Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Empowering Children Through a Mobile Application for Sexual Abuse Prevention: The Supporting Roles of Parents and Teachers in a Cluster-Randomized Controlled Trial in Indonesia
Authors Solehati T ![]() , Hermayanti Y
, Hermayanti Y ![]() , bin Hazmi H
, bin Hazmi H ![]() , Trisyani M, Yusuf M, Kosasih CE
, Trisyani M, Yusuf M, Kosasih CE ![]() , Nurfirdausi Islamah R
, Nurfirdausi Islamah R
Received 28 March 2025
Accepted for publication 20 September 2025
Published 3 October 2025 Volume 2025:18 Pages 6343—6360
DOI https://doi.org/10.2147/JMDH.S530036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Tetti Solehati,1 Yanti Hermayanti,1 Helmy bin Hazmi,2 Mira Trisyani,1 Muhammad Yusuf,3 Cecep Eli Kosasih,4 Rachelya Nurfirdausi Islamah5
1Department of Maternity Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, Indonesia; 2Faculty of Medicine and Health Sciences, Universiti Malaysia Sarawak, Kota Samarahan, Sarawak, Malaysia; 3Hermina Hospital Kemayoran, Kota Jakarta Pusat, Jakarta, Indonesia; 4Department of Critical Nursing, Faculty of Nursing, Universitas Padjadjara, Sumedang, Indonesia; 5Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia
Correspondence: Tetti Solehati, Department of Maternity Nursing, Faculty of Nursing, Universitas Padjadjaran, West Java, Indonesia, Jl. Raya Ir. Soekarno KM. 21, Hegarmanah, Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +6281224836837, Email [email protected]
Background: Child sexual abuse (CSA) is a significant issue, partly due to the lack of evidence-based prevention programs involving parents and teachers. In Indonesia, no integrated CSA prevention app exists for parents, teachers, and children. This study evaluated the effectiveness of the Child Sexual Abuse Prevention Mobile Application (CSAP_Mob App) in empowering parents and teachers to improve children’s knowledge and attitudes, as well as parental and teacher knowledge and communication practices. The primary outcome is the change in children’s knowledge and attitudes, while the secondary outcome is the change in knowledge and communication practices among parents and teachers.
Methods: This cluster-randomized controlled trial included 56 teachers, 207 parents, and 212 children from elementary schools in two regencies in West Java, Indonesia. The intervention group received sexual abuse prevention education for four weeks via the CSAP_Mob App, while the control group followed standard school procedures. Effectiveness was assessed through pre- and post-tests measuring parents’ and teachers’ knowledge and communication practices, as well as children’s knowledge and attitudes toward recognizing and avoiding CSA. We used the Wilcoxon test to examine changes within groups and the Mann–Whitney U-test to compare differences between groups and calculate effect sizes.
Results: The intervention group showed a significant improvementin knowledge and communication practices among parents (p=0.001; 0.015) and teachers (p=0.001; 0.001), Conversely, parents (p=0.214; 0.870) and teachers (p=0.025; 0.936) in the control group showed no significant improvement. Both groups of children improved in knowledge and attitudes (p = 0.001). Significant differences were observed between the control and intervention groups following the intervention in children’s knowledge (p=0.001) and attitudes (p=0.001), as well as in parents’ knowledge (p=0.001), and teachers’ knowledge (p=0.001) and communication practices (p=0.001). Moderate effect size gains in children’s knowledge and attitudes, as well as in parents’ and teachers’ knowledge and communication practices, indicate the app’s effectiveness with parent and teacher involvement.
Conclusion: CSAP Mob Application effectively improved children’s knowledge and attitudes on sexual abuse prevention, as well as parents’ and teachers’ knowledge and communication practices. These findings highlight the importance of empowering parents and teachers through mobile-based interventions to strengthen child sexual abuse prevention efforts.
Clinical Trial Registration: NCT06752265.
Keywords: a randomized controlled trial, child sexual abuse, Indonesia, mobile application, prevention
Introduction
Child sexual abuse (CSA) is a global public health issue,1 with severe short- and long-term effects,2 including post-traumatic stress, behavioral and cognitive disorders, academic failure,3 nightmares, low self-worth,4 and impaired social interactions.5 The phenomenon of CSA is like an iceberg, where the prevalence is likely to be higher than reported because many cases go unreported by families6 or undetected.7 On average, children first experience CSA at the age of 7.5–14 years.4
Cases of CSA in Indonesia are rising, with reported cases increasing from 81 in 2017 to 350 in 2019, according to the Indonesian Witness and Victim Protection Agency.8 West Java has one of the highest CSA rates,9 with 52% of violence cases involving CSA.10 A study of 377 students in West Java found that 44.8% had poor CSA knowledge, and 71.6% had not received prevention information.11 Research from 2017–2018 also revealed that elementary schools lacked CSA prevention programs, with cultural taboos being a significant obstacle to implementation.12
The government has implemented various prevention programs, such as the Republic of Indonesia Child Protection Law Number 23 of 200213 and the Republic of Indonesia Law on Sexual Violence Number 12 of 2022,14 the Child-friendly Regency/City Development program, child protection movement campaigns, Integrated Service Centers for the Protection of Women and Children, and the National Movement Against Violence on Children.15 However, CSA cases continue to rise16 due to a lack of integrated, prevention-focused efforts involving families, schools, and communities.17 Existing programs remain broad and do not specifically address sexual abuse.18
Educating parents and teachers is essential,19 as they are children’s primary sources of essential sexuality education.20,21 Engaging parents in CSA prevention helps children develop self-protection skills.22 Collaboration between parents and teachers ensures safety at home and school. Empowering parents through school-based programs aligns with the Indonesian Ministry of Women Empowerment and Child Protection’s 2020–2030 plan, which prioritizes CSA prevention actions by involving families, schools, and communities in an integrated and comprehensive manner.23
In the Industry 4.0 era, social media is a powerful tool for CSA prevention due to its broad reach and influence on children.24 While various CSA prevention methods exist, including mobile applications,25,26 web-based training (online videos),27 and role-playing,28,29 there is currently no integrated application for parents, teachers, and children in Indonesia. The Child Sexual Abuse Prevention Mobile Application (CSAP_Mob App) addresses this gap by using engaging, modern methods to improve knowledge and communication skills.
The CSAP_Mob App is an Android-based educational tool designed to improve knowledge and communication practices among parents, teachers, and children over nine days. The CSAP_Mob application was developed based on a combination of the PRECEDE–PROCEED Model30 and Social Cognitive Theory.31 The PRECEDE–PROCEED Model provided a structured framework for identifying predisposing, enabling, and reinforcing factors influencing CSA prevention in the Indonesian context. At the same time, Social Cognitive Theory contributed behavioral change principles centered on observational learning, self-efficacy, and reinforcement. This theoretical basis guided the app’s focus on enhancing children’s knowledge and attitudes, while simultaneously empowering parents and teachers as role models and facilitators of preventive communication. These theoretical constructs were translated into interactive multimedia features, including TikTok, short videos, narrated PowerPoint slides, thematic prevention songs, and the TANGKIS slogan (“Tangkal Kekerasan Seksual”—Prevent Sexual Violence) to strengthen key prevention messages. The CSAP_Mob App can be downloaded using the Android operating system. The CSAP_Mob App consists of a nine-part series incorporating multimedia elements such as video stories, songs, documents, and TikTok, making it the first to use TikTok for CSA prevention. The inclusion of TikTok-style short videos, story videos, thematic songs, narrated PowerPoint slides, and the TANGKIS slogan was based on evidence that visually engaging, short-form, and familiar media formats improve user engagement, attention retention, and message recall among youth.32–34
In Indonesia, about 40% of Generation Z children use TikTok, making the platform a major challenger to Meta’s longstanding dominance in user engagement. Gen Z favors video-based and livestream content, which drives the popularity of TikTok.35 The use of TikTok among younger generations has significantly shaped their behavior.36 These multimedia elements were selected to cater to diverse learning styles (visual, auditory, and kinesthetic), enhance motivation, and increase the likelihood of sustained behavior change. The combination of traditional and novel media also aligns with the principles of Social Cognitive Theory by providing opportunities for modelling, reinforcement, and repeated exposure to prevention messages.
At the same time, disparities in digital access and literacy remain a challenge in Indonesia, particularly in rural communities. Although smartphone penetration is increasing rapidly, limited internet coverage and uneven digital literacy may hinder the equitable adoption of mobile health innovations. Addressing these contextual barriers is therefore critical to ensuring the feasibility and scalability of technology-based interventions for child sexual abuse prevention. To strengthen engagement, the app incorporated features inspired by popular social media platforms such as TikTok. Evidence indicates that short, visually engaging, and interactive digital formats can enhance learning, motivation, and retention, especially among younger users.
Research in 2019–2023 shows positive effects on parents’ and teachers’ knowledge, attitudes, and communication,37 though its direct impact on children has yet to be studied. To improve CSA prevention, effective primary prevention strategies are needed. The CSAP_Mob App aims to engage parents and teachers in enhancing children’s knowledge and attitudes toward CSA prevention. This study analyzed the app’s impact on elementary school children’s knowledge and attitudes through parent and teacher empowerment.
Methods
Study Design
This study utilized a cluster-randomized controlled trial design (cluster-RCT), with pre- and post-test assessments conducted to compare two groups: an intervention group receiving education through the CSAP_Mob App and a control group receiving standard school-based education. These assessments measured changes in knowledge and communication practices among parents and teachers, as well as changes in knowledge and attitudes among students resulting from the intervention. The research spanned four weeks, covering the pre-test, intervention, and post-test phases.
Sample Size Estimation and Setting
The study was conducted in two elementary schools in Bandung Regency and two elementary schools in Sumedang Regency, West Java, Indonesia, between March and December 2024. The location was chosen based on the high incidence of CSA in West Java.9 The inclusion criteria include: willing to be respondents, are parents who have elementary school children in two elementary schools in Bandung Regency and two elementary schools in Sumedang Regency (parents respondents), teacher in two elementary schools in Bandung Regency and two elementary schools in Sumedang Regency (teacher respondents), children in elementary school children in two elementary schools in Bandung Regency and two elementary schools in Sumedang Regency (children respondents), in good health, have a cellphone, understand Indonesian, can read, willing to complete all study procedures and provide informed consent.
The sample size for parents and children was calculated using Cohen’s D formula with a standard power analysis of 0.80 and a significance level (α) of 0.05.38 The authors based their estimates on previous intervention studies, where the mean for group 1 (M1) was 46.01 with a standard deviation (SD1) of 7.53, and the mean for group 2 (M2) was 42.73 with a standard deviation (SD2) of 7.78.39 Using Cohen’s D formula (1988),16,38 an effect size (ES) of 0.428 was calculated. This ES value was then entered into the G*Power 3.1.9.7 program, which determined a required sample size of 87. The sample size was rounded to 90 and was added by 27 to account for an anticipated attrition rate of 30%, resulting in a final sample size of 117 participants for each group (intervention and control) across parents and children.
Stratified cluster random sampling was employed to select parents and children, resulting in a total of 212 child participants (95 in the control group and 117 in the intervention group) and 207 parent participants (94 in the control group and 113 in the intervention group). Total sampling was used for teachers, with 56 teacher participants (27 in the control group and 29 in the intervention group). In total, the study included 475 participants.
Randomization
Each student and their parent who agreed to participate in the study were assigned a random number. Subsequently, 117 children and 117 parents were randomly allocated to either the intervention or control group using SPSS. The randomization process was carried out by each homeroom teacher using a random number generator, which was assigned to each student. The students or parents did not know which number they were assigned. Written consent was obtained from all participants. The participants remained unaware of their group assignment until just before the intervention began. Since all teachers were included in the study, no randomization was conducted for them.
Blinding
The study was carried out in Bandung Regency and Sumedang Regency. In Bandung Regency, Kota Baru Elementary School served as the intervention group, while Cangkuang Elementary School served as the control group. In Sumedang Regency, Hegarmanah Elementary School was assigned as the intervention group, and Cikuda Elementary School as the control group. There was no interaction between the schools or groups, as their locations were geographically distant from one another.
Instrument
The research instrument for parents and teachers consisted of a questionnaire assessing knowledge and communication practices, which was tested on 295 respondents (154 parents and 141 elementary school teachers) from 8 elementary schools in Bandung Regency and 10 in Bandung City, West Java, Indonesia. The questionnaire demonstrated an item correlation validity of 0.202–0.550 with a reliability test (Cronbach’s alpha) of 0.776 for knowledge and an item correlation validity of 0.191–0.674 with a reliability test (Cronbach’s alpha) of 0.819 for communication practices. The Parental and Teacher Knowledge Questionnaire consisted of 30 multiple-choice items developed based on CSA prevention guidelines and previously validated instruments. Each correct answer was scored as “1” and each incorrect answer as “0”, producing a total raw score ranging from 0 to 30. Parental and teacher communication practices were measured using a 17-item Communication Practices Questionnaire, where each item was rated on a 4-point frequency scale ranging from 1 = never to 4 = always. Negatively worded items were reverse-coded. Scores were summed to obtain a total ranging from 17 to 68. The total score ranges from 0 to 100. Higher scores indicate better knowledge and more positive communication practices.
In the children’s group, data collection used a questionnaire on knowledge and attitudes that had been tested on 20 respondents in elementary schools in Bandung Regency. The questionnaire had a content validity of 0.89 with a reliability test (Cronbach’s alpha) of 0.66 for knowledge and a content validity of 0.218 with a reliability test (Cronbach’s alpha) of 0.629 for attitudes. The Knowledge Questionnaire comprised 7 multiple-choice items, each scored 1 for a correct answer and 0 for an incorrect answer, yielding a total score of 0–7. Attitudes toward CSA prevention were assessed using 11 multiple-choice items scored in the same manner (0–11). The total score ranges from 0 to 100, with higher scores indicating better knowledge and more positive attitudes.
Study Intervention and Procedure
The intervention was the CSAP_Mob App, developed using behavioral theory and expert input (R&D approach, Sugiono, 2015). Featuring interactive short videos and TikTok-inspired content tailored to the Indonesian context, the app’s feasibility was validated by experts, and usability and acceptability were tested with 143 parents and teachers.
Participants were required to download the app, register, and log in before accessing any content. The app consisted of nine sequential learning modules on key topics in CSA prevention. Advancement to the next module was permitted only after completing the current one. The intervention lasted nine consecutive days, with one module assigned per day. Daily reminders were sent via a dedicated WhatsApp group created by the research team. Upon completing the ninth module, participants (parents and teachers) were instructed to submit a screenshot of their completion status in this group.
Although the app recorded log-ins and controlled sequential access, it did not yet feature an integrated back-end analytics dashboard to automatically capture detailed engagement metrics such as time spent per module or frequency of revisits. Consequently, engagement was monitored using a combination of in-app progression control, daily WhatsApp reminders, and screenshot verification. Only participants who completed all nine modules were included in the analysis.
The app’s content covers key topics, including CSA prevention strategies, the appropriate age to begin CSA education, identifying perpetrators or predators, the importance of communication between parents and teachers, and breaking the cultural taboo surrounding CSA discussions, an aspect not commonly addressed in previous studies. Additionally, the CSAP_Mob App features a discussion forum for CSA prevention-related conversations. By using this platform, parents, teachers, and children receive the same educational material without needing to meet at a specific time or place. They can access CSA prevention content anytime, anywhere, without disrupting their daily activities. Figure 1 shows features of the CSAP_Mob App for parents and elementary school teachers that have undergone content validity testing and black box testing.
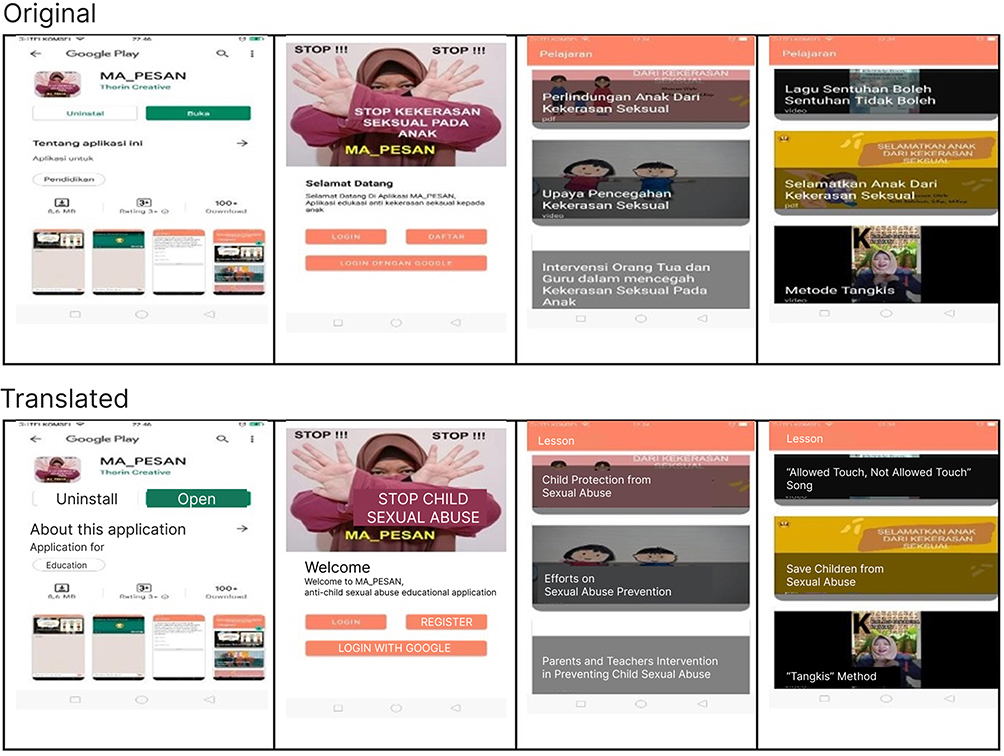 |
Figure 1 Features of the CSAP_Mob App for parents and teachers. |
After obtaining ethical approval from the Universitas Padjadjaran Institutional Review Board (Ethical Committee No. 783/UN6.KEP/EC/2024) by the Declaration of Helsinki, the researcher introduced themselves and provided all respondents with a clear explanation of the study’s purpose, procedures, and their right to withdraw at any time. Participants who agreed to take part were then asked to sign a written informed consent form.40 Each parent and teacher received a briefing session that provided the necessary information regarding their participation, the purpose and significance of the study, and their rights to participate. They carefully guided the participants in instructions on how to fill out the questionnaire. Informed consent was obtained from the parent and teacher participants. In the case of child participants, informed consent was obtained from their parents, and assent from the children was obtained verbally. The respondents could leave the study at any time and decide not to respond to the question. The researcher kept the data of respondents confidential.
Each participant received a unique code that they could use as their identifying number on all data collection forms. The first page of the questionnaire included instructions on how to fill it out, while the second page contained characteristic data. Along with the research team, parents and teachers completed the questionnaire. Parents, educators, and children were asked to complete a questionnaire about their knowledge of CSA prevention (which had three possible answers) and communication practices (which included four possible answers). Children were asked to complete a questionnaire about their knowledge of CSA prevention (which had two possible answers) and attitudes (which included two possible answers). The study team oversaw the arrangement of the private room and seats to prevent teachers, parents, and children from talking to each other while data was being collected. For children, data was collected via a paper self-reported questionnaire for twenty minutes in the school hall. Teachers and parents who agreed to take part in the study received products and phone credit. It was voluntary to participate. Every participant’s name was kept anonymous. The participants in the study did not experience any physical or psychological harm.
Respondents were randomly assigned to the intervention and control groups. Tests were given to both the control and intervention groups before and after the intervention. The pre-test was used to evaluate the base knowledge and communication practices of parents and teachers, as well as the children’s base knowledge and attitudes. The flow diagram of the study can be seen in Figure 2.
 |
Figure 2 Flow diagram of the randomized controlled trial. |
On the first day of the study, participants in the intervention group completed a pre-test before being instructed to download the CSAP_Mob App on their Android devices. The app provided information and communication strategies for preventing child sexual abuse (CSA). Over the next nine days, they received daily educational content through the app, with one series per day. Teachers and parents were required to read and understand the theoretical material provided in the app. The educational content was structured as follows:
- Day 1: PowerPoint on “Sexual Violence Against Children”
- Day 2: Cartoon video on “Prevention of CSA”
- Day 3: PowerPoint on “Protecting Children from CSA”
- Day 4: Cartoon video on “Prevention of CSA”
- Day 5: PowerPoint on “Parental and Teacher Intervention in CSA Prevention”
- Day 6: Video song on “Allowed and Not Allowed Touch”
- Day 7: PowerPoint on “Saving Children from Sexual Violence”
- Day 8: TikTok video on the “TANGKIS Method”
- Day 9: Informational video on “CSA Prevention”
For the next four weeks, parents and teachers were responsible for conveying the information they learned to their children daily. Regular reminders were sent via a dedicated WhatsApp group to encourage engagement with the CSAP_Mob App and ensure they shared the material with their children. After four weeks, the knowledge and communication practices of parents and teachers were reassessed. Additionally, child participants completed a questionnaire measuring their knowledge and attitudes toward CSA prevention before and after their parents and teachers implemented the CSAP_Mob App intervention. One month later, their knowledge and attitudes were reassessed.
On the second day of the study, the control group took a pre-test before receiving CSA prevention education based on the standard practices followed in their schools. This education was provided to teachers, parents, and children over four weeks. After four weeks, a post-test was conducted.
The post-test for both the intervention and control groups included the same questions as the pre-test. It was administered via Google Forms for parents and teachers, while children completed it on paper. Respondents were not informed that the pre-test and post-test contained identical questions. The researcher ensured that all ethical research principles were upheld to protect participants. Additionally, all respondents received merchandise and transportation compensation. This study posed no risk of harm to participants and was registered with ClinicalTrials.gov under Identifier: NCT06752265.
Statistical Analysis
A series of analyses was undertaken to evaluate the trial, including participant characteristics, homogeneity testing, pre- and post-intervention mean scores, between-group comparisons, and effect size estimation. Raw pre- and post-test scores were collected, verified, coded, and entered into SPSS version 24 for analysis. Descriptive statistics summarized participants’ demographic data. Homogeneity between the two groups was assessed using the Chi-square test for categorical variables and the Mann–Whitney U-test for numerical variables. Normality of pre- and post-test scores in both groups was examined with the Kolmogorov–Smirnov test, which indicated non-normal distribution. Consequently, the Wilcoxon signed-rank test was applied for within-group comparisons, while the Mann–Whitney U-test was used for between-group comparisons and effect size estimation. Statistical significance was set at p < 0.05.
All analyses were performed according to the pre-specified study protocol, with children’s knowledge and attitudes as the primary outcomes. Secondary analyses involving teachers and parents were exploratory. No formal statistical corrections for multiple testing (eg, Bonferroni or Holm adjustments) were applied to avoid increasing the risk of Type II error, given the relatively small number of hypotheses tested. Findings from secondary and exploratory analyses should therefore be interpreted with caution and considered hypothesis-generating.
Results
Characteristics and Homogeneity Tests
The findings from these analyses provide important insights into participant characteristics, group comparability, and the effectiveness of the intervention, as reflected in the changes in mean scores and effect sizes. In the children group, the average age of respondents is 9 years or in their early teens, amounting to 65 children (30.8%). Most of the respondents are female, amounting to 110 (51.9%). Most of the respondents, 139 children (65.6%), have never received information about the CSA prevention song, whereas 141 respondents (66.5%) have received information about CSA prevention. The complete data can be seen in Table 1.
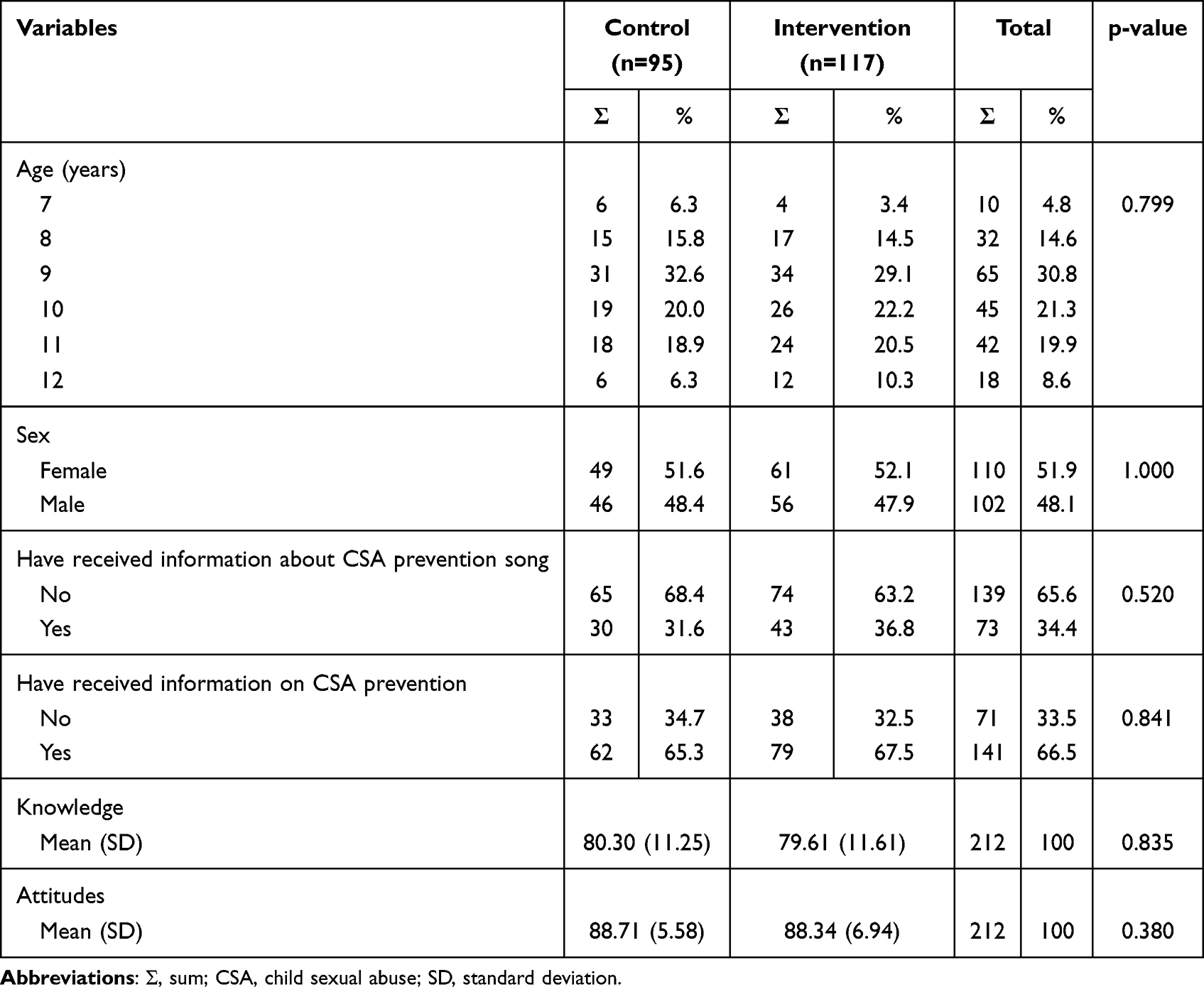 |
Table 1 Characteristic Distribution and Homogeneity Test in the Children Group Year 2024 (n=212) |
Among the parent group, most respondents were between 36 and 45 years old (late adulthood), predominantly female, unemployed, had a high school education, and earned below the regional minimum wage (RMW). The majority had previously received information on CSA prevention. The complete data can be seen in Table 2.
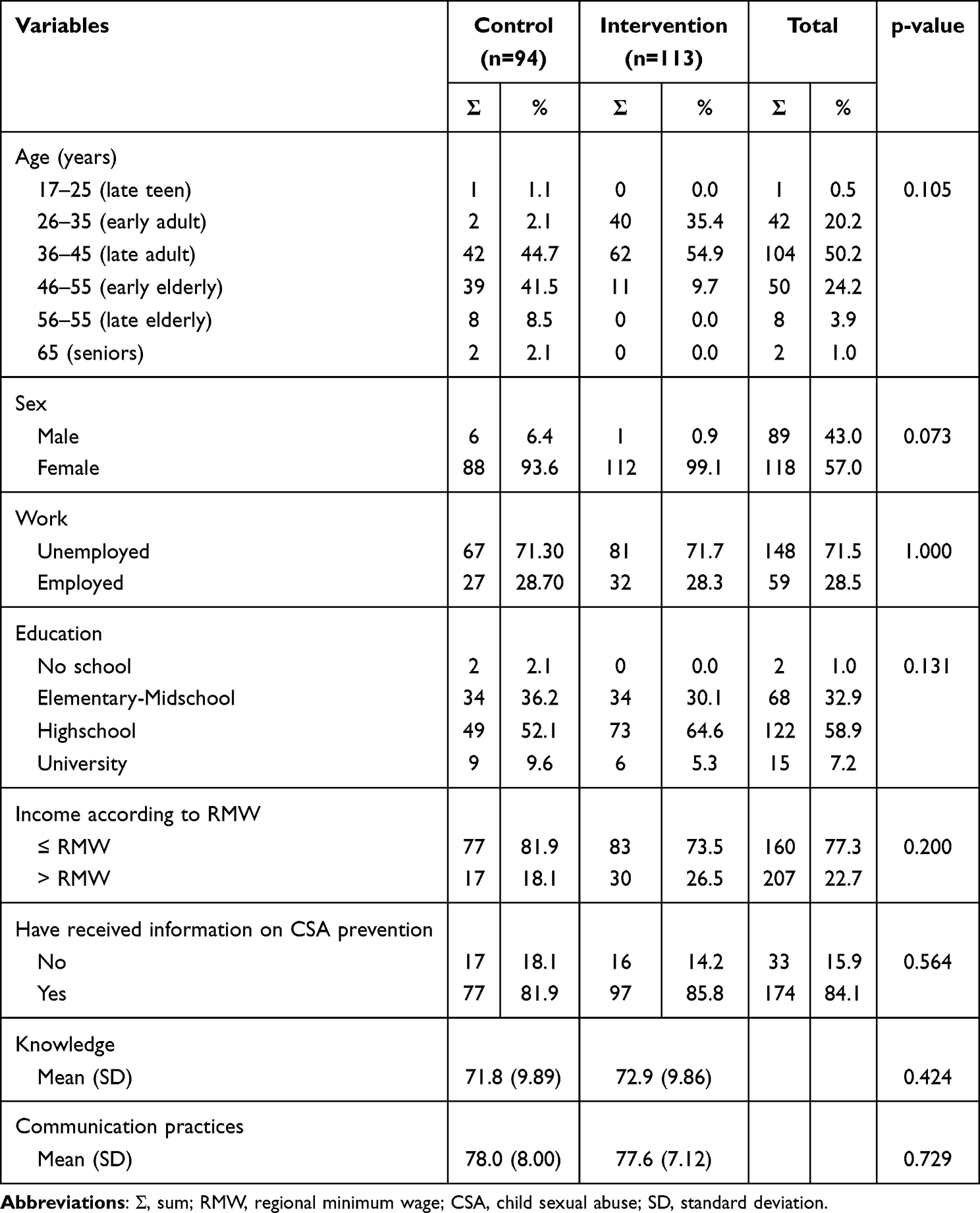 |
Table 2 Characteristic Distribution and Homogeneity Test in the Parent Group Year 2024 (n=207) |
In the teacher group, most respondents were between 26 and 45 years old (middle and late adulthood), predominantly female, had a university education, and earned above the regional minimum wage (RMW). The majority had previously received information on CSA prevention. The complete data can be seen in Table 3.
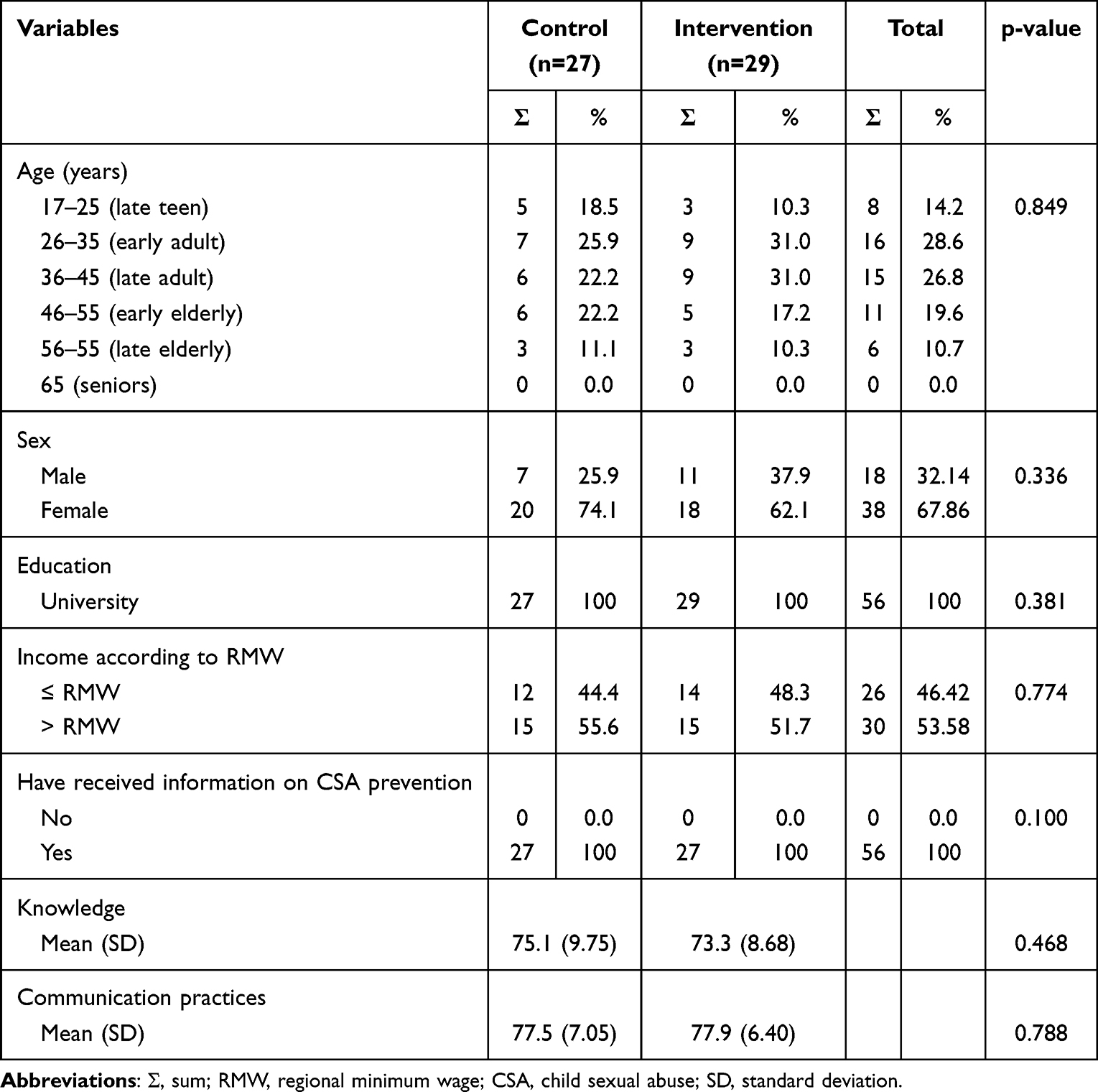 |
Table 3 Characteristic Distribution and Homogeneity Test in the Teacher Group Year 2024 (n=56) |
Pre-Test and Post-Test in All Groups
The difference between pre-test and post-test in the children group can be seen in Table 4.
 |
Table 4 Distribution of Average Pre-Test and Post-Test of Knowledge and Attitude in Children Control and Intervention Groups Year 2024 (n=212) |
- KnowledgeThe average pre-test knowledge score in the treatment group was 79.61, while that for the control group was 80.30. The average post-test knowledge score in the treatment group was 94.63, while that for the control group was 87.37. The results of the analysis showed that there was a significant difference in the average knowledge score in the treatment group (p = 0.001; α = 0.05) and the control group (p = 0.001; α = 0.05) after the post-test period.
- AttitudesThe average pre-test attitude score in the treatment group was 88.34, while for the control group it was 88.71. The average attitude score in the post-test treatment group was 98.83, while for the control group it was 96.65. The results of the analysis showed that there was a significant difference in the average attitude score in the treatment group (p = 0.001; α = 0.05) and control group (p = 0.001; α = 0.05).
The difference between pre-test and post-test in the parent group can be seen in Table 5.
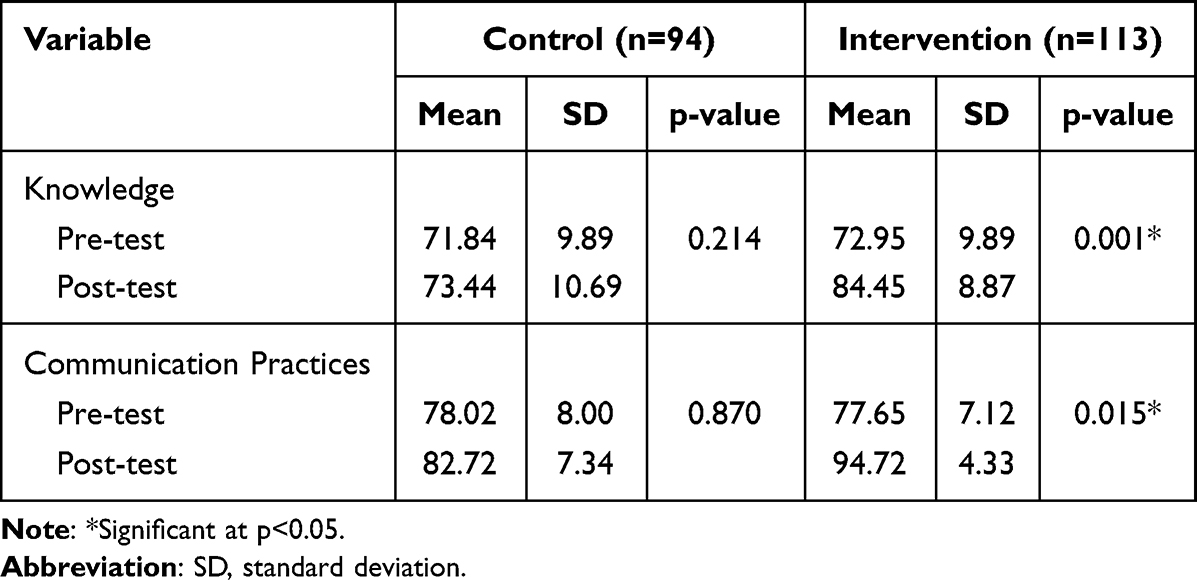 |
Table 5 Distribution of Average Pre-Test and Post-Test of Knowledge and Communication Practices in Parents Control and Intervention Groups Year 2024 (n=207) |
- KnowledgeThe average pre-test knowledge score in the treatment group was 72.95, increasing to 84.45 in the post-test, while the pre-test score in the control group was 71.84, increasing to 73.44 in the post-test. The results of the analysis showed that there was a significant difference in the average knowledge score in the treatment group after the post-test period (p = 0.001; α = 0.05), while in the control group, there was no significant difference in the average knowledge score (p = 0.214; α = 0.05).
- Communication practicesThe average pre-test score for communication practices in the treatment group was 77.65, increasing to 94.72 in the post-test, while for the control group it was 78.02, increasing to 82.72 in the post-test. The results of the analysis showed that there was a significant difference in the average score of communication practice in the treatment group (p = 0.015; α = 0.05), but there was no significant difference in the control group (p = 0.087; α = 0.05) after the post-test period.
The difference between pre-test and post-test in the teacher group can be seen in Table 6.
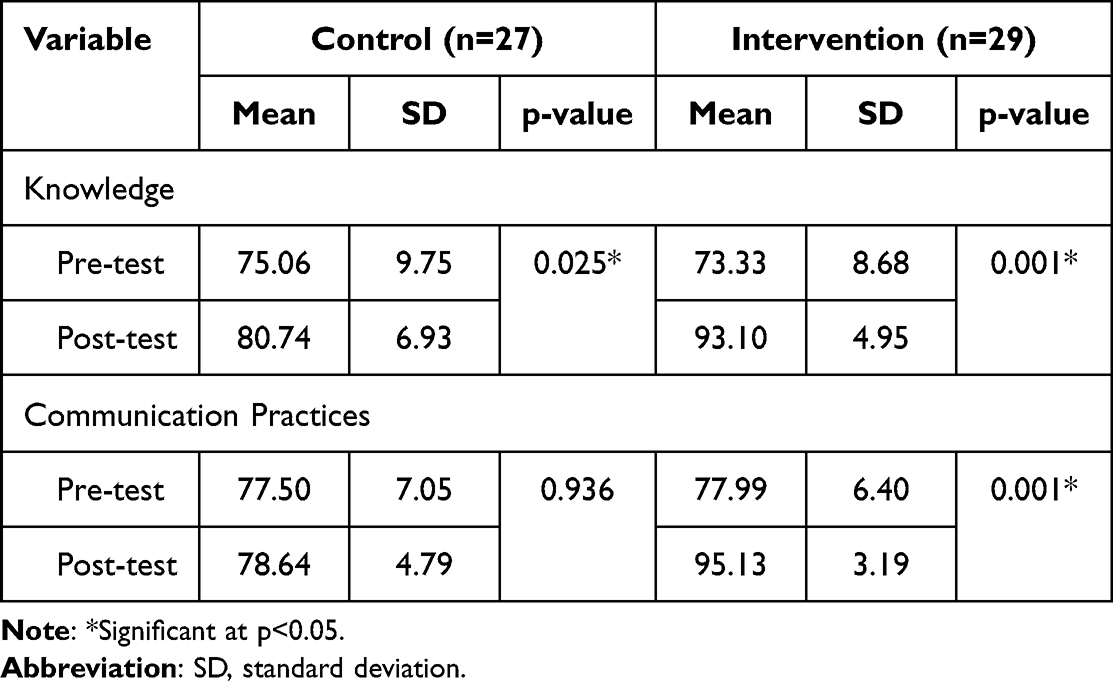 |
Table 6 Distribution of Average Pre-Test and Post-Test of Knowledge and Communication Practices in Teachers Control and Intervention Groups Year 2024 (n=56) |
- KnowledgeThe average pre-test knowledge score in the treatment group was 73.33, increasing to 93.10 in the post-test, while the pre-test score for the control group was 75.06, increasing to 80.74 in the post-test. The results of the analysis showed that there was a significant difference in the average knowledge score in the treatment group after the post-test period (p = 0.001; α = 0.05) and control (p = 0.025; α = 0.05).
- Communication practicesThe average pre-test score of communication practice in the treatment group was 77.99, increasing to 95.13 in the post-test, while the pre-test score of the control group was 77.50, increasing to 78.64 in the post-test. The results of the analysis showed that there was a significant difference in the average score of communication practice in the treatment group (p = 0.001; α = 0.05) and the control group (p = 0.936; α = 0.05) after the post-test period.
The comparison of children’s knowledge and attitude between the intervention and control groups can be seen in Table 7.
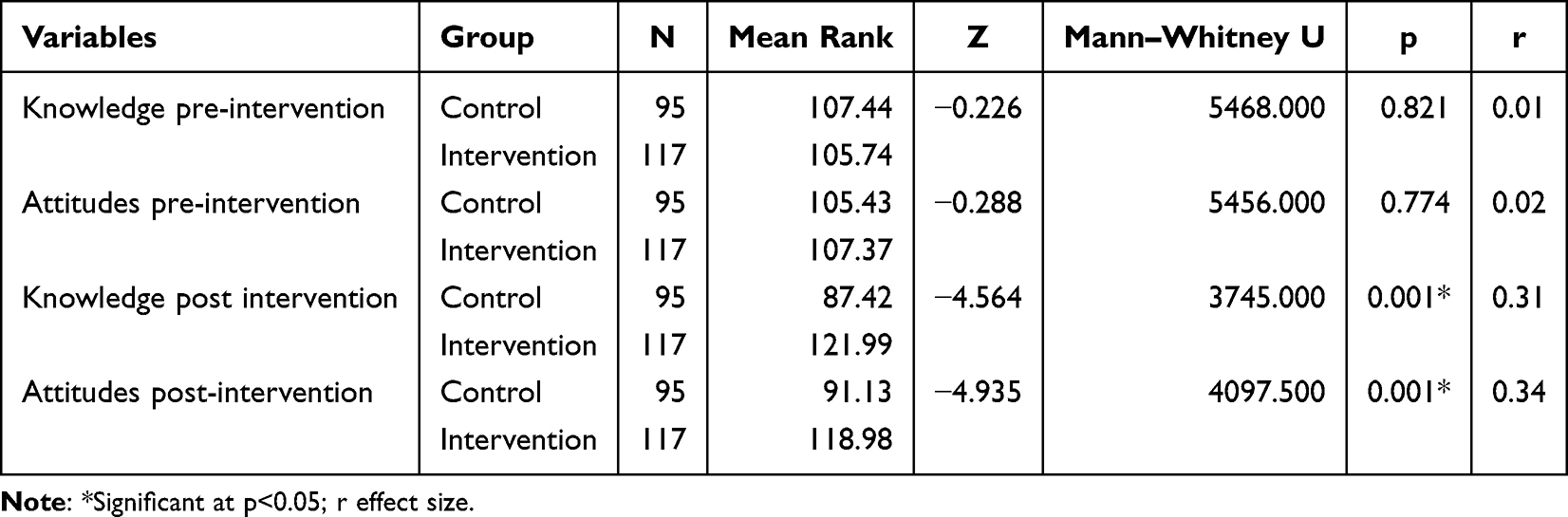 |
Table 7 Comparison of Children Knowledge and Attitude Between Intervention and Control Group Based on Mann–Whitney |
In the pre-test, no statistically significant differences were found between the intervention and control groups in either knowledge (p = 0.821, r = −0.01) or attitudes (p = 0.774, r = −0.02), indicating that both groups were comparable at baseline. After the intervention, statistically significant differences emerged in both knowledge (p = 0.001, r = −0.31) and attitudes (p = 0.001, p < 0.05, r = −0.34), representing medium effects according to Cohen’s criteria. These findings suggest that the mobile application, combined with the involvement of parents and teachers, produced moderate yet meaningful improvements in children’s knowledge and attitudes toward CSA prevention. The results highlight that the intervention was not only effective in enhancing knowledge but also in fostering more positive attitudes—an essential factor for sustaining preventive behaviours over time.
The comparison of parental knowledge and communication practice between intervention and control group can be seen in Table 8.
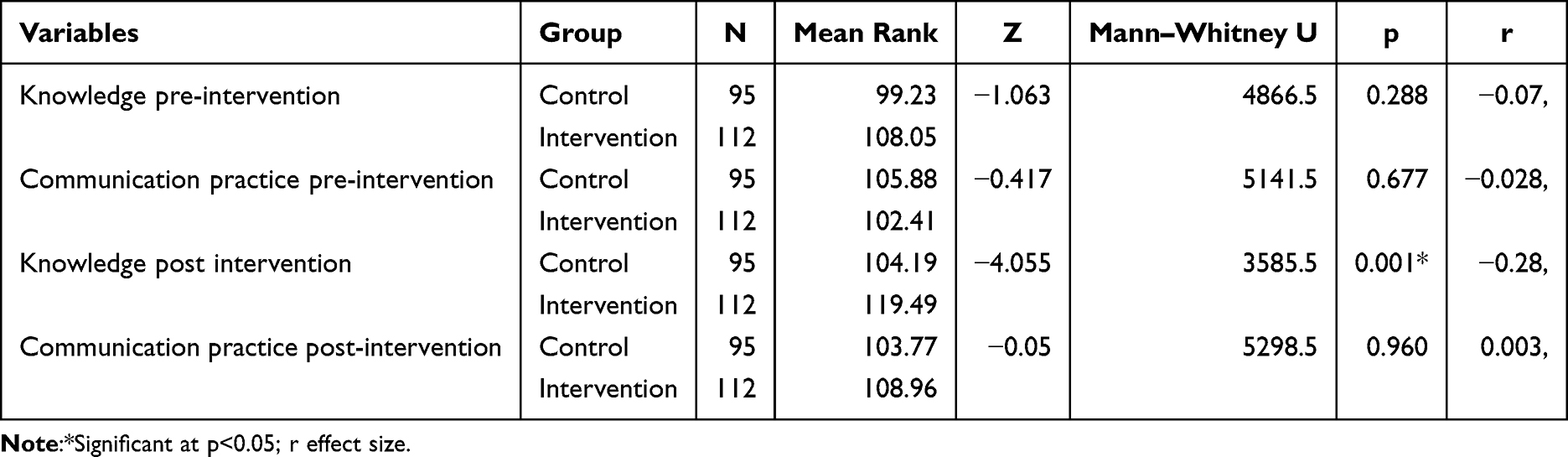 |
Table 8 Comparison of Parental Knowledge and Communication Practices Between Intervention and Control Group Based on Mann–Whitney |
Before the intervention, no statistically significant differences were observed between the control and intervention groups in parental knowledge p = 0.288, r = –0.07) or communication practice (p = 0.677, r = −0.028). After the intervention, parental knowledge showed a statistically significant difference (p = 0.001, r = –0.28), with higher post-test scores in the intervention group, indicating greater improvement compared to the control group. In contrast, parental communication practice remained statistically similar between groups (p. = 0.960, r = −0.003).
The comparison of teacher knowledge and attitude between the intervention and control groups can be seen in Table 9
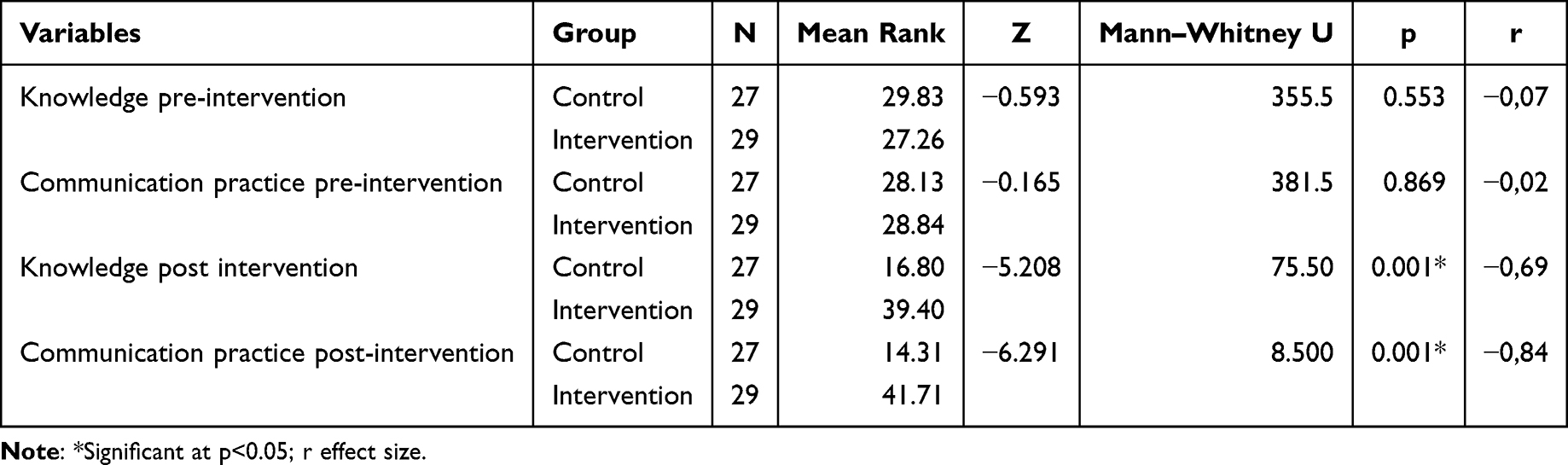 |
Table 9 Comparison of Teachers Knowledge and Communication Practices Between Intervention and Control Group Based on Mann–Whitney |
Before the intervention, no statistically significant differences were found between the control and intervention groups in either teacher knowledge (p = 0.553, r = –0.07) or communication practice (p = 0.869, r = −0.02). After the intervention, significant differences emerged in both knowledge (p = 0.001, r = –0.69) and communication practice (p = 0.001, r = –0.84), with the intervention group achieving higher scores and demonstrating greater improvements than the control group.
Discussion
This study was conducted to test the CSAP_Mob App on students’ knowledge of CSA prevention by empowering teachers and parents in implementing the intervention. The results showed a significant difference in children’s knowledge and attitude scores related to CSA prevention after the intervention. This study found that the CSAP_Mob App with parent and teacher empowerment helped improve children’s acquisition and retention of knowledge and attitudes.
The study results showed a significant increase in average pre- and post-test knowledge scores among parents and teachers in the intervention group. In contrast, no significant change was observed in the control group. Between-group comparisons confirmed that the intervention group achieved higher knowledge scores than the control group. Among child respondents, both the intervention and control groups showed significant improvements in knowledge from pre- to post-test, which may partly be explained by the Indonesian government’s concurrent implementation of a national CSA prevention program in elementary schools, providing general information and awareness activities to students and teachers. Such exposure likely contributed to the improvements observed in the control group. Nevertheless, the intervention group demonstrated significantly greater gains in knowledge scores, highlighting the added effectiveness of the CSAP_Mob application. The intervention group’s gains indicate that the mobile application, combined with active parental and teacher involvement, provided additional, targeted benefits beyond those offered by the government program. Baseline comparisons among children revealed no notable differences in knowledge between the intervention and control groups, suggesting a comparable starting point. Following the intervention, the intervention group achieved a moderate improvement in CSA prevention knowledge compared to the control group, corresponding to a medium effect size, indicating that the mobile application reinforced by parental and teacher engagement was more effective in enhancing children’s understanding of CSA prevention than the general information provided through the national school program.
The CSAP_Mob App effectively increased knowledge among parents, teachers, and children in the intervention group. Designed to educate and improve communication practices, the app helped parents and teachers absorb and relay CSA prevention information to children. Children benefited both directly from the app and through guided learning from familiar figures, enhancing their comfort and engagement. The significant knowledge improvement among parents and teachers highlights the app’s effectiveness, reinforcing the role of education in positively shaping children’s knowledge, attitudes, and behaviors.41,42 The CSAP_Mob App addresses barriers in CSA prevention, such as parents’ discomfort discussing sexual topics, beliefs that sex education is inappropriate for children, embarrassment, reliance on religious teachings, and shifting responsibility to peer groups, as reported by Wibowo (2014).43 Zakiyah et al (2016) identified three main barriers to parental knowledge in sexuality education: discomfort in discussing the topic, perception that children are not ready, and uncertainty about effective communication.44 Wilson et al (2010) highlighted that discomfort impedes effective communication about sexuality, which remains a taboo subject in Indonesian families.45 Zakiyah et al further showed that many parents perceive early sexuality education as inappropriate or equate it with teaching sexual relations.44 The CSAP_Mob App overcomes these challenges by providing culturally tailored content aligned with Indonesian values, making CSA prevention education more accessible and acceptable The app helps parents deliver sex education using simple language and engaging methods such as videos, images, TikTok, and songs, making learning appealing and cost-effective. Interactive formats enhance knowledge retention.46 Studies indicate that multimedia approaches, including songs and videos,47 effectively improve knowledge and attitudes. Web-based training further expands access to CSA prevention education, overcoming time and geographic barriers.48
The effectiveness of CSA prevention education depends on age-appropriate content and delivery methods.49,50 Parents and teachers can employ various techniques in CSA prevention programs by engaging children as both active and passive participants, with active participation involving direct engagement physically, verbally, or both, while passive participation does not require direct involvement.49,51 The CSAP_Mob App enhances parents’ and teachers’ knowledge, enabling them to transfer CSA prevention information effectively to children.
Significant improvements were observed in children’s attitudes toward CSA prevention in both the intervention and control groups from pre- to post-test, with the intervention group showing a markedly greater increase. The increase in the control group may be attributed to the recent implementation of the national CSA prevention program in elementary schools by the Indonesian government, which provided general information and awareness activities to students and teachers in both intervention and control schools. Gains in the intervention group, however, were directly linked to the CSAP_Mob App, which leveraged social media as an educational tool to reinforce positive attitudes, highlighting its value as a health education approach in the digital era.52 Comparative analysis confirmed a statistically significant difference in post-intervention attitudes between the intervention and control groups. At baseline, no significant differences were observed, confirming comparability. After the intervention, children in the intervention group demonstrated substantial improvements, while the control group showed minimal change. These findings suggest that the mobile application, combined with parental and teacher support, effectively fostered positive attitudes, which are crucial for children to adopt and sustain preventive behaviors. Overall, these results underscore the importance of integrating digital interventions with adult guidance to enhance knowledge and attitudinal readiness for CSA prevention.
Health education aims to promote health by enhancing knowledge to influence attitudes and behaviors.53 Its effectiveness depends on methods, material quality, educators, and media selection.54 Each educational medium has its strengths and limitations, making it essential to carefully select and adapt media based on the content, setting, and target audience.55 Education can be delivered through conventional54 or technology-based approaches, with the internet enabling broader access and overcoming geographical barriers.56 This allows healthcare professionals to reach more people, improving public knowledge and attitudes.
Educating children through social media platforms like the CSAP_Mob App is crucial, as they are the largest group of internet users.57 By training parents through the app, they can effectively educate their children, fostering engagement and direct guidance. Social media is widely used in Indonesia,58 making it a powerful tool for communication and learning.59 The CSAP_Mob App provides an interactive, user-friendly, and engaging approach to CSA prevention, aligning with key educational principles to positively influence attitudes and behaviors.
Parents and teachers in the intervention group significantly improved their communication practices, whereas no changes were observed in the control group. The CSAP_Mob App contributed to these gains, supporting previous findings that digital tools can facilitate preventive actions.60 Effective communication is essential for conveying CSA prevention information to children. Among parents, within-group analysis revealed progress in communication practices following the intervention; however, when compared with the control group, the difference was not statistically significant, suggesting that improvements were insufficient to create a clear distinction between groups. Contributing factors may include limited parent–child interaction time, cultural taboos around discussing sexual topics, and parents’ limited communication skills. These findings align with previous studies indicating that behavioral changes, particularly in communication, often require more time than knowledge gains. Additional strategies, such as practical communication training, social support, and reinforcement of parents’ mentoring role, are recommended to maximize the intervention’s impact. In contrast, teachers demonstrated significant improvements in communication practices both within the intervention group and compared to the control group, reflecting the ease with which professional pedagogical skills can integrate intervention materials into educational activities. Teachers’ confidence in addressing sensitive topics and their professional role in child interaction make them key agents in CSA prevention, though sustained support through school policies and ongoing training remains essential.
These findings relate closely to the fact that many parents hesitate to implement CSA prevention due to limited skills or a lack of appropriate language.22 Effective communication is a key protective factor against CSA,61 enabling parents to identify risks, set boundaries, monitor activities, and address concerns, thus strengthening prevention efforts.62 Despite societal and technological changes, 70% of Indonesian parents continue to use traditional parenting methods, according to the Indonesian Child Protection Commission.63 Many parents feel uncomfortable discussing sex, resulting in hesitation to educate their children. Research by Wibowo et al shows that most parents, despite recognizing its importance, have not provided sexuality education even as children reach adolescence.43 Modern parenting approaches emphasizing supervision, guidance, and strong parent-child communication are essential for CSA prevention.64,65 Tools like the CSAP_Mob App help parents and teachers convey CSA-related information effectively, teach self-protection skills, and educate parents on risk factors and prevention strategies, fostering safer home environments through monitoring, open discussions, and careful caregiver selection.66
Although mobile and digital interventions for CSA prevention have increased in recent years, the evidence base remains limited and heterogeneous, mainly focusing on feasibility, usability, or app evaluations67,68 rather than randomized controlled trials. This study provides novel, context-specific evidence from Indonesia, where no integrated mobile app has previously targeted children, parents, and teachers simultaneously. Findings align with previous mobile app-based CSA prevention studies,25,69 reporting increases in knowledge, awareness, and protective behaviors. Unlike most prior interventions focused solely on children, the CSAP_Mob App engages children, parents, and teachers simultaneously, reinforcing prevention messages across home and school settings. Cultural context remains central, as norms such as discomfort discussing sexual topics and gendered communication patterns can limit direct knowledge transfer but enable attitude change through modelling, empathy-building, and caregiver-led dialogue.
Finally, broader implementation of mobile-based CSA prevention programs in rural Indonesian settings faces challenges such as limited internet connectivity, lower smartphone ownership, and variable technological literacy among children, parents, and teachers, which may hinder access and engagement. To address these barriers, the CSAP_Mob App provides offline-accessible content, simplified navigation, and minimal text complexity, ensuring usability across diverse literacy levels and bridging the digital divide.70–72 While the integration of social media–inspired features (eg, TikTok-style videos) enhanced engagement, the long-term effectiveness and sustainability of such approaches require further investigation.
Despite these promising results, A methodological limitation of this study is the absence of an integrated back-end analytics dashboard to capture detailed usage data, including time spent per module, number of log-ins, or frequency of revisits. Although log-ins were tracked and sequential completion enforced, real-time automated analytics were unavailable during the trial. To ensure engagement and data credibility, multi-step verification strategies were implemented, including mandatory registration, sequential module progression, daily WhatsApp reminders, and screenshot submission of module completion. Only participants completing all nine modules were included in the analysis, reducing the risk of partial exposure. Future iterations of the app will incorporate a back-end analytics dashboard to provide comprehensive engagement tracking, enhancing the quality and robustness of subsequent evaluations.
Limitations
This study has several limitations. The CSAP_Mob app did not include an integrated analytics dashboard, so detailed usage metrics (eg, time spent per module, frequency of log-ins) were not automatically captured. The power calculation for sample size was based on children’s mean score, and it may not translate to parents’ or teachers’ knowledge outcomes. Engagement verification relied partly on participant-submitted screenshots, which may be less precise than automated tracking. The four-week intervention limits the assessment of the long-term sustainability of knowledge, attitudes, and behaviors. Furthermore, this study did not incorporate qualitative perspectives, which could have provided richer insights into participants’ experiences, perceptions, and contextual factors affecting engagement. Finally, the study was conducted in two districts of West Java, Indonesia, which may limit the generalizability of the findings to other regions with different cultural or digital access contexts.
Conclusion
CSAP Mob Application, a fully developed and functional Android-based CSA prevention tool, effectively improved knowledge and attitudes among children while simultaneously engaging parents and teachers in the prevention process. The app’s sequential learning modules, combined with daily WhatsApp reminders and screenshot verification, ensured high participant engagement and data credibility. Despite the absence of integrated back-end analytics, this study demonstrates the feasibility and potential impact of an integrated, culturally tailored mobile intervention for CSA prevention in Indonesia.
For future research, we recommend increasing the sample size to enhance statistical power and generalizability, employing cluster randomization to reduce selection bias, extending the follow-up period to assess long-term sustainability of outcomes, and including qualitative perspectives to gain deeper insights into participants’ experiences and contextual factors. Additionally, future studies could explore the role of mobile technology in educational communication, examining how mobile applications can enhance parent-child and teacher-child interactions in learning contexts alongside CSA prevention. Incorporating back-end analytics and broader accessibility features may further improve engagement, effectiveness, and scalability of the mobile CSA prevention program.
Registration
The study was registered in ClinicalTrials.gov under Identifier: NCT06752265.
IRB Approval
The study was approved by the Institutional Review Board of Universitas Padjadjaran Ethical Committee number 783/UN6.KEP/EC/2024. The study complies with the Declaration of Helsinki.
Data Sharing Statement
The corresponding author can provide the datasets created and/or examined during the current investigation upon reasonable request.
Acknowledgments
We would like to thank the Director of Research and Community Service of Universitas Padjadjaran who has assisted in this research through the Unpad Lecturer Competency Research Grant or Hibah Riset Kompetensi Dosen Unpad (RKDU) 2024.
Funding
We would like to thank the Director of Research and Community Service of Universitas Padjadjaran who has assisted in this research through the Unpad Lecturer Competency Research Grant or Hibah Riset Kompetensi Dosen Unpad (RKDU) 2024, under grant number 1909/UN6.3.1/PT.00/2024.
Disclosure
The authors report no conflicts of interest in this study.
References
1. Abourjaily E, Guastaferro K, McElwee K, Connell CM. Universal parent-focused child sexual abuse prevention: a quasi-experimental protocol. PLoS One. 2025;20(1):e0314459. doi:10.1371/journal.pone.0314459
2. World Health Organization. Responding to Children and Adolescents Who Have Been Sexually Abused: WHO Clinical Guidelines; 2017.
3. Al-rasheed M. Child sexual abuse prevention programs for kindergartners: a survey of public actions, attitudes, and beliefs in Kuwait. Child Adolesc Social Work J. 2017;34(4):361–368. doi:10.1007/s10560-016-0466-0
4. Choudhary V, Satapathy S, Sagar R. Qualitative study on the impact of child sexual abuse: perspectives of children, caregivers, and professionals in indian context. J Child Sexual Abuse. 2019;28(4):489–510. doi:10.1080/10538712.2018.1563262
5. Tardif-Williams CY, Tanaka M, Boyle MH, MacMillan HL. The impact of childhood abuse and current mental health on young adult intimate relationship functioning. J Interpers Violence. 2017;32(22):3420–3447. doi:10.1177/0886260515599655
6. Salloum A, Johnco C, Zepeda-Burgos RM, et al. Parents’ knowledge, attitudes, and experiences in child sexual abuse prevention in El Salvador. Child Psychiatry Human Dev. 2020;51(3):343–354. doi:10.1007/s10578-019-00946-w
7. Basilyous L, Durgampudi P. Child sexual abuse in Saint Lucia. Int Public Health J. 2016;8(3):365–370.
8. LPSK. Lembaga perlindungan Saksi dan Korban 2019. Available from: https://lokadata.id/artikel/2020-kekerasan-pada-anak-tak-menurun.
9. Jabar Lawan Kekerasan Seksual terhadap Anak. 2016. Available from: http://bappeda.jabarprov.go.id/jabar-lawan-kekerasan-seksual-terhadap-anak/.
10. Sundari. Jawa barat darurat kekerasan seksual terhadap anak. Majalah Tempo. 2014.
11. Solehati T, Pramukti I, Kosasih CE, Hermayanti Y, Mediani HS. Determinants of sexual abuse prevention knowledge among children’s schools in west java indonesia: a cross-sectional study. Soc Sci. 2022;11(8):337. doi:10.3390/socsci11080337
12. Solehati T, Kosasih CE, Hermayanti Y, Mediani HS. Child sexual abuse prevention: a qualitative study of teachers’ educational needs. Belitung Nurs J. 2023;9(6):554–562. doi:10.33546/bnj.2792
13. Presiden Republik Indonesia. Undang-Undang Republik Indonesia Nomor 23 Tahun 2002 Tentang Perlindungan Anak. Jakarta: Negara Republik Indonesia; 2002.
14. Presiden Republik Indonesia. Undang-Undang Republik Indonesia Nomor 12 Tahun 2022 Tentang Tindak Pidana Kekerasan Seksual. Jakarta: Negara Republik Indonesia; 2022.
15. Kementerian Pemberdayaan Perempuan dan Perlindungan Anak. Pedoman Perlindungan Anak Terpadu Berbasis Masyarakat (PATBM), Edisi I. 2015.
16. Kim S-J, Kang K-A. Effects of the child sexual abuse prevention education (C-SAPE) program on South Korean fifth-grade students’ competence in terms of knowledge and self-protective behaviors. J School Nurs. 2017;33(2):123–132. doi:10.1177/1059840516664182
17. Utami PN. Pencegahan kekerasan terhadap anak dalam perspektif hak atas rasa aman di nusa tenggara barat. Jurnal HAM. 2018;9(1):1–17. doi:10.30641/ham.2018.9.1-17
18. Wismayanti YF, O’Leary P, Tilbury C, Tjoe Y. Child sexual abuse in Indonesia: a systematic review of literature, law and policy. Child Abuse Negl. 2019;95:104034. doi:10.1016/j.chiabu.2019.104034
19. Kenny MC, Wurtele SK. Preventing childhood sexual abuse: an ecological approach. J Child Sexual Abuse. 2012;21(4):361–367. doi:10.1080/10538712.2012.675567
20. Yıldız G, Cavkaytar A. Effectiveness of a sexual education program for mothers of young adults with intellectual disabilities on mothers’ attitudes toward sexual education and the perception of social support. Sexual Disabil. 2017;35(1):3–19. doi:10.1007/s11195-016-9465-5
21. Lak P, Noroozi M, Ehsanpoor S. Comparing the effect of two methods of group education and education by multimedia compact disk on mothers’ knowledge and attitude about child sexual abuse. Ann Trop Med Public Health. 2017;10(6):1720. doi:10.4103/ATMPH.ATMPH_610_17
22. Babatsikos G. Parents’ knowledge, attitudes and practices about preventing child sexual abuse: a literature review. Child Abuse Review. 2010;19(2):107–129. doi:10.1002/car.1102
23. Kemen PPPA. Kekerasan anak masih marak terjadi, perkuat sdm penyedia layanan perlindungan anak 2020. Available from: https://kemenpppa.go.id/index.php/page/read/29/2911/kekerasan-anak-masih-marak-terjadi-perkuat-sdm-penyedia-layanan-perlindungan-anak.
24. Brassard MR, Fiorvanti CM. School‐based child abuse prevention programs. Psychol Schools. 2015;52(1):40–60. doi:10.1002/pits.21811
25. Moon KJ, Park KM, Sung Y. Sexual Abuse Prevention Mobile Application (SAP_MobAPP) for primary school children in Korea. J Child Sexual Abuse. 2017;26(5):573–589. doi:10.1080/10538712.2017.1313350
26. Dale R, Shanley DC, Zimmer-Gembeck MJ, Lines K, Pickering K, White C. Empowering and protecting children by enhancing knowledge, skills and well-being: a randomized trial of Learn to BE SAFE with Emmy™. Child Abuse Negl. 2016;51:368–378. doi:10.1016/j.chiabu.2015.07.016
27. Rheingold A, Danielson C, Davidson T, Self-Brown S, Resnick H. Video intervention for child and caregiver distress related to the child sexual abuse medical examination: a randomized controlled pilot study. J Child Family Stud. 2013;22(3):386–397. doi:10.1007/s10826-012-9591-3
28. Chen Y-C, Fortson BL, Tseng K-W. Pilot evaluation of a sexual abuse prevention program for Taiwanese children. J Child Sexual Abuse. 2012;21(6):621–645. doi:10.1080/10538712.2012.726699
29. Baker CK, Naai R, Mitchell J, Trecker C. Utilizing a train-the-trainer model for sexual violence prevention: findings from a pilot study with high school students of Asian and Pacific Islander descent in Hawai ‘i. Asian Am J Psychol. 2014;5(2):106–115. doi:10.1037/a0034670
30. Green L, Kreuter MW. Health Program planning:An Educational and Ecological Approach.
31. Bandura A. Social foundations of thought and action: a social cognitive theory. 1986;1986:2.
32. Luik J, Setiawan D, Sitindjak RHI. Media logic and educational micro-content: presentational themes and approaches on TikTok. Commun Rev. 2025;28(2):170–196. doi:10.1080/10714421.2025.2452086
33. Montag C, Yang H, Elhai JD. On the psychology of tiktok use: a first glimpse from empirical findings. 2021;9–2021.
34. Wulandari RT, Anisa N. Development of thematic-based motion and song learning videos to stimulate work: art of kindergarten teacher’s ability. Universal J Educ Res. 2019;7(12A):27–34. doi:10.13189/ujer.2019.071904
35. Research Institute I. Indonesia Gen Z Report. IDN Times 2022; Available from: https://cdn.idntimes.com/content-documents/indonesia-gen-z-report-2022.pdf.
36. Pedrouzo SB, Krynski L. Hyperconnected: children and adolescents on social media. The TikTok phenomenon. Arch Argent Pediatr. 2023;121(4):e202202674. doi:10.5546/aap.2022-02674.eng
37. Solehati T. Pengembangan Mobile Application Pencegahan Kekerasan Seksual Anak Usia Sekolah Dasar Dengan Melibatkan Peran Orang Tua dan Guru Sekolah di Jawa Barat. Bandung, Jawa Barat, Indonesia, Fakultas Kedokteran Universitas Padjadjaran (Dissertation, Unpublished) 2023.
38. Cohen J. Statistical power analysis for the behavioral sciences–second edition. 12 lawrence erlbaum associates Inc. Hillsdale New Jersey. 1988;13.
39. Czerwinski F, Finne E, Alfes J, Kolip P. Effectiveness of a school-based intervention to prevent child sexual abuse—Evaluation of the German IGEL program. Child Abuse Negl. 2018;86:109–122. doi:10.1016/j.chiabu.2018.08.023
40. Polit DF, Beck CT. Study Guide for Essentials of Nursing Research: Appraising Evidence for Nursing Practice. Lippincott Williams & Wilkins; 2013.
41. Bieri FA, Gray DJ, Williams GM, et al. Health-education package to prevent worm infections in Chinese schoolchildren. N Engl J Med. 2013;368(17):1603–1612. doi:10.1056/NEJMoa1204885
42. Iskandarsyah A, Shabrina A, Siswadi AGP. Usability and acceptability of JAGA SEHAT: mobile application to improve knowledge about healthy lifestyle. J Multidiscip Healthc. 2022;15(null):115–124. doi:10.2147/JMDH.S342913
43. Wibowo RS. Fungsi Orang Tua dalam Sosialisasi Pendidikan Seks Kepada Remaja. Solidarity. 2014;3(1).
44. Zakiyah R, Prabandari YS, Triratnawati A. Tabu, hambatan budaya pendidikan seksualitas dini pada anak di Kota Dumai. Berita Kedokteran Masyarakat. 2016;32(9):323–330. doi:10.22146/bkm.10557
45. Situmorang A. Adolescent Reproductive Health in Indonesia. Jakarta: STARH Program; 2003.
46. Hung IC, Kinshuk, Chen N-S, Chen N-S. Embodied interactive video lectures for improving learning comprehension and retention. Comput Educ. 2018;117:116–131. doi:10.1016/j.compedu.2017.10.005
47. Solehati T, Maryati I, Kosasih CE, Hermayanti Y, Mediani HS. Effect of sexual abuse prevention education using video and song on knowledge and attitudes of elementary school students: a pilot study. Malaysian J Med Health Sci. 2022;18(SUPP3):91–95.
48. Rheingold AA, Zajac K, Patton M. Feasibility and acceptability of a child sexual abuse prevention program for childcare professionals: comparison of a web-based and in-person training. J Child Sexual Abuse. 2012;21(4):422–436. doi:10.1080/10538712.2012.675422
49. Martyniuk H, Dworkin E. Child Sexual Abuse Prevention: Programs for Children. National Sexual Violence Resource Center; 2011. 1.
50. Walsh K, Zwi K, Woolfenden S, Shlonsky A. School‐based education programmes for the prevention of child sexual abuse. Cochrane Database Syst Rev. 2015(4).
51. Walsh K, Zwi K, Woolfenden S, Shlonsky A. School-based education programmes for the prevention of child sexual abuse. Cochrane Database Syst Rev. 2015;2015(4):CD004380. doi:10.1002/14651858.CD004380.pub3
52. Puspitasari IW, Wulandari D, Duhida F. Hubungan pemanfaatan media internet dengan sikap siswa terhadap kemampuan dalam antisipasi tindak KSA (Kekerasan Seksual Anak) di pengajian anak-anak Al-Falaah blunyahgede yogyakarta. Jurnal Kesehatan Vokasional. 2017;2(2):182–190. doi:10.22146/jkesvo.30334
53. Glanz K, Rimer B, Viswanath K. Health Behavior and Health Education: Theory, Research and Practice.(Jossey-Bass). San Francisco, CA, USA; 2008.
54. Notoatmodjo S. Konsep Perilaku Kesehatan Dalam: Promosi Kesehatan Teori & Aplikasi Edisi Revisi. Jakarta: 2010.
55. Gejir IN, Agung AAG, Ratih IADK, et al. Media Komunikasi Dalam Penyuluhan Kesehatan. Penerbit Andi; 2017.
56. Maryono Y, Istiana BP. Teknologi Informasi Dan Komunikasi. Bandung. 2008.
57. Vlachopoulou E, Boutsouki C. Facebook usage among teenagers–the effect of personality and peer group pressure; an exploratory study in Greece. Int J Internet Market Adver. 2014;8(4):285–299. doi:10.1504/IJIMA.2014.067661
58. APJII.Laporan survei penetrasi & profil perilaku pengguna internet Indonesia. 2018.
59. Patino A, Pitta DA, Quinones R. Social media’s emerging importance in market research. J Consum Market. 2012;29(3):233–237. doi:10.1108/07363761211221800
60. Cho H-J, Kim J-M. Development of conversion smart monitoring app for elementary school student. J Digital Convergence. 2015;13(4):211–217. doi:10.14400/JDC.2015.13.4.211
61. Rudolph J, Zimmer-Gembeck MJ, Shanley DC, Hawkins R. Child sexual abuse prevention opportunities: parenting, programs, and the reduction of risk. Child Maltreatment. 2018;23(1):96–106. doi:10.1177/1077559517729479
62. Wong PY, How CH, Yi Wong PC. Management of child abuse. Singapore Med J. 2013;54(10):533–537. doi:10.11622/smedj.2013196
63. Setyawan D. KPAI: pelaku kekerasan terhadap anak tiap tahun meningkat. Komisi Perlindungan Anak Indonesia. 2015.
64. Ardiana DPY, Loekito LH. Perancangan multimedia interaktif untuk materi perlindungan anak terhadap pelecehan seksual berbasis mobile. 2019.
65. Breiding MJ, Reza A, Gulaid J, et al. Risk factors associated with sexual violence towards girls in Swaziland. Bulletin of the World Health Organization. 2011;89(3):203–210. doi:10.2471/BLT.10.079608
66. Mendelson T, Letourneau EJ. Parent-Focused prevention of child sexual abuse. Prevent Sci. 2015;16(6):844–852. doi:10.1007/s11121-015-0553-z
67. Malamsha MP, Sauli E, Luhanga ET. Development and validation of a mobile game for culturally sensitive child sexual abuse prevention education in tanzania: mixed methods study. JMIR Serious Games. 2021;9(4):e30350. doi:10.2196/30350
68. Zerin M, Rahman SMS, Fahmida NN, Zerin SN, Islam MN. Evaluating and developing educational gaming applications to raise awareness of child sexual abuse.
69. Kang SR, Kim S-J, Kang K-A. Effects of child sexual abuse prevention education program using hybrid application (CSAPE-H) on Fifth-Grade students in South Korea. J School Nurs. 2022;38(4):368–379. doi:10.1177/1059840520940377
70. Lavrinenko O, Ignatjeva S, Betlej A, Danileviča A, Menshikov V, Rybalkin O. Mobile internet in the EU: problems and perspectives. Entrepreneurship Sustainability Issues. 2022;9(3):369–383. doi:10.9770/jesi.2022.9.3(22)
71. Delaporte A, Bahia K. The State of Mobile Internet Connectivity 2022. GSMA; 2022.
72. Qiang Z. Digital Progress and Trends Report 2023. The World Bank Washington, DC; 2024.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.