Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Emollients “Plus” are Beneficial in Both the Short and Long Term in Mild Atopic Dermatitis
Authors Cestari S, Correia P ![]() , Kerob D
, Kerob D
Received 19 June 2023
Accepted for publication 1 August 2023
Published 8 August 2023 Volume 2023:16 Pages 2093—2102
DOI https://doi.org/10.2147/CCID.S417622
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Anne-Claire Fougerousse
Silmara Cestari,1 Priscila Correia,2 Delphine Kerob3
1Department of Dermatology, Sírio Libanês Hospital, São Paulo, Brazil; 2Scientific Expertise, L’Oréal Brazil, Rio de Janeiro, Brazil; 3Medical Direction, La Roche-Posay Laboratoire Dermatologique, Levallois-Perret, France
Correspondence: Priscila Correia, Scientific Expertise, L’Oréal Brazil, Rio de Janeiro, Brazil, Email [email protected]
Introduction: Atopic dermatitis (AD) is a chronic relapsing disease with a pathophysiology including skin barrier damage, microbiome disbalance and inflammation. Classically, emollients maintaining a healthy microbiome are recommended as the basis of any AD severity management.
Objective: To assess the benefit of a light balm containing vitamin E, tocopherol and glycerine and enriched with Aqua posae filiformis and microresyl (Emollient+) in subjects with mild AD over a period of 168 days.
Materials and Methods: For this open-label study, subjects above 3 years of age with mild and stable AD for at least 6 months before inclusion and with a SCORAD score of < 25 were eligible. Assessments took place at baseline, D14, D28, D84 and D168, and included SCORAD, flare frequency, severity of clinical signs and symptoms, skin hydration status using a Corneometer and local tolerance. QoL was assessed using the DLQI or CDLQI questionnaire. Subjects used Emollient+ at least once daily.
Results: Overall, 56 subjects were included in this study. The mean age was 25.0± 20.0 years (45% children); 69.6% were females. Except for erythema in the paediatric population, all clinical parameters had significantly (all p < 0.05) improved at D28. At D168, SCORAD, signs and symptoms had significantly (all p < 0.05) improved in the global, adult and paediatric population at D168 compared to baseline. So did flares, skin hydration and QoL. The regimen was very well tolerated.
Conclusion: Emollient+ is highly beneficial and well tolerated in mild AD with early benefits in improving AD signs and symptoms and skin hydration as well as the QoL of subjects as soon as D28.
Clinicaltrials.gov identifier: NCT05783453.
Keywords: atopic dermatitis, emollients, long term use
Introduction
Atopic dermatitis (AD) is a complex, chronic relapsing skin disease characterized by underlying skin barrier porosity, microbiome disbalance, changes in pH, transepidermal water loss and type-2 inflammation.1–5 Staphylococci colonization or infection has been associated with this pathology and the proportion of Staphylococcus sequences, especially that of S. aureus, was shown to be more important during disease flares than at baseline or post treatment.5–7
The clinical diagnosis of AD is based on the clinical assessment of signs, including erythema, oedema, oozing, lichenification and xerosis or dry skin, that can be localized or affect a widespread body surface area. Mild to moderate AD is symptomatic and intense pruritus, desquamation, and sleep loss are frequently reported symptoms.8,9
Currently, the use of emollients, including active ingredients maintaining a healthy skin microbiome, is recommended in the daily management of AD of any severity.2,10–13 Published and yet unpublished data show that they allow the skin barrier function to improve and reduce skin sensitivity to irritants, improve pruritus and the vicious itch/scratch cycle, decrease flares of inflammatory lesions and spare the need to use TCS.14–17 For these reasons, emollients are part of therapeutic management and present a non-medicated means to increase time between relapses.
In mild to moderate AD, a light balm (LIPIKAR BAUME LIGHT AP+M, La Roche-Posay Laboratoire Dermatologique, hereafter Emollient+) containing vitamin E, tocopherol and glycerine and enriched with Aqua posae filiformis and microresyl and enriched with Aqua posae filiformis and microresyl that prevents biofilm has shown to decrease flares and to restore a healthy microbiome compared to a control emollient.18 Moreover, another study shows that Emollient+ significantly reduces pruritus compared to usual emollients in moderate to severe AD patients under systemic therapy.19
AD and its relapses heavily impact the patients’ quality of life (QoL), expenditures and society costs.20–23 Recent cost-effectiveness studies have demonstrated that, as a maintenance regimen, the applied emollient is a cost-effective option compared to no treatment in adult subjects with AD patients.24,25
The present study assessed the clinical benefit and local tolerance of a Emollient+ in subjects aged above 3 years with mild atopic dermatitis and benefit after 168 days of use.
Materials and Methods
This open-label study was conducted at one investigational site in Rio de Janeiro, Brazil, between December 2021 and July 2022. The study received ethics committee approval by PRÓ-CARDÍACO Hospital on 17 December 2021 (CAAE: 54184421.3.0000.5533). The study complied with Good Clinical Practices and the principles of the Declaration of Helsinki. All subjects and their caregivers, if aged less than 18 years, provided written informed consent prior to participation and consented to the use of their photographs for publication purposes. The study is currently registered under the identifier number NCT05783453 in the Clinical trial PRS database.
Subjects above 3 years of age and of any phototype were eligible for participation in this investigation if they presented with mild and stable AD for at least 3 months AD was to be diagnosed at least 6 months before inclusion. The SCORAD score was to be above 25 points and patients had received stable AD treatment.26
The overall study duration was 168 days, subjects were asked to attend the study site at baseline, D14, D28, D84 and D168.
Subjects were asked to apply Emollient+ on lesional and non-lesional areas of the face and body twice daily and to stop their current AD treatment for the entire course of the study.
At baseline, the investigator assessed AD severity according to the SCORAD tool, the severity of clinical signs (erythema, excoriation, lichenification, lesional/non-lesional zone dryness and body skin dryness) on a scale from 0 = none to 3 = severe, and occurrence and intensity of flares during the 6 and 3 month periods preceding inclusion on a scale from 0 = none to 4 = very severe, and asked the subjects to self-evaluate the severity of their AD symptoms (itching, tingling, burning) on a visual analog scale from 0 = none to 3 = very severe. The skin hydration status was assessed using a Corneometer (Courage + Khazaka electronic GmbH, Cologne, Germany) on defined lesional and non-lesional areas. Subjects aged above 16 years were asked to complete a DLQI questionnaire, subjects aged between 3 and 15 years or their caregivers completed a CDLQI questionnaire.27,28 Tolerance was evaluated through clinical dermatological evaluation and spontaneously subject-reported events through the studies. Subjects or their care-giver(s) were asked to evaluate the cosmeticity, perceived efficacy and acceptability using a specifically developed questionnaire on a 5-point scale (I totally agree, I partially agree, neither agree or disagree, I partially disagree and I totally disagree) 14, 28, 84 and 168 days after the product application; the questionnaire is available upon request from the corresponding author.
Signs and symptoms, QoL, instrumental parameters as well as local tolerance and subject satisfaction with Emollient+ were assessed at all post-baseline visits. AD flares were assessed at D84 and/or D168.
Quantitative variables were summarized using the minimum, maximum and measures of central tendency such as the mean and median, as well as measures of dispersion such as the standard deviation (SD). Qualitative variables were summarized in the form of counts and percentages. The mean percentage change of each parameter at each post-baseline timepoint (where applicable) was calculated compared to baseline. The evolution over time was calculated for each parameter using either the Student’s Paired t-test or the Wilcoxon Signed Rank Test depending on the normality of the difference data. The latter was tested using a Shapiro Wilk test at 1% level of significance. A 0.5% significance level was set. Microsoft Excel 2010 or above and IBM SPSS version 19.0 were used for the statistical analysis.
Results
Demographic and Baseline Data
Global Population
Overall, 56 subjects were included in this study. The mean age was 25.0±20.0 years (45% were children); 69.6% were females, and the remaining 30.4% were males. The subjects had phototype II–VI, of which the majority had phototype IV (58.9%). Of the subjects who reported flares within the last 6 months before baseline (n = 35), 61.8% had mild and 35.3% moderate flare intensity, the mean quantity was 3.1. Flare intensity within the 3 months prior to baseline (n = 27) was mild in 73.1%, and moderate in 26.9% of subjects. The mean quantity of flares had decreased to 1.8.
Adult Population
The adult population (n = 31) was aged 40.0±13.0 years on average; 83.9% were female and 16.1% male subjects. Phototype IV (61.3%) was the main phototype observed, followed by phototype V (16.1%). A total of 52.6% of subjects with flares (n = 19) had mild and 42.1% moderate flares over the 6 months prior to inclusion, with, on average, 2.3 flares observed. Within the 3 months prior to inclusion, 78.6% of subjects with flares (n = 14) reported mild and 21.4% moderate flares; the average number of flares was 1.4.
Paediatric Population
In the paediatric population (n = 25), the mean age was 7.0±3.0 years. Female subjects represented 52.0% of this population, the remaining were male subjects (48.0%). Fifty-six percent (56.0%) reported phototype IV and 16.1% phototype V. Six months before inclusion, 73.3% of the paediatric population with flares (n = 16) reported mild and 26.7% moderate flares; the average number of flares was n = 4.1. Three months prior to inclusion, 66.7% of subjects with flares (n = 13) reported mild and 33.3% moderate flares. Overall, 2.3 flares were reported for this period.
Detailed demographic and disease data at baseline are given in Table 1.
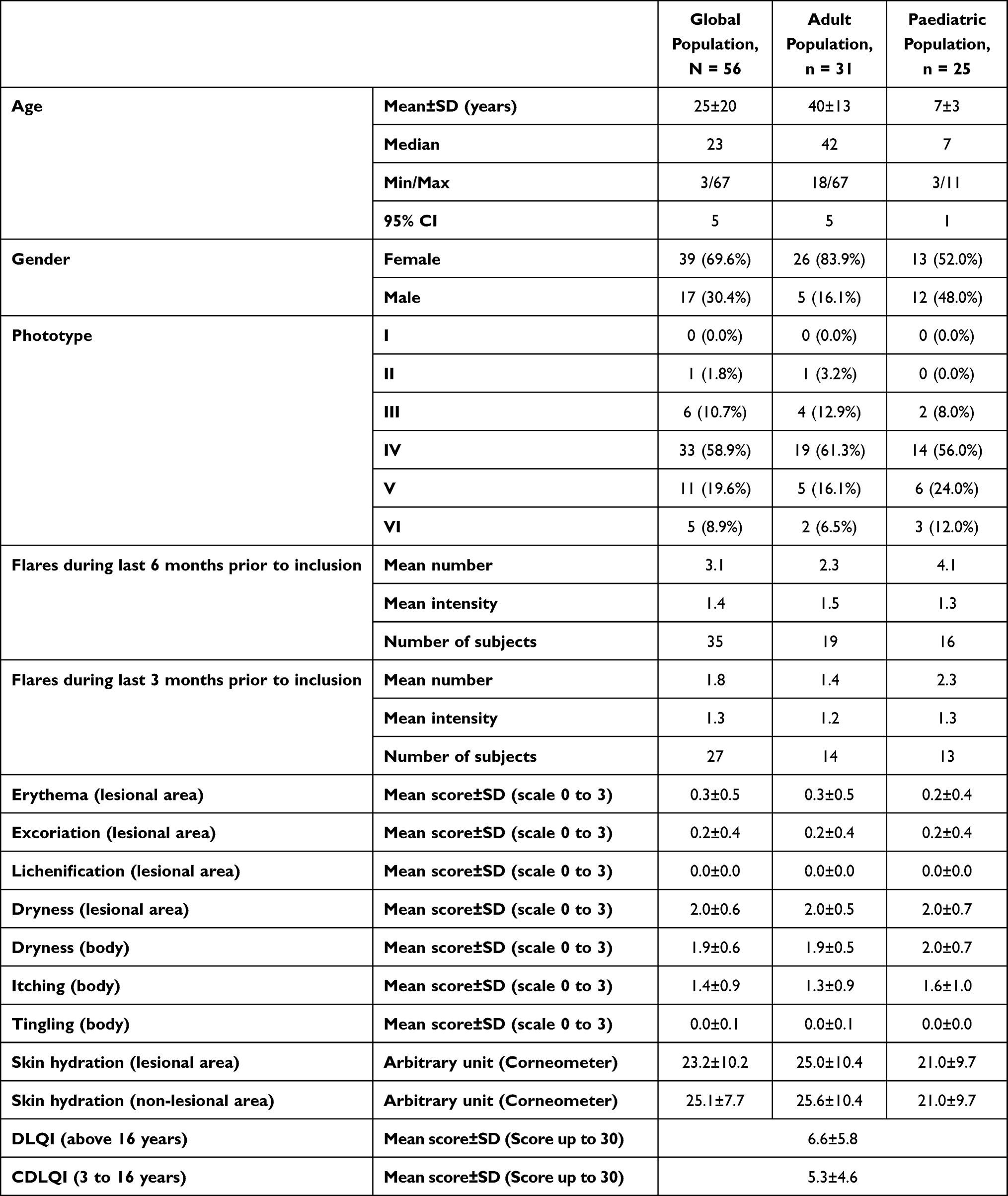 |
Table 1 Demographic and Baseline Disease Data |
SCORAD
AD flare reduction was assessed during the first 28 days. On D14 and D28 there was a significant improvement in area, intensity and symptoms when compared to baseline. The improvement was, respectively, 35.3% and 40.4%. On D14, 66.7% of subjects showed an improvement ≥4 units from baseline and on D28 an improvement of 67.9%.
The maintenance phase was assessed from D28 to D168. On D168 there was a significant (p = 0.014) improvement of 17.5% when compared to D28On D168, 32.1% of subjects showed an improvement ≥4 units from D28.
Figure 1 details the evolution of SCORAD over time for the different populations.
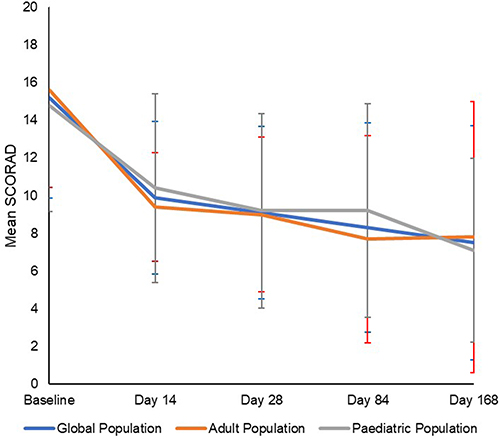 |
Figure 1 SCORAD evolution over time in the global, adult and paediatric population. The SCORAD had significantly (p < 0.001) improved in all populations as early as D14 lasting until the end of the study. |
Flares
In the global and paediatric populations, the number of flares reported during the 6 and 3 months had decreased at D84/D168 and slightly increased in the adult population. In all groups, the intensity of flares had decreased, with a majority of subjects reporting mild flares. Details are provided in Table 2.
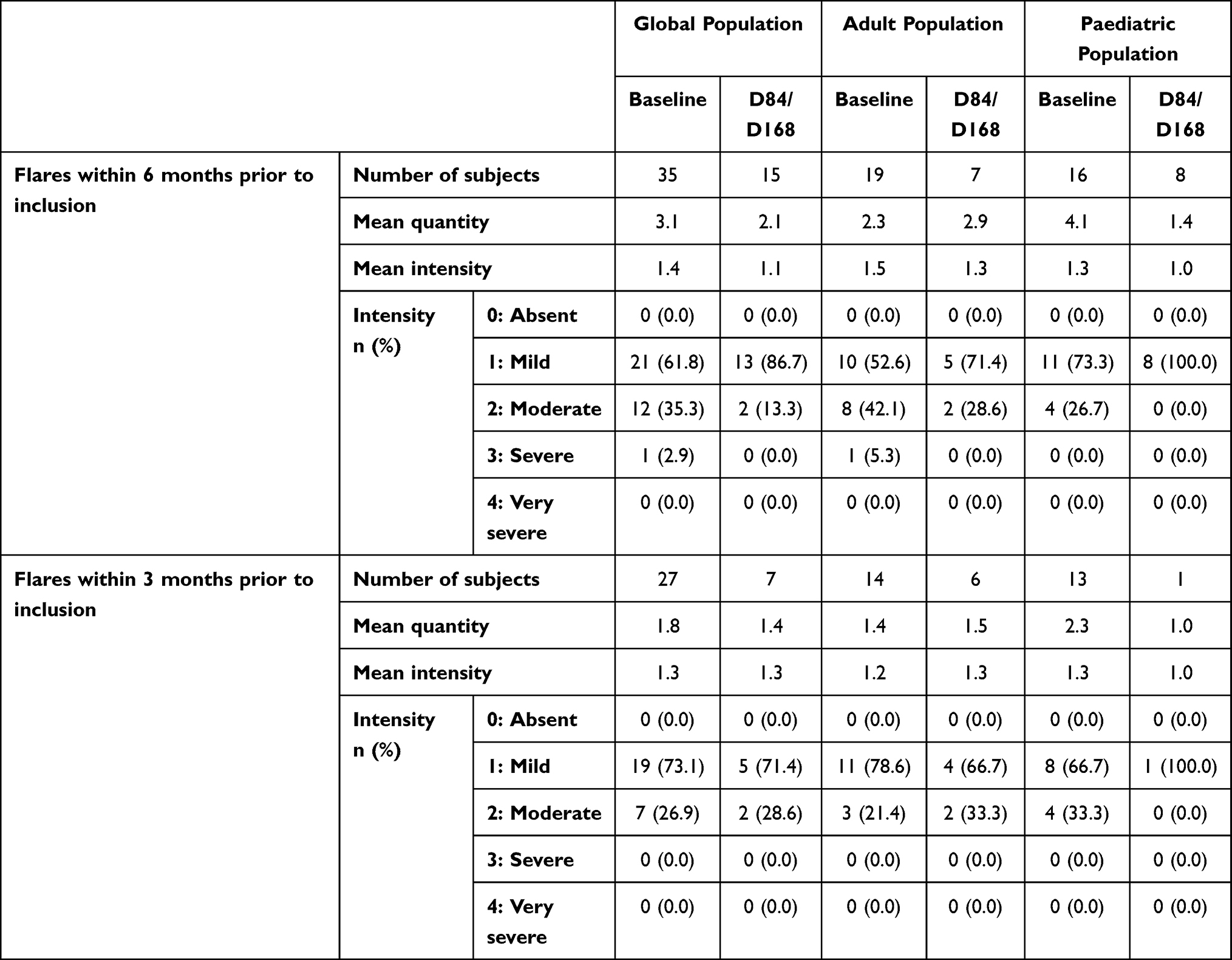 |
Table 2 Evolution Over Time of Flares |
Clinical Signs and Symptoms
After 168 days of continued use of Emollient+, erythema had significantly (all p ≤ 0.025) decreased in all groups from baseline. The decrease was statistically significant (all p ≤ 0.002) in the global and adult population at D14, 28, 84, and 168.
According to the investigator, skin dryness on lesional and non-lesional areas had significantly (p < 0.001) improved with Emollient+ in all populations and at all post-baseline visits. This significant (p < 0.001) improvement was also observed for body skin dryness.
Figure 2 shows the evolution over time for erythema and body skin dryness.
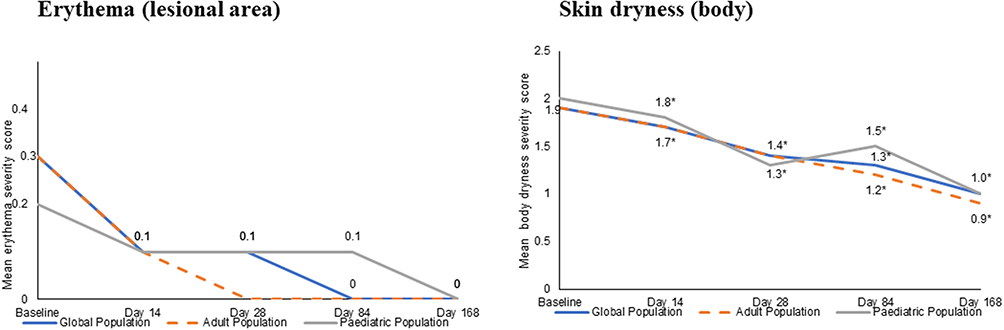 |
Figure 2 Evolution over time of clinical signs in the global, adult and paediatric population. Clinical signs had significantly (p < 0.008) improved in the global and adult population at all post-baseline visits and in the paediatric population at D168 (p = 0.025). Skin dryness had significantly (p < 0.001) improved from baseline as early as D14, sustaining until D168. |
Excoriation had significantly (all p ≤ 0.021) improved in the global population after 14, 28 and 168 days. In the adult population, a significant (all p ≤ 0.034) improvement was observed at D14, 28 and 84, while in the paediatric population, a significant (p = 0.025) improvement was observed at D24 only.
No change of the lichenification, oedema, oozing or desquamation status compared to baseline was observed in any of the populations or at any visit.
Subject-reported itching had significantly (all p ≤ 0.009, Figure 3) decreased in all groups and at all post-baseline visits. No change from baseline was observed for tingling or burning.
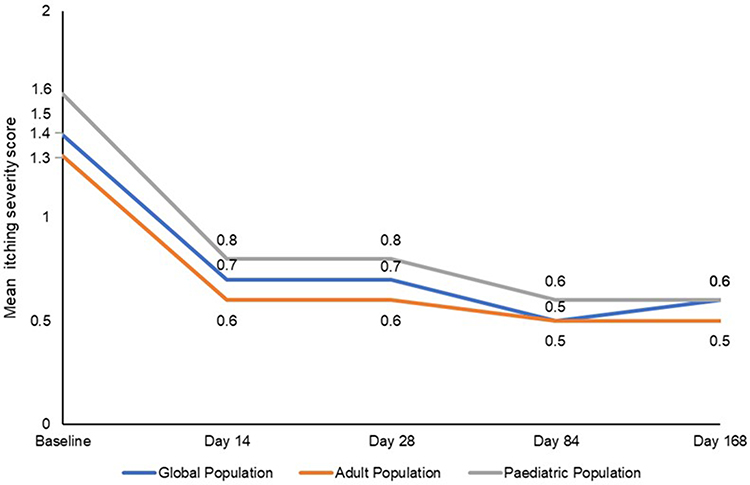 |
Figure 3 Evolution over time of subject-reported itch in the global, adult and paediatric population. For itch, differences from baseline were statistically significant (all p ≤ 0.009) in all 3 populations at all post-baseline visits. |
Instrumental Evaluations of Skin Hydration
The instrumental assessment of skin hydration showed that Emollient+ significantly improves skin hydration in lesional areas as early as D14 in the global (p = 0.004) and adult population (p = 0.003) but not in the paediatric population (p = 0.323). The statistical significance of improvement compared to baseline was always more important after 28 days of use (all p < 0.001) in all 3 populations. Details are given in Figure 4. In non-lesional areas, skin hydration had significantly (p < 0.001) improved in all three populations, starting from D14 and lasting until D168.
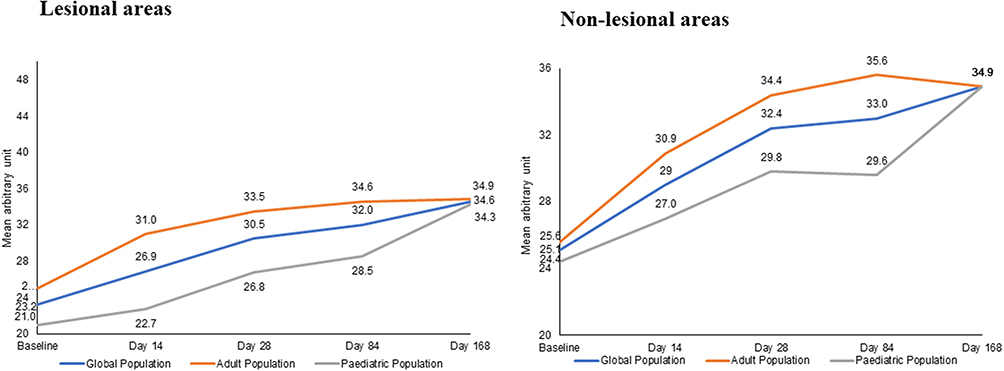 |
Figure 4 Evolution over time of skin hydration assessed with a Corneometer in the global, adult and paediatric population. Skin hydration had significantly (p < 0.001) improved in lesional areas as early as D14 in the global and adult population and in the paediatric population after 28 days sustaining until D168. In non-lesional areas of all populations, skin hydration had significantly (p < 0.001) improved as early as D14. |
Quality of Life
The daily use of Emollient+ significantly (p < 0.001) improved the subjects’ QoL over time. The DLQI baseline score decreased by 77.7% at D14, by 87.4% at D28, by 89.3% at D84 and by 89.8% at D168. The CDLQI baseline score decreased by 48.1% at D14, 51.9% at D28, by 67.5% at D84 and by 84.2% at D168.
See Figure 5 for a detailed over-time evolution of QoL parameters.
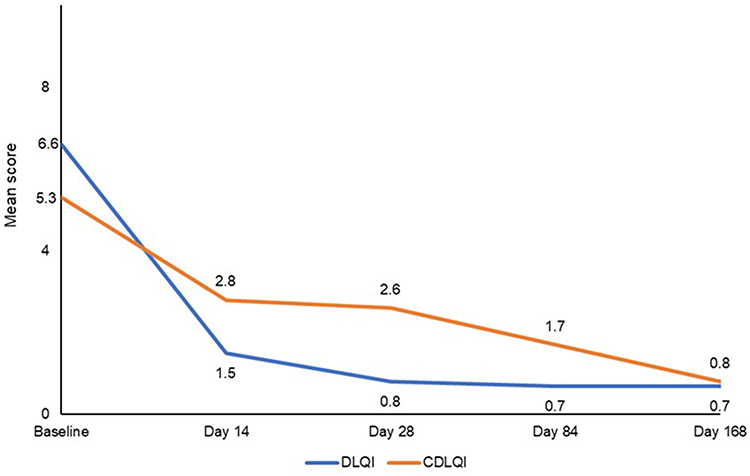 |
Figure 5 Evolution over time of quality of life (DLQI and CDLQI). Quality of life had significantly (p < 0.001) improved from baseline in the adult and paediatric population as early as D14. |
Subject Satisfaction
The cosmetic qualities of Emollient+ were highly appreciated by more than 80.0% of all subjects at all time points.
Local Tolerance
Emollient+ was very well tolerated with no product-related tolerance issues at any of moment of the study.
Discussion
Results from the present study which was conducted between the end of summer and winter seasons, a period known for triggering AD flares, show that the continued use of Emollient+ significantly (all p < 0.05) reduces clinical signs and symptoms, except erythema in the paediatric population and increases skin hydration in subjects with mild AD after 28 days.29 In a recently, yet not published study, Emollient+ was able to significantly reduce pruritus compared to the usual emollients in moderate to severe AD patients under systemic therapy.19 In parallel to the reduction of clinical signs and symptoms, the subjects’ QoL had significantly improved (p < 0.001) after 14 days of daily use of the supplemented emollient and remained improved during the entire duration of the study. This difference was clinically significant after 28 days in adults and after 168 days in children with DLQI scores being below 1.0. Moreover, the number and intensity of flares had globally decreased, even though a slight, but clinically irrelevant, increase in their number was observed in adults. Applying Emollient+ improved clinical signs and symptoms in subjects with atopic or seborrheic dermatitis.30–34
During AD flares, the loss of bacterial diversity and the predominance of Staphylococcus (S.) species, especially S. epidermidis and S. aureus, correlates with the severity of AD.35–37 Microresyl was added to limit the formation of the S. aureus biofilm, while Aqua posae filiformis helps to restore the healthy skin microbiota.18,38 Thus, Emollient+ may help to reduce dysbiosis and restore the natural skin barrier which was indirectly shown by the significantly (p < 0.001) improved skin hydration, as early as D14.
In conclusion, the present study confirms the clinical benefit of Emollient+ in managing mild AD and maintaining the results obtained after 28 days of improving AD signs and symptoms for up to 168 days, as well as skin hydration and the QoL of subjects. Emollient+ was highly appreciated and very well tolerated.
Data Sharing Statement
Priscila Correia, the corresponding author, will share the study protocol and all data collected and statistically analysed in relationship with this study, except identified participant data, upon reasonable request for one year after publication of this manuscript.
Ethical Statement
The study received ethics committee approval by PRÓ-CARDÍACO Hospital on 17 December 2021 (CAAE: 54184421.3.0000.5533). All subjects and their caregivers, if applicable, provided written informed consent prior to participation and consented to the use of their photographs for publication purposes.
Acknowledgments
The authors acknowledge Daniele Miranda and Camila Valpacos from Centre International de Dévéloppement Pharmaceutique (CIDP), Brazil, for the study conduct, Guenaëlle Le Dantec and Caroline Le Floc’h, La Roche-Posay Laboratoire Dermatologique, France, for the scientific input and Karl Patrick Göritz, SMWS, France, for the writing support.
Funding
This study was financed by L’Oréal Brazil.
Disclosure
PC and DK are employees of L’Oréal Group. SC is a consultant to L’Oréal Brazil. The authors report no other conflicts of interest in this work.
References
1. Kim J, Kim BE, Leung DYM. Pathophysiology of atopic dermatitis: clinical implications. All Astm Proc. 2019;40(2):84–92.
2. Bieber T. Atopic dermatitis: an expanding therapeutic pipeline for a complex disease. Nature Rev Drug Disc. 2022;21(1):21–40.
3. Alenius H, Sinkko H, Moitinho-Silva L, et al. The power and potential of BIOMAP to elucidate host-microbiome interplay in skin inflammatory diseases. Exp Dermatol. 2021;30(10):1517–1531. doi:10.1111/exd.14446
4. Marini A, Aue N, Demessant AL, Salah S, Kerob D, Luger TA. Increased skin pH and transepidermal water loss may serve as predictor for atopic dermatitis flares. J Eur Acad Dermatol Venereol. 2023;37(2):e252–e4. doi:10.1111/jdv.18558
5. Edslev SM, Agner T, Andersen PS. Skin microbiome in atopic dermatitis. Acta Derm Venereol. 2020;100(12):adv00164. doi:10.2340/00015555-3514
6. Koh LF, Ong RY, Common JE. Skin microbiome of atopic dermatitis. Allergol Int. 2022;71(1):31–39. doi:10.1016/j.alit.2021.11.001
7. Baldwin HE, Bhatia ND, Friedman A, Eng RM, Seite S. The role of cutaneous microbiota harmony in maintaining a functional skin barrier. J Drugs Dermatol. 2017;16(1):12–18.
8. Avena-Woods C. Overview of atopic dermatitis. Am J Manag Care. 2017;23(8 Suppl):S115–s23.
9. Maliyar K, Sibbald C, Pope E, Gary Sibbald R. Diagnosis and management of atopic dermatitis: a review. Adv Skin Wound Care. 2018;31(12):538–550. doi:10.1097/01.ASW.0000547414.38888.8d
10. Ring J, Alomar A, Bieber T, et al. Guidelines for treatment of atopic eczema (atopic dermatitis) Part II. J Eur Acad Dermatol Venereol. 2012;26(9):1176–1193. doi:10.1111/j.1468-3083.2012.04636.x
11. Wollenberg A, Christen-Zäch S, Taieb A, et al. ETFAD/EADV Eczema task force 2020 position paper on diagnosis and treatment of atopic dermatitis in adults and children. J Eur Acad Dermatol Venereol. 2020;34(12):2717–2744. doi:10.1111/jdv.16892
12. Katoh N, Ohya Y, Ikeda M, et al. Clinical practice guidelines for the management of atopic dermatitis 2018. J Dermatol. 2019;46(12):1053–1101. doi:10.1111/1346-8138.15090
13. Wollenberg A, Barbarot S, Bieber T, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part I. J Eur Acad Dermatol Venereol. 2018;32(5):657–682. doi:10.1111/jdv.14891
14. Maintz L, Bieber T, Simpson HD, Demessant-Flavigny AL. From skin barrier dysfunction to systemic impact of atopic dermatitis: implications for a precision approach in dermocosmetics and medicine. J Pers Med. 2022;12(6):893. doi:10.3390/jpm12060893
15. Elias PM. Optimizing emollient therapy for skin barrier repair in atopic dermatitis. Ann Allergy Asthma Immunol. 2022;128(5):505–511. doi:10.1016/j.anai.2022.01.012
16. Zhong Y, Samuel M, van Bever H, Tham EH. Emollients in infancy to prevent atopic dermatitis: a systematic review and meta-analysis. Allergy. 2022;77(6):1685–1699. doi:10.1111/all.15116
17. Zelenkova H, Kerob D, Salah S, Demessant-Flavigny A-L. Impact of daily use of emollient ‘plus’ on corticosteroid consumption in patients with atopic dermatitis: an open, randomized controlled study. Eur Acad Dermatol Venereol. 2023;37(Suppl 5):27–34. doi:10.1111/jdv.18947
18. Seité S, Zelenkova H, Martin R. Clinical efficacy of emollients in atopic dermatitis patients - relationship with the skin microbiota modification. Clin Cosmet Investig Dermatol. 2017;10:25–33. doi:10.2147/CCID.S121910
19. Magnolo N, Jaenicke T, Tsianakas A, et al. Comparison of different skin care regimens in patients with moderate to severe atopic dermatitis receiving systemic treatment: a randomized controlled trial. Eur Acad Dermatol Venereol. 2023;37(Suppl 5):18–26. doi:10.1111/jdv.18949
20. Silverberg JI, Gelfand JM, Margolis DJ, et al. Patient burden and quality of life in atopic dermatitis in US adults: a population-based cross-sectional study. Ann All Astm Immunol. 2018;121(3):340–347.
21. Xu X, van Galen LS, Koh MJA, et al. Factors influencing quality of life in children with atopic dermatitis and their caregivers: a cross-sectional study. Sci Rep. 2019;9(1):15990. doi:10.1038/s41598-019-51129-5
22. Drucker AM, Wang AR, Li WQ, Sevetson E, Block JK, Qureshi AA. The burden of atopic dermatitis: summary of a report for the National Eczema Association. J Invest Dermatol. 2017;137(1):26–30. doi:10.1016/j.jid.2016.07.012
23. Ali F, Vyas J, Finlay AY. Counting the burden: atopic dermatitis and health-related quality of life. Acta Derm Venereol. 2020;100(12):adv00161. doi:10.2340/00015555-3511
24. Cabout E, Eymere S, Launois R, et al. Cost-effectiveness of emollients in the prevention of relapse among French patients with atopic dermatitis. Acta Derm Venereol. 2021;101(7):adv00509. doi:10.2340/00015555-3873
25. Cabout E, Eymere S, Launois R, Aslanian F, Taïeb C, Seité S. Cost effectiveness of emollients in the prevention of relapses in atopic dermatitis. Clin Cosm Inv Dermatol. 2020;13:987–996. doi:10.2147/CCID.S279233
26. Severity scoring of atopic dermatitis: the SCORAD index. consensus report of the European task force on atopic dermatitis. Dermatology. 1993;186(1):23–31. doi:10.1159/000247298
27. Lewis-Jones MS, Finlay AY. The Children’s Dermatology Life Quality Index (CDLQI): initial validation and practical use. Br J Dermatol. 1995;132(6):942–949. doi:10.1111/j.1365-2133.1995.tb16953.x
28. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)--a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210–216. doi:10.1111/j.1365-2230.1994.tb01167.x
29. Hamann CR, Andersen YMF, Engebretsen KA, et al. The effects of season and weather on healthcare utilization among patients with atopic dermatitis. J Eur Acad Dermatol Venereol. 2018;32(10):1745–1753. doi:10.1111/jdv.15023
30. Gueniche A, Knaudt B, Schuck E, et al. Effects of nonpathogenic gram-negative bacterium Vitreoscilla filiformis lysate on atopic dermatitis: a prospective, randomized, double-blind, placebo-controlled clinical study. Br J Dermatol. 2008;159(6):1357–1363. doi:10.1111/j.1365-2133.2008.08836.x
31. Volz T, Skabytska Y, Guenova E, et al. Nonpathogenic bacteria alleviating atopic dermatitis inflammation induce IL-10-producing dendritic cells and regulatory Tr1 cells. J Invest Dermatol. 2014;134(1):96–104. doi:10.1038/jid.2013.291
32. Gueniche A, Cathelineau AC, Bastien P, et al. Vitreoscilla filiformis biomass improves seborrheic dermatitis. J Eur Acad Dermatol Venereol. 2008;22(8):1014–1015. doi:10.1111/j.1468-3083.2007.02508.x
33. Del Rosso JQ, Kircik LH, Zeichner J, Stein Gold L. The clinical relevance and therapeutic benefit of established active ingredients incorporated into advanced foam vehicles: vehicle characteristics can influence and improve patient outcomes. J Drugs Dermatol. 2019;18(2s):s100–s7.
34. Zeichner J, Seite S. From probiotic to prebiotic using thermal spring water. J Drugs Dermatol. 2018;17(6):657–662.
35. Grice EA, Kong HH, Conlan S, et al. Topographical and temporal diversity of the human skin microbiome. Science. 2009;324(5931):1190–1192. doi:10.1126/science.1171700
36. Findley K, Grice EA. The skin microbiome: a focus on pathogens and their association with skin disease. PLoS Pathog. 2014;10(10):e1004436. doi:10.1371/journal.ppat.1004436
37. Kong HH, Oh J, Deming C, et al. Temporal shifts in the skin microbiome associated with disease flares and treatment in children with atopic dermatitis. Genome Res. 2012;22(5):850–859. doi:10.1101/gr.131029.111
38. Al-Ghazzewi FH, Tester RF. Impact of prebiotics and probiotics on skin health. Benef Microbes. 2014;5(2):99–107. doi:10.3920/BM2013.0040
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.