Back to Journals » Therapeutics and Clinical Risk Management » Volume 19
Emerging Treatment Options for Myelofibrosis: Focus on Anemia
Authors Sastow D, Tremblay D ![]()
Received 8 May 2023
Accepted for publication 25 June 2023
Published 28 June 2023 Volume 2023:19 Pages 535—547
DOI https://doi.org/10.2147/TCRM.S386802
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Dahniel Sastow,1 Douglas Tremblay2
1Department of Internal Medicine, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 2Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, NY, USA
Correspondence: Douglas Tremblay, Tisch Cancer Institute, Division of Hematology/Oncology, Icahn School of Medicine at Mount Sinai, 1 Gustave L Levy Place, Box 1079, New York, NY, 10029, USA, Email [email protected]
Abstract: Myelofibrosis (MF) is a hematologic malignancy characterized by abnormal proliferation of myeloid cells and the release of pro-inflammatory cytokines, leading to progressive bone marrow dysfunction. The introduction of ruxolitinib just over a decade ago marked a significant advancement in MF therapy, with JAK inhibitors now being the first-line treatment for reducing spleen size and managing symptoms. However, early JAK inhibitors (ruxolitinib and fedratinib) are often associated with cytopenias, particularly thrombocytopenia and anemia, which limit their tolerability. To address these complications, pacritinib has been developed and recently approved for patients with thrombocytopenia, while momelotinib is in development for those with anemia. Although JAK inhibitors have significantly improved the quality of life of MF patients, they have not demonstrated the ability to reduce leukemic transformation and their impact on survival is debated. Numerous drugs are currently being developed and investigated in clinical trials, both as standalone therapy and in combination with JAK inhibitors, with promising results enhancing the benefits of JAK inhibitors. In the near future, MF treatment strategies will involve selecting the most suitable JAK inhibitor based on individual patient characteristics and prior therapy. Ongoing and future clinical trials are crucial for advancing the field and expanding therapeutic options for MF patients.
Keywords: myelofibrosis, emerging therapy, momelotinib, anemia, JAK inhibitors
Introduction
Myelofibrosis (MF) is a hematologic malignancy characterized by the pathologic proliferation of myeloid cells and the release of pro-inflammatory cytokines, resulting in progressive functional decline of the bone marrow (BM).1 MF can manifest as a primary disorder, known as primary myelofibrosis (PMF), or arise from an antecedent myeloproliferative neoplasm (MPN) such as essential thrombocythemia (ET) or polycythemia vera (PV).2 Common symptoms associated with MF include splenomegaly, constitutional symptoms (fever, night sweats, weight loss), and progressive cytopenias, which increase the risk of infections, bleeding, and the need for transfusions.3
Anemia is common in newly diagnosed MF patients, with 38% of patients having a hemoglobin less than 10g/dL at diagnosis3 and becomes even more prevalent as the disease progresses. Anemia has been shown to both be a negative prognostic indicator4 and results in a decreased quality of life.5 The etiology of anemia is multifactorial, but fibrosis of normal hematopoietic tissue is a significant contributing factor, with a study of 490 bone marrow biopsy samples showing an association between higher grades of reticulin fibrosis and severe anemia.6 Other potential contributors to anemia in MF include ineffective erythropoiesis due to extramedullary hematopoiesis,7 splenic sequestration of red blood cells, and the upregulation of hepcidin due to the pro-inflammatory environment in MF patients.8 Furthermore, given the widespread use of Janus Kinase (JAK) inhibitors, there is a growing degree of treatment-related anemia in MF patients.
Current front-line treatments for MF aim to alleviate symptoms by inhibiting the Janus kinase/signal transducer and activator of transcription proteins (JAK/STAT) pathway, which is uniformly upregulated in MF patients.9 To date, the FDA has approved three JAK inhibitors, ruxolitinib, fedratinib, and pacritinib, for the treatment of MF. Despite the significant activity of JAK inhibitors to reduce spleen size and alleviating constitutional symptoms, cytopenias continue to pose a significant challenge in the initiation and maintenance of these medications. Phase 3 trials of ruxolitinib and fedratinib revealed that over 40% of patients experienced grade 3/4 anemia.10,11 Additionally, even with strict platelet cutoffs to entry criteria of >100 x 109/L (COMFORT-1) and >50 x 109/L (JAKARTA), the treatment arms still reported a >10% incidence of grade 3/4 thrombocytopenia.10,11 Consequently, two newer JAK inhibitors, namely momelotinib and pacritinib, have been developed with activity in patients with baseline anemia12,13 and thrombocytopenia.14,15
In this review, we begin by providing a comprehensive overview of the major clinical trials of the first three JAK inhibitors to receive FDA approval, with an emphasis on their impact on anemia. We then delve into the details of momelotinib, focusing on the results of the MOMENTUM trial and the effects of momelotinib on patients with anemia. Additionally, we discuss overall survival (OS) data for JAK inhibitors and its shortcomings in disease modification. Finally, we spotlight some of the most promising non-JAK inhibitors currently under investigation with the potential to improve response rates and alter the progression of disease. We conclude by discussing the current and future landscape of MF treatment.
JAK Inhibitors
Ruxolitinib
Ruxolitinib, a JAK1/JAK2 inhibitor, was the first JAK inhibitor approved for the treatment of MF, based on two landmark phase 3 clinical trials: COMFORT-I and COMFORT-II. In COMFORT-I, 309 patients with intermediate-2 or high-risk MF were randomly assigned to ruxolitinib or placebo (Table 1). The primary endpoint was a reduction of spleen volume by at least 35% (SVR35%). At 24 weeks, 42% of patients in the treatment arm achieved SVR35%, compared to 0.7% in the placebo arm (p < 0.001). Moreover, two-thirds of the patients who initially responded to the medication maintained their response for a minimum of 48 weeks.10
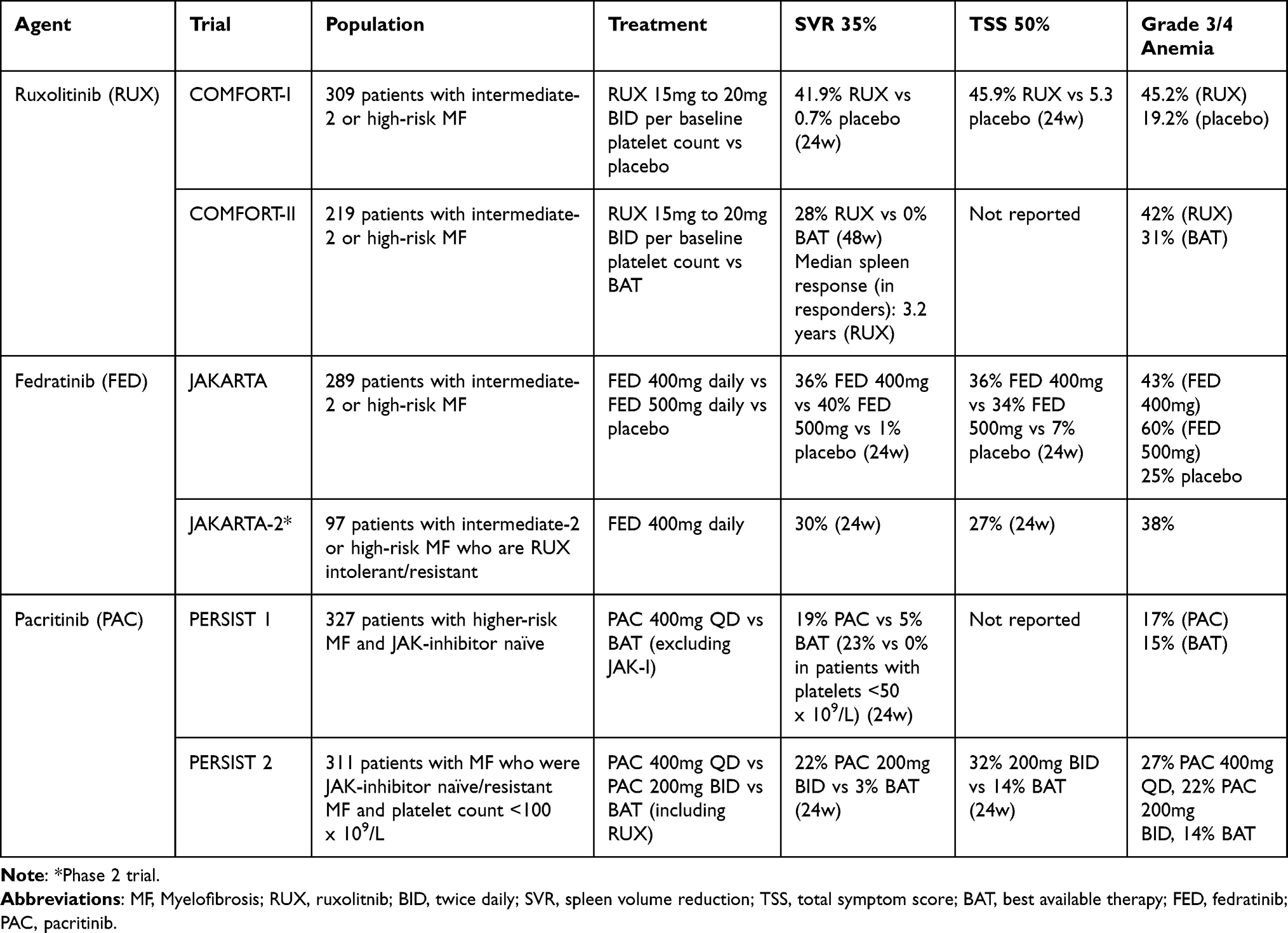 |
Table 1 Major Trials of Approved JAK Inhibitors |
COMFORT-II, in contrast, compared ruxolitinib to best available therapy (BAT), as opposed to placebo in COMOFORT-I. At 48 weeks, SVR35% was achieved in 28% of patients in the ruxolitinib group compared to 0% in the BAT group.16 Reduction in symptom score, a key secondary endpoint, was also significant in both COMFORT-I and COMFORT-II in the ruxolitinib arm compared to the control arms.10,16
In both trials, the most common toxicity was anemia, with grade 3/4 anemia occurring in the treatment arms at 45.2% and 42% in COMFORT-I and COMFORT-II, respectively.10,16 Notably, in COMFORT-I, about half of these events occurred during the first 8 weeks of therapy and peaked at 8 to 12 weeks before returning to similar levels of those in the placebo arm and to about 0.5g/dL below their starting hemoglobin level.10 Both studies allowed for transfusions to support patients who developed significant anemia.
Given the negative prognostic impact of baseline anemia in MF, investigators sought to understand if ruxolitinib-induced anemia carries the same negative prognostic implications. In their pooled analysis of COMFORT-I and COMFORT-II patients, the study confirmed that baseline anemia (before treatment with JAK inhibitor) was associated with shortened OS, but new or worsening anemia during the treatment period had no effect on OS.17 Treatment-related anemia with ruxolitinib therefore does not appear to carry a negative prognostic impact.
The REALISE Phase 2 study evaluated a novel dosing strategy of 10mg twice daily in MF patients with a baseline hemoglobin <10g/dl (18% transfusion dependent), with uptitration after 12 weeks to a maximum of 25mg twice daily. Overall, 70% of patients reach SVR50%. Importantly, this dosing regimen resulted in stable median hemoglobin levels and transfusion requirements as compared to baseline.18
The median duration of response on the COMFORT I and II trials was approximately 3 years,19,20 suggesting the need for further therapy even in patients who tolerate and improve with ruxolitinib initially. Ruxolitinib remains the front-line treatment for MF patients with a platelet count of >50 x 109/L, however treatment-related anemia remains a concern, especially in patients who are severely anemic but not yet transfusion dependent.
Febratinib
Fedratinib, a JAK2/FLT3 inhibitor, was the second JAK2 inhibitor approved by the FDA for intermediate-2 or high-risk MF in patients ruxolitinib naïve or resistant, based on the JAKARTA and JAKARTA-2 trials (Table 1).21 In the phase 3 JAKARTA trial, 289 adults were randomly assigned to once daily oral fedratinib at either 400 or 500mg daily, or placebo with a primary endpoint of SVR35% at 24 weeks, which was reached in 36% and 40% of patients receiving 400mg and 500mg of fedratinib, respectively, compared to 1% in the placebo group. The secondary endpoint of reduction of symptom response was also achieved. However, 43% and 58% of patients in the 400mg and 500mg groups, respectively, developed grade 3/4 anemia compared to 25% in the placebo arm.11
JAKARTA2 was a phase 2 trial that enrolled patients who were resistant or intolerant to ruxolitinib after at least 14 days of treatment. This single-arm, open label trial evaluated the efficacy of 400mg daily of fedratinib, with a primary outcome of SVR35%. Of the 97 patients enrolled, 55% reached SVR35%, although 38% reported grades 3/4 anemia.22 In an updated analysis of the JAKARTA2 population, the intention-to-treat analysis showed an SVR35% rate of 31% and a subgroup of patients who met more stringent definitions of prior ruxolitnib failure had a SVR35% of 30%.23
The JAKARTA2 trial was terminated early due to the concerns about Wernicke encephalopathy (WE) in the earlier JAKARTA trial. However, further review indicated that these patients either did not have WE or had other conditions predisposing them to encephalopathy.24 Consequently, the phase 3b FREEDOM trial investigated fedratinib in patients with more than 3 months of previous ruxolitnib treatment. The study employed proactive strategies to mitigate both thiamine level decreases and gastrointestinal toxicity. The trial enrolled 38 patients who were treated with 400mg of fedratinib, and it was capped early due to accrual challenges during the COVID-19 pandemic. The primary analysis revealed that 26% of patients achieved SVR35% by the end of cycle 6. Notably, no patients required discontinuation due to low thiamine levels, and there were no cases of WE reported.25 Currently, the phase 3 FREEDOM2 trial is ongoing, which compares fedratinib against BAT for ruxolitinib resistant or intolerant patients (NCT03952039). Fedratinib remains an option for symptom and spleen management in MF patients, especially after ruxolitinib failure/intolerance, although similar concerns related to cytopenias exist as with ruxolitinib.
Pacritinib
Pacritinib, a JAK2/IRAK1 inhibitor, is the most recent JAK inhibitor to be approved and holds a distinct advantage in that it can be given in patients with a platelet count as low as <50 x 109/L. The efficacy of pacritinib in reducing spleen size and improving symptoms in patients with MF has been demonstrated in several trials, including PERSIST-1, which enrolled JAK inhibitor naïve patients to pacritinib or placebo, and PERSIST-2 (Table 1). Focusing on PERSIST-2, 311 patients with MF and baseline platelet counts of <100 x 109/L were randomized to receive pacritinib 200mg twice daily, 400mg once daily, or BAT, which could have included ruxolitinib. The combined pacritinib arms showed a significantly higher SVR35% compared to the BAT arm (18% vs 3%, p < 0.001). Total symptom score improvement by greater than 50% (TSS50%) was higher in the pacritinib arms than in the BAT arm (25% vs 14%), although the difference was not statistically significant (p = 0.08). However, the pacritinib 200mg twice daily arm did reach statistical significance for both co-primary endpoints compared with BAT. Improvements in hemoglobin and reductions in transfusion burden were observed, most notable in the pacritinib 200mg twice daily arm.26 A retrospective analysis of the 189 patients in both PERSIST trials with severe thrombocytopenia (platelet counts <50k x 109/L) showed that the improvements in SVR35% and TSS50% were preserved in this sub-population, without any excess major adverse events.14 Pacritinib is being further evaluated in the phase 3 PACIFICA of pacritinib 200mg twice daily versus physician’s choice in patients with MF and severe thrombocytopenia.27
The significant degree of treatment-related anemia by ruxolitinib and fedratinib has generated interest in the ability of pacritinib to maintain or even improve hemoglobin levels. One hypothesized mechanism is the enhanced erythropoiesis via interleukin 1 receptor associated kinase 1 (IRAK1) inhibition by pacritinib. IRAK1 is a serine/threonine kinase that ultimately results in the activation of NFkB, a transcription factor that regulates interleukin-6 (IL-6). IL-6 is the main cytokine implicated in stimulating hepcidin production. IRAK1 downregulates this pathway and should lead to a decrease in hepcidin production.28 Another explanation is the inhibition by pacritinib of activin A receptor type 1 (ACVR1), which is also known to mediate hepcidin production. A recent analysis of a subgroup of patients in the PERSIST-2 trial, who were transfusion dependent at baseline, found a significant increase in transfusion independence in the pacritinib arm compared to BAT (24% vs 5%, p = 0.013). This effect size was maintained even among patients who had not received ruxolitinib within 30 days prior to pacritinib initiation, suggesting a pacritinib treatment effect rather than a rebound effect after ruxolitinib discontinuation. The study was also able to measure the degree of ACVR1 inhibition and found pacritinib to be a highly potent ACVR1 inhibitor, with no significant ACVR1 inhibition by ruxolitinib or fedratinib.12
Pacritinib is now being used regularly in the first- and second-line treatment of MF patients with thrombocytopenia. This is especially true of patients with severe thrombocytopenia, who were excluded from ruxolitinib and fedratinib Phase III trials and are at risk for worsening their cytopenias with other JAK inhibitors.
Momelotinib
Momelotinib is a selective JAK1 and JAK2 inhibitor that also targets activin A receptor type 1 (ACVR1). Inhibition of ACVR1 has been demonstrated to reduce hepcidin transcription (a protein that is commonly elevated in MF), which in turn increases available iron stores and subsequently increases hemoglobin production.12 Furthermore, the JAK/STAT3 pathway is activated by IL-6 which in turn increases the production of hepcidin. Momelotinib’s inhibition of JAK1 and JAK2 further blocks hepcidin production by downregulating the JAK/STAT3 pathway.29 With high rates of anemia observed with previous JAK inhibitors, momelotinib was designed to not only reduce spleen size and alleviate symptoms through its JAK inhibition, but also to prevent or improve existing anemia.
Phase I/II Trials
The first major trial for momelotinib in MF was a phase I/II dose escalation/confirmation trial (Table 2). The maximum tolerated dose in the dose escalation phase was determined to be 300mg daily. Subsequently, patients were given either 150mg or 300mg daily and 48% of patients overall achieved a SVR35% with no significant difference between the groups. Regarding anemia, the median hemoglobin at baseline was 9.4g/dl, with 55% of patients being transfusion dependent. Overall, 70% patients who received a transfusion over the prior month before the study achieved a minimum of 12 weeks without another transfusion on momelotiib, while 59% of patients overall demonstrated clinical improvement in anemia per the International Working Group-Myeloproliferative Neoplasm Research and Treatment (IWG-MRT) criteria (defined as a hemoglobin improvement ≥2g/dL in transfusion independent patients with hemoglobin <10g/dL). Notable adverse effects included grade 3/4 thrombocytopenia (32%) and peripheral neuropathy (22%).30 A follow-up study, involving 166 patients, largely confirmed earlier findings. In this study, 75% of transfusion dependent patients achieved a transfusion independent response, and patients with anemia at baseline experienced a mean hemoglobin increase of 2.4g/dl. Spleen response was reached in 40% of patients who presented with palpable splenomegaly at baseline. Peripheral neuropathy remained a common side effect, occurring in 27% of patients.31
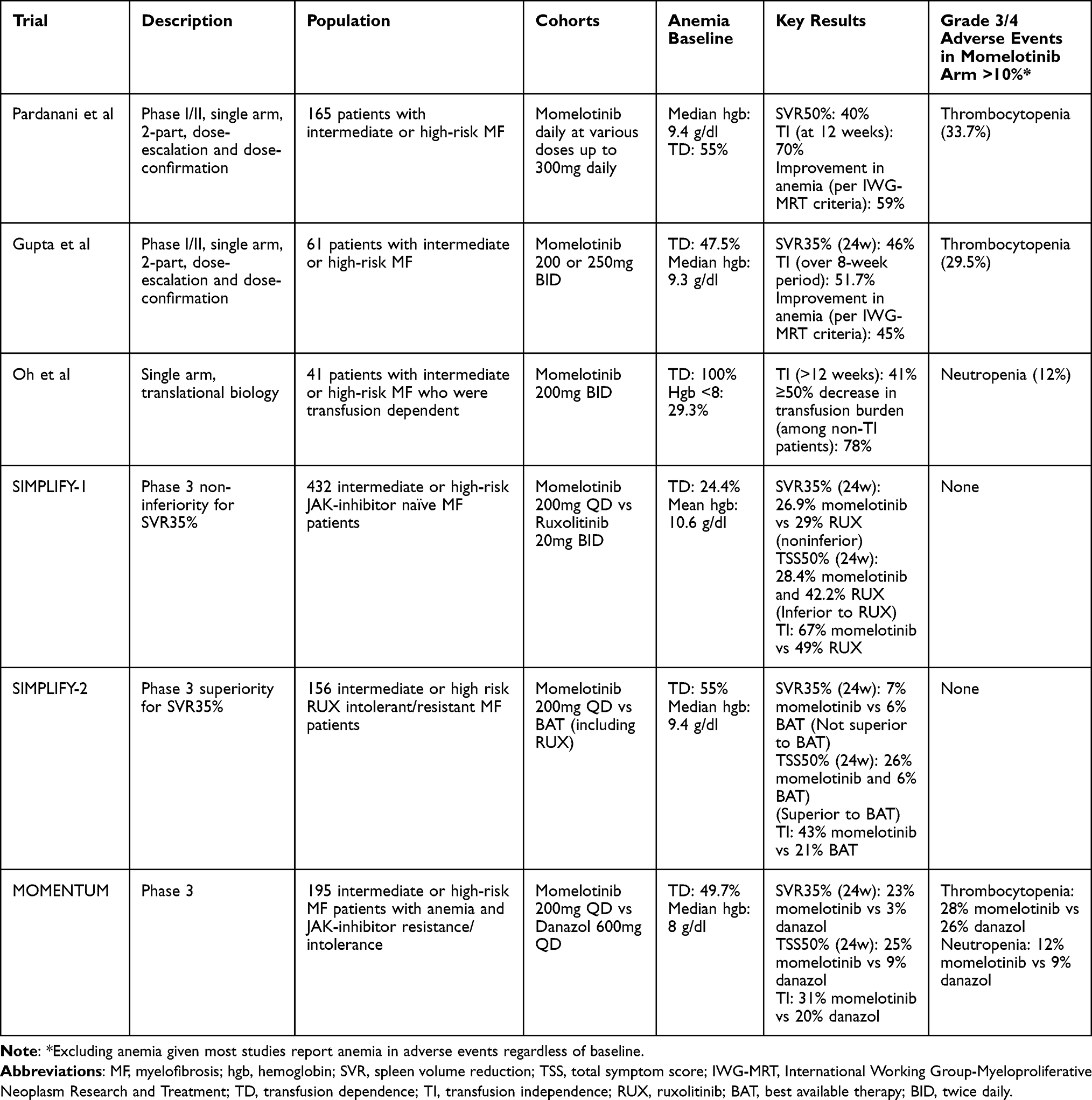 |
Table 2 Clinical Trials Involving Momelotinib |
A second phase I/II trial of momelotinib aimed to evaluate the safety and therapeutic benefit of twice-daily dosing. Sixty-one patients were enrolled in the dose escalation phase. The optimal dosing of 200mg twice daily was then used in the expanded phase 2 component. In this phase, 46% achieved SVR35% at 24 weeks. Per the IWG-MRT criteria, 45% of patients also experienced an anemia response, with 52% of transfusion-dependent patients achieving transfusion independence over an 8-week period. Peripheral neuropathy occurred in 44% of patients (41% with grade 1/2, 3% with grade 3), with other adverse effects including diarrhea (46%), thrombocytopenia (39%), and dizziness (36%).32
To further investigate the impact and mechanism of anemia improvement with momelotinib, a phase 2 open-label study enrolled 41 transfusion-dependent patients with MF who were treated with momelotinib 200mg tablets daily (bioequivalent to 300mg capsule dose).13 Forty-one percent of patients achieved transfusion independence for more than 12 weeks. Of the patients that did not reach 12 weeks of transfusion independence, 78% achieved a greater than 50% decrease in transfusion requirements for over 8 weeks. Moreover, momelotinib treatment led to an acute and persistent decrease in hepcidin, which was more pronounced in the patients who achieved transfusion independence. Patients who reached transfusion independence also had lower inflammatory markers (CRP), increased markers essential for erythropoiesis (liver iron concentration, serum iron, ferritin, and transferrin saturation) and markers of increased BM function (erythrocytes, reticulocytes, platelets). This study helps confirm the mechanism of momelotinib’s anemia benefit by via ACVR1 inhibition, leading to downregulation of hepcidin and resulting in an increase in available iron and erythropoiesis.13
SIMPLIFY-1
In the first phase 3 trial of momelotinib, 432 patients with high-risk, intermediate-2 risk, or symptomatic intermediate-1 risk MF were assigned to either momelotinib 200mg daily or ruxolitinib 20mg twice daily for 24 weeks (allowing for crossover to momelotinib after 24 weeks) to assess non-inferiority. The primary outcome of SVR35% was 27% and 29% in the momelotinib and ruxolitinib groups, respectively (non-inferior, p = 0.11). The secondary outcome of TSS50% was reached in 42% of patients in the ruxolitinib arm and 28% of patients in the momelotinib arm (p = 0.98), failing to meet non-inferiority. Transfusion independence at week 24 was reached in 67% of patients in the momelotinib arm compared to 49% in the ruxolitinib arm (p < 0.001), and the median RBC units transfused were also lower in the momelotinib arm compared to the ruxolitinib arm (0 vs 0.4, p < 0.001). Fewer patients required dose reduction in the momelotinib arm (26%) than in the ruxolitinib arm (56%). Grade 3/4 anemia occurred in only 5.6% of patients in the momelotinib arm compared to 23% in the ruxolitinib arm. Treatment-emergent peripheral neuropathy was double in those patients receiving momelotinib (10% vs 5%).33
SIMPLIFY-2
The second phase 3 trial of momelotinib, SIMPLIFY-2, included patients with MF who had prior treatment with ruxolitinib, and either required red blood cell transfusions, dose reductions, or had grade 3/4 thrombocytopenia, anemia, or bleeding while on treatment. One hundred and fifty-six patients were randomly assigned to momelotinib 200mg daily or BAT (ruxolitinib was allowed and used in 89% of patients in this arm) for 24 weeks before allowing momelotinib treatment in the control arm. Only 7% of patients achieved SVR35% in the momelotinib arm compared to 6% in the BAT arm (p = 0.90). The low levels of SVR35% in this study compared to SIMPLIFY-1 are attributed to the lack of a washout period after ruxolitinib, as well as the inclusion of patients who had already failed to reach SVR35% during their ruxolitinib use (making them less likely to reach that mark with another JAK inhibitor). However, the secondary endpoint of TSS50% did reach statistical significance (p = 0.0006), with 26% of patients in the momelotinib arm and 6% in the BAT arm reaching this endpoint. The momelotinib group had lower rates of red blood cell transfusions (median rates of 0.5 units/month vs 1.2 units/month, p = 0.39) and higher rates of transfusion independence at week 24 compared to BAT (43% vs 21%, p = 0.0012). The rates of grade 3/4 anemia and thrombocytopenia were similar between the groups. Peripheral neuropathy occurred in 11% in patients taking momelotinib compared to 0 in those not taking momelotinib.34
MOMENTUM
MOMENTUM is the most recently published phase III trial of momelotinib. Eligible patients were required to have a baseline hemoglobin of <10g/dl and previous exposure to another JAK-inhibitor for either >90 days or for >28 days if complicated by transfusion dependent anemia or grade 3/4 anemia, thrombocytopenia, or hematoma. Compared to SIMPLIFY-2, patients were required to have a washout of previous JAK-inhibitors with no therapy for at least 2 weeks before entering the trial. One hundred and ninety-five patients were randomly assigned to either momelotinib 200mg daily or danazol for a 24-week period. Danazol was chosen as the comparator given its recommendation to treat anemia in MF patients per the National Comprehensive Cancer Network at the time of the trial.35 The primary outcome of the study, TSS50% at 24 weeks, was reached by 25% of patients in the momelotinib group compared to 9% in the danazol group (p = 0.0095). It is important to note that many of the symptoms documented in the TSS scoring system are unrelated to anemia and would not be expected to improve with danazol treatment.36 SVR35% was greater in the momelotinib group than the danazol group (23% vs 3%, p = 0.0006), which is also not surprising given danazol having no evidence in decreasing spleen size. Regarding anemia benefits, transfusion independence at 24 weeks was achieved by 31% of patients receiving momelotinib compared to 20% receiving danazol (p = 0.0064, reaching non-inferiority). Due to non-inferiority being reached, a superiority test was done, finding a treatment difference of 11% (p = 0.086). Grade 3/4 thrombocytopenia and neutropenia were similar between the two groups. The most common grade 3/4 non-hematologic adverse events were acute kidney injury (3% with momelotinib, 9% with danazol) and pneumonia (2% with momelotinib, 9% with danazol).37
In summary, these studies demonstrate that momelotinib is a promising option for patients with anemic MF who are either JAK inhibitor naïve or refractory/intolerant to ruxolitinib. It is important to note that momelotinib’s efficacy in reducing spleen size, alleviating symptoms, and improving anemia is maintained even in patients with thrombocytopenia, as showed by a pooled analysis of both SIMPLIFY trials.15 This is in contrast to ruxolitinib, where dose reductions in thrombocytopenic patients led to decreased spleen size reduction and symptomatic improvement compared to non-thrombocytopenic patients who did not dose reduce.15 Now, with three available JAK inhibitors and momelotinib poised to be approved, the question arises about the potential survival benefit of this class of medications.
JAK Inhibitor Survival Data
Although the development of JAK inhibitors has had an undeniable positive impact on the lives of MF patients, specifically improving symptoms and reducing spleen size, there is no clear evidence of a long-term OS benefit or disease-modifying capacity associated with this class of drugs. While some phase III JAK inhibitor trials and long-term follow-ups have shown trends towards an OS benefit,37,38 none of these studies were powered to detect survival outcomes.
The first promising study indicating long-term OS with JAK inhibitors was a pooled analysis of COMFORT-I and COMFORT-II where the risk of death was reduced by 30% in patients randomized to the ruxolitinib arm versus the control arm (HR 0.70, p = 0.0065). This OS benefit increased even further after correcting for high crossover rates to ruxolitinib after placebo/BAT (HR 0.35, CI 0.23–0.59). Furthermore, patients who started on ruxolitinib had a better OS compared to those patients who started on placebo/BAT and crossed over to ruxolitinib (HR 0.53, p = 0.0013).38 However, given the nature of long-term follow-up studies and the absence of randomization and controls, drawing definite conclusions from this type of analysis is difficult. A Cochrane systematic review in 2015 concluded that there is low-quality evidence for the effect of ruxolitnib on survival compared to placebo.39 Since then, multiple studies have continued to investigate a possible survival benefit of ruxolitinib. In one study, 1010 patients from the ERNEST study in Europe were prospectively followed and median OS was compared between patients receiving only hydroxyurea and patients receiving ruxolitnib (in the front-line or after hydroxyurea). Medium OS in patients exposed to ruxolitinib was 7.7 years compared to 3.4 years in patients treated with only hydroxyurea (P = 0.002).40 Another study, retrospectively analyzing MF from the US Medicare Fee-for-Service claims database, found a decreased mortality risk in patients exposed to ruxolitinib compared to those not exposed to ruxolitinib (HR 0.61, P = 0.002).41 Prospective clinical trials powered to detect OS are needed to confirm these findings.
Determining the survival impact of fedratinib and pacritinib is complicated by early trial terminations for both agents, censoring follow up data. Regardless, attempts have been made to determine the impact of fedratinib on survival. In the JAKARTA trial, there was a prolongation of median progression free survival (PFS) with fedratinib compared to placebo (HR 0.42, p = 0.004), but no significant OS benefit after 1 year. In JAKARTA-2, survival was censored for at study termination, but the 18-month survival rate in the fedratinib arm was 67%, which compares favorably to the OS of patients who discontinue ruxolitinib.24,42 Regarding pacritinib, in both PERSIST-1 and 2, there was no significant OS difference at 24 weeks between the pacritinib and control arms.26,43
Survival analysis has been explored for momelotinib-treated patients. In SIMPLIFY-1, OS was similar between the momelotinib arm and ruxolitinib arm (HR 1.02 CI 0.73–1.43) as were two-year OS and leukemia free survival. In SIMPLIFY-2, the two-year OS was 65.8% compared to 61.2% (HR 0.98, CI 0.59–1.62) in the momelotinib arm compared to the BAT arm (in patients with prior ruxolitinib exposure). Notably, based on retrospective analysis of both studies, momelotinib use was associated with improved OS in multivariate analysis in patients with a week 24 transfusion independence response in JAK inhibitor naïve patients (HR 0.311, p < 0.0001). This suggests an association between improving transfusion dependence with momelotinib and OS, a finding that requires further study.44 In the MOMENTUM trial, OS and LFS favored momelotinib versus danazol, but results were not statistically significant (OS HR 0.73, p = 0.35; OS LFS 0.65, p = 0.17). Due to high rates of crossover in phase III trials, the effect of momelotinib on OS will likely be difficult to discern in long-term follow-up of these trials.37
Given the lack of major improvement in OS from this class of medications alone and the poor outcomes in the increasingly prevalent population of MF patients with suboptimal response or progression on JAK inhibitors, there has been a shift towards developing drugs that can potentially change the rate of progression of the underlying disease. More recent trials are including endpoints such as reductions in BM fibrosis, driver mutation allele burden, leukemic transformation, and overall survival.45,46 These newer agents are being studied alone and in conjunction with JAK inhibitors to both improve response rates and potentially achieve disease modification.
Novel Combination Therapy
Pelabresib
Pelabresib is a bromodomain and extra-terminal domain (BET) inhibitor that is now being studied with ruxolitinib in patients with MF (Table 3). BET inhibition has been shown in mouse models to work synergistically with JAK inhibition to reduce the burden of MPN disease and potentially prolong survival.47 The phase 2 MANIFEST trial had 4 treatment arms. Arm 1 was pelabresib monotherapy after ruxolitinib failure in MF patients, arm 2 added on pelabresib to MF patients with inadequate response to ruxolitinib, while arm 3 enrolled JAK inhibitor naïve MF patients to get pelabresib plus ruxolitinib (arm 4 was open to patients with essential thrombocythemia). While arms 1 and 2 showed some improvement in SVR35% and TSS50%, arm 3 showed the most promising results. Arm 3 enrolled 84 patients to receive the pelabresib/ruxolitinib combination. At 24 weeks, 68% of patients achieved SVR35 (60% at 48 weeks) and 56% achieved TSS50%. Additionally, 36% of patients had improvements in their hemoglobin levels, 28% had improvements in BM fibrosis, and 25% had a reduction in their JAK2V617F mutant allele fraction (which was associated with SVR35% response). The most common grade 3/4 adverse effects were anemia (35%) and thrombocytopenia (12%). Eighty out of the 84 patients enrolled in the trial tolerated the combination of drugs for greater than 24 weeks.48 Following the success of arm 3 of the phase 2 MANIFEST trial, a phase III trial (MANIFEST-2) is enrolling JAK inhibitor naïve patients to receive either pelabresib and ruxolitinib versus placebo and ruxolitinib. The primary outcome is SVR35% at 24 weeks and secondary outcomes include TSS50%, improvements in BM fibrosis, RBC transfusion rates, conversion to transfusion independence, survival (OS, PFS) and transformation to acute myeloid leukemia.49 This study will hopefully open the door for additional future combination therapies that can further improve the depth and duration and spleen and symptom response, as well potentially alter the disease course in MF patients.
 |
Table 3 Novel Agents |
Navitoclax
Another potential target for synergistic combination therapy in MF patients is B-Cell Lymphoma-2/extra-large (BCL-2/BCL-xL) inhibition. The JAK-STAT pathway increases BCL-2/BCL-xL and the inhibition of both targets has been shown to overcome JAK2 inhibitor resistance and induce apoptosis in JAK2V617F mutated cells.50–52 Navitoclax is a BCL-2/BCL-xL inhibitor that is being studied in combination with ruxolitinib in MF patients. The REFINE study is a Phase II open label trial assessing the efficacy and safety of navitoclax. In Cohort 1a, 34 patients already receiving ruxolitinib for greater than 12 weeks were enrolled and continued their current ruxolitinib dose while adding on navitoclax daily. SVR35% was achieved in 31% and TSS50% in 33% of patients. Improvement in BM fibrosis by at least 1 grade was achieved in 38% of patients, while reductions in JAK2V617F variant allele frequency (VAF) by at least 20% was achieved in 23% of patients. Importantly, patients with improvements in BM fibrosis and a reduction in VAF by at least 20% had improved OS compared to patients who did not reach both benchmarks. This suggests the possibility of disease modification in those that responded to the drug combination, although these metrics have not been validated as surrogate endpoints. Of note, there was a high-rate of treatment related reversible thrombocytopenia (88%) with navitoclax.53
Cohort 2 of the REFINE trial enrolled 30 patients who were previously, but not actively, taking JAK inhibitors and started them on Navitoclax monotherapy. These patients had a similar side effect profile of those in Cohort 1a including thrombocytopenia (53%), diarrhea (30%), and nausea (27%). Only three patients discontinued the medication due to adverse effects. Efficacy analyses for navitoclax monotherapy are still pending.54
Cohort 3 of the REFINE trial investigated navitoclax and ruxolitinib in JAK inhibitor naïve patients. Thirty-two patients received the combination therapy. SVR35% at week 24 was reached in 52% of patients. BM fibrosis improvement was reached in 35% and complete resolution of BM fibrosis in 22% of patients. Reduction in JAK2V617F VAF by at least 20% or 50% was achieved 50% and 36% of patients, respectively.55 Phase III trials are currently ongoing to test the combination of navitoclax and ruxolitinib in both JAK inhibitor naïve (TRANSFORM-1, NCT04472598) and relapsed/refractory (TRANSFORM-2, NCT04468984) MF patients.50
Luspatercept
Luspatercept is a recombinant fusion protein that acts as a transforming growth factor beta (TGF-β) trap and ultimately works to improve anemia by inhibiting growth differentiation factor 11 (GDF11). GDF11 is a key inhibitor of late-stage erythroid differentiation, which has been shown to be upregulated in MDS and MF patients.56 Luspatercept has been already approved for the treatment of anemia in myelodysplastic syndrome (MDS) and beta thalassemia, but is now being studied in patients with MF. In a phase 2 study, 74 patients with MF and anemia were enrolled and stratified based on their level of transfusion dependence and their current use of ruxolitinib. All patients received luspatercept every 21 days. The primary endpoint of a hemoglobin increase of ≥1.5g/L (for 12 consecutive weeks) in patients who were transfusion independent at baseline was reached in 21% and 10% of patients with and without ruxolitnib respectively. The primary endpoint of transfusion independence in patients who were transfusion dependent at baseline was reached in 32% and 10% of patients with and without ruxolitinib, respectively. The most common grade 3/4 adverse effects were hypertension (11%), bone pain (8%), and diarrhea (4%).57 The INDEPENDENCE trial (NCT04717414) is an ongoing phase 3 trial assessing luspatercept against placebo in transfusion dependent patients receiving a stable dose of a JAK inhibitor.
INCB00928 (ALK2 Inhibitor)
As seen with momelotinib and pacritinib, ACVR1 inhibition leads to significant improvement in anemia in MF patients. The ACVR1 gene encodes a serine/threonine kinase called activin receptor-like kinase 2 (ALK2). In preclinical models, knockout of ALK2 leads to decreased hepcidin and elevated serum iron levels. INCB00928 is a potent ALK2 inhibitor that in mouse modules improved RBC count, hemoglobin, and hematocrit levels, while decreasing hepcidin levels in a dose-dependent manner.58 NCT04455841 is an ongoing Phase 1/2 dose escalation/expansion study evaluating INCB00928 alone and in combination with ruxolitinib in transfusion dependent MF patients. As of November 2022, 15 patients were enrolled in the dose escalation phase and the maximum tolerated dose was not yet reached. No dose limiting toxicities occurred and a reduction in hepcidin levels was observed in both the monotherapy and the ruxolitinib groups.59
There are currently many new agents under investigation for treating MF alone or in combination with JAK inhibitors. Navetmadlin, a human double-minute homolog 2 (HDM2) inhibitor, has shown promise in phase II trials and is currently in a phase III trial (BOREAS) for patients with relapsed/refractory MF.60 Another promising drug is imetelstat, a telomerase inhibitor, which has also been successful in phase II trials and is currently being studied in a phase III trial (IMpactMF) against BAT for MF patients refractory to JAK inhibitors.61 Other agents currently being investigated are TP-3654 (PIM-1 inhibitor), PXS5505 (pan-lysyl oxidase inhibitor), TL-895 (tyrosine kinase inhibitor), selinexor (selective inhibitor of nuclear export, SINE, inhibitor), and bomedemstat (lysine-specific demethylase 1, LSD1, inhibitor).
Conclusion
Currently, there are 3 FDA approved JAK-inhibitors for the treatment of MF. Ruxolitinib is frequently given as first line in patients without significant cytopenias, due to its well-established track record of improving symptoms and reducing spleen size. Fedratinib serves as an alternative first-line option but is more commonly reserved as a second-line treatment in cases of ruxolitnib failure, as demonstrated in the JAKARTA-2 trial. Pacritinib, specifically approved for patients with a platelet count <50x109/L, is the preferred treatment for patients with moderate to severe thrombocytopenia, either as the front line or when refractory/intolerant to other JAK-inhibitors. Finally, although not yet approved as of the writing of this manuscript, momelotinib shows promise in treating MF patients with anemia, especially those with transfusion dependence. The results of the SIMPLIFY-1, SIMPLIFY-2, and MOMENTUM trials not only demonstrate improvements in symptom score and spleen reduction, but also suggest a possible treatment for MF-related anemia. All three trials show a decrease in overall transfusions and an increase in transfusion independence.
Given evidence of improving hemoglobin with both pacritinib and momelotinib, determining the optimal treatment of anemic MF patients is unknown. Although unlikely to be performed, future studies comparing pacritinib and momelotinib in patients with anemia and/or thrombocytopenia would be of obvious importance. Absent these prospective evaluations, retrospective evaluations after availability of both agents will be important. Of note, in the previously discussed study evaluating anemia benefit with pacritinib and momelotinib, pacritinib was found to be four times more potent as an inhibitor of ACVR1 as compared with momelotinib using the HotSpot assay assessed in this analysis.12 However, based on presently available data, there is more evidence supporting the use of momelotinib to improve anemia in MF patients given the robust findings in prospective phase III trials powered to detect improvement in anemia, while the pacritinib data available is largely retrospective/post hoc. Additional research is needed to evaluate pacritinib’s ability to improve anemia, as well as momelotinib’s efficacy in patients with severe thrombocytopenia. A decision regarding which agent to choose may also incorporate non-hematologic side effects of each agent including high rates of gastrointestinal side effects with pacritinib (diarrhea, nausea, vomiting) and peripheral neuropathy with momelotinib.
The future of therapy in MF will likely involve selecting the optimal JAK inhibitor based on individual patient characteristics and previous medication exposure, followed by determining the usefulness of add-on therapies and selecting the most appropriate combination (Figure 1). Pelabresib, navitoclax, luspatercept, and ALK2 inhibitors are currently in phase 3 trials as upfront treatment and additional agents are also being evaluated as add-on therapies. Although ruxolitinib is currently being explored as the partner JAK inhibitor to novel therapies, future trials would benefit from exploring combinations with other JAK inhibitors such as pacritinib and momelotinib, particularly in patients with cytopenias. These novel therapies will hopefully provide deeper responses than JAK inhibitors alone, which is critically important given the poor outcomes in patients who eventually become refractory to one or another JAK inhibitor. These novel drugs may also offer the potential for disease modification and achieve important outcomes such as reversal of BM fibrosis, decreased leukemic progression and ultimately improved OS, which has largely been absent with the current JAK inhibitors.
 |
Figure 1 Proposed positioning of front line JAK inhibitors for the treatment of myelofibrosis. The initial selection of a JAK inhibitor should be based primarily on the presence of anemia and thrombocytopenia. The optimal choice in patients with concurrent anemia and thrombocytopenia remains unclear although should be influence by the severity of each cytopenia. |
With the approval of the first JAK inhibitor just over a decade ago, the future of MF therapy is extremely promising. We now have the choice of several JAK inhibitors that can improve symptoms and quality of life for patients with MF. These JAK inhibitors can now be tailored to individual patients based on their underlying comorbidities and cytopenias. Additionally, there are several exciting new classes of drugs being tested with and without JAK inhibitors to potentially reverse aspects of this disease and prolong patients’ lives. Clinical trials are ongoing and continuously needed to advance the field and expand the therapeutic possibilities for MF patients.
Disclosure
Dr Douglas Tremblay reports grants, personal fees from CTI Biopharma, grants from Astellas Pharma, grants from Gilead, personal fees from Novartis, personal fees from AbbVie, personal fees from Sierra Oncology, personal fees from GSK, personal fees from Cogent Biosciences, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Abdel-Wahab OI, Levine RL. Primary myelofibrosis: update on definition, pathogenesis, and treatment. Annu Rev Med. 2009;60:233–245. doi:10.1146/annurev.med.60.041707.160528
2. Reilly JT, McMullin MF, Beer PA, et al. Guideline for the diagnosis and management of myelofibrosis. Br J Haematol. 2012;158(4):453–471. doi:10.1111/j.1365-2141.2012.09179.x
3. Tefferi A, Lasho TL, Jimma T, et al. One Thousand Patients with Primary Myelofibrosis: The Mayo Clinic Experience. Elsevier; 2012.
4. Cervantes F, Dupriez B, Pereira A, et al. New prognostic scoring system for primary myelofibrosis based on a study of the international working group for myelofibrosis research and treatment. Blood. 2009;113(13):2895–2901. doi:10.1182/blood-2008-07-170449
5. Tefferi A, Hudgens S, Mesa R, et al. Use of the functional assessment of cancer therapy− anemia in persons with myeloproliferative neoplasm-associated myelofibrosis and anemia. Clin Ther. 2014;36(4):560–566. doi:10.1016/j.clinthera.2014.02.016
6. Guglielmelli P, Rotunno G, Pacilli A, et al. Prognostic impact of bone marrow fibrosis in primary myelofibrosis. A study of the AGIMM group on 490 patients. Am J Hematol. 2016;91(9):918–922. doi:10.1002/ajh.24442
7. Wang X, Cho SY, Hu CS, Chen D, Roboz J, Hoffman R. CXC motif chemokine 12 influences the development of extramedullary hematopoiesis in the spleens of myelofibrosis patients. Exp Hematol. 2015;43(2):100–109. e1. doi:10.1016/j.exphem.2014.10.013
8. Pardanani A, Finke C, Abdelrahman RA, Lasho TL, Tefferi A. Associations and prognostic interactions between circulating levels of hepcidin, ferritin and inflammatory cytokines in primary myelofibrosis. Am J Hematol. 2013;88(4):312–316. doi:10.1002/ajh.23406
9. Rampal R, Al-Shahrour F, Abdel-Wahab O, et al. Integrated genomic analysis illustrates the central role of JAK-STAT pathway activation in myeloproliferative neoplasm pathogenesis. Blood. 2014;123(22):e123–e133. doi:10.1182/blood-2014-02-554634
10. Verstovsek S, Mesa RA, Gotlib J, et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N Engl J Med. 2012;366(9):799–807. doi:10.1056/NEJMoa1110557
11. Pardanani A, Harrison C, Cortes JE, et al. Safety and efficacy of fedratinib in patients with primary or secondary myelofibrosis: a randomized clinical trial. JAMA Oncol. 2015;1(5):643–651. doi:10.1001/jamaoncol.2015.1590
12. Oh ST, Mesa R, Harrison C, et al. Pacritinib is a potent ACVR1 inhibitor with significant anemia benefit in patients with myelofibrosis. Blood. 2022;140(Supplement 1):1518–1521. doi:10.1182/blood-2022-156936
13. Oh ST, Talpaz M, Gerds AT, et al. ACVR1/JAK1/JAK2 inhibitor momelotinib reverses transfusion dependency and suppresses hepcidin in myelofibrosis phase 2 trial. Blood Adv. 2020;4(18):4282–4291. doi:10.1182/bloodadvances.2020002662
14. Verstovsek S, Mesa R, Talpaz M, et al. Retrospective analysis of pacritinib in patients with myelofibrosis and severe thrombocytopenia. Haematologica. 2022;107(7):1599. doi:10.3324/haematol.2021.279415
15. Kiladjian JJ, Platzbecker U, Mayer J, et al. Momelotinib’s spleen, symptom and anemia efficacy is maintained in intermediate/high risk myelofibrosis patients with thrombocytopenia. Blood. 2020;136:43–44. doi:10.1182/blood-2020-135880
16. Harrison C, Kiladjian -J-J, Al-Ali HK, et al. JAK inhibition with ruxolitinib versus best available therapy for myelofibrosis. N Engl J Med. 2012;366(9):787–798. doi:10.1056/NEJMoa1110556
17. Gupta V, Harrison C, Hexner EO, et al. The impact of anemia on overall survival in patients with myelofibrosis treated with ruxolitinib in the COMFORT studies. Haematologica. 2016;101(12):e482. doi:10.3324/haematol.2016.151449
18. Cervantes F, Ross DM, Radinoff A, et al. Efficacy and safety of a novel dosing strategy for ruxolitinib in the treatment of patients with myelofibrosis and anemia: the REALISE phase 2 study. Leukemia. 2021;35(12):3455–3465. doi:10.1038/s41375-021-01261-x
19. Harrison CN, Vannucchi AM, Kiladjian -J-J, et al. Long-term findings from COMFORT-II, a phase 3 study of ruxolitinib vs best available therapy for myelofibrosis. Leukemia. 2016;30(8):1701–1707. doi:10.1038/leu.2016.148
20. Verstovsek S, Mesa RA, Gotlib J, et al. Long-term treatment with ruxolitinib for patients with myelofibrosis: 5-year update from the randomized, double-blind, placebo-controlled, phase 3 COMFORT-I trial. J Hematol Oncol. 2017;10(1):1–14. doi:10.1186/s13045-017-0417-z
21. Mullally A, Hood J, Harrison C, Mesa R. Fedratinib in myelofibrosis. Blood Adv. 2020;4(8):1792–1800. doi:10.1182/bloodadvances.2019000954
22. Harrison CN, Schaap N, Vannucchi AM, et al. Janus kinase-2 inhibitor fedratinib in patients with myelofibrosis previously treated with ruxolitinib (Jakarta-2): a single-arm, open-label, non-randomised, phase 2, multicentre study. Lancet Haematol. 2017;4(7):e317–e324. doi:10.1016/S2352-3026(17)30088-1
23. Harrison CN, Schaap N, Vannucchi AM, et al. Fedratinib in patients with myelofibrosis previously treated with ruxolitinib: an updated analysis of the JAKARTA2 study using stringent criteria for ruxolitinib failure. Am J Hematol. 2020;95(6):594–603. doi:10.1002/ajh.25777
24. Waksal JA, Tremblay D, Mascarenhas J. Clinical utility of fedratinib in myelofibrosis. Onco Targets Ther. 2021;14:4509. doi:10.2147/OTT.S267001
25. Gupta V, Yacoub A, Verstovsek S, et al. Safety and efficacy of fedratinib in patients with Primary (P), Post-Polycythemia Vera (Post-PV), and Post-Essential Thrombocythemia (Post-ET) Myelofibrosis (MF) previously treated with ruxolitinib: primary analysis of the FREEDOM trial. Blood. 2022;140(Supplement 1):3935–3937. doi:10.1182/blood-2022-156669
26. Mascarenhas J, Hoffman R, Talpaz M, et al. Pacritinib vs best available therapy, including ruxolitinib, in patients with myelofibrosis: a randomized clinical trial. JAMA Oncol. 2018;4(5):652–659. doi:10.1001/jamaoncol.2017.5818
27. Mascarenhas J, Gerds AT, Kiladjian -J-J, et al. PACIFICA: a randomized, controlled phase 3 study of pacritinib versus physician’s choice in patients with primary or secondary myelofibrosis and severe thrombocytopenia. Blood. 2022;140(Supplement 1):9592–9594. doi:10.1182/blood-2022-163456
28. Yacoub A, Mesa RA, Oh ST. Long-term hematologic improvement in a patient with cytopenic myelofibrosis treated with pacritinib; 2023.
29. Wrighting DM, Andrews NC. Interleukin-6 induces hepcidin expression through STAT3. Blood. 2006;108(9):3204–3209. doi:10.1182/blood-2006-06-027631
30. Pardanani A, Laborde R, Lasho T, et al. Safety and efficacy of CYT387, a JAK1 and JAK2 inhibitor, in myelofibrosis. Leukemia. 2013;27(6):1322–1327. doi:10.1038/leu.2013.71
31. Pardanani A, Gotlib J, Roberts A, et al. Long-term efficacy and safety of momelotinib, a JAK1 and JAK2 inhibitor, for the treatment of myelofibrosis. Leukemia. 2018;32(4):1034–1037. doi:10.1038/leu.2017.330
32. Gupta V, Mesa RA, Deininger MW, et al. A phase 1/2, open-label study evaluating twice-daily administration of momelotinib in myelofibrosis. Haematologica. 2017;102(1):94. doi:10.3324/haematol.2016.148924
33. Mesa RA, Kiladjian -J-J, Catalano JV, et al. SIMPLIFY-1: a phase III randomized trial of momelotinib versus ruxolitinib in janus kinase inhibitor-naive patients with myelofibrosis. J Clin Oncol. 2017;35(34):3844–3850. doi:10.1200/JCO.2017.73.4418
34. Harrison CN, Vannucchi AM, Platzbecker U, et al. Momelotinib versus best available therapy in patients with myelofibrosis previously treated with ruxolitinib (SIMPLIFY 2): a randomised, open-label, phase 3 trial. Lancet Haematol. 2018;5(2):e73–e81. doi:10.1016/S2352-3026(17)30237-5
35. Mesa RA, Jamieson C, Bhatia R, et al. NCCN guidelines insights: myeloproliferative neoplasms, version 2.2018. J Natl Compr Canc Netw. 2017;15(10):1193–1207. doi:10.6004/jnccn.2017.0157
36. Gwaltney C, Paty J, Kwitkowski VE, et al. Development of a harmonized patient-reported outcome questionnaire to assess myelofibrosis symptoms in clinical trials. Leuk Res. 2017;59:26–31. doi:10.1016/j.leukres.2017.05.012
37. Verstovsek S, Gerds AT, Vannucchi AM, et al. Momelotinib versus danazol in symptomatic patients with anaemia and myelofibrosis (MOMENTUM): results from an international, double-blind, randomised, controlled, phase 3 study. Lancet. 2023;401(10373):269–280. doi:10.1016/S0140-6736(22)02036-0
38. Verstovsek S, Gotlib J, Mesa RA, et al. Long-term survival in patients treated with ruxolitinib for myelofibrosis: COMFORT-I and-II pooled analyses. J Hematol Oncol. 2017;10:1–6. doi:10.1186/s13045-017-0527-7
39. Martí‐Carvajal AJ, Anand V, Sola I. Janus kinase‐1 and Janus kinase‐2 inhibitors for treating myelofibrosis. Cochrane Database Syst Rev. 2015;(4). doi:10.1002/14651858.CD010298.pub2
40. Guglielmelli P, Ghirardi A, Carobbio A, et al. Impact of ruxolitinib on survival of patients with myelofibrosis in the real world: update of the ERNEST Study. Blood Adv. 2022;6(2):373–375. doi:10.1182/bloodadvances.2021006006
41. Verstovsek S, Parasuraman S, Yu J, et al. Real-world survival of US patients with intermediate-to high-risk myelofibrosis: impact of ruxolitinib approval. Ann Hematol. 2022;2022:1–7.
42. Harrison C, Kiladjian -J-J, Verstovsek S, et al. MPN-164: overall survival (OS) and progression-free survival (PFS) in patients treated with fedratinib as first-line myelofibrosis (MF) therapy and after prior ruxolitinib (RUX): results from the Jakarta and JAKARTA2 trials. Clin Lymphoma Myeloma Leuk. 2021;21:S356. doi:10.1016/S2152-2650(21)01822-X
43. Mesa RA, Vannucchi AM, Mead A, et al. Pacritinib versus best available therapy for the treatment of myelofibrosis irrespective of baseline cytopenias (PERSIST-1): an international, randomised, phase 3 trial. Lancet Haematol. 2017;4(5):e225–e236. doi:10.1016/S2352-3026(17)30027-3
44. Mesa R, Harrison C, Oh ST, et al. Overall survival in the SIMPLIFY-1 and SIMPLIFY-2 phase 3 trials of momelotinib in patients with myelofibrosis. Leukemia. 2022;36(9):2261–2268. doi:10.1038/s41375-022-01637-7
45. Vachhani P, Verstovsek S, Bose P. Disease modification in myelofibrosis: an elusive goal? J Clin Oncol. 2022;40(11):1147–1154. doi:10.1200/JCO.21.02246
46. Pemmaraju N, Verstovsek S, Mesa R, et al. Defining disease modification in myelofibrosis in the era of targeted therapy. Cancer. 2022;128(13):2420–2432. doi:10.1002/cncr.34205
47. Kleppe M, Koche R, Zou L, et al. Dual targeting of oncogenic activation and inflammatory signaling increases therapeutic efficacy in myeloproliferative neoplasms. Cancer Cell. 2018;33(1):29–43. e7. doi:10.1016/j.ccell.2017.11.009
48. Mascarenhas J, Kremyanskaya M, Patriarca A, et al. MANIFEST: pelabresib in combination with ruxolitinib for janus kinase inhibitor treatment-naïve myelofibrosis. J Clin Oncol;2023.
49. Harrison CN, Gupta VK, Gerds AT, et al. Phase III MANIFEST-2: pelabresib+ ruxolitinib vs placebo+ ruxolitinib in JAK inhibitor treatment-naive myelofibrosis. Future Oncol. 2022;18(27):2987–2997. doi:10.2217/fon-2022-0484
50. Tremblay D, Mesa R, Paiva CE. New treatments for myelofibrosis. Curr Treat Options Oncol. 2023;24:1–15. doi:10.1007/s11864-022-01044-1
51. Waibel M, Solomon VS, Knight DA, et al. Combined targeting of JAK2 and Bcl-2/Bcl-xL to cure mutant JAK2-driven malignancies and overcome acquired resistance to JAK2 inhibitors. Cell Rep. 2013;5(4):1047–1059. doi:10.1016/j.celrep.2013.10.038
52. Lu M, Wang J, Li Y, et al. Treatment with the Bcl-xL inhibitor ABT-737 in combination with interferon α specifically targets JAK2V617F-positive polycythemia vera hematopoietic progenitor cells. Blood. 2010;116(20):4284–4287. doi:10.1182/blood-2010-04-279125
53. Pemmaraju N, Garcia JS, Potluri J, et al. Addition of navitoclax to ongoing ruxolitinib treatment in patients with myelofibrosis (REFINE): a post-hoc analysis of molecular biomarkers in a phase 2 study. Lancet Haematol. 2022;9(6):e434–e444. doi:10.1016/S2352-3026(22)00116-8
54. Pullarkat V, Cruz-Chacon A, Gangatharan S, et al. P1070: navitoclax monotherapy in patients with myelofibrosis previously treated with JAK-2 inhibitors: safety and tolerability. HemaSphere. 2022;6:960–961. doi:10.1097/01.HS9.0000847148.78233.c8
55. Passamonti F, Foran JM, Tandra A, et al. The combination of navitoclax and ruxolitinib in JAK inhibitor-naïve patients with myelofibrosis mediates responses suggestive of disease modification. Blood. 2022;140(Supplement 1):583–585. doi:10.1182/blood-2022-157949
56. Suragani RN, Cadena SM, Cawley SM, et al. Transforming growth factor-β superfamily ligand trap ACE-536 corrects anemia by promoting late-stage erythropoiesis. Nat Med. 2014;20(4):408–414. doi:10.1038/nm.3512
57. Gerds AT, Vannucchi AM, Passamonti F, et al. A phase 2 study of luspatercept in patients with myelofibrosis-associated anemia. Blood. 2019;134:557. doi:10.1182/blood-2019-122546
58. Chen Y, Stubbs MC, Pusey M, et al. Characterization of INCB00928, a potent and selective ALK2 inhibitor for the treatment of anemia. Blood. 2020;136:52. doi:10.1182/blood-2020-136138
59. Mohan SR, Oh ST, Ali H, et al. A phase 1/2 study of INCB000928 as monotherapy or combined with Ruxolitinib (RUX) in Patients (Pts) with anemia due to Myelofibrosis (MF). Blood. 2022;140(Supplement 1):3943–3944. doi:10.1182/blood-2022-169210
60. Verstovsek S, Al-Ali HK, Mascarenhas J, et al. BOREAS: a global, phase III study of the MDM2 inhibitor navtemadlin (KRT-232) in relapsed/refractory myelofibrosis. Future Oncol. 2022;18:4059–4069. doi:10.2217/fon-2022-0901
61. Mascarenhas J, Harrison CN, Kiladjian -J-J, et al. Imetelstat in intermediate-2 or high-risk myelofibrosis refractory to JAK inhibitor: iMpactMF phase III study design. Future Oncol. 2022;18(22):2393–2402. doi:10.2217/fon-2022-0235
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.