Back to Journals » Open Access Emergency Medicine » Volume 18
Emergency Department Clinician Perspectives on an EMR-Adjacent Microsoft Teams Consultation Workflow
Authors Rosen C, Ng N, Shawl A, Mathews K, Armanious A, Khodorkovsky B, Mohamadi A, Hahn B ![]()
Received 15 May 2026
Accepted for publication 10 July 2026
Published 15 July 2026 Volume 2026:18 624827
DOI https://doi.org/10.2147/OAEM.S624827
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Carly Rosen,1,2 Norman Ng,1,2 Arsalan Shawl,1,2 Kurien Mathews,1,2 Alexia Armanious,1,2 Boris Khodorkovsky,1,2 Amin Mohamadi,1,2 Barry Hahn1– 3
1Northwell Health, New Hyde Park, NY, USA; 2Department of Emergency Medicine, Staten Island University Hospital, Staten Island, NY, USA; 3Department of Emergency Medicine, Hadassah University Medical Center–Ein Kerem, Jerusalem, Israel
Correspondence: Barry Hahn, Department of Emergency Medicine, Staten Island University Hospital, 475 Seaview Avenue, Staten Island, NY, 10305, USA, Email [email protected]
Background: Communication failures in the emergency department (ED) can delay consultations and worsen crowding. Hospitals now use phone-based systems, EMR-integrated secure chat, and EMR-adjacent messaging platforms for consultant communication, but few studies describe ED clinician experience with these workflows.
Objective: To describe ED clinicians’ perceived acceptability of, and experience with, an EMR-adjacent Microsoft Teams–based consultation workflow used alongside a telephone-based consultation pathway.
Methods: We conducted a single-center post-implementation survey of clinicians who used a Microsoft Teams consultation workflow in an academic ED. The primary analysis focused on ED clinician responses; consulting clinician responses were reported descriptively because of the low estimated non-ED response rate.
Results: Of 121 respondents, 82 were ED clinicians, and 39 were consulting clinicians. Among ED clinicians, 78.0% reported high acceptability of the Teams consultation workflow, 85.4% perceived improvements in the workflow, and 89.0% perceived a positive impact on patient care. Delays remained common, with 24.4% of ED clinicians reporting that responses were often delayed. Consulting clinician responses are reported descriptively only because of the low estimated non-ED response rate.
Conclusion: ED clinicians reported high perceived acceptability of an EMR-adjacent Microsoft Teams consultation workflow used alongside a telephone-based consultation pathway. These results reflect post-implementation clinician perceptions and do not establish improved consultation timeliness, patient flow, or clinical outcomes.
Keywords: emergency service, communications, consultations
Introduction
Effective communication in the emergency department (ED) is critical for timely diagnosis, treatment, and consultation. Many EDs rely on hospital-issued mobile phones, pagers, or operator-mediated callback systems for direct voice communication with consultants. At our institution, this pathway primarily uses SpectraLink (Spectra) phones (SpectraLink Corp, Boulder, CO). These devices can make it challenging to reach specialists, are prone to dropped calls or battery failure, and do not generate a durable written record of the interaction.1,2 Hospitals now use a range of consultation communication pathways, including direct telephone calls, pager-based callback systems, hospital-issued mobile devices, EMR-integrated secure messaging tools such as Epic Secure Chat, and EMR-adjacent secure messaging platforms configured for clinical use. These systems differ in their integration with the medical record, support for asynchronous communication, notification design, documentation trail, and capacity for closed-loop communication. For ED clinicians, the practical question is whether these tools make consultation easier, more traceable, and less disruptive during clinical care.
As hospitals adopt integrated digital systems, secure messaging platforms have emerged to support real-time team communication.3 These tools allow clinicians to send written consult messages that can be reviewed later by other members of the care team. Microsoft Teams (Microsoft Corp, Redmond, WA) is one such EMR-adjacent platform and has been implemented in some healthcare settings as a secure environment for clinical messaging, file sharing, and interdisciplinary collaboration.4 Teams creates timestamped message threads that can be followed across shifts and by multiple members of a service. Prior studies of secure messaging and consult workflows have reported shorter time to consultant response, improved ED length of stay (LOS), and high user satisfaction, while also noting increased message volume and communication burden.5–7
At our institution, before implementing Microsoft Teams Channels, ED clinicians relied on answering services, pagers, and hospital-distributed Spectra phones to reach consultants. In 2023, the ED collaborated with consulting services to create Microsoft Teams Channels for consultation requests and related discussions. Messages within Teams are timestamped and can be reviewed by members of the relevant clinical team. Clinicians often include patient identifiers or clinical information from the electronic medical record (EMR). Still, Teams is an EMR-adjacent secure messaging platform and is not directly integrated with the EMR. Formal consultation recommendations and clinical documentation remain in the EMR according to usual institutional practice.
Less is known about how ED clinicians experience EMR-adjacent messaging tools when they are layered onto existing phone-based consultation pathways. Inefficient consultation processes can prolong ED LOS and contribute to crowding, while structured electronic pathways may improve timeliness and user satisfaction.8 To address this gap, we conducted a single-center post-implementation survey focused primarily on ED clinicians’ perceived acceptability of, and experience with, a Microsoft Teams–based consultation workflow used alongside the prior Spectra phone pathway.
Methods
Study Design and Setting
We conducted a single-center, post-implementation cross-sectional survey focused primarily on ED clinicians’ experience with a Microsoft Teams–based consultation workflow at Staten Island University Hospital North Campus (SIUH), a 500-bed academic tertiary care center in Staten Island, New York. The hospital manages approximately 97,000 patient visits annually and is designated as a Level I trauma center and a comprehensive stroke center. The Teams implementation occurred before survey administration, and the survey was conducted from January 2025 to June 2025. The Northwell Health Institutional Review Board approved this study (Protocol #23-0372).
Teams Channels were introduced as an operational initiative before the conception of this study, and we did not perform a pre-implementation or baseline survey of the prior Spectra-only workflow. As a result, our evaluation focuses on clinicians’ retrospective perceptions of change rather than prospectively measured pre–post differences. When we refer to “improvement” in workflow or patient care, we are describing respondents’ perceived improvement relative to their prior consultation experience, not objectively measured changes in processes or outcomes.
At the time of the survey, the ED and many adult medical and surgical consulting services used Teams as the default mechanism for initiating ED consultations, while the legacy Spectra phone system remained available as the primary pathway for a minority of services and as a backup when consultants could not be reached on Teams.
Microsoft Teams was deployed through the institution’s enterprise Microsoft 365 environment and configured for clinical use in accordance with institutional information security policies. The platform was approved by hospital information technology and compliance leadership for communication containing protected health information. Access was restricted to authenticated institutional users, and Teams Channels were limited to relevant ED and consulting service members. Teams messages were not considered part of the legal medical record, and clinicians were expected to document formal consultation recommendations in the EMR, as usual.
Over the preceding 30 months, more than 15 Microsoft Teams Channels had been established for communication between the ED and consulting services, with additional subchannels created to improve efficiency. Before implementing Microsoft Teams Channels, most consultation communication used hospital-distributed handheld Spectra phones, answering services, pagers, or operator-mediated callback pathways. In this prior workflow, ED clinicians contacted a service-specific number or a paging pathway and waited for a return call from the consultant. This process relied on synchronous communication and was associated with frequent interruptions, misheard or misspelled patient identifiers, and limited ability to track or verify consult requests. The Microsoft Teams workflow was introduced to create a more consistent written pathway for consult requests while preserving phone-based escalation for urgent situations.
Intervention: Microsoft Teams Consultation Workflow
Implementation of Microsoft Teams Channels occurred in stages. Initially, ED clinicians received orientation to Microsoft Teams for internal communication and access to shared resources, which created familiarity with the platform. An ED leadership–driven training model was used to support troubleshooting, promote appropriate digital communication, and encourage adoption.
Dedicated Teams Channels approved for PHI-containing communication were created for specific consulting services in collaboration with system informatics and departmental leaders. Consulting clinicians could view and respond within their respective specialty channels. To initiate a consult, the ED clinician selected the appropriate specialty Channel and transmitted the patient’s name, location, brief diagnosis, callback number, and relevant clinical context. Consultants were expected to acknowledge receipt (for example, with “okay” or selecting the thumbs-up “like” button) within approximately 15–20 minutes. Life-threatening emergencies continued to be managed via direct phone calls or the activation of institutional emergency response pathways, and a lack of response on Teams reverted to the standard telephone workflow.
Survey Development
In January 2025, we developed a brief electronic survey to gather opinions and feedback regarding the Microsoft Teams consultation channels. A multidisciplinary group developed the survey, including ED attending physicians, advanced care providers (ACPs), residents, consulting physicians, nursing leadership, informatics staff, and quality improvement personnel. Items were derived from prior literature on secure clinical messaging and ED consultation workflows, as well as local workflow priorities, including documentation quality, timeliness of consultant responses, and interdepartmental communication needs. We used neutral item stems and balanced response options, such as improved workflow, no change, or interrupted workflow, and positive impact, no significant impact, or negative impact on patient care, to reduce wording bias and avoid preferentially cueing positive responses. Items were organized a priori into three conceptual domains: overall acceptability (satisfaction) with Microsoft Teams Channels, perceived impact on workflow, and perceived impact on patient care. The complete survey instrument is provided in Supplemental Table 1.
The instrument included three respondent-characteristic items, eight closed-ended experience items, and two free-text questions. Closed-ended experience items used three-category response scales tailored to each question. The brief response format was chosen to facilitate completion during clinical work. The two free-text questions asked about additional positive and negative workflow effects. The survey was created and administered using Microsoft Forms (Microsoft Corporation, Redmond, WA).
A small group of ED and consulting clinicians reviewed the draft survey for clarity and usability. Based on their feedback, we made minor wording and formatting changes before wider distribution. We did not perform formal psychometric validation, factor analysis, test-retest reliability assessment, or Cronbach’s alpha calculation, because the goal was to obtain a brief, pragmatic assessment of clinician perceptions rather than to develop a reusable multi-item scale.
Participants and Survey Administration
The survey was sent to ED clinicians, including attending physicians, physician assistants (PAs), and emergency medicine (EM) residents, to elicit their input on using Microsoft Teams for consultations. Additionally, the Email was sent to the chair or administrator of each consulting department, with a request to distribute it to all providers (residents, fellows, nurse practitioners, PAs, and attendings). All providers eligible to receive or respond to ED consultation requests via Microsoft Teams were invited to participate. Respondents were also asked to self-identify their clinical role and department. Within the ED, this invitation included 73 attending physicians, 40 ACPs, and 30 emergency medicine residents. Based on hospital credentialing data and departmental listserv rosters, the survey link was distributed to approximately 900–1000 non-ED consulting clinicians across services such as internal medicine, general surgery, neurology, cardiology, and other inpatient and on-call specialties. The survey was distributed via institutional Email using a link to a Microsoft Forms questionnaire and remained open for 22 weeks. Participation was voluntary and anonymous, and no incentives were provided.
The survey was initially forwarded to each department’s Email listserv in the middle of the month, with a reminder sent two weeks later. Participants responded by clicking the Microsoft Forms survey link, and data were collected anonymously. No identifying information was requested. The survey was sent out to all managers twice, about two weeks apart. Another Email was sent approximately three months later to all ED staff, providing an additional opportunity to respond. Because responses were anonymous, duplicate submissions could not be formally excluded; all completed surveys were retained for analysis.
Measures and Data Analysis
The primary measures were responses to eight closed-ended experience items addressing satisfaction, perceived workflow impact, ease of initiating or receiving a consultation, self-rated proficiency, ease of reaching the consulting team, preferred communication method, frequency of response delays, and perceived impact on patient care. The two free-text items asked respondents to describe additional positive and negative effects of the Teams workflow.
Survey responses were collected electronically via Microsoft Forms and exported to Microsoft Excel (Microsoft Corporation, Redmond, WA) for analysis. All quantitative analyses were performed in Microsoft Excel. Data were stored on institutional systems with access restricted to the study team. Analyses were primarily descriptive and exploratory rather than designed to test prespecified hypotheses. We summarized Likert-scale items using descriptive statistics, including counts and percentages for each response option. Where appropriate, categories were collapsed (eg, agreement vs non-agreement) to describe overall trends. Partially completed surveys were included in the analysis, and item-level denominators are reported to reflect missing responses. Free-text responses were reviewed qualitatively using an inductive content analysis approach. Two investigators independently reviewed and coded responses, identified recurring themes (such as perceived advantages, challenges, and suggestions for improvement), and resolved discrepancies by discussion.
Because the estimated response rate among non-ED clinicians was very low, the study’s primary interpretation focused on responses from ED clinicians. Non-ED responses were retained to provide descriptive context but were not used to support primary conclusions about multidisciplinary acceptability. ED versus non-ED comparisons are presented descriptively in Supplemental Table 2 and should be interpreted as exploratory and potentially subject to substantial response bias. We did not adjust p-values for multiple comparisons, and inferential testing, where reported, should be interpreted as descriptive rather than confirmatory.
Results
Respondent Characteristics
Of the 121 respondents, 82 (67.8%) were ED clinicians, and 39 (32.2%) were clinicians from non-ED consulting services (Table 1). Among ED respondents (n = 82), 49 (59.8%) were attending physicians, 18 (22.0%) were ACPs, and 15 (18.3%) were resident physicians. Among non-ED respondents (n = 39), 15 (38.5%) were attending physicians, 13 (33.3%) were ACPs, 8 (20.5%) were resident physicians, and 3 (7.7%) were fellow physicians. Because the hospital-wide denominator was estimated from listserv and credentialing data, the overall institutional response rate was estimated to be below 10%. Within the ED specifically, staffing includes 73 attending physicians, 40 ACPs, and 30 residents, yielding an approximate ED response rate of 57% and capturing the majority of the ED physician and ACP workforce. In contrast, departmental listserv rosters indicate that Teams-eligible non-ED consultants substantially outnumbered the 39 non-ED respondents. Therefore, non-ED responses are reported descriptively only and are not used to support primary conclusions about multidisciplinary acceptability.
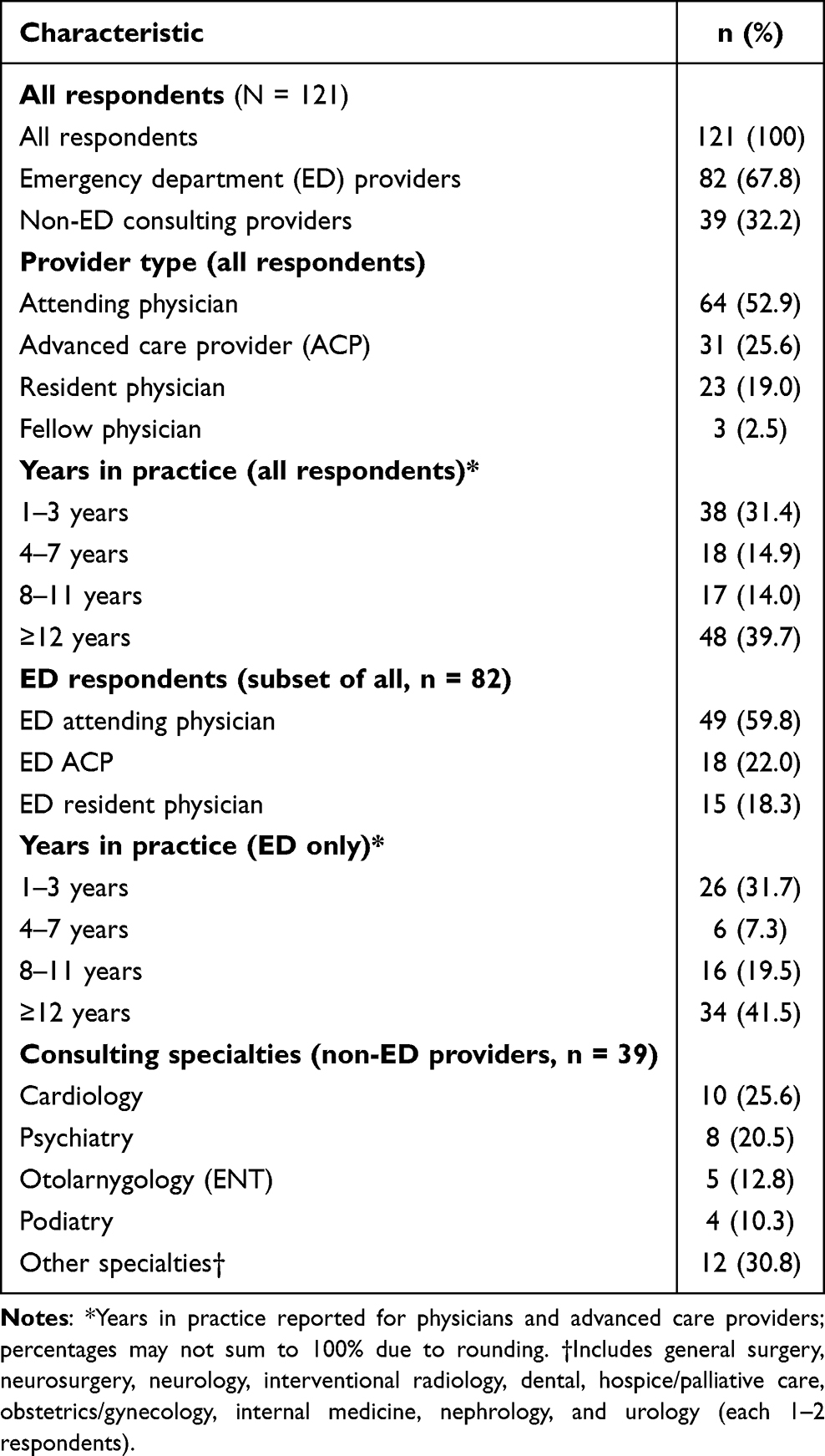 |
Table 1 Characteristics of Survey Respondents |
ED Clinician Acceptability, Workflow, and Perceived Patient-Care Impact
Table 2 summarizes key survey outcomes by provider group. Among ED respondents, overall acceptability was high: 78.0% rated their satisfaction as 3 (satisfied), and none selected 1 (not satisfied). Most ED respondents also reported perceived workflow benefit, with 85.4% stating that Teams improved their workflow compared with the prior Spectra-based pathway (Figure 1). Non-ED responses are shown in Table 2 and Supplemental Table 2 for descriptive context only.
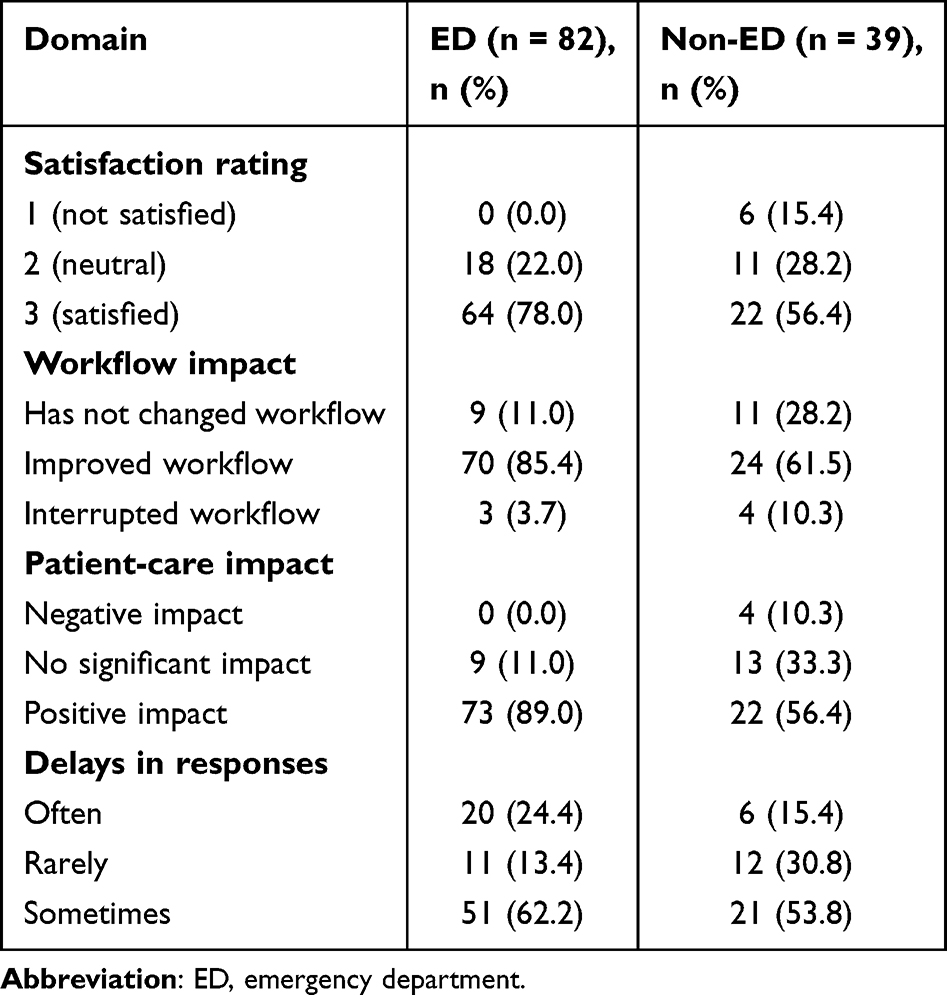 |
Table 2 Survey Outcomes Among ED vs Non-ED Providers |
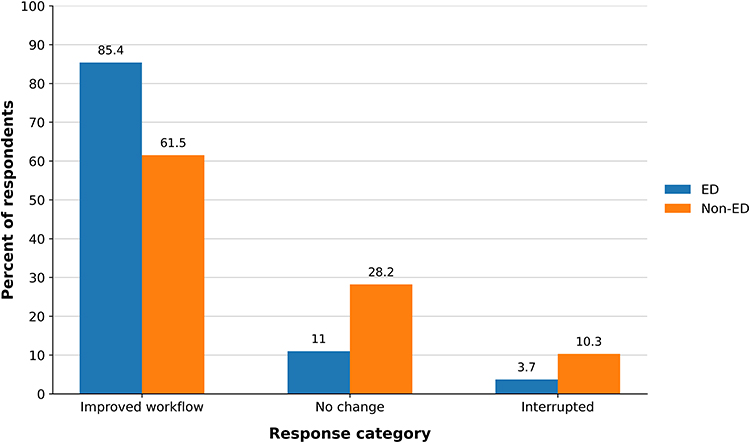 |
Figure 1 Workflow impact of Microsoft Teams vs Spectra. |
Among ED respondents, 89.0% believed that Teams had a positive impact on patient care, 11.0% reported no significant effect, and none reported a negative impact (Figure 2). These findings reflect perceived patient-care impact rather than measured clinical outcomes. Non-ED responses are shown descriptively in Table 2 and Supplemental Table 2.
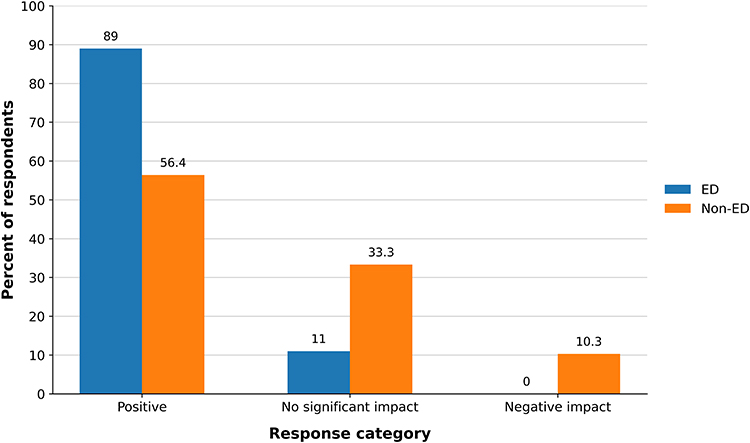 |
Figure 2 Perceived impact of Microsoft Teams on patient care. |
Delays in Teams-Based Consultation Responses
Delays in responses using Teams were common in both groups (Table 2). Most ED and non-ED respondents reported that they “sometimes” encountered delays, and 20 of 82 ED respondents (24.4%) and 6 of 39 non-ED respondents (15.4%) reported “often” encountering delays. Detailed ED-only distributions for individual survey items and delay frequency are provided in Supplemental Tables 3 and 4. Because non-ED responses were limited, delay findings are interpreted primarily from the ED clinician’s perspective.
Usability and Preferred Communication Pattern
Among ED respondents, Teams was generally rated as easy to use and familiar. Detailed ED-only distributions for individual survey items are provided in Supplemental Table 3. Across the full respondent group, Teams-favorable communication patterns were common, but non-ED responses were limited and are reported descriptively only. Overall, 49.6% of respondents preferred a combination of Teams and Spectra phones, 39.7% preferred to continue communication via Teams after the initial consult, and 10.7% preferred Spectra-based communication after the initial consult.
Free-Text Comments on Workflow and Communication
Free-text responses provided additional context regarding perceived effects on workflow. Positive comments frequently described reduced “phone tag”, clearer and timestamped documentation of consultation requests (“I like that everything is written and timestamped”), and the ability to review and respond to messages asynchronously while managing other tasks. Negative comments commonly cited missed or delayed notifications when not actively monitoring devices, reliance on personal phones and battery life, increased message volume, and concerns that, for time-critical emergencies, direct telephone calls or existing escalation pathways remained preferable to Teams-based communication (“Sometimes it feels like messages sit for a long time before anyone responds”). Because this was not a formal qualitative study, these comments should be viewed as illustrative rather than definitive qualitative findings.
Discussion
Communication failures in the ED can contribute to delays and adverse events. In this single-center post-implementation survey, ED clinicians reported high perceived acceptability of an EMR-adjacent Microsoft Teams consultation workflow used alongside a telephone-based consultation pathway. Most ED respondents perceived that Teams improved workflow and patient care compared with their prior Spectra-only experience. Delayed responses, notification burden, and continued reliance on fallback telephone communication remained common. These results describe ED clinician perceptions and do not show that Teams improved consultation timeliness, patient flow, or clinical outcomes. Because responses from consulting clinicians were limited, this study cannot determine multidisciplinary acceptance of the workflow. It also cannot evaluate the effectiveness of the consultation process as a two-sided interaction, because the experience of consulting services was not adequately represented.
Our findings are consistent with prior work suggesting that electronic and mobile communication tools may improve perceived efficiency and documentation while also increasing message volume. However, unlike studies of EMR-integrated tools such as Epic Secure Chat or integrated consult orders, the workflow described here used Microsoft Teams as an EMR-adjacent platform rather than a native EMR function. EMR-integrated tools may offer advantages for documentation and direct linkage to the medical record. In contrast, EMR-adjacent channel-based platforms may support shared visibility across teams, persistent service-specific threads, and multidisciplinary participation. This study does not show that Teams is superior to EMR-integrated secure chat or telephone-based consultation; it describes one ED’s use of Teams as an adjacent consult pathway.
Free-text comments showed why some ED clinicians valued the Teams workflow. ED clinicians commonly described value in having a timestamped written record of consult requests and responses, fewer repeated phone calls, and the ability to review messages across shifts. In practice, a shared thread can make it easier to clarify recommendations and confirm plans, although we did not measure closed-loop communication, communication errors, missed recommendations, medication-order discrepancies, or discrepancies between Teams messages and EMR documentation. These comments should therefore be interpreted as perceived workflow advantages rather than evidence of improved communication safety.
The same workflow also created familiar problems seen with other secure messaging systems, including delayed replies, message volume, and notification volume.9 Despite high ratings for ease of use, a substantial proportion of ED respondents reported that reaching consultants for additional information was only moderately easy, and relatively few felt that delays in care due to consultant response times were rare. Qualitative feedback noting “over usage resulting in watered down communication” suggests that constant access may contribute to information overload or weaken perceived urgency when expectations for responsiveness are not clearly defined. This highlights that secure messaging can change the format of communication without necessarily solving the operational problem of consultant responsiveness.
For ED leaders considering EMR-adjacent messaging tools, the operational lesson is straightforward. Teams may be acceptable to ED clinicians and may make consult requests easier to track, but the workflow needs clear rules. Institutions should define which services use Teams, expected response times, escalation steps for unanswered messages, documentation expectations in the EMR, and situations in which direct phone calls or emergency response pathways remain mandatory. Non-ED clinician responses in this study were limited and should be treated as signals for further study rather than representative estimates of consultant experience.
A stronger evaluation would link clinician perceptions with objective workflow and patient-level data. Future studies should use consult-level Teams timestamps to measure time from request to acknowledgment and from acknowledgment to consultant evaluation. They should also examine ED length of stay, communication errors, and agreement between Teams messages and EMR documentation. These data would show whether shorter response times, shorter ED stays, or fewer communication and documentation errors accompany perceived communication benefits. Multicenter studies could assess whether these patterns are reproducible across institutions, consultation models, and EMR systems. Studies focused on consulting services could clarify barriers to timely responses, preferred notification workflows, and specialty-specific use cases. A more complete evaluation would require adequate consultant participation and objective measures of response time, communication quality, and workflow impact from both sides of the consultation.
Limitations
This study was conducted at a single academic ED, which limits generalizability to hospitals with different staffing models, consultant structures, or communication systems. Response rates were uneven across groups. Within the ED, approximately 57% of eligible physicians and ACPs responded, so the findings likely reflect the views of much of the ED clinician workforce and should be interpreted as primarily ED-focused. In contrast, the denominator for Teams-eligible non-ED consultants was substantially larger than the number of non-ED responses, so consultant views are likely under-represented. Non-ED results should therefore be viewed as exploratory. Because consultation is a two-sided process, the limited consultant response prevents the workflow from being assessed by both participating groups. The study, therefore, describes the ED clinician’s perspective rather than the effectiveness of the full consultation workflow. Selection bias is likely because clinicians with strong positive or negative opinions may have been more likely to complete the survey. The workflow was developed and promoted by ED leadership, which may also have influenced both adoption and survey responses. ED clinicians may have been more likely to view the intervention favorably because it originated within their department. Although the survey was anonymous, this does not eliminate the possibility of social desirability or sponsorship bias. These institutional factors further limit generalizability to hospitals with different implementation models. Comparisons between ED and non-ED respondents should therefore be interpreted cautiously and considered hypothesis-generating. Although Teams was deployed through an institutionally approved enterprise environment for PHI-containing communication, it was not integrated with the EMR, and Teams messages were not part of the legal medical record. This limits generalizability to hospitals that rely primarily on EMR-integrated secure chat tools and reinforces the need for formal EMR documentation of consultation recommendations.
The survey instrument also limits interpretation. We used a three-point Likert scale to keep the survey brief and maximize completion, but this limited the granularity of responses. Although items were derived from prior literature and local workflow priorities and reviewed by a multidisciplinary group, we did not perform formal psychometric testing, such as factor analysis or Cronbach’s alpha. The domains of satisfaction, workflow, and perceived patient-care impact are, therefore, face-valid groupings rather than validated subscales.
All improvement findings are retrospective perceptions relative to the prior Spectra-only workflow, not measured pre- and post– changes. We cannot determine whether perceived communication benefits translated into operational or clinical gains. The available dataset did not include consult-level Teams time stamps, patient identifiers, ED length of stay, communication errors, or paired Teams and EMR documentation. We therefore could not evaluate consultation response times, patient flow, communication safety, or documentation concordance. The survey also did not assess burnout, cognitive load, closed-loop communication, missed recommendations, or the downstream effects of increased messaging on interruptions and workload. These limitations preclude causal inferences about the effect of Teams on operational performance or patient outcomes. The results are best viewed as hypothesis-generating.
Conclusions
In this single-center post-implementation survey, ED clinicians reported high perceived acceptability of an EMR-adjacent Microsoft Teams consultation workflow used alongside a telephone-based consultation pathway. These results reflect clinician perceptions, not objective evidence of improved consultation timeliness, patient flow, or clinical outcomes. Delays, notification burden, and continued telephone escalation show that secure messaging still needs response-time expectations, governance, and clear EMR documentation practices.
AI Statement
AI was used to assist with language editing and manuscript organization. It was not used for data analysis, statistical testing, generation of results, or scientific interpretation. All content was reviewed and revised by the authors, who take full responsibility for the final manuscript.
Ethics and Consent to Participate
The Northwell Health Institutional Review Board approved this study (Protocol #23-0372). Participation was voluntary, and responses were collected anonymously.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Best J. Slow death of the bleep: why hospital pagers won’t die. BMJ. 2021;372:n684. doi:10.1136/bmj.n684
2. Luu T, Spiegelman L, Nykin D, et al. Implementation of an electronic health record-based messaging system in the emergency department: effects on physician workflow and resident burnout. J Patient Saf. 2022;18(2):e542–10. doi:10.1097/PTS.0000000000000869
3. Baratta LR, Harford D, Sinsky CA, et al. Characterizing the patterns of electronic health record-integrated secure messaging use: cross-sectional study. J Med Internet Res. 2023;25:e48583. doi:10.2196/48583
4. Lawson L, Barros RDM, Evans J, et al. Being a ‘Teams’ player: a quality improvement project expanding the role of Microsoft Teams to improve communication and efficiency of junior doctors in a ward-based hospital setting. Future Healthc J. 2023;10(Suppl 3):89–90. doi:10.7861/fhj.10-3-s89
5. Jung KY, Kim S, Kim K, et al. Frequent mobile electronic medical records users respond more quickly to emergency department consultation requests: retrospective quantitative study. JMIR Mhealth Uhealth. 2020;8(2):e14487. doi:10.2196/14487
6. Ravi A, Shochat G, Wang RC, et al. Improvements to emergency department length of stay and user satisfaction after implementation of an integrated consult order. J Am Coll Emerg Physicians Open. 2023;4(2):e12922. doi:10.1002/emp2.12922
7. Hoonakker PLT, Carayon P, Cartmill RS. The impact of secure messaging on workflow in primary care: results of a multiple-case, multiple-method study. Int J Med Inform. 2017;100:63–76. PMID: 28241939; PMCID: PMC8365630. doi:10.1016/j.ijmedinf.2017.01.004
8. Siemieniak S, Dehaan S, Matlock A. Evaluating the impact of emergency department length of stay in a military training hospital following the implementation of a standardized paging system. Cureus. 2024;16(6):e62102. doi:10.7759/cureus.62102
9. Lou SS, Lew D, Baratta LR, et al. Secure messaging and telephone use for clinician-to-clinician communication. JAMA Network Open. 2024;7(6):e2417781. doi:10.1001/jamanetworkopen.2024.17781
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.