Back to Journals » Patient Preference and Adherence » Volume 17
Empowering Healthcare Through User Feedback: A Multidimensional Analysis of the Knowledge
Authors Richards M ![]() , Inkeroinen S
, Inkeroinen S ![]() , Katajisto J, Muje S, Virtanen H
, Katajisto J, Muje S, Virtanen H ![]() , Leino-Kilpi H
, Leino-Kilpi H ![]()
Received 26 June 2023
Accepted for publication 11 November 2023
Published 5 December 2023 Volume 2023:17 Pages 3155—3165
DOI https://doi.org/10.2147/PPA.S425866
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Minna Richards,1 Saija Inkeroinen,1 Jouko Katajisto,2 Sasu Muje,1 Heli Virtanen,1 Helena Leino-Kilpi1,3
1Department of Nursing Science, University of Turku, Turku, Finland; 2Department of Mathematics and Statistics, University of Turku, Turku, Finland; 3Turku University Hospital, Turku, Finland
Correspondence: Saija Inkeroinen, Department of Nursing Science, University of Turku, Medisiina B, Kiinamyllynkatu 10, Turku, 20520, Finland, Email [email protected]
Purpose: Feedback from service users is a valuable source for improving the quality of care and services, potentially reflecting the successes and failures in providing empowering healthcare. In supporting empowerment, the multidimensionality of knowledge of service users is assumed to be a crucial factor, yet feedback has not been explored from the perspective of empowering knowledge. In this study, the aim was to analyze the knowledge areas expressed in the service users’ feedback from the point of view of empowering knowledge.
Patients and Methods: This was a retrospective study utilizing systematically collected service-user feedback from a feedback register of one university hospital district in Finland. Free-form feedback (n = 26,374) along with structured evaluative feedback was given by the patients themselves or their significant others, either by text message or using a feedback form, in 2019. The content of the feedback was analyzed according to the empowering knowledge areas (biophysiological, cognitive, functional, experiential, ethical, social, and financial), quantified, and analyzed statistically in relation to the background characteristics of service users.
Results: Service users gave multidimensional free-form feedback about the knowledge and educational practices in care and services. In the free-form feedback, the most common empowering knowledge areas were biophysiological and cognitive ones, whilst experiential, ethical, social, and financial areas were the least common. The highest ratings of structured evaluative feedback were associated with the cognitive and ethical areas.
Conclusion: Register-based feedback is systematic data for quality evaluation. In this study, service users seem to actively evaluate the knowledge procession in care and services, and therefore, they can be actors involved in developing the quality of educational practices. It does, however, indicate a need to add multidimensionality and improve the quality of the knowledge, and by that, advance the potential of empowerment among diverse service users.
Keywords: empowerment, feedback, health information, hospitals, district, knowledge, patient satisfaction, service users
Introduction
Feedback from service users can inform the development of healthcare into a more empowering and participatory direction, as instructed by international regulations and strategies.1,2 Collecting feedback is fundamental in improving and assessing the quality of provided care and thus, it is of interest for healthcare organizations.3–5 Important aspects of the quality can be investigated with systematically collected feedback illustrating, for example, service users’ experiences, perceptions, and satisfaction with the provided care.6 Transforming feedback to benefit healthcare service users faces continual challenges.2,7–10 There is a knowledge gap in research evidence about feedback from the point of view of empowerment of service users in healthcare.
Empowerment is a fundamental basis in healthcare, supporting service users’ own power in relation to the care and services.11 In this study, we theoretically focus on service users’ knowledge and educational activities as empowering factors in healthcare.11–14 Empowerment is a multidimensional concept which can be defined as a theory, process, intervention, and outcome on several levels.11,15,16 Empowerment relates to strengthening self-determination, enabling mastery, and increasing power.16 Co-creation of knowledge (instead of knowledge transfer) in healthcare can work as a prerequisite for empowerment.14,15 Empowering knowledge supports individuals to gain control and support decision-making and behavioral activities and by that, it can enhance management of one’s health and care.14 Meeting service users’ knowledge expectations can contribute to attaining health-related goals and improving the quality of healthcare.12,17 In order to be empowering, knowledge should be understandable and clear for service users as well as being sufficient18 and multi-dimensional.13 Empowering patient education can function as a key activity in promoting empowering, participatory and high-quality healthcare.
Empowering knowledge has been indicated to be multidimensional, consisting of at least seven areas: biophysiological (eg, health condition, symptoms and corresponding treatments), cognitive (eg, using and evaluating acquired knowledge towards one’s health benefit), functional (eg, mind and body functions such as mobility, rest, nutrition, and ability to act), experiential (eg, earlier experiences related to power and management of one’s health issues), ethical (eg, perceptions of being valued and respected), social (eg, social interactions and relationships), and financial (eg, resources and costs of care).13 These empowering knowledge areas have been studied in the hospital context,12 but previous studies on feedback from service users’ knowledge perspective are lacking.4 Therefore, specific interest was generated towards hospital service users’ feedback on the knowledge. In this study, both patients themselves and their significant others are referred to as service users.
The aim of the study was to analyze the knowledge areas expressed in the service users’ feedback from the point of view of empowering knowledge, assuming that multidimensional knowledge increases the potential for being empowered. The ultimate goal was to acquire person-centered evidence to improve the quality of educational practices in care and healthcare services. The following research questions were addressed:
- What empowering knowledge areas do service users express in their feedback?
- What knowledge-related evaluative feedback is given by service users when empowering knowledge areas are expressed?
- What, if any, is the connection between empowering knowledge areas and the background characteristics of service users?
Materials and Methods
Study Design and Data
This was a retrospective study utilizing a standard feedback register in one university hospital district in Finland. Feedback was given by service users (the patients themselves or significant others). The inclusion criteria were 1) the free-form feedback includes content about knowledge and 2) the feedback is recorded in the register between January 1st and December 31st, 2019 (representing a random year).
Data Collection
In this study, the feedback was extracted from the feedback register. An IT specialist with expertise in healthcare register data and affiliated with a clinical data informatics organization of the university hospital district extracted the data according to the research plan and cleaned and partly pseudonymized it. The IT specialist sent it securely to the researchers in June 2020 in the form of MS Excel files. The data was not linked to any other register data.
The data was originally collected in the register by the university hospital district using either text messages or feedback forms. After discharge from hospital care or services, text messages are systematically sent to all patients, who respond by replying to the text message. The feedback forms are available in both electronic and paper format, the electronic one on the website of the university hospital district and the paper version on the premises of the university hospital district. The paper forms are returned to the hospital staff in person or by mail, after which they are entered in the register.
Instruments
The text message and feedback form were developed in a national feedback network in 2007–2011. In this network, the aim was to scope national patient-feedback methods and standardize their practices. In the development of the feedback form, previous literature about patient feedback, relevant legislation, expert panels, consultations (healthcare quality working groups, universities, and statisticians) and benchmarking feedback forms nationally were utilized as well as comment rounds with the management of the hospital districts. In further development work, the National Institute for Health and Welfare evaluated and recommended the contents and modes of feedback, which were incorporated in both the text message and the feedback form.19
The text message had two parts: 1) free-form feedback and 2) structured evaluative feedback. In the free-form feedback part, there was an open-ended question requesting free-format feedback about the care and services. In structured evaluative feedback, there was a structured item evaluating the understandability of the knowledge processed in care and services on a Likert scale of 1–5 (1 = completely disagree, 5 = completely agree). No background characteristics were available from the text message data.
The feedback form consisted of three parts: 1) free-form feedback, 2) structured evaluative feedback, and 3) background characteristics. In the first part, there was an open-ended question asking for free-format feedback about the care and services. As for the second part, the structured evaluative feedback consisted of six structured items evaluating the patient’s care on a Likert scale of 1–5 (1 = completely disagree, 5 = completely agree). The items concerned 1) the sufficiency of instructions before the care, 2) understandability and 3) sufficiency of the information during the care, 4) clarity of contact instructions, 5) quality of the instructions for the home, and 6) knowledge of continued care. Based on these six items, a sum variable (SumKnow) was formed. In this study, Cronbach’s alpha was 0.955. The third part included background characteristics: evaluator (patient/significant other), patient’s gender, age, mode of arrival to the hospital (elective/emergency), and general evaluation of the quality of care on a Likert scale of 1–5 (1 = completely disagree, 5 = completely agree, a higher value indicating higher quality of care).
Analysis
Statistical methods were used for analyzing both the quantified empowering knowledge areas of the free-form feedback and the structured evaluative feedback items. Before quantification of the empowering knowledge areas, content analysis was used to analyze free-form feedback as follows.20 First, among all free-form feedback (n = 26,374), those related to knowledge were identified (n = 3113). In this identification, the terms knowledge, information, patient education and their synonyms were used. Second, the identified knowledge-related free-form feedback (n = 3113) was classified according to the seven empowering knowledge areas13 by using a matrix. In each area, descriptive quotes were identified. For supporting the validity, one researcher analyzed all the data, and the second researcher analyzed 10% and borderline cases. In the case of discrepancies in the analysis, in all phases, the final decision was made in the research group.
Statistical analysis was performed by using SPSS 26 software. Descriptive statistics were used to analyze the empowering knowledge areas service users expressed in their feedback and inferential statistics for analysis of knowledge-related evaluative feedback and the connections between empowering knowledge areas and the background characteristics of service users. The characteristics of the feedback and the service users giving the feedback were reported using frequencies, percentages, medians, mean values, and SD. The sum variable (SumKnow) based on six structured evaluative feedback items of the feedback form was formed by adding up the items and dividing the calculated sum by the number of variables. For the analysis of the reliability of the SumKnow, Cronbach’s alpha coefficients and item analysis of the compatibility of single responses within the instrument were used to provide evidence of internal consistency. Comparisons between the feedback of patients and significant others were done by using two-sample t-tests and Chi-Square tests. Comparison between empowering knowledge areas in the text messages and feedback forms were tested with Oneway ANOVA. Multifactor Analysis of Variance was used to find connections between the background characteristics and the sum variable (Main effect model). Sidak adjustments for multiple comparisons were used for pairwise comparisons. Statistical test was considered to be significant if the p-value was ≤ 0.05.
Ethics
In this study, good scientific practice was followed.21 Ethical approval was received from the Ethics Committee for Human Sciences at the University of Turku (8/2020, March 23rd, 2020) and permission to use the register data was given by the university hospital district (J15/20, May 13th, 2020). Originally, register data of the university hospital district included voluntarily given feedback by non-identifiable service users. According to Finnish law,22,23 the permission of the public register holder allows the use of the register data for research purposes (Article 38). In the case of the service user had given any identifiable information, the data was anonymized by the register holder. Researchers had no contact with the service-users and the quotes do not include any possibility to identify the users or the units of the district. Anonymity was protected also in data management, based on the guidelines of the University. Researchers have no conflicts of interest in this study.
Results
Characteristics of the Feedback and the Service Users Giving Feedback
The number of knowledge-related free-form feedback provided by the service users (patients and their significant others) was 3113. Out of 2457 text messages, 2198 expressed at least one empowering knowledge area, and as for the 656 feedback forms, 606 expressed at least one empowering knowledge area.
The background characteristics of the service users giving feedback were available from the feedback forms (n = 656) while the background characteristics of the service users giving feedback by text messages remain unknown (n = 2457). Feedback forms were provided by both patients (81%, n = 502) and significant others (18%, n = 111). Patients gave feedback regarding their own care while significant others gave feedback on patients’ care. It was not possible to match the feedback provided by patients and their significant others and the data may thus include multiple feedback on one patient’s care.
The patients were mainly women who came to the hospital care or services electively (Table 1). Feedback by significant others was most commonly given on behalf of children (< 18-year-olds) and patients arriving for emergency care. As for the general evaluation of the quality of care, patients evaluated it higher than significant others.
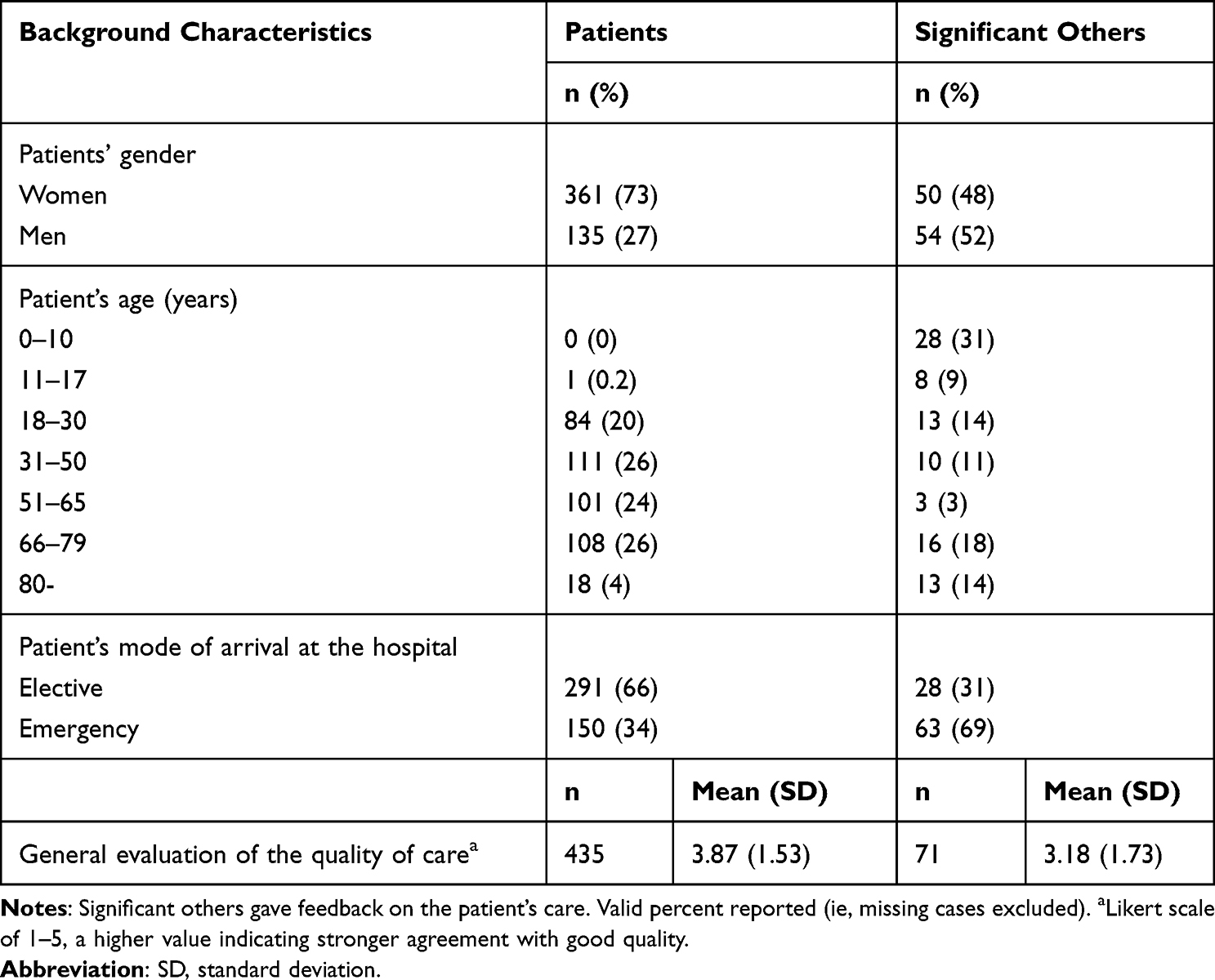 |
Table 1 The Background Characteristics of Service Users Giving Feedback |
Empowering Knowledge Areas in Feedback
The knowledge areas were analyzed from the free-form feedback based on the seven empowering knowledge areas.13 A single text message or feedback form could include multiple empowering knowledge areas. The biophysiological (n = 1665) and cognitive (n = 1265) areas emerged most frequently in the free-form feedback. Other areas – functional (n = 358), experiential (n = 183), ethical (n = 176), social (n = 144), and financial (n = 27) – emerged less frequently. To illustrate the free-form feedback given on each area, quotes are provided (Table 2).
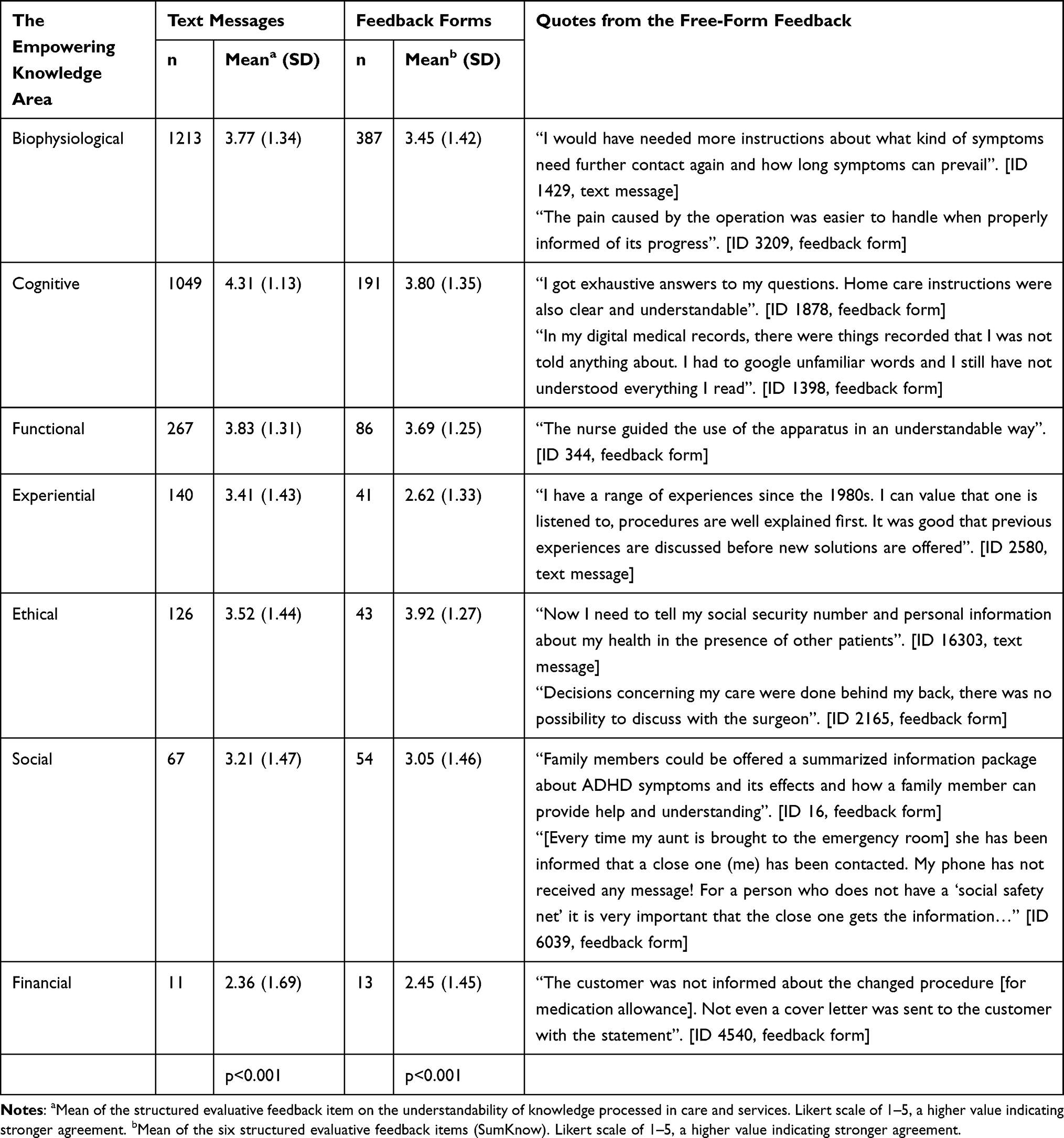 |
Table 2 Descriptive Quotes and Structured Evaluative Feedback on Knowledge Processed in Patient’s Care and Services in Free-Form Feedback Including the Empowering Knowledge Areas |
Empowering Knowledge Areas and Structured Evaluative Feedback on Knowledge
For each free-form feedback including the empowering knowledge area, the mean of the structured evaluative feedback on the knowledge processed in patient’s care and services was analyzed (Table 2). These mean values were statistically significantly different among the knowledge areas in both the text messages and feedback forms. In text messages, the mean of the structured evaluative feedback was the highest when the cognitive area emerged (4.31). In feedback forms, the mean of the structured evaluative feedback (SumKnow) was the highest when ethical (3.92) and cognitive areas (3.80) emerged. The lowest mean was in the financial area (with a mean in text messages and feedback forms of 2.36 and 2.45, respectively).
For feedback forms, the mean of the structured evaluative feedback was compared between the free-form feedback where each of the empowering knowledge areas emerged and the free-form feedback where the corresponding area did not emerge (but the feedback included knowledge-related free-form feedback). In a few empowering knowledge areas, there was a statistical difference (Table 3). Among both patients and significant others, those giving free-form feedback including the experiential area gave lower structured evaluative feedback compared to those whose free-form feedback did not include the experiential area. Among patients, the structured evaluative feedback was higher when the cognitive area emerged in the free-form feedback.
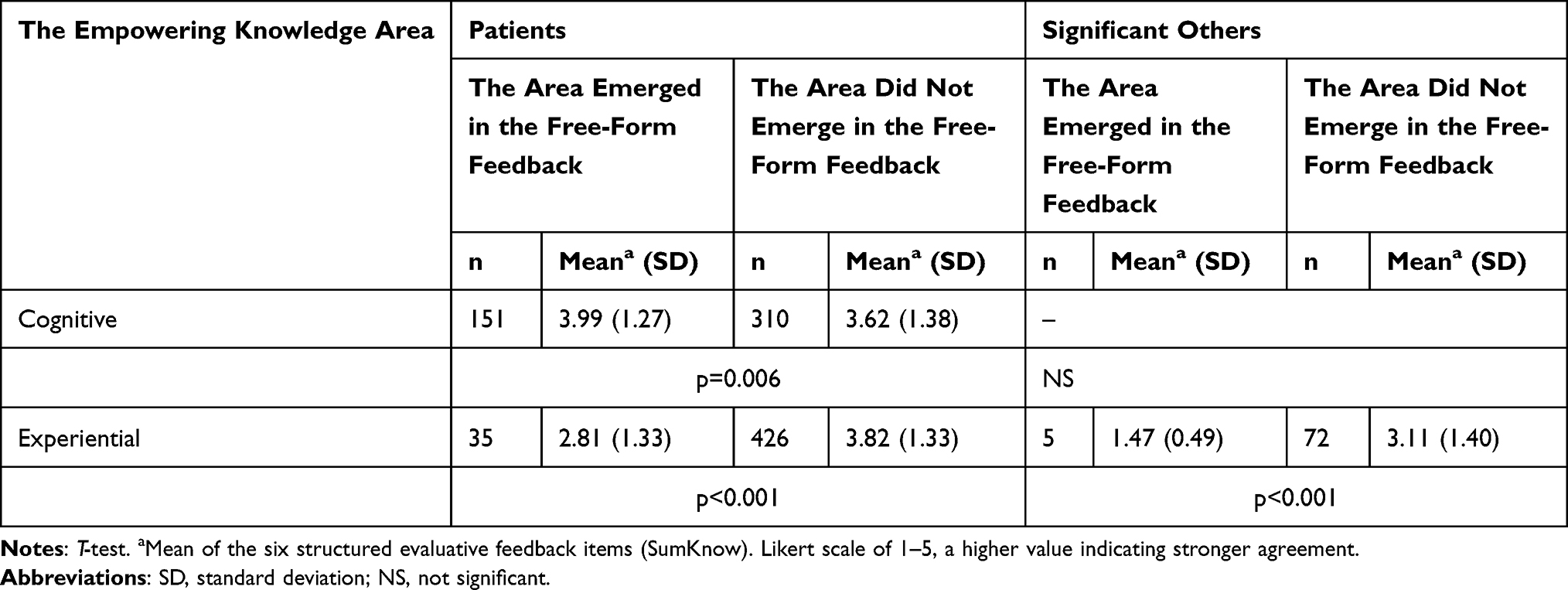 |
Table 3 Comparison of the Structured Evaluative Feedback (Only Statistically Significant Results Included) |
The Connection Between Empowering Knowledge Areas and the Background Characteristics of Service Users Giving Feedback
There was a statistical difference between patients and significant others in the proportion of free-form feedback including the social area (p < 0.001). Among significant others, the social area was expressed more frequently (n = 46, 41%) than among patients (n = 20, 4%). In other empowering knowledge areas, there were no statistical differences between patients and significant others.
Regarding the connection with other background characteristics in the feedback form, a separate analysis was done for patients and significant others on whether or not the free-form feedback included each of the empowering knowledge areas. All the background characteristics, ie, patient’s age, gender, and mode of arrival to the hospital as well as the general evaluation of the quality of care had a statistically significant connection with at least one empowering knowledge area (Table 4).
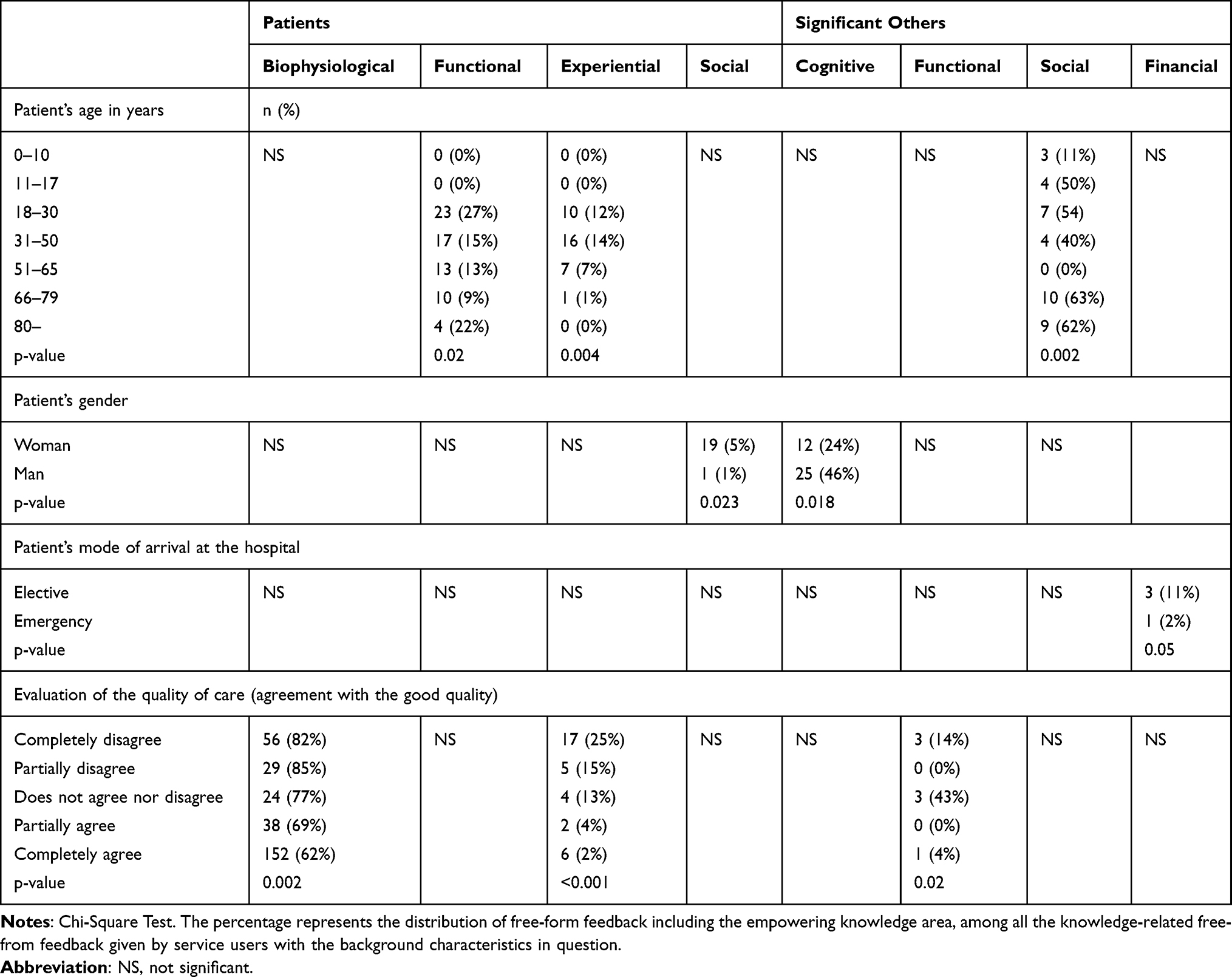 |
Table 4 The Connection Between Empowering Knowledge Areas Emerged in Free-Form Feedback and the Background Characteristics of Service Users (Only Statistically Significant Results Included) |
As for patient’s age, patients aged 18–30 years gave free-form feedback on the functional area (p = 0.02). Patients rarely gave free-form feedback on the experiential area, except for a few cases in the age group 18–65 years (p = 0.004). Significant others gave more free-form feedback on the social area when the patient was 66 years or older (p = 0.002).
Regarding the gender of the patient, male patients gave less free-form feedback on the social area compared to female patients (p = 0.023). Significant others gave more free-form feedback on the cognitive area when the patient was a man (p = 0.018).
As for the mode of arrival to care and services, there was barely a statistical connection with free-form feedback including the financial area by significant others when the patient’s mode of arrival to care or services was elective (p = 0.05).
As for the general evaluations of the quality of care, there was a statistical connection with the biophysiological and experiential areas among patients and with the functional area among significant others. While most of the patients giving free-form feedback on the biophysiological area completely agreed that the quality was good, the number of those completely or partially disagreeing was higher among patients who gave feedback on the biophysiological area compared to those who did not (p = 0.002). This also applied to the experiential area (p < 0.001). As for significant others, many chose a neutral response (ie, did not agree or disagree on the good quality) when the functional area emerged in feedback (p = 0.02).
Discussion
The aim of the study was to analyze the knowledge areas expressed in service users’ feedback from the point of view of empowering knowledge in order to acquire person-centered evidence to improve the quality of educational practices in healthcare services. Service users’ feedback is relevant for empowering and participatory healthcare, which current international strategies aim for,1,2 and multidimensional knowledge can increase the potential for being empowered.12,13 The main result was the multidimensionality of the empowering knowledge areas emerging from the free-form feedback, emphasizing the biophysiological and cognitive areas. This may indicate that service users attempt to deliver experiences related to these knowledge areas to participate in the assurance or improvement of the quality of care and services.
Empowering Knowledge Areas
The emphasis on the biophysiological area is consistent with earlier studies, but the frequent emergence of the cognitive area in service users’ knowledge-related free-form feedback is a new finding. The biophysiological area has been reported to be the most frequently expected and delivered in empowering patient education studies.12,24,25 This is not surprising, especially in the hospital environment, as visits are often related to somatic illnesses and symptoms. As for the cognitive area, one possible implication is that service users actively evaluate their knowledge and knowledge processing in the care and service. This is imperative for an individual’s capacity to access, acquire, process, and understand knowledge, which plays a fundamental part in self-management in various health conditions.14,18 Furthermore, the finding might indicate service users’ potential and desire to partner in developing educational practices. However, we do not know the content of the free-form feedback on the cognitive area, which is why further research is needed, with inductive content analysis or new data, for example, to confirm this new finding.
Service users giving feedback on the cognitive area evaluated the knowledge the highest, along with the ethical area. This finding may suggest that service users perceive the educational practices as high in terms of the quality and the knowledge as corresponding with their expectations. In contrast, the financial and experiential areas were evaluated as the lowest. Regarding the financial area, the amount of free-form feedback provided was the lowest; nevertheless, the low evaluation is alarming. Service users expect empowering knowledge concerning the costs, benefits, and other financial issues as out-of-pocket payments are increasing in many countries, including Finland.26 The low evaluation can be due to insufficient knowledge among patients25 and significant others24 as negative feedback can associate with poor quantity and quality of the knowledge processed in care and services.27 Furthermore, unmet expectations for financial knowledge have been reported in earlier studies as well.28 As for the experiential area, the low evaluations indicate a remaining challenge to acknowledge the service users’ emotions, previous experiences, and their utilization in educational practices. This is central to empowering and participatory healthcare:2 The failure to recognize service users’ experiential knowledge can lead to hindrance to participating and taking control of one’s health and life and therefore, this is a deficit in quality. For quality improvements, healthcare providers are expected to invest in educational practices by providing, for example, tools for identifying service users’ knowledge expectations and by providing healthcare professionals with sufficient competence to realize patient education concerning the area of experiential knowledge.
Empowering Knowledge Areas’ Connection with the Background Characteristics of Service Users
Patients and their significant others gave feedback on the patient’s care from different perspectives. For this reason, when possible, their feedback was analyzed separately in this study. This solution was successful in terms of identifying the differences between feedback by patients and their significant others. One interesting difference was feedback including the social area. Although the number of feedback was rather small, statistical analysis was able to show that significant others gave significantly more feedback including the social area. This was even more common when feedback was related to older patient’s care, highlighting the importance of significant others in securing a social safety net for aging patients. This has implications in terms of creating and improving family-centered educational practices, especially in countries with an aging population, such as Finland. The contributions of significant others to the health and care of patients are undisputed, especially in the field of empowering healthcare.
The negative connection between the feedback including biophysiological and experiential areas and general evaluations of the quality of care may indicate deficiencies in educational practices directed at supporting the knowledge of service users in these areas. This has special importance for the biophysiological area because it was the area that came up the most in the feedback. As for the experiential area, there might be a problem in the educational approach to service users’ previous experiences and emotions because it was also associated with low evaluations of the knowledge. This finding calls for further investigation so that service users have their experiential knowledge expectations met. In terms of other background characteristics, there were differences in the emerging empowering knowledge areas and their connections with patient’s age, gender, and mode of arrival to care and services. However, these were rather illogical, stand-alone findings, which are difficult to extrapolate. These findings can be due to the limited numbers of feedback forms in these areas and more research with larger samples or qualitative methods is warranted on these factors in the feedback on empowering knowledge.
Practice Implications
These findings have implications for empowering patient education. Patient education aims to continuously support service users in acquiring and processing empowering knowledge. The cognitive area is an important aspect to consider when incorporating the totality of empowering knowledge in patient education. From an empowerment perspective, service users are active and engage in educational practices with professionals, which enables them to become more independent and responsible, participate in and have a sense of mastery and control of their care.16 As the frequent emergence of the cognitive area in this study shows, service users actively evaluate their knowledge in the feedback. Utilizing learning theories in developing patient education can further support individual learning by taking into consideration the knowledge construction models and by facilitating service users to recognize their learning capabilities and preferences. This might require healthcare education and management to invest in pedagogical support and competence of patient educators. Furthermore, new opportunities for supporting empowerment can be discovered with technology, which can offer flexible web-based content designs and telehealth solutions for engaging and activating patients in their health behavior journeys.29
Implications for Future Research
There are several implications for future research. The data collection year of the study, 2019, provides a precious opportunity to evaluate knowledge and quality of care and services in hospitals by being the year just before the global COVID-19 pandemic. These results describe the care and services of the “old normal” in healthcare and can thus act as a useful reference point for future studies, as studies suggest that the pandemic had a negative impact on quality.30 The future research questions could relate to comparing or following up on the changes and development in knowledge, educational practices, and quality of hospitals from the perspective of service users.
In the evaluation of quality, efficiency, and effectiveness of care, national feedback registers continue to support healthcare providers to further develop services. Especially, written free-form feedback can be an opportunity for service users to reflect on and share challenging aspects of their care. Future studies can use these service user-reported outcome measures, but specifically designed feedback instruments based on the framework of empowerment could be beneficial for confirming the results of this study. In addition, future studies might consider exploring the connection between feedback and care by measuring clinical outcomes, for example.
Strengths and Limitations
The strengths and limitations of this study are related to the study design and data. Regarding the study design, register-based studies have benefits in terms of sample size; however, secondary data may have limitations in terms of bias, confounding, and missing data.31 The feedback register of the university hospital district provided extensive data and both free-form and structured feedback, which offered multifaceted data to answer the research questions. The instruments were nationally developed and used continuously, making it possible to replicate, repeat or compare the study and its results. A limitation is that it was not possible to link the data (eg, patients and their significant others).
Regarding the data, the strength is that the feedback was given spontaneously and voluntarily, so we can assume that the patients and significant others have presented important knowledge-related issues after authentic healthcare situations. This type of evidence has special importance for the development of empowering and participatory healthcare for diverse patients and populations. The weakness of the data is related to the nature of the feedback register of the hospital district. The data included limited background characteristics of service users and it did not enable estimation of the possible context-related factors related to the feedback given. The feedback rarely described the field of healthcare, health condition, and corresponding educational activity; therefore, the results can be interpreted on a descriptive level.
Conclusion
The knowledge-related feedback provided by healthcare service users, ie, patients and their significant others, was multidimensional. The emphasis was on the biophysiological and cognitive areas of empowering knowledge. The service users giving feedback on the cognitive area evaluated the knowledge processed in the care and services as high whereas the lowest evaluations associated with feedback on the financial area. As supporting empowerment is assumed to require attention on multiple areas of knowledge, along with a patient- and family-oriented approach, the results indicate that consistent work is needed to improve empowering patient education in order to identify and respond to the knowledge expectations of service users.
Acknowledgments
The abstract of this paper was presented at the 23rd International Nursing Ethics Conference: Thirty Years of Nursing Ethics: Looking Back, Looking Forward and the European Nursing Congress: Future Proof Nursing as oral presentations with interim findings.
Disclosure
Dr Helena Leino-Kilpi reports grants from Turku University Hospital, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. European Parliament. Council of the European Union. Regulation (EU) 2021/522; 2021. Available from: http://data.europa.eu/eli/reg/2021/522/oj.
2. Hall AE, Bryant J, Sanson‐Fisher RW, Fradgley EA, Proietto AM, Roos I. Consumer input into health care: time for a new active and comprehensive model of consumer involvement. Health Expect. 2018;21(4):707–713. doi:10.1111/hex.12665
3. Bastemeijer CM, Boosman H, van Ewijk H, et al. Patient experiences: a systematic review of quality improvement interventions in a hospital setting. Patient Relat Outcome Meas. 2019;10:157–169. doi:10.2147/PROM.S201737
4. Boylan AM, Turk A, van Velthoven MH, Powell J. Online patient feedback as a measure of quality in primary care: a multimethod study using correlation and qualitative analysis. BMJ Open. 2020;10(2):e031820. doi:10.1136/bmjopen-2019-031820
5. Leino-Kilpi H, Vuorenheimo J. Patient satisfaction as an indicator of the quality of nursing care. Nord J Nurs Res. 1992;12(3–4):22–28. doi:10.1177/010740839201200308
6. Berger S, Saut AM, Berssaneti FT. Using patient feedback to drive quality improvement in hospitals: a qualitative study. BMJ Open. 2020;10(10):e037641. doi:10.1136/bmjopen-2020-037641
7. Baines R, Regan de Bere S, Stevens S, et al. The impact of patient feedback on the medical performance of qualified doctors: a systematic review. BMC Med Educ. 2018;18(1):173. doi:10.1186/s12909-018-1277-0
8. Kaipio J, Stenhammar H, Immonen S, Axelsson M, Lantto M, Lahdenne P. Improving hospital services based on patient experience data: current feedback practices and future opportunities. IOS Press. 2018;2018(266–210):5. doi:10.3233/978-1-61499-852-5-266
9. Kumah E, Osei-Kesse F, Anaba C. Understanding and using patient experience feedback to improve health care quality: systematic review and framework development. J Patient Cent Res Rev. 2017;4(1):24–31. doi:10.17294/2330-0698.1416
10. Wong E, Mavondo F, Fisher J. Patient feedback to improve quality of patient-centred care in public hospitals: a systematic review of the evidence. BMC Health Serv Res. 2020;20(1):530. doi:10.1186/s12913-020-05383-3
11. Kuokkanen L, Leino-Kilpi H. Power and empowerment in nursing: three theoretical approaches. J Adv Nurs. 2000;31(1):235–241. doi:10.1046/j.1365-2648.2000.01241.x
12. Leino-Kilpi H, Inkeroinen S, Cabrera E, et al. Instruments for patient education: psychometric evaluation of the Expected Knowledge (EKhp) and the Received Knowledge of Hospital Patients (RKhp). J Multidiscip Healthc. 2020;13:1481–1505. doi:10.2147/JMDH.S271043
13. Leino-Kilpi H, Luoto E, Katajisto J. Elements of empowerment and MS patients. J Neurosci Nurs. 1998;30(2):116–123. doi:10.1097/01376517-199804000-00005
14. Funnell MM, Anderson RM, Arnold MS, et al. Empowerment: an idea whose time has come in diabetes education. Diabetes Educ. 1991;17(1):37–41. doi:10.1177/014572179101700108
15. Castro EM, Van Regenmortel T, Vanhaecht K, Sermeus W, Van Hecke A. Patient empowerment, patient participation and patient-centeredness in hospital care: a concept analysis based on a literature review. Patient Educ Couns. 2016;99(12):1923–1939. doi:10.1016/j.pec.2016.07.026
16. Halvorsen K, Dihle A, Hansen C, et al. Empowerment in healthcare: a thematic synthesis and critical discussion of concept analyses of empowerment. Patient Educ Couns. 2020;103(7):1263–1271. doi:10.1016/j.pec.2020.02.017
17. Leino-Kilpi H, Gröndahl W, Pekonen A, et al. Knowledge received by hospital patients-a factor connected with the patient-centred quality of nursing care: connection of quality and knowledge. Int J Nurs Pract. 2015;21(6):689–698. doi:10.1111/ijn.12277
18. Anderson RM, Funnell MM. Patient empowerment: myths and misconceptions. Patient Educ Couns. 2010;79(3):277–282. doi:10.1016/j.pec.2009.07.025
19. Peränen N, Sainio S. Asiakaspalautteen Kansallisen Keruun Yhtenäistäminen - Sisällölliset Ehdotukset - Projektin Loppuyhteenveto [Harmonisation of customer feedback collection - content suggestions - final summary of the project]; 2018. Available from: http://urn.fi/URN:NBN:fi-fe2019081424200.
20. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
21. ALLEA. The European code of conduct for research integrity – revised edition 2023; 2023. Available from: http://www.doi.org/10.26356/ECOC.
22. Ludvigsson JF, Håberg SE, Knudsen GP, et al. Ethical aspects of registry-based research in the Nordic countries. Clin Epidemiol. 2015;7:491–508. doi:10.2147/CLEP.S90589
23. Ministry of Social Affairs and Health, Finnish Government. Secondary use of health and social data. Ministry of Social Affairs and Health. Available from: https://stm.fi/en/secondary-use-of-health-and-social-data.
24. Copanitsanou P, Sourtzi P, Cano S, et al. Empowering education of arthroplasty patients’ significant others in three Southern European countries. Int J Older People Nurs. 2018;13(3):e12193. doi:10.1111/opn.12193
25. Klemetti S, Leino-Kilpi H, Cabrera E, et al. Difference between received and expected knowledge of patients undergoing knee or hip replacement in seven European countries. Clin Nurs Res. 2015;24(6):624–643. doi:10.1177/1054773814549992
26. Keskimäki I, Tynkkynen L, Reissell E, et al. Finland: Health System Review. World Health Organization 2019 (acting as the host organization for, and secretariat of, the European Observatory on Health Systems and Policies); 2019:1–166.
27. Kee JWY, Khoo HS, Lim I, Koh MYH. Communication skills in patient-doctor interactions: learning from patient complaints. Health Prof Educ. 2018;4(2):97–106. doi:10.1016/j.hpe.2017.03.006
28. Copanitsanou P, Valkeapää K, Cabrera E, et al. Total joint arthroplasty patients’ education on financial issues and its connection to reported out-of-pocket costs—a European Study. Nurs Forum. 2017;52(2):97–106. doi:10.1111/nuf.12171
29. Umar A, Mundy D. Re-thinking models of patient empowerment. Stud Health Technol Inform. 2015;209:175–181.
30. Tuczyńska M, Staszewski R, Matthews-Kozanecka M, Żok A, Baum E. Quality of the healthcare services during COVID-19 pandemic in selected European countries. Front Public Health. 2022;10:870314. doi:10.3389/fpubh.2022.870314
31. Benchimol EI, Smeeth L, Guttmann A, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015;12(10):e1001885. doi:10.1371/journal.pmed.1001885
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patient-Centered Communication Among Pharmacy Professionals Working in Hospitals and Drug Retail Outlets in Asmara, Eritrea: Knowledge, Attitude, Self-Efficacy and Barriers
Michael E, Nurahmed A, Mihreteab H, Nurhussien M, Adem M, Goitom A, Mihreteab Siele S, Tesfamariam EH, Abdu N
Integrated Pharmacy Research and Practice 2022, 11:153-164
Published Date: 6 October 2022