Back to Journals » International Journal of Women's Health » Volume 14
End-Users Satisfaction with Positive Deviance Approach as an Intervention to Promote Exclusive Breastfeeding in Jimma, Ethiopia: A Multi-Level Analysis
Authors Siraneh Y ![]() , Woldie M
, Woldie M ![]() , Birhanu Z
, Birhanu Z
Received 11 November 2021
Accepted for publication 4 February 2022
Published 11 February 2022 Volume 2022:14 Pages 179—197
DOI https://doi.org/10.2147/IJWH.S349053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Yibeltal Siraneh,1 Mirkuzie Woldie,1,2 Zewdie Birhanu3
1Department of Health Policy and Management, Faculty of Public Health, Jimma University, Jimma, Ethiopia; 2Fenot Project, Department of Population and Public Health, University of British Columbia, Addis Ababa, Ethiopia; 3Department of Health, Behavior and Society, Faculty of Public Health, Jimma University, Jimma, Ethiopia
Correspondence: Yibeltal Siraneh, Email [email protected]
Background: Positive deviance approach (PDA) was implemented as an intervention strategy to address the poor practice of exclusive breastfeeding (EBF) in Jimma town, Ethiopia. Understanding the end-users satisfaction and its drivers is essential to determine whether this approach will be viable in the long run. Therefore, we determined the level of users’ satisfaction with the intervention and identified multi-level predictors to explain variability.
Methods: The data for this follow-up study were collected from September 01 to 25, 2020 among the study participants who were living in the intervention clusters of an earlier trial. A sample of 260 participants were invited to respond to an interviewer-administered structured questionnaire that assessed both individual and community-level variables. The developed tool was refined using experts’ view (face validity) and using factor analysis (FA) to validate the satisfaction measurement scales (construct validity). The mean scores were standardized using Percentages Scale Mean Score (PSMS) formulae. Two-level mixed-effects linear regression (linear mixed models) were performed to fit individual, community, and mixed-level variables. All assumptions were checked for each analysis as appropriate and β-estimates at 95% CI and p-value of < 0.05 were considered to declare a level of significance.
Results: The overall level of end-users’ satisfaction (PSMS) with PDA as an intervention to improve EBF was 50.9% with a maximum score of 99% and a minimum of 8%. Of the emerged satisfaction measuring scales, the standardized mean score for the user empowerment scale was the highest (53.7%). Five scales were emerged with 84.2% of the total variability explained in users’ satisfaction. The mixed-effect model revealed that age, occupation, experience of breastfeeding (BF), knowledge, attitude, self-efficacy, main source of BF information, previous home visit/support received from HEPs, participation in any social activities, and perceived community support for BF were independent two-level predictors of satisfaction.
Conclusion: As an intermediate outcome, more than half of the end-users of the PDA intervention were satisfied. End-users’ satisfaction with PDA as an intervention to promote EBF was predicted by multi-level factors. If they chose to use PDA as an intervention, Health program managers should be mindful of the two-level factors identified in this study.
Keywords: intermediate outcome, user satisfaction, multi-level predictors, follow-up study, Ethiopia
Background
Exclusive Breastfeeding (EBF) is the practice when the infant has received only breast milk except for supplements, or medicines in the first six months.1,2 World Health Organization (WHO) guide for essential newborn care emphasized early initiation and EBF as the primary focus of care.3 However, in Ethiopia, poor breastfeeding (BF) is reported especially in an urban setting.4–7 Due to many reasons and contextual factors, timely initiation and EBF is challenging.5,8–12 The challenges could be attributed to mother’s age, occupation (maternal employment and maternal leave), marital status, sex preference, wealth status, mode and place of delivery, limited social and community/family support especially at urban setting, mis-use and mis-understanding the benefits of industrial products, gaps in pre-disposing, enabling and re-enforcing factors of EBF.5,8–13 To promote EBF as it is a proven intervention, there are considerable challenges of selecting an approach that fulfils the need and expectation of mothers.1,14–16
In Jimma town, implementation research (integration of trial with participatory design) was conducted earlier which aimed to address the challenges of practicing EBF. The intervention was guided by Positive Deviance Approach (PDA) to promote EBF. This approach was implemented at community setting (home-based) by trained positive deviants (PDs). Context-based series of principles were followed while implementing the intervention.5
Measuring different types of outcomes is recommended in implementation research. However, defining the outcome measure of a given intervention is controversial and subjective to the goal or objective of the intervention depicted at the design stage. Generally, an outcome is defined as effects upon the target population which is measured among the end-users of the service.17 To understand the variety of these effects, most of the intervention may have primary, secondary, or sometimes tertiary outcome measures.17,18 Those outcomes could be implementation outcomes, service/client outcomes, or behavioral/clinical outcomes.15,19 The conceptual distinction among these three types of outcomes is also another source of disagreement among scholars. Of which, service outcome is an intermediate outcome which could be effectiveness, efficiency, safety, client-centeredness from an interventionist perspective, while satisfaction from the end-users perspective.19
Evidence of systematic review reported that among intervention studies included in the review, in 57.1% of the studies, clinical or behavioral outcomes were preferred and measured.20 This means in a given intervention study, intermediate service outcomes were less measured as compared to the ultimate outcomes.20 Thus, there are key questions in evaluating implementation research such as how to conceptualize and measure an intermediate outcome (user satisfaction).15,17 Measuring the intermediate outcome is equally important in understanding the effect of the intervention on the ultimate outcome.15 In many implementation types of research, the challenge is not only selecting a certain approach but also measuring its short-term and long-term outcomes at the same time.15,17,19,20
In this study, an outcome is conceptualized and measured as an intermediate result of the service provided as perceived by the end-users.19 End-user satisfaction is the general service outcome measure of a given intervention including the process and intermediate results. Intermediate outcome is measured by psychomotor domain after the actual encounter of the overall services, while implementation outcomes are measured by the cognitive and affective domain of the respondent from general understanding, perception, and encounter of each segment of the service.19,21 According to WHO and Enola Proctor’s implementation framework, measuring intermediate outcome can address both the concern of program responsiveness and client responsiveness, while measuring implementation outcome focus only on the program responsiveness, fidelity, and future fate.15,19,21 As an intermediate outcome, user satisfaction represents a complex mixture of perceived need, individually determined expectations, and experience of service which could be health or non-health-related matters.19,22
These outcomes may be measured at any stage (pre-implementation, throughout implementation, post-implementation) according to the nature of the intervention and outcome of interest.19 Selection of outcomes may be differentially relevant to various stakeholders.15 However, to ensure the transferability of intermediate outcomes across a range of settings, stakeholders’ priority should be represented in the measurement process.17,19,23 The literature suggests that studies usually capture those outcome measures (user satisfaction) at different times after the initial implementation.19,21,22 But some studies fail to specify a timeframe or are inconsistent in the choice of a time point.14,19,24
However, in this study, the intermediate outcome was not measured, characterized/described, and the variability was not predicted in the earlier trial. Hence, understanding the end-user’s level of satisfaction and its drivers is essential to determine whether this approach will be viable in the long run. Therefore, this study aimed to determine the level of end-users’ satisfaction with PDA implemented to promote EBF among the intervention group and identified multi-level predictors of satisfaction.
Methods and Participants
Study Design and Setting
This cross-sectional follow-up study was conducted in Jimma town, Ethiopia from September 01–25, 2020 among the intervention clusters of an earlier trial.5 Jimma town has 17 kebeles (smallest administrative units) all of which are working sites for urban Health Extension Professionals (HEPs). There were a total of 59 HEPs assigned and working for community-based health services during the study period in all kebeles of the town. In the intervention clusters of the trial study, there were 8 HEPs with health worker to population and household ratio was being less than the national standard (1:1500 and 1:500 respectively). The actual ratio of HEPs to households and population in Jimma are 1:745 and 1:3254, respectively.25
Description of the PDA and Activities
The intervention was guided by a PDA as a community-based strategy to promote EBF. The strategies were designed through the active participation of different stakeholders including the end-users. For the intervention clusters, the trial design was integrated with the participatory approach to become an implementation study. The PD inquiry and approach were defined and contextualized. Why and how the integration was made, implementation steps, and process were explained and discussed with stakeholders and co-created.
The home-based informational counseling and social support activities were implemented for 7 months with 6 visits in 2018. It was implemented in 3 clusters. Worth explaining shortly; home-based, comprehensive, and personalized informational counseling and social support services were provided for the mothers who were in the intervention group. Selected and trained positive deviants were the agents for each visit in addition to the usual routine community-based services. The intervention was also considered the participation of their relevant others. The counseling contents of EBF were adapted from WHO guideline26 and used to train PDs. At each of the six visits, the psychosocial support (emotional and appraisal) and verification of their understanding was the pillar to make sure about the plan of care, experience sharing and expectations, beliefs, and myths related to EBF. The PDs followed the five key points during the visits as appropriate;
- Developing an empathic relationship with the mother and other family members.
- Collaborating with the family in an equal partnership (knowledge, attitude, and skill of EBF shared) and the family brought their own experience and resources.
- Gently probing the individuals’ and family’s BF beliefs, attitudes and stimulating alternative ideas so that facilitate communication to provide specific/relevant information.
- Practical support and motivating the mother and other key family members to put knowledge into practice.
- Finally, appraisal of any difficulty faced during BF was done. Then every month the research team collected feedback from the PDs if they were challenged with any technical and medical issues of breastfeeding while counseling.5
Detailed information about the study design and setting, intervention approach, implementation process, main intervention activities, and specific time of visit with intervention package/content were reported in an earlier published article.5
Study Participants and Sample Size
This service outcome (end-users’ satisfaction) survey was conducted among intervention groups of the earlier trial. Among the six clusters (kebeles) which were randomly selected, three clusters were randomized for the intervention: Mendera-Kochi, Ginjo-Gudiru, and Awetu-Mendera.25 The number of mothers in the intervention clusters was 130. Name of kebele and village, personal contacts/phone number, and house number of each study participant were documented and available to use for this follow-up data collection. All mothers who enrolled into and received the intervention, and one relevant other who was nominated by the respective mother were included in this study.
The sample size for this specific follow-up study was estimated considering the number of end-users in the intervention group (n=130 mothers) of a cluster RCT study and one relevant other (n=130) to make the sample size double (2x) to minimize sampling error since we considered clusters in the study. Therefore, the final sample size for this study was 260.
Study Variables, and Measurements
The dependent variable was end-users’ satisfaction with the PDA intervention (counseling and social support service by PDs). Independent variables were individual-level factors such as socio-demographic characteristics of respondent (age, sex, educational status, ethnicity, religion, marital status, occupational status, monthly income), BF related factors (previous experience of BF/support, intention to BF/support), and post-implementation predisposing factors (knowledge of EBF, attitude/subjective norm towards EBF, self-efficacy to BF). Community-level factors were area of residency/cluster, existence of perceived functional Health Development Army (HDA) network, participation in any social activity, receiving support/visit from a HEP, previous main source of BF information, the village/zone where the assigned PD is living, educational status of the assigned PDs, and perceived community support for BF.
The dependent variable (users’ satisfaction) was defined as the feeling of the respondent about the informational and social support provided at home by PD. It is about the whole process of the intervention, the benefit received, and judged by the end-users after the actual encounter of the service. It is also a perceived need, individually determined expectations, and experience with PDA intervention. Satisfaction with various aspects of the intervention/service delivered, support, approach, and user participation was measured using a five-point Likert scale. The scale ranged from 1 (strongly dissatisfied) to 5 (strongly satisfied). The total number of items was 30.
Knowledge of EBF was measured using 17 items that assessed participants’ understanding about EBF with Yes=1 (correct) or No=0 (incorrect) responses. Attitude toward EBF was measured using 12 items with a five-point Likert agreement scale (1-strongly disagree to 5-strongly agree). Self-efficacy to BF/supporting the feeding mother was measured using 11 items with a five-point Likert agreement scale (1-strongly disagree to 5-strongly agree). Responses to negatively worded statements were reverse-scored before analysis. The remaining variables were measured using nominal responses, and the responses to some variables such as age and monthly income were categorized. Considering the positive influence on the outcome variable, nominal responses were represented by 0=failure, and 1=success.
Tool Development and Data Collection Technique
Interviewer administered, and structured questionnaire was used to collect the data. The tool for the predisposing factors was adapted from reliable and validated sources in English23,27–29 and then translated into local languages (Amharic and Afan Oromo). However, socio-demographic and BF-related variables, community-level factors, and end-users satisfaction measuring items were developed. Initially, 35 items were developed to measure satisfaction.
Then, members of the face validation panel were chosen considering the objective of this study and professional mix. To ensure face validity, the draft questionnaire was reviewed by expert panel including 3 MPH students, 2 Ph.D. students, and 2 academic staff with MPH. They were given the initial questionnaire with 35 items to review. In this stage, we asked them to comment on items’ understandability, logical order, duplication of items with the same meaning, readability, relevance, simplicity, language clarity such as wording and sentence structures. Then based on their comments, relevant modification was made, and five items were dropped. The final modified tool was translated into Amharic and Afan Oromo by language experts, and then back-translated into English by a third party who had research experience to ensure meaning equivalence.
Next, four health science graduates in the nursing and Public health profession were recruited for data collection and supervision. Three data collectors and one supervisor were trained on the procedure of data collection, the content of the pre-tested tool and ethical considerations. The trained professionals collected the data under close supervision. Each interview was conducted at the study subject’s homes based on their willingness to participate. A noise-free area for the interview was selected based on the context of each mother’s home setting. The interviewing time was estimated to take 25 to 30 minutes.
Data Management and Analysis
Data were entered into Epidata 3.1 and then exported to SPSS version 21.0 software for analysis. Socio-demographic characteristics of the participants were summarized using proportions for categorical variables, and means or medians for continuous variables.
The validity of the satisfaction measuring tool was checked using Exploratory Factor Analysis (EFA)/Factor Analysis (FA) to indicate the scale constructs. The purpose of doing EFA was to explore and validate constructs, reduce the data, and create satisfaction factor scores for regression modeling. All the assumptions of principal component analysis (PCA) were checked. The case to variable ratio was 8.5 to 1. Bartlett’s Test of Sphericity was significant at p<0.05. Overall sampling adequacy was checked using Kaiser-Meyer-Olkin (KMO) which was >0.5. The correlation matrix showed more than 2 cells with a coefficient of 0.3 to 0.9. Varimax rotation was employed during factor extraction to minimize the cross-loading of items. Reliability of items (inter-item consistency) was checked using the reliability coefficient (Cronbach alpha values) >0.70.
The mean score was used to dichotomize responses to satisfaction with PDA, knowledge of EBF, attitude towards EBF, and self-efficacy to BF measuring scales. Those who scored greater than or equal to the mean score were considered as “satisfied”; otherwise “dissatisfied”. Respondents who scored greater than or equal to the mean score were considered to have a “good knowledge”; otherwise “poor knowledge.” Likewise, the mean value was used to categorize the respondents having a “favorable” attitude or “unfavorable” attitude; and having a “good self-efficacy” or “poor self-efficacy”. This was helpful to describe the proportion of satisfaction against the background characteristics and facilitate easy understanding among the readers (program managers and implementers). Using the mean score for categorization avoids miss-classification, and the data were normally distributed.
In addition to this, standardizing the satisfaction measurement scale for PDA was done. Standardized percentages of the mean scores were created, ranging from “0%” to “100%”. For each case, it was calculated using the formulae;30,31 Percentages of Scale Mean Score (%SMS)=[Actual score-Potential minimum]/[Potential maximum-potential minimum]*100%. The mean scores for all scales were reported as %SMS. A higher score indicates higher level of satisfaction with the service provided and approach. This facilitates comparison with others’ findings.
Two-level mixed-effects linear regression analyses (linear mixed models) were performed. The data were at the individual (mothers and their relevant others) and community (cluster) levels. Individuals were nested in their respective clusters of the interventional study. The unit of analysis for the community-level variables was the cluster. There were three clusters in which 254 individuals were nested. Multi-Level Modeling (MLM) was used to estimate the correct standard errors to control bias not addressed by the classical linear regression which is employed to identify general predictors. To address this shortcoming, four models were fitted to identify two-level predictors of the end-users’ satisfaction.
First, two-level analyses were done to identify the candidates at a p-value <0.25 using mixed-model simple linear regression analysis. Then, the final two-level mixed-effect multiple linear regression models were fitted to identify the independent predictors. Fixed (residuals) and random (intercept) effects were analyzed to assess the individual and cluster level variations respectively. Random effects model estimate to see the variability within the clusters and between the three clusters, while fixed effects models only estimate within-cluster variability. All assumptions were checked for the mixed-effects linear regression model.
During the analysis, four models were fitted, null model (empty model without factors), model-1 (containing only individual factors), model-2 (containing only cluster/community factors), and model-3 (both the individual and community-level factors). An empty model without any factors/covariates was fitted to see the variance of the outcome variable and to justify the likelihood of using consecutive models. The intra-cluster correlation (ICC) was calculated which is one of the basic assumptions to conduct a multi-level mixed-effect model. The variation between clusters on satisfaction score was >0.1 (recommended cut-off point), while the variance and ICC must be >0 to analyze cluster-level factors. In this study, ICC was 0.16 at the empty model. If no such observed variability among the three clusters, GLM or GEE at an advanced level or the classical linear regression model could fit to identify the general factors without leveling, unlike this study. The variance at corresponding 95% CI was used to see the variation due to the effects of leveled factors for each model using ICC so that to identify the variance explained by the leveled factors. The higher the ICC, the more relevant were the community characteristics for understanding individual variation in satisfaction composite score.
In the subsequent models, β-estimates were used to see the measure of association and its magnitude. The variability on the estimate of beta (β)-values explained by successive models was calculated using percentage variance in the mean score. The Variance Change in Percentages’ Mean Score (VCPMS) was used to show the change in cluster-level variance between the empty and consecutive models. Akaike information criterion (AIC) was used to see the fitness of each model with a lower value indicating more fitness. Adjusted R-square change was used to show explained variation by each model. As reported in the empty model, 16.1% of the variations in satisfaction scores could be attributed to community/cluster-level factors. The values of the log-likelihood results were presented. Multi-collinearity between covariates was assessed with individual correlation values less than ten.32 All statistical analyses were performed at the 95% confidence interval with a 5% level of significance, and only significant variables from the final model were retained for interpretation.
Ethical Considerations
The letter of ethical approval was secured from the Institutional Review Board (IRB), Jimma University, Institute of Health with Ref. No: IHRPGD/728/2020 and dated as 27/08/2020, for this follow-up study. A permission/support letter was obtained from Jimma town health office and respective Kebeles/clusters. Informed written consent was taken from each participant. They were informed about their full right to participate or refuse participation in this follow-up study. Confidentially kept identifiers, taken during enrollment for the trial, were used to reach out for this follow-up study. This study was conducted in accordance with the Declaration of Helsinki.
Results
Socio-Demographic Characteristics
The response rate for this follow-up study was 97.7% (254/260). The mean age was 30.2 (±8.1) ranging from 18 to 60 years. The majority (59.8%) were between the age group of 25–34 years. Three-fourths (76.4%) of the study respondents were females. Almost all (96.9%) were ever-married, and 70.9% can read and write. More than one third (37.8%) were merchants, and 65% had estimated monthly net income of 33.1 USD or less (during data collection, the average exchange rate was 1USD=36.65Birr) (Table 1).
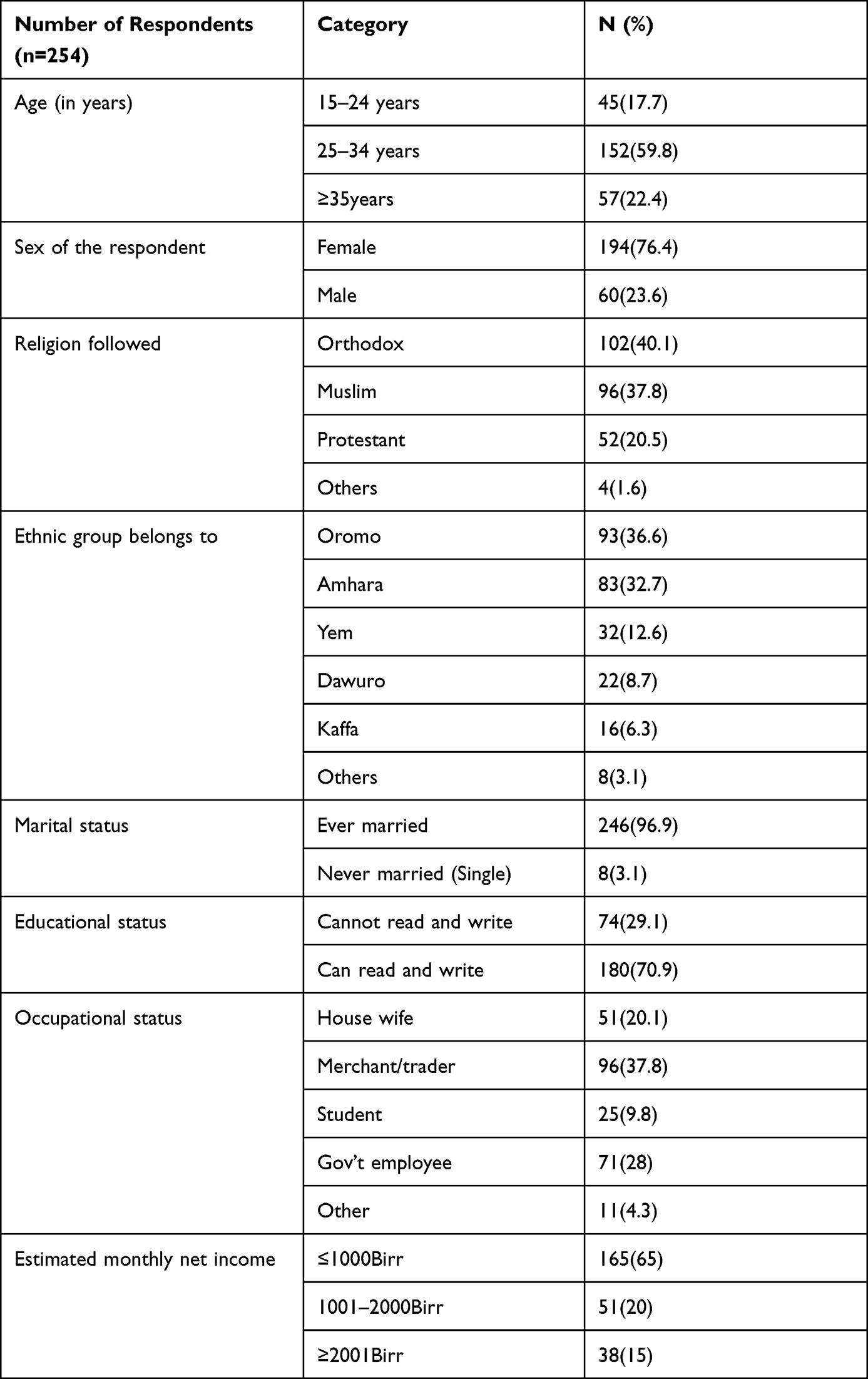 |
Table 1 Socio-Demographic Characteristics of End-Users of the Positive Deviance Approached Intervention, a Follow-Up Study, Jimma Town, September 2020 |
Description of the Satisfaction Measurement Scales
Satisfaction measurement scales were identified using PCA/EFA. Each emerged latent component/scale (factor with Eigenvalue greater than one extracted) was named considering the common concept of all items loaded to it. Twenty-eight items having a communality of >0.50 were retained on five components/scales. These were named as counselor/PD and counseling sessions, user empowerment, intervention approach (PDA) and health outcome, various aspects of the intervention (service delivered), and user engagement with 9, 7, 6, 3, and 3 items retained respectively. In the process, two items were removed due to a commonality value <0.5. No item was removed due to cross-loading. The item loading value of >0.4 was considered as a cut-off point. The emerged scales explained 84.2% of the total variability which is greater than the cut-off point (60% of TVE). The higher factor score created on a factor analysis indicates a higher degree of satisfaction with PDA. The Cronbach alpha’s reliability coefficient for these items loaded to the above five scales were 0.97, 0.92, 0.90, 0.85, and 0.82 respectively (Table 2).
 |
Table 2 Emerged Satisfaction Measurement Scales with Respective Item Loading Resulted from PCA, and Descriptive Measures to Each Item, a Follow-Up Study, Jimma, September 2020. (n=254) |
Among the items loaded to “Counselor/PD and counseling sessions” scale, the highest raw mean score belonged to the satisfaction with “practical information (skill) shared to you about EBF” and “emotional supporting ability of PD/counselor”, 3.1 (SD1.3) and 3.1 (SD1.4) respectively. Of the items measuring the “user empowerment” scale, the highest raw mean scored was to the satisfaction with “way of information communicated to you is trialable” and “credible information you received”, 3.3 (SD1.3). Of the items measuring the “intervention approach (PDA) and health outcome” scale, the raw mean score for the satisfaction with “positive deviant (counselor) assigned to you based on the new way” was among the three items highly scored 3.1 (SD1.3). However, the raw mean scores for all items loaded to the “various aspects of the intervention/service provided”, and “user engagement” scales, were highly and equally scored, 2.8 and 3.1 respectively (Table 2).
Level of Satisfaction with the PDA Intervention
The overall level of end-users’ satisfaction (PSMS) with PDA as an intervention to promote EBF was 50.9% with a maximum score of 99% and a minimum of 8%. Of the emerged satisfaction measuring scales, the PSMS for user empowerment scale was the highest (53.7%) followed by user engagement (51.7%), while the PSMS for the counselor and counseling sessions was the lowest (49.2%). However, the scale’s raw mean score of this factor was the highest (26.7 ± 10.3) which is an unstandardized one. All emerged scales taken together explained 84.2% of the total variability in users’ satisfaction. When participants were categorized into two using a simple mean score, 54.3% of the end-users were satisfied (scored ≥85.8), while by using the PSMS, 50.4% of the end-users’ were satisfied (scored ≥244.5). The overall satisfaction scales’ raw mean score was 85.8 ± 22.3, while the PSMS was 50.9%. The satisfied proportion (50.4%) is almost consistent with the overall satisfaction’s PSMS (50.9%=the sum of the five scales’ PSMS divided by 5) (Table 3).
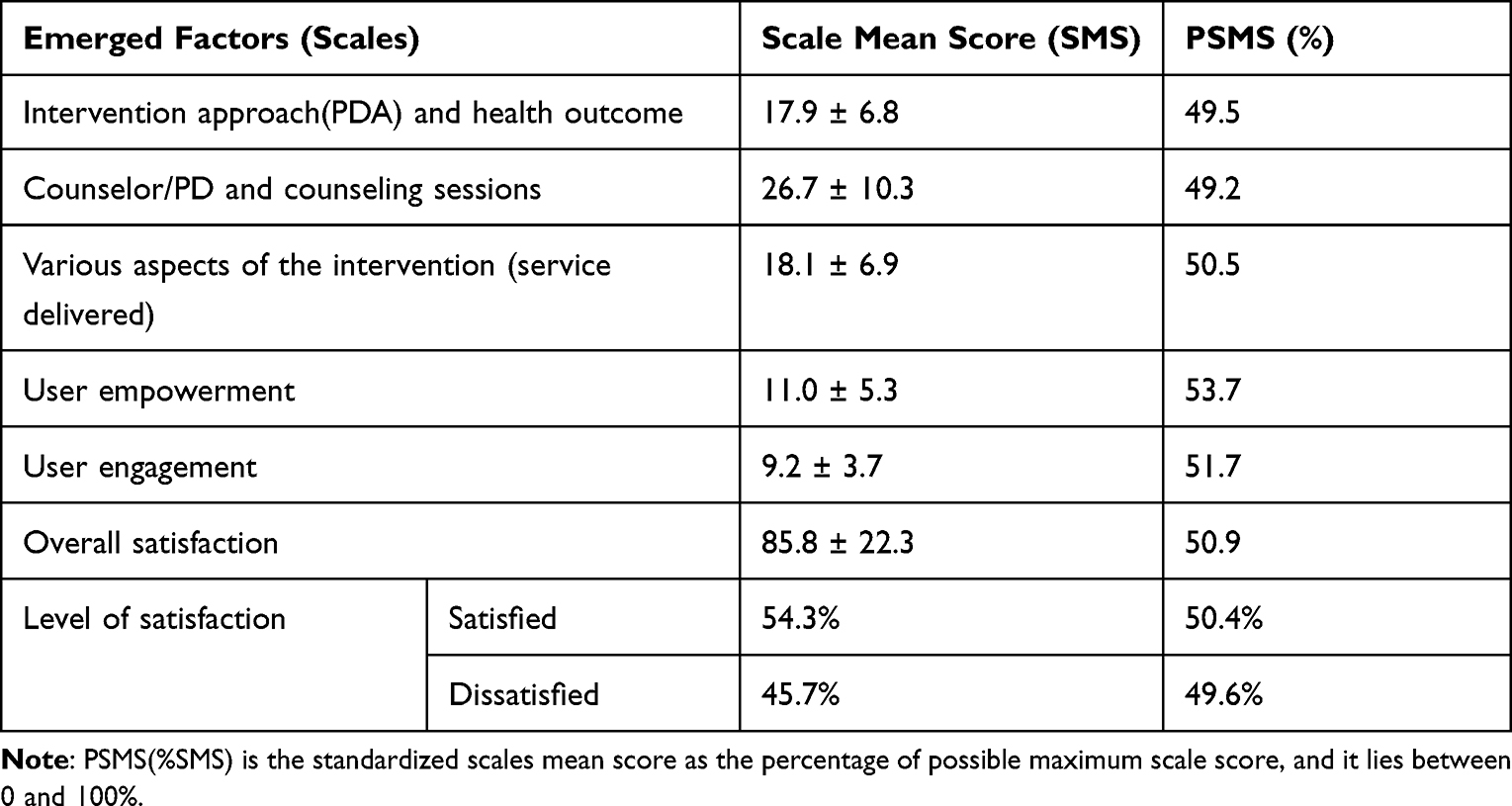 |
Table 3 Standardized PSMS, and Level of End-Users’ Satisfaction with PDA Intervention, a Follow-Up Study, Jimma Town, September 2020. (n=254) |
Individual-Level Characteristics and Users’ Satisfaction with PDA
More than two-thirds (68.8%) of the satisfied and half (49.1%) of those dissatisfied with PDA as an intervention to promote EBF were between the age of 25–34 years. Most of the satisfied respondents (81.2%) were females. Most (94.9%) of the satisfied and nearly all (99.1%) of the dissatisfied respondents were ever-married. Of the satisfied group, one-third (32.6%) were government employees, while from the dissatisfied group, half (50%) were a merchant. Most (88.4%) of the satisfied, and (93.1%) of the dissatisfied with PDA intervention had previous experience of BF or supported the mother to do so. Similarly, most of (84.8%) the satisfied and dissatisfied (88.8%) group had an intention to BF for the current baby or support the mother. More than two-thirds (70.3%) from the satisfied group, and 69% from dissatisfied group had a good knowledge of BF. Similarly, more than half (52.9%) from the satisfied group and 57.8% from the dissatisfied group had a favorable attitude towards BF. Although the majority (61.6%) of the satisfied group had good self-efficacy about BF, half (50.9%) of the dissatisfied group had poor self-efficacy about BF (Table 4).
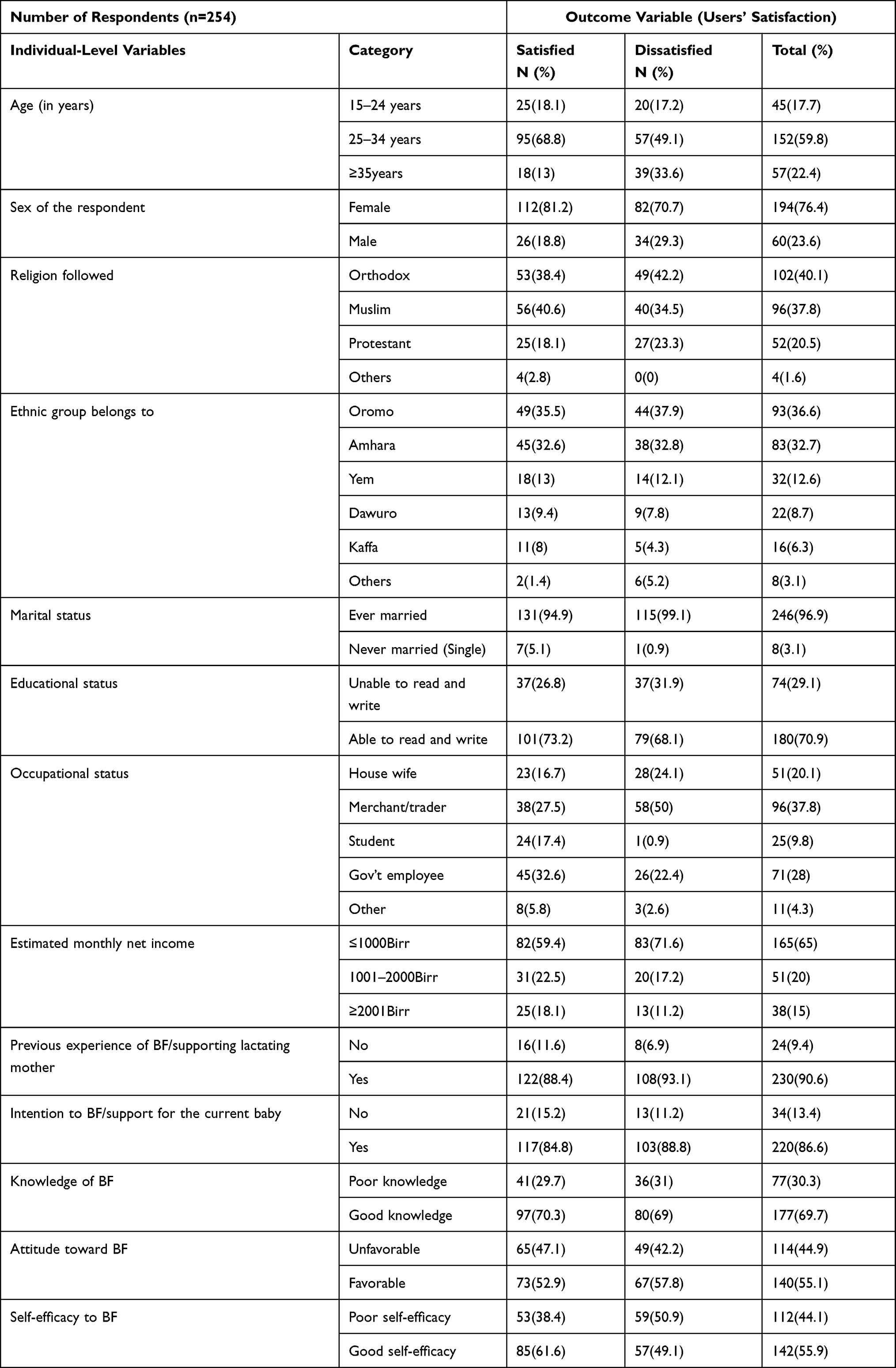 |
Table 4 Individual-Level Characteristics and Satisfaction of End-Users with Positive Deviance Approach of Intervention, a Follow-Up Study, Jimma Town, September 2020 |
Community-Level Characteristics and Users’ Satisfaction
Of all respondents, 31.5%, 34.6%, and 33.9% were living in Cluster-I, Cluster-II, Cluster-III respectively. At the community-level before the PDA intervention, more than one-third (38.4%) of the satisfied, and 35.3% of the dissatisfied respondents with PDA as an intervention strategy to promote EBF were mainly received BF information from urban HEPs. The majority (61.6%) of the satisfied and 57.8% of the dissatisfied received home-based visit/support from urban HEPs previously. The majority (67.4%) of the satisfied, and 62.1% of the dissatisfied were perceived as no functional HDA network in their village. However, three-fourths (75.4%) of those who were satisfied were participating in any social support activities. Whereas majority (64.7%) of those dissatisfied with the new approach were not participating or had limited participation in any social support activities. The majority (63%) of the satisfied, and 54.3% of those dissatisfied were living in the same village/zone where the assigned positive deviant is living. Around two-thirds (64.5%) of those satisfied respondents with PDA were counseled and supported by a PD who can read and write. However, more than half (55.1%) of the satisfied, and 92.2% of the dissatisfied perceived as no community support to practice EBF (Table 5).
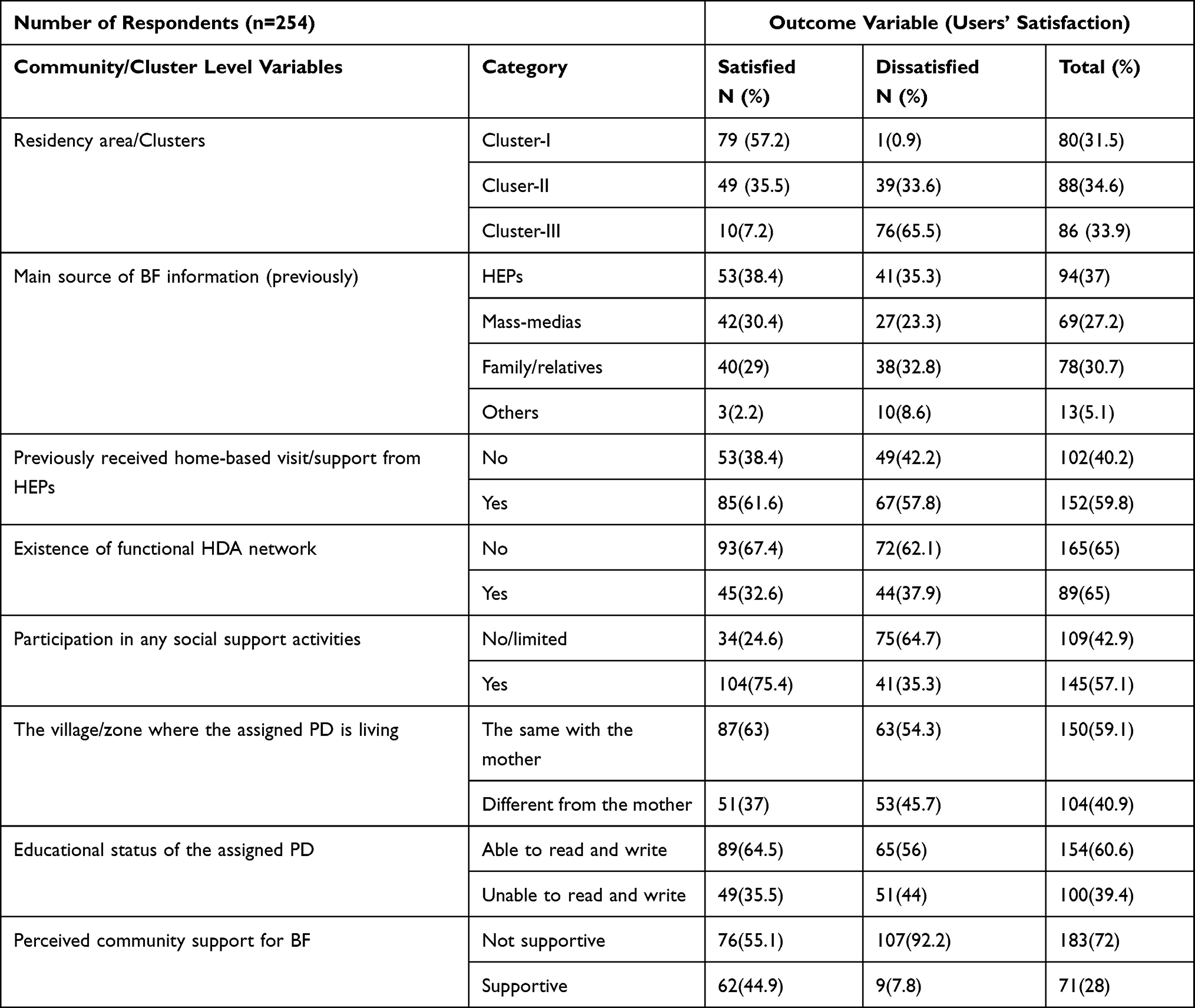 |
Table 5 Community-Level Characteristics and Satisfaction of End-Users with the Positive Deviance Approach of Intervention, a Follow-Up Study, Jimma Town, September 2020 |
Measure of Variation in Satisfaction
Multi-level mixed model random-effects were analyzed to check the variation of satisfaction score due to the leveled factors considered in this study. The empty model showed that there was a significant variation in the grand mean score of satisfaction among the three clusters (MV: 85.75, 95% CI: 83.00–88.50, p < 0.05). All the subsequent models remained significant at 95% CI (p < 0.05). At the empty model, a standard error of 43.97 was observed indicating significant variation before adjustment for individual and community-level factors while decreased along with the subsequent models. At the empty model, 16.1% of the variations in satisfaction could be attributed to community characteristics without controlling other factors. The higher the ICC, the more relevant were the community characteristics. Accordingly, the mixed model was fitted to determine the predictors of satisfaction (Table 6).
 |
Table 6 Multi-Level Mixed Model Random-Effects (Measure of Variation) of Users’ Satisfaction with the PDA Intervention, a Follow-Up Study, Jimma Town, September 2020. (n=254) |
As reported in the ICC (model 1), 14.2% variability in the satisfaction score was due to community-level factors after controlling for individual-level factors, while in the final model, 25.6% of the variation in the satisfaction score was observed after adding individual and community-level factors. The Variance Change in Percentages’ Mean Score (VCPMS) was used to show the change in cluster-level variance between the empty and consecutive models. This means the variability on satisfaction score was explained for successive models using this variance change. The AIC (log-likelihood) values were consistently decreased from the empty model to Model 3 implying the models were a better fit to the data. This was also confirmed by comparing with Bayesian information criterion (BIC) values. In each model, all the AIC values are less than BIC values. The consistent decrement in these values helps to select covariance structure with the best fit model. About 57.4% (Adjusted R2) of the satisfaction score was explained by the empty model considering clusters as an explanatory variable. This shows there was still unexplained variation (42.6%) among the clusters. There was no multicollinearity in all models (Table 6).
Multi-Level Predictors of Satisfaction
Independent predictors of end-users satisfaction with PDA as an intervention to promote EBF were determined using four successive linear mixed models. Before fitting each model, candidate variables were selected at P<0.25. Then candidates were fitted into the successive models and significant predictors were retained and reported. Finally, the full (mixed) model revealed that age, occupational status, experience of BF/support, knowledge of BF, attitude towards BF, self-efficacy of BF, main source of information about BF at community-level, previous home visit/support received from HEPs, participation in any social activities and perceived community-level support for BF were independent predictors (Table 7).
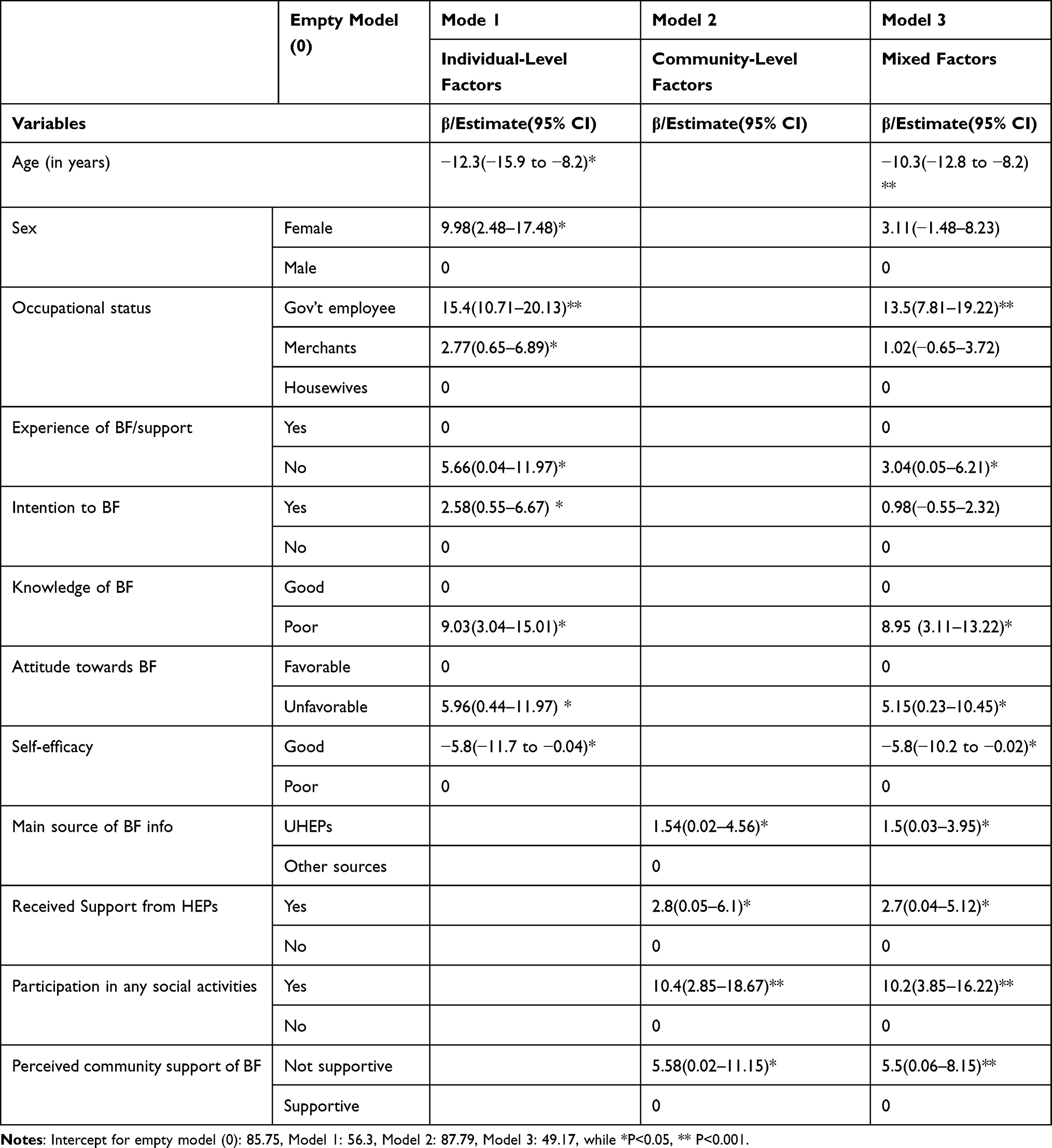 |
Table 7 Multi-Level Predictors of User Satisfaction with the PDA Intervention Using Linear Mixed Models, a Follow-Up Study, Jimma Town, September 2020. (n=254) |
A unit (one year) increment in age resulted in a decrement of the satisfaction score by 10.3 (β=−10.3, 95% CI:-12.8 to −8.2). However, the satisfaction score was 13.5 times (β=13.5, 95% CI: 7.81–19.22) higher among government employees as compared to the housewives. Similarly, it was 3.04 times (β=3.04, 95% CI: 0.05–6.21) higher among those without experience of BF or supporting lactating mothers compared to their counterparts. The satisfaction score was 8.9 times (β=8.95, 95% CI: 3.11–13.22), and 5.15 times (β=5.15, 95% CI: 0.23–10.45) higher among those who had poor knowledge, and unfavorable attitude towards BF as compared to their counterparts respectively. Also, the satisfaction score was 5.8 times (β=−5.8, 95% CI: −10.2 to −0.02) lower among those with a good level of self-efficacy compared to their counterparts. The satisfaction score was 1.5 times (β: 1.5, 95% CI: 0.03–3.95) higher among those who informed of BF from HEPs as compared to those who informed from any other sources. In the same way, the satisfaction score was 2.7 (β=2.7, 95% CI: 0.04–5.12) times higher among those who previously received support from HEPs compared to their counterparts. The satisfaction score was 10.2 times (β=10.2, 95% CI: 3.85–16.22) higher among those who participated in any social activities compared to their counterparts. The satisfaction score was 5.5 times (β=5.5, 95% CI:0.06–8.15) higher among those who perceived no community support for BF compared to their counterparts (Table 7).
Discussion
Out of the service outcomes (intermediate results), satisfaction is the main measure from the end-user perspective that is why we conceptualized and measured satisfaction from their point of view15,19,21 to understand whether the intervention satisfied them. Measuring intermediate service outcomes can address both the concern of program responsiveness, client responsiveness, and the interaction towards each other.21 However, in this study, we measured only client responsiveness (user’s satisfaction) which is the reflection of both. Client satisfaction represents a complex mixture of perceived need, individually determined expectations, and experience of care/service received from the PDA intervention which could be health or non-health-related matters.19,22
In the measurement and validation process of users’ satisfaction, PSMS was analyzed to standardize the measurement scales and to facilitate comparison with other future findings regardless of the number of items and response categories used. This concept was verified by our findings that the standardized mean score showed as satisfaction related to the user empowerment was the highest that contribute for the overall satisfaction level. Whereas the raw mean (unstandardized) resulted as satisfaction related with counselor and counseling sessions was the highest contributor. This fact was reflected on the overall level of satisfaction differently, which means when responses were dichotomized using a simple/raw mean score, 54.3% of the end-users were satisfied; while by using the PSMS, 50.4% of them were satisfied. This implies that categorizing responses using the raw (unstandardized) mean score overestimates the level (proportion) of satisfaction under the study. The 50.4% of satisfaction is almost consistent with the overall satisfaction’s PSMS (50.9%). This indicates that we should always use the standardized scale mean score to generalize the finding and to compare with others’ findings regardless of the number of items and response categories. Hence, using the standardized (PSMS) mean score to dichotomize respondents is more acceptable and avoids misclassification which is also supported by other studies.30,31
In this study, the level of end-users satisfaction with the PDA intervention and its multi-level predictors were measured and analyzed, considering it as one of the main proxy indicators of service outcome measurement.19 Overall, more than half of the users of the PDA as an intervention to promote EBF were satisfied. Of the emerged satisfaction measuring scales, the PSMS for user empowerment scale was the highest. Higher satisfaction score implies the higher responsiveness of the approach to the needs of the mothers and their relevant others in practicing and promoting EBF. This concept was supported by a study conducted elsewhere.31 The overall level of satisfaction observed in our study is less compared to the baby-friendly interventional study reported from Norway (76.2%).33 This discrepancy might be due to the setting (urban and rural) difference; in our case, the urban community might expect more that would affect their level of satisfaction. In addition, the approach difference might be also a reason. In our case, it is a community-based approach (by, from, and to the community) unlike the other’s in which they followed a mixed approach (facility and community-based approach). However, in our study, the user satisfaction was highly explained (84.2%).
We considered user satisfaction as an intermediate service outcome where knowledge of its multi-level predictors would improve the quality of decisions about the use of the PDA-guided intervention. This helps to understand what to consider, how, and on whom the PDA be implemented effectively to the satisfaction of the end-users. Our findings indicated that end-user satisfaction was predicted by multi-level factors such as individual-level, community-level and mixed-effect factors. The mixed-effect model revealed that age, occupation, experience of BF/support, knowledge, attitude, self-efficacy, main source of BF information, previous home visit/support received from HEPs, participation in any social activities, and perceived community-level support to practice BF were independent predictors of satisfaction with the PDA intervention.
Our findings are consistent with those of earlier reports.16,34,35 Those studies revealed as community-based intervention modified the dietary practices through identifying community-level factors, community factors influence the intervention effect, and psycho-social variables were associated with healthy infant growth. Also a study conducted in Norway shows the intervention participants were well satisfied due to integrated intervention with community-level structure.33 Hence, satisfaction with PDA as an intervention to promote EBF is highly context-specific being influenced by community-level factors in addition to the individual variations. This was further supported by the results of measure of the variations of satisfaction in our study. The empty model showed that there was a significant variation in the grand mean score of satisfaction among the three clusters, the standard error indicated significant variation before adjustment for multi-level factors, and 16.1% of the variations in satisfaction could be attributed to community characteristics without controlling other factors. This finding implied that community characteristics are very relevant for a better understanding of individual variation in satisfaction which is consistent with what others reported.33,36 About 57.4% (Adjusted R2) of the satisfaction score was explained by the empty model considering clusters as an explanatory variable. This shows there was still unexplained variation (42.6%) among the clusters that could be attributed to other factors.
The estimated value showed that when users’ age increases, their satisfaction with the PDA intervention decreased significantly. This might be due to having ample experience related to infant care and EBF, in that case, they may not need additional support or could be unhappy about the informational and social support provided. In fact, “I know all type” and “nothing new” biases might affect the supporting process37 and their satisfaction. In addition, government employees were highly satisfied as compared to housewives. While this is not straightforward to reason out, one of the service packs (breast milk expression) may be attractive for those who are working, and those on maternity leave might have time to receive the support. Likewise, those who have no experience of BF or supporting lactating mothers were more satisfied than their counterparts. This result supports the aging-related dissatisfaction, and it might be due to seeking help and support is the concern of those with less or no experience leading to a higher level of satisfaction. Such socio-demographic variables were also reported as a predictor elsewhere.38 This explains why those with poor knowledge, unfavorable attitude, and poor self-efficacy were highly satisfied compared to their counterparts.
The community-level factors implied that those who previously received support from HEPs, and who were informed about BF by HEPs were highly satisfied with PDA compared to their counterparts. This indicates that the new approach could supplement and synergize the existing strategies of promoting EBF by HEPs.39 Participating in any social activity was also a positive driver of satisfaction with the new approach. This nature of the intervention promotes social support, information exchange, and break urban social distancing which is all easier for those who participate in social activities. This finding supports the sustainability (scale-up) of the PDA which could minimize the negative perceptions about EBF prevailing in the community. This means, through this approach, those who feel as EBF is impossible, non-beneficial, and not supported by the community, could be encouraged to practice and get satisfied by the support.5,39 Without improving end-users’ satisfaction, achieving the desired outcome such as EBF may not be possible.15,17–19 The observed level of satisfaction with PDA might be one of the reasons for the reported effectiveness in the earlier study.5
Implications and Limitations of the Study
The observed level of satisfaction and identified predictors imply that although all respondents are living in the same city, community/cluster level variation can differently influence end-users satisfaction beyond their individual differences. Hence, community-based interventions such as the one used in the earlier trial should be well-informed by contextual factors with special due attention to the community-level factors as emphasized by other evidences.33,35 This means, PDA as an intervention to promote EBF can satisfy end-users if its multi-level predictors are considered during intervention regardless of the positive deviants’ educational status, common living area with the mother to be supported, and existence of functional HDA. The measures of variation confirm that factors influence satisfaction should be considered while designing PDA to promote EBF in similar settings. Although some variation is inevitable, it could be minimized to ensure that majority of the clients/users are satisfied by considering the two-level factors that explained part of the unexplained variations (42.6%).
Our study had some limitations, such as self-report bias, recall bias, social desirability bias, and misclassification bias while dichotomizing at analysis. To minimize reporting bias, participants were assured about the study objectives and anonymity. Recall bias is a possibility since this survey was conducted as a follow-up study after 18 months of the actual intervention. However, this may not be much of a problem since the intervention period was 7 months with intensive and active involvement of the users. To minimize misclassification bias during analysis, the standardized mean score was used30,31 and the data were normally distributed. In fact, this is more relevant for only cluster-level analysis, unlike ours which was both at individual and clusters level. Multi-level factors might not be restricted only to those variables included in this study; rather other factors could be there to explain the unexplained variations in satisfaction.
Conclusion
Overall, more than half of the end-users of the PDA intervention were satisfied. The total variability in users’ satisfaction with PDA was well explained by the five satisfaction measurement scales for which the user empowerment contributed the highest. A higher satisfaction implies the higher responsiveness of the approach to the need of the mothers and their relevant others in practicing and promoting EBF. End-users satisfaction was predicted by two-levels such as individual and community factors. The final mixed-effect model revealed that participants’ age, occupation, experience of BF/support, knowledge of BF, attitude toward EBF, self-efficacy to BF, main source of BF information, previous home visit/support received from HEPs, participation in any social activities and perceived community-level support for BF were independent predictors. These confirm the context-based nature of the approach that is sensitive to such variability. Therefore, to use PDA as an intervention to promote EBF, the two-level factors should be considered to satisfy mothers and their relevant others.
Abbreviations
BF, Breastfeeding; CHWs, Community Health Workers; CI, Confidence Interval; EBF, Exclusive Breast Feeding; EFA, Exploratory Factor Analysis; FA, Factor Analysis; GA, Gestational age; GEE, Generalized Estimating Equation; GLM, General Linear Model; HAD, Health development army; HEPs, Health Extension Professionals; MLM, Multi-Level Modeling; NMR, Neonatal Mortality Rate; PCA, Principal Component Analysis; PD, Positive Deviance; PDA, Positive Deviance Approach; PDI, Positive Deviance Inquiry; PDs, Positive Deviants; PHC, Primary Health Care; PNC, Post-Natal Care; PSMS (%SMS), Percentages of Scale Mean Score; RCT, Randomized Controlled Trial; SPSS, Statistical Package for Social Sciences; UHEPs, Urban Health Extension professionals; UNICEF, The United Nations International Children’s Emergency Fund; WHDA, Women Health Development Army; WHO, World Health Organization.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article. For some methodological details about the interventional study, a previously published article was cited in this paper.
Acknowledgment
We acknowledge Jimma University (JU), and the lead of Engine Project (Dr. Beyene Wondafrash) for the financial support provided to conduct this follow-up study. In addition, thanks to International Institute for Primary Healthcare-Ethiopia (IIFPHC-E) and John Hopkins University-USA for the financial and technical support provided for the previous trial, unless which this a follow-up study couldn’t be done. We also thank Jimma Town Health Office, study participants and data collectors.
Disclosure
The authors have disclosed that they do not have any potential conflicts of interest, financial or otherwise in this work.
References
1. World Health Organization. Exclusive breastfeeding for optimal growth, development and health of infants; 2019:85.
2. Khan J, Vesel L, Bahl RMJ. Timing of breast feeding initiation and exclusivity of breastfeeding during the first month of life: effects on neonatal mortality and morbidity–a systematic review and meta-analysis. Matern Child Heal J. 2015;19(4):68–79.
3. World Health Organization. Guidelines for essential newborn care encompass; 2017:125.
4. Seifu W, Assefa G, Egata G. Prevalence of exclusive breast feeding and its predictors among infants aged six months in Jimma. J Pediatr Neonatal Care. 2014;11(3):1–6.
5. Siraneh Y, Woldie M, Birhanu Z. Effectiveness of positive deviance approach to promote exclusive breastfeeding practice: a cluster randomized controlled trial. Risk Manag Healthc Policy. 2021;14:3483–3503. doi:10.2147/RMHP.S324762
6. Central Statistical Agency (CSA) [Ethiopia] and ICF International (USA). Ethiopia demographic and health survey 2016: key indicators report: addis Ababa, Ethiopia, and Rockville. Maryland, USA: CSA and ICF; 2016.
7. Centeral Statistical Agency FDR of E. Mini demographic and health survey 2019. AddisAbaba: MOH; 2019:15.
8. Alamirew MW, Bayu NH, Birhan Tebeje N, Kassa SF. Knowledge and attitude towards exclusive breast feeding among mothers attending antenatal and immunization clinic at Dabat Health Center, Northwest Ethiopia: a cross-sectional institution based study. Nurs Res Pract. 2017;2017:1–9. doi:10.1155/2017/6561028
9. Ayalew T. Exclusive breastfeeding practice and associated factors among first-time mothers in Bahir Dar city, North West Ethiopia, removed: a community based cross sectional study. Heliyon. 2020;6(9):e04732. doi:10.1016/j.heliyon.2020.e04732
10. Kavle JA, Lacroix E, Dau H, Engmann C. Addressing barriers to exclusive breast-feeding in low- and middle-income countries: a systematic review and programmatic implications. Public Health Nutr. 2017;20(17):3120–3134. doi:10.1017/S1368980017002531
11. Tsegaw SA, Dawed YA, Amsalu ET. Individual level and community level factors affecting exclusive breast feeding among infants under-six months in Ethiopia using multilevel analysis. Ital J Pediatr. 2021;47(1):1–13. doi:10.1186/s13052-021-01062-z
12. Tsegaw SA, Dawed YA, Amsalu ET. Exploring the determinants of exclusive breastfeeding among infants under-six months in Ethiopia using multilevel analysis. PLoS One. 2021;16(1):1–17. doi:10.1371/journal.pone.0245034
13. Chen J, Xin T, Gaoshan J, et al. The association between work related factors and breastfeeding practices among Chinese working mothers: a mixed-method approach. Int Breastfeed J. 2019;14(1):1–13. doi:10.1186/s13006-019-0223-z
14. Leykum LK, Pugh JA, Lanham HJ, Harmon J, McDaniel RR. Implementation research design: integrating participatory action research into randomized controlled trials. Implement Sci. 2009;4(1):1–8. doi:10.1186/1748-5908-4-69
15. Proctor E. Implementation outcomes. In: 2011 National Child Welfare Evaluation Summit Washington DC. 2011:5–15.
16. Zeitlin M, Vynckt S. The use of nutritional “positive deviants” to identify approaches for modification of dietary practices. Am J Public Health. 1976;66(1):38–42. doi:10.2105/AJPH.66.1.38
17. Rossi PH, Lipsey MW, GT H. Evaluation: A Systematic Approach.
18. Velentgas P, Dreyer NA, Nourjah P. Outcome definition and measurement. In: Developing a Protocol for Observational Comparative Effectiveness Research: A User’s Guide. Agency for Healthcare Research and Quality (US); 2013:3–15.
19. Proctor E, Silmere H, Raghavan R, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011;65:76.
20. Calder S, Ward R, Jones M, Johnston J, Claessen M. The uses of outcome measures within multidisciplinary early childhood intervention services: a systematic review. Disabil Rehabil. 2018;40(22):2599–2622. doi:10.1080/09638288.2017.1353144
21. De Silva A. A Framework for Measuring Responsiveness. World Health Organisation; 2000:1–42.
22. El Shabrawy AM, Mahmoud MEA. A study of patient satisfaction with primary health care services in Saudi Arabia. J Community Health. 1993;18(1):49–54. doi:10.1007/BF01321520
23. Pérez D, Van Der SP, Zabala C, Castro M, Lefèvre P. A modified theoretical framework to assess implementation fidelity of adaptive public health interventions. Implement Sci. 2016;11(91):1–11. doi:10.1186/s13012-016-0457-8
24. Hovmand PS, Gillespie DF. Implementation outcome study. J Behav Health Serv Res. 2010;37(79):30–45.
25. Jimma Town health office. Jimma Town health office annual report of 2017; personal communication; 2017.
26. World Health Organization. Breastfeeding counselling a training course participants â€TM manual part one Sessions; 2009:1–9.
27. Rye M, Torres EM, Friborg O, Skre I, Aarons GA. The Evidence-based Practice Attitude Scale- 36 (EBPAS-36): a brief and pragmatic measure of attitudes to evidence-based practice validated in US and Norwegian samples. Implement Sci. 2017;12(44):1–11. doi:10.1186/s13012-017-0573-0
28. Mora A, Russell D, Dungy C, Losch MDL, Dusdieker L. The Iowa infant feeding attitude scale: analysis of reliability and validity. J Appl Soc Psychol. 1999;29(11):2362–2380. doi:10.1111/j.1559-1816.1999.tb00115.x
29. Tengku Ismail TASZ, Sulaiman Z. Reliability and validity of a Malay-version questionnaire assessing knowledge of breast feeding. Malays J Med Sci. 2010;17(3):32–39.
30. Legesse MT, Salgedo WB. Adult patient satisfaction with in-patient nursing care in a referral and teaching hospital in Southern Nations Nationalities and Peoples’ Region (SNNPR), Ethiopia. J Nurs Care. 2016;5:334.
31. Siraneh Y, Ololo S, Tsega G, et al. Level and factors associated with professional commitment of health professionals providing institutional delivery services in public health facilities, Southwest Ethiopia. Ethiop J Health Sci. 2018;28(4):495–504. doi:10.4314/ejhs.v28i4.15
32. Larsen K, Merlo J. Appropriate assessment of neighborhood effects on individual health: integrating random and fixed effects in multilevel logistic regression. Am J Epidemiol. 2005;161(1):81–88. doi:10.1093/aje/kwi017
33. Bærug A, Langsrud Ø, Løland BF, Tufte E, Tylleskär T, Fretheim A. Effectiveness of baby-friendly community health services on exclusive breastfeeding and maternal satisfaction: a pragmatic trial. Matern Child Nutr. 2016;12(3):428–439. doi:10.1111/mcn.12273
34. Bolles K, Speraw C, Berggren G, Lafontant JG. Ti Foyer (Hearth) community-based nutrition activities informed by the positive deviance approach in leogane, haiti: a programmatic description. Food Nutr Bull. 2002;23(4):11–17. doi:10.1177/15648265020234S103
35. Zeitlin M, Ghassemi H, Mansour M. Positive deviance in child nutrition: with emphasis on psychosocial and behavioral aspects and implications for development. The United Nations University; 1990:163. Available from: https://corporatefinanceinstitute.com/resources/knowledge/trading-investing/list-top-10-types-cognitive-bias/.
36. Alemayehu B, Ayele BT, Kloos H, Ambelu A. Individual and community-level risk factors in under-five children diarrhea among agro-ecological zones in southwestern Ethiopia. Int J Hyg Environ Health. 2020;224:113447. doi:10.1016/j.ijheh.2019.113447
37. Inc. CE. Cognitive Bias: listof the top 10 most important biases in learning behavior; 2021. Available from: https://corporatefinanceinstitute.com/resources/knowledge/trading-investing/list-top-10-types-cognitive-bias/.
38. Srivastava A, Avan BI, Rajbangshi P, Bhattacharyya S. Determinants of women’s satisfaction with maternal health care: a review of literature from developing countries. BMC Pregnancy Childbirth. 2015;15(1):1–12. doi:10.1186/s12884-015-0525-0
39. Srivastava A, Gwande K, Bhattacharya S, Singh VK. Impact of the positive deviance approach on breastfeeding practices among tribal pregnant women: a before – after intervention study. CHRISMED J Heal Res. 2019;6(2):222–228. doi:10.4103/cjhr.cjhr_165_18
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.