Back to Journals » International Journal of Women's Health » Volume 14
Emergency Contraceptive Pill Use and its Impact on Condom Utilization Among University Students: A Cross-Sectional Study
Authors Genemo ES, Korsa AT ![]() , Bayisa HG
, Bayisa HG
Received 29 May 2022
Accepted for publication 3 August 2022
Published 18 August 2022 Volume 2022:14 Pages 1115—1126
DOI https://doi.org/10.2147/IJWH.S375841
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Edao Sado Genemo,1 Ayana Tadesse Korsa,2 Habte Gebeyehu Bayisa2
1Department of Pharmacy (Pharmacoepidemiology and Social Pharmacy Unit), Institute of Health Sciences, Wollega University, Nekemte, Ethiopia; 2Department of Pharmacy (Clinical Pharmacy Unit), Institute of Health Sciences, Wollega University, Nekemte, Ethiopia
Correspondence: Ayana Tadesse Korsa, Department of Pharmacy, Institute of Health Sciences, Wollega University, P.O Box 395, Nekemte, Ethiopia, Tel +251912143175, Email [email protected]; [email protected]
Purpose: Emergency contraceptive pills (ECPs) prevent unplanned pregnancy but not sexually transmitted infections (STIs), and the practice of ECP may affect condom use. This study, therefore, aimed to assess ECP use and its impact on condom utilization among female students of private universities in Nekemte town, western Ethiopia.
Methods: An institution-based cross-sectional study was conducted on 400 female students in three different private universities from February 1 to 28, 2019. Study samples were selected through simple random sampling technique. Data collected from a structured self-administered questionnaire were analyzed using SPSS version 23.0. Bivariate and multivariate logistic regression were performed to determine factors associated with condom utilization, and statistical significance was set at 95% confidence interval (CI) using a p-value of < 0.05 as a cutoff point.
Results: The response rate was 95.3% (381/400). Overall, 51.4% (196/381; 95% CI = 45.1%, 57.7%) had awareness of ECP. Besides, 186 (48.8%) students reported history of sexual intercourse, of which 115 (61.8%) have ever practiced ECP and 96 (51.6%) have ever used condom. However, only 11 (5.9%) have ever utilized ECP and condom concurrently. Use of ECPs (adjusted odds ratio (AOR) = 0.32; 95% CI = 0.164, 0.632; p = 0.001), belief that condom prevents STI (AOR = 3.17; 95% CI = 1.045, 8.646; p = 0.041) and thought that ECP does not prevent STI (AOR = 2.217; 95% CI = 1.172, 4.59; p = 0.032) had statistically significant association with condom utilization.
Conclusion: The practice of ECP was average, while dual method contraception use was low in the study area. History of ECP use and beliefs that ECP is not effective to prevent STI or condom protects against STI were factors associated with condom use.
Keywords: condom, emergency contraception, female students, Nekemte
Introduction
The emergency contraceptive pill (ECP) is a hormone contraceptive used to prevent unintended pregnancy that may occur after unprotected sexual intercourse.1 The ECPs include combined estrogen and progestin pills, progestin-only pills and ulipristal acetate (UPA).1,2 All ECP types can decrease the risk of unintended pregnancy and unsafe abortion by 75% to 85% when used correctly within 72 hours of sexual intercourse.3,4
Unintended pregnancy and abortions have become global public health issues.5 Global estimates show that 121 million unintended pregnancies on average occurred each year between 2015 and 2019 of which around 73 million (61%) ended in induced abortions among women aged 15–49 years worldwide.5,6 Sub-Saharan Africa had the highest incidence of unintended pregnancy (91/1000 women) and abortion rate was 37%.5 In Ethiopia, the overall prevalence of unintended pregnancy was estimated at 28%; 2,060,000 pregnancies were unintended and 632,000 (31%) ended in abortions.7,8 According to World Health Organization (WHO), at least 10 million unintended pregnancies and an estimated 5.6 million abortions occur each year among adolescent girls aged 15–19 years in the developing world.43 Similarly, about one third (31.8%) of unmarried female university students experienced unintended pregnancies in many China universities.44 In sub-Saharan Africa, the prevalence of unintended pregnancy among young women (15–24 years of age) ranged from 9.4% to 59.6% with a rate of 34.9% in Ethiopia.45
Effective contraception has a lion’s share in reducing incidence of unintended pregnancies and induced abortions.2,7,14 ECPs are used with a wide range of prevalence among sexually active women, worldwide.2–4,9 For instance, certain multinational analysis of ECP use indicated that the proportions of ECP use varies from below 0.1% in Chad to 12% in Colombia.10 Other studies also reported that the magnitude of ECP practice among female university students varies across countries in Africa: 21.2% in South Africa,11 20% in Kenya12 and 15.2% in Nigeria.13 The Ethiopian Demographic Health Survey of 2016 (EDHS 2016) reports showed that practice and knowledge of emergency contraception was 4% and 19%, respectively among Ethiopian women aged 15–49.14 Also, the rate of ECP use among female university students ranges from 4.9–78.1% with a pooled prevalence of 34.5%, according to a recent systematic review conducted in the country.15
Hormonal contraceptives including ECP are very effective in preventing unintended pregnancy but not human immunodeficiency virus (HIV) and other sexually transmitted infections (STIs).9,16 Apart from abstinence, condom is the only method which gives protection against HIV and other STIs.1 If used consistently, condom can provide dual protection against unplanned pregnancy and STIs.16–18 However, studies have shown that females who practice ECP do not necessarily utilize condoms for STI prevention.17–20 To illustrate, according to the Canadian contraception study of 2002, concurrent use of condoms was indicated only by 13% of oral contraceptive users20 and only 11% of women with or at high risk of HIV had used both contraception methods in another study.18 On the other hand, only small proportions (7% to 10%) reportedly used condoms primarily to prevent STIs17,20 and prevalence of STI among female university students was 26.3% in Sweden,46 27.7% in Southern Nigeria47 and ranged 6.4% to 18.2% in Ethiopia.24,26
Although the direct relationship between ECP use and acquisition of STI is not established, studies suggested that unrestricted access to ECP leads to increase sexual risk behaviors and STIs.16–21 Moreover, there is a rising concern to understand whether the increasing access to ECP impose negative impact on condom use and escalate STI rates.16,19,22,23 For instance, condom use decreased from 49% to 41% between 2009 and 2014 among female university students in Sweden,48 the prevalence of unprotected sex (non-use of condom), despite knowing its consequences, was very high (60.7%) among female undergraduate students in Nigeria49 and the majority (52.2%) of female students in Ghana preferred ECP to condoms to prevent pregnancy and STIs.34 Likewise, among female university students in Ethiopia, non-use of condom was highly prevalent (57.2%) and significantly associated with acquisition of STIs;24 inconsistent condom use was 66.2%, the odds of inconsistent condom use was more than two-fold in female students than in males and private university students were more susceptible to risky sexual behaviors than public university students.25
Although both condom and ECPs are available over-the-counter (OTC) and ECPs are more expensive than condom, ECPs are more often and repeatedly used by young women (those aged between 15–25 years), according to other studies conducted in Ethiopia.50,51 It was also stated that young females only care about preventing pregnancy and have forgotten about STIs/HIV, thus neglecting condom use.50 Besides, the key stakeholders were uncomfortable with high sales of ECPs50 and pharmacists expressed concerns that the use of ECPs will lead to irresponsible behavior among young people and reduced condom use.51
It is evident that investigating the effects of ECP use on condom utilization is important to realize sexual risk behaviors in youths.19,23,25,29 Pertaining to this issue, our comprehensive literature search indicated only two studies previously conducted in the country.26,27 Nonetheless, as far as our knowledge is concerned, no research has been done in our study area. Nekemte, one of the biggest towns in western Ethiopia, is home for one federal university and several private universities and colleges. Most students come from surrounding areas and neighboring regional states to study while they live away from their families. Thus, they could highly engage in risky sexual behaviors due to a sense of independence from restrictions and parental impact.25 Therefore, this study was aimed to assess the knowledge, attitude and practice of ECP and the impact of ECP use on condom utilization among female students of different private universities in Nekemte town, western Ethiopia. The findings of this study would help to devise strategies to promote dual method contraception for protections against unintended pregnancy and STIs.
Methods
Study Settings and Period
This study was conducted from February 1 to 28, 2019 among female students who were studying in different private universities found in Nekemte town, which is located 331 km to west of Addis Ababa, the capital city of Ethiopia. Generally, there were three private universities in the town when the study was conducted. These universities are Rift Valley University (RVU), New Generation University (NGU) and Dandi Boru University (DBU). They enroll students in regular, evening and weekend modalities, and majority of their students come from surrounding areas.
Study Design
An institution-based cross-sectional study was conducted to assess ECP use and its impact on condom utilization among female students pursuing undergraduate studies in the mentioned settings.
Study Population
A total of 2153 undergraduate female students who were regularly enrolled in the respective universities during the study period were considered as the study population.
Sample Size Determination and Sampling
A single population proportion formula was used to calculate the minimum sample size with the following assumptions: ECP utilization of 47% (P = 0.47) from a previous study of female university students in Ethiopia,26 95% confidence interval (CI), 5% margin of error (d = 0.05) which yielded a sample size of 382 students. After adding 5% compensation for non-response rate, the final target sample size of approximately 400 students was determined.
Out of the total 2153 female students mentioned earlier, 1114 (51.7%) were from RVU, 646 (30%) were from NGU, and 393 (18.3%) were from DBU. Accordingly, study participants were allocated to each university proportional to the size of female students they had. Thus, 207 students from RVU, 120 students from NGU and 73 students from DBU were randomly selected and included to the study. A simple random sampling technique was employed to select samples by using the list of female students in each university as a sampling frame.
Data Collection Process
A pre-tested and structured self-administered questionnaire was used to collect data for this study. We thoroughly reviewed similar surveys conducted in the country,26–28 to prepare the instrument. The questionnaire was categorized into different sections including socio-demographic characteristics, sexual and reproductive health profiles, knowledge, attitude and practice of ECP use and condom utilization. It was initially developed in English language and then translated to Afaan Oromo (a commonly spoken language in the study area). The translated questionnaire was cross-checked by an independent language professional for consistency ahead of using. Subsequently, it was pretested among 20 female students (5% of the sample size) who did not participate in the study. Data were collected by three BSc Nursing holders who were employees of public health institutions in the town. Data quality was assured through pre-testing, training of data collectors prior to their deployment, checking filled data for completeness and accuracy and daily on-site supervision by the research investigators.
Data Management and Analysis
Data were coded and entered into Epi Data version 3.1 and then, exported for analysis to statistical package for social sciences (SPSS) for windows version 23.0. Descriptive statistics was used to describe socio-demographics, sexual and reproductive health profiles, knowledge and level of ECP use as well as condom use. On the other hand, both bivariate and multivariate logistic regression analyses were computed to determine factors associated with condom utilization. Variables with a p-value of ≤ 0.05 in the bivariate analysis were put into the multivariate logistic regression model to adjust for confounding. Preceding to the multivariate analysis, multicollinearity diagnostic was executed and there was no major interaction between the explanatory variables. In the multivariate analysis, AOR with 95% CI was calculated and statistical significance was determined using a p-value of <0.05 as a cut-off point.
Operational Definitions
Ever use of ECP: proportion of sexually active female students who used ECP for contraception whenever they had sexual intercourse before the survey.
Ever use of condom: proportion of sexually active female students who utilized condom whenever they had sexual intercourse before the survey.
Ever use of condom and ECP: proportion of sexually active female students who used both condom and ECP whenever they had sexual intercourse before the survey.
Non-use of ECP: proportion of sexually active female students who never used ECP whenever they had sexual intercourse before the survey.
Results
Socio-Demographic Characteristics of the Respondents
A total of 381 students completed the questionnaires making a response rate of 95.25%. The mean (±SD) age of the respondents was 20.5 (±2.51) years. Approximately half (48.5%) of the total respondents were within the age group of 20–24 years. Nearly ninety percent (87.9%) of the students were ethnically Oromo and 217 (57%) were followers of protestant religion. Majority (90.6%) of the students were unmarried and more than half (55.9%) were originally from urban areas (Table 1).
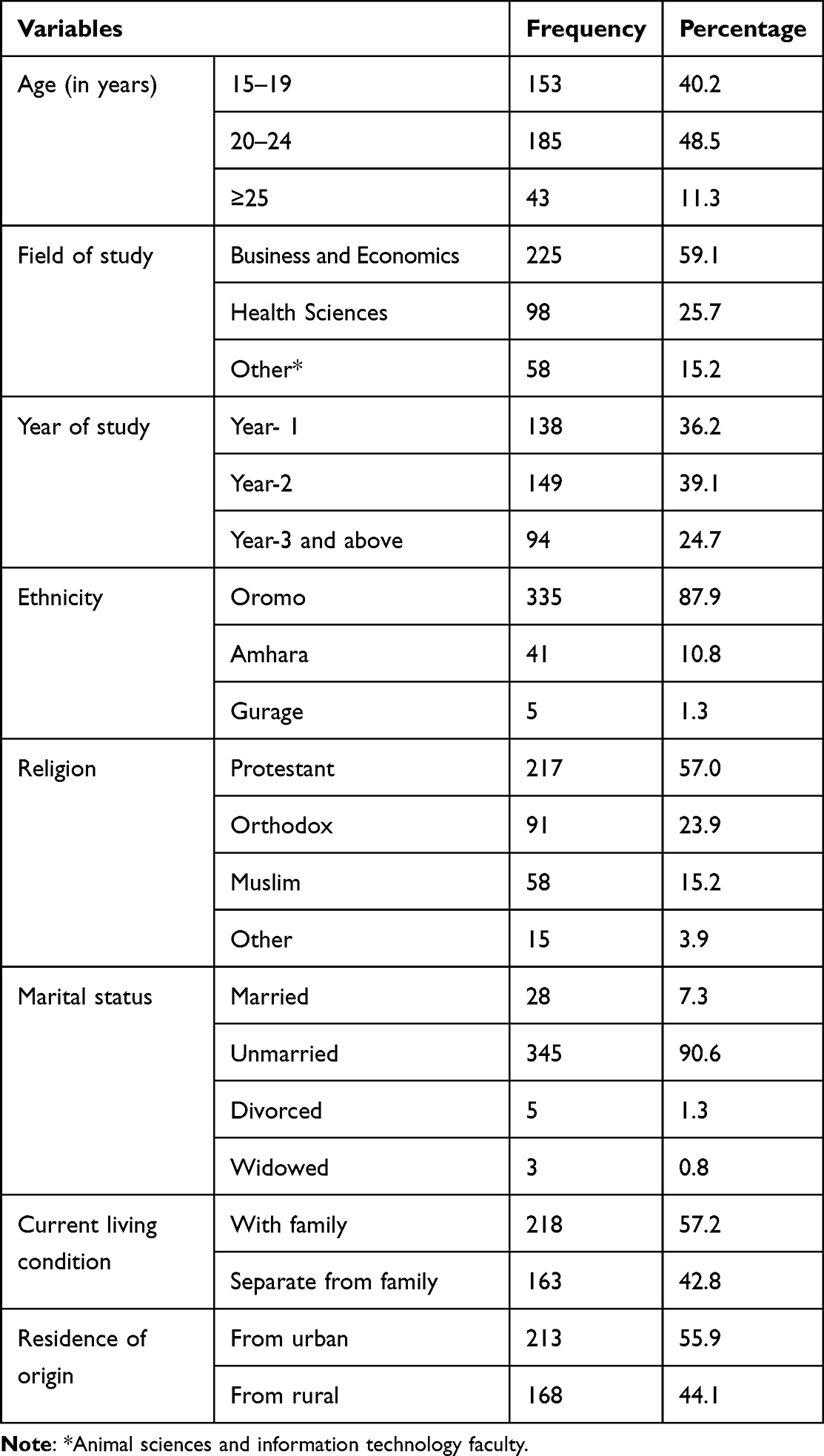 |
Table 1 Socio-Demographic Characteristics of Female Private University Students in Nekemte Town, February, 2019 (n = 381) |
Sexual and Reproductive Health Characteristics of the Respondents
The results revealed that 186 (48.8%) students out of the total participants have ever had sexual intercourse. Accordingly, more than four-fifth (81.7%) had their first sex at the age of ≤ 20 years, 82 (44.1%) reported first sex with a casual friend and 83 (44.6%) indicated sexual desire as the main reason to have first sex. The mean (±SD) age at first sex was 17.02 (±1.53) years. Also, the majority (61.3%) had sex with two or more sex partners and 36 (19.4%) reported history of STIs (Table 2).
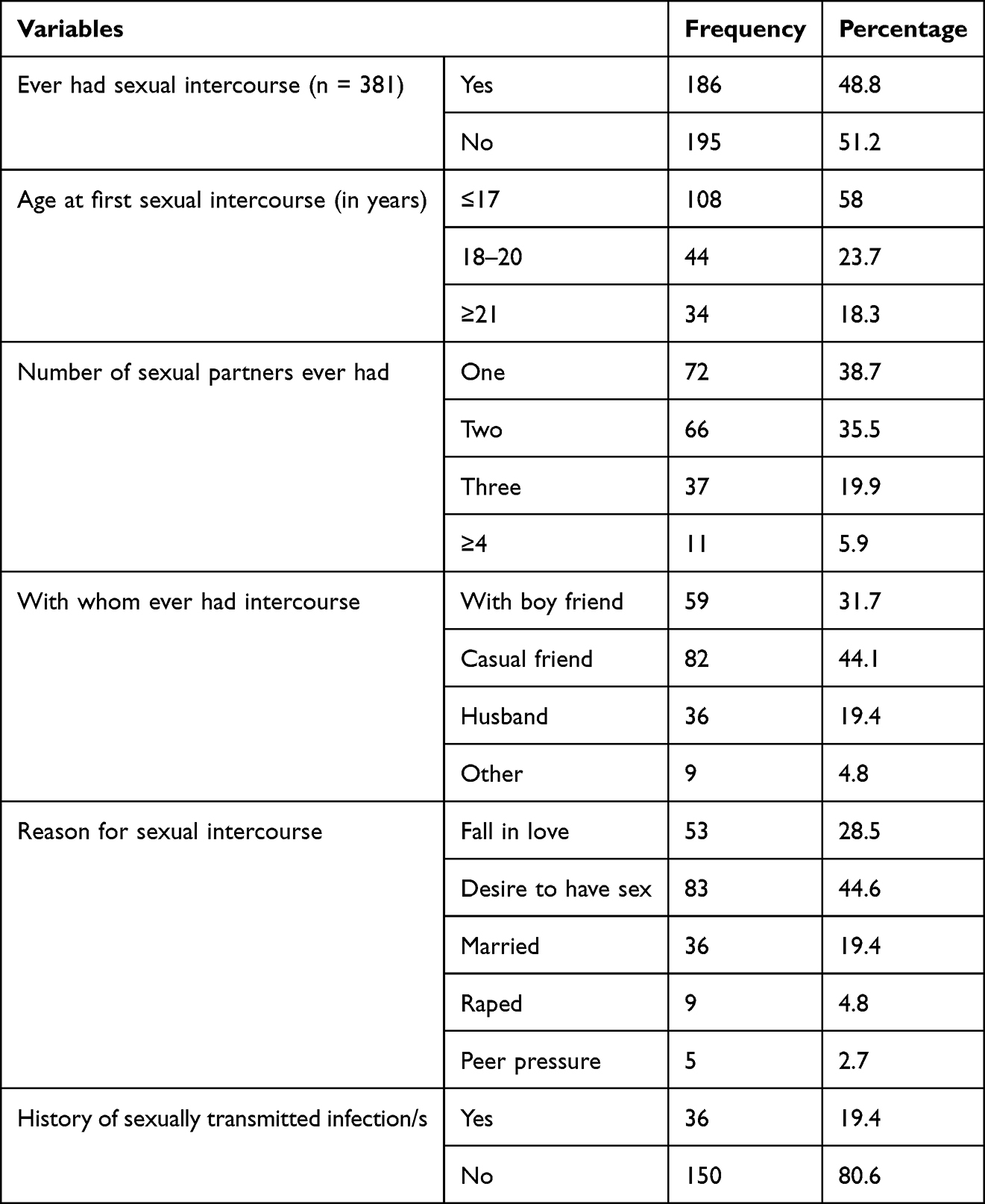 |
Table 2 Sexual and Reproductive Health Characteristics of Female Private University Students in Nekemte Town, February, 2019 (n = 186) |
Knowledge, Attitudes and Practice of Contraception
Out of the total respondents, 196 (51.4%; 95% CI, 45.1–57.7%) and 210 (55.1%; 95% CI, 47.7–62.5%) have ever heard about ECP and condom, respectively. Among the students who had awareness of ECP, 111 (56.6%) correctly answered the right time to take ECP (within 72 hours of having unprotected sex), whereas 94 (47.9%) of them thought that ECP can prevent STIs. On the other hand, 98 (46.7%) female students, among those who knew about condom, believed that it protects against STIs (Table 3).
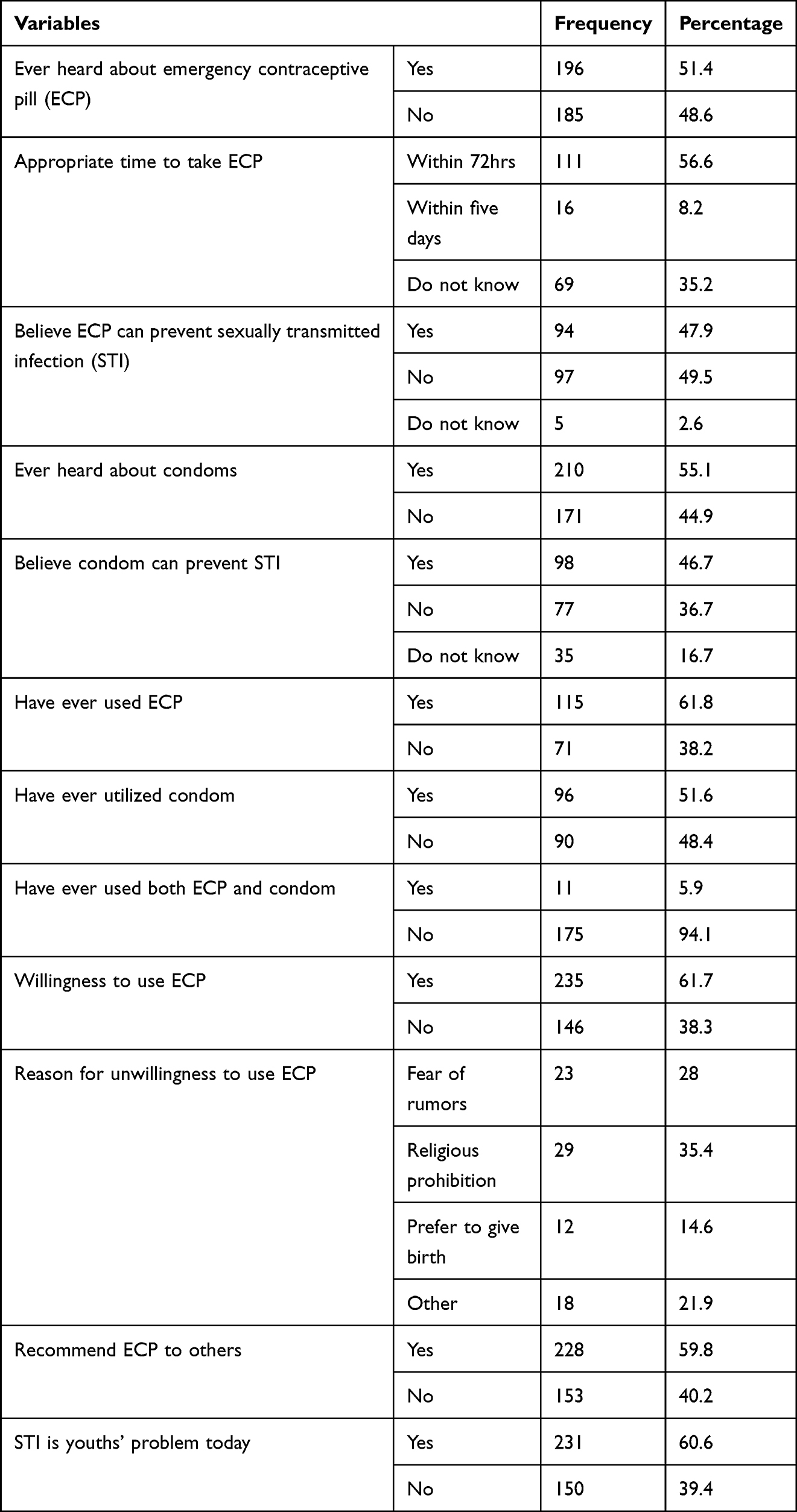 |
Table 3 Knowledge, Attitudes and Practice of Contraception Among Female Private University Students in Nekemte Town, February, 2019 |
Amongst the respondents who had history of sexual intercourse, 115 (61.8%) and 96 (51.6%) have ever used ECP and condom, respectively; only 11 (5.9%) have ever utilized both methods concurrently (Table 3).
About two-third (61.7%) of the respondents showed willingness to use ECP whenever they need to; also, 228 (59.8%) of the students agreed to recommend ECP to other persons (Table 3).
Factors Associated with Condom Utilization
The findings of bivariate analysis revealed that awareness of ECP, practice of ECP, beliefs that ECP can prevent STI, that condom can protect against STI and STI is a problem of young people had statistically significant association with condom utilization. However, in multivariate analysis, only three factors including ever practice of ECP, beliefs about ECP can prevent STI and condom protects against STI were remained statistically significant. Accordingly, sexually active female students who have ever practiced ECP were 0.32 times less likely to utilize condom than the ones who did not use ECP (AOR = 0.32; 95% CI, 0.164–0.632). Conversely, female undergraduates who believed that ECP does not prevent STI were just above 2 times more likely to use condom when compared to those who thought it does (AOR= 2.217; 95% CI, 1.172–4.59). Further, female students who said that condom effectively prevents STI had 3 times more chance to practice condom than their counterparts who believed oppositely (AOR= 3.17; 95% CI, 1.045–8.646) (Table 4).
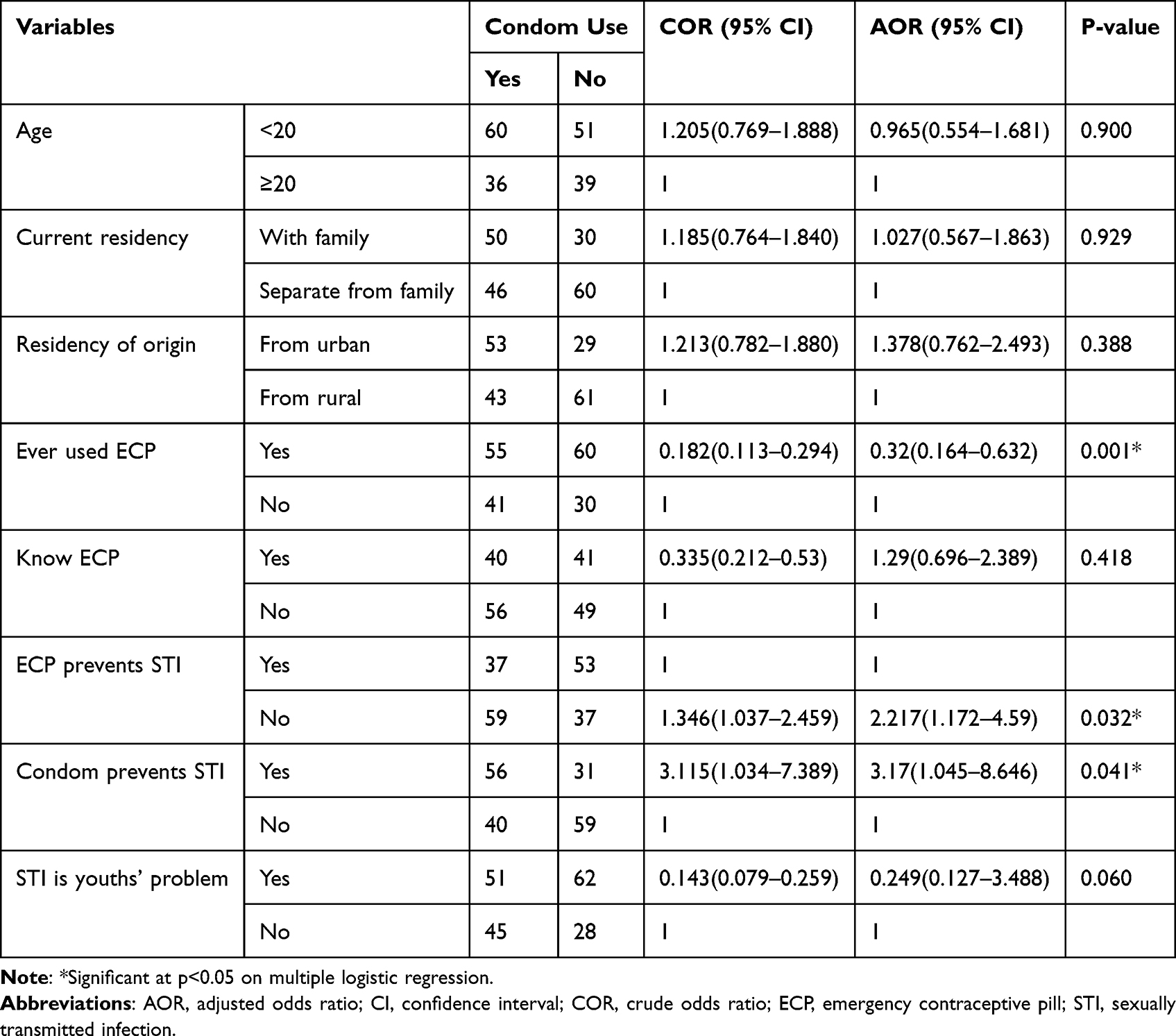 |
Table 4 Factors Associated with Condom Utilization Among Female Private University Students in Nekemte Town, February, 2019 (n = 186) |
Discussion
There is a growing concern regarding the increasing access to and use of ECP and its potential impact on sexual risk taking behaviors and STIs.18–23,26,29 In lieu of this, the present study examined the practice of ECP and its influence on condom use among female students of private universities in Nekemte town, western Ethiopia.
In this study, more than half (51.4%; 95% CI, 45.1–57.7%) of the respondents had awareness of ECP. This is lower than the reports of previous studies conducted in different universities of Ethiopia (67% to 95.9%)26–28,30,31 and Kenya (86.4%)12 but much higher than that of a Nigerian university (14.6%).13 It is consistent with results from a South African university (49.8%).11 Rate of sexually active women, accessibility of information on contraception, sexual and reproductive health education, socio-cultural differences and level of urbanizations of the study areas might be accountable for the discrepancy.10,15,22
According to this study, ECP was utilized by the majority (61.8%) of female undergraduates who had history of sexual intercourse. This figure is higher than previous reports from different universities of African countries such as South Africa (21.2%), Kenya (20%), Nigeria (15.2%) and Rwanda (5%).11–13,32 Similarly, lower results were reported among female university students in Ethiopia that ranged from 4.7% in Adama to 47.1% in Northwest Ethiopia.26,27,30,33 Awareness of ECP, availability and accessibility of ECP in community, perceived risk of pregnancy as well as denominators used for calculations of ECP use might explain the disagreement.
We also found that a substantial proportion of the respondents would use ECP when needed and would recommend it to other persons. This is similar with earlier studies conducted elsewhere.11,26,27,30–33 In this context, it might be suggested that there is a readiness among female undergraduates to practice ECP which is also supported by an evidence from EDHS 2016.14
In the present study, knowledge of correct timing of ECP (56.5%) was better than prior findings in Jimma (48.6%) and Mizan-Tepi (28.3%) universities of Ethiopia.27,30 However, more than half of the study participants replied that ECP is effective to prevent STIs and I did not know responses combined. Alternatively, the respondents who believed that ECP is not effective to prevent STIs were about two times more likely to use condom than their counterparts (AOR= 2.217; 95% CI, 1.172–4.59). This indicates that female students who knew ECP cannot give protection against STIs would use condom which provides effective protection against disease as well as pregnancy. In line with this, according to a study conducted in Ghana, knowledge of STI prevention determined method of contraception used among high school girls so that those who want to avoid STIs would use condom rather than ECP.34 It is imperative to provide health education on hormonal contraception and risks of STIs/HIV while condom use should be promoted for dual protection against infection and unintended pregnancy. Besides, contraceptive counseling should emphasize the need for condom use among sexually active women not in mutually monogamous relationships with uninfected partners.16
Our findings also showed that slightly more than half (51.6%) of the sexually active students utilized condom while only 46.7% of them believed that condom protects against STI. Furthermore, the students who thought that condom prevents STI were three times more likely to use condom than those who did not believe effectiveness of condom (AOR = 3.17; 95% CI, 1.045–8.646). This is consistent with the results of preceding studies conducted in Ethiopia.26,27 The result suggests that perceived efficacy of condom to prevent STIs is a predictor of condom utilization among female university students. According to a recent study conducted in Ethiopia, intention to use condom was significantly associated with perceived benefit of using condom to prevent STIs and the respondents with high perceived benefit of using condom were about 1.6 times more likely to use condom than their counterparts.52 Likewise, the 2002 Canadian contraception survey revealed that majority of respondents believed condoms were more effective for STI prevention than for pregnancy prevention while 46% of them have ever used condoms primarily for STI prevention.20 Preferences to use condom may be attributed to various factors such as marital status, age, number of sexual partners, knowledge and positive attitudes of condom use, and knowledge and perceived risk of STIs/HIV.29,32,37,38
Moreover, in the current study, female university students who have ever used ECP were 0.32 times less likely to use condom than non-users of ECP (AOR = 0.32; 95% CI, 0.164–0.632). Hence, it could be inferred from this finding that ever practice of ECP adversely affects condom use. In line with this, a number of studies revealed that increased access to and practice of ECP significantly reduced condom utilizations.18–20,26,27,29 Despite the OTC availability of both contraception methods and ECPs are more costly than condom, ECPs are predominantly and repetitively used by young females in Ethiopia.50,51 As the primary goal of most consistent ECP users is to prevent pregnancy rather than STI, they do not necessarily consider condoms.19–21 According to Galavotti et al,18 consistent pills-only users appeared more confident to have low chances of pregnancy than condom-only users. In addition, misbeliefs that ECP can prevent STIs18,20,26,27,29,34 and perceptions that one is not susceptible to STIs/HIV while taking pills-only regimen might contribute to non-use of condoms.18,21 The Canadian contraception survey20 and a national-level study from USA35 indicated also that providing individuals with OTC access to ECP leads to increase STI rates. This can be due to the reason that increased access to ECP may influence a person’s sexual behaviors such as more predisposition to have sex, higher number of sexual encounters and less tendency to use condoms.35 On the contrary, others argued that OTC access to and use of ECP does not increase STI rates and has no effect on condom use22,23 while history of ECP use was strongly correlated with high condom usage, according to another study conducted in Mexico.36
Unintended pregnancy and STIs/HIV remain highly prevalent amongst adolescent girls and women living in sub-Saharan Africa.5,39 Although dual method contraception is highly effective to tackle such problems, few proportion (5.9%) of sexually active students reportedly used dual contraception, in our study. This is lower than figures reported from Canada (13%), Northern California (7%) and Nigeria (20.6%).20,41,42 Reasons of opting to use dual contraception may include having multiple sexual partners, prior STI encounters, fear of contracting infections, history of unintended pregnancy and intentions to avoid pregnancy.20,42 Thus, adolescent girls and young women should be guaranteed the rights to full and unbiased information on STI and HIV risk factors as well as pros and cons of different contraceptive methods.39 This should also include the message that methods other than condoms do not prevent STIs/HIV whereas dual method contraception is an effective option.39,40 More importantly, implementation of comprehensive sexual and reproductive health education on contraception and risks of HIV and other STIs should be ensured in higher education institutions.
Limitations of the study were described as follows:
Firstly, our study population comprised only three private universities in the town so that the results could not be generalized to all ECP users in the study area. Secondly, the study might not be free of information bias as it involved sensitive issues such as sexual activity and sexual risk behavior. Thirdly, cause-effect relationship could not be determined due to the nature of the study design. Nonetheless, this study vividly presented the adverse effect of ECP use on condom utilization and it is the first of its kind to investigate such issue among female university students in western Ethiopia.
Conclusion
In conclusion, the rate of ECP use among female university students was found to be average. History of ECP use, assuming that ECP does not prevent STI and believing that condom protects against STI were factors associated with condom utilization. More specifically, female students who have ever practiced ECP tend to use condom significantly lower than those who had no history of ECP use. As a result, this may lead to increase risky sexual behaviors and STI rates.
In recommendations, sexually active women who use ECPs should also consider condoms for prevention of STIs/HIV and dual method contraception use should be promoted as well. Sexual and reproductive health lessons have to be executed in private universities/colleges as similar as in public universities/colleges in the country. Finally, we would like to endorse prospective researchers to investigate cause-effect relationships between the practice of ECP and condom use.
Abbreviations
AOR, Adjusted Odds Ratio; COR, Crude Odds Ratio; CI, Confidence Interval; DBU, Dandi Boru University; ECP, Emergency Contraceptive Pill; EDHS, Ethiopian Demographic Health Survey; HIV, Human Immunodeficiency Virus; NGU, New Generation University; RVU, Rift Valley University; STI, Sexually Transmitted Infection.
Data Sharing Statement
Additional materials will be available from the corresponding author on any reasonable request.
Ethics Approval and Informed Consent
Ethical clearance was pursued from the institutional review board (IRB) of Institute of Health Sciences of Wollega University to conduct this study. Besides, a letter of permission was written from the research and technology transfer vice president office of Wollega University to the three private Universities. Subsequently, authorization was obtained from deans (executive directors) of the respective Universities to conduct this study in their campuses. This study was conducted in comply with the Declaration of Helsinki. The purpose of the study was explained to the study participants prior to the study commencement and they were assured of the right to refuse participating in or withdraw from the study at any time as well. Consequently, written informed consents were sought from the study participants who aged 18 years and above whereas, parental written consents were obtained for the respondents under 18 years of age, in advance. Also, personal identifiers were avoided from the questionnaire and data collected from the respondents were kept confidential.
Acknowledgments
The authors would like to thank the data collectors, and deans of respective private universities.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave approval to all versions of the article submitted for publication; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The study was conducted by a funding from Wollega University Research and Technology Transfer vice President office.
Disclosure
The authors declare that they have no competing interests.
References
1. World Health Organization Department of Reproductive Health and Research (WHO/RHR) and Johns Hopkins Bloomberg School of Public Health/Center for Communication Programs (CCP), Knowledge for Health Project. Family Planning: A Global Handbook for Providers. Baltimore and Geneva: CCP and World Health Organization; 2018.
2. Trussell J, Raymond EG, Cleland K. Emergency contraception: a last chance to prevent unintended pregnancy. Contemp Readings L Soc Just. 2014;6(2):7–38.
3. World Health Organization. Emergency contraception; 2018. Available from: http://www.who.int/en/news-room/fact-sheets/detail/emergency-contraception.
4. International Consortium for Emergency Contraception (ICEC). Emergency Contraceptive Pills: Medical and Service Delivery Guidelines.
5. Bearak J, Popinchalk A, Ganatra B, et al. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Glob Health. 2020;8:e1152–61. doi:10.1016/S2214-109X(20)30315-6
6. World Health Organization. Abortion; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/abortion.
7. Alene M, Yismaw L, Berelie Y, Kassie B, Yeshambel R, Assemie MA. Prevalence and determinants of unintended pregnancy in Ethiopia: a systematic review and meta-analysis of observational studies. PLoS One. 2020;15(4):e0231012. doi:10.1371/journal.pone.0231012
8. Guttmacher Institute. Ethiopia country profile; 2022. Available from: https://www.guttmacher.org/geography/africa/ethiopia.
9. Joint United Nations Programme on HIV/AIDS (UNAIDS). Global Report: UNAIDS Report on the Global AIDS Epidemic 2012. Geneva: UNAIDS; 2012.
10. Palermo T, Bleck J, Westley E. Knowledge and use of emergency contraception: a multicountry analysis. Int Perspect Sex Reprod Health. 2014;40(2):79–86. doi:10.1363/4007914
11. Hoque ME, Ghuman S. Knowledge, practices, and attitudes of emergency contraception among female university students in South Africa. PLoS One. 2012;7(9):e46346. doi:10.1371/journal.pone.004634
12. Nyambura MG, Kiarie JN, Orang’o O, Okube OT. Knowledge and utilization of emergency contraception pills among female undergraduate students at the University of Nairobi, Kenya. Open J Obstetrics Gynaecol. 2017;7:989–1005. doi:10.4236/ojog.2017.79100
13. Amina MD, Regmi K. A quantitative survey on the knowledge, attitudes and practices on emergency contraceptive pills among adult female students of a tertiary institution in Kaduna, Nigeria. Prim Health Care. 2014;4:1. doi:10.4172/2167
14. Central Statistical Agency (CSA) (Ethiopia) and ICF. Ethiopia Demographic and Health Survey 2016. Rockville: CSA and ICF; 2016.
15. Fikre R, Amare B, Tamiso A, Alemayehu A. Determinant of emergency contraceptive practice among female university students in Ethiopia: systematic review and meta-analysis. Contracept Reprod Med. 2020;5:18. doi:10.1186/s40834-020-00123-8
16. Family Health International (FHI). Hormonal Contraception and HIV. Network. 2007;24(1):3–23.
17. Willard C, Markus JS. Dual protection against unintended pregnancy and sexually transmitted infections: what is the best contraceptive approach? Sex Transm Dis. 2002;29(3):168–174. doi:10.1097/00007435-200203000-00007
18. Galavotti C, Schnell DJ. Relationship between contraceptive method choice and beliefs about HIV and pregnancy prevention. Sex Transm Dis. 1994;21(1):5–7. doi:10.1097/00007435-199401000-00002
19. Traeen B, Lewin B, Sundet JM. Use of birth control pills and condoms among 17-19-year-old adolescents in Norway: contraceptive versus protective behavior? AIDS Care. 1992;4(4):371–380. doi:10.1080/09540129208253108
20. Fisher WA, Boroditsky R, Morris B. The 2002 Canadian Contraception Study: part I. J Obstet Gynaecol Can. 2004;26(6):580–590. doi:10.1016/S1701-2163(16)30377-2
21. Hickey MT, Shedlin MG. Emergency contraceptive pill users’ risk perceptions for sexually transmitted infections and future unintended pregnancy. J Am Assoc Nurse Pract. 2017;1–8. doi:10.1002/2327-6924.12485
22. Raine TR, Harper CC, Rocca CH, et al. Direct access to emergency contraception through pharmacies and effect on unintended pregnancy and STIs. JAMA. 2005;293(1):54–62. doi:10.1001/jama.293.1.54
23. Richard AC, Ralph JD, Gina MW, et al. Oral contraceptive use may not preclude condom use: a study of non-pregnant African-American adolescent females. Sex Transm Infect. 2007;83:216–218. doi:10.1136/sti.2006.022442
24. Kassie BA, Yenus H, Berhe R, Kassahun EA. Prevalence of sexually transmitted infections and associated factors among the University of Gondar students, Northwest Ethiopia: a cross-sectional study. Reprod Health. 2019;16:163. doi:10.1186/s12978-019-0815-5
25. Gebresllasie F, Tsadik M, Berhane E. Potential predictors of risk sexual behavior among private college students in Mekelle City, North Ethiopia. Pan Afr Med J. 2017;28:151. doi:10.11604/pamj.2017.28.151.5370
26. Wasie B, Belyhun Y, Moges B, Amare B. Effect of emergency oral contraceptive use on condom utilization and sexual risk taking behaviors among university students, Northwest Ethiopia: a cross-sectional study. BMC Res Notes. 2012;5:501. doi:10.1186/1756-0500-5-501
27. Mohammed T, Teshale C, Musa S, Gedamu S. The effect of emergency contraception use on condom use: a cross sectional survey among students of Jimma Technical and Vocational Training College, Jimma, Ethiopia. IJPSR. 2015;6(2):219–226.
28. Ahmed FA, Moussa KM, Petterson KO, Asamoah BO. Assessing knowledge, attitude, and practice of emergency contraception: a cross- sectional study among Ethiopian undergraduate female students. BMC Pub Health. 2012;12:110–116. doi:10.1186/1471-2458-12-110
29. Figueiredo R, Segri NJ. Use of male condoms among adolescents with free access at emergency contraception—study among students from the public education system of the Sao Paulo, Brazil. World J AIDS. 2014;4:178–186. doi:10.4236/wja.2014.42023
30. Shiferaw BZ, Gashaw BT, Tesso FY. Factors associated with utilization of emergency contraception among female students in Mizan-Tepi University, Southwest Ethiopia. BMC Res Notes. 2015;8:817. doi:10.1186/s13104-015-1812-6
31. Fekadu Y. Knowledge, attitude and utilization of emergency contraception among health science and medical students of Arba Minch University. J Women Health Care. 2017;6(4). doi:10.4172/2167-0420.1000383
32. Uwamariya J, Nyandwi JB, Mukanyangezi MF, Kadima JN. Sexual activity and emergency contraception among female Students in the University of Rwanda. IJTDH. 2015;8(4):170–177. doi:10.9734/IJTDH/2015/18475
33. Dejene T, Tsion A, Tefera B. Knowledge, attitude and practice of emergency contraceptives among Adama University female students. Ethiop J Health Sci. 2010;20(3):195–202.
34. Yeboah T, Appai TP. Does knowledge of modern contraceptives and sexually transmitted infections affect contraceptive use and sexual behaviour? Evidence from senior high school girls in the Akuapem North Municipality, Ghana. GeoJournal. 2015. doi:10.1007/s10708-015-9667-x
35. Mulligan K. Access to emergency contraception and its impact on fertility and sexual behavior. Health Econ. 2016;25:455–469. doi:10.1002/hec.3163
36. Walker DM, Torres P, Gutierrez JP, Flemming K, Bertozzi SM. Emergency contraception use is correlated with increased condom use among adolescents: results from Mexico. J Adolesc Health. 2004;35(4):329–334. doi:10.1016/j.jadohealth.2004.07.001
37. Muluken D, Maereg W. Predictors of consistent condom use among university students: hierarchical analysis Debre Berhan. Global J Med Public Health. 2012;1(4):23–28.
38. Adih WK, Alexander CS. Determinants of condom use to prevent HIV infection among youth in Ghana. J Adolesc Health. 1999;24:63–72. doi:10.1016/S1054-139X(98)00062-7
39. World Health Organization. Actions for Improved Clinical and Prevention Services and Choices: Preventing HIV and Other Sexually Transmitted Infections Among Women and Girls Using Contraceptive Services in Contexts with High HIV Incidence. Geneva: World Health Organization; 2020.
40. Pazol K, Kramer MR, Hogue CJ. Condoms for dual protection: patterns of use with highly effective contraceptive methods. Public Health Rep. 2010;125(2):208–217. doi:10.1177/003335491012500209
41. Raine T, Minnis AM, Padian NS. Determinants of contraceptive method among young women at risk for unintended pregnancy and sexually transmitted infections. Contraception. 2003;68:19–25. doi:10.1016/S0010-7824(03)00107-0
42. Buraimo O, Simkhada P, Watson P, Taddese HB. Correlates and barriers of dual-method contraception among college youths in Nigeria. J Contracept Stud. 2017;2(2):7. doi:10.21767/2471-9749.100030
43. World Health Organization. Adolescent pregnancy. 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/adolescent-pregnancy.
44. Wang H, Long L, Cai H, et al. Contraception and unintended pregnancy among unmarried female university students: a cross-sectional study from China. PLoS One. 2015;10(6):e0130212. doi:10.1371/journal.pone.0130212
45. Iyanda AE, Dinkins BJ, Osayomi T, Adeusi TJ, Lu Y, Oppong JR. Fertility knowledge, contraceptive use and unintentional pregnancy in 29 African countries: a cross-sectional study. Int J Public Health. 2020;65:445–455. doi:10.1007/s00038-020-01356-9
46. Ehrsson YT, Stenhammar C, Rosenblad A, Akerud H, Larsson M, Tyden T. Self-reported sexually transmitted infections among female university students. Ups J Med Sci. 2016;121(1):45–49. doi:10.3109/03009734.2015.1093568
47. Nzoputam C, Adam VY, Nzoputam O. Knowledge, prevalence and factors associated with sexually transmitted diseases among female students of a Federal University in Southern Nigeria. Venereology. 2022;1:81–97. doi:10.3390/venereology1010006
48. Stenhammar C, Ehrsson YT, Akerud H, Larsson M, Tyden T. Sexual and contraceptive behavior among female university students in Sweden – repeated surveys over a 25-year period. Acta Obstet Gynecol Scand. 2015;94:253–259. doi:10.1111/aogs.12565
49. Ajayi AI, Nwokocha EE, Akpan W, Adeniyi OV, Goon DT. “It’s sweet without condom”: understanding risky sexual behavior among Nigerian female university students. Online J Health Allied Scs. 2017;16(4):9.
50. Both R, Samuel F. Keeping silent about emergency contraceptives in Addis Ababa: a qualitative study among young people, service providers and key stakeholders. BMC Women Health. 2014;14:134. doi:10.1186/s12905-014-0134-5
51. Gold E. DKT Ethiopia’s Post-Pill Emergency Contraceptive: An Assessment of Provider and Customer Attitudes and Behaviors. Addis Ababa: DKT Ethiopia; 2011.
52. Abera H, Tamiru F, Kibret GD. Intention toward condom use and its associated factors among students of Debre Work Senior Secondary and Preparatory School, East Gojjam Zone, Amhara Region, Ethiopia. HIV/AIDS Res Palliat Care. 2017;9:137–143. doi:10.2147/HIV.S130145
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.