Back to Journals » Substance Abuse and Rehabilitation » Volume 17
Emergency Department Peer Recovery Support Services for Individuals with Substance Use Disorders: A Systematic Review of Comparative Studies
Authors Chardavoyne PC, Bormann NL ![]() , Smartt AB
, Smartt AB ![]() , Nickels ZC, Gerberi D
, Nickels ZC, Gerberi D ![]() , Arndt S, Oesterle TS
, Arndt S, Oesterle TS ![]()
Received 29 April 2026
Accepted for publication 17 June 2026
Published 19 June 2026 Volume 2026:17 609242
DOI https://doi.org/10.2147/SAR.S609242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Rajendra Badgaiyan
Paige C Chardavoyne,1 Nicholas L Bormann,1 Addison B Smartt,2 Zachary C Nickels,3 Dana Gerberi,4 Stephan Arndt,5,6 Tyler S Oesterle1
1Department of Psychiatry and Psychology, Mayo Clinic, Rochester, MN, USA; 2Mayo Clinic Alix School of Medicine, Mayo Clinic, Phoenix, AZ, USA; 3Department of Emergency Medicine, Mayo Clinic, Rochester, MN, USA; 4Mayo Clinic Libraries, Mayo Clinic, Rochester, MN, USA; 5Department of Psychiatry, Carver College of Medicine, University of Iowa, Iowa City, IA, USA; 6Department of Biostatistics, College of Public Health, University of Iowa, Iowa City, IA, USA
Correspondence: Nicholas L Bormann, Department of Psychiatry and Psychology, Mayo Clinic, 200 First St SW, Rochester, MN, 55905, USA, Email [email protected]
Abstract: Individuals with substance use disorders (SUDs) access care through emergency departments (EDs) more frequently than the general population, representing a critical opportunity for addiction treatment linkage. Peer recovery support services (PRSS) utilize individuals with lived recovery experience to provide peer support for those struggling with addiction. This service may be particularly helpful in the ED, where prior negative experiences can erode patient trust and care often involves extended waiting periods during which motivation can fluctuate. PRSS may enhance engagement in this setting by offering relationship-based support from someone who patients can identify with and who can provide practical information on service navigation. We conducted a systematic review of comparative studies evaluating ED-based PRSS for individuals with SUDs versus a non-PRSS comparator (eg, usual care). A medical librarian searched the literature through 8/2025; 1,801 citations were retrieved, 708 duplicates were removed, 1,093 records were screened, and 127 studies underwent full-text review. Nine studies published between 2011 and 2025, representing 14,883 unique individuals, met inclusion criteria. Most (seven) were considered moderate regarding global risk of bias. Types of substance and outcomes varied by study; opioids (n=7) were the most commonly evaluated substance, while overdose (n=6), all-cause hospital return (n=3), all-cause mortality (n=3), and SUD treatment linkage (n=3) were the most commonly evaluated outcomes. The findings were mixed; PRSS has not yet demonstrated clear superiority over non-PRSS comparators, though this may evolve as research continues. Consisting solely of quantitative studies, the present review fails to capture the qualitative patient experience of working with a peer, which may have been a positive, recovery-promoting encounter, even in the absence of statistical significance. While ED-based PRSS interventions are individualized services that promote connection and may increase patient comfort, the current evidence base remains heterogeneous, limited in comparative studies, and subject to bias.
Keywords: peer recovery support, substance use outcomes, patient engagement, service navigation
Introduction
Substance use disorders (SUDs) are highly prevalent in the United States (US), with 2024 national survey data suggesting that up to 17% of the population met SUD criteria in the past year.1 These individuals often lack an established primary care provider and have increased utilization of emergency department (ED) services.2 In 2024 alone, there were over 8 million ED visits related to substance use in the United States.3 Notably, individuals with SUDs demonstrate higher rates of repeat emergency care than those without SUDs.4 One study comparing repeat ED admissions for patients with and without SUDs found that individuals with SUDs had 32% higher odds of ED re-presentation within 72 hours.4 Unfortunately, this higher visit volume has not translated into increased addiction treatment engagement. Presently, approximately one-fifth of individuals in need of SUD treatment receive it, despite an increased emphasis on screening, brief intervention, and referral pathways.1,5 Therefore, while the ED represents a critical location to identify individuals with SUDs and connect them to treatment, successful implementation in this setting has been challenging.
Barriers to SUD treatment access exist at the structural, societal, and individual levels. A lack of options in one’s immediate area, insurance coverage issues, limited social support, fears or negative beliefs about treatment, and stigma may all contribute.6 In the ED, these barriers can be amplified given an increased occurrence of negative attitudes towards patients with SUDs and clinician time constraints.7 Incorporating individuals with lived addiction experience who are in recovery into healthcare teams represents an important patient-centered approach to addressing these barriers and improving care experiences.
Peer recovery support services (PRSS) are a bidirectional, relationship-based intervention that utilizes peers with lived experience in recovery to assist others in engaging with treatment and sustaining recovery through self-disclosure and sharing their story.8 Key features of PRSS include meeting individuals where they are at, strengthening motivation for change, accompanying individuals to treatment, and enhancing the support system.9 PRSS are commonly facilitated through state initiatives, hospital programs, and community organizations. Individual states in the US determine the required certification and training for peers providing PRSS, which results in heterogeneity amongst peers.10 In addition to peer training variation, additional potential peer-level threats to the effectiveness of PRSS include difficulties with boundaries, biases based on peer lived experiences, and peer burnout.11,12 There are also potential patient-level threats to the effectiveness of PRSS including comorbid non-substance use-related mental health diagnoses. The literature suggests that individuals with a SUD and a co-occurring mental health diagnosis are at elevated risk of poor outcomes, including clinical and utilization outcomes, following various treatment interventions.13
Despite potential challenges, there are several reasons why PRSS in the ED may be particularly well suited for patients with SUDs. The ED setting can be a crisis window where having a supportive peer may be particularly helpful. In the ED, patients with SUDs may encounter stigma from healthcare providers and may feel distrust towards the healthcare system.14 Acutely, if patients are agreeable to interventions in the ED, perhaps through the encouragement of a peer, this may increase their subsequent treatment engagement.15 Further, peers can provide additional interventions, including overdose prevention education and naloxone kit distribution.16,17 This places peers as part of broader overdose prevention strategies, which can begin in the ED.
Despite appearing to be an appropriate fit, in the ED compared to other treatment settings, it has been more challenging to demonstrate benefit from PRSS for patients with SUDs.18 In their 2025 systematic review, Eddie et al described outcomes for patients with SUDs across multiple care settings Globally, they found that PRSS improved treatment linkage and engagement most strongly, with less benefit established for substance use-related outcomes (such as overdose). However, they identified the ED as the treatment setting showing the least promise for PRSS.18
ED specific distinctions may help explain this finding. The ED emphasizes acute care rather than longitudinal management, which may complicate comparisons with long-term outpatient settings. Patients also present to the ED in various medical states, including intoxication, withdrawal, or with other medical illnesses, which may limit their ability to engage with PRSS at that time. Finally, PRSS implementation across EDs can be very diverse, limiting the ability to pool effects.
Given these fundamental differences and ED-specific nuances, evaluating PRSS for patients with SUDs in the ED warrants a dedicated systematic review. This systematic review evaluates the effectiveness of ED-based PRSS, with a focus on comparative studies to assess whether these interventions improve clinical and healthcare-utilization outcomes for patients with SUDs and, where findings are mixed, to identify implementation factors that may explain observed variability.
Materials and Methods
The literature was searched by a medical librarian for the concepts of ED, substance abuse, and peer support. Search strategies were created using a combination of keywords and standardized index terms. Searches were run on August 13, 2025 in EBSCO CINAHL (1963+), Ovid Cochrane Central Register of Controlled Trials (1991+), Ovid Embase (1974+, including records from ClinicalTrials.gov), Ovid Medline (1946+ including epub ahead of print, in-process and other non-indexed citations), Ovid PsycINFO (1806+), and Web of Science Core Collection (Science Citation Index Expanded 1975+ and Emerging Sources Citation Index 2015+). After limiting results to English language, a total of 1,801 citations were retrieved. Deduplication was performed automatically in Covidence leaving 1,126 citations for screening. Full search strategies are provided in the Supplemental File. Additional, post-search references were used for context and not considered for inclusion in the systematic review.
Eligibility Criteria
Studies that involved PRSS, defined as an intervention from an individual with lived experience with substance use recovery whose role was to provide support, motivation, and treatment linkage, delivered in the ED for patients using one or more substances were explored. Study participants of all demographics were included. Although studies with participants of any age were evaluated, those investigating exclusively pediatric patients (age<18 years) were ultimately excluded due to differences between adults and children in approaching addiction treatment (Figure 1). Further, publications with any type of comparison or control group were assessed; however, due to the desire to include the highest-level studies in the present review, studies without a control group reporting patient-level outcomes were ultimately excluded. Three study team members (PCC, ABS, and ZCN) completed abstract screening while two study team members (PCC and NLB) reviewed full text for inclusion. At all stages, disagreements were discussed with TSO being the final arbitrator.
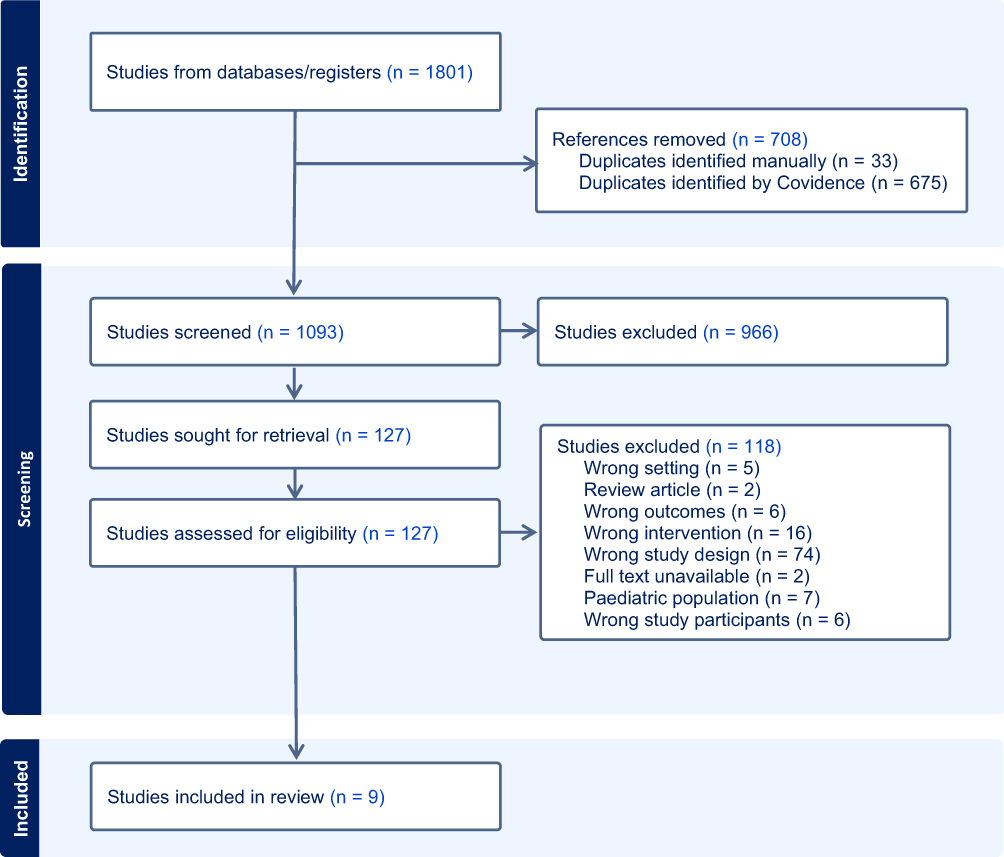 |
Figure 1 PRISMA diagram. |
Study Evaluation
Studies were evaluated for risk of bias using the Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for Quantitative Studies.19,20 The first six categories of this tool (selection bias, study design, confounders, blinding, data collection methods, and withdrawals and drop-outs) were assessed for each study. This resulted in a rating (weak, moderate, or strong) for each of the six domains and an overall rating (weak, moderate, or strong).
Data Synthesis
A spreadsheet containing the headings included in Table 1 was created by PCC and sent to ABS and ZCN. Data from the nine included studies was independently extracted in parallel by PCC and either ABS or ZCN. Once completed, PCC compared the extracted data and verified the findings with the original research study. TSO was available to resolve any disagreements as the final arbitrator.
Reported outcomes for each of the nine studies were extracted. The four outcomes with the clearest overlap across the studies were selected for further analysis. Due to the limited number of studies and study heterogeneity regarding aspects such as study design, intervention components, comparator groups, and duration, a meta-analysis was not completed.
Results
Study Selection
The process of evaluating identified studies is outlined in Figure 1. The literature search yielded 1,801 studies, reduced to 1,093 for screening after duplicate removal. One hundred twenty-seven studies underwent full-text review. Of these, nine studies met the full inclusion criteria for the present systematic review (Table 1). The most common exclusion reasons during full-text review were wrong study design (74 studies) and wrong intervention (16 studies).
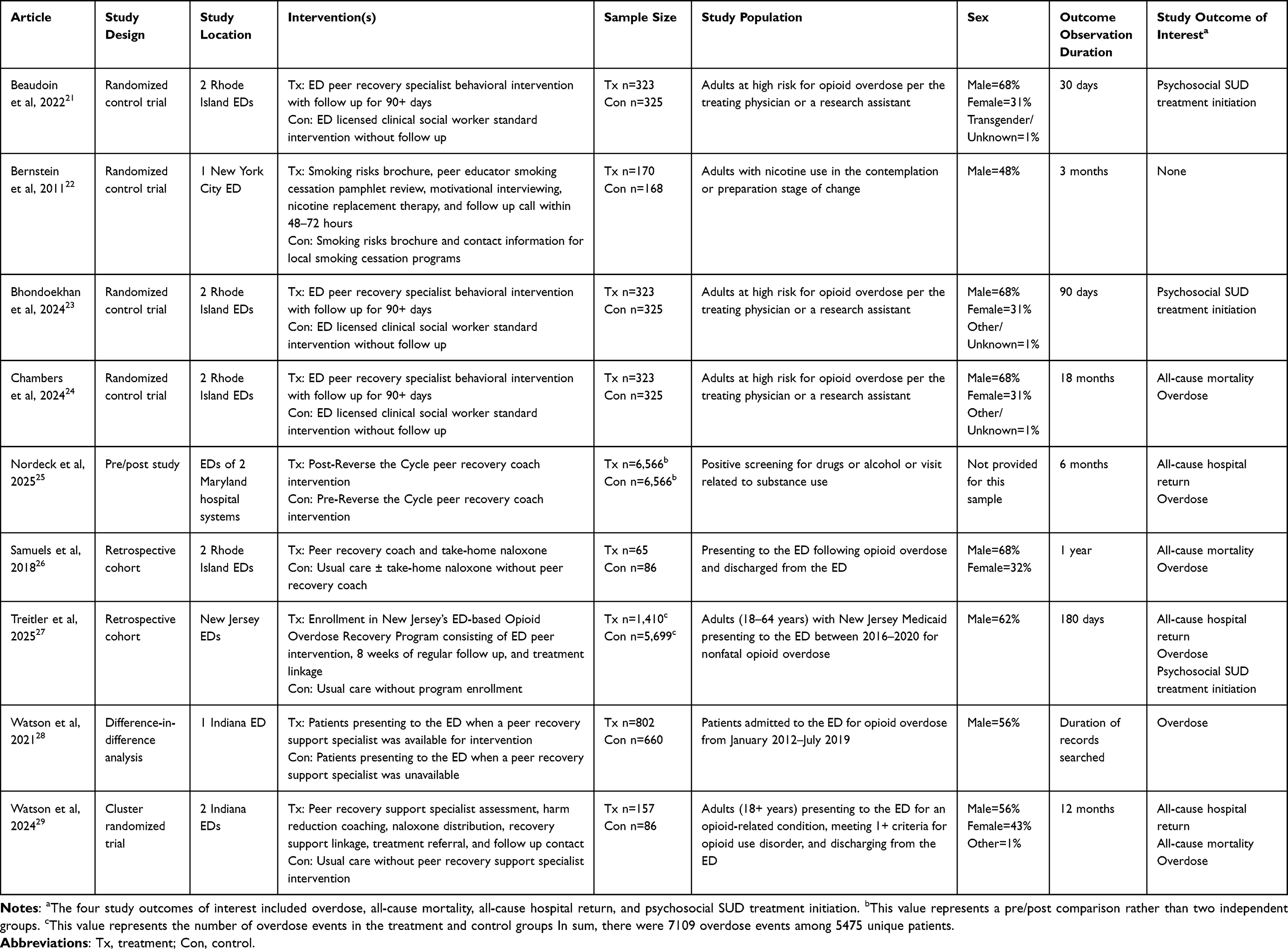 |
Table 1 Overview of Included Studies |
Each of the nine studies included ED-based PRSS at their core However, there was heterogeneity across studies with regards to specifics of the peer intervention (Table 1). In some of the studies, PRSS was part of a named intervention program, including The Mosaic Group’s Reverse the Cycle,25 the New Jersey Opioid Overdose Recovery Program,27 and Project Planned Outreach, Intervention, Naloxone, and Treatment (POINT).28,29 The nine included studies comprised four RCTs, one pre/post study, two retrospective cohort studies, one cluster-randomized trial, and one difference-in-difference analysis. These studies involved 14,883 patients. Three of the studies analyzed the same dataset.21,23,24 Patients from these three studies were counted only once. In Nordeck et al (2025), though 10,462 patients were eligible for PRSS, only 6,566 received the intervention, had non-missing data, and were included in the intervention-versus-control group analysis Therefore, the patient number of 6,566 was used in the above summation25 Finally, though 7,109 visits were included in the Treitler et al (2025) study analysis, this represented 5,475 unique patients Patients were represented more than once when they re-presented to the ED with an overdose at a time that fell outside of the 6 months before and 6 months after any prior overdose presentation27 When outcomes from the nine individual included studies were analyzed, four outcomes emerged as those with the most overlap across studies. These four were overdose, all-cause mortality, all-cause hospital return, and psychosocial SUD treatment initiation, which will be discussed in detail.
Outcome 1: Overdose
The most common overlapping outcome amongst the identified studies was overdose (6 studies).24–29 However, it should be noted that the definitions of overdose varied across studies, which may limit direct comparison between studies.
The earliest of the six included studies exploring overdose was Samuels et al (2018), who conducted a retrospective cohort study involving 151 patients presenting to the ED following an opioid overdose26 Based on the availability of services and discretion of the patient and clinician, participants were distributed into the following cohorts: i) peer recovery coach plus take-home naloxone, ii) take home naloxone without peer recovery coach, and iii) usual care Repeat overdose within one year occurred in 23.2% of individuals who received usual care (95% confidence interval (CI)=14.2–35.9), 20.0% of individuals who received a peer recovery coach plus take-home naloxone (95% CI=11.9–31.7), and 11.5% of individuals who received take-home naloxone alone (95% CI=3.6–31.0). The differences among groups were not significant.
In their 2021 study, Watson et al performed a difference-in-difference analysis of outcomes for 1,462 individuals who presented to a single ED for opioid overdose from January 2012 to July 2019 when Project POINT (an ED intervention including peer support) was (treatment) and was not (control) present28 A difference-in-difference analysis was selected as the analysis to compare outcome changes in the treatment and control groups before and after POINT was implemented, due to concerns that participants in the treatment and control groups would differ by more factors than exclusively POINT participation Subsequent overdose was identified using current procedural terminology (CPT) codes for drug poisoning. Their analysis yielded no significant effect (p=0.856) from POINT intervention with regards to subsequent overdose/drug poisoning during the data collection timeframe.
Watson et al followed up their 2021 work with a cluster randomized trial involving 243 adults presenting to two EDs (distinct from the site of their earlier study) for an opioid-related condition, meeting one or more criteria for opioid use disorder, and discharging from the ED29 A variety of administrative records were utilized to measure outcomes, including medical records and vital records from hospital and state levels. At one, three, and 12 months post index ED visit, there was no statistically significant difference between the intervention and control arms regarding overdose-related ED re-presentation. At 12 months, 7% of individuals in the control arm and 3% of individuals in the intervention arm died of overdose. This difference was not statistically significant (p=0.07).
Chambers et al, in their randomized control trial (RCT) published in 2024, compared outcomes following behavioral interventions delivered by PRSS versus licensed clinical social workers (LICSWs) in two EDs24 Patients were identified by ED clinician referral and research assistant electronic medical record review Eligibility criteria included adults at high risk of opioid overdose, as defined by ED presentation for opioid overdose, ED treatment for complications of opioid use disorder, or a history of opioid overdose in the past year A total of 648 patients (shared dataset with Beaudoin et al and Bhondoekhan et al)21,23 were randomized into the two treatment arms At 18 months post index ED visit, 251% in the PRSS group had a nonfatal opioid overdose compared to 292% in the LICSW group This difference was not statistically significant (p=0.24). The authors did note that a prior opioid overdose was linked to an increased likelihood of experiencing a nonfatal overdose in the study timeframe. The study team adjusted for this risk factor when reporting the lack of statistically significant difference in effectiveness of ED behavioral intervention delivered by PRSS versus LICSW for subsequent nonfatal overdose (relative risk=0.86, 95% CI=0.67–1.11). As part of the secondary outcomes, the authors analyzed fatal opioid overdoses. At 18 months post index ED visit, fewer individuals in the PRSS arm had a fatal opioid overdose (3.4%) than individuals in the LICSW arm (4.6%), though a measure of statistical significance was not reported for this. The cumulative incidence of death from fatal opioid overdose was not statistically different between groups (p=0.42).
Treitler et al (2025) conducted a retrospective cohort study that included 5,475 unique patients who had ED visits for nonfatal opioid overdose between 2016 and 2020 as identified by state Medicaid claims27 Participants were separated into cohorts based on whether the patient received ED-based PRSS (with associated post ED discharge follow-up) Patients were eligible for the study at multiple timepoints if there was no overlap between 6 months pre and 6 months post index ED visit. Propensity score matching identified the control group. Within 180 days of the index ED visit, the percentage of repeat medically treated opioid overdose was the same between the PRSS cohort and the non-PRSS cohort (25%) (risk difference= −0.01, 95% CI= −0.03–0.02). Further, the percentage of repeat medically treated any drug overdose was similar between the PRSS cohort and the non-PRSS cohort (26% versus 27%, respectively) (risk difference= −0.01, 95% CI= −0.04–0.02). No statistically significant difference was noted when PRSS participants were compared to non-participants for opioid overdose (hazard ratio=0.92, 95% CI=0.72–1.18) or any drug overdose (hazard ratio=0.88, 95% CI=0.69–1.12).
Finally, a pre/post study by Nordeck et al (2025) explored several outcomes, including overdose25 The study involved 6,566 patients in seven hospital sites who received PRSS intervention in 2022. Eligibility criteria included positive substance use screening or ED presentation related to SUD. However, some individuals received PRSS as they were assumed eligible for the intervention without documented rationale. Analysis revealed that PRSS was associated with decreased odds of overdose-related hospital utilization 6 months pre compared to 6 months post receipt of ED-based PRSS intervention (odds ratio (OR)=0.54, 95% CI=0.47–0.63, p<0.001). Notably, overdose-related hospital utilization was measured using hospital ICD-10 codes for opioid intoxication and poisoning.
Outcome 2: All-Cause Mortality
Three studies explored all-cause mortality.24,26,29 Additional details about these study methodologies can be found in the previous section, and results related to all-cause mortality will be discussed further here. Samuels et al (2018) underwent a retrospective cohort study of individuals presenting to the ED for opioid overdose who received i) peer recovery coach plus take-home naloxone, ii) take home naloxone without peer recovery coach, and iii) usual care26 Similar to their findings with overdose, at 1 year post index ED visit, all-cause mortality was 6.7% (95% CI=2.5–16.7) with usual care, 3.1% (95% CI=0.8–11.7) with a peer recovery coach plus take-home naloxone, and 3.8% (95% CI=0.5–23.8) with take-home naloxone alone. These percentages were not statistically significant.
Watson et al (2024) also explored all-cause mortality for patients in the intervention (POINT program) versus control arms29 No statistically significant differences in all-cause mortality between groups were observed at one (no deaths), three (p=1.0), or 12 (p=0.10) months. Although the percentage of all-cause deaths at 12 months was 10.5% in the control group and 4.5% in the intervention group, this difference was not statistically significant.
Chambers et al (2024) also explored all-cause mortality.24 Their study was a RCT looking at outcomes for participants determined to be at high risk of opioid overdose who received a behavioral intervention in the ED by a PRSS (treatment arm) or a LICSW (control arm) (shared dataset with Beaudoin et al and Bhondoekhan et al)21,23 All-cause mortality was another secondary study outcome. At 18 months post index ED visit, less individuals in the PRSS arm had a fatal opioid overdose (5.0%) than individuals in the LICSW arm (6.5%), though a measure of statistical significance was not identified. The authors noted that 70.3% of fatalities were secondary to fatal opioid overdose. The cumulative incidence of all-cause mortality was not statistically different between groups (p=0.40).
Outcome 3: All-Cause Hospital Return
Three studies analyzed all-cause hospital return.25,27,29 In their 2024 study, Watson et al also explored all-cause hospital readmission in the form of all-cause ED re-presentation for the intervention (POINT program) versus the control arm.29 The percentages of participants in both groups with all-cause hospital return at one, three, and 12 months were very similar. No statistically significant difference was appreciated at any of the three time points (p=0.90, 0.42, and 0.98 at one, three, and 12 months, respectively).
Treitler et al (2025) conducted a retrospective cohort study of patients presenting to the ED with nonfatal opioid overdose identified through state Medicaid claims27 Several outcomes were measured between patients who did and did not receive PRSS using propensity-matched controls. Within 180 days of the index ED visit, slightly fewer individuals in the PRSS cohort had a subsequent all-cause hospital return (ED or inpatient visit) (58%) than the control group (60%) (risk difference= −0.03, 95% CI= −0.06–0.00). When time-to-event outcomes were analyzed, PRSS was associated with significantly lower hazard of all-cause hospital return (ED or inpatient visits) (hazard ratio=0.83, 95% CI=0.72–0.97) compared to control. However, this time-to-event finding was not observed for opioid-related hospital returns (hazard ratio=0.85, 95% CI=0.69–1.05).
In a recent retrospective pre/post analysis, Nordeck et al (2025) analyzed all-cause hospital return for 6,566 patients 6 months before and after ED-based PRSS implementation PRSS was associated with decreased odds of any hospital event, either inpatient or ED visit, with OR=0.18 post-intervention as measured by hospital service data (95% CI=0.16–0.20, p<0.001).25 Further, also measured by hospital service data, PRSS was associated with decreased odds of all-cause ED visits (OR=0.20, 95% CI=0.19–0.22, p<0.001); however, PRSS was associated with increased odds of all-cause inpatient admissions post-intervention (OR=1.45, 95% CI=1.34–1.56, p<0.001).
Outcome 4: Psychosocial SUD Treatment Initiation
Additionally, three studies looked at psychosocial SUD treatment.21,23,27 Beaudoin et al (2022) conducted a RCT of 648 participants (shared dataset with Chambers et al and Bhondoekhan et al)23,24 determined to be at high risk for subsequent opioid overdose, defined as presenting to the ED for opioid overdose at the index ED visit, receiving treatment related to opioid use disorder at the index ED visit, or having a history of opioid overdose in the last year These participants were randomized to ED behavioral intervention from a PRSS or LICSW and 30-day outcomes were reported.21 A later paper reported 18-month outcomes.24 Among participants screened, the most common reason for not participating in the study was not wanting to wait for the intervention. At 30 days post ED visit, 30% of individuals in the LICSW arm and 32% of individuals in the PRSS arm were enrolled in a SUD treatment program; there was no statistically significant difference in relative risk between the two interventions via two different models (p values of 0.633 and 0.673). Analyses revealed that prior SUD treatment increased the likelihood of SUD treatment post index ED visit for both groups, without an outcome difference between arms, when prior to enrollment SUD treatment was controlled for.
Subsequently, a secondary analysis of the study data shared by Beaudoin et al and Chambers et al was completed by Bhondoekhan et al and published in 2024.23 They explored SUD treatment engagement via pharmacologic and non-pharmacologic treatment modalities within 90 days of the index ED visit. For statistical analysis, the treatment modalities were combined; no statistically significant difference in time to SUD treatment engagement (p=0.50) or type of SUD treatment (p=0.88) was observed when the ED behavioral intervention was delivered by a PRSS versus a LICSW. Regarding non-pharmacologic treatment, at 90 days post index ED visit, the percentage of individuals engaged with residential treatment was 13.9% and 14.2% in the LICSW versus PRSS arms, respectively, while the percentage of individuals engaged with intensive outpatient or outpatient treatment was 5.1% and 3.6% in the LICSW versus PRSS arms, respectively.
In their recent retrospective cohort study published in 2025, Treitler et al also compared SUD treatment between patients who had and had not received ED-based PRSS after presenting for nonfatal opioid overdose as identified by state Medicaid claims.27 Psychosocial treatment initiation was defined as any psychosocial services claim with SUD diagnosis within 60 days of index ED visit discharge. Psychosocial treatment engagement was defined as two or more additional psychosocial services within 30 days of psychosocial treatment initiation. Following propensity score matching, individuals who were enrolled in PRSS were significantly more likely to initiate psychosocial SUD treatment within 60 days of the index ED visit (16%) compared to those who were not enrolled in PRSS (11%) (risk difference=0.04, 95% CI=0.02–0.06). Further, individuals who were enrolled in PRSS were more likely to engage with psychosocial SUD treatment within 30 days of enrollment (24%) compared to those in the non-PRSS control group (18%) (risk difference=5.71, 95% CI=3.45–7.98).
Additional Study
One study that met systematic review inclusion criteria did not include one of these most common outcomes.22 This study was a RCT published in 2011, which included 338 participants with regular cigarette smoking in the contemplation or preparation stages of change, randomized to usual care (smoking cessation brochure) versus enhanced care (smoking cessation brochure, motivational interview, nicotine replacement therapy, and follow-up call within 3 days after ED discharge). Notable exclusion criteria included individuals at other stages of change and those managed in the psychiatric ED. At 3 months, individuals in both groups made attempts to quit, had 7 days of abstinence prior to their 3-month follow-up call, and engaged with smoking cessation discussions. However, no statistically significant difference in 7-day abstinence before follow-up (p=0.68) or other measured metrics between usual care and enhanced care was observed. Notably, via stratified analysis, individuals were more likely to have 7-day abstinence before follow-up if they had a tobacco-related ED discharge diagnosis (p=0.002) but less likely to have 7-day abstinence before follow-up if they believed they had a chronic tobacco-related illness (p=0.02).
Risk of Bias
Utilizing the Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for Quantitative Studies,19,20 most studies (n=7) were noted to be moderate risk of bias (some risk of bias), with one of the remaining two being weak (significant risk of bias) and another being strong (minimal risk of bias) (Table 2). The section with the weakest ratings across the studies was selection bias. In this section, many studies fell short in how representative individuals selected to participate in the study were of the target population.
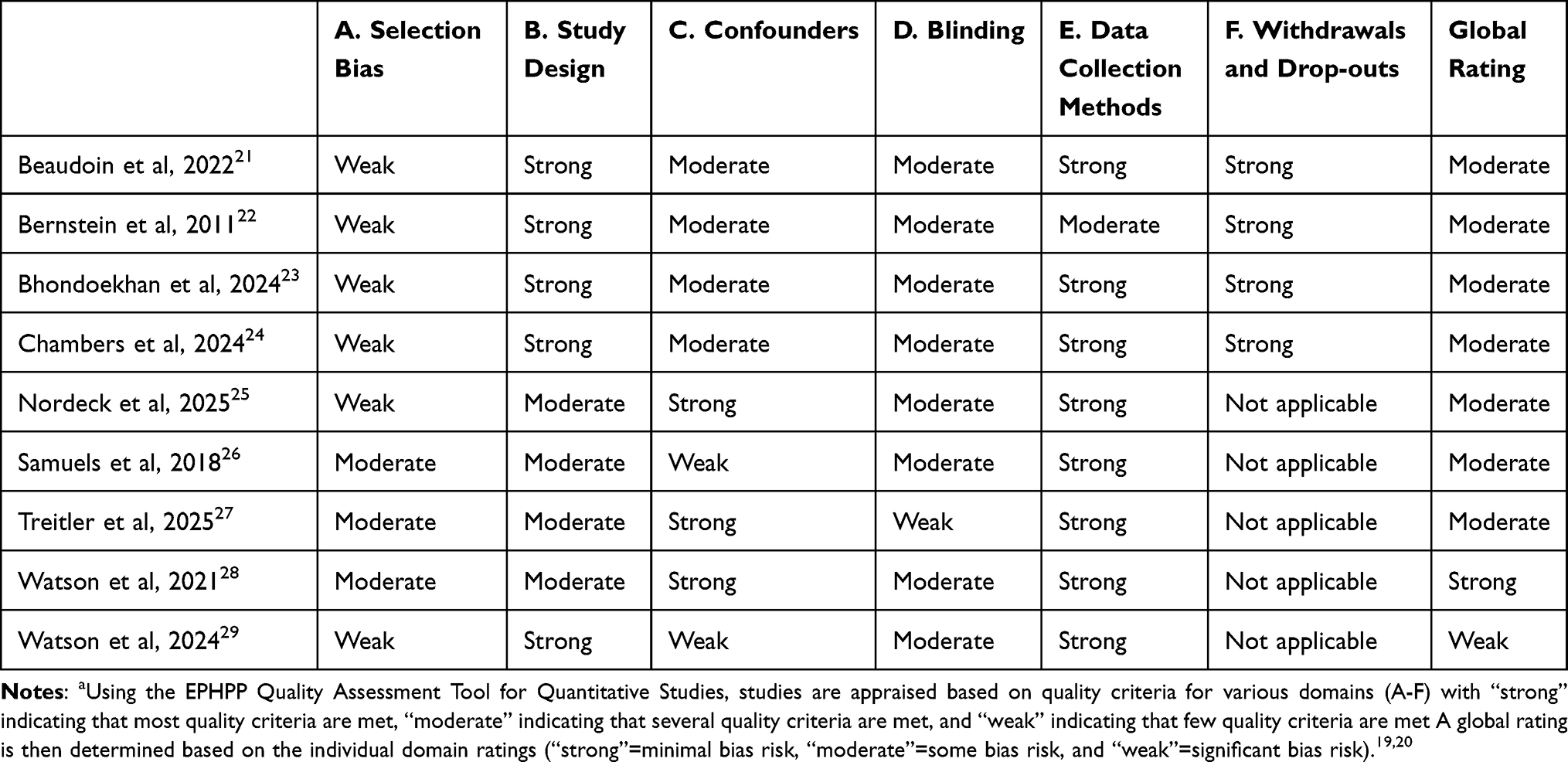 |
Table 2 Included Study Risk of Bias Using the EPHPP Quality Assessment Tool for Quantitative Studiesa |
Discussion
The present systematic literature review identified nine studies evaluating PRSS in the ED for patients with SUDs Across the included studies, overlapping outcomes included overdose (n=6), all-cause mortality (n=3), all-cause hospital return (n=3), and psychosocial SUD treatment initiation (n=3) Of the eight studies with one or more of the aforementioned outcomes, two demonstrated positive results: Treitler et al (2025) for psychosocial SUD treatment initiation and all-cause hospital return and Nordeck et al (2025) for overdose and all-cause hospital return25,27 The two studies with positive results were determined to be at moderate global bias risk Of the remaining six studies with one or more desired outcome, one was considered strong, one was considered weak, and four were considered moderate with regard to global risk of bias.19,20
Across the eight studies with one or more of the overlapping outcomes (overdose, all-cause mortality, all-cause hospital return, and psychosocial SUD treatment initiation), there was substantial heterogeneity between the treatment group interventions. Though all treatment groups received PRSS, in some studies PRSS was part of a multicomponent program. The two studies with positive results were Treitler et al (2025) and Nordeck et al (2025) Participants in the former study received PRSS as part of the New Jersey Opioid Overdose Recovery Program (OORP), which involved ED-based peer intervention, regular follow-up contact post-ED intervention, assistance with treatment linkage, and a particular focus on linkage and retention in treatment with medications for opioid use disorder27 Participants in the latter study received PRSS as part of Mosaic Group’s Reverse the Cycle (RTC) Program, which involved ED-based peer consultation and assistance with treatment linkage25 Further, based on the intervention description, there appears to be additional emphasis on ED initiation of medication for opioid use disorder treatment when applicable along with resources to address social needs.25 Though these interventions were slightly different, they fall within the services PRSS provides.8 It is also notable that some studies with negative results also utilized PRSS as part of a multicomponent program,26,28,29 suggesting that positive findings may not have been due to the multicomponent nature of studies alone.
Taken together, PRSS shows some promise to improve some outcomes for patients with SUDs in the ED. However, evidence for this in the literature remains mixed and PRSS has yet to demonstrate superiority to usual care. There are many possibilities for why the ED lags behind other treatment settings in demonstrating benefits for patients with SUDs following PRSS, including potential patient-level and system-level differences in the ED setting.
Patient-Level Differences
Patients with SUDs presenting to the ED may arrive by family vehicle, emergency medical services, or law enforcement. This is a striking difference from other care settings and may reflect a group less ready to change their substance use patterns. Studies have highlighted that readiness to change can be a strong predictor of subsequent SUD treatment initiation.30 Further, in their 2022 study, Ware et al explored factors among individuals who were and were not linked to care following ED-based PRSS31 Through multivariable logistic regression, they identified that one factor increasing the odds of successful treatment linkage was being in the “action” stage of change (OR=2.33, 95% CI=1.47–3.69, p<0.001). This calls into question whether PRSS effectiveness is more dependent on the patient’s motivation for treatment than details of the PRSS intervention itself.
When analyzing the included study methodologies, selection bias due to individuals opting in or out of the studies may contribute to the lack of observed differences (Table 2). Consider Watson et al (2024) where many patients were approached for the PRSS or control arm (476 and 358, respectively, for a sum of 834)29 Yet a significant number in both groups were unable to engage or declined participation In the end, 243 individuals (157 in the PRSS arm and 86 in the control arm) met inclusion criteria, agreed to participate, engaged, and had records available for analysis; this represents 29% of the individuals approached This raises concern for selection bias.
Additionally, patients presenting to the ED often experience increased psychosocial complexity, including unstable housing and other unmet social needs, which may impede SUD treatment engagement and, subsequently, patient-specific outcomes, following PRSS. The extent to which housing instability and similar psychosocial complexities specifically impact outcomes from ED-based PRSS has not been extensively explored. Although more generally, housing instability is one psychosocial factor that has been associated with greater substance use severity and complexity in patients presenting to the ED.32 This highlights how unmet social determinants of health may attenuate the impact of PRSS in the ED.
Additional exploration of the psychosocial factors that predict patient engagement with ED-based PRSS is warranted. Findings from such work could aid clinicians in identifying which patients may benefit from ED-based PRSS. These insights would also assist in increasing the rigor of ED-based PRSS research studies by providing additional guidelines for patient matching. In the present review, the two studies with positive findings for the outcomes of interest were Treitler et al (2025) and Nordeck et al (2025)25,27 The former was a retrospective cohort study of patients with ED visits for nonfatal opioid overdose with a treatment arm (received ED-based PRSS) and control arm (did not receive ED-based PRSS, identified using propensity score matching) The latter was a pre/post study of outcomes for a cohort of patients pre and post ED-based PRSS. Based on the study designs utilizing propensity score matching or evaluating the same patient group at different timepoints, these studies may represent two where more patient-level variables, which may influence outcomes, were controlled for.
Systems-Level Differences
At the systems level, ED-based PRSS may be less fully integrated into clinical workflows compared to other treatment settings. Limited integration could lead to service delays, which may have downstream effects, including reduced opportunities for timely engagement and decreased effective linkage to ongoing care. Three of the included studies utilized the same dataset but varied in the studied outcome and/or timepoint.21,23,24 Beaudoin et al explored psychosocial SUD treatment initiation within 30 days of the index ED visit, where PRSS was delivered.21 The authors note that the most common reason individuals failed to participate in the study was not wanting to wait for the PRSS intervention. This highlights the need for PRSS to be readily and quickly available for patients in clinical settings, as well as the need for PRSS to be easily accessible in research studies exploring PRSS to include the largest number of study participants and generate the highest quality data.
Navigating These Differences
Studies of PRSS for patients with SUDs in treatment settings have focused on SUD treatment engagement and patient-level outcomes, establishing more benefit for the former than the latter.18 The more supported benefit observed with treatment engagement suggests that ED-based PRSS may target proximal behavioral and relational aspects of recovery more closely than longer-term clinical endpoints. The outcome measures of overdose, all-cause mortality, all-cause hospital return, and psychosocial SUD treatment initiation have been explored in many studies exclusively in the ED setting. However, patient- and system-level differences inherent to the ED setting may necessitate the utilization of additional outcome measures to assess the effectiveness of PRSS. Kirk et al in a recent study commented on the focus to date on quantitative (versus qualitative) studies in this area of ED-based PRSS.33 Further, they note that future work should expand to more patient-centered outcomes, including the subjective experience of working with peers. This aligns with results from a recent meta-analysis involving PRSS for mental health generally which demonstrated improvement in psychosocial (empowerment and self-reported recovery) but not clinical (hospitalizations or mental health symptoms) outcomes following PRSS.34 Further work understanding the patient experience with ED-based PRSS may glean additional insights to better understanding the shortcomings to date in the studies of ED-based PRSS.
It is also possible that ED-based PRSS studies need to monitor outcomes for a longer duration of time for the benefit of PRSS to be revealed. This is supported by the Watson et al (2024) study where the outcomes of overdose and all-cause mortality approached statistical significance as time went on at 12 months29 This calls into question what other study design adjustments need to be made to account for patient-level differences in the ED.
Limitations
The current systematic review has several limitations. Though a considerable number of patients were involved in the nine studies, this was a small number of total studies. Further, three of the nine studies utilized the same dataset.21,23,24 Additionally, six of the studies were rated as weak in terms of selection bias using the EPHPP Quality Assessment Tool for Quantitative Studies.19,20 Across most studies, this was primarily the result of concerns related to how representative included individuals were of the target population.
Other limitations result from similarities and differences across studies. Regarding the former, there was significant homogeneity between studies in the type of substance use that was explored. The nine studies involved seven distinct datasets; of these, five involved opioid use, one involved nicotine use, and one involved any substance use. The latter was the study by Nordeck et al, a pre/post study of outcomes for a single group 6 months before and 6 months after PRSS25 In the 6 months post PRSS, there was a reduction in overdose and all-cause hospital return Further studies are needed to better understand patient outcomes for those with concerning use of all substances following PRSS, particularly for patients using non-opioids Additionally, more studies explored long-term clinical outcomes, which may underscore more short-term relational and engagement effects of PRSS.
There are also limitations originating from differences across studies Variability existed with respect to study design, who the peer was (their background, experience, and training), the support the peer provided, the control group intervention, study outcomes, and outcome duration. Significant study heterogeneity was noted by Mahon in a 2025 umbrella review of PRSS in substance use settings.35 Methodologically, Mahon also calls for an increase in PRSS mixed-methods studies, as the ability of RCTs to study this topic may be limited. Of the nine studies identified in the present review, five used a randomized design (four RCTs and one cluster-randomized trial). Given the scarcity of research into ED-based PRSS for patients with SUDs, increasing the number and types of studies in this area will fortify the evidence base.
Conclusion
Nine studies of ED-based PRSS met the inclusion criteria and were analyzed during the present systematic review. The nine studies varied in multiple ways, including the details of the PRSS intervention and the duration of the outcomes studied. Yet, the nine studies were similar in other ways: most (seven) focused on opioid use, the majority (eight) included one or more of four overlapping outcomes, most (seven) were considered moderate with regard to global risk of bias, and all were quantitative. The current, limited literature of ED-based PRSS for patients with SUDs remains mixed, though two studies demonstrated positive results: Treitler et al (2025) for psychosocial SUD treatment initiation and all-cause hospital return and Nordeck et al (2025) for overdose and all-cause hospital return25,27 The two studies with positive findings were determined to be at moderate risk of global bias19,20 Interpretation is limited by the paucity of studies, outcome variation, varying follow-up periods, and selection bias.
Taken together, PRSS remains promising in theory as an ED-based intervention to improve clinical and utilization outcomes for individuals with SUDs, though has yet to demonstrate superiority to usual care. Limitations for ED-based PRSS include patient- and system-level challenges, including readiness to change and integration of PRSS into ED workflows. A strength of ED-based PRSS may be its relational component; future studies should use a qualitative or mixed-methods versus exclusively quantitative design to further explore this. In addition, future studies should explore ED-based PRSS for patients without opioid use exclusively, as the current evidence base is heavily weighted towards ED-based PRSS for individuals with concerning opioid use, and incorporate strategies to minimize selection bias. With the present literature base, ED-based PRSS for individuals with SUDs remains a reasonable approach to integrate into clinical workflows given its patient-centered rationale, the lack of negative outcomes, and potential benefits for this high-risk population.
Data Sharing Statement
Data used was derived from published literature and is publicly available. The Methods section details the search strategy employed.
Disclosure
The authors report no conflicts of interest in this work.
References
1. National Survey on Drug Use and Health (NSDUH). key substance use and mental health indicators in the United States annual national report. National Survey on Drug Use and Health (NSDUH); 2025. Available from: https://www.samhsa.gov/data/data-we-collect/nsduh-national-survey-drug-use-and-health/national-releases/2024#annual-national-report.
2. Lewer D, Freer J, King E, et al. Frequency of health-care utilization by adults who use illicit drugs: a systematic review and meta-analysis. Addiction. 2020;115(6):1011–13. doi:10.1111/add.14892
3. Drug Abuse Warning Network (Dawn): national estimates from drug-related emergency department visits, 2024. Substance Abuse and Mental Health Services Administration (SAMHSA). Available from: https://www.samhsa.gov/data/report/2024-national-estimates-drug-related-emergency-department-visits.
4. Zhang X, Wang N, Hou F, et al. Emergency department visits by patients with substance use disorder in the United States. West J Emerg Med. 2021;22(5):1076–1085. doi:10.5811/westjem.2021.3.50839
5. Hadani Y, Tarikogullari I, Oesterle TS, et al. Care coordination in screening, brief intervention, and referral to treatment (SBIRT): a scoping review. Am J Addict. 2026;35(1):22–35. doi:10.1111/ajad.70104
6. Farhoudian A, Razaghi E, Hooshyari Z, et al. Barriers and facilitators to substance use disorder treatment: an overview of systematic reviews. Subst Abuse. 2022;16:11782218221118462. doi:10.1177/11782218221118462
7. Mendiola CK, Galetto G, Fingerhood M. An exploration of emergency physicians’ attitudes toward patients with substance use disorder. J Addict Med. 2018;12(2):132–135. doi:10.1097/ADM.0000000000000377
8. What are peer recovery support services? U.S. Department of Health and Human Services Substance Abuse and Mental Health Services Administration Center for Substance Abuse Treatment. Available from: https://library.samhsa.gov/product/what-are-peer-recovery-support-services/sma09-4454.
9. Stack E, Hildebran C, Leichtling G, et al. Peer recovery support services across the continuum: in community, hospital, corrections, and treatment and recovery agency settings - A narrative review. J Addict Med. 2022;16(1):93–100. doi:10.1097/ADM.0000000000000810
10. Horn K, Flinn RE, Hagaman AM, et al. Systematizing peer recovery support services for substance use disorder: a taxonomy for measuring recovery milestones. Front Public Health. 2025;13:1529078. doi:10.3389/fpubh.2025.1529078
11. Eddie D, Hoffman L, Vilsaint C, et al. Lived experience in new models of care for substance use disorder: a systematic review of peer recovery support services and recovery coaching. Front Psychol. 2019;10:1052. doi:10.3389/fpsyg.2019.01052
12. Brant K, Quadri O, McCracken A, Jones A. The benefits and potential biases of lived experience in substance use treatment services. J Soc Work Pract Addict. 2025;25(4):442–458. doi:10.1080/1533256X.2025.2534338
13. Scott KD, Gorey KM. Concurrent disorders and treatment outcomes: a meta-analysis. J Dual Diagn. 2025;21(3):251–265. doi:10.1080/15504263.2025.2515015
14. Hawk K, McCormack R, Edelman EJ, et al. Perspectives about emergency department care encounters among adults with opioid use disorder. JAMA Netw Open. 2022;5(1):e2144955. doi:10.1001/jamanetworkopen.2021.44955
15. Treitler P, Crystal S, Cantor J, et al. Emergency department peer support program and patient outcomes after opioid overdose. JAMA Netw Open. 2024;7(3):e243614. doi:10.1001/jamanetworkopen.2024.3614
16. Qeadan F, Madden EF, Tingey B, Egbert J, Venner KL, English K. Evaluating risk factors and protective clinical interventions for opioid use disorder and overdose in American Indian/Alaska Native populations. J Ethn Subst Abuse. 2026;1–24. doi:10.1080/15332640.2026.2657000
17. Jack HE, Arif SA, Moore MA, et al. Peer support for patients with opioid use disorder in the emergency department: a narrative review. J Am Coll Emerg Physicians Open. 2024;5(4):e13253. doi:10.1002/emp2.13253
18. Eddie D, O’Connor JB, George SS, et al. Peer recovery support services and recovery coaching for substance use disorder: a systematic review. Curr Addict Rep. 2025;12:40. doi:10.1007/s40429-025-00645-8
19. Quality Assessment Tool for Quantitative Studies. Effective public health practice project. Available from: http://www.ephpp.ca/tools.html.
20. Armijo-Olivo S, Stiles CR, Hagen NA, Biondo PD, Cummings GG. Assessment of study quality for systematic reviews: a comparison of the cochrane collaboration risk of bias tool and the effective public health practice project quality assessment tool: methodological research. J Eval Clin Pract. 2012;18(1):12–18. doi:10.1111/j.1365-2753.2010.01516.x
21. Beaudoin FL, Jacka BP, Li Y, et al. Effect of a peer-led behavioral intervention for emergency department patients at high risk of fatal opioid overdose: a randomized clinical trial. JAMA Netw Open. 2022;5(8):e2225582. doi:10.1001/jamanetworkopen.2022.25582
22. Bernstein SL, Bijur P, Cooperman N, et al. A randomized trial of a multicomponent cessation strategy for emergency department smokers. Acad Emerg Med. 2011;18(6):575–583. doi:10.1111/j.1553-2712.2011.01097.x
23. Bhondoekhan F, Li Y, Hallowell BD, et al. Engagement in substance use disorder treatment after an emergency department visit among persons at high risk of opioid overdose: a prediction analysis. Drug Alcohol Depend Rep. 2024;13:100287. doi:10.1016/j.dadr.2024.100287
24. Chambers LC, Li Y, Hallowell BD, et al. Effect of a peer-led emergency department behavioral intervention on non-fatal opioid overdose: 18-month outcome in the Navigator randomized controlled trial. Addiction. 2024;119(12):2116–2128. doi:10.1111/add.16581
25. Nordeck CD, Oros M, Raley H, Smith S, Gryczynski J. Changes in hospital utilization following peer-led intervention for substance use disorders in hospital emergency departments. Am J Emerg Med. 2025;95:167–172. doi:10.1016/j.ajem.2025.05.049
26. Samuels EA, Bernstein SL, Marshall BDL, Krieger M, Baird J, Mello MJ. Peer navigation and take-home naloxone for opioid overdose emergency department patients: preliminary patient outcomes. J Subst Abuse Treat. 2018;94:29–34. doi:10.1016/j.jsat.2018.07.013
27. Treitler P, Lloyd K, Cantor J, et al. Treatment initiation and outcomes associated with receipt of emergency department-based peer support following opioid overdose. Ann Emerg Med. 2025;86(5):463–474. doi:10.1016/j.annemergmed.2025.06.616
28. Watson DP, Weathers T, McGuire A, et al. Evaluation of an emergency department-based opioid overdose survivor intervention: difference-in-difference analysis of electronic health record data to assess key outcomes. Drug Alcohol Depend. 2021;221:108595. doi:10.1016/j.drugalcdep.2021.108595
29. Watson DP, Tillson M, Taylor L, et al. Results from the POINT pragmatic randomized trial: an emergency department-based peer support specialist intervention to increase opioid use disorder treatment linkage and reduce recurrent overdose. Subst Use Addctn J. 2024;45(3):378–389. doi:10.1177/29767342231221054
30. Ryus CR, D’Onofrio G, Canty T, Pantalon MV, Heimer R, Hawk K. Self-reported readiness-to-change alcohol use in emergency department patients with alcohol use disorder is associated with linkage to treatment. Ann Emerg Med. 2026;87(2):275–277. doi:10.1016/j.annemergmed.2025.09.027
31. Ware OD, Buresh ME, Irvin NA, Stitzer ML, Sweeney MM. Factors related to substance use treatment attendance after peer recovery coach intervention in the emergency department. Drug Alcohol Depend Rep. 2022;5:100093. doi:10.1016/j.dadr.2022.100093
32. Doran KM, Rahai N, McCormack RP, et al. Substance use and homelessness among emergency department patients. Drug Alcohol Depend. 2018;188:328–333. doi:10.1016/j.drugalcdep.2018.04.021
33. Kirk MR, Etchart H, Soske J, et al. Certified peer recovery support specialists and substance use related emergency department visits: a mixed methods study of the patient experience. J Subst Use Addict Treat. 2025;169:209563. doi:10.1016/j.josat.2024.209563
34. White S, Foster R, Marks J, et al. The effectiveness of one-to-one peer support in mental health services: a systematic review and meta-analysis. BMC Psychiatry. 2020;20(1):534. doi:10.1186/s12888-020-02923-3
35. Mahon D. Umbrella review of systematic reviews of peer support in substance use settings. Ment Health Soc Incl. 2025;29(5):535–550. doi:10.1108/MHSI-01-2025-0002
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.