Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Empirical Study on the Operational Status and Key Influencing Factors of Outpatient Multidisciplinary (MDT) Service Model: A Cross-Sectional Study in Sichuan Province, China
Authors Wang H ![]() , He Q, Guo Y, Feng G, He X, Wan Z
, He Q, Guo Y, Feng G, He X, Wan Z
Received 15 March 2025
Accepted for publication 13 July 2025
Published 31 July 2025 Volume 2025:18 Pages 4431—4442
DOI https://doi.org/10.2147/JMDH.S528489
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
HuanLin Wang,1,2 Qian He,1,2 Yuan Guo,2 GuoWen Feng,1,2 Xuan He,1,2 Zhi Wan1,2
1Rare Diseases Center West China Hospital of Sichuan University, Chengdu, Sichuan, People’s Republic of China; 2Department of Outpatient West China Hospital of Sichuan University, Chengdu, Sichuan, People’s Republic of China
Correspondence: Zhi Wan, Email [email protected]
Background: Currently, there is a lack of baseline research on outpatient Multi-Disciplinary Team (MDT) services. Through conducting a cross-sectional survey in Sichuan Province, China, this study aims to explore the current status and influencing factors of outpatient MDT services, providing a reference for their further development.
Methods: A questionnaire survey was conducted in June 2024 on tertiary medical institutions in Sichuan Province using the cluster sampling method. A total of 203 valid questionnaires were collected, yielding an effective response rate of 91.0%. Descriptive statistics, correlation, and difference tests were employed to analyze the survey data.
Results: The development rate of outpatient MDT in tertiary medical institutions in Sichuan Province was 77.3%, and the start-up time was mainly concentrated in the past five years. About 87.3% of the hospitals set up fixed MDT teams with the number of ≤ 10, which was still in the development stage. In terms of MDT organization and management, 96.8% of the hospitals have issued relevant management systems, but the cognitive differences of MDT function positioning lead to significant heterogeneity in organization and management and operation mode. The analysis of key influencing factors shows that team dynamics is the primary internal driving factor, while medical insurance policy is the primary external influencing factor.
Conclusion: Medical institutions need to promote the standardized development of outpatient MDT from the two dimensions of system construction and mechanism innovation: first, improve the institutionalized management framework: integrate the core link of MDT into the hospital quality management system through the construction of standardized workflow. Second, establish a refined assessment mechanism: focus on process indicators such as the standardized rate of case discussion and the implementation rate of the scheme, support an interdisciplinary performance incentive system, and mobilize the enthusiasm of departments and doctors to promote their rapid development.
Keywords: multi-disciplinary team, outpatient MDT, current situation survey, influence factor
Introduction
With the evolution of the medical model and the increasing demand for individualized patient care, the multi-disciplinary team (MDT) model has emerged as a crucial component in the modern healthcare system.1,2 By harnessing the specialized knowledge and skills of various disciplines, the MDT model offers patients a holistic and tailored diagnosis and treatment plan, thereby enhancing diagnostic and treatment efficiency, improving patient prognosis, and boosting patient satisfaction.3 The concept of MDT mode originated from the pilot of diagnosis and treatment of difficult and difficult diseases in children in the 1960s. Early practice emphasized the importance of multidisciplinary cooperation.4,5 Since then, European and American countries have taken the lead in promoting the MDT model in the field of cancer. In 1993, the United Kingdom incorporated the MDT model into the community health care system.6 In 1997, the International Working Group on Colorectal Cancer (IWGCRC) clearly recommended the MDT model and stipulated the composition of MDT members.7 In 2007, the United Kingdom passed the National Health Service System (NHS) tumor diagnosis and treatment specification legislation, which stipulates that all tumor patients must go through MDT discussion, laying the core position of MDT in tumor diagnosis and treatment.8 In 2013, the European Union listed MDT as the key link of cancer treatment through the policy statement of the European cooperation for action against cancer (EPAAC).9,10 At present, European and American countries have successively established localized MDT implementation systems, and gradually formed a whole process management mode covering pre-diagnosis evaluation, clinical decision-making and postoperative follow-up.11–13
Compared with developed countries in Europe and the United States, China’s adoption of MDT model started relatively late. In 2010, the former Ministry of Health of China introduced the MDT model in the Code for《Diagnosis and Treatment of Colorectal Cancer (2010 Edition)》.14 Thanks to policy guidance and innovative exploration by medical institutions, three types of MDT models have gradually emerged: outpatient, inpatient, and remote MDT. The outpatient MDT is a team composed of relatively fixed experts from at least three related disciplines. For a certain disease with complex condition, multidisciplinary expert discussions are held at regular intervals and locations in the outpatient department to formulate the best diagnosis and treatment scheme for patients. In the context of China’s national conditions, outpatient MDT, as a new diagnosis and treatment model, has been widely promoted and rapidly developed in large domestic hospitals.15,16 However, owing to the vast territory and the varying economic and cultural landscapes across different regions, as well as significant disparities in medical development levels, outpatient MDT currently lacks a unified standard in areas such as team construction, operational models, process management, and quality control. This has led to uneven development, impeding the promotion of outpatient MDT.14,17
Guided by the needs of industry development, the research team conducted a baseline survey on the current implementation status of outpatient multidisciplinary team (MDT) clinics in tertiary public hospitals in Sichuan Province. Through in-depth mining and analysis of the survey data, this study aims to understand the implementation status of tertiary public hospitals in western China, identify key issues and core needs in outpatient MDT practices, and explore internal and external influencing factors affecting the development of outpatient MDT. The findings are expected to provide references for the further promotion and standardization of the outpatient MDT model.
Methods
Research Object
The respondents were managers of outpatient departments of tertiary public medical institutions from 18 prefecture level cities and 3 autonomous prefectures in Sichuan Province.
Investigation Methods
On the basis of consulting a large number of literatures, combined with the actual operation characteristics of outpatient MDT work, the researchers designed a questionnaire under the guidance of experts. The questionnaire covers five dimensions, including the basic situation of medical institutions, the current situation of outpatient MDT, organization and management, quality control and internal and external factors affecting the development of MDT, with a total of 42 items. In terms of sampling method, the research team determined that the minimum sample size to meet the requirements of statistical analysis was 168 based on the total number of tertiary public hospitals in Sichuan Province in 2021 (n = 299) in the 2022 China Health Statistical Yearbook, using the stratified sampling sample size calculation formula. In view of the homogeneity of the three-level hospital management system, the study adopted the cluster sampling method. With the strong support of Sichuan outpatient management medical quality control center, the questionnaire was distributed to the three-level public medical institutions in the province in the form of electronic questionnaire (questionnaire star) on June 27, 2024. Strict quality control is implemented in this survey: the director of the outpatient department is limited to be the only person responsible for filling in and submitting only one questionnaire in each institution to ensure the professionalism and uniqueness of the data source.
Statistical Methods
IBM SPSS 25.0 software was used to establish the database and analyze the survey data. Qualitative data such as the basic situation, development status and organization management of medical institutions were analyzed by descriptive statistics, expressed in frequency and percentage. The influencing factors of outpatient MDT were analyzed using chi-square test and Mann–Whitney U-test for univariate correlation analysis. The comparative analysis of internal and external influencing factors scores of MDT between grade III grade A hospitals and grade B hospitals was conducted by Mann Whitney U-test of independent samples. P < 0.05 means statistically significant.
Results
Reliability and Validity Analysis
This study employed Cronbach’s alpha coefficient to assess the reliability of the questionnaire. The results indicated that Cronbach’s alpha was 0.891, exceeding the threshold of 0.70, thus demonstrating high internal consistency and good reliability of the questionnaire. To validate the structural validity of the questionnaire, we utilized the KMO (Kaiser-Meyer-Olkin) measure and the Bartlett’s test of sphericity. The KMO value of 0.852 signifies that the questionnaire data is suitable for factor analysis. Additionally, the P-value from Bartlett’s test of sphericity was less than 0.05, indicating statistical significance, further affirming the good structural validity of the questionnaire data.
Basic Information of Medical Institutions
A total of 223 questionnaires were collected in this survey, of which 203 were valid, resulting in an effective response rate of 91.0%. According to descriptive statistical analysis, there are 108 tertiary Grade III Class A hospitals (53.2%) and 95 tertiary Grade III Class A hospitals (46.8%). The types of hospitals include 138 comprehensive hospitals (68.0%), 29 specialist hospitals (14.3%), and 36 traditional Chinese medicine hospitals (17.7%). There are 11 hospitals with annual outpatient volume of less than 100,000 (5.4%) person-times, 106 hospitals with 100,000 to 500,000 (52.2%) person-times, 53 hospitals with 500,000 to 1 million (26.1%) person-times, and 33 hospitals with over 1 million (16.3%) person-times. There are 8 hospitals with annual discharge of less than 5,000 patients (3.9%) person-times, 18 hospitals with 5,000 to 10,000 patients (8.9%) person-times, 128 hospitals with 10,000 to 50,000 patients (63.1%) person-times, and 49 hospitals with over 50,000 patients (24.1%) person-times.
Current Status of Outpatient MDT Operations
Out of 203 hospitals, 157 have implemented outpatient MDT, with an implementation rate of 77.3%. Among them, 114 (72.6%) hospitals have designated personnel for managing outpatient MDT, and 135 (86.0%) hospitals have established dedicated MDT consultation rooms for this purpose. The statistical analysis reveals a significant correlation between the implementation of outpatient MDT services and factors such as hospital level, hospital type, average annual outpatient volume, and average annual discharge volume, with a P-value of less than 0.001 (For further details, please refer to Table 1).
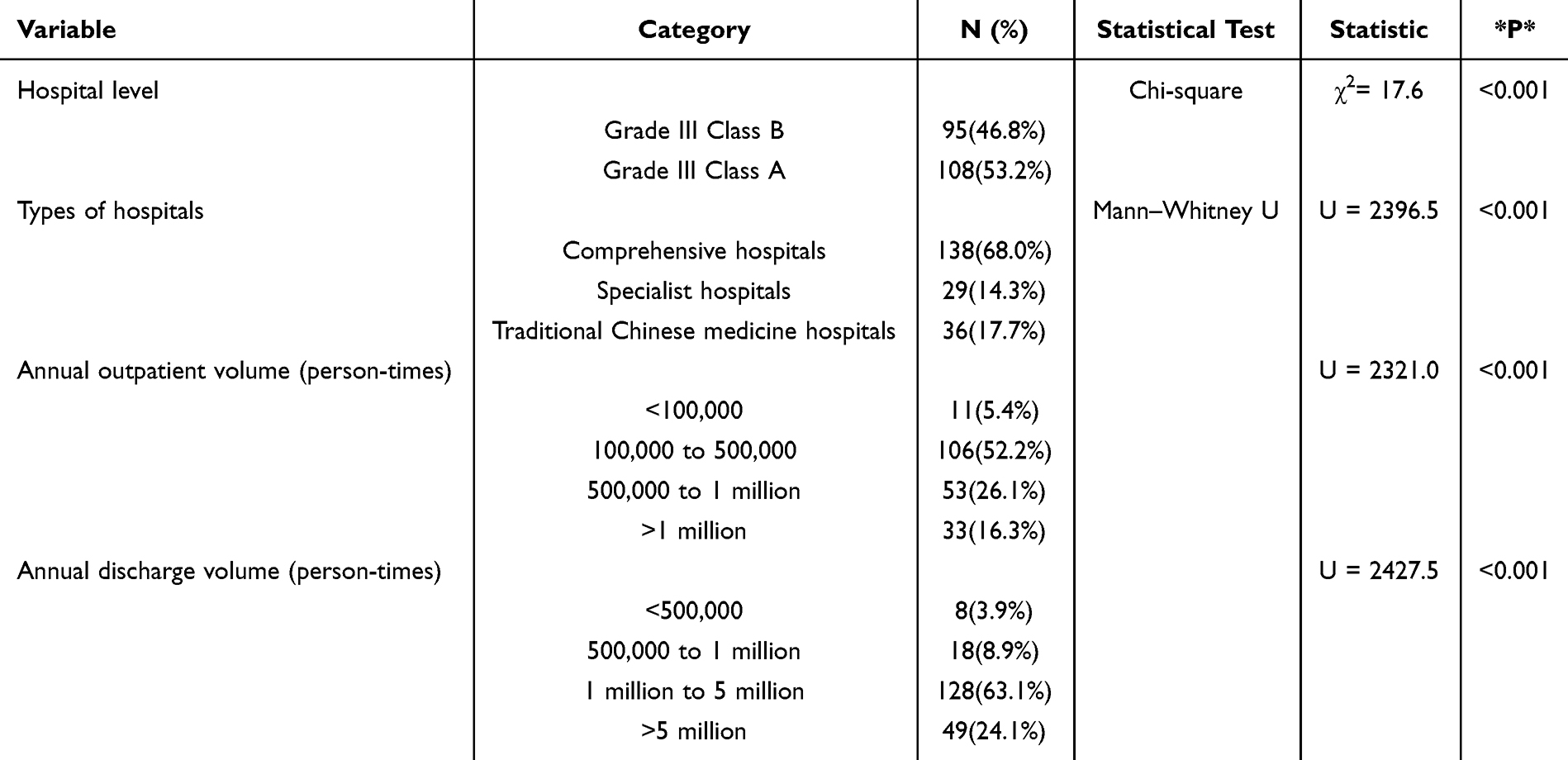 |
Table 1 Correlation Analysis of Outpatient MDT Service Implementation |
The forms of outpatient MDT, ranked from most common to least common, are: offline MDT meetings (98.7%), remote collaboration MDT between medical institutions (21.0%), internet hospital online MDT (12.1%), and others (7%). Other forms of implementation include the MDT discussion format that combines online and offline methods. This format involves some experts offline and some online, utilizing remote application systems to conduct interdisciplinary discussions across time and space, and develop diagnosis and treatment plans for patients. Among the 157 hospitals that have carried out outpatient MDT, 58 (36.9%) implement the three fixed modes of MDT (fixed personnel, time, and location), while 30 (19.1%) hospitals do not have fixed personnel, time, and location for MDT operation. They mainly form expert teams and arrange interdisciplinary discussions on a temporary basis to meet the personalized diagnosis and treatment needs of patients. There are various ways to make appointments for outpatient MDT, and the proportion of appointment methods from high to low is doctor recommendation (77.7%), on-site review application (74.5%), online appointment for patients (36.9%), and out of hospital referral (18.5%).
About 87.3% of the hospitals had less than 10 outpatient MDT categories, and 89.1% of the hospitals had an average monthly MDT service volume of 50 people or less. Among the 157 hospitals that have implemented outpatient MDT, 14 (8.9%) have established MDT for rare diseases. The five most commonly developed rare disease MDT categories are neuroendocrine tumors, amyloidosis, neurofibroma, retinoblastoma, and hypertrophic cardiomyopathy.
In terms of information construction, 36 (22.9%) hospitals have specialized information system support work, of which 33 (21.0%) hospitals have built standardized MDT database to manage patients (see Table 2 for details).
 |
Table 2 Outpatient MDT Operation Status (N = 203) |
In terms of charging standards, currently outpatient MDT in Sichuan Province has not been included in medical insurance reimbursement. About 88 (56.1%) of the government departments in the urban areas where hospitals are located have issued clear outpatient MDT charging standards. Out of 88 hospitals, 56 (63.6%) have a charging standard of 400 RMB or less per patient visit, while 32 (36.4%) have a charging standard of 401–600 RMB per patient visit.
Outpatient MDT Organizational Management
The survey results showed that 152 (96.8%) hospitals had a clear outpatient MDT system, 111 (70.7%) hospitals had a standard approval process for the establishment of outpatient MDT, 121 (77.1%) hospitals required at least three or more departments to form an MDT team, while 36 (22.9%) hospitals formed an MDT team on demand, without the requirement of the number of departments.
In terms of personnel management, regarding the qualification requirements for MDT team leaders: 79.7% of hospitals demand that the MDT leader should hold the qualification of Senior Registrar; 14.0% of hospitals require the MDT leader to have at least 5 years of experience as a Registrar; 6.4% of hospitals have no specific requirements. As for the qualification criteria for MDT team participating experts: 52.2% of hospitals insist that MDT participating experts must meet the criteria of Senior Registrar; 40.1% of hospitals demand that participating experts have at least 5 years of experience as a Registrar; 7.7% of hospitals have no such requirements. Furthermore, 75.2% of hospitals’ MDT teams are supported by dedicated secretaries to assist with team work, and 88.5% of hospitals provide training for MDT team members.
In terms of operation and management, 61 hospitals (38.9%) have established inclusion criteria for MDT team discussions, while 96 hospitals (61.2%) lack specific inclusion criteria. It is up to the MDT team experts to review and decide whether patients require an MDT discussion. Among the 157 hospitals that have implemented outpatient MDT, 70.1% assess doctors’ visits to the MDT clinic through the following methods: manual check-in (63.1%) and system check-in (7.0%). Additionally, 94 hospitals (59.9%) currently utilize MDT electronic medical records and 134 hospitals (85.4%) conduct follow-up management for patients after diagnosis (See Table 3 for details).
 |
Table 3 Outpatient MDT Quality Management |
In terms of performance management and incentive mechanisms, among the 157 hospitals that have implemented outpatient MDT, 56 (35.7%) have incorporated the workload of outpatient MDT into the performance evaluation of participating departments, while 25 (15.9%) have included it in the performance evaluation of participating doctors.
Internal and External Influencing Factors of Outpatient MDT Development
To further analyze the internal and external factors influencing the development of outpatient MDT, the research team adopted the Likert 5-point scale, with the outpatient department managers rating the influencing factors on a scale of 1 to 5. The survey results revealed that the most significant internal factor affecting outpatient MDT was “team dynamics: effective MDT assessment and incentive mechanisms” (mean = 3.99), while the foremost external factor was “medical insurance policy: clear charging standards and policy support” (mean = 3.85) (Refer to Figures 1 and 2 for details).
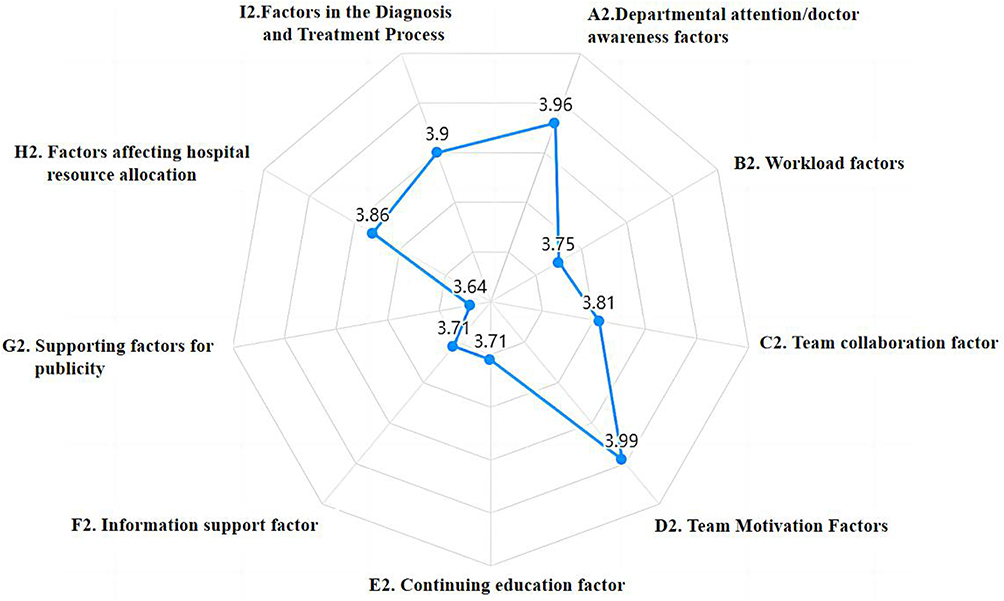 |
Figure 1 Radar chart of internal influencing factors in outpatient MDT. |
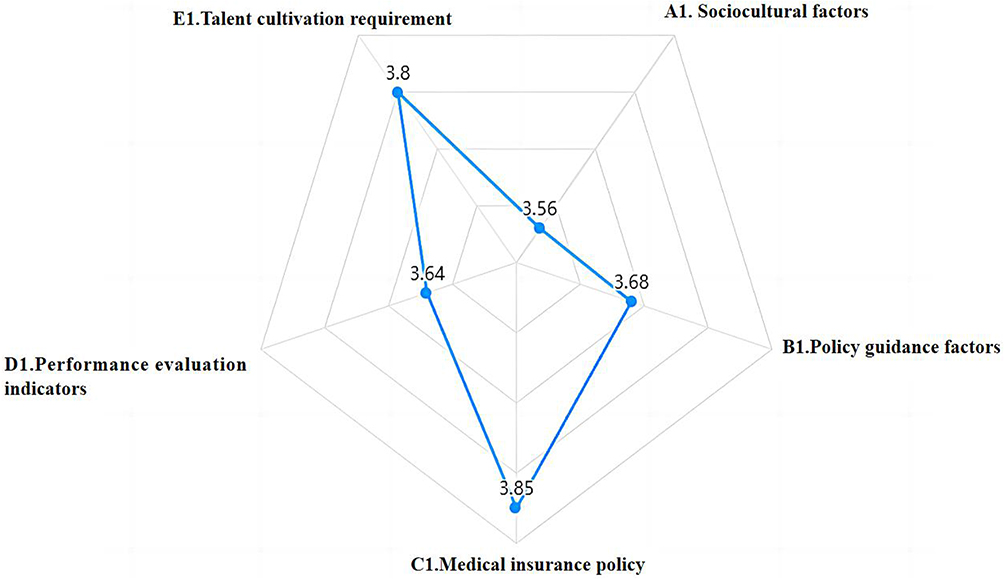 |
Figure 2 Radar chart of external influencing factors for outpatient MDT. |
To analyze and compare the differences in the scores of influencing factors for MDT development between Grade III Class A hospitals and Grade III Class B hospitals, the research team categorized the data into these two groups to assess disparities between hospitals of different levels. The statistical results indicated that hospitals of different levels exhibited differences in various internal and external sub-factors influencing the development of outpatient MDT. Among these, the sub-factor with the greatest difference in external factors was “health insurance policy support” (Cohen’s d = 0.741), while the sub-factor with the most significant difference in internal factors was “diagnosis and treatment process” (Cohen’s d = 0.6). Please refer to Table 4 for further details.
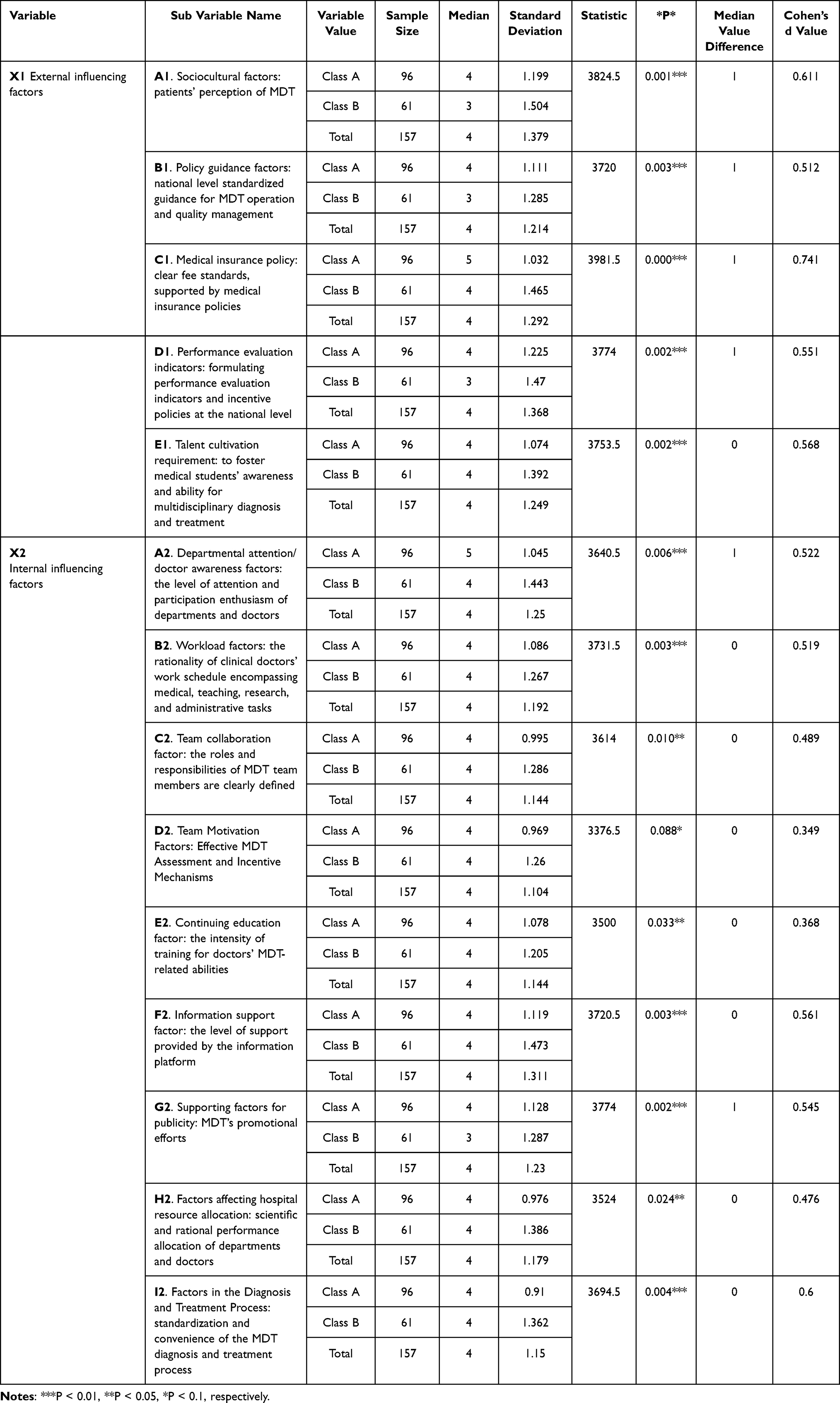 |
Table 4 Analysis of Differences in the Scores of Factors Affecting MDT Development Between Grade III Class A and Grade III Class B Hospitals |
Discussion
The survey results show that the development rate of outpatient MDT in tertiary medical institutions in Sichuan Province is 77.3%, and the development time is mainly concentrated in the past five years. About 87.3% of hospitals have fixed MDT teams ≤10, reflecting that they are still in the primary stage of development. Compared with European and American countries, the German Cancer Center certification requires that the MDT case coverage rate be ≥90%,19 while the National Health Service (NHS) in the UK requires all cancer patients to accept MDT through legislation, and the MDT participation is included in the core index of hospital evaluation.20,21 Whether the government puts forward mandatory requirements for MDT coverage may be one of the institutional factors affecting development.
In terms of the organization and management of MDT, 96.8% of the hospitals have issued relevant management systems, but they have different understanding of the concept and functional orientation of MDT, and there are great differences in the form of development and outpatient mode. For example, with regard to the outpatient MDT model, although the National Health Commission of China issued the Interim Provisions on outpatient quality management in medical institutions in June 2022, which proposed that “the outpatient MDT should be provided with multidisciplinary medical services by a relatively fixed expert team at a fixed time and place”, that is, the “three fixed” outpatient model. The survey results show that the current outpatient MDT implementation rate of the “three fixed” visiting mode is relatively low, only 36.9% of the hospitals implement it, and some hospitals still stay in the traditional consulting mode, that is, temporarily initiate the consultation, temporarily establish the expert team, and arrange the consultation time. Due to the lack of fixed team cooperation, it may lead to the lack of multi-disciplinary cooperation, and it is difficult to reach a consensus. Compared with European and American countries, the UK National Health Service (NHS) ensures service consistency through standardized MDT processes (such as weekly fixed meetings and electronic case sharing),22,23 while Germany requires that MDT meetings must be regularly attended by core specialists.19 This shows the importance of standardized management of MDT operation.
In terms of hospital internal management mechanism, only 35.7% of hospitals included MDT in department assessment, and 15.9% included physician performance. This shows that most hospitals generally ignore the incentive mechanism construction closely related to the personal interests of departments and doctors when promoting the implementation of MDT. The study found that “team dynamics factor” was the largest internal factor affecting the development of outpatient MDT, which also confirmed that medical institutions should promote the sustainable development of MDT through system design (assessment and performance), cognitive improvement and management tool innovation. The survey shows that “medical insurance policy” is the primary external factor affecting the development of outpatient MDT, which is consistent with international experience. For example, Germany included MDT in the DRG payment system and compensated according to the case weight; The national health service system (NHS) in the UK has set up a special package charge for MDT to encourage departments to continue to participate.24,25 Therefore, clarifying and standardizing the MDT charging standard is the core measure to promote its development, which should be the key development direction in the future.
The outpatient MDT model is still in the stage of continuous development in China. Our research method has limitations in using cross-sectional survey research. It is necessary to comprehensively and objectively reflect the overall development status of outpatient MDT in medical institutions in China. In the future, we will conduct cluster stratified sampling research and analysis on tertiary hospitals in China, so as to provide reference for further promotion and development of outpatient MDT model.
Conclusion
This study, conducted through a survey of tertiary medical institutions in Sichuan Province, revealed that outpatient MDT services currently lack a unified standard in crucial aspects, including organizational structure, personnel qualifications, operational modes, and service procedures. It is advisable for medical institutions to enhance the institutional management of outpatient MDT, establish clear and standardized workflows, devise scientific and effective evaluation mechanisms, and integrate core aspects of outpatient MDT into the hospital’s quality management system, encompassing indicators such as the standardization rate of MDT case discussions and project implementation rates. Additionally, medical institutions should offer corresponding performance incentive schemes to motivate doctors’ participation, thereby fostering the continuous optimization and refinement of outpatient MDT services.
Data Sharing Statement
Results data are available upon request to the corresponding author.
Ethical Approval
This study has been approved by the Biomedical Ethics Review Committee of West China Hospital, Sichuan University.
Acknowledgments
This study received substantial support from the Sichuan Medical and Health Quality Control Center, enabling the successful completion of the research task.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analyses and interpretation, or in all these areas, took part in drafting, revising or critically reviewing the article, gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
National Natural Science Foundation of China (NSFC): 72374148, Science/Technology Project of Sichuan province: 2024YFFK0061 and 1·3·5 Projects for Artificial Intelligence (ZYAI24015): West China Hospital, Sichuan University.
Disclosure
The authors reports no conflicts of interest in this work.
References
1. Berumen KS, Sánchez-Navarro A, Velázquez A, et al. Multispecialty sessions model for comprehensive care and decision-making in cancer patients. Ecancermedicalscience. 2025;19. doi:10.3332/ecancer.2025.1830
2. Soukup T, Lamb BW, Arora S, et al. Successful strategies in implementing a multidisciplinary team working in the care of patients with cancer: an overview and synthesis of the available literature. J Multidiscip Healthc. 2018;11:49–61. doi:10.2147/JMDH.S117945
3. Fradgley EA, Booth K, Paul C, et al. Facilitating high quality cancer care: a qualitative study of Australian chairpersons’ perspectives on multidisciplinary team meetings. J Multidiscip Healthc. 2021;14:3429–3439. doi:10.2147/JMDH.S332972
4. Bhumbra R. Effects of multidisciplinary team working on breast cancer survival: retrospective, comparative, interventional cohort study of 13 722 women. BMJ. 2013;362.doi: 10.1136/sbmj.f362
5. Taylor C, Munro AJ, Glynne-Jones R, et al. Multidisciplinary team working in cancer: what is the evidence? BMJ. 2010;340:340c951. doi:10.1136/bmj.c951
6. Lamb BW, Taylor C, Lamb JN, et al. Facilitators and barriers to teamworking and patient centeredness in multidisciplinary cancer teams: findings of a national study. Ann Surg Oncol. 2012;20(5):1408–1416. doi:10.1245/s10434-012-2676-9
7. Van de Velde CJ, Boelens PG, Borras JM, et al. EURECCA colorectal: multidisciplinary management: European consensus conference colon & rectum. Eur J Cancer. 2014;50:1.e1–1.e34. doi:10.1016/j.ejca.2013.06.048
8. Hoinville L, Taylor C, Zasada M, et al. Improving the effectiveness of cancer multidisciplinary team meetings: analysis of a national survey of MDT members’ opinions about streamlining patient discussions. BMJ Open Qual. 2019;8:e000631. doi:10.1136/bmjoq-2019-000631
9. Borras JM, Albreht T, Audisio R, et al. Policy statement on multidisciplinary cancer care. Eur J Cancer. 2013;50(3):475–480. doi:10.1016/j.ejca.2013.11.012
10. Wagland R, Brindle L, James E, et al. Facilitating early diagnosis of lung cancer amongst primary care patients: the views of GPs. Eur J Cancer Care. 2017;26(3). doi:10.1111/ecc.12704
11. Perry N, Broeders M, de Wolf C, et al. European guidelines for quality assurance in breast cancer screening and diagnosis. Fourth edition--summary document. Ann Oncol. 2007;19(4):614–622. doi:10.1093/annonc/mdm481
12. Rankin NM, Fradgley EA, Barnes DJ. Implementation of lung cancer multidisciplinary teams: a review of evidence-practice gaps. Transl Lung Cancer R. 2020;9(4):1667–1679. doi:10.21037/tlcr.2019.11.32
13. Winters DA, Soukup T, Sevdalis N, et al. The cancer multidisciplinary team meeting: in need of change? History, challenges and future perspectives. Bju Int. 2021:128. doi:10.1111/bju.15495
14. Song P, Wu Q, Huang Y. Multidisciplinary team and team oncology medicine research and development in China. Biosci Trends. 2010;4(4):151–160. PMID: 20811133.
15. Jing XM, Chen P, Li SF, et al. Effect of multidisciplinary treatment (MDT) on survival outcomes of lung cancer patients: experiences from China. Asia-Pac J Clin Onco. 2024;20. doi:10.1111/ajco.13972
16. Cui P, Yin B, Zhang Y, et al. Similarities and differences of lung cancer (LC) multidisciplinary teams (MDTs) in China compared to Europe and Canada. J Clin Oncol. 2025;42. doi:10.1200/jco.2024.42.16_suppl.e13562
17. Van W, Liu Y, Twum P, et al. National equity of health resource allocation in China: data from 2009 to 2013. Int J Equity Health. 2016;15:68. doi:10.1186/s12939-016-0357-1
18. Characterizing different multidisciplinary team models implemented within one comprehensive. Cancer Center.
19. Deutsche Krebsgesellschaft (DKG. OnkoZert Manual: Certification Requirements for Organ Cancer Centers [EB/OL]. Berlin, Germany: OnkoZert GmbH. 2023. Available from: https://www.onkozert.de. Accessed July 22, 2025.
20. Hughes C, Homer J, Bradley P, et al. An evaluation of current services available for people diagnosed with head and neck cancer in the UK 2009-2010. Clin Oncol. 2012;24:e187–e192. doi:10.1016/j.clon.2012.07.005
21. Kunkler IH, Fielding RG, Brebner J, et al. A comprehensive approach for evaluating telemedicine-delivered multidisciplinary breast cancer meetings in southern Scotland. J Telemed Telecare. 2005;11 Suppl 1:71–73. doi:10.1258/1357633054461804
22. Prades J, Remue E, van Hoof E, et al. Is it worth reorganising cancer services on the basis of multidisciplinary teams (MDTs)? A systematic review of the objectives and organisation of MDTs and their impact on patient outcomes. Health Policy. 2015:119. doi:10.1016/j.healthpol.2014.09.006.
23. Raine R, Xanthopoulou P, Wallace I, et al. Determinants of treatment plan implementation in multidisciplinary team meetings for patients with chronic diseases: a mixed-methods study. BMJ Qual Saf. 2014;23(10):867–876. doi:10.1136/bmjqs-2014-002818
24. Aggarwal A, Simcock R, Price P, et al. NHS cancer services and systems-ten pressure points a UK cancer control plan needs to address. Lancet Oncol. 2024;25(8):e363–e373. doi:10.1016/S1470-2045(24)00345-0
25. Prades J, Remue E, van Hoof E, et al. Is it worth reorganising cancer services on the basis of multidisciplinary teams (MDTs)? A systematic review of the objectives and organisation of MDTs and their impact on patient outcomes. Health Policy. 2014;119(4):464–474. doi:10.1016/j.healthpol.2014.09.006
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.