and identified eleven subjects with the thickest L2 layer who were next qualified for the BT procedure. As expected, compared to baseline, there was a significant decrease in the thickness of the bronchial wall layers after BT. In particular, we showed a significant reduction (~10% on average) in the thickness of L2, representing the ASM layer. These changes were accompanied by a substantial drop in ASM mass determined by histological examination of bronchial wall biopsies. Thus, our data suggest that EBUS imaging could be used effectively to assess the outcome of BT treatment. Previous studies, which implemented different imaging techniques, revealed similar changes in the bronchial wall after BT. For example, a small study by Ya et al34 showed a decrease in the total thickness of the bronchial wall assessed by EBUS in two patients with severe asthma subjected to BT. Similarly, Zanon et al,18 in a group of 26 patients with severe asthma, noted ~25% reduction in the median thickness of the airway wall after the BT procedure, as evidenced by CT imaging. Furthermore, in 17 patients with severe asthma treated with BT, Konietzke et al19 observed a decrease in bronchial wall thickness determined by quantitative CT using a combined analysis of the 2nd-7th generation of the airways. Another case report demonstrated a significant long-term reduction in bronchial wall thickness measured by OCT in an asthma patient who clinically responded well to BT therapy.20 These results, together with our data, indicate that non-invasive imaging methods may be useful in assessing response to BT treatment.
Interestingly, after BT therapy, we noted a significant ~60% decrease in ASM mass in the bronchial biopsy histology, which is consistent with the results described by other investigators. Initial data describing a post-BT decrease in ASM mass originated from animal studies, which also showed a concomitant decrease in bronchial hyperreactivity.35 Pioneering research in patients qualified for lung resection showed that BT performed 3 weeks before surgery resulted in a significant reduction in ASM mass.36 Subsequent studies confirmed the decrease in ASM mass after BT in asthma patients.15–17,37–39 The analysis of the data pooled for 99 severe asthmatic patients undergoing BT treatment in 7 centers showed a significant reduction in ASM mass from 16.1% to 4.4% in 6 weeks, which remained unchanged after one year.40
In addition to the ASM mass, we also evaluated other structural changes in bronchial mucosa specimens, such as goblet cell metaplasia, RBM thickness, and inflammatory cell influx. It turned out that the number of inflammatory cells in the bronchial biopsy specimens, including eosinophils, neutrophils, and mast cells, was similar at baseline and after BT. This is consistent with data published by Pretolani et al37 and Papakonstantinou et al,38 who did not observe significant changes in the number of eosinophils, neutrophils, and lymphocytes up to 3 months post-BT. These data suggest that clinical improvement following BT is not associated with short- and long-term changes in the inflammatory pattern in the bronchial wall. Furthermore, in the current study, we did not detect any significant difference in the number of goblet cells in the bronchial mucosa. These results align with those obtained by Jendzjowsky et al39 and the ASMATHERM study,37 which did not show goblet cell hyperplasia or any changes in the subepithelial mucous glands one year after BT. However, they are inconsistent with those reported by Salem et al,41 who observed decreased airway mucin production after BT, and with a case report published by Nagano et al.42 The latter demonstrated a decrease in the goblet cell hyperplasia after BT. This discrepancy may be due to a different observation time or the sheer heterogeneity of the inflammation and the extent of structural changes in the airways, taking into account the small number of patients analyzed in these studies.
Reticular basement membrane thickening is one of the characteristic features of airway remodeling that occurs in asthma. Nevertheless, this histological characteristic may be present even in early asthma process43 and has not been associated with asthma severity or symptom duration.43,44 There is also no association between RBM thickening and lung function.43,45 Considering the above, we evaluated the potential effects of BT therapy on RBM thickness. As it turned out, there was no significant decrease in the thickness of RBM after BT therapy. Similarly to the present study, several investigators did not observe any changes in the thickness of RBM after BT,38,39 while others demonstrated a significant decrease.15,16,37,40 This indicates that RBM thickness reflects likely structural changes related to the response of epithelial cells to the predominant pattern of airway inflammation, which did not change considerably after BT.
Importantly, we confirmed significant clinical improvement related to BT treatment. Both the degree of asthma control measured by ACT and the quality of life determined by the AQLQ questionnaire improved considerably after the procedure. This was accompanied by a significant decrease in the exacerbation rate, including the most severely requiring hospitalization, which is consistent with earlier reports showing improvement in asthma course after the BT procedure.7,46 Unexpectedly, the clinical benefits associated with BT were not correlated with decreased bronchial wall layer thickness, a reduction in ASM mass, or with spirometry measures. Previously published data on the possible association between the decrease in ASM and clinical improvement are inconclusive. For example, Pretolani et al37 reported a reduction in the area of ASM one year after BT that was correlated with improved asthma control and life quality, but not with spirometry values. However, several other reports did not demonstrate any association between the decrease in ASM mass after BT and clinical improvement.15,16,40 Finally, the recently published multicenter TASMA study47 also reported a reduction in ASM mass after BT, but this was not associated with clinical improvement. It should be noted that the lack of association between either the baseline thickness of the L2 layer (also ASM) or its reduction after BT with clinical improvement suggests that the therapeutic effect of BT is not associated solely with decrease in smooth muscle mass of the bronchial wall. This has already been suggested by Chernyavsky et al48 who described in vitro and in silico modeling of the acute effects of BT on ASM. They suggested that the magnitude of the ASM mass reduction after BT was not sufficient to explain the observed clinical benefits, implying more complex mechanisms of BT. Thermoplasty most likely targets not only the ASM layer but could also have a larger impact on other components of the airway wall such as epithelial cells, nerves, glands, and the extracellular matrix. Some of the effects of BT are probably transient, for example, a potential inflammatory response to BT-induced airway injury, while others persist, leading to improved clinical outcomes.
Despite earlier attempts to identify factors associated with a better response to BT, to date, potential predictors of a favorable response to this therapy are unknown. In our study, there was no association between baseline clinical parameters, thickness of the bronchial layers in EBUS, histological data and clinical improvement after BT. So far the data are inconclusive and need to be confirmed in larger study groups. The good responders to BT described by Ladjemi et al49 were younger compared with partial responders, they also showed a history of atopy and increased numbers of blood eosinophils and IgE levels. In turn, Langton et al50 demonstrated a positive correlation between improvement in asthma control and the number of radiofrequency activations during the procedure.
Some limitations of the present study need to be emphasized. Such limitations primarily address the small number of subjects included in the BT-treated group, selected based on the thickest ASM layer in EBUS. Therefore, we cannot exclude similar effects of BT in the group of individuals with thinner ASM mass. Also, there is no control to show how ASM changes in 12 months in patients without BT treatment. The influence of administration of high doses of prednisone during 3 BT procedures on the study outcomes cannot be ruled out either. As described by Papakonstantinou et al,38 the effects of BT on airway structure and histology may vary depending on asthma phenotypes or endotypes. The low number of participants in our study does not allow investigation of that issue.
In conclusion, our results indicate that the BT procedure leads to a significant decrease in the ASM layer as measured by EBUS and histological examination. EBUS may be a valuable tool in assessing the reduction of airway wall thickness after BT; however, it does not predict a favorable clinical response to BT treatment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by the Polish National Science Center grant (UMO-2014/15/B/NZ5/03493).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43(2):343–373. doi:10.1183/09031936.00202013
2. Sullivan SD, Rasouliyan L, Russo PA, Kamath T, Chipps BE; TENOR Study Group. Extent, patterns, and burden of uncontrolled disease in severe or difficult-to-treat asthma. Allergy. 2007;62(2):126–133. PMID: 17298420. doi:10.1111/j.1398-9995.2006.01254.x
3. Hekking PW, Wener RR, Amelink M, Zwinderman AH, Bouvy ML, Bel EH. The prevalence of severe refractory asthma. J Allergy Clin Immunol. 2015;135(4):896–902. PMID: 25441637. doi:10.1016/j.jaci.2014.08.042
4. Solèr M, Matz J, Townley R, et al. The anti-IgE antibody omalizumab reduces exacerbations and steroid requirement in allergic asthmatics. Eur Respir J. 2001;18(2):254–261. doi:10.1183/09031936.01.00092101
5. Pavord ID, Korn S, Howarth P, et al. Mepolizumab for severe eosinophilic asthma (DREAM): a multicentre, double-blind, placebo-controlled trial. Lancet. 2012;380(9842):651–659. PMID: 22901886. doi:10.1016/S0140-6736(12)60988-X
6. Cox PG, Miller J, Mitzner W, Leff AR. Radiofrequency ablation of airway smooth muscle for sustained treatment of asthma: preliminary investigations. Eur Respir J. 2004;24(4):659–663. PMID: 15459147. doi:10.1183/09031936.04.00054604
7. Wechsler ME. Bronchial thermoplasty for asthma: a critical review of a new therapy. Allergy Asthma Proc. 2008;29(4):365–370. PMID: 18702882. doi:10.2500/aap.2008.29.3133
8. d’Hooghe JNS, Goorsenberg AWM, Ten Hacken NHT, et al.; TASMA research group. Airway smooth muscle reduction after bronchial thermoplasty in severe asthma correlates with FEV1. Clin Exp Allergy. 2019;49(4):541–544. PMID: 30723963. doi:10.1111/cea.13365
9. James AL, Bai TR, Mauad T, et al. Airway smooth muscle thickness in asthma is related to severity but not duration of asthma. Eur Respir J. 2009;34(5):1040–1045. PMID: 19282340. doi:10.1183/09031936.00181608
10. Pepe C, Foley S, Shannon J, et al. Differences in airway remodeling between subjects with severe and moderate asthma. J Allergy Clin Immunol. 2005;116(3):544–549. PMID: 16159622. doi:10.1016/j.jaci.2005.06.011
11. Zuyderduyn S, Sukkar MB, Fust A, Dhaliwal S, Burgess JK. Treating asthma means treating airway smooth muscle cells. Eur Respir J. 2008;32(2):265–274. PMID: 18669785. doi:10.1183/09031936.00051407
12. Castro M, Rubin AS, Laviolette M, et al.; AIR2 Trial Study Group. Effectiveness and safety of bronchial thermoplasty in the treatment of severe asthma: a multicenter, randomized, double-blind, sham-controlled clinical trial. Am J Respir Crit Care Med. 2010;181(2):116–124. PMID: 19815809; PMCID: PMC3269231. doi:10.1164/rccm.200903-0354OC
13. Cox G, Thomson NC, Rubin AS, et al.; AIR Trial Study Group. Asthma control during the year after bronchial thermoplasty. N Engl J Med. 2007;356(13):1327–1337. PMID: 17392302. doi:10.1056/NEJMoa064707
14. Pavord ID, Cox G, Thomson NC, et al.; RISA Trial Study Group. Safety and efficacy of bronchial thermoplasty in symptomatic, severe asthma. Am J Respir Crit Care Med. 2007;176(12):1185–1191. PMID: 17901415. doi:10.1164/rccm.200704-571OC
15. Chakir J, Haj-Salem I, Gras D, et al. effects of bronchial thermoplasty on airway smooth muscle and collagen deposition in asthma. Ann Am Thorac Soc. 2015;12(11):1612–1618. PMID: 26325484. doi:10.1513/AnnalsATS.201504-208OC
16. Salem IH, Boulet LP, Biardel S, et al. Long-term effects of bronchial thermoplasty on airway smooth muscle and reticular basement membrane thickness in severe asthma. Ann Am Thorac Soc. 2016;13(8):1426–1428. PMID: 27509158. doi:10.1513/AnnalsATS.201603-182LE
17. Facciolongo N, Di Stefano A, Pietrini V, et al. Nerve ablation after bronchial thermoplasty and sustained improvement in severe asthma. BMC Pulm Med. 2018;18(1):29. PMID: 29422039; PMCID: PMC5806286. doi:10.1186/s12890-017-0554-8
18. Zanon M, Strieder DL, Rubin AS, et al. Use of MDCT to assess the results of bronchial thermoplasty. AJR Am J Roentgenol. 2017;209(4):752–756. PMID: 28796545. doi:10.2214/AJR.17.18027
19. Konietzke P, Weinheimer O, Wielpütz MO, et al. Quantitative CT detects changes in airway dimensions and air-trapping after bronchial thermoplasty for severe asthma. Eur J Radiol. 2018;107:33–38. PMID: 30292270. doi:10.1016/j.ejrad.2018.08.007
20. Kirby M, Ohtani K, Lopez Lisbona RM, et al. Bronchial thermoplasty in asthma: 2-year follow-up using optical coherence tomography. Eur Respir J. 2015;46(3):859–862. PMID: 26022958. doi:10.1183/09031936.00016815
21. Goorsenberg AWM, Hooghe JNS, de Bruin DM, van den Berk IAH, Annema JT, Bonta PI. Bronchial thermoplasty-induced acute airway effects assessed with optical coherence tomography in severe asthma. Respiration. 2018;96(6):564–570. PMID: 30110691; PMCID: PMC6390463. doi:10.1159/000491676
22. Vaselli M, Wijsman PC, Willemse J, Goorsenberg AWM, Feroldi F. Polarization sensitive optical coherence tomography for bronchoscopic airway smooth muscle detection in bronchial thermoplasty-treated patients with asthma. Chest. 2021;160(2):432–435. PMID: 33785301; PMCID: PMC8411445. doi:10.1016/j.chest.2021.03.042
23. Soja J, Grzanka P, Sładek K, et al. The use of endobronchial ultrasonography in assessment of bronchial wall remodeling in patients with asthma. Chest. 2009;136(3):797–804. PMID: 19429721. doi:10.1378/chest.08-2759
24. Górka K, Gross-Sondej I, Górka J, et al. Assessment of airway remodeling using endobronchial ultrasound in asthma-COPD overlap. J Asthma Allergy. 2021;14:663–674. PMID: 34163179; PMCID: PMC8214023. doi:10.2147/JAA.S306421
25. Kita T, Fujimura M, Kurimoto N, et al. Airway wall structure assessed by endobronchial ultrasonography and bronchial hyperresponsiveness in patients with asthma. J Bronchology Interv Pulmonol. 2010;17(4):301–306. PMID: 23168950. doi:10.1097/LBR.0b013e3181f9f09b
26. Gorska K, Korczynski P, Mierzejewski M, et al. Comparison of endobronchial ultrasound and high resolution computed tomography as tools for airway wall imaging in asthma and chronic obstructive pulmonary disease. Respir Med. 2016;117:131–138. PMID: 27492523. doi:10.1016/j.rmed.2016.06.011
27. Bonta PI, Chanez P, Annema JT, Shah PL, Niven R. Bronchial thermoplasty in severe asthma: best practice recommendations from an expert panel. Respiration. 2018;95(5):289–300. PMID: 29669351; PMCID: PMC6492603. doi:10.1159/000488291
28. Sokolowski JW, Burgher LW, Jones FL, Patterson JR, Selecky PA; Medical Section of the American Lung Association. Guidelines for fiberoptic bronchoscopy in adults. Am Rev Respir Dis. 1987;136(4):1066. PMID: 3662229. doi:10.1164/ajrccm/136.4.1066
29. Nakano Y, Müller NL, King GG, et al. Quantitative assessment of airway remodeling using high-resolution CT. Chest. 2002;122(6Suppl):271S–275S. PMID: 12475796. doi:10.1378/chest.122.6_suppl.271S
30. Awadh N, Müller NL, Park CS, Abboud RT, FitzGerald JM. Airway wall thickness in patients with near fatal asthma and control groups: assessment with high resolution computed tomographic scanning. Thorax. 1998;53(4):248–253. PMID: 9741365; PMCID: PMC1745194. doi:10.1136/thx.53.4.248
31. Coxson HO, Eastwood PR, Williamson JP, Sin DD. Phenotyping airway disease with optical coherence tomography. Respirology. 2011;16(1):34–43. PMID: 21044229. doi:10.1111/j.1440-1843.2010.01888.x
32. d’Hooghe JNS, Goorsenberg AWM, de Bruin DM, Roelofs JJTH, Annema JT, Bonta PI. Optical coherence tomography for identification and quantification of human airway wall layers. PLoS One. 2017;12(10):e0184145. PMID: 28981500; PMCID: PMC5628810. doi:10.1371/journal.pone.0184145
33. Bullone M, Beauchamp G, Godbout M, Martin JG, Lavoie JP. Endobronchial ultrasound reliably quantifies airway smooth muscle remodeling in an equine asthma model. PLoS One. 2015;10(9):e0136284. PMID: 26348727; PMCID: PMC4562526. doi:10.1371/journal.pone.0136284
34. Ya S, Haidong H, Chengjie Z, et al. Tentative study on radial endobronchial ultrasonography evaluating airway wall thickness before and after bronchial thermoplasty. Respir Med Case Rep. 2022;36:101571. PMID: 35036303; PMCID: PMC8749159. doi:10.1016/j.rmcr.2021.101571
35. Danek CJ, Lombard CM, Dungworth DL, et al. Reduction in airway hyperresponsiveness to methacholine by the application of RF energy in dogs. J Appl Physiol. 2004;97(5):1946–1953. PMID: 15258133. doi:10.1152/japplphysiol.01282.2003
36. Miller JD, Cox G, Vincic L, Lombard CM, Loomas BE, Danek CJ. A prospective feasibility study of bronchial thermoplasty in the human airway. Chest. 2005;127(6):1999–2006. PMID: 15947312. doi:10.1378/chest.127.6.1999
37. Pretolani M, Bergqvist A, Thabut G, et al. Effectiveness of bronchial thermoplasty in patients with severe refractory asthma: clinical and histopathologic correlations. J Allergy Clin Immunol. 2017;139(4):1176–1185. PMID: 27609656. doi:10.1016/j.jaci.2016.08.009
38. Papakonstantinou E, Koletsa T, Zhou L, et al. Bronchial thermoplasty in asthma: an exploratory histopathological evaluation in distinct asthma endotypes/phenotypes. Respir Res. 2021;22(1):186. PMID: 34183014; PMCID: PMC8240300. doi:10.1186/s12931-021-01774-0
39. Jendzjowsky N, Laing A, Malig M, et al. Long-term modulation of airway remodelling in severe asthma following bronchial thermoplasty. Eur Respir J. 2021;59(1):2100622. PMID: 34049950. doi:10.1183/13993003.00622-2021
40. Russell R, Aubier M, Pretolani M, et al. Bronchial thermoplasty leads to rapid and persistent improvements in airway remodeling. European Respiratory Society; 2019. Available from: https://www.ers-education.org/lr/show-details/?idP=237470.
41. Haj Salem I, Gras D, Joubert P, et al. Persistent reduction of mucin production after bronchial thermoplasty in severe asthma. Am J Respir Crit Care Med. 2019;199(4):536–538. PMID: 30540915. doi:10.1164/rccm.201811-2064LE
42. Nagano N, Iikura M, Ito A, Miyawaki E, Hashimoto M, Sugiyama H. Bronchial thermoplasty for severe asthma with mucus hypersecretion. Intern Med. 2019;58(11):1613–1616. PMID: 30713306; PMCID: PMC6599928. doi:10.2169/internalmedicine.1730-18
43. Payne DN, Rogers AV, Adelroth E, et al. Early thickening of the reticular basement membrane in children with difficult asthma. Am J Respir Crit Care Med. 2003;167(1):78–82. PMID: 12502479. doi:10.1164/rccm.200205-414OC
44. Jeffery PK. Remodeling in asthma and chronic obstructive lung disease. Am J Respir Crit Care Med. 2001;164(10 Pt 2):S28–38. PMID: 11734464. doi:10.1164/ajrccm.164.supplement_2.2106061
45. Kościuch J, Przybyłowski T, Górska K, et al. Zależność pomiedzy grubościa błony podstawnej oskrzeli i wybranymi parametrami czynności układu oddechowego u chorych na astme [Relationship between airway basement membrane thickness and lung function tests in patients with asthma]. Pneumonol Alergol Pol. 2009;77(3):256–263. Polish. PMID: 19591096
46. Chupp G, Kline JN, Khatri SB, et al. Bronchial thermoplasty in patients with severe asthma at 5 years: the post-FDA approval clinical trial evaluating bronchial thermoplasty in severe persistent asthma study. Chest. 2022;161(3):614–628. PMID: 34774528. doi:10.1016/j.chest.2021.10.044
47. Goorsenberg AWM, Shah PL, Annema JT, Bonta PI; TASMA research group. Bronchial thermoplasty induced airway smooth muscle reduction and clinical response in severe asthma. The TASMA randomized trial. Am J Respir Crit Care Med. 2021;203(2):175–184. PMID: 32721210. doi:10.1164/rccm.201911-2298OC
48. Chernyavsky IL, Russell RJ, Saunders RM, et al. In vitro, in silico and in vivo study challenges the impact of bronchial thermoplasty on acute airway smooth muscle mass loss. Eur Respir J. 2018;51(5):1701680. PMID: 29700102; PMCID: PMC6003767. doi:10.1183/13993003.01680-2017
49. Ladjemi MZ, Di Candia L, Heddebaut N, et al. Clinical and histopathologic predictors of therapeutic response to bronchial thermoplasty in severe refractory asthma. J Allergy Clin Immunol. 2021;148(5):1227–1235.e6. PMID: 33453288. doi:10.1016/j.jaci.2020.12.642
50. Langton D, Sha J, Ing A, Fielding D, Thien F, Plummer V. Bronchial thermoplasty: activations predict response. Respir Res. 2017;18(1):134. PMID: 28676053; PMCID: PMC5496290. doi:10.1186/s12931-017-0617-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.