")
Back to Journals » Research and Reports in Urology » Volume 13
Emerging Data on the Safety and Efficacy of Transurethral Water Vapour Therapy for Benign Prostatic Hyperplasia
Authors Jones P , Siena G, Hameed BMZ, Somani BK
Received 23 March 2021
Accepted for publication 30 April 2021
Published 20 May 2021 Volume 2021:13 Pages 273—282
DOI https://doi.org/10.2147/RRU.S273686
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jan Colli
Patrick Jones,1,2 Giampaolo Siena,3 BM Zeeshan Hameed,2,4 Bhaskar K Somani2,5
1Department of Urology, Haukeland University Hospital, Bergen, Norway; 2EAU Young Academic Urology Urolithiasis and Endourology Working Party, Arnhem, Netherlands; 3Department of Urology, Careggi University Hospital, Florence, Italy; 4Kasturba Medical College Manipal, Manipal Academy of Higher Education, Manipal, Karnataka, India; 5Department of Urology, University Hospital Southampton, Southampton, UK
Correspondence: Patrick Jones
Department of Urology, Haukeland University Hospital, Bergen, Norway
Tel/Fax +447950050667
Email [email protected]
Abstract: Benign prostate disease is a disease of prevalence and over 25% of men affected by bothersome lower urinary tract symptoms (LUTS) as a result of it will require surgical intervention during their lifetime. While transurethral resection of the prostate (TURP) has served as the cornerstone treatment for many years, there now exist a multitude of minimally invasive alternatives including the Rezum system. The latter is a novel form of transurethral water vapour therapy, which is attracting increasing attention. It utilizes convective water vapour energy (WAVE) and thereby radiofrequency (RF) in order to generate heat energy. Early studies have demonstrated promising results. To date there have been 12 studies published on Rezum, however only one randomized trial. This review offers an overview and evaluation of this emerging evidence.
Keywords: Rezum, BPH, prostate, benign prostatic hyperplasia, minimally invasive surgery
Introduction
Benign prostatic hyperplasia (BPH) is a disease of prevalence and its natural history renders 25% of men to be affected by bothersome lower urinary tract symptoms (LUTS) caused by bladder outflow obstruction during their lifetime.1,2 The sequelae are far reaching and can significantly affect their quality of life.3 In cases refractory to conservative and medical treatments, surgery represents the next step in the management pathway. While transurethral resection of the prostate (TURP) has served as the cornerstone treatment for many years, there now exist a multitude of minimally invasive alternatives, which achieve effect through a range of mechanisms of action.4 For example, prostatic urethral lift and iTIND rely principally on mechanical decompression whereas prostate artery embolization (PAE) induces glandular ischemia.5,6,7 In order to achieve general uptake, new treatment modalities are required to demonstrate sufficient improvement across both objective and subjective outcome measures as well as maintaining a strong safety profile. Improvements should be durable and sustained at long term follow up while striving to adhere to a favorable financial model.
The Rezum system is a novel device, which utilizes convective water vapour energy (WAVE) and thereby radiofrequency (RF) in order to generate heat energy.8 Large volumes of stored energy (540 cal/mL H2O) are released when the water vapour (approx. 103°C) makes contact with the tissue and subsequent condensation occurs. Cell necrosis ensues as a result of temperature change. Through use of these steam injections, transurethral delivery of this energy can be targeted with precision and overlapping lesions are formed in the desired anatomical location. While still relatively new, early studies have demonstrated promising results and it obtained approval by the US Food and Drug Administration (FDA) in 2015 and the National Institute for Health and Care Excellence (NICE) guidelines in 2018.9 While there has been an increasing amount of emerging data on Rezum, critical evaluation of its safety and efficacy remains under-reported. This review therefore aimed to deliver such an appraisal and provide an overview of its current status.
Methods
A comprehensive review of world literature was performed in order to find original studies on Rezum. Bibliographic databases searched included Medline, Google Scholar, Cochrane database and center for trials. All study types were considered eligible as long as full text articles were available in English language, and the search was completed in January 2021.
Rezum
To date there have been 12 studies published on Rezum, which have included 1391 patients (mean age 68.7 years, range: 46–90) (Tables 1 and 2).9–20 Over half of these studies (n=7) have been published in the past 2 years, reflecting the increasing interest and uptake of this novel intervention. There has only been one randomized study and the remainder represent cohort studies (5x retrospective and 6 x prospective). Seven of these studies were performed in a multi-center setting.10–12,14,17,18 The randomized study used a sham procedure as a comparator.14 This consisted of rigid cystoscopy with simulated active treatment sound effects. Across the studies, the mean prostate volume was 61.6 cc (range: 19.5–183). The mean number of steam injections administered was 6.5 (range: 4–10) in the seven studies, which reported this.9,13,14,18,19 Duration of follow up ranged from 1 week (proof of concept study) to 5 years.9,14 Selection criteria for studies are summarized in Table 3.
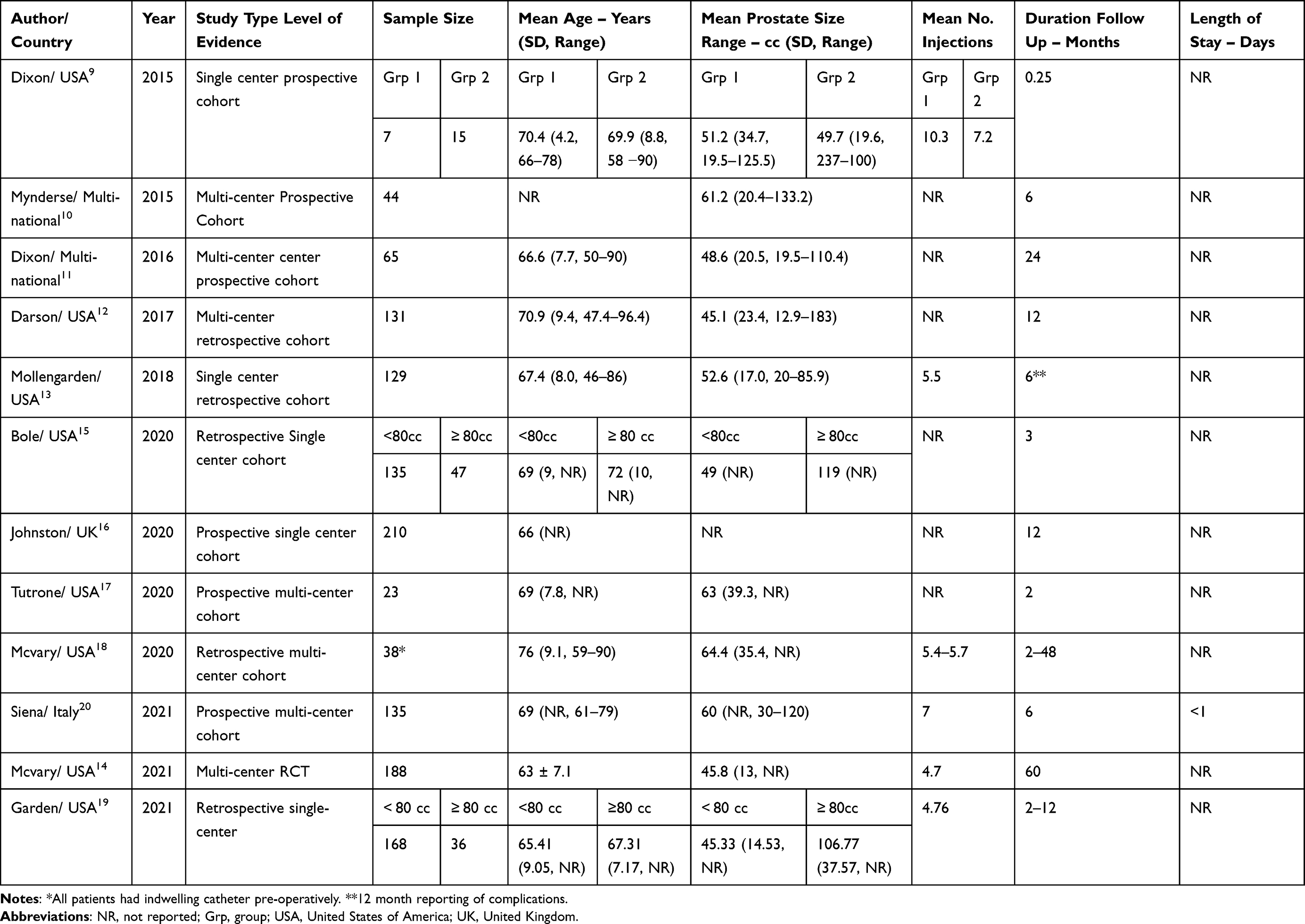 |
Table 1 Baseline Demographics of the Included Studies |
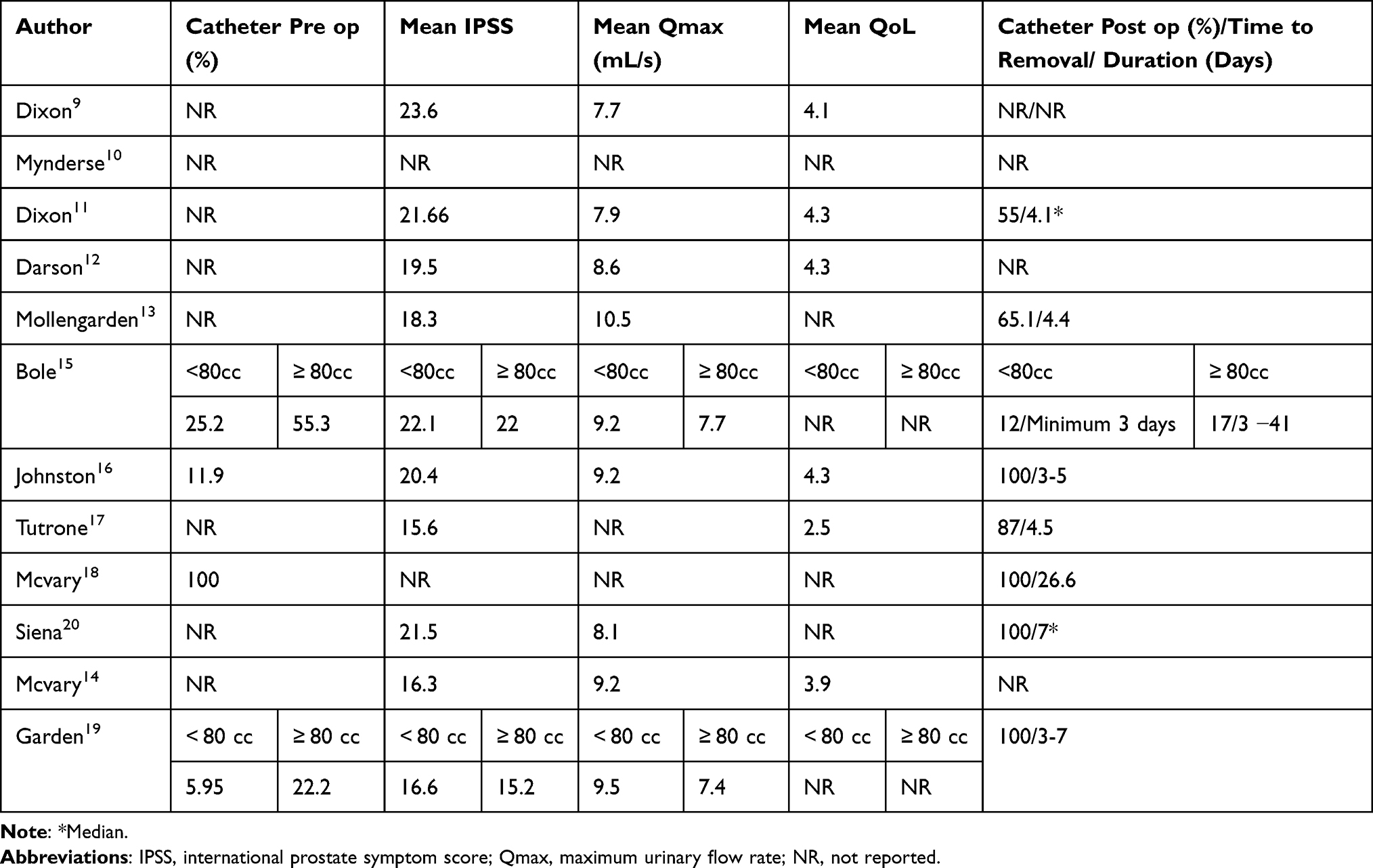 |
Table 2 Additional Characteristics |
 |
Table 3 Selection Criteria of Included Studies |
Efficacy
In 2020, a Cochrane review was published on this technology, however it only considered data from one study, the randomized trial.14,21 The heterogeneity of parameters reported among published studies and wide range of follow up periods preclude formal meta-analysis in previous and current study. However, consistent improvements in clinical outcomes after Rezum can be observed across all the studies.
Eight of the studies reported on change in international prostate symptom score (IPSS) and each of these revealed improvements (Table 4).11–16,19,20 In their prospective single center study of 210 patients, Johnston et al recorded mean improvement in IPSS of 78.5% after 12 months (20.4 vs 4.3, p<0.001) and mean improvement of 97.5% in maximum urinary flow rate (Qmax) of 97.5% (9.2 vs 18.2 mL/s, p<0.001) over the same time period.16 These changes represent the most pronounced across all reported studies. Other studies have recorded at least 30% improvement in IPSS and McVary et al reported a mean change of −48% at the five year follow up assessment (<0.001).14 This improvement had been stable since the 12 month follow up assessment when the mean improvement recorded was 52.2% (p<0.001). This was mirrored in the results for Qmax, where mean improvement was 49% (9.9 vs 14, p<0.001) after five years. Quality of life (QoL) data were reported by only four studies, however these all demonstrated improvement.11,12,14,16 Mean change in QoL scores ranged from 37.8% to 72%. Again, in the five year follow up study of the randomized trial, the result had plateaued and remained largely similar since the initial 12-month assessment (45% improvement).14 Dixon et al also reported a statistically significant mean improvement in QoL at two year follow up (4.4 vs 1.8, p<0.001).11
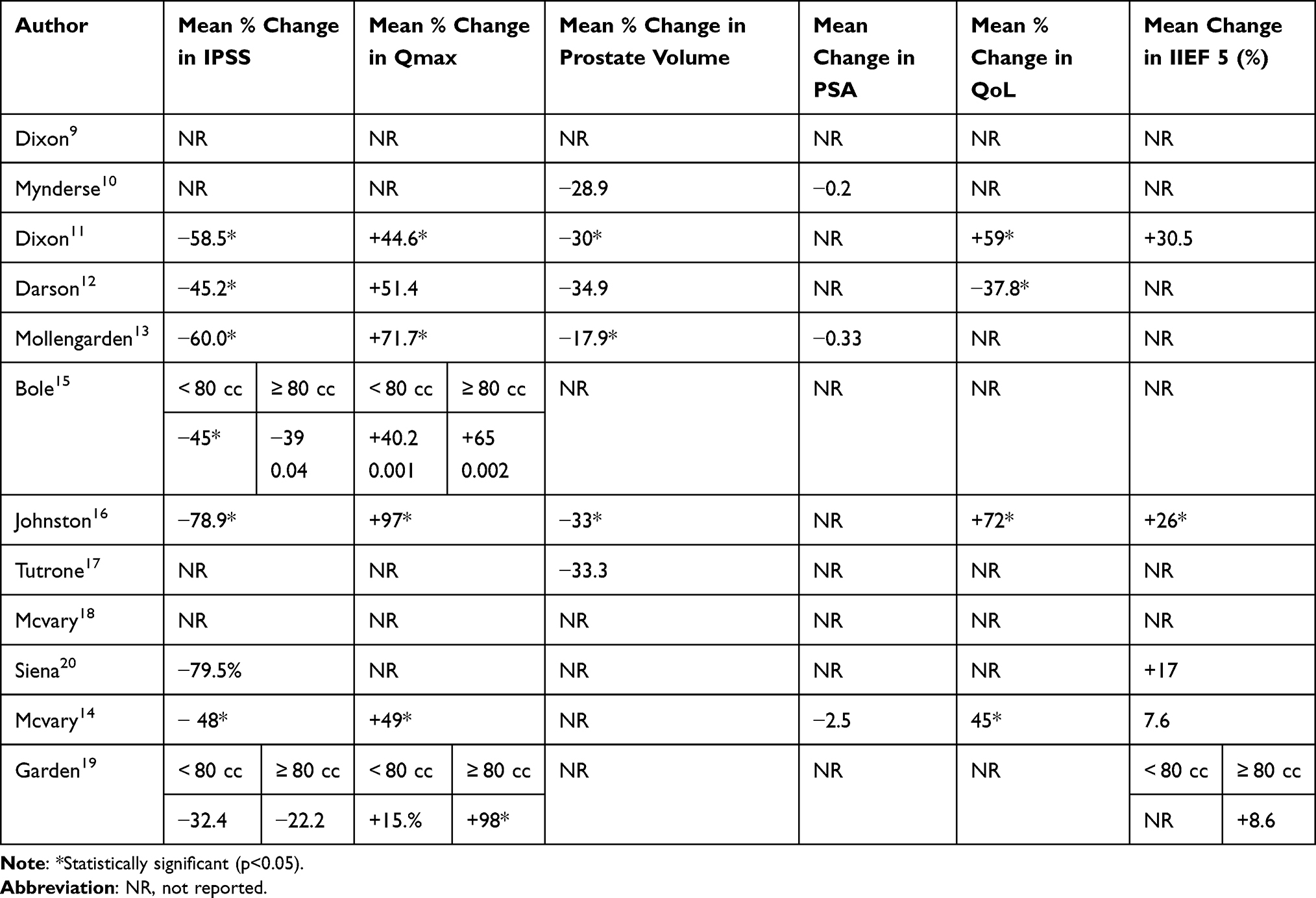 |
Table 4 Clinical Outcomes of the Included Studies |
As well as the advantage of Rezum in treating patients with an obstructing median lobe, this intervention may offer the potential to become a standard treatment for patients with large prostate burden. While Rezum is acknowledged in the European Association of Urology (EAU) guidelines as a new intervention in the surgical management of BPH, it has yet to receive any formal recommendation.2 However, NICE recommends its application only in the setting of prostate size between 30–80cc.8 Two studies specifically analyzed the feasibility of Rezum in larger prostate size (>80cc).15,19 Bole et al reported statistically significant improvements in IPSS (22 vs 13.4, p=0.04), post void residual (PVR) (305 vs 149 mL, p=0.05), and Qmax (7.7 vs 12.7mL/s, p=0.002) in a patient group (mean prostate volume 119cc).15 Furthermore, 55.3% were catheter dependent pre-operatively. The application of Rezum in catheter dependent patients with complete urinary retention would be a further advantage. In 2020, McVary et al reported findings from a registry of patients (n=38) with this clinical profile.18 73% of these patients achieved a catheter free status and the median length of time to achieve this was 26 days (range: 4–65) after the procedure.
Safety
The most common low-grade complications (Clavien <2) associated with this intervention are urinary tract infection (UTI), urinary retention, hematuria and new onset bothersome lower urinary tract symptoms such as frequency and urgency. As demonstrated in Table 5, there is a range of these reported low-grade complications. Garden et al reported that hematuria, urgency, and frequency occurred in 39.29%, 30.36%, and 30.95% of patients respectively.19 In the randomized trial performed by McVary et al, this same group of bothersome symptoms was also captured, albeit with lower rates.14 In contrast, in other studies no such bothersome symptoms were reported. Given that many patients do experience such self-resolving bothersome symptoms of this nature, similar to the post PAE syndrome, these symptoms may not have been captured in some studies as patients presented to primary care or their symptoms resolved in time.22 Most studies recorded rates of UTI between 10–20%. Similar to other adverse events such as dysuria and hematuria, a main reason for this is considered to be due to both the catheter being left in situ 5–7 days after the procedure and the necrotic tissue produced after the procedure. Increasingly therefore, a short course of antibiotics is recommended as part of the post intervention care plan. Rates of urinary retention varied from zero cases in some studies to as high as 33.8%.11 Given the limited number of studies which have been performed using Rezum, this may be part of the evolution of patient selection for this procedure as the optimal candidate is being determined as well as the expected learning curve for centers newly adopting the technique. Inclusion criteria also varied across the studies, which also likely contributed to this. For example, Darson et al left patient selection to the discretion of the clinician whereas stricter measures were followed in other studies.12
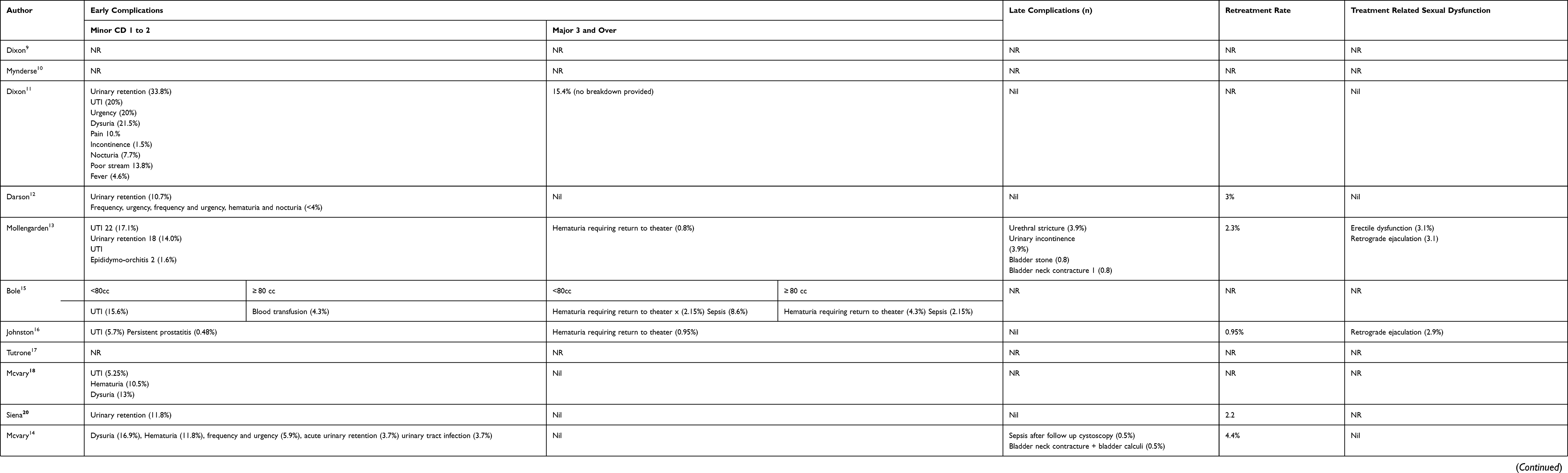 |
Table 5 Complications (Early, Late) Reported in the Studies Including Sexual Dysfunction and Retreatment Rates |
Rates of serious adverse events were low across all the studies and these were all related to either sepsis or hematuria requiring return to theater to achieve endoscopic control. Late complications have been rare and include bladder neck contracture as reported in two studies.13,14 No study recorded late complication rate above 5%. No deaths were recorded across any of the studies.
Re-treatment rates also appear low although only a single study has achieved follow up to five years where the rate was 4.4%.14 The range of re-treatment rates reported at 12 month follow up was 0.95% to 8.33%. In contrast, the re-treatment rate at five years reported in the LIFT study was 13.6%.24 Tolerability and patient satisfaction appear favorable. Johnston et al reported that 91% of patients would be prepared to go through repeat Rezum procedure if ultimately required.16
Sexual Dysfunction
Six studies reported on incidence of de-novo sexual dysfunction occurring post treatment.11–14,16,19 Three of these reported no new cases.11,12,14 New onset erectile dysfunction (3.1%) was reported by Mollengarden et al and only in one other study.13,19 Two studies revealed cases of retrograde ejaculation, however, rates were noticeably low (<6%).13,16 Gupta et al compared outcomes of randomized trial 3 year follow up data with the Medical Therapy of Prostatic Symptoms (MTOPS) study (n=1209) in order to determine if either pharmacotherapy or a single surgical intervention (Rezum) caused more deterioration in sexual symptoms among sexually active men.25 Their findings concluded that both finasteride and combination therapy resulted in significant reduction in sexual desire as well as worsening of both erectile and ejaculatory function. In contrast, Rezum was not associated with negative impact on any of these domains. Four studies included a validated tool, International Index of Erectile Function (IIEF-5) as part of evaluation of treatment impact.11,14,16,19 All of them reported improvements, which ranged from 7.6–30.5%.
Morphological Changes
In 2015, Dixon et al reported findings from an early, proof of concept study and performed gadolinium enhanced magnetic resonance imaging (MRI) at one week post surgery.9 The mean volume of coalesced lesion was 9.6cm3 and the largest recorded in the series was 35.1 cm3. More recently, Mynderse et al enrolled 45 patients to also undergo regular imaging surveillance with MRI.10 Early imaging at one week post procedure revealed similar results. The mean volume of the coalesced lesion created was 8.2 cm3 (0.5–24.0 cm3). At 6 months follow up, the mean reduction in volume of prostate was −28.9% and −38% in the transition zone. Three further studies have reported greater than 30% reduction in prostate volume.12,16,17 The lack of specimen retrieval does represent a disadvantage of Rezum and as a consequence no histopathological analysis is possible. Little is known currently regarding interpretation of PSA values post Rezum treatment in regard to evaluation for possible prostate cancer. There is also a lack of data on impact of Rezum treatment on later surgery for both BPH and prostate cancer.
Cost
None of the included studies provided information regarding cost of Rezum. However, a recent cost effectiveness analysis by Ulchacker et al offers an early insight into the economic status of this device, which is favorable.26 The cost for Rezum was given as $2489 (US), which includes cost for pre-operative assessment with cystoscopy, transrectal ultrasound (TRUS) and urodynamic study (UDS) as well as post-operative assessment and one year follow up appointment. This was cheaper than for TURP ($4821), although their evaluation determined inferiority of clinical outcomes achieved with Rezum compared to TURP. However, when stratified according to outcomes based on cost, these two interventions were aligned and were the most cost-effective treatments compared to both branded and generic combination therapy (5α-reductase inhibitor + α-blocker), urolift and greenlight procedure. Cost modeling data reported by NICE, estimate that over a four-year period, Rezum is able to provide savings of £569 and £651 compared to TURP and holmium laser enucleation of the prostate (HoLEP) respectively.8 It is difficult to know if these projected savings are realistic due to expert evaluations largely relying on the randomized trial data as it is the only study to achieve four year follow up to date. The key driver for this cost saving when compared with such other standard BPH treatments, relies on the provision of Rezum as a day case surgery procedure. Length of stay and therefore determination of success at performing Rezum as a day case procedure was poorly reported across the studies and therefore it is difficult to truly evaluate the feasibility of establishing a day case service. A fundamental component of why it can be done as an ambulatory procedure is the lack of general anesthetic and even intravenous sedation required. However, outside of the trial context, most units appeared to carry out Rezum under general anesthetic, at least in the early period. Therefore, there remains a lack of real-world data providing evidence of this nature.
Limitations and Further Limitations
While there has been a recent surge in studies on Rezum, which all deliver promising early results, there is a lack of randomized trial data. Future studies, which compare against other standard BPH surgeries are warranted as at present only one sham study exists in world literature. The Comparing uroLift Experience Against Rezum (CLEAR) study, a randomized trial, is currently ongoing. Caution should also be noted when interpreting these early results as in the setting of both pilot studies and clinical trials, inclusion/exclusion criteria can be very strict when in reality the demographics of patients who present in clinic and require surgical intervention for BPH are typically much broader. Standardized evaluation parameters will aid future evaluation of Rezum’s efficacy. To date, no studies have formally assessed the learning curve for the procedure. However, expert opinion (Level V evidence) has highlighted that it is straight forward for those with sufficient endoscopic experience.
Conclusion
Current evidence regarding Rezum demonstrates that it holds a strong efficacy and safety profile. While low grade side effects such as self-resolving bothersome LUTS appear to be present in up to one third of patients, serious adverse events seldom appear. Lack of or minimal de-novo sexual dysfunction appears to be consistently maintained across all evidence available and represents a further advantage of this procedure. Future studies with intervention comparators and longer follow up will provide important data to help delineate its formal position in the treatment algorithm as well as establish the patient profile most suitable for this particular surgery.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Speakman M, Kirby R, Doyle S, Ioannou C. Burden of male lower urinary tract symptoms (LUTS) suggestive of benign prostatic hyperplasia (BPH) - focus on the UK. BJU Int. 2015;115(4):508–519. PMID: 24656222. doi:10.1111/bju.12745
2. Lee SWH, Chan EMC, Lai YK. The global burden of lower urinary tract symptoms suggestive of benign prostatic hyperplasia: a systematic review and meta-analysis. Sci Rep. 2017. 7(1):7984. doi:10.1038/s41598-017-06628-8. PMID: 28801563. PMCID: PMC5554261.
3. Pinto JD, He HG, Chan SW, Wang W. Health-related quality of life and psychological well-being in men with benign prostatic hyperplasia: an integrative review. Jpn J Nurs Sci. 2016;13(3):309–323. PMID: 26782969. doi:10.1111/jjns.12115
4. Christidis D, McGrath S, Perera M, Manning T, Bolton D, Lawrentschuk N. Minimally invasive surgical therapies for benign prostatic hypertrophy: the rise in minimally invasive surgical therapies. Prostate Int. 2017. 2:41–46. doi:10.1016/j.prnil.2017.01.007. PMID: 28593165. PMCID: PMC5448728.
5. Jones P, Rai BP, Aboumarzouk O, Somani BK. UroLift: a new minimally-invasive treatment for benign prostatic hyperplasia. Ther Adv Urol. 2016. 6:372–376. doi:10.1177/1756287216671497. PMID: 27904652. PMCID: PMC5117169.
6. Carnevale FC, Iscaife A, Yoshinaga EM, Moreira AM, Antunes AA, Srougi M. Transurethral Resection of the Prostate (TURP) Versus Original and PErFecTED Prostate Artery Embolization (PAE) Due to Benign Prostatic Hyperplasia (BPH): preliminary results of a single center, prospective, urodynamic-controlled analysis. Cardiovasc Intervent Radiol. 2016;39(1):44–52. PMID: 26506952. doi:10.1007/s00270-015-1202-4
7. Jones P, Rai BP, Nair R, Somani BK. Current status of prostate artery embolization for lower urinary tract symptoms: review of world literature. Urology. 2015;86(4):676–681. [PMID: 26238328.]. doi:10.1016/j.urology.2015.05.011
8. Westwood J, Geraghty R, Jones P, Rai BP, Somani BK. Rezum: a new transurethral water vapour therapy for benign prostatic hyperplasia. Ther Adv Urol. 2018. 10(11):327–333. doi:10.1177/1756287218793084. PMID: 30344644. PMCID: PMC6180381.
9. Rezum for treating lower urinary tract symptoms secondary to benign prostatic hyperplasia. Medical technologies guidance [MTG49]. Available from: https://www.nice.org.uk/guidance/mtg49.
10. Dixon CM, Rijo Cedano E, Mynderse LA, Larson TR. Transurethral convective water vapor as a treatment for lower urinary tract symptomatology due to benign prostatic hyperplasia using the Rezūm(®) system: evaluation of acute ablative capabilities in the human prostate. Res Rep Urol. 2015;7:13–18. doi:10.2147/RRU.S74040. PMID: 25674555. PMCID: PMC4321608.
11. Mynderse LA, Hanson D, Robb RA, et al. Rezūm system water vapor treatment for lower urinary tract symptoms/benign prostatic hyperplasia: validation of convective thermal energy transfer and characterization with magnetic resonance imaging and 3-dimensional renderings. Urology. 2015;86(1):122–127. PMID: 25987496. doi:10.1016/j.urology.2015.03.021
12. Dixon CM, Cedano ER, Pacik D, et al. Two-year results after convective radiofrequency water vapor thermal therapy of symptomatic benign prostatic hyperplasia. Res Rep Urol. 2016;8:207–216. doi:10.2147/RRU.S119596
13. Darson MF, Alexander EE, Schifman ZJ, et al. Procedural techniques and multicenter postmarket experience using minimally invasive convective radiofrequency thermal therapy with Rezūm system for treatment of lower urinary tract symptoms due to benign prostatic hyperplasia. Res Reports Urol. 2017;9:159–168. doi:10.2147/RRU.S143679
14. Mollengarden D, Goldberg K, Wong D, Roehrborn C. Convective radiofrequency water vapor thermal therapy for benign prostatic hyperplasia: a single office experience. Prostate Cancer Prostatic Dis. 2018;21(3):379–385. PMID: 29282358. doi:10.1038/s41391-017-0022-9
15. McVary KT, Gittelman MC, Goldberg KA, et al. Final 5-year outcomes of the multicenter randomized sham-controlled trial of rezūm water vapor thermal therapy for treatment of moderate-to-severe lower urinary tract symptoms secondary to benign prostatic hyperplasia. J Urol. 2021;19. doi:10.1097/JU.0000000000001778. PMID: 33872051
16. Bole R, Gopalakrishna A, Kuang R, et al. Comparative postoperative outcomes of rezūm prostate ablation in patients with large versus small glands. J Endourol. 2020;34(7):778–781. PMID: 32408768. doi:10.1089/end.2020.0177
17. Johnston MJ, Noureldin M, Abdelmotagly Y, et al. Rezum water vapour therapy: promising early outcomes from the first UK series. BJU Int. 2020;126(5):557–558. PMID: 32777175. doi:10.1111/bju.15203
18. Tutrone RF, Schiff W. Early patient experience following treatment with the UroLift prostatic urethral lift and Rezum steam injection. Can J Urol. 2020;27(3):10213–10219. PMID: 32544043.
19. McVary KT, Holland B, Beahrs JR. Water vapor thermal therapy to alleviate catheter-dependent urinary retention secondary to benign prostatic hyperplasia. Prostate Cancer Prostatic Dis. 2020;23(2):303–308. doi:10.1038/s41391-019-0187-5. PMID: 31740738. PMCID: PMC7237346.
20. Garden EB, Shukla D, Ravivarapu KT, et al. Rezum therapy for patients with large prostates (≥ 80 g): initial clinical experience and postoperative outcomes. World J Urol. 2021. doi:10.1007/s00345-020-03548-7
21. Siena G, Cindolo L, Ferrari G, et al. Water vapor therapy (Rezūm) for lower urinary tract symptoms related to benign prostatic hyperplasia: early results from the first Italian multicentric study. World J Urol. 2021:1–6. doi:10.1007/s00345-021-03642-4. PMID: 33787986. PMCID: PMC8010783.
22. Kang TW, Jung JH, Hwang EC, Borofsky M, Kim MH, Dahm P. Convective radiofrequency water vapour thermal therapy for lower urinary tract symptoms in men with benign prostatic hyperplasia. Cochrane Database Syst Rev. 2020. 3(3):CD013251. doi:10.1002/14651858.CD013251.pub2. PMID: 32212174. PMCID: PMC7093307.
23. Gratzke C, Bachmann A, Descazeaud A, et al. EAU guidelines on the assessment of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. Eur Urol. 2015;67:1099–1109. doi:10.1016/j.eururo.2014.12.038
24. Roehrborn CG, Barkin J, Gange SN, et al. Five year results of the prospective randomized controlled prostatic urethral L.I.F.T. study. Can J Urol. 2017;24(3):8802–8813. PMID: 28646935.
25. Gupta N, Rogers T, Holland B, Helo S, Dynda D, McVary KT. Three-year treatment outcomes of water vapor thermal therapy compared to doxazosin, finasteride and combination drug therapy in men with benign prostatic hyperplasia: cohort Data from the MTOPS Trial. J Urol. 2018;200(2):405–413. PMID: 29499208. doi:10.1016/j.juro.2018.02.3088
26. Ulchaker JC, Martinson MS. Cost-effectiveness analysis of six therapies for the treatment of lower urinary tract symptoms due to benign prostatic hyperplasia. Clinicoecon Outcomes Res. 2017;10:29–43. doi:10.2147/CEOR.S148195. PMID: 29343977. PMCID: PMC5749396.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.