")
Back to Journals » Psychology Research and Behavior Management » Volume 15
Emotional Functioning in the Context of Health Behaviors During the COVID-19 Pandemic in Health Sciences Students: The Polish Case
Authors Dębska-Janus M , Dębski P, Główczyński P, Rozpara M , Badura-Brzoza K
Received 2 December 2021
Accepted for publication 4 March 2022
Published 19 April 2022 Volume 2022:15 Pages 953—964
DOI https://doi.org/10.2147/PRBM.S352279
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Małgorzata Dębska-Janus,1 Paweł Dębski,2 Patryk Główczyński,2 Michał Rozpara,1 Karina Badura-Brzoza2
1Institute of Sport Sciences, The Jerzy Kukuczka Academy of Physical Education in Katowice, Katowice, Poland; 2Chair and Clinical Department of Psychiatry, Faculty of Medical Sciences in Zabrze, Medical University of Silesia in Katowice, Katowice, Poland
Correspondence: Paweł Dębski, Tel/Fax +48 322854358, Email [email protected]
Purpose: The fear for health, uncertainty, loss of freedom, boredom, and frustration accompanying the COVID-19 pandemic caused mental health burdens. Young people are particularly at a risk of emotional functioning problems. The aim of this manuscript was to verify the relationships between health behaviors and emotional functioning in health sciences students during the third wave of the COVID-19 pandemic in Poland.
Patients and Methods: The study group comprised 493 Polish health sciences students (314 women, 179 men) aged 21.5 ± 2.25 years. The intensity of health behaviors was examined using the Health Behavior Inventory (HBI). The Hospital Anxiety and Depression Scale (HADS) was carried out to assess symptoms of anxiety and depression. Stress levels were examined with the Perceived Stress Scale (PSS-10). The online versions of psychological scales were created using Google Forms software.
Results: Mild anxiety symptoms were observed in 21% of examined students and moderate-to-severe in 28%. Mild depressive symptoms were observed in 14% of the study group, and 8% of the examined students suffered from moderate-to-severe depression. The mean perceived stress result was high (22.2 ± 4.1 pts.). The overall intensity of health behavior was, at the mean level, significantly higher in females compared to males. The odds of developing severe symptoms in terms of anxiety, depression, and stress in students with high levels of health-related behaviors were respectively: four times, more than seven times, and nine times lower compared to students with lower levels of these behaviors.
Conclusion: Undertaking regular pro-health behavior decreased the odds of developing severe symptoms of anxiety, depression, and stress in health sciences students during the COVID-19 pandemic.
Keywords: anxiety, depression, stress, COVID-19 pandemic, students, health behaviors
Introduction
Since the first case of severe acute respiratory syndrome–coronavirus 2 (SARS-CoV-2) was reported in Wuhan, and soon after its epidemic spread in China was announced, cases of infections were diagnosed in most countries throughout the world as their number rapidly increased. Finally, in March 2020, the World Health Organization announced the global spread of coronavirus disease (COVID-19) as a pandemic. In order to reduce the viral spread of SARS-CoV2, restrictions such as extensive limitations on freedom of movement, the closure of non-essential businesses, and the requirement to stay at home except for limited purposes were imposed.1 Similar to previous pandemics, the limitation of social life exacerbated mental impairments for people all over the world.2–4
The fear for health, uncertainty, loss of freedom, boredom, and frustration accompanying the COVID-19 pandemic caused mental health burdens.2–5 The results of researches aimed at the diagnosis of emotional functioning during the pandemic reality indicated that significant percentages of populations all over the world have experienced at least moderate symptoms of depression and anxiety and high levels of stress.4,6–11 A particularly high increase in emotional health impairments was observed in the incidence of depression.9,10,12
It is foreseen that the negative mental health consequences caused by COVID-19 will last for years.13 Therefore, the need to conduct research that verifies the effectiveness of various coping strategies with these mental health burdens appeared.14–19 Among the practices that may support emotional functioning in the pandemic reality, health behaviors are often mentioned.4 Thus far, the results of few studies aimed at diagnosing the intensity of health behaviors and their relations with mental health and well-being during the pandemic have been published,20–22 but none of them concerned Poles. Their results indicated that health behaviors are an important predictor of emotional functioning during a pandemic. It was also observed that the intensity of the fear of COVID-19 as well as the adherence to preventive behaviors are associated with the knowledge and perception of health risk connected with the virus.23,24
The first case of SARS-CoV2 infection in Poland was diagnosed on March 4, 2020. During the first three waves of the pandemic, the following restrictions were imposed: limitation of movement, closure of non-essential businesses (beauty, food and beverages, hotel, fitness, and culture services), closure of nurseries and kindergartens (1st wave), distance education, and social distancing. The third wave of the SARS-CoV-2 virus pandemic in Poland lasted from March to May 2021, with the peak incidence in early April. The dynamics of the development of infections in this period was as follows: on March 1, 2021, the number of new infections was 4786 cases (24 deaths), on April 1, 2021 it was as many as 35,251 cases (621 deaths), then the number of infections began to decline compared to the April peak - 6469 new infections were detected (423 deaths) on May 1, 2021. In connection with the third wave of the pandemic, the Polish government introduced a tightening of restrictions on March 27, 2021. Schools and nurseries, shopping malls, hairdressing and beauty salons, large-area DIY and furniture stores were closed. The activity of support facilities was limited to professional sports. There was a limit of one person per 20 m2 also in postal and commercial points of sale with an area of more than 100 m2 and in places of religious worship. The restrictions were in force until April 18, 2021.
The above mentioned limitations particularly affected social life and the economy, generating a great sense of uncertainty among the population as a consequence. At that time, several studies aimed at the diagnosis of mental health in selected groups of Poles were conducted.25–29 Similar to the results of research conducted in other countries, these studies showed the aggravation of mental disorders during the COVID-19 pandemic. Young people are particularly at a risk of emotional functioning problems. Social distancing in the period of increased need for social relationships and their indispensability in the formation of psychological maturity and identity results in the significant deterioration of mental well-being.29–31 The results of the previous researches indicated the increase in anxiety and stress level in university students during pandemic.23,24,32–34 It was also observed that their emotional functioning varied depending on the level of confidence in pandemic control, perceived support, perception of health risk connected with the virus and resources for fighting infection.24,35,36 Hence, health sciences students who are generally characterized by a higher level of health awareness, including the risks posed by the SARS-COv2 virus seem to be an interesting group to observe. According to the publications, this high health awareness may, on the one hand, translate into their greater severity of anxiety and stress during a pandemic,37 and on the other may protect against the severe mood disorders.38
Therefore, the aim of this manuscript was to verify the relationships between health behaviors and emotional functioning in health sciences students during the third wave of the COVID-19 pandemic in Poland.
Materials and Methods
Study Group
Health sciences students attending two universities in southern Poland (Medical University of Silesia – medical faculty, Academy of Physical Education in Katowice – non-medical faculty) were invited to participate in the research (via university e-learning platforms). The total number of students was 930, while 550 of them took part in the study. The criteria for inclusion in the study group were as follows: age up to 30 years old, declared lack of mental disorders, and consent to the implementation of the full research program. Ultimately, the research group consisted of 493 students (314 women and 179 men) aged 21.5 ± 2.25 years (19–27 years old). Both the gender distribution and mean age of the study participants were similar to the values characterizing the total number of students of the faculties examined in the study (58% of the total number of students comprised women, mean age was 22.5 ± 4.2 years). The sociodemographic characteristics of the subjects are presented in Table 1.
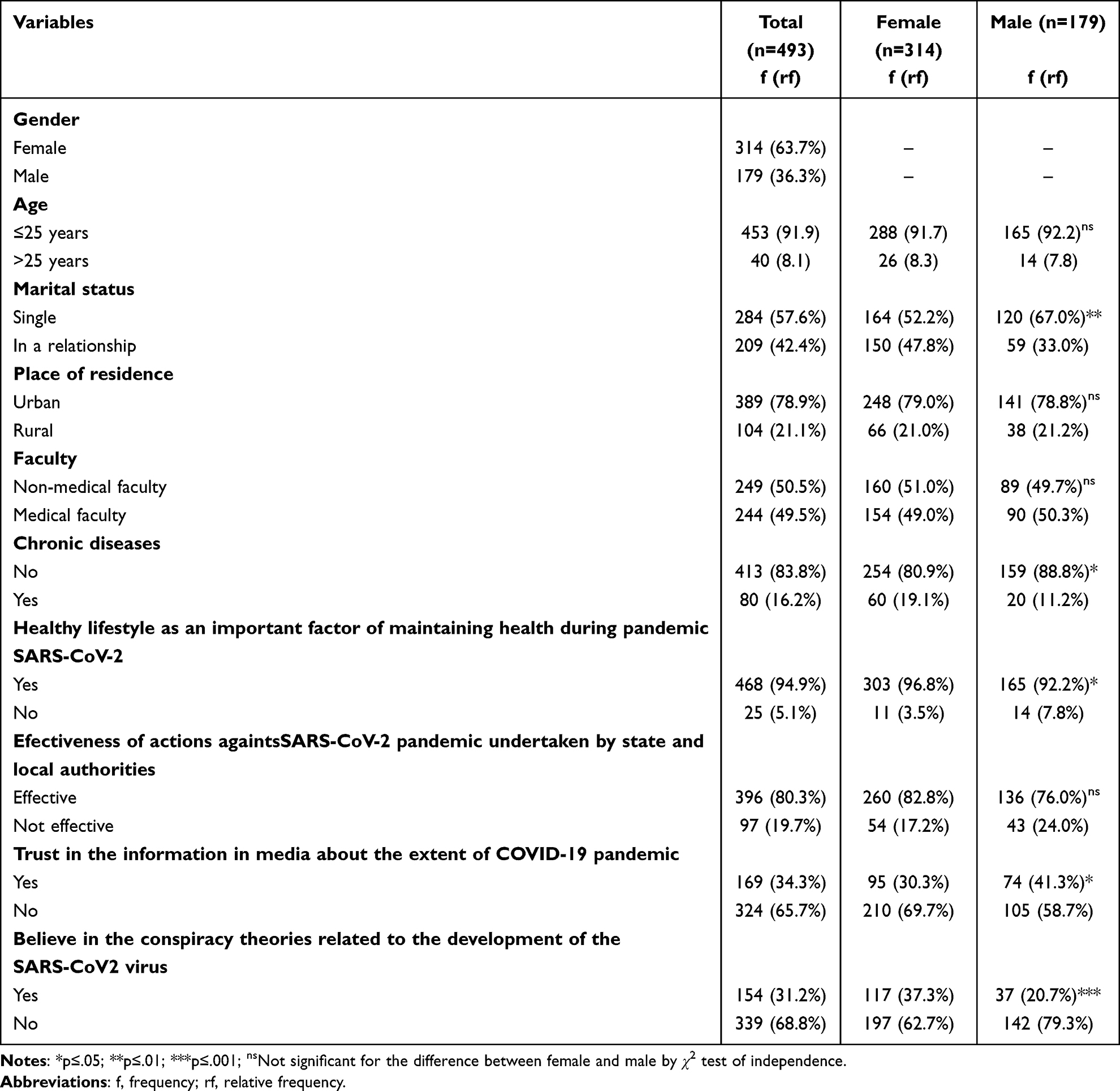 |
Table 1 Sociodemographic Characteristics of the Study Group |
Almost all surveyed students (95%) considered a healthy lifestyle to be an important factor in maintaining one’s health, especially during a pandemic. In the opinion of the vast majority of research participants (80%), the actions of state and local authorities aimed at improving the epidemiological situation in Poland (sanitary regime, social distancing) were effective. At the same time, the majority of students (66%) did not trust the information provided by the media about the extent of the COVID-19 pandemic, and 31% of the study group believed in conspiracy theories related to its development (Table 1).
Methods
Psychological tests were conducted. The intensity of health behaviors was examined using the Health Behavior Inventory (HBI) developed by Z. Juczyński.39 In terms of emotional functioning, the level of anxiety, depression, and perceived stress were verified. The assessment of symptoms of anxiety and depression was carried out using the Hospital Anxiety and Depression Scale (HADS) by Zigmond and Snaith40 in a Polish adaptation by Majkowicz et al41. Stress levels were examined with the Perceived Stress Scale (PSS-10) by S. Cohen, T. Kamarck, R. Mermelstein42 in a Polish adaptation by Z. Juczyński, N. Ogińska-Bulik.43 The online versions of psychological scales were created using Google Forms software. In the Particulars part of the survey besides the sociodemographic questions, 4 yes-or-no questions concerning attitudes towards SARS-CoV-2/COVID-19 pandemic were included (“Do you think that healthy lifestyle is an important factor in maintaining one’s health, especially during a pandemic?”, “Do you think that the actions of state and local authorities aimed at improving the epidemiological situation in Poland are effective?”, “Do you trust the information provided by the media about the extent of the COVID-19 pandemic?” and “Do you believed in conspiracy theories related to the SARS-CoV2 virus development?”).
Health Behaviors Inventory
The scale comprises 24 statements describing health behaviors (HBs) in four categories (independent variables – IVs): Positive Mental Attitude (PMA) (avoiding strong emotions, tension, and stressful and depressing situations), Proper Eating Habits (PEH) (type and frequency of food consumed), Preventive Actions (PA) (following health recommendations, obtaining information about health and illness), and Pro-health Activities (PhA) (everyday habits: sleep, recreation, physical activity). The frequency of each statement is scored on five-point scale (1–5), where 1 means almost never, 2 – rarely, 3 – occasionally, 4 – often, and 5 – almost always. The sum of the scores from the whole questionnaire forms the general indicator of the intensity of HBs. The raw scores are transformed into Standard-Ten-Score-scale (1–10 Sten), where 1–4 Sten means low scores, 5–6 Sten – average scores, and 7–10 Sten – high scores. The tool’s reliability is 0.85 for the entire inventory, whereas for individual categories (PMA, PEH, PA, PhA), the Cronbach’s alpha coefficients range from 0.60 to 0.65.39 For the current study, the Cronbach’s alpha coefficients are 0.85 for the entire scale, and from 0.65 to 0.80 for the categories.
Hospital Anxiety and Depression Scale
The scale consists of 14 items which are divided into two subscales (dependent variables – DVs): the anxiety subscale (HADS-A) and the depression subscale (HADS-D). Each subscale is composed of 7 statements which assess respondents’ moods over the past week. The subjects assess how much they identify with each statement on a 4-point scale (from 0 to 3). The scores obtained for each subscale are summed (ranging from 0–21) and the severity of anxiety and depressive symptoms are assessed (0–7 points – non-minimal anxiety/depression, 8–10 – mild anxiety/depression, 11–14 – moderate anxiety/depression, 15–21 – severe anxiety/depression).41,44 According to the literature, scores ≥8 are established as an optimal cut-off score for both HADS-A and HADS-D subscales.40,45 In the current study, both subscales have strong internal consistency reliability (Cronbach’s alpha for HADS-A = 0.85, HADS-D = 0.75).
Perceived Stress Scale
This is a 10-item self-reported measure of global perceived stress (dependent variable – DV). Participants assess statements concerning how frequently they notice their life as unpredictable, uncontrollable, and overloaded within the previous month on a 5-point Likert scale (0–4) where 0 means never, 1 – almost never, 2 – sometimes, 3 – fairly often, 4 – very often). A total score is computed by reverse scoring the four positively worded items and then summing all the scale items (ranging from 0–21). The higher the result, the greater the intensity of the stress. According to the developers’ guideline,43 the raw data is transformed into Standard-Ten-Score-scale (1–10 Sten), where 1–4 Sten means low level of perceived stress, 5–6 Sten – moderate level, and 7–10 Sten – high level. The PSS-10 has demonstrated appropriate reliability (Cronbach’s alpha from 0.75–0.91).23,26 For the current study, the Cronbach’s alpha coefficient is: 0.89.
Social Demographic Characteristics
During the study, gender, age, marital status, place of residence, and field of study were also obtained. Gender and field of study were treated in the research as confounding variables (CVs).
Respondents were also asked to assess the effectiveness of the actions of state and local government authorities aimed at improving the epidemiological situation, the role of lifestyle in counteracting the development of the pandemic, and the reasons for its outbreak, which were obtained on the basis of 4 questions at the end of the online form.
Procedures
The students who expressed their willingness to participate in the study were assigned to a specific edition of the research and informed about its date and time by e-mail. The research was conducted during the third wave of SARS-CoV-2/COVID-19 in Poland (March-May 2021). Due to the restrictions, the study was conducted in electronic form, via MS Teams by the authors of this manuscript platform. Before the survey, supervisors informed the participants about the aim of the study and discussed the filling instructions for the conducted tests.
Ethics
The study procedures were reviewed by the Research Ethics Committee of the Medical University of Silesia in Katowice (PCN/0022/KB/277/19). It complies with the Declaration of Helsinki. All subjects were familiarized with the aim of the study prior to data collection. Participants were informed about the anonymity and voluntariness of participation in the research and could discontinue their participation at any time. Returning the tests after completing them was the same as consenting with the use of the information collected during the examination.
Analysis
For the measures used, Cronbach’s alpha coefficients in the study sample were determined. The frequency (f) and relative frequency in percent (rf) of variable categories (gender: female, male; marital status: single, in a relationship; place of residence: urban, rural; faculty: non-medical faculty, medical faculty) were calculated. The data was analyzed in terms of arithmetic means (M) and standard deviation (SD). The normality of the data distribution was assessed with the Shapiro–Wilk test (W). In order to estimate the relationship among the variables, multinomial logistic regression analysis was conducted. The variant of the sequential introduction of independent variables into the regression model was used (the technique of controlling the influence of confounding variables). Depression, anxiety, and stress were modeled as dependent variables, health behaviors as an independent variable, and sociodemographic variables (gender and faculty) as confounding variables. In step 1 of the regression, health behavior variables were entered as the independent variable. Gender and faculty of the studies were added as confounding variables in steps 2 and 3, respectively. The relationships between the variables were assessed on the basis of the odds ratio statistics (OR) and the 95% confidence interval for the OR. The level of statistical significance was set at α =0.05. Statistical calculations were made using IBM SPSS Statistics 26.0 (IBM Corporation, Armonk, NY, USA).
Results
The mean score of anxiety among the study group was 8.0 ± 4.3 points, which allows the estimation of its level as mild. Of the whole study group, 51% (252) had non-to-minimal, 21% (102) – mild, and 28% (139) – moderate-to-severe anxiety symptoms. The mean score of depressive symptoms was 5.0 ± 3.5 points (minimal level). Mild depressive symptoms were observed in 14% (68) of the study group and 8% (38) of examined students suffered from moderate-to-severe depression. Anxiety levels were significantly higher in female students compared to males. The mean perceived stress result was 22.2 ± 4.1 points, which allows the estimation of its level as high. It was observed that 53% (259) of students experienced high and 24% (116) medium levels of stress. The independent sample t-test revealed a significant intersexual difference in stress level. The overall intensity of health behavior was, at the mean level, significantly higher in females compared to males. The frequency of undertaking HBs across the subscales was similar (Table 2).
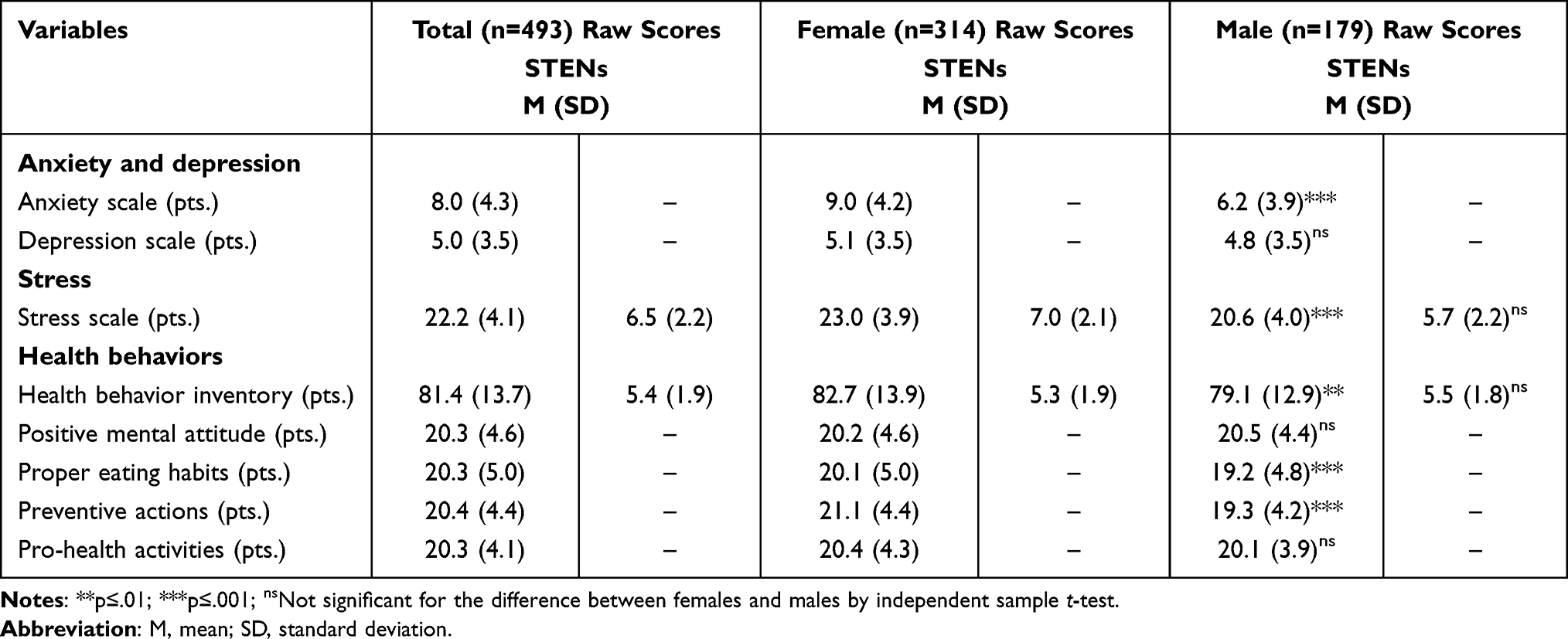 |
Table 2 Characteristics of Emotional Functioning and Health Behaviors During the Third Wave of the COVID-19 Pandemic in Examined Students |
Multinomial logistic regression analysis revealed that the intensity of health behaviors and gender were factors significantly associated with anxiety levels among healthcare/health sciences students. Those with a high intensity of health behaviors were 4 times more likely to have non-minimal anxiety symptoms compared to students with a low health behavior index [aOR: 4.1, 95% CI: 2.36–6.96]. After gender was included in the model, these odds increased both in students with a high intensity of HBs (by 152%, up to 5.6 times) and in subjects with an average intensity of HBs (by 19%, up to 2.9 times. Healthcare students who had an average frequency of health behaviors were 2.7 times more likely to have non-minimal anxiety symptoms as opposed to those with a low frequency. Regarding gender, among students with the same HBs intensity females were 80% less likely to have non or minimal anxiety levels when compared to men with the same level of health behavior intensity. The odds of having non or minimum anxiety levels were about 80% greater for males than females. Including the faculty as confounding variable in the model did not significantly change the relationship between anxiety levels and intensity of HBs (Table 3).
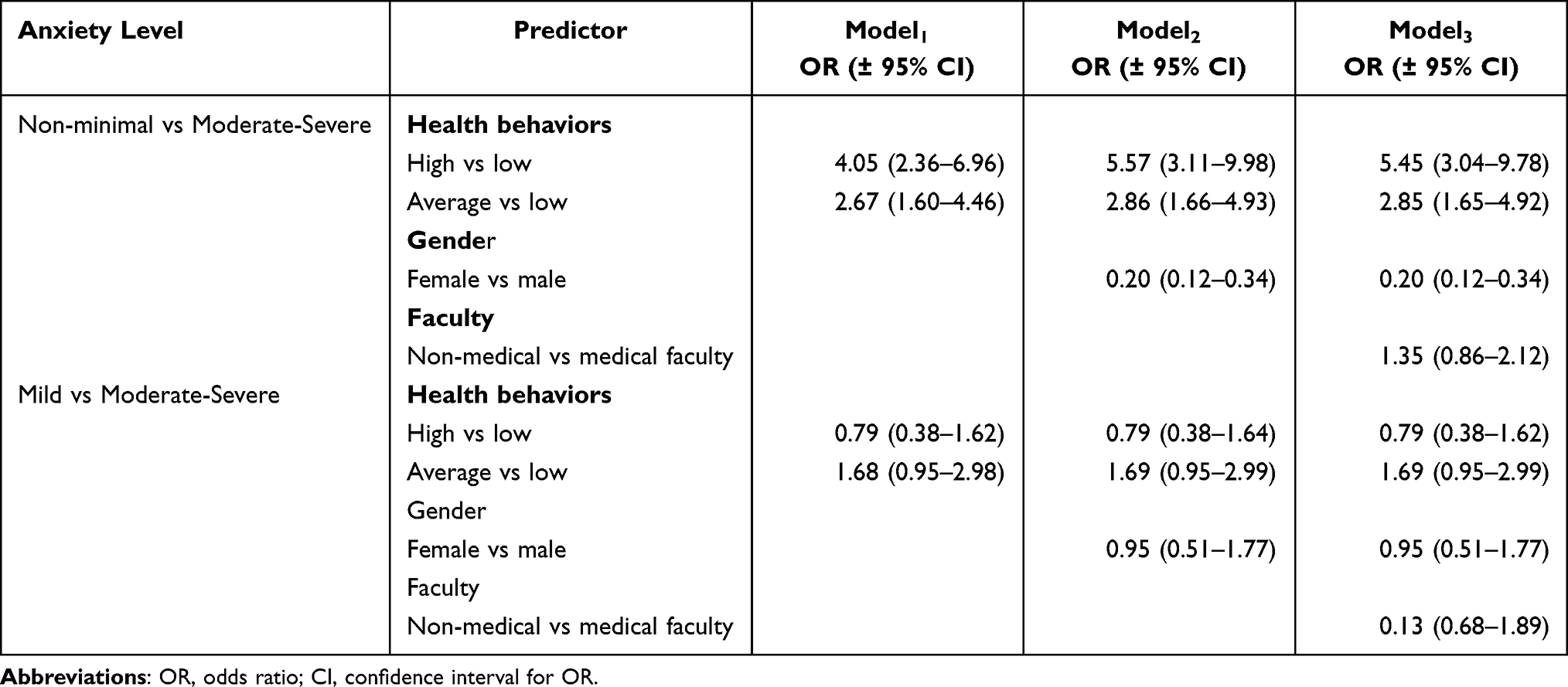 |
Table 3 Intensity of Health Behaviors and Anxiety Levels in Health Sciences Students |
According to the results of multinomial logistic regression, a positive mental attitude (OR:1.44, 95%, CI:1.33–1.56, p<0.001) and preventive actions (OR:0.87, 95%, CI:0.81–0.94, p<0.001) were significant categories of health behaviors to predict/assess the odds of the occurrence of non-minimal anxiety symptoms. An increase in PMA by 1 point resulted in a 44% increase in the odds of having non-minimal anxiety levels, compared to a 13% decrease in PA. After gender and faculty were included in the model, these odds increased by 1% in the case of PMA and decreased up to 10% in PA. In the case of mild anxiety symptoms, only PMA was significant for assessing the odds of the occurrence of minimal anxiety symptoms.
It was observed that the intensity of health behaviors is positively and significantly related to the severity of depression symptoms. The odds of having minimal, not moderate-severe depression symptoms were 7.3 times greater for students with a high intensity of health behaviors and 6.8 times greater in those with an average intensity of health behaviors compared to subjects with low health behavior inventory results. The conditional probability of having mild, not moderate-severe depression level was 4.8 times greater for students with moderate, not low HBs. Once gender and faculty are taken into account, the odds for minimal and mild depression did not change significantly (Table 4).
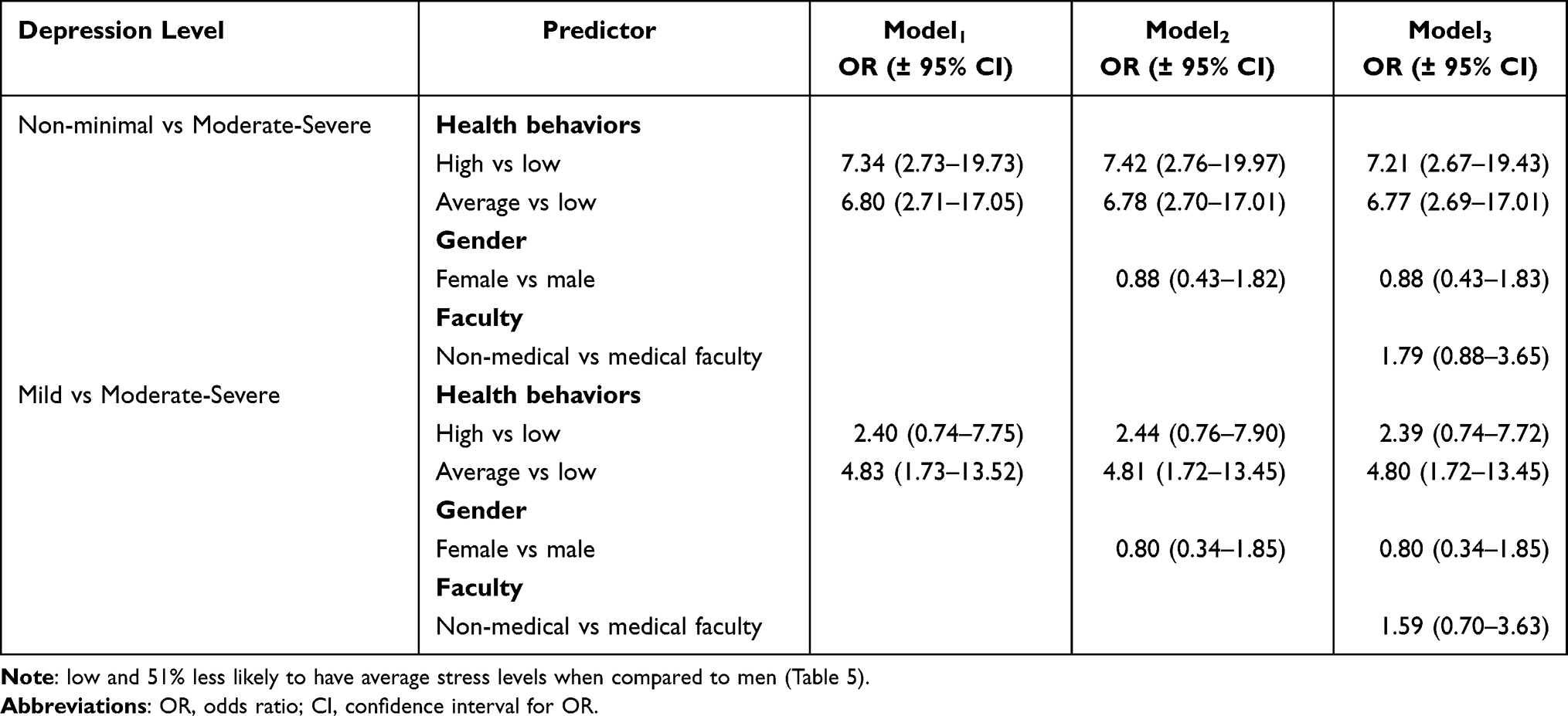 |
Table 4 Intensity of Health Behaviors and the Level of Depression in Health Sciences Students |
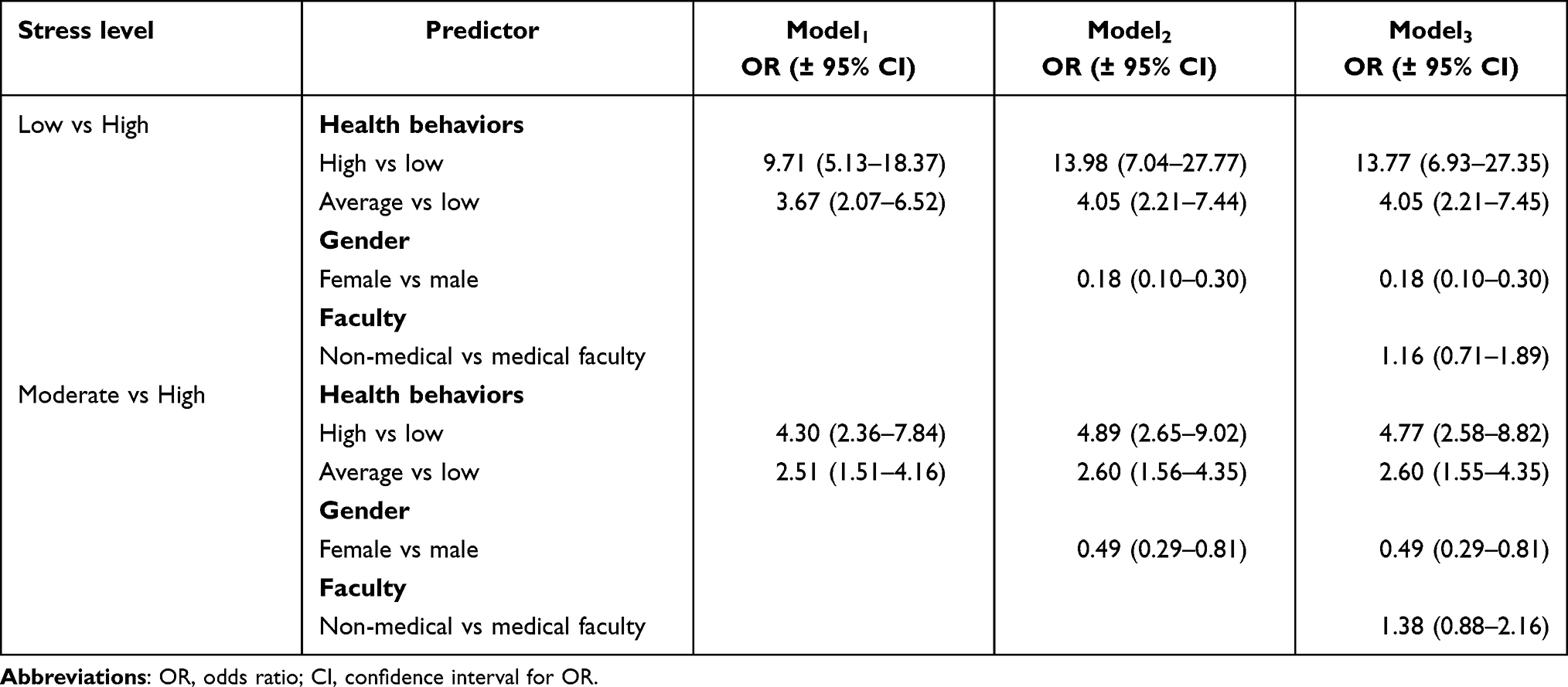 |
Table 5 Intensity of Health Behaviors and Stress Levels in Examined Students |
Regarding the categories of health behaviors, only Positive Mental Attitude was a significant variable for assessing the probability of the occurrence of minimal (OR:1.49, 95%, CI:1.33–1.68, p<0.001) and mild (OR:1.20, 95%, CI:1.06–1.36, p<0.001) depression symptoms, not moderate-severe. An increase in PMA by 1 point resulted in 49% and 20% increases in the odds of having non-minimal or mild depression levels, respectively. Including gender and faculty as confounding variables in the model did not significantly change these relationships (non-minimal vs moderate-severe: Model 2 and 3 – OR:1.50, 95%, CI:1.33–1.69, p<0.001; mild vs moderate-severe: Model 2 and 3 – OR:1.20, 95%, CI:1.06–1.35, p<0.001).
It was revealed that healthcare students with high and average intensity of health behaviors are more likely to have low (consecutively 9.7 times, 3.7 times) or moderate (consecutively 4.3 times, 2.5 times), not high stress levels compared to those with a low frequency of HBs. After gender and faculty were included in the model, these odds increased both in students with a high intensity of HBs (consecutively up to 13.8 times, 4.8 times) and in subjects with an average intensity of HBs (consecutively up to 4.1 times, 2.6 times). Among students with the same HBs intensity, females were 82% less likely to have low and 51% less likely to have average stress levels when compared to men (Table 5).
The multiple logistic regression indicated that each category of Health Behavior Inventory is significantly related with the occurrence of low and not high stress levels (PMA: OR:1.59, 95%, CI:1.45–1.75, p<0.001; PEH: OR:0.92, 95%, CI:0.86–0.98, p<0.001; PA: OR:0.89, 95%, CI:0.82–0.96, p<0.001; PhA: OR:1.10, 95%, CI:1.01–1.19, p<0.001). The odds of having moderate and not high stress levels increased by 30% in students with a high PMA. Among students with the same intensity of HBs categories, females were 81% less likely to have low (OR:0.19, 95%, CI:0.10–0.35, p<0.001) and 51% less likely to have average (OR:0.49, 95%, CI:0.28–0.85, p<0.001) stress levels when compared to men.
Discussion
Accompanying the COVID-19 fear for health connected with loss of freedom, uncertainty and frustration generated by the social life and economic limitations have significantly impacted mental health of populations all over the world.2–46The similar psychosocial phenomena were observed during the previous pandemics (Ebola, AH1N1 influenza, MERS-CoV)47–50 It is indicated that the group that is particularly at risk from the psychological point of view during the pandemic are young people.29–31
In our study, alarming results were obtained regarding the severity of symptoms of anxiety, depression, and stress in students of health promoting faculties during the third wave of the COVID-19 pandemic in Poland; mild severity of anxiety was diagnosed in 21% of respondents and moderate or severe in another 28%. In the case of the exacerbation of depression symptoms, this was 14% and 8%, respectively. High levels of stress were observed in 51% of the respondents and moderate levels in 24%. These results are alarming, considering the fact that excessive anxiety tension is a psychopathological factor and may contribute to the development of anxiety disorders or the activation of other psychological problems.51,52
Problems in the emotional functioning of students during the SARS-CoV-2 pandemic have also been demonstrated by the results of studies conducted in other countries. An analysis of the mental state of students in different parts of the world revealed the presence of anxiety disorders in 11–39% of respondents. Depressive disorders were diagnosed in 22–48% of students.6,34,53–55Moreover, it turned out that a higher anxiety levels were observed in students from rural areas and those in non-medical faculties.56 Living in cities, or alternatively living with a family, have been identified as factors protecting against the occurrence of increased anxiety.6 What is more, significantly higher level of anxiety occurs in higher-year students than those in their first year of studies.55
The causes of the alarming severity level of symptoms of anxiety and depression during the COVID-19 pandemic are seen primarily in the long-term stressful situation, which is based on the threat to human health and life, a disturbed sense of security exacerbated by the unpredictability of the disease, and the restrictions in social functioning resulting from the epidemiological situation.57 The SARS-CoV-2 virus pandemic, apart from being a direct threat to human health, significantly limits activities related to building one’s social network, creating interpersonal relationships, and learning to use the resources of interpersonal cooperation that determine functioning in difficult situations. Restrictions were introduced to reduce the spread of the virus, including on ceasing to participate in classes and the need to adapt to the model of distance learning, the inability to participate in cultural and entertainment events, limiting direct contact only to members of one’s household, significantly reduced the possibility of implementing psychological developmental tasks related to the age of early adulthood, contributing to the deterioration of quality of life.26,29 It can therefore be concluded that the pandemic blocked the traditional possibility of meeting amongst a group of students, leading to a deterioration of their emotional functioning.
The main purpose of this study was to identify the relationship between the frequency of undertaking health behaviors and the emotional functioning of healthcare students during the SARS-COV2 virus pandemic. The results of multiple logistic regression indicated that the overall intensity of healthy behaviors significantly reduced the occurrence of high levels of anxiety, depression, and stress symptoms among the respondents. The chance of serious symptoms in the scope of components of emotional health in students with high levels of health behaviors during the third wave of the COVID-19 pandemic were, respectively, four times, more than seven times, and nine times lower compared to students with lower levels of these behaviors. It can therefore be concluded that pro-health behaviors allow students of health promoting faculties to better function mentally in the pandemic reality.
In non-pandemic conditions, many studies have been conducted on the general relationship between the severity of health behaviors and symptoms of depression, anxiety, and stress in people of different ages and health statuses.23,36,58–62 The results of these studies indicate that a low intensity of health-related behaviors is conducive to negative phenomena in the area of mood and emotions, while regular pro-health behavior may be a protective factor. The verification of this relationship during the COVID-19 pandemic in the group of students was made only in a few countries,20–22 and none of them concerned Polish students. The authors of these studies confirm the observations made in this study – health behaviors are an important predictor of symptoms of depression, anxiety, and stress in students during a pandemic. Behaviors related to a positive mental attitude, which seem to play a particularly important role in preventing the development of undesirable phenomena within affect, fit into the concept of the so-called salutogenesis, ie a model emphasizing pro-health psychological properties. Mental hygiene, promoting an optimistic, coherent, task-oriented style of action in people, favors the activation of homeostatic and immune mechanisms of the body, supports coping with inflammation, and prevents the development of anxiety-depressive states.63–65 These mechanisms are extremely desirable, especially in a situation involving a disturbed sense of security and increased anxiety regarding the health of oneself and one’s relatives caused by the SARS-COv2 virus epidemic.
The obtained research results emphasize the increased need to promote healthy behaviors in the current epidemiological situation. In addition to primary measures aimed at limiting the possibility of the spread of the SARS-COv2 virus, such as intensified hygiene procedures and the introduction of restrictions in the field of social life, state decision-makers and organizations supporting public health must also intensify practical activities aimed at reducing the long-term negative consequences of the pandemic in the field of mental functioning. The popularization of pro-health behaviors on the main news websites, broadcasting in the media additional programs teaching relaxation techniques, and presenting the importance and possibilities of implementing an appropriate dose of physical activity, sleep, or a diet supporting immunity, all seem to be good practices for supporting emotional functioning. In the case of students, a particularly effective channel of communication of the above-mentioned practices may be their implementation within the framework of conducted didactic activities.
Several limitations of this study should be mentioned. The study covered a selected social group – healthcare students. Members of this group are generally characterized by a higher level of health awareness, including the risks posed by the SARS-COv2 virus, which may translate into their greater severity of anxiety and stress during a pandemic.37 This is a preliminary study and the research should be extended to the diagnosis of other social groups as well as the verification of the relationship between health behavior and emotional functioning in these groups in the period involving the stabilization of the epidemiological situation. It would also be advisable to diagnose the key health-enhancing behaviors with the use of specific tools that optimize the reliability of obtained data, such as accelerometers to verify the physical activity level,66,67 24-hour nutrition interviews for the assessment of dietary intake,68 Ego-resiliency and DS-14 Tests69,70 to verify predisposition to coping with stress.
Conclusion
In the course of this study, it was confirmed that regular pro-health behavior plays a protective role in the mental health of students during the COVID-19 pandemic. The odds of developing severe symptoms in terms of anxiety, depression, and stress in students with high levels of health-related behaviors during the third wave of the COVID-19 pandemic were, respectively, four times, more than seven times, and nine times lower compared to students with lower levels of these behaviors. The results obtained underline the increased need to promote health behaviors in the current epidemiological situation in order to reduce the long-term negative consequences of the pandemic in the field of mental health. State decision-makers and public health organizations should spread the knowledge about the health-enhancing character of such behaviors and popularize them via special programs in media, schools and universities.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Milne GJ, Xie S. The effectiveness of social distancing in mitigating COVID-19 spread: a modelling analysis. medRxiv. 2020;20040055. doi:10.1101/2020.03.20.20040055
2. Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet Lond Engl. 2020;395(10227):912–920. doi:10.1016/S0140-6736(20)30460-8
3. Dong L, Bouey J. Public mental health crisis during COVID-19 pandemic, China. Emerg Infect Dis. 2020;26(7):1616–1618. doi:10.3201/eid2607.200407
4. Fischer R, Bortolini T, Karl JA, et al. Rapid review and meta-meta-analysis of self-guided interventions to address anxiety, depression, and stress during COVID-19 social distancing. Front Psychol. 2020;11:563876. doi:10.3389/fpsyg.2020.563876
5. Heitzman J. Impact of COVID-19 pandemic on mental health. Psychiatr Pol. 2020;54(2):187–198. doi:10.12740/PP/120373
6. Cao W, Fang Z, Hou G, et al. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020;287:112934. doi:10.1016/j.psychres.2020.112934
7. Bäuerle A, Teufel M, Musche V, et al. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: a cross-sectional study in Germany. J Public Health. 2020;42(4):672–678. doi:10.1093/pubmed/fdaa106
8. Shevlin M, McBride O, Murphy J, et al. Anxiety, depression, traumatic stress and COVID-19-related anxiety in the UK general population during the COVID-19 pandemic. BJPsych Open. 2020;6(6). doi:10.1192/bjo.2020.109
9. Mazza C, Ricci E, Biondi S, et al. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: immediate psychological responses and associated factors. Int J Environ Res Public Health. 2020;17(9):3165. doi:10.3390/ijerph17093165
10. Planchuelo-Gómez Á, Odriozola-González P, Irurtia MJ, de Luis-garcía R. Longitudinal evaluation of the psychological impact of the COVID-19 crisis in Spain. J Affect Disord. 2020;277:842–849. doi:10.1016/j.jad.2020.09.018
11. Salari N, Hosseinian-Far A, Jalali R, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Glob Health. 2020;16(1):57. doi:10.1186/s12992-020-00589-w
12. Ueda M, Stickley A, Sueki H, Matsubayashi T. Mental health status of the general population in Japan during the COVID-19 pandemic. Psychiatry Clin Neurosci. 2020;74(9):505–506. doi:10.1111/pcn.13105
13. O’Sullivan O. Long-term sequelae following previous coronavirus epidemics. Clin Med. 2021;21(1):e68–e70. doi:10.7861/clinmed.2020-0204
14. Franco E, Urosa J, Barakat R, Refoyo I. Physical activity and adherence to the Mediterranean diet among Spanish employees in a health-promotion program before and during the COVID-19 pandemic: the sanitas-healthy cities challenge. Int J Environ Res Public Health. 2021;18(5):2735. doi:10.3390/ijerph18052735
15. Ahorsu DK, Imani V, Lin CY, et al. Associations between fear of COVID-19, mental health, and preventive behaviours across pregnant women and husbands: an actor-partner interdependence modelling. Int J Ment Health Addict. 2020:1–15. doi:10.1007/s11469-020-00340-x
16. Hoying J, Melnyk BM, Hutson E, Tan A. Prevalence and correlates of depression, anxiety, stress, healthy beliefs, and lifestyle behaviors in first-year graduate health sciences students. Worldviews Evid Based Nurs. 2020;17(1):49–59. doi:10.1111/wvn.12415
17. Engida ZT, Shiferaw DS, Ketaro MK, et al. COVID-19-related anxiety and the coping strategies in the Southeast Ethiopia. Psychol Res Behav Manag. 2021;14:1019–1031. doi:10.2147/PRBM.S309806
18. Alijanzadeh M, Ahorsu DK, Alimoradi Z, et al. Fear of COVID-19 and trust in the healthcare system mediates the association between individual’s risk perception and preventive COVID-19 behaviours among Iranians. Int J Environ Res Public Health. 2021;18(22):12146. doi:10.3390/ijerph182212146
19. Holshue ML, DeBolt C, Lindquist S, et al. First case of 2019 novel coronavirus in the United States. N Engl J Med. 2020;382(10):929–936. doi:10.1056/NEJMoa2001191
20. Mata J, Wenz A, Rettig T, et al. Health behaviors and mental health before and during the COVID-19 pandemic: a longitudinal population-based survey. Social Sci Med. 2020. doi:10.31234/osf.io/qbgh7
21. Choompunuch B, Suksatan W, Sonsroem J, Kutawan S, In-udom A. Stress, adversity quotient, and health behaviors of undergraduate students in a Thai university during COVID-19 outbreak. Belitung Nurs J. 2021;7(1):1–7. doi:10.33546/bnj.1276
22. Kim YJ, Cho JH. Correlation between preventive health behaviors and psycho-social health based on the leisure activities of South Koreans in the COVID-19 crisis. Int J Environ Res Public Health. 2020;17(11):4066. doi:10.3390/ijerph17114066
23. Lovell GP, Nash K, Sharman R, Lane BR. A cross-sectional investigation of depressive, anxiety, and stress symptoms and health-behavior participation in Australian university students. Nurs Health Sci. 2015;17(1):134–142. doi:10.1111/nhs.12147
24. Pramukti I, Strong C, Sitthimongkol Y, et al. Anxiety and suicidal thoughts during the COVID-19 pandemic: cross-country comparative study among Indonesian, Taiwanese, and Thai University Students. J Med Internet Res. 2020;22(12):12. doi:10.2196/24487
25. Bidzan-Bluma I, Bidzan M, Jurek P, et al. A polish and German population study of quality of life, well-being, and life satisfaction in older adults during the COVID-19 pandemic. Front Psychiatry. 2020;11. doi:10.3389/fpsyt.2020.585813
26. Juchnowicz D, Baj J, Forma A, et al. The outbreak of SARS-cov-2 pandemic and the well-being of polish students: the risk factors of the emotional distress during COVID-19 lockdown. J Clin Med. 2021;10((5)):944. doi:10.3390/jcm10050944
27. Chodkiewicz J, Miniszewska J, Krajewska E, Biliński P. Mental health during the second wave of the COVID-19 pandemic—Polish studies. Int J Environ Res Public Health. 2021;18(7):3423. doi:10.3390/ijerph18073423
28. Rogowska AM, Kuśnierz C, Bokszczanin A. Examining anxiety, life satisfaction, general health, stress and coping styles during COVID-19 pandemic in polish sample of university students. Psychol Res Behav Manag. 2020;13:797–811. doi:10.2147/PRBM.S266511
29. Szczepańska A, Pietrzyka K. The COVID-19 epidemic in Poland and its influence on the quality of life of university students (young adults) in the context of restricted access to public spaces. J Public Health. 2021. doi:10.1007/s10389-020-01456-z
30. Liu CH, Stevens C, Conrad RC, Hahm HC. Evidence for elevated psychiatric distress, poor sleep, and quality of life concerns during the COVID-19 pandemic among U.S. young adults with suspected and reported psychiatric diagnoses. Psychiatry Res. 2020;292:113345. doi:10.1016/j.psychres.2020.113345
31. Eckersley RM, Wierenga A, Wyn J. Life in a time of uncertainty: optimising the health and wellbeing of young Australians. Med J Aust. 2005;183(8):402–404. doi:10.5694/j.1326-5377.2005.tb07102.x
32. Sharma R, Bansal P, Chhabra M, Bansal C, Arora M. Severe acute respiratory syndrome coronavirus-2-associated perceived stress and anxiety among Indian medical students: a cross-sectional study. Asian J Soc Health Behav. 2021;4(3):98. doi:10.4103/shb.shb_9_21
33. Lu MY, Ahorsu DK, Kukreti S, et al. the prevalence of post-traumatic stress disorder symptoms, sleep problems, and psychological distress among COVID-19 Frontline healthcare workers in Taiwan. Front Psychiatry. 2021;12:1143. doi:10.3389/fpsyt.2021.705657
34. Wang X, Hegde S, Son C, Keller B, Smith A, Sasangohar F. Investigating mental health of US college students during the COVID-19 pandemic: cross-sectional survey study. J Med Internet Res. 2020;22(9):e22817. doi:10.2196/22817
35. Wathelet M, Duhem S, Vaiva G, et al. Factors associated with mental health disorders among university students in France confined during the COVID-19 pandemic. JAMA Netw Open. 2020;3(10):e2025591. doi:10.1001/jamanetworkopen.2020.25591
36. Strine TW, Chapman DP, Balluz L, Mokdad AH. Health-related quality of life and health behaviors by social and emotional support. Their relevance to psychiatry and medicine. Soc Psychiatry Psychiatr Epidemiol. 2008;43(2):151–159. doi:10.1007/s00127-007-0277-x
37. Komer L. COVID-19 amongst the pandemic of medical student mental health. Int J Med Stud. 2020;8(1):56–57. doi:10.5195/ijms.2020.501
38. Tran TV, Nguyen HC, Pham LV, et al. Impacts and interactions of COVID-19 response involvement, health-related behaviours, health literacy on anxiety, depression and health-related quality of life among healthcare workers: a cross-sectional study. BMJ Open. 2020;10(12):e041394. doi:10.1136/bmjopen-2020-041394
39. Juczyński Z. Narzędzia Pomiaru w Psychologii Zdrowia. Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego; 2012.
40. Snaith RP, Zigmond AS. The hospital anxiety and depression scale. Br Med J Clin Res Ed. 1986;292(6516):344. doi:10.1136/bmj.292.6516.344
41. Majkowicz M. Praktyczna ocena efektywności opieki paliatywnej—wybrane techniki badawcze. In: Ocena Jakości Opieki Paliatywnej w Teorii i Praktyce.
42. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396. doi:10.2307/2136404
43. Juczyński Z, Ogińska Bulik N. Narzędzia Pomiaru Stresu i Radzenia Sobie Ze Stresem. Pracownia Testów Psychologicznych Polskiego Towarzystw Psychologicznego; 2012.
44. Stern AF. The hospital anxiety and depression scale. Occup Med. 2014;64(5):393–394. doi:10.1093/occmed/kqu024
45. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res. 2002;52(2):69–77. doi:10.1016/s0022-3999(01)00296-3
46. Cohen S. Perceived stress in a probability sample of the United States. In: The Social Psychology of Health. The Claremont Symposium on Applied Social Psychology. Sage Publications, Inc; 1988:31–67.
47. Goodwin R, Gaines SO, Myers L, Neto F. Initial psychological responses to swine flu. Int J Behav Med. 2011;18(2):88–92. doi:10.1007/s12529-010-9083-z
48. Al Najjar NS, Attar LM, Farahat FM, Al Thaqafi A. Psychobehavioural responses to the 2014 Middle East respiratory syndrome-novel Corona virus [MERS CoV] among adults in two shopping malls in Jeddah, western Saudi Arabia. EMHJ-East Mediterr Health J. 2016;22(11):817–823.
49. Van Bortel T, Basnayake A, Wurie F, et al. Psychosocial effects of an Ebola outbreak at individual, community and international levels. Bull World Health Organ. 2016;94(3):210–214. doi:10.2471/BLT.15.158543
50. Thompson RR, Garfin DR, Holman EA, Silver RC. Distress, worry, and functioning following a global health crisis: a national study of Americans’ Responses to Ebola. Clin Psychol Sci. 2017;5(3):513–521. doi:10.1177/2167702617692030
51. Scarella TM, Boland RJ, Barsky AJ. Illness anxiety disorder: psychopathology, epidemiology, clinical characteristics, and treatment. Psychosom Med. 2019;81(5):398–407. doi:10.1097/PSY.0000000000000691
52. Carleton RN, Afifi TO, Taillieu T, et al. Anxiety-related psychopathology and chronic pain comorbidity among public safety personnel. J Anxiety Disord. 2018;55:48–55. doi:10.1016/j.janxdis.2018.03.006
53. Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):E1729. doi:10.3390/ijerph17051729
54. Odriozola-González P, Planchuelo-Gómez Á, Irurtia MJ, de Luis-garcía R. Psychological effects of the COVID-19 outbreak and lockdown among students and workers of a Spanish university. Psychiatry Res. 2020;290:113108. doi:10.1016/j.psychres.2020.113108
55. Kecojevic A, Basch CH, Sullivan M, Davi NK. The impact of the COVID-19 epidemic on mental health of undergraduate students in New Jersey, cross-sectional study. PLoS One. 2020;15(9):e0239696. doi:10.1371/journal.pone.0239696
56. Chang J, Yuan Y, Wang D. Mental health status and its influencing factors among college students during the epidemic of COVID-19. Nan Fang Yi Ke Da Xue Xue Bao. 2020;40(2):171–176. doi:10.12122/j.issn.1673-4254.2020.02.06
57. Serafini G, Parmigiani B, Amerio A, Aguglia A, Sher L, Amore M. The psychological impact of COVID-19 on the mental health in the general population. QJM Int J Med. 2020;113(8):531–537. doi:10.1093/qjmed/hcaa201
58. Barros MB, de A Lima MG, Azevedo RCS, et al. Depression and health behaviors in Brazilian adults – PNS 2013. Rev Saúde Pública. 2017;51. doi:10.1590/S1518-8787.2017051000084
59. Allgöwer A, Wardle J, Steptoe A. Depressive symptoms, social support, and personal health behaviors in young men and women. Health Psychol off J Div Health Psychol Am Psychol Assoc. 2001;20(3):223–227.
60. Liu Y, Ozodiegwu ID, Yu Y, Hess R, Bie R. An association of health behaviors with depression and metabolic risks: data from 2007 to 2014 U.S. National Health and Nutrition Examination Survey. J Affect Disord. 2017;217:190–196. doi:10.1016/j.jad.2017.04.009
61. Mason JE, LeBouthillier DM, Asmundson GJG. Relationships between health behaviors, posttraumatic stress disorder, and comorbid general anxiety and depression. Cogn Behav Ther. 2019;48(3):184–199. doi:10.1080/16506073.2018.1498119
62. Duivis HE, de Jonge P, Penninx BW, Na BY, Cohen BE, Whooley MA. Depressive symptoms, health behaviors, and subsequent inflammation in patients with coronary heart disease: prospective findings from the heart and soul study. Am J Psychiatry. 2011;168(9):913–920. doi:10.1176/appi.ajp.2011.10081163
63. Scheier MF, Carver CS. Dispositional optimism and physical health: a long look back, a quick look forward. Am Psychol. 2018;73(9):1082–1094. doi:10.1037/amp0000384
64. Giltay EJ, Zitman FG, Kromhout D. Dispositional optimism and the risk of depressive symptoms during 15 years of follow-up: the Zutphen Elderly Study. J Affect Disord. 2006;91(1):45–52. doi:10.1016/j.jad.2005.12.027
65. Segerstrom SC. Optimism and immunity: do positive thoughts always lead to positive effects? Brain Behav Immun. 2005;19(3):195–200. doi:10.1016/j.bbi.2004.08.003
66. Troiano RP, McClain JJ, Brychta RJ, Chen KY. Evolution of accelerometer methods for physical activity research. Br J Sports Med. 2014;48(13):1019–1023. doi:10.1136/bjsports-2014-093546
67. Rowlands AV, Edwardson CL, Davies MJ, Khunti K, Harrington DM, Yates T. Beyond cut points: accelerometer metrics that capture the physical activity profile. Med Sci Sports Exerc. 2018;50(6):1323–1332. doi:10.1249/MSS.0000000000001561
68. Slimani N, Deharveng G, Charrondière RU, et al. Structure of the standardized computerized 24-h diet recall interview used as reference method in the 22 centers participating in the EPIC project. European Prospective investigation into cancer and nutrition. Comput Methods Programs Biomed. 1999;58(3):251–266. doi:10.1016/s0169-2607(98)00088-1
69. Denollet J. DS14: standard assessment of negative affectivity, social inhibition, and type D personality. Psychosom Med. 2005;67(1):89–97. doi:10.1097/01.psy.0000149256.81953.49
70. Farkas D, Orosz G. Ego-resiliency reloaded: a three-component model of general resiliency. PLoS One. 2015;10(3):e0120883. doi:10.1371/journal.pone.0120883
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.