Back to Journals » Journal of Pain Research » Volume 12
Emotional Effects on Factors Associated with Chronic Low Back Pain
Authors Ouchi K, Watanabe M, Tomiyama C, Nikaido T ![]() , Oh Z, Hirano T, Akazawa K, Mandai N
, Oh Z, Hirano T, Akazawa K, Mandai N
Received 14 July 2019
Accepted for publication 22 November 2019
Published 17 December 2019 Volume 2019:12 Pages 3343—3353
DOI https://doi.org/10.2147/JPR.S223190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Micheal Schatman
Koichi Ouchi,1 Mayumi Watanabe,2–4 Chikako Tomiyama,5 Takuya Nikaido,6 Zaigen Oh,2 Toru Hirano,7 Kohei Akazawa,1 Nozomu Mandai3
1Department of Medical Informatics, Niigata University Medical and Dental Hospital, Niigata, Japan; 2Faculty of Health Sciences, Kansai University of Health Sciences, Osaka, Japan; 3Center for Humanities and Sciences, Ibaraki Prefectural University of Health Sciences, Ibaraki, Japan; 4Faculty of Science and Engineering, Chuo University, Tokyo, Japan; 5Graduate School of Health Sciences, Niigata University, Niigata, Japan; 6Department of Orthopaedic Surgery, Fukushima Medical University School of Medicine, Fukushima, Japan; 7Department of Orthopedic Surgery, Uonuma Institute of Community Medicine, Niigata University Medical and Dental Hospital, Niigata, Japan
Correspondence: Mayumi Watanabe
Faculty of Health Sciences, Kansai University of Health Sciences, 2-11-1 Wakaba, Kumatoricho, Sennan-gun, Osaka 590-0482, Japan
Tel +81-72-453-8251
Fax +81-72-453-0276
Email [email protected]
Purpose: Although chronic low back pain (CLBP) has profound effects on patients, society, and economy, its causes are difficult to identify. Psychogenic effects or social stress is known to affect CLBP; hence, investigation of its underlying causes requires a multifactorial approach. We determined the factors associated with CLBP by using an Internet-based survey. To prevent CLBP, we need to understand its cause and background.
Patients and methods: A total of 1000 participants either with (+) or without (−) CLBP answered the Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ), which assesses five domains of CLBP: low back pain, lumbar function, walking ability, social life function and mental health. We also administered a new questionnaire for participants, that comprised five different domains: Body, Lifestyle, Emotion, Diet, and Social. To evaluate psychogenic effects on CLBP, we added two original factors, namely outshout and HIE, which have not yet been studied. HIE is a traditional concept (sense) of “feeling cold” or “chilly.” All participants completed both questionnaires.
Results: Multivariate logistic regression analysis extracted four factors (sleep, room temperature, outshout, and HIE) that were associated with CLBP. The mental health domain was assessed using the JOABPEQ for each of these factors. The factors outshout and HIE differed between CLBP (+) and CLBP (−) patients. CLBP (−) participants also showed a difference in Sleep and HIE factors.
Conclusion: Among psychogenic effects, Emotion was common to all the four extracted factors. There was no common physical divisor. Therefore, we hypothesized that acute low back pain might develop into CLBP in the presence of psychological stress or other emotional factors such as outshout or HIE. Hence, we need to consider both physical and psychogenic effects in the prevention and treatment of CLBP. Furthermore, appropriate evaluation and treatment of psychological stress may be effective in reducing CLBP.
Keywords: Japanese Orthopaedic Association Back Pain Evaluation Questionnaire, JOABPEQ, outshout, HIE, nonspecific low back pain
Plain Language Summary
Current lifestyle, improper sleeping habits, and unhealthy diet lead to psychological or social stress, which in turn is known to influence the development of chronic lower back pain (CLBP). However, the exact causes of CLBP are yet to be revealed. To shed more light on this issue, we undertook an Internet-based survey in which the participants had to answer a questionnaire related to five aspects of CLBP: low back pain, lumbar function, walking ability, social life function and mental health. In addition, we included two new variables, namely outshout (the expression of anger through outburst) and HIE (feeling of coldness). Based on our results, we think that psychological stress (especially emotional disturbance such outshout or HIE) could promote acute low back pain to develop into CLBP. We therefore recommend that timely diagnosis and treatment of psychological stress could help to minimize the incidence of CLBP.
Introduction
Low back pain (LBP) that persists for more than three months is defined as chronic low back pain (CLBP). Particularly, among carers and factory workers, CLBP frequently causes work absenteeism and has profound effects on the patients themselves, society, and the economy.1 In 2016, the Japanese Ministry of Health, Labour and Welfare estimated that 28 million people nationwide suffer from CLBP.2 Although some local governments in the country recently started a program of domiciliary visits to treat patients with CLBP, the effectiveness of this program has not yet been assessed.
LBP is often prolonged because the identification of its cause is difficult; physical factors such as smoking or lack of exercise have been implicated as the cause of prolonged LBP.3,4 However, 85% of CBLP is nonspecific, with no identified physiological, neural, or orthopedic disorders in the spine.5 Most CLBP cases show substantial discrepancies between the objective observations of medical practitioners and patients’ subjective complaints, thus suggesting causes other than physiological disorders. As psychogenic effects could affect CLBP, a multifaceted approach to both diagnosis and treatment is necessary.6
The Japanese Orthopaedic Association has recently developed a pain evaluation questionnaire (the Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ)) to assess five key domains of CLBP: low back pain, lumbar function, walking ability, social life function and mental health.7–9 It was subsequently suggested that psychological effects or social stress might also affect CLBP.10 To augment the JOABPEQ, we prepared a new questionnaire comprising five domains (Body, Lifestyle, Emotion, Diet, and Social) and further investigated psychogenic effects on CLBP using the original factors Outshout and HIE, which have not yet been identified.
We conducted a cross-sectional study on various factors using a web-based questionnaire-answering system to assess the possibility of profound psychogenic effects on CLBP, to hypothesize the development of CLBP, and to propose a new approach to CLBP, particularly nonspecific CLBP.
Methods
Participants
Participants were recruited from a database that is administered by a Japanese survey company (Cross Marketing Inc., Tokyo, Japan). Questionnaires were administered using an Internet-based survey conducted by a Japanese survey company (Cross Marketing Inc., Tokyo, Japan). From a total of 300,000 people listed in a database administered by this company, a subsample of 5000 subjects was drawn using random sampling stratified by age and place of residence. This subsample was re-sampled by proportional allocation to balance the gender ratio, yielding a final sample of 1000 subjects, including 519 males and 481 females. All participants used a web-based questionnaire-answering system provided by the survey company. Before starting the investigation, we informed all subjects that the data collected would be used only for research and that they could withdraw from the study at any time. We explained that their participation would be kept confidential. Informed consent was obtained from all subjects prior to enrollment. All 1000 subjects who accessed the survey web page responded and gave us informed consent before starting the questionnaire. This study was approved by the Medical Ethics Committee of Ibaraki Prefectural University of Health Sciences (Ibaraki, Japan, e135-h291212).
Chronic Low Back Pain
Chronic low back pain (CLBP) refers to pain, stiffness, decreased movement of the lower back, and difficulty in straightening one’s lower back, experienced for more than three months. Participants were divided into two groups: CLBP (−) (n = 714, 71.4%) and CLBP (+) (n = 286, 28.6%). In addition to the new questionnaire (Appendix), clinical details such as visits to doctors or diagnostic imaging were recorded (Figure 1).
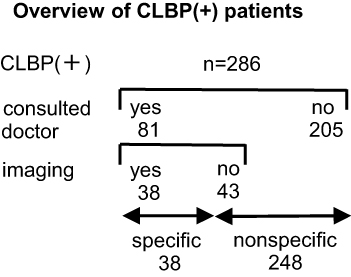 |
Figure 1 Overview of CLBP (+) patients. The total number of CLBP (+) subjects was 286. Eighty-one of them consulted doctors, while 205 of them did not. Thirty-eight of them had specific CLBP, whose cause was organic, and the rest of them (248) had nonspecific CLBP, whose cause was not organic. |
JOABPEQ
All subjects completed the JOABPEQ, a specific instrument for LBP evaluation developed by the Japanese Orthopaedic Association in 2007 by referring to Rolland-Morris Disability Questionnaire Score or SF36 (Medical Outcomes Study, a 36-Item Short-Form Health Survey).
JOABPEQ includes 25 questions in five domains: low back pain, lumbar function, walking ability, social life function and mental health. The score of each domain was calculated according to the official guidelines and ranged from 0 to 100 points. The lower the score, the worse is the patient’s condition. Participants were asked to report on various aspects of their CLBP condition during the preceding week.7–9
New Questionnaire (Body, Lifestyle, Emotion, Diet and Social)
The new questionnaire that we developed is presented in the Appendix.
Body [Age, Gender and Body Mass Index (BMI)]
The domain of Body has three subfactors of Age, Gender and Body Mass Index (BMI). In this study, subjects were drawn using random sampling stratified by age and gender in advance as mentioned. Subjects were asked to indicate the appropriate category for age [20–29, 30–39, 40–49, 50–59 (years)] and Gender (Male, Female).
Similar to previous studies, we also calculated BMI4,11,12 by asking their height (cm) and weight (kg), and then applied the following formula: BMI = weight (kg) ÷ height (m)2. We then categorized the subjects into three groups based on their BMI (<18.5, 18.5–24.9, ≥25.0)
Lifestyle [(Exercise, Bathing, Cigarette, Sleep and Room Temperature (RT)]
Lifestyle [Exercise,13 Bathing,14–16 Cigarette,4,17 Sleep18–20 and Room Temperature (RT)]21–23 affects CLBP. We asked subjects to select the frequency of their exercise (Hardly, Frequently, N/A), the style of their personal washing [Shower only, Bath (<10 min), Bath (≥10 min)], and the number of cigarettes smoked per day (0, 1–20, ≥20). We also asked them the duration of sleep (<6, 6–7, 7–8, ≥8 hrs per night) and the RT (<18 or ≥18 °C) of the location from where they were answering our questionnaire.
Emotion (Happiness, Anger, Outshout and HIE)
Researchers have reported that emotion can affect CLBP, therefore, we asked the subjects to select the frequency of their emotions of happiness and anger from never, sometimes, or frequently.24 We also asked participants to indicate frequency of outshout (the expression of anger through outburst) (Never, Sometimes, Frequently).
HIE, a well-known concept within traditional Chinese medicine (TCM), is a subjective sense of “feeling cold” or “chilly”. “Mild” HIE is a simple sense of being chilly, whereas “severe” indicates feelings of discomfort.25–28 Therefore, first we asked participants about the presence or absence of HIE, and if present, its severity (Never, Mild, Severe).
Diet (Red Meat, White Meat and Cold Food)
In accordance with previous studies, we asked the subjects to rate the frequency of intake of red meat, white meat, and cold food (Hardly, Frequently, N/A).28,29
Social (Occupation and Residence)
One’s social situation may influence CLBP; therefore, we asked subjects to provide information about their occupation (Manager, Full-time, Part-time/no job)30,31 and residence (North area, East, area, West area, South area of Japan).32
Outshout and HIE–Original Factors
Although the causes of CLBP are difficult to identify, researchers have reported the possibility of emotional influence on CLBP.10,24 We constructed an original factor, Outshout, in the emotional domain because emotion may affect our behavior and health through the hypothalamic-pituitary-adrenal system.33,34 For example, laughter, an expression of the emotion happiness, has a positive physiological effect.35,36 Conversely, it is known that anger may exacerbate LBP.37–40 In order to compare the effect of emotions on LBP, an objective indicator of emotional status is required; that is why we devised the outcome measure that we named “outshout.” The action of shouting out loud is considered as an expression of anger and/or frustration. We analyzed the frequency of outshout, with the reasoning that we could infer a higher degree of emotional turmoil from an increased frequency of outshout.
The second original factor that we incorporated into our new questionnaire was HIE in the emotion domain. This is a subjective sense of “feeling cold” or “chilly.” In traditional Chinese medicine (TCM), HIE is called Xuhan, and it is known to induce pain including CLBP.41 Local/small studies25–28 cannot be a good evidence. We quantified HIE (a traditional concept) by measuring body temperature (a modern concept) because according to a recent study, HIE may be modified by multiple factors including emotion.42 Other information that might affect both body temperature and HIE was obtained through the questionnaire, such as the RT while answering the questionnaire and the current diet followed.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics software for Windows version 25.0 (IBM Corp., Armonk, NY, USA). Means (± standard deviations) were used to characterize the distributions of continuous variables.
First, Pearson’s chi-squared test was conducted to study the two groups [CLBP (+) or CLBP (−)] and determine candidate factors of the multivariate analysis.
Next, multiple logistic regression analysis with forward stepwise model selection was performed to determine the factors significantly associated with CLBP. Candidate factors of the multivariate analysis are shown in Tables 1 and 2. The values are expressed as 95% confidence interval and adjusted odds ratio (OR). The dependent variable in the multiple logistic regression models was binary: CLBP (−) and CLBP (+), and the null hypothesis was that the probability of observing a regression coefficient of 0 or 1 is influenced solely by chance rather than by any of the independent variables.
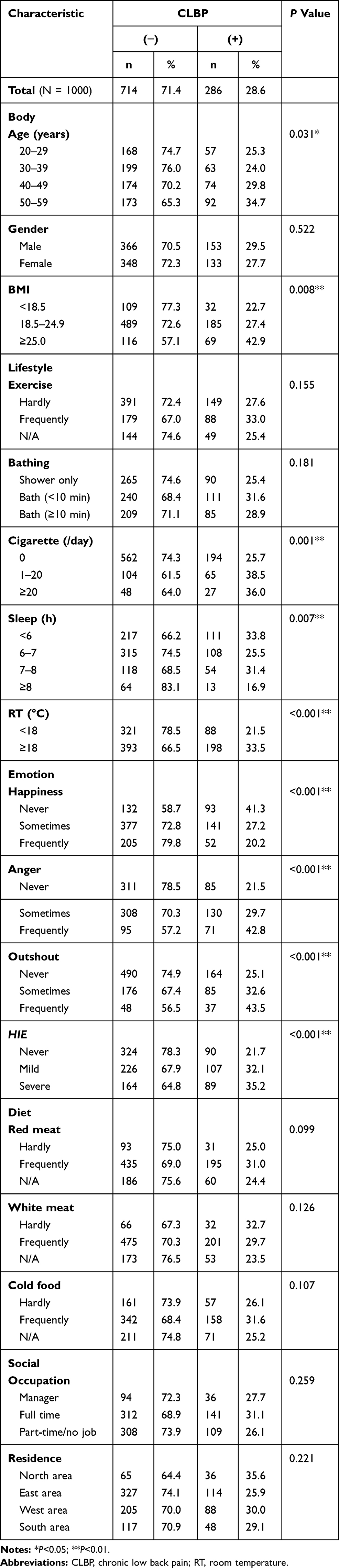 |
Table 1 Characteristics of the CLBP (+) and CLBP (−) Groups |
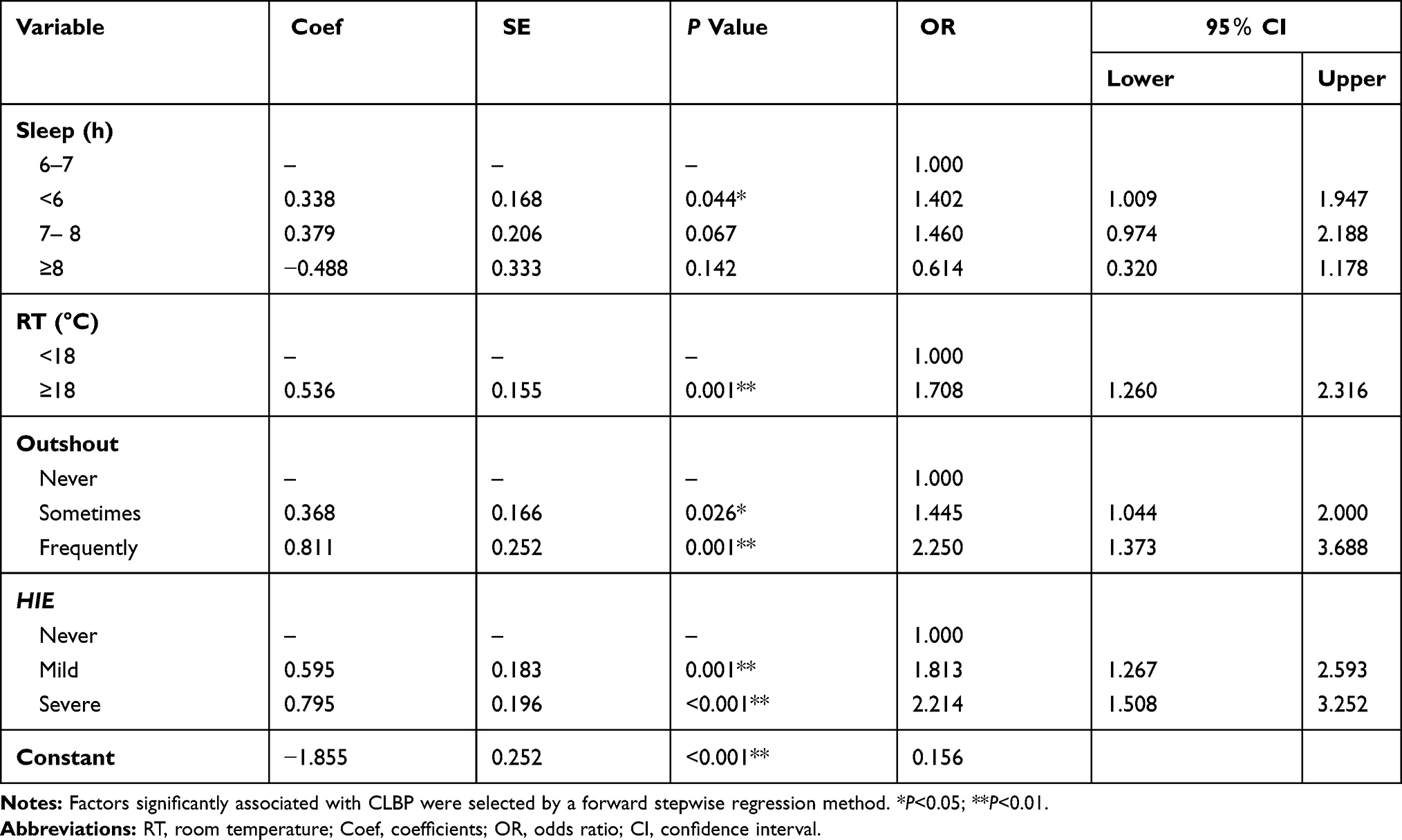 |
Table 2 Results of Multivariate Logistic Regression Analysis |
Axillary temperatures of the two groups were compared using Student’s t-test to study the possibility that low temperature affects CLBP. The relationship between CLBP and HIE was assessed using Spearman’s rank correlation coefficient. Each domain of the JOABPEQ (rank scale) was evaluated independently.
Finally, to study the psychological effects on CLBP, a Mann–Whitney U-test was conducted to compare the medians of each factor among the CLBP (+) patients. The association between the domain of mental health disorders (JOABPEQ) and the significant factors identified by multiple logistic regression analysis was assessed by differences in these medians.
All statistical tests were two-tailed, and a statistical significance was set at P<0.05.
Results
Nine Factors Significantly Associated with CLBP
The basic characteristics of the participants included this study is shown in the table. Of our 1000 participants (average age ± SD; 40.5 ± 10.8 years), 286 (28.6%) were grouped as CLBP (+) patients, including 153 males and 133 females (Table 1). We conducted Pearson’s chi-squared test to compare the two groups [CLBP (+) or CLBP (−)] and determine candidate factors of the multivariate analysis. Our result identified 9 factors [(1) – (9)] in 3 domains (Body, Lifestyle and Emotion) that were significantly associated with CLBP: in the Body domain, 1) Age (P = 0.031), 2) BMI (P = 0.008); in the Lifestyle domain, 3) Cigarettes/day (P = 0.001), 4) Sleep (h) (P = 0.007), 5) RT (P < 0.001); and in the Emotion domain, 6) Happiness, 7) Anger, 8) Outshout, and 9) HIE (P < 0.001 for factors 6–9). It is noteworthy that all factors in the Emotion domain showed highly significant association with CLBP.
Four Factors Significantly Associated with CLBP
Four independent variables that showed interactions or multicollinearity among each other were excluded from the multivariate logistic regression analysis: 1) BMI (with Age), 2) Cigarettes/day (with Age and Outshout), 3) Happiness (with Sleep), and 4) Anger (with Outshout). Multivariate logistic regression analysis was conducted, thus identifying further four factors that were associated with CLBP (Table 2).
For Sleep, the OR for the “<6” category was significantly higher than that for “6 to 7,” which was the average sleeping duration of Japanese people in 2016 (1.000 and 1.402, respectively).43 For RT (°C), the OR for the ≥18 °C group was higher than that for the <18 °C group (1.000 vs 1.708). For Outshout, OR increased with an increase in the frequency: ORs for “sometimes” and “frequently” were higher than that for “never” (1.000, 1.445, and 2.250, respectively); HIE showed a similar tendency, with ORs for “mild” and “severe” higher than that for “never” (1.000, 1.813, and 2.214, respectively).
Possibility of the Effect of Low Body Temperature (BT) on CLBP
There was no significant difference in body temperature observed between the two groups (36.18 ± 036 and 36.16 ± 0.37 °C for CBLP (−) and (+), respectively, P = 0.525, Student’s t-test). The same was true for subgroups of CBLP (−) and (+) according to age or gender (Table 3).
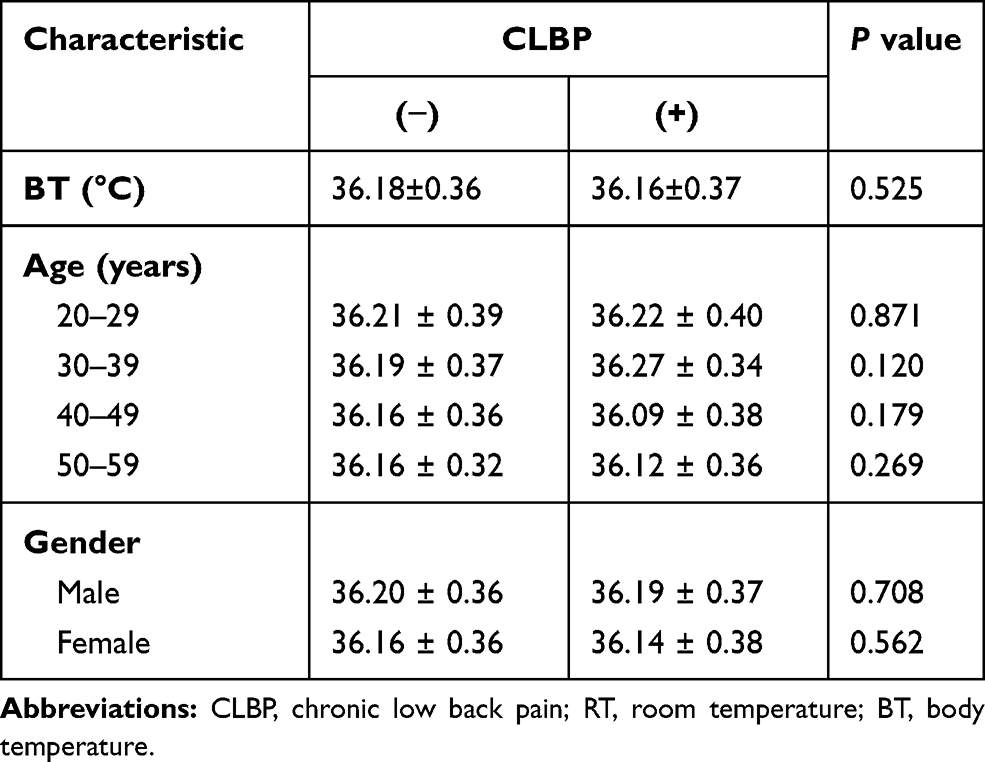 |
Table 3 Possibility of the Effect of Low Temperature on CLBP (Student’s t-Test) |
Relationship Between HIE and CLBP
Spearman’s rank correlation coefficients assessing the relationship between HIE and each of the five domains of the JOABPEQ identified the possible effects of HIE on CLBP (Table 4). HIE was negatively related to all five domains, with mental health disorders showing the strongest correlation (rs = −0.232, P < 0.001, Table 4).
 |
Table 4 Effect of HIE on CLBP |
Association of Mental Health Domain (JOABPEQ) with Sleep, RT, Outshout, and HIE
The scores of mental health (JOABPEQ) domain on four factors (Sleep, RT, Outshout, and HIE) indicated significant associations between CLBP and these factors (Table 2). We compared the score of OR = 1.000 (□) and that of OR > 1.000 (■) for each factor among CLBP (+) patients. In this study, CLBP (+) patients had a significant difference in the factors of Outshout and HIE (P < 0.05, Figure 2).
 |
Figure 2 The scores of “mental health” on the four factors among CLBP (+) patients. We compared the score of OR = 1.000 (□) and that of OR > 1.000 (■) for each factor among CLBP (+) patients. ━, median; *P < 0.05. Abbreviations: CLBP, chronic low back pain; RT, room temperature. |
Discussion
Four Factors (Sleep, RT, Outshout, and HIE) Associated with CLBP
We analyzed the results of the questionnaire consisting of 18 factors that belong to five domains. Of the 18 factors, four were identified to have significant association with CLBP: 1) Sleep (h), 2) RT (°C), 3) Outshout, and 4) HIE, which are described below (Tables 1 and 2).
Sleep
First, our result showed that OR of the <6 h group, less than the Japanese average sleeping hours, was significantly higher than that of the 6–7 h group, the Japanese average sleeping hours. As sleeping duration is related to time spent lying down, individuals with longer habitual sleep periods may experience decreased physical stress that leads to lumbar spine dysfunction. Many studies suggest that inappropriate sleeping duration worsens CLBP.44–47
Moreover, the autonomic nervous system (ANS) that controls our whole body shifts from sympathetic nerve dominance during waking to parasympathetic nerve dominance during sleep.48 An inappropriate sleep affects the function of ANS and circulation.44–47 In the long term, inappropriate sleep periods may induce the onset of depression as psychogenic stress.
RT
For the RT factor, the OR for the “≥18 °C” group was prominently higher than that of the “<18 °C” group in association with CLBP. It is known that the incidence of CLBP increases in cold seasons.49 It is considered that cold stimulation may affect and induce vasoconstriction, circulation insufficiency, or hypothermia.50 On the other hand, it is known that immersion in warm baths may ameliorate mild LBP because it elevates body temperature and improves circulation.14–16
In our study, most CLBP (+) subjects had mild LBP; therefore, they might prefer warmer RT to reduce their LBP by elevating their body temperature or by the improvement of circulation. In our 286 CLBP (+) subjects, only 38 had undergone imaging tests and received a clinical diagnosis of an organic cause (Figure 1). The remaining 248 subjects might be considered to have nonspecific LBP. Moreover, 205 CLBP subjects reported that their CLBP was not severe enough to warrant regular visits to doctors. A further study is needed to determine the association between severe CLBP and RT.
Outshout
The OR increased with an increase in the frequency of this new factor (Table 2). As mentioned earlier in the Methods section, Outshout, a psychological factor, affects CLBP. Both the expression of anger and attempts to inhibit this emotion are harmful to our health and are associated with coronary diseases.51 Rather than having the expected cathartic effect, the expression of anger is accompanied by elevated psychological stress and aggression.52,53 Thus, the stress underlying Outshout might increase for anger, possibly causing circulatory insufficiency and CLBP because of increase in the secretion of stress hormones such as adrenaline or cortisol.54,55 Moreover, patients reporting frequent Outshout may be more affected by psychological stress than those reporting its occasional occurrence. This may explain why OR for patients in the former category was higher than that for those in the latter category. In this study, the presence of alexithymia in study subjects, which is a marked dysfunction in emotional awareness, was not confirmed. Although it is a rare case, further research on this topic is warranted.
HIE
HIE is a well-known concept within TCM and has both physical and psychological stress components.56,57 Table 2 shows a positive association between HIE and CLBP. As long as HIE remains within the level of “mild,” psychological stress is hardly detectable, but once HIE progresses from “mild” to “severe,” reflecting increased psychological stress, it causes pain in the lower back, neck, shoulder, eyes, and other parts of the body. “Mild” HIE is a simple sense of being chilly, whereas “severe” indicates feelings of discomfort. Our results showed that the OR for patients reporting “severe” HIE was higher than that for reporting “mild,” probably reflecting increased psychological stress in the former group (Table 2).
The Possibility of Physical Effects Common to Four Factors
To discover a cause or exacerbating factor of CLBP, we considered which physical effect might be common to the four factors of Sleep, RT, Outshout, and HIE. Circulatory insufficiency or hypothermia were considered as possibilities. Therefore, the CLBP (−) and CLBP (+) groups were compared to analyze the possibility of the association between decreased body temperature (axilla) and CLBP. However, no significant difference was observed between the two groups. The same result was obtained when these two groups were divided into subgroups according to their age or gender (Table 3). This may be attributed to the wide physical variation among our subjects, who included both males and females aged from 20 to 59 years.
The Possibility of Psychogenic Effects Common to Four Factors and Their Association with CLBP
To determine the possibility of psychogenic effects on CLBP, the Spearman’s rank correlation coefficient test was conducted with HIE and JOABPEQ data. The mental health domain showed the highest correlation among the five domains (rs = −0.232, P < 0.001, Table 4).
Moreover, CLBP (+) patients showed significant difference in the score of “mental health” only in Outshout and HIE. They indicated difference neither Sleep nor RT (P < 0.05, Figure 2). The former factors belong to Emotion while the latter ones belong to Lifestyle.
Therefore, those significant differences support the possibility that emotional stress may be more severe than physical one. In short, Lifestyle might induce acute LBP, however, it could decrease by the improvement of Sleep or RT, for example. However, at this time point, data for acute LBP are inefficient, therefore, further investigation is needed.
Hypothesized Development from Acute to Nonspecific LBP and the Possibility of a New Approach to CLBP
In our consideration of the association between mental health (a domain of JOABPEQ) and the four factors significantly associated with CLBP (Sleep, RT, Outshout, and HIE), two important results were found. First, multivariate logistic regression analysis highlighted only two domains (Lifestyle and Emotion) out of five that were related to CLBP. Second, interestingly it was shown that all factors within the Emotion domain differed significantly between participants with and without CLBP. These findings led us to propose a hypothesis about the onset of nonspecific LBP without organic causes (Figure 3).
 |
Figure 3 A hypothesis for the development of nonspecific low back pain. |
In some patients, LPB may be caused by only physical factors; these patients can often recover within three months. However, when emotional factors also contribute to their LBP, patients may suffer for over three months. We hypothesize that psychological factors may lead from acute LBP to CLBP, thus explaining why 85% of CBLP is nonspecific; emotional factors are undetectable by conventional medical checks, such as various imaging techniques.
Even if physical stress from poor Lifestyle induced acute LBP, this could be ameliorated with adequate sleeping time or improvement of circulation. However, when psychological stress exists, which may potentially induce Outshout or HIE, this might prolong acute LBP and lead to nonspecific LBP, even if the organic cause itself could be managed.
It is, therefore, possible that psychological stress, such as Outshout or HIE, might underlie CLBP. Hence, consideration of both physical and psychogenic effects is of key importance for the prevention of CLBP. The development of therapies for CLBP should include appropriate evaluation and treatment of psychogenic effects, particularly those related to emotion.
CLBP patients might benefit from psychosocial treatment. Recent RCT studies of cognitive behavioral therapy,58 the addition of therapeutic alliance,59 and mindfulness60 revealed the effectiveness of psychosocial treatment on CLBP, for example. Thus, the psychological factors are important to take into account when examining and treating these patients.
Limitations
The first limitation of this study is the limited sample size; thus, further research on a larger scale is required to assess our findings. Second, because the invitation for participation in the survey was sent over the Internet, only those participants who frequently use the Internet might have participated, and hence, the sample size was small. Therefore, this study sample may not be a representative of the wider population. These would be valuable factors to assess in any future study, and some of the conclusions drawn here will lead to further debate.
Conclusion
We identified that our factors (Sleep, RT, Outshout, and HIE) are significantly associated with an increase in ORs for CLBP. This suggests that appropriate understanding, evaluation of, and approach to psychogenic effects, especially those of emotion, are important for multifaceted treatment of CLBP.
Acknowledgments
The authors thank all volunteers who participated in this study. We would also like to thank Editage for assistance in English language editing. This study was supported by The Uchida Energy Science Promotion Foundation (Grant no. 1-1-59) and the Japan Society for the Promotion of Science’s Grants-in-Aid for Scientific Research (Kakenhi Grant No. 19K10727).
Author Contributions
KO, MW and CT contributed to conception and design, analysis, drafting and critical revision of the manuscript. TN and ZO contributed to conception, interpretation, drafting and critical revision of the manuscript. TH and KA contributed to conception and design, interpretation, drafting and critical revision of the manuscript. NM contributed to conception, data analysis, drafting and critical revision of the manuscript. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work, ensuring integrity and accuracy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mathew J, Singh SB, Garis S, et al. Backing up the stories: the psychological and social costs of chronic low-back pain. Int J Spine Surg. 2013;7:e29–e38. doi:10.1016/j.ijsp.2013.02.001
2. Ministry of Health, Labour and Welfare. Comprehensive survey of living conditions; 2016. Available from: https://www.mhlw.go.jp/toukei/saikin/hw/k-tyosa/k-tyosa16/dl/04.pdf.
3. Shmagel A, Foley R, Ibrahim H. Epidemiology of chronic low back pain in US adults: data from the 2009–2010 national health and nutrition examination survey. Arthritis Care Res (Hoboken). 2016;68:1688–1694. doi:10.1002/acr.v68.11
4. Power C, Frank J, Hertzman C, et al. Predictors of low back pain onset in a prospective British study. Am J Public Health. 2001;91:1671–1678. doi:10.2105/AJPH.91.10.1671
5. Deyo RA, Weinstein JN. Low back pain. N Engl J Med. 2001;344:363–370. doi:10.1056/NEJM200102013440508
6. Konno S, Sekiguchi M. Association between brain and low back pain. J Orthop Sci. 2018;23:3–7. doi:10.1016/j.jos.2017.11.007
7. Fukui M, Chiba K, Kawakami M, et al. Japanese Orthopaedic Association back pain evaluation questionnaire. Part 2. verification of its reliability: the subcommittee on low back pain and cervical myelopathy evaluation of the clinical outcome committee of the Japanese Orthopaedic Association. J Orthop Sci. 2007;12:526–532. doi:10.1007/s00776-007-1168-4
8. Fukui M, Chiba K, Kawakami M, et al. Japanese orthopaedic association back pain evaluation questionnaire. Part 3. validity study and establishment of the measurement scale: subcommittee on low back pain and cervical myelopathy evaluation of the clinical outcome committee of the Japanese Orthopaedic Association, Japan. J Orthop Sci. 2008;13:173–179. doi:10.1007/s00776-008-1213-y
9. Fukui M, Chiba K, Kawakami M, et al. JOA back pain evaluation questionnaire (JOABPEQ)/JOA cervical myelopathy evaluation questionnaire (JOACMEQ). The report on the development of revised versions. The subcommittee of the clinical outcome committee of the Japanese orthopaedic association on low back pain and cervical myelopathy evaluation. Orthop Sci. 2009;14:348–365.
10. Nikaido T, Fukuma S, Wakita T, et al. Development of a profile scoring system for assessing the psychosocial situation of patients with chronic musculoskeletal pain. J Pain Res. 2017;10:1853–1859. doi:10.2147/JPR
11. Konishi H, Kaneda K, Takemitsu Y, et al. A study of medico-social factors related to delayed return to work in worker with low back pain. JJOMT. 2006;54:183–187.
12. Matsumoto M, Kinoshita G, Shiraki T, et al. Addressing occupational low back pain (OLBP): the role of good posture and education. J Lumbar Spine Disord. 2001;7:73–78. doi:10.3753/yotsu.7.73
13. Hartvigsen J, Christensen K. Active lifestyle protects against incident low back pain in seniors: a population-based 2-year prospective study of 1387 Danish twins aged 70–100 years. Spine (Phila Pa 1976). 2007;32:76–81. doi:10.1097/01.brs.0000250292.18121.ce
14. Freiwald J, Hoppe MW, Beermann W, et al. Effects of supplemental heat therapy in multimodal treated chronic low back pain patients on strength and flexibility. Clin Biomech (Bristol, Avon). 2018;57:107–113. doi:10.1016/j.clinbiomech.2018.06.008
15. Baig AAM, Ahmed SI, Ali SS, et al. Role of posterior-anterior vertebral mobilization versus thermotherapy in non specific lower back pain. Pak J Med Sci. 2018;34:435–439. doi:10.12669/pjms.342.12402
16. Pittler MH, Karagülle MZ, Karagülle M, et al. Spa therapy and balneotherapy for treating low back pain: meta-analysis of randomized trials. Rheumatology (Oxford). 2006;45:880–884. doi:10.1093/rheumatology/kel018
17. Hestbaek L, Leboeuf-Yde C, Kyvik KO. Are lifestyle-factors in adolescence predictors for adult low back pain? A cross-sectional and prospective study of young twins. BMC Musculoskelet Disord. 2006;7:27. doi:10.1186/1471-2474-7-27
18. Nakajima H. Association between sleep duration and hemoglobin A1c level. Sleep Med. 2009;10:937–938. doi:10.1016/j.sleep.2009.05.001
19. Youngstedt SD, Kripke DF. Long sleep and mortality: rationale for sleep restriction. Sleep Med Rev. 2004;8:159–174. doi:10.1016/j.smrv.2003.10.002
20. Kripke DF, Garfinkel L, Wingard DL. Mortality associated with sleep duration and insomnia. Arch Gen Psychiatry. 2002;59:131–136. doi:10.1001/archpsyc.59.2.131
21. Nakajima Y, Schmidt SM, Malmgren Fänge A, et al. Relationship between perceived indoor temperature and self-reported risk for frailty among community-dwelling older people. Int J Environ Res Public Health. 2019;16:613. doi:10.3390/ijerph1604061316
22. Tsuboi S, Mine T, Tomioka Y. Are cold extremities an issue in women’s health? Epidemiological evaluation of cold extremities among Japanese women. Int J Women Health. 2019;11:31–39. doi:10.2147/IJWH.S190414
23. Hayashi Y, Schmidt SM, Malmgren Fänge A, et al. Lower physical performance in colder seasons and colder houses: evidence from a field study on older people living in the community. Int J Environ Res Public Health. 2017;14:651. doi:10.3390/ijerph14060651
24. Yang H, Haldeman S, Lu ML, et al. Low back pain prevalence and related workplace psychosocial risk factors: a study using data from the 2010 national health interview survey. J Manipulative Physiol Ther. 2016;39:459–472. doi:10.1016/j.jmpt.2016.07.004
25. Yamato T, Aomine M. Physical characteristics and living environment in female students with cold constitution. HEP. 2002;29:878–884. doi:10.7143/jhep.29.878
26. Saga M, Imai M. Study of painful chills and associated factors in female university students. Ishikawa j Nurs. 2012;9:91–99.
27. Imai M, Akasofu K, Fukunishi H. Subjective chills and their related factors in adult women. Ishikawa J Nurs. 2007;4:55–64.
28. Sannomaru Y, Akiyama T, Numajiri S. Relationship of lifestyle and frequency of certain types of food intake on the chilliness of female college students. J Jpn Soc Food Life. 2016;26:197–204.
29. Nagata C, Wada K, Tamura T, et al. Hot-cold foods in diet and all-cause mortality in a Japanese community: the Takayama study. Ann Epidemiol. 2017;27:194–199. doi:10.1016/j.annepidem.2017.01.005
30. Kaneda K, Shirai Y, Miyamoto M. An epidemiological study on occupational low back pain among people who work in construction. J Nippon Med Sch. 2001;68:310–317. doi:10.1272/jnms.68.310
31. Matsudaira K, Kawaguchi M, Isomura T, et al. Assessment of psychosocial risk factors for the development of non-specific chronic disabling low back pain in Japanese workers-findings from the Japan Epidemiological Research of Occupation-related Back Pain (JOB) study. Ind Health. 2015;53:368–377. doi:10.2486/indhealth.2014-0260
32. Ling Y, Watanabe M, Yoshii H, et al. Characteristics linked to the reduction of stigma towards schizophrenia: a pre-and-post study of parents of adolescents attending an educational program. BMC Public Health. 2014;14:258. doi:10.1186/1471-2458-14-258
33. Selye H. Stress and the general adaptation syndrome. Br Med J. 1950;1:1383–1392. doi:10.1136/bmj.1.4667.1383
34. McEwen BS. Protection and damage from acute and chronic stress: allostasis and allostatic overload and relevance to the pathophysiology of psychiatric disorders. Ann N Y Acad Sci. 2004;1032:1–7. doi:10.1196/annals.1314.001
35. Hayashi K, Kawachi I, Ohira T, et al. Laughter is the best medicine? A cross-sectional study of cardiovascular disease among older Japanese adults. J Epidemiol. 2016;26:546–552. doi:10.2188/jea.JE20150196
36. Sakurada K, Konta T, Watanabe M, et al. Associations of frequency of laughter with risk of all-cause mortality and cardiovascular disease incidence in a general population: findings from the Yamagata study. J Epidemiol. 2019. doi:10.2188/jea.JE20180249
37. Carson JW, Keefe FJ, Lowry KP, et al. Conflict about expressing emotions and chronic low back pain: associations with pain and anger. J Pain. 2007;8:405–411. doi:10.1016/j.jpain.2006.11.004
38. Burns JW, Gerhart JI, Bruehl S, et al. Anger arousal and behavioral anger regulation in everyday life among patients with chronic low back pain: relationships to patient pain and function. Health Psychol. 2015;34:547–555. doi:10.1037/hea0000091
39. Nisenzon AN, George SZ, Beneciuk JM, et al. The role of anger in psychosocial subgrouping for patients with low back pain. Clin J Pain. 2014;30:501–509. doi:10.1097/AJP.0000000000000019
40. Bruehl S, Liu X, Burns JW, et al. Associations between daily chronic pain intensity, daily anger expression, and trait anger expressiveness: an ecological momentary assessment study. Pain. 2012;153:2352–2358. doi:10.1016/j.pain.2012.08.001
41. Mori H, Kuge H, Sakaguchi S, et al. Determination of symptoms associated with hiesho among young females using hie rating surveys. J Integr Med. 2018;16:34–38. doi:10.1016/j.joim.2017.12.005
42. Uchida Y, Tsunekawa C, Sato I, et al. Effect of the menstrual cycle phase on foot skin temperature during menthol application in young women. Therm Biol. 2019;85:102401. doi:10.1016/j.jtherbio.2019.102401
43. Ministry of Health, Labour and Welfare. National health and nutrition survey report; 2017. Available from: https://www.mhlw.go.jp/content/10904750/000351576.pdf.
44. Yabe Y, Hagiwara Y, Sekiguchi T, et al. Late bedtimes, short sleeping time and longtime video-game playing are associated with low back pain in school-aged athletes. Eur Spine J. 2018;27:1112–1118. doi:10.1007/s00586-017-5177-5
45. Generaal E, Vogelzangs N, Penninx BW, et al. Insomnia, sleep duration, depressive symptoms, and the onset of chronic multisite musculoskeletal pain. Sleep. 2017;40. doi:10.1093/sleep/zsw030
46. Gottlieb DJ, Redline S, Nieto FJ, et al. Association of usual sleep duration with hypertension: the sleep heart health study. Sleep. 2006;29:1009–1014. doi:10.1093/sleep/29.8.1009
47. Kaneita Y, Ohida T, Uchiyama M, et al. The relationship between depression and sleep disturbances: a Japanese nationwide general population survey. J Clin Psychiatry. 2006;67:196–203. doi:10.4088/JCP.v67n0204
48. Suzuki S, Toyabe S, Moroda T, et al. Circadian rhythm of leucocytes and lymphocytes subsets and its possible correlation with the function of the autonomic nervous system. Clin Exp Immunol. 1997;110:500–508. doi:10.1046/j.1365-2249.1997.4411460.x
49. Igarashi H. Epidemiological studies on low back pain in a small rural community. Kitakanto Med j. 1968;18:99–150. doi:10.2974/kmj1951.18.99
50. Burström L, Järvholm B, Nilsson T, et al. Back and neck pain due to working in a cold environment: a cross-sectional study of male construction workers. Int Arch Occup Environ Health. 2013;86:809–813. doi:10.1007/s00420-012-0818-9
51. Denollet J, Gidron Y, Vrints CJ, et al. Anger, suppressed anger, and risk of adverse events in patients with coronary artery disease. Am J Cardiol. 2010;105:1555–1560. doi:10.1016/j.amjcard.2010.01.015
52. Bushman BJ, Baumeister RF, Stack AD. Catharsis, aggression, and persuasive influence: self-fulfilling or self-defeating prophecies? J Pers Soc Psychol. 1999;76:367–376. doi:10.1037/0022-3514.76.3.367
53. Bushman BJ. Does venting anger feed or extinguish the flame? Catharsis, rumination, distraction, anger, and aggressive responding. Personality Social Psychol Bull. 2002;28:724–731. doi:10.1177/0146167202289002
54. Watanabe M, Tomiyama-Miyaji C, Kainuma E, et al. Role of alpha-adrenergic stimulus in stress-induced modulation of body temperature, blood glucose and innate immunity. Immunol Lett. 2008;115:43–49. doi:10.1016/j.imlet.2007.09.010
55. Kainuma E, Watanabe M, Tomiyama-Miyaji C, et al. Association of glucocorticoid with stress-induced modulation of body temperature, blood glucose and innate immunity. Psychoneuroendocrinology. 2009;34:1459–1468. doi:10.1016/j.psyneuen.2009.04.021
56. Mozaffarieh M, Fontana GP, Schötzau A, et al. Thermal discomfort with cold extremities in relation to age, gender, and body mass index in a random sample of a Swiss urban population. Popul Health Metr. 2010;8:17. doi:10.1186/1478-7954-8-17
57. Yoshino T, Katayama K, Munakata K, et al. Statistical analysis of hie (cold sensation) and hiesho (cold disorder) in kampo clinic. Evid Based Complement Alternat Med. 2013;2013:398458. doi:10.1155/2013/398458
58. Ikemoto T, Miki K, Matsubara T, et al. Psychological Treatment strategy for chronic low back pain. Spine Surg Relat Res. 2018;3:199–206. doi:10.22603/ssrr.2018-0050
59. Fagundes FR, de Melo Do Espírito Santo C, de Luna Teixeira FM, et al. Effectiveness of the addition of therapeutic alliance with minimal intervention in the treatment of patients with chronic, nonspecific low back pain and low risk of involvement of psychosocial factors: a study protocol for a randomized controlled trial (TalkBack trial). Trials. 2017;18:49. doi:10.1186/s13063-017-1784-z
60. Cherkin DC, Sherman KJ, Balderson BH, et al. Effect of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care on back pain and functional limitations in adults with chronic low back pain: a randomized clinical trial. JAMA. 2016;315:1240–1249. doi:10.1001/jama.2016.2323
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.